")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Correlation Between Systemic Immune Inflammatory Index and Suicidal Attempt in Patients with First-Episode Untreated Depression and its Risk Factors
Authors Wu Y, Jiang W, Chen M, Jiang Q, Huang H, Guo W, Yuan Y
Received 19 January 2025
Accepted for publication 28 March 2025
Published 11 April 2025 Volume 2025:21 Pages 827—839
DOI https://doi.org/10.2147/NDT.S512964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Yigao Wu,1,2,* Wenhao Jiang,1,* Man Chen,2 Qin Jiang,2 Huilan Huang,2 Wenbin Guo,3 Yonggui Yuan1
1Department of Psychiatry and Psychosomatics, Zhongda Hospital, School of Medicine, Jiangsu Provincial Key Laboratory of Brain Science and Medicine, Southeast University, Nanjing, People’s Republic of China; 2Department of Medical Psychology, The First Affiliated Hospital of Wannan Medical College, Wuhu, People’s Republic of China; 3Department of Psychiatry, National Clinical Research Center for Mental Disorders, and National Center for Mental Disorders, The Second Xiangya Hospital of Central South University, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yonggui Yuan, Department of Psychiatry and Psychosomatics, ZhongDa Hospital, School of Medicine, Jiangsu Provincial Key Laboratory of Brain Science and Medicine, Southeast University, No. 87 Dingjiaqiao, Gulou District, Nanjing, 210009, People’s Republic of China, Tel +86-025-83285124, Email [email protected]
Objective: To examine the relationship between the systemic immune inflammatory index (SII) and suicide attempts (SA) in individuals experiencing their first episode of major depressive disorder (MDD).
Methods: A retrospective analysis of 338 MDD patients (2020– 2023) at the First Affiliated Hospital of Wannan Medical College and 76 healthy controls (HC) was conducted. MDD patients were categorized based on their history of SA. Differences in SII and clinical characteristics were analyzed, and a receiver operating characteristic (ROC) curve was used to determine the optimal SII cutoff for predicting SA. Binary logistic regression identified independent risk factors associated with SA.
Results: MDD patients exhibited higher levels of neutrophils, platelets, and SII compared to HC (all p< 0.05). SA Patients had higher HDRS scores, neutrophil counts, mean platelet counts, and SII values compared to those without SA (all p< 0.05). ROC analysis identified an optimal SII cutoff of 515.3, with 67% sensitivity, 70% specificity, and an area under the curve (AUC) of 0.692. After adjusting for gender, age, body mass index, disease duration, and quality of life, individuals with elevated SII values were 8.318 times more likely to have recent SA (OR=8.318, 95% CI: 3.767– 17.546, p< 0.05). Patients with high SII values were 14.101 times more likely to have recent SA compared to those with low SII values (OR=14.101, 95% CI: 5.356– 34.235, p< 0.05). However, high SII was not identified as a significant risk factor for previous SA (OR=0.607, 95% CI: 0.061– 4.961, p> 0.05).
Conclusion: SII represents a cost-effective and accessible method for evaluating suicide risk in patients with MDD.
Keywords: systemic immune inflammatory index, first-episode, major depressive disorder, suicide attempts, immune
Introduction
Depression is a common mental disorder marked by enduring feelings of sadness, frequently coupled with cognitive impairments and decreased levels of involvement.1 In severe cases, it can result in self-harm, suicide, and other dangerous behaviors.2 The etiology of depression is complex and multifaceted. Current research on the subject encompasses genetic factors, biochemistry, neuroendocrine dysfunction, neuroplasticity, neuroelectrophysiology, neuroimaging, and psychosocial factors.3–5 Despite extensive studies in these areas, a comprehensive mechanism that fully explains the origins of depression has yet to be established.
The issue of suicide is a significant public health problem on a global scale. According to statistics, the number of people who die of suicide every year in the world (about 800,000 people) accounts for 1.5% of the total number of deaths every year (data from WHO).6 Among those at risk of suicide, depression is the most prevalent underlying condition. The suicidal tendencies of individuals with depression pose challenges in effectively treating the mental illness and place significant strain on families and society.7 Current research predominantly focuses on the social psychology aspects of suicidal behavior in individuals with depression, with limited exploration into the biological mechanisms. Previous research has shown that changes in brain structures in specific regions, impaired functioning of brain circuits, and imbalance in important neurobiological stress response mechanisms, like the immune system and HPA axis, are associated with the onset of depression and later suicidal tendencies.8,9 Additionally, alterations in monoamine neurotransmitters, specifically 5-HT, BDNF, nerve growth factor, as well as neuroplasticity, have also been linked to suicidal inclinations.10–12 However, the precise pathogenesis of suicidal behavior in depression remains unclear, and reliable biomarkers for predicting such behavior are lacking at this stage.
