")
Back to Journals » Journal of Pain Research » Volume 18
Comparison of Surgical Anesthesia Onset Between Dural-Puncture Epidural and Standard Epidural Techniques for Emergency Cesarean Section: Protocol for a Randomized Controlled Trial
Authors Zhou S , Cao X, Zhou Y, Xu Z
Received 29 December 2024
Accepted for publication 3 May 2025
Published 16 May 2025 Volume 2025:18 Pages 2509—2519
DOI https://doi.org/10.2147/JPR.S514780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Shuangqiong Zhou,* Xiuhong Cao,* Yao Zhou, Zhendong Xu
Department of Anesthesiology, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhendong Xu, Department of Anesthesiology, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, 2699 Gaoke West Road, Shanghai, 201204, People’s Republic of China, Email [email protected]
Purpose: The dural-puncture epidural (DPE) and standard epidural (EP) techniques are well-established methods for neuraxial analgesia during labor. However, there is limited knowledge regarding the conversion of DPE-induced labor analgesia to surgical anesthesia during cesarean sections, particularly regarding efficacy and timing. This study will compare the surgical anesthesia onset time between DPE and EP in parturients undergoing emergency cesarean delivery after conversion from labor analgesia.
Patients and Methods: This double-blind, randomized clinical study will include 124 parturients. Parturients aged ≥ 18 years with singleton pregnancies who request labor analgesia will be randomly assigned to receive either DPE or EP anesthesia in the labor and delivery rooms. Participants will be excluded if they have contraindications to neuraxial anesthesia, back surgery or scoliosis history, significant fetal anomalies, or a known allergy to any of the study medications. Epidural labor analgesia will be maintained using a low concentration of ropivacaine in combination with sufentanil, delivered through the epidural catheter. During delivery, an emergency intrapartum cesarean section following labor analgesia may be necessary among these parturients. Parturients requiring intrapartum cesarean delivery following labor analgesia will be eligible. Epidural extension anesthesia will be administered in the operating room. The primary outcome measure will be the time from chloroprocaine administration to the achievement of a surgical level of anesthesia, defined as a T6 sensory block. Secondary outcomes will include epidural anesthesia quality, incidence of conversion to cesarean section between the two techniques, and maternal and neonatal outcomes.
Conclusion: This study will estimate the onset time to achieve surgical anesthesia during epidural extension using a DPE compared to an EP technique. The results may provide a deeper understanding of the advantages of the DPE technique in labor analgesia, as well as determine the onset time and reliability of anesthesia block during conversion from labor analgesia to cesarean delivery.
Trial Registration: ChiCTR2400089237. Registered September 4, 2024.
Keywords: labor analgesia, parturient, onset time, delivery, intrapartum cesarean delivery
Introduction
Neuraxial analgesia is considered the gold standard for pain management during labor and delivery.1–4 When a parturient fails to deliver vaginally and requires an emergency cesarean section, anesthetics can be administered using the existing epidural catheter previously placed for providing labor analgesia.5
A key benefit of epidural labor analgesia is its ability to be rapidly converted to epidural surgical anesthesia, facilitating cesarean delivery and reducing the risks associated with general anesthesia.6 This is especially crucial during emergency cesarean sections, where prompt anesthesia can enhance surgical efficiency, lower maternal and neonatal risks, and improve maternal outcomes and comfort. Overall, optimizing anesthesia efficiency during emergency cesarean delivery can result in better outcomes for both mother and baby.7–9
The standard epidural (EP) technique involves catheter placement into the epidural space without puncturing the dura mater. This approach is more commonly used for labor analgesia and provides continuous pain relief without the risks associated with dural puncture. The dural-puncture epidural (DPE) technique involves puncturing the dura mater, followed by the infusion of epidural local anesthetic drugs into the epidural space. This technique often provides a more rapid onset of anesthesia than epidural technique, as the puncture of the dura allows for a better distribution of the anesthetic. Recently, DPE has gained popularity.10,11 The use of DPE in labor analgesia has been associated with a more rapid onset of pain relief. Additionally, when combined with programmed intermittent epidural bolus (PIEB) technology, DPE can effectively reduce the volume of analgesic required, without increasing the risk of adverse effects.12,13 Of course, there are different perspectives. Xiao et al14 found that when analgesia was maintained using a PIEB, no significant advantage in analgesia onset with DPE compared to the EP analgesia occurred. However, research on the effects of a DPE on the onset time and reliability of surgical anesthesia block in patients undergoing intrapartum cesarean delivery with epidural extension anesthesia is limited.