In recent years, the immune system has garnered considerable attention in the pathophysiological mechanisms of suicidal behavior. Suicide attempts are considered to be closely related to a pro-inflammatory state, and an increasing number of studies have indicated that immune system dysfunction may be associated with the suicidal vulnerability of patients with depression.13 Specifically, multiple studies have found that the levels of inflammatory cytokines are significantly increased in patients with depression, and these cytokines not only participate in the pathogenesis of depression but may also promote suicidal behavior.14,15 For example, the study by Black et al showed that the levels of IL-1β and IL-6 in the post-mortem brain tissue of suicide victims were significantly increased, while the level of IL-8 in the cerebrospinal fluid was decreased, indicating that cytokines may play an important role in suicidal behavior.16 In addition, the study by Janelidze et al also found that the levels of IL-6 and TNF-α were significantly higher in depressed patients with a history of suicide attempts than in those without suicidal ideation and in healthy controls.17–19 However, although these inflammatory cytokines are considered to be potential biomarkers, their high detection costs and the difficulty in obtaining results quickly limit their widespread application in clinical practice. Therefore, it is particularly important to find a more economical, readily available, and effective biomarker.20
The systemic immune inflammation index (SII), an emerging inflammatory biomarker, is calculated based on the counts of neutrophils, lymphocytes, and platelets, and can reflect the body’s immune-inflammatory status. SII has shown promising applications in the diagnosis and prognosis of various diseases, including cardiovascular diseases, infectious diseases, and certain cancers.21 Recent studies have also indicated that SII levels are associated with the severity of major depressive disorder (MDD) and poor prognosis.22 However, research on the relationship between SII and suicidal behavior in patients with depression is still relatively limited. This study aims to explore the correlation between SII levels and suicide attempts (SA) in patients with first-episode, untreated MDD, in order to assess whether SII can serve as a biomarker for suicide risk in patients with MDD.23
Although there is potential for SII to predict depression, there is limited research on its connection with suicidal behavior. This research aimed to explore the relationship between SII and prior suicidal attempts in drug-naïve patients experiencing their first episode of MDD at our hospital, in order to determine if SII can serve as a biomarker for past suicidal behavior in individuals with MDD.
Materials and Methods
Inclusion and Exclusion Criteria of Clinical Information and Research of Participants
The research centered on individuals going through their initial bout of MDD and receiving outpatient treatment at the First Affiliated Hospital of Wannan Medical College in Anhui Province from November 2020 to November 2023. Healthy volunteers were also recruited during this time frame.
The difference of exclusion criteria between the depression group and the healthy control group aims to control the inflammatory related confounding factors (depression group) and ensure the baseline health status of the control group (healthy control group), so as to enhance the effectiveness of the comparison between the two groups:
Patients with Depression
Inclusion criteria: (1) 18–55 years old and right-handed; (2) Patients diagnosed with MDD based on the ICD-10 diagnostic criteria,24 confirmed by a psychiatrist or higher level of medical professional, and who have not yet received any form of medication, physical therapy, or psychological treatment; (3) Willing and able to cooperate in completing various tests and examinations.
Exclusion criteria: (1) Individuals may also have other mental disorders that meet criteria for additional mental disorders as outlined in the ICD-10; (2) The patient is classified as obese, with a BMI exceeding 30 kg/m2 (Obese patients were excluded to avoid the potential impact of adipose tissue associated inflammation on SII); (3) The patient did not quit smoking, that is, the patient smoked more than or equal to 10 cigarettes a day (Patients with smoking ≥ 10 cigarettes/day were excluded because they may confuse the association between SII and suicidal behavior through pro-inflammatory effects); (4) Having tumors, diabetes, or other serious physical diseases (Patients with metabolic diseases such as diabetes were excluded to avoid the interference of their chronic inflammatory state on the research results); (5) Currently receiving immunosuppressive agents or related anti-inflammatory drugs for treatment.
Healthy Control Group
Inclusion criteria: (1) 18–55 years old and right-handed; (2) Not diagnosed with any depressive disorder according to ICD-10 criteria; (3) No history of mental illness; (4) No serious physical diseases; (5) No current suicidal thoughts or previous SA.
Exclusion criteria: (1) No family history of mental illness; (2) History of infection or immune system-related diseases in the past 2 weeks; (3) Pregnant women and women who are breastfeeding; (4) Currently or in the past 6 months Contains psychoactive substance dependence or abuse.
Approval for this study was obtained from the Ethics Committee of the First Affiliated Hospital of Wannan Medical College. The research adhered to ethical principles outlined in the Declaration of Helsinki (Ethical Approval Number: 2023–69).