Rao et al15 compared anesthesia onset for elective cesarean delivery among DPE, EP, and combined spinal-epidural anesthesia techniques. The results demonstrated that DPE anesthesia provided faster onset and superior block quality than EP anesthesia and that the impact of DPE anesthesia on maternal hemodynamic parameters was less than that of combined spinal-epidural anesthesia during cesarean delivery. Similarly, Sharawi et al16 evaluated the effects of the DPE technique and compared them with those of the EP technique for conversion to epidural anesthesia in elective cesarean deliveries. To simulate the transition during labor analgesia, DPE or EP techniques were implemented approximately 1 hour before entry into the operating room, with maintenance of a certain block level with analgesics. The results demonstrated that the DPE technique achieved a more rapid anesthesia onset, superior block quality, and a more favorable risk-to-benefit ratio compared to the EP technique. However, both studies included only pregnant women undergoing elective cesarean deliveries; therefore, the chosen timing and patient selection may not accurately reflect the urgency and conditions associated with emergency cesarean deliveries. The patency of the DPE puncture site may decrease or the site may even close as labor progresses, potentially slowing the diffusion of medication from the epidural space to the subarachnoid space. Therefore, further research is needed to validate the application of the DPE technique in transitioning to cesarean delivery during labor analgesia.
Accordingly, we designed this prospective, double-blind, multicenter, randomized clinical trial to evaluate whether the DPE technique offers efficacy compared to the EP technique for epidural extension anesthesia in parturients undergoing intrapartum cesarean delivery following labor analgesia. Our hypothesis is that the DPE technique