Informed consent, duly signed by the eligible patients and their parents, was collected, with an option for participants to withdraw from the study anytime. Initially, 402 cases were considered, with 45 cases excluded for not meeting inclusion criteria, 7 cases were excluded because of incomplete registration information or lack of necessary clinical data, and 12 cases excluded due to personal or illness-related factors. Finally, this study analyzed the information of 338 depressed patients, as shown in Figure 1.
 |
Figure 1 Flow chart of subjects in depression group. |
The control group comprised 76 healthy volunteers who met the inclusion criteria for the healthy control group. Their basic information, including age, gender, and BMI, was matched with that of the patients in the depression group. All healthy volunteers had no personal history of any mental disorder or SA.
Evaluation and Measurement of Attempted Suicide
The research documented the presence of SA in individuals and determined if these incidents occurred in the year prior to admission, utilizing a binary variable (presence or absence). Affirmative replies were validated by assessing the timing, subjective intensity, and frequency of SA. Recent SA were those occurring within 30 days, while past SA were those occurring more than 30 days ago. The researchers considered a 30-day period to be a reasonable timeframe, striking a balance between short-term events and including too many past events.
Clinical Data Collection
Clinical information, blood indicators, HDRS scores, disease course, and diagnosis details are extracted from our hospital’s electronic medical record system. Diagnosis of MDD and assessment of SA are conducted by seasoned psychiatrists with formal training. Peripheral venous blood is drawn from MDD patients within 24 hours of admission, collected in the morning on an empty stomach. The blood is then analyzed using a fully automatic blood cell analyzer for routine testing.
Statistical Analysis
The analysis of all data was done using SPSS 24.0 software. Categorical variables were assessed using frequencies and proportions, while continuous variables were described using means and standard deviations to outline the characteristics of the participants at baseline. Different statistical tests, such as Student’s t-test, Mann–Whitney U, or chi-square test, were employed to compare group variances. By utilizing the participant’s history of SA as the benchmark, the study employed the receiver operating characteristic curve (ROC) to compute the area under the curve (AUC). The presence of SA among patients with MDD was evaluated based on the SII upon admission, determining the optimal cutoff value for SII. Patients were then divided into high SII and low SII categories according to this threshold. Subsequent analysis involved binary logistic regression to explore the connection between SA and SII levels at admission. A significance level of P<0.05 was utilized.
Results
Social Demography of Participants
The study included 338 patients with depression and 76 healthy volunteers. The group of healthy volunteers consisted of 28 males and 48 females, ranging in age from 18 to 53 years old, with an average age calculated at 27.62 ± 7.69 years. Among the patients diagnosed with depression, 57 individuals (16.9%) had a history of previous SA, while 281 individuals (83.1%) did not. Of these patients, 116 (34.3%) were male and 222 (65.7%) were female. Within the group of patients with a personal history of SA, there were 36 females (63.2%) and 21 males (36.8%). The patients’ ages ranged from 18 to 52 years, with an average age of 25.88±7.78 years. Among the depressed patients without a history of SA, 186 were female (66.2%) and 95 were male (33.8%). The participants’ ages varied from 18 to 53 years, with a mean age of 27.97±7.64 years. Statistical analyses indicated that there were no notable differences between the groups concerning age, gender, and BMI (p>0.05) (Table 1).
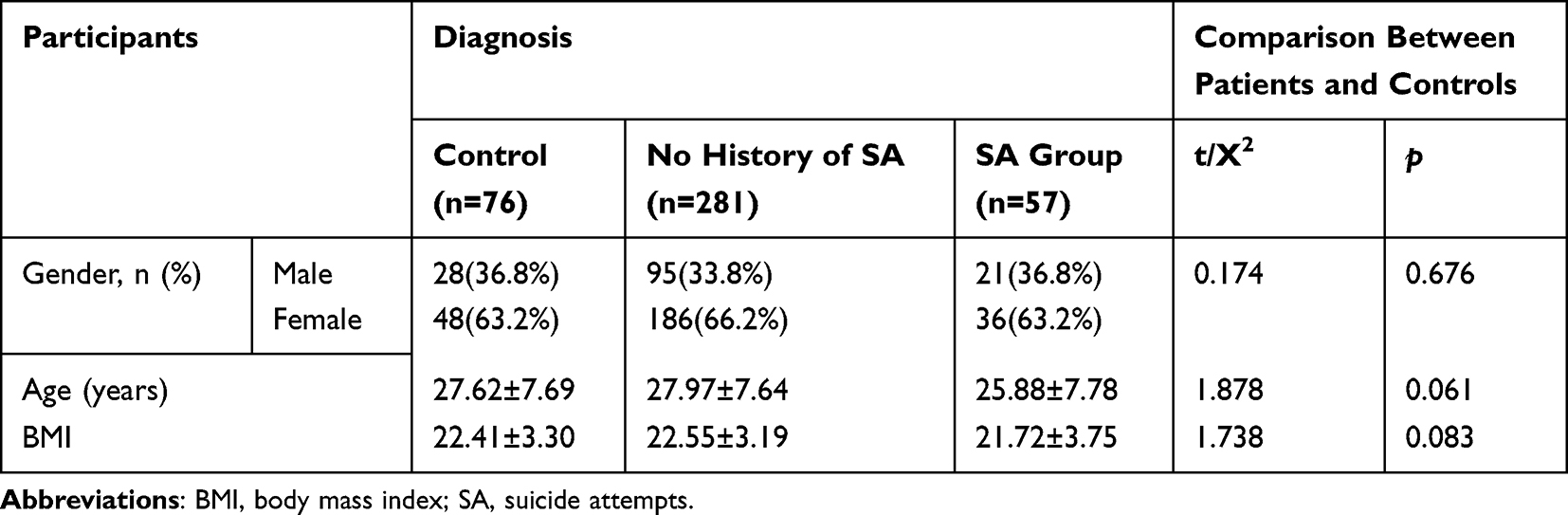 |
Table 1 General Clinical Basic Information of Participants |
Leukocyte and Inflammation Ratio: Difference Between Depression and Healthy Control Group
No significant statistical difference was found in the lymphocyte count between the group of depressed patients (No History of SA or SA Group) and the control group of healthy participants (p>0.05).
The group of patients suffering from depression, regardless of a history of SA, showed a significantly higher neutrophil count (p<0.05), average platelet count (p<0.05), and mean SII (p<0.05) when compared to the healthy control group.
In the study, individuals in the “SA Group” showed notably elevated levels of “Neutrophil counts” (p<0.05) (Figure 2A), “Platelet counts” (p<0.05) (Figure 2C), and “SII” (p<0.05) (Figure 2D) in comparison to those in the “No History of SA Group”. In addition, the index “Lymphocyte counts” has no difference among the groups (p>0.05) (Figure 2B). Please consult Table 2 and Figure 2 for comprehensive information.
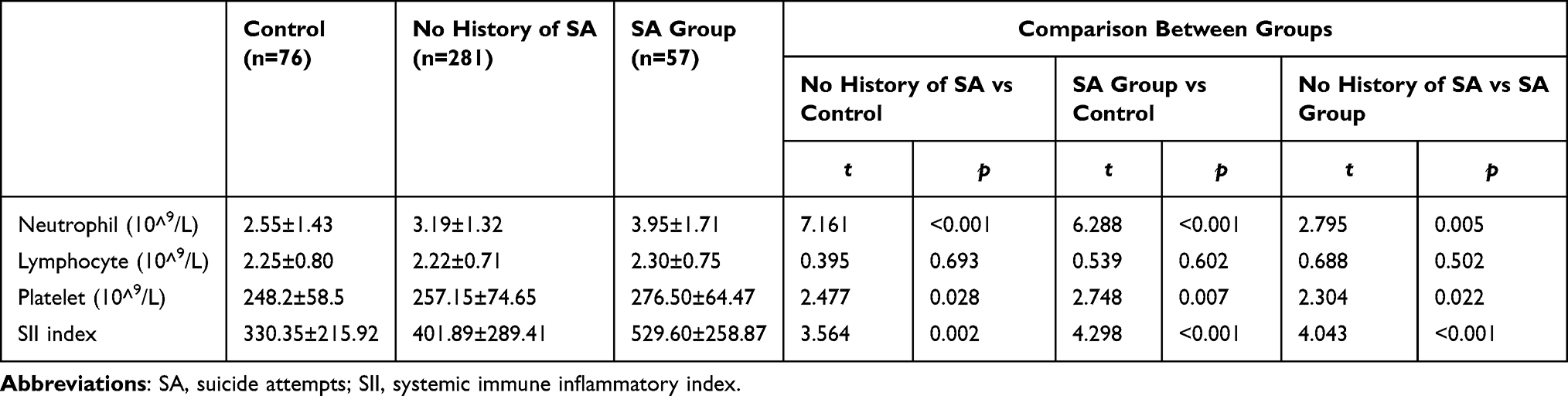 |
Table 2 Comparison of Distribution of White Blood Cells and Platelets Between Healthy Control Group and Depressed Patients |
 |
Figure 2 Comparison of the distribution of leukocyte and inflammation ratio between depression and healthy control group (A) Neutrophil (10^9/L); (B) Lymphocyte (10^9/L); (C) Platelet (10^9/L); (D) SII index. Abbreviation: SA, suicide attempts; SII, systemic immune inflammatory index. Note: Compared with each other group: *P<0.05, **P<0.01, ***P<0.001. NS: No Significance. |
Clinical Characteristics of Patients with Depression
In individuals who have a previous record of SA, the mean number of tries was 1.29±0.65 (p<0.05). Additionally, those with a history of SA exhibited notably elevated HDRS scores in comparison to individuals lacking such a history (p<0.05). Please see Table 3 for additional information.