will result in a more rapid onset of surgical anesthesia compared to the EP technique. The primary study objective is to compare the analgesic efficacy and anesthesia management of these two techniques during the transition to cesarean delivery, focusing on pain control, anesthesia effectiveness, and complications. The secondary objectives include evaluating maternal and neonatal outcomes, resource utilization, and the feasibility of implementing these techniques in clinical practice.
Materials and Methods
Study Design
This prospective, double-blind, multicenter randomized clinical study aims to compare the effects of DPE and EP techniques on anesthesia onset time in parturients who require conversion to cesarean delivery during labor analgesia. The protocol will be in accordance with the Standard Protocol Items: Recommendations for Interventional Trials reporting guidelines.17 Outcome evaluators, data managers, and statisticians will remain unaware of group allocations. A schematic representation of the study is provided in Figure 1, whereas the timeline for participant enrollment, interventions, and evaluations is detailed in Table 1.
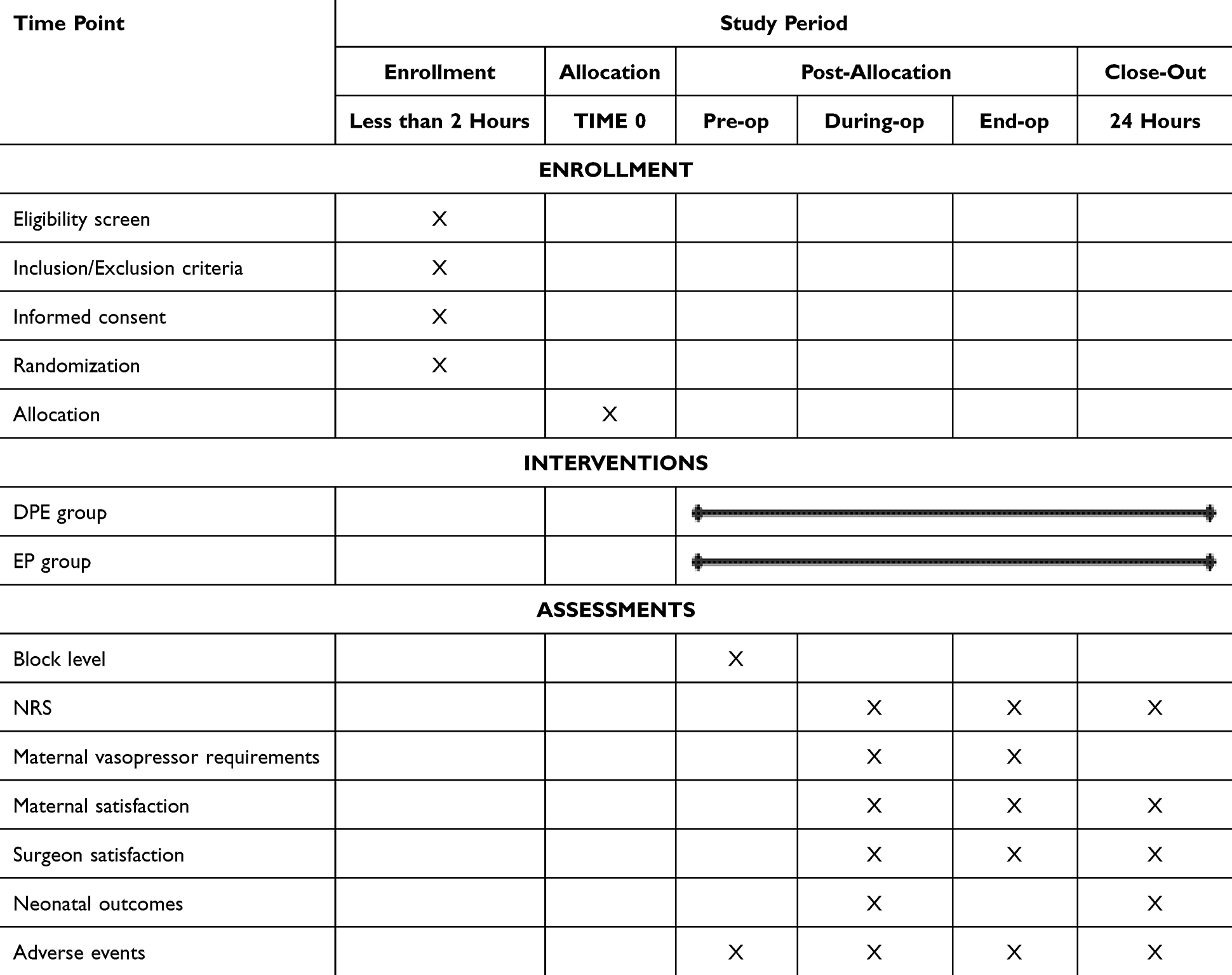 |
Table 1 Schedule of Enrollments, Interventions, and Assessments |
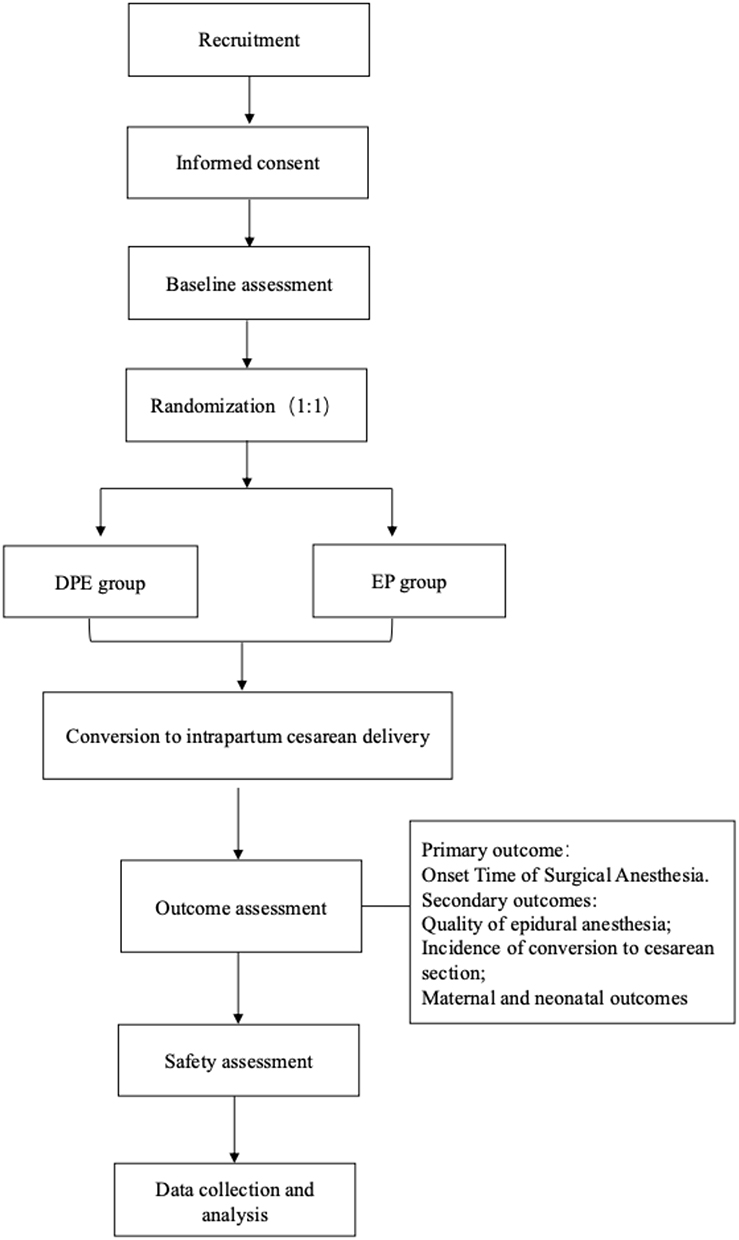 |
Figure 1 Study flowchart. Abbreviations: DPE, dural-puncture epidural; EP, epidural procedure. |
Recruitment
Participants will be recruited from the Shanghai First Maternity and Infant Hospital, Shanghai Jiading Maternal and Child Health Hospital, and the International Peace Maternity and Child Health Hospital, China. Participant eligibility will be assessed by the researchers according to the criteria outlined in the subsequent Inclusion and Exclusion Criteria subsection. The Shanghai First Maternity and Infant Hospital will conduct interventions and take responsibility for data management.