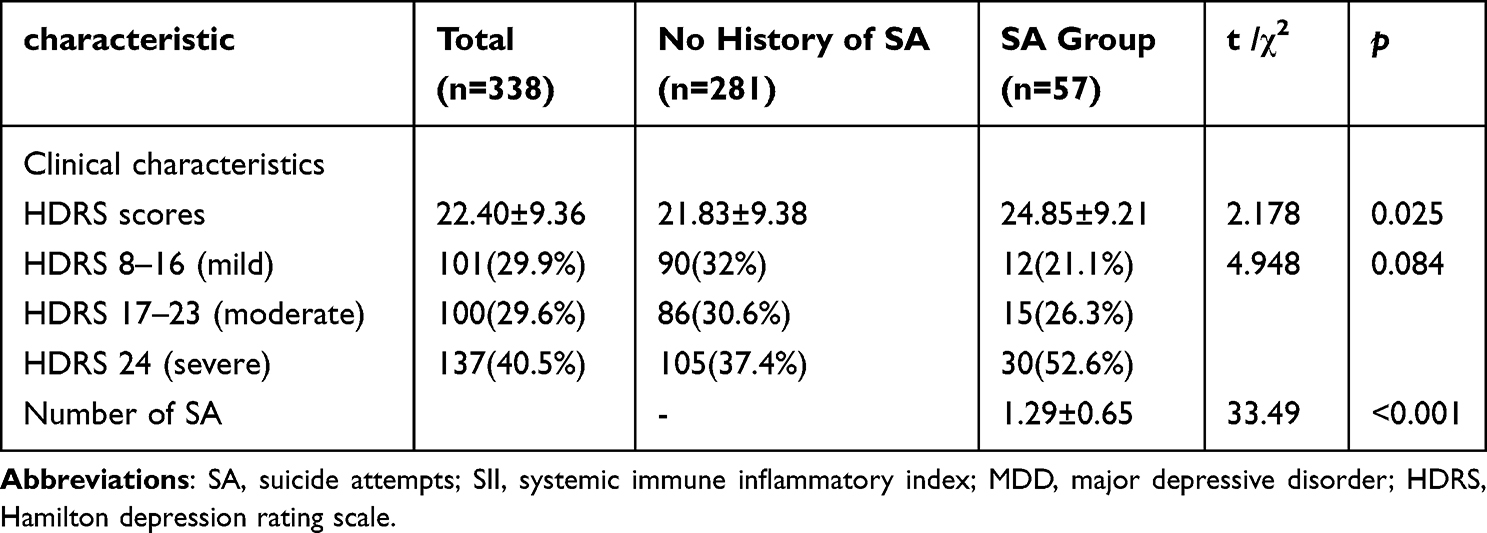 |
Table 3 Clinical Characteristics of MDD Patients With or Without Personal History of SA |
Analysis of Variables Related to SII
The study found significant correlations between SII and depression severity (r=0.143, p=0.031), number of SAs (r=0.225, p<0.001), and BMI (r=0.265, p<0.001). In contrast, a negative correlation was found between SII and the progression of the disease (r=−0.161, p=0.018). However, there was no correlation found between SII and the age factor (r=0.051, p=0.517). Additional information can be found in Table 4.
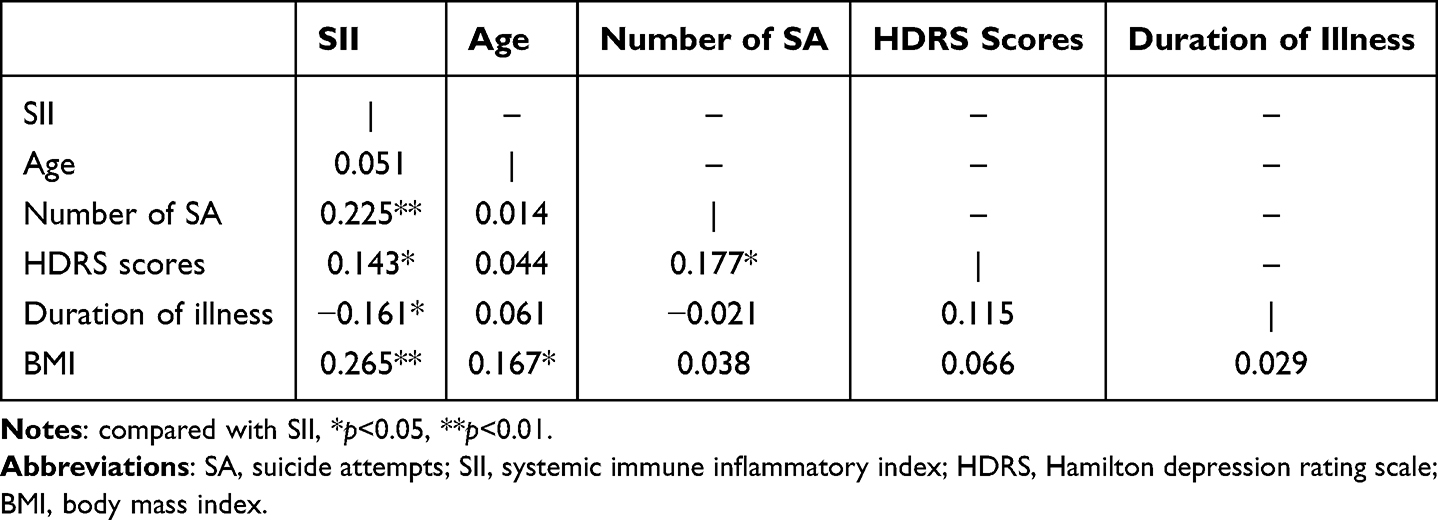 |
Table 4 Spearman Correlation Analysis of SII |
Comparison of Gender Differences in Basic Information and Clinical Indicators of Patients
Considering gender differences, it was observed that female patients were younger on average (p<0.05) and exhibited higher SII index scores (p<0.05). However, no statistically significant differences were detected in BMI and other clinical test indicators (p>0.05). For further information, please refer to Table 5.
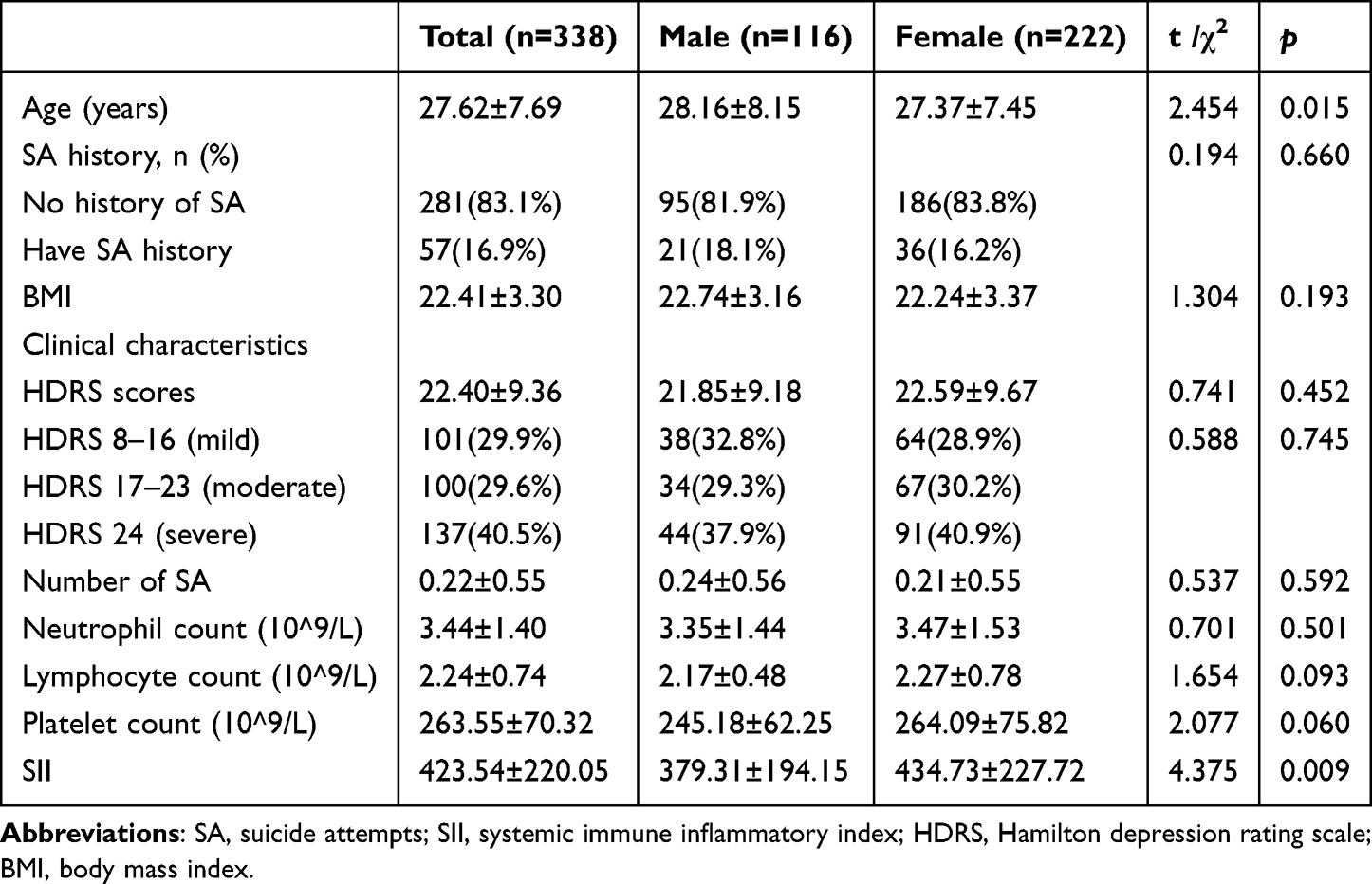 |
Table 5 Compare the Differences in Basic Information and Clinical Indicators Between Different Sexes of Patients |
ROC Curve Analysis
In the analysis conducted using ROC, it was found that the area under the curve for the indicator of Neutrophil count was 0.643 (with a 95% CI of 0.566–0.719, and a p-value of less than 0.001). The ideal threshold value for forecasting SA in patients with MDD was established to be 4.45, exhibiting a sensitivity of 53%, and a specificity of 79%; The ROC curve area for the Lymphocyte count indicator is 0.545 (95% CI: 0.465–0.625, p=0.272). In patients with MDD, the best cutoff value for Lymphocyte count to predict SA is 2.49, showing a sensitivity of 47% and a specificity of 63%; In MDD patients, the ROC curve demonstrated an area of 0.612 (95% CI: 0.534–0.690, p=0.006) pertaining to the Platelet count indicator. An optimal cutoff value of 242.8 for Platelet count in predicting SA was identified, showing a sensitivity of 76% and specificity of 47%.