Registration and Ethical Considerations
This trial has been registered in the Chinese Clinical Trial Registry (Registration number: ChiCTR2400089237). The study protocol has been approved by the Ethics Committee of Shanghai First Maternity and Infant Hospital, Shanghai, China (KS2407). This trial will be conducted in accordance with the Declaration of Helsinki.
Epidural analgesia executors will explain the study details to the eligible parturients and provide them with the informed consent document. After the parturients sign the consent documents, they will be enrolled in the study. Participation is entirely voluntary, and the parturients retain the right to withdraw from the study at any point without any consequences. All personal and medical information related to the participants will be handled with strict confidentiality and in compliance with privacy regulations.
Inclusion and Exclusion Criteria
The enrollment criteria include parturients with age 18–45 years, singleton pregnancies, and gestational age ≥37 weeks, assessed to deliver vaginally, with the American Society of Anesthesiologists classification II, in active labor with cervical dilation <5 cm, and with understanding of the research process and ability to cooperate to complete the trial.
The exclusion criteria are individuals with contraindications for neuraxial anesthesia (such as coagulation disorders, scoliosis and lumbar surgery history, lower extremity neurological dysfunction, poorly controlled psychosomatic disorder), allergy to ropivacaine or sufentanil, hypertension, preeclampsia, diabetes, or cardiopulmonary disease, fetal distress or fetal abnormalities, refusal to participate in the trial, and use of other analgesics during the prior 4 hours of labor.
Dropout Criteria
Follow-up assessments will be discontinued under the following circumstances: failure to correctly position the catheter in the intended point, accidental dural puncture, failure to achieve effective labor analgesia, occurrence of severe complications, anesthetic incidents, or anaphylactic reactions, and participant withdrawal from the study.
Allocation and Blinding
Eligible primiparous women who meet the inclusion criteria will be randomly assigned to receive either EP or DPE analgesia. Thereafter, parturients who undergo emergency cesarean delivery after receiving labor epidural analgesia will be included in this study.
The randomized sequence will be generated using Excel (Microsoft, Redmond, WA, USA). Based on the sequence, parturients who meet the inclusion and exclusion criteria will be assigned to either the EP or DPE group in a 1:1 ratio. The allocation information will be concealed with opaque, sealed envelopes to maintain blinding. Epidural procedures will be performed by the attending anesthesiologist. The anesthesiologist will use ultrasound to locate the L3-4 intervertebral space before performing the puncture. The team performing the epidural technique will not be allowed to participate in the subsequent stages of the study.
The study will be conducted using a double-blind design. The personnel administering labor analgesia will not be involved in subsequent data collection. Due to the same puncture site (L3/4) and the identical appearance and model of the indwelling epidural catheter, blinding can be effectively achieved. Anesthesia providers managing the conversion to cesarean delivery, outcome assessors, data analysts, and study participants will remain blinded to group assignments.
Epidural Placement
Participants will receive epidural analgesia in the designated labor room and delivery ward according to random assignment. The procedure will be performed at the L3/4 interspace in the lateral position, using a 17-gauge Touhy needle from a midline approach with a saline loss-of-resistance technique. In the DPE group, the dura will be punctured using a 25-gauge, pencil-point needle (Pencan; B Braun, Melsungen, Germany) with a needle-through-needle technique, and spontaneous reflux of cerebrospinal fluid will be confirmed. In both groups, a flexible 19-gauge, spring closed-tip catheter (Perfix; B Braun) will be inserted 5 cm into the epidural space. To exclude intravascular or intrathecal placement, a test dose will be administered with 3 mL of 1.5% lidocaine and 1:200 000 epinephrine. Approximately 5 min after a negative test dose, the participants will receive up to 10 mL of 0.1% ropivacaine with 0.5 μg/mL sufentanil. Analgesia maintenance will be applied using a programmed intermittent bolus mode. The bolus will be set as 10 mL, with an interval time of 50 min.18 For patient-controlled analgesia, the impact dose will be set as 8 mL, and the locking time will be 15 min (Apon MC ZZB-I; Jiangsu Apon Medical Technology, Jiangsu Province, China).
Twenty min following administration of the loading dose (10 mL), if the numerical rating scale (NRS) score exceeds 3, an additional bolus (8 mL) will be administered. Thirty minutes after the loading dose, if the NRS score remains above 3 or an asymmetric block is observed, the patient will be classified as having analgesia failure, and the parturient will be withdrawn from the study. Parturients with successful blocks who experience breakthrough pain (pain that is intolerable to the parturients) can press the patient-controlled analgesia button to receive an additional bolus of 8 mL. The next programmed bolus will be subsequently triggered after 50 min.
The sensory blockade level to pinprick will be evaluated bilaterally along the mid-clavicular line from caudal to cephalad, and the upper sensory blocking level will be defined as the point the patient can no longer feel sharp sensation. The level corresponding to the umbilicus will be considered the T10 dermatomal level.
Protocol for Epidural Extension Anesthesia
Parturients requiring conversion to intrapartum cesarean section during labor will be transferred to the operating room, where standard electrocardiographic monitoring will be performed, and sensory and motor block will be assessed using the modified Bromage score. Fetal heart rate will be monitored intermittently prior to the start of surgery.
Epidural extension anesthesia will be standardized. A co-load of lactated Ringers’ solution (500 mL) will be administered intravenously during approximately 15 min. After confirming negative aspiration of the epidural catheter, 5 mL of 3% chloroprocaine will be administered as a test dose, and the patient will be monitored for signs of intravascular injection or accidental intrathecal injection. If no abnormal signs are observed within 3 min, an additional 15 mL of 3% chloroprocaine will be delivered during approximately 1 min. The initiation of this injection will be defined as time 0 and the beginning of epidural extension. A blinded investigator will assess the block at 1-min intervals, initially moving from a caudal to a cranial direction and then more frequently as the block intensifies. The pain measurement tool in the combined spinal-epidural anesthesia kit will provide the standardized sharp-pain stimulus.
If a T6 bilateral block is not achieved within 10 min after the start of epidural extension, 5-mL aliquots of epidural 3% chloroprocaine will be administered every 5 min, up to a total maximum cumulative dose of 30 mL. If the desired T6 block is not reached within 20 min, the attending anesthesiologist will employ a different anesthetic technique according to clinical discretion. Maternal hypotension (SBP reduction >20% preoperative baseline value or SBP <90 mm Hg) will be treated with 40 µg of phenylephrine if the HR is >60 bpm and with 6 mg of ephedrine if the HR is ≤60 bpm.
Outcomes
This trial aims to compare the surgical anesthesia onset time between the DPE and EP techniques in parturients undergoing emergency cesarean delivery after conversion from labor analgesia.
Baseline Data and Expected Parameters
Demographic data, including age, height, body weight, gestational week, blood pressure, heart rate, and oxygen saturation, will be systematically recorded before epidural labor analgesia.
Primary Outcome
The primary outcome is surgical anesthesia onset time. The time from chloroprocaine administration to achieving a T6 sensory block will be recorded in minutes. A T6 sensory block will be determined by the loss of sharp sensation to a pinprick.
Secondary Outcomes
The secondary outcomes include: (1) sensory block level upon transfer to the operating room; (2) failure to achieve a surgical block within 15 min of epidural extension anesthesia; (3) requirement for intraoperative analgesia supplementation; (4) requirement for repeat neuraxial procedure; (5) conversion to general anesthesia; and (6) incidence of conversion to intrapartum cesarean section between the two techniques. The intraoperative analgesia supplementation rate is defined as the need of any rescue medication to manage discomfort or pain during intrapartum cesarean delivery. The choice of medication will be at the anesthesiologist’s clinical discretion. All components of the composite outcome will be treated as binary measures, and the presence of any event will be considered positive for the secondary outcome (collapsed composite).
Other secondary outcomes include maternal satisfaction and surgeons satisfaction regarding the block using a scale from 0 (very dissatisfied) to 10 (very satisfied); pain score during surgery; adverse events (AEs) such as self-reporting of nausea, vomiting, or pruritus; timings including the duration from primary outcome to surgery start and surgery duration; maternal vasopressor requirements (intraoperative dose administered); epidural block assessments; neonatal outcomes (Apgar score at 1 and 5 min and umbilical cord blood gasses); and other AEs, including local anesthetic systemic toxicity, high spinal block levels (characterized by exaggerated cranial spread of spinal anesthesia resulting in hand weakness, breathing difficulties, and in severe cases, unconsciousness); and post-dural puncture headache assessed on postpartum day 3.
The quality of epidural anesthesia will be measured by the need for supplemental analgesia and will be defined as the requirement for additional boluses of local anesthetic or intravenous opioid administration.
The incidence of cesarean section transfer will be defined as the frequency and cause of cesarean section transfer during labor analgesia and will be compared between the two techniques.
The maternal and neonatal outcomes will be determined using assessments of maternal hemodynamic stability, nausea, vomiting, pruritus, and Apgar scores of the newborns at 1 and 5 min.
Sample Size Determination
The primary outcome of the study is the time to achieve a T6 sensory block following the administration of the epidural medication. According to Sharawi et al,16,19 when comparing different local anesthetics for epidural anesthesia during elective cesarean section conversion and the epidural anesthesia onset time between DPE and EP techniques during cesarean section conversion, the mean onset time is 655 ± 258 s or 655 s (437–926 s) for chloroprocaine and 422 s (290–546 s) for the DPE group. Based on our preliminary data, we hypothesize that a difference of at least 2 min in anesthesia onset between the EP and DPE groups will represent a clinically significant difference, with a standard deviation of 3 min.
By setting the two-tailed alpha at 0.05 and the power at 0.9 (90% power), a sample size of 49 participants per group is warranted. Considering potential dropout and other unforeseen factors, at least 62 participants should be enrolled in the study.