ROC analysis showed an AUC of 0.692 for the SII index with a 95% CI of 0.620–0.764 (p<0.001). The optimal cut-off point for the SII in predicting SA among patients with MDD was identified as 515.3, yielding a sensitivity of 67% and a specificity of 70%. With this threshold, participants were divided into high (n=80, 23.7%) and low (n=258, 76.3%) SII groups. Please see Table 6 and Figure 3 for further information.
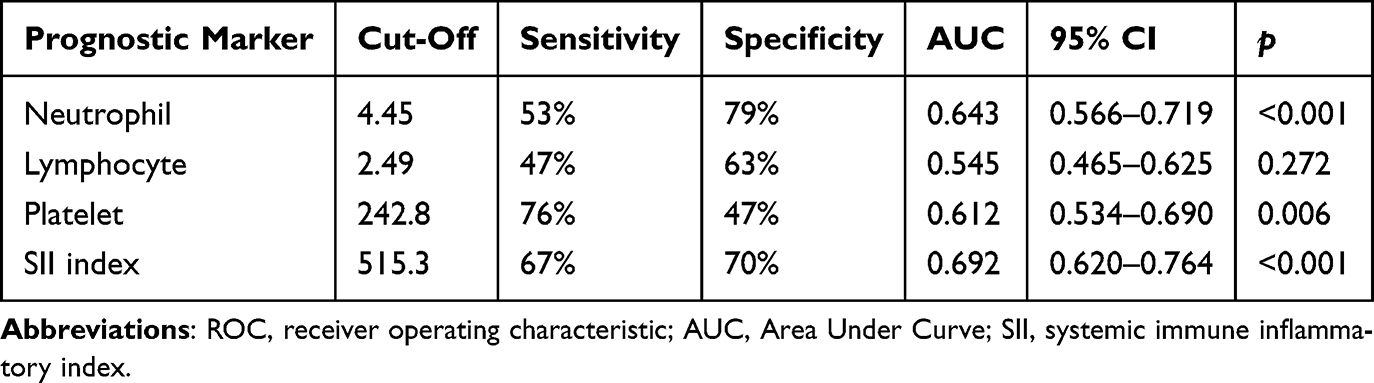 |
Table 6 Prognostic Accuracy of ROC Curve in Predicting Various Indexes |
 |
Figure 3 ROC curve analysis. Abbreviation: ROC, receiver operating characteristic. |
Binomial Logistic Regression Analysis
For binary multi-factor logistic regression analysis, the study included dependent variables such as Total SA, Recent SA (≤7 days), and Past SA (>7 days), coded as positive (1) or negative (0). The independent variables considered were gender (male=1, female=2), age in years, BMI, disease duration in months, HDRS score, and SII level (high SII=1, low SII=0).
After adjusting for demographic factors such as gender, age, BMI, disease duration, and HDRS score, individuals with a high SII value had a significantly increased risk of Total SA compared to those with a low SII value (OR=8.318, 95% CI: 3.767–17.546, p<0.001). The risk of recent SA was also substantially elevated in patients with a high SII value compared to those with a low SII value (OR=14.101, 95% CI: 5.356–34.235, p<0.001). However, a high SII value was not found to be associated with Past SA risk (OR=0.607, 95% CI: 0.061–4.961, p=0.547). Refer to Table 7 for further information.