Statistical Analyses
Statistical analyses will include analyses of numerical variables, categorical variables, and time-to-event variables. Missing data will be handled using appropriate imputation techniques. Additionally, we will compare participant baseline characteristics of those with and without missing data to assess whether the missingness is related to certain study variables.
Data will be documented and analyzed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). The primary analysis will adhere to the intention-to-treat principle. Normally distributed variables will be presented as mean ± standard deviation, whereas non-normally distributed variables will be reported as median (interquartile range). The independent t-test and the Wilcoxon rank-sum test will be employed to compare differences between the two groups. Categorical data, such as the incidence of side effects, will be expressed as percentages and analyzed using the chi-square test or Fisher’s exact test. A Kaplan–Meier survival analysis, accompanied by Log rank tests, will be utilized to compare the time to the loss of sharp sensation at the T6 dermatome between the two groups.
A Cox regression model will be employed to compare the rate of T6 sharp sensation block between the two groups, adjusted for age, body mass index, race and ethnicity, surgical indications, epidural bolus dose in the labor ward, epidural infusion duration, and preoperative sensory and motor block. A univariate logistic regression analysis will be used to assess the secondary composite outcomes of epidural anesthesia quality. Continuous data between the two groups will be compared using the Wilcoxon rank-sum test. Binary or categorical variables will be compared using the chi-square (χ2) or Fisher’s exact test. P < 0.05 will be considered statistically significant.
Adverse Event Report
The safety evaluation indicators include the occurrence date, frequency, severity, and duration of AEs during the treatment course. In this trial, AEs associated with DPE and EP will primarily include maternal hypotension, pruritus, nausea, vomiting, local anesthetic systemic toxicity, post-dural puncture headache, high spinal block levels, and other discomforts. AEs occurring throughout the study will be systematically assessed and documented by the investigators. In the event of an AE, prompt emergency management will be initiated. For serious AEs, investigators are required to immediately report the incident to the principal investigator and the institutional ethics committee, who will determine whether the participant should be withdrawn from the study.
Quality Control, Data Management, and Monitoring
Before recruitment, the research team will undergo comprehensive clinical training to ensure the smooth progression of the study. This training will include a thorough review of the study protocol, standard operating procedures, and evaluation scales. Each clinical researcher will be familiarized with the study processes and specific implementation guidelines to enhance internal consistency of observations, thereby ensuring the reliability of the study’s conclusions. All interventions will be performed by experienced anesthesiologists. Additionally, outcome assessors will receive standardized training to accurately record outcome measures and consistently complete the case report forms (CRFs).
All outcomes and findings from the clinical study will be validated by participants and cross-verified to guarantee data reliability and authenticity. Data will be meticulously collected and recorded in the CRFs, with a secondary review conducted by two independent investigators, both blinded to the randomization. Data quality will be monitored regularly by research assistants and overseen by study monitors. The original CRFs, along with all other study documentation, will be securely stored at the Shanghai First Maternity and Infant Hospital to ensure integrity and confidentiality.
Discussion
This randomized controlled trial aims to compare the effects of DPE and EP on anesthesia onset time for intrapartum cesarean delivery following conversion from labor analgesia. The primary findings are expected to provide valuable insights into optimal anesthesia management for intrapartum cesarean delivery, where rapid and effective anesthesia is crucial. This study will focus on the practicality of DPE use during the labor-to-cesarean transition and represents the first randomized clinical trial to compare DPE use for conversion to surgical anesthesia during an emergency cesarean delivery.
Based on previous studies, we anticipate that the DPE technique will result in faster anesthesia onset compared to EP in scenarios of labor epidural analgesia extended for intrapartum cesarean delivery. The potential benefits of DPE are grounded in its ability to enhance the spread of local anesthetics, resulting in quicker and more reliable surgical anesthesia. Faster surgical anesthesia onset can reduce reliance on additional anesthetic interventions, thereby improving maternal and neonatal outcomes, particularly in urgent situations.
The DPE technique, which creates an “epidural-to-spinal conduit”, has demonstrated advantages in labor analgesia, including faster analgesia onset, better sensory block, and reduced need for supplemental doses.20 However, studies comparing DPE and EP techniques for intrapartum cesarean delivery anesthesia, especially regarding onset time, are limited. The study conducted by Sharawi et al16 on elective cesareans found that the DPE technique provided faster anesthesia and better block quality than the EP technique; however, their study was limited to pregnant women undergoing elective cesarean delivery, with the DPE technique performed approximately 1 h before entering the operating room. Regrettably, due to the short observation-interval, their study did not account for the patency of the DPE puncture as labor progressed.
Few studies have specifically examined the role of DPE in cesarean delivery anesthesia following conversion from labor analgesia. We designed this clinical trial to validate the applicability of DPE in transitioning to cesarean delivery during labor analgesia. This study aims to provide critical data on whether the benefits of DPE during labor indicate a faster surgical anesthesia onset during cesarean sections.
We believe that the findings of this study will be clinically significant and relevant for patients requiring emergent cesarean delivery under epidural extension anesthesia. A recent study by Palmer et al21 evaluated operating room-to-incision times for emergency cesarean deliveries (those involving an immediate threat to the life of the mother or fetus) based on the anesthetic technique used. Their study found that general anesthesia is associated with the shortest operating room-to-incision time (6 min) and with the poorest neonatal outcomes. Furthermore, some studies suggest that general anesthesia may be a risk factor for postpartum depression in mothers.22–25 Although previous research concerning scheduled cesarean deliveries has been conducted, our study will be set within the clinical context of intrapartum cesarean delivery and provides important insights about the selection of anesthesia techniques during labor.
Study Limitations
Despite its rigorous design, this study has potential limitations. One is the urgency of a cesarean section after conversion from labor analgesia. For an immediate threat to the life of the woman or fetus, general anesthesia may be prioritized due to time constraints, leading to missed cases. Additionally, variability in physician experience across different hospitals may influence the outcomes. To minimize these biases, we will provide standardized training to all participating physicians and implement uniform protocols across study sites. This study adopts a randomized controlled design, which enhances its scientific rigor. The random assignment of participants to the DPE and EP groups should minimize selection bias. Additionally, the double-blind design ensures that both the researchers and participants are unaware of the group assignments, further reducing observation bias. By involving multiple centers, we expect to increase the external validity of the study, making the results more widely applicable. The current study is limited to a 24-hour postoperative follow-up period because any potential technical differences between the two approaches are generally expected to manifest within this timeframe.
Conclusion
This study aims to determine whether DPE provides faster and higher-quality anesthesia than that of EP when converting from labor analgesia to cesarean delivery. The results will offer valuable insights for optimizing obstetric anesthesia and improving maternal and neonatal outcomes. The findings of this study could pave the way for more personalized obstetric anesthesia protocols tailored to the specific needs of parturients.
Abbreviations
AE, adverse event; CRF, case report form; DPE, dural-puncture epidural; EP, standard epidural technique; NRS, numerical rating scale; PIEB, programmed intermittent epidural bolus.
Data Sharing Statement
This is the protocol of an ongoing clinical trial; therefore, to date, there are no data available. After completion of this trial, data requested for public purposes will be provided.
Ethics Approval and Informed Consent
This trial has been registered at the Chinese Clinical Trial Registry (Registration number: ChiCTR2400089237). The study protocol has been approved by the Ethics Committee of Shanghai First Maternity and Infant Hospital, Shanghai, China (KS2407). This trial will be conducted in accordance with the Declaration of Helsinki. Before epidural analgesia, investigators who have been trained for the study will assess patients with the inclusion and the exclusion criteria. Patients who meet the inclusion criteria will be invited to this study. Investigators in each center will adequately explain this trial to interested potential participants in detail and provide them with the informed consent form. Participants should be fully informed that they have the right to decide whether to participate or not. The informed consent form will be signed by the participant or his/her trustee or guardian and may be withdrawn at any time during the trial. Written informed consent and the patient’s baseline data will be obtained before randomization.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, including conception, study design, execution, or all these aspects; took part in drafting, revising, or critically reviewing the article; agree on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Shuangqiong Zhou and Xiuhong Cao contributed equally to this work.
Funding
This work was supported by the grants of Science and Technology Commission of Shanghai Municipality (22Y11905900).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nanji JA, Carvalho B. Pain management during labor and vaginal birth. Best Pract Res Clin Obstet Gynaecol. 2020;67:100–112. doi:10.1016/j.bpobgyn.2020.03.002
2. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 209: obstetric analgesia and anesthesia. Obstet Gynecol. 2019;133(3):e208–e225. doi:10.1097/AOG.0000000000003132
3. Guglielminotti J, Landau R, Daw J, Friedman AM, Chihuri S, Li G. Use of labor neuraxial analgesia for vaginal delivery and severe maternal morbidity. JAMA Network Open. 2022;5(2):e220137. doi:10.1001/jamanetworkopen.2022.0137
4. Kearns RJ, Kyzayeva A, Halliday LOE, Lawlor DA, Shaw M, Nelson SM. Epidural analgesia during labour and severe maternal morbidity: population based study. BMJ. 2024;385:e077190. doi:10.1136/bmj-2023-077190
5. Hawkins JL. Epidural analgesia for labor and delivery. N Engl J Med. 2010;362(16):1503–1510. doi:10.1056/NEJMct0909254
6. Liang Z, Zhou T, Wang M, Li Y. Neonatal outcomes when intravenous esketamine is added to the parturients transferred from labor analgesia to emergency cesarean section: a retrospective analysis report. BMC Anesthesiol. 2023;23(1):168. doi:10.1186/s12871-023-02132-x
7. Gosset M, Ilenko A, Bouyou J, Renevier B. Emergency caesarean section. J Visc Surg. 2017;154(1):47–50. doi:10.1016/j.jviscsurg.2016.09.012
8. Fernandes NL, Dyer RA. Anesthesia for urgent cesarean section. Clin Perinatol. 2019;46(4):785–799. doi:10.1016/j.clp.2019.08.010
9. Heller G, Bauer E, Schill S, et al. Decision-to-delivery time and perinatal complications in emergency cesarean section. Dtsch Arztebl Int. 2017;114(35–36):589–596. doi:10.3238/arztebl.2017.0589
10. Gunaydin B, Erel S. How neuraxial labor analgesia differs by approach: dural puncture epidural as a novel option. J Anesth. 2019;33(1):125–130. doi:10.1007/s00540-018-2564-y
11. Contreras F, Morales J, Bravo D, et al. Dural puncture epidural analgesia for labor: a randomized comparison between 25-gauge and 27-gauge pencil point spinal needles. Reg Anesth Pain Med. 2019;44:750–753. doi:10.1136/rapm-2019-100608
12. Song Y, Du W, Zhou S, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg. 2021;132(4):971–978. doi:10.1213/ANE.0000000000004768
13. Cappiello E, O’Rourke N, Segal S, Tsen LC. A randomized trial of dural puncture epidural technique compared with the standard epidural technique for labor analgesia. Anesth Analg. 2008;107(5):1646–1651. doi:10.1213/ane.0b013e318184ec14
14. Yao H-Q, Qian J, Dong FY, et al. Comparison of the dural puncture epidural and the standard epidural techniques in patients having labor analgesia maintained using programmed epidural boluses: a prospective double-blinded randomized clinical trial. Reg Anesth Pain Med. 2024:rapm–2024–105468. doi:10.1136/rapm-2024-105468
15. Rao W-Y, Xu F, Dai S-B, et al. Comparison of dural puncture epidural, epidural and combined spinal-epidural anesthesia for cesarean delivery: a randomized controlled trial. Drug Des Devel Ther. 2023;17:2077–2085. doi:10.2147/DDDT.S415684
16. Sharawi N, Williams M, Athar W, et al. Effect of dural-puncture epidural vs standard epidural for epidural extension on onset time of surgical anesthesia in elective cesarean delivery: a randomized clinical trial. JAMA Network Open. 2023;6(8):e2326710. doi:10.1001/jamanetworkopen.2023.26710
17. Chan A-W, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Rev Panam Salud Publica. 2015;38(6):506–514.
18. Yao H-Q, Huang J-Y, Deng J-L, et al. Randomized assessment of the optimal time interval between programmed intermittent epidural boluses when combined with the dural puncture epidural technique for labor analgesia. Anesth Analg. 2023;136(3):532–539. doi:10.1213/ANE.0000000000006201
19. Sharawi N, Bansal P, Williams M, Spencer H, Mhyre JM. Comparison of chloroprocaine versus lidocaine with epinephrine, sodium bicarbonate, and fentanyl for epidural extension anesthesia in elective cesarean delivery: a randomized, triple-blind, noninferiority study. Anesth Analg. 2021;132(3):666–675. doi:10.1213/ANE.0000000000005141
20. Chau A, Bibbo C, Huang -C-C, et al. Dural puncture epidural technique improves labor analgesia quality with fewer side effects compared with epidural and combined spinal epidural techniques: a randomized clinical trial. Anesth Analg. 2017;124(2):560–569. doi:10.1213/ANE.0000000000001798
21. Palmer E, Ciechanowicz S, Reeve A, Harris S, Wong DJN, Sultan P. Operating room-to-incision interval and neonatal outcome in emergency caesarean section: a retrospective 5-year cohort study. Anaesthesia. 2018;73(7):825–831. doi:10.1111/anae.14296
22. Chen Y-C, Liang F-W, Ho C-H, et al. Anesthesia for cesarean delivery and subsequent depression: a nationwide retrospective cohort study. J Affect Disord. 2024;364:108–115. doi:10.1016/j.jad.2024.07.147
23. Hung K-H, Tsao S-L, Yang S-F, et al. Association of general anesthesia and neuraxial anesthesia in caesarean section with maternal postpartum depression: a retrospective nationwide population-based cohort study. J Pers Med. 2022;12(6):970. doi:10.3390/jpm12060970
24. Guglielminotti J, Li G. Exposure to general anesthesia for cesarean delivery and odds of severe postpartum depression requiring hospitalization. Anesth Analg. 2020;131(5):1421–1429. doi:10.1213/ANE.0000000000004663
25. Guglielminotti J, Monk C, Russell MT, Li G. Association of general anesthesia for cesarean delivery with postpartum depression and suicidality. Anesth Analg. 2024. doi:10.1213/ANE.0000000000007314
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.