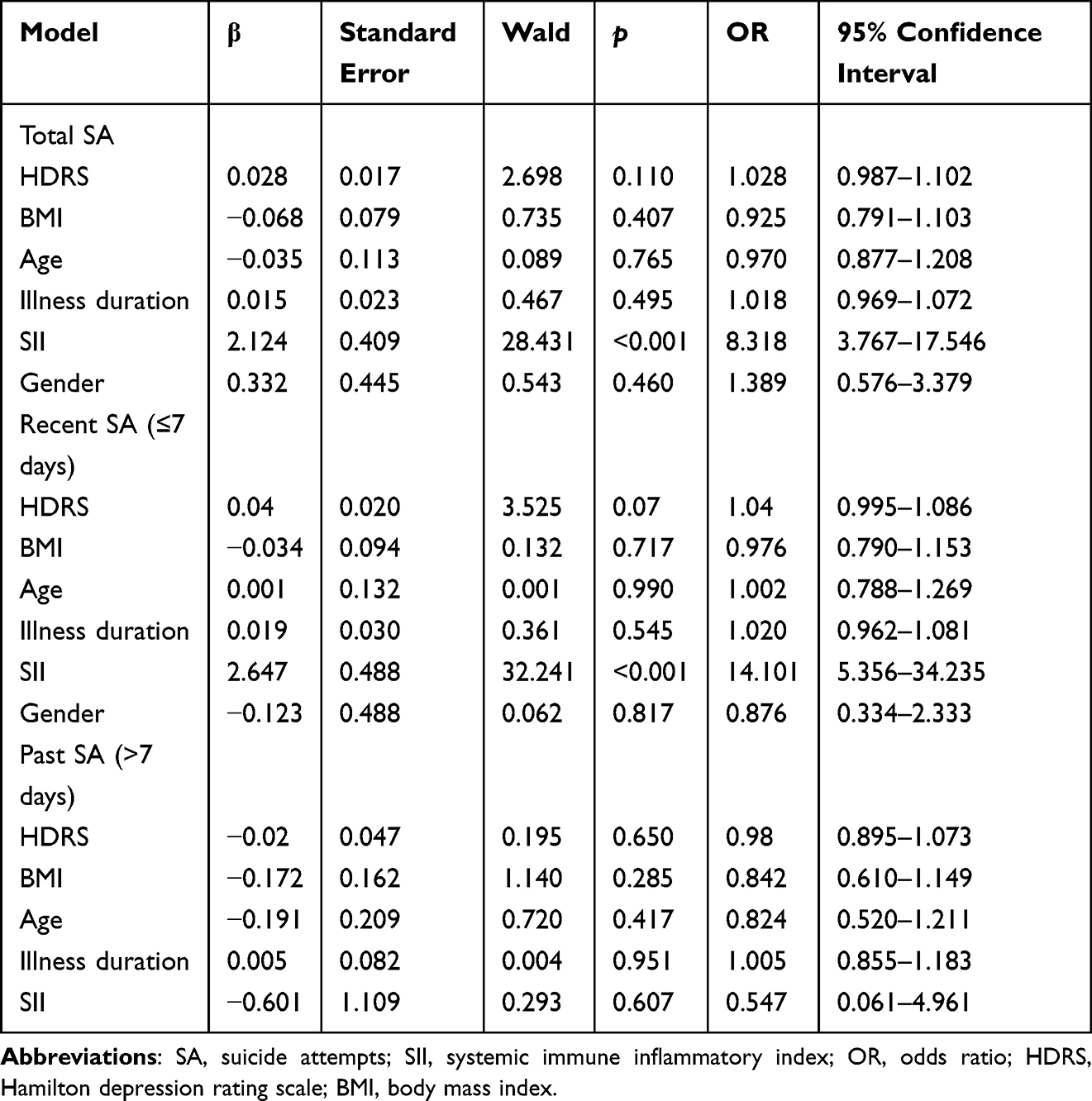 |
Table 7 Binomial Logistic Regression Analysis |
Discussion
The objective of the research was to investigate the correlation between SA and SII among individuals with first-episode MDD who were not taking any medication. The findings revealed that participants with elevated SII had an 8.318-fold higher risk of SA in comparison to those with lower SII levels. High levels of SII upon initial evaluation were identified as a noteworthy autonomous hazard factor for suicidal actions in patients with MDD. The investigation proposes an ideal SII cutoff of 515.3 (sensitivity: 67%, specificity: 70%). Former research has demonstrated that the use of antidepressant medications can effectively decrease inflammation levels in patients.25,26 As a result, this study focused on patients who had not previously received antidepressant treatment to eliminate any potential influence of these drugs on inflammatory markers in patients. This approach allowed for more clinically relevant conclusions to be drawn.
The process of suicidal activity in patients with depressive disorder is highly intricate. It is commonly believed that this process can be categorized into three stages: forming suicidal ideation, developing a suicide plan, and carrying out suicidal behavior. In a study of 111 patients with mental disorders who had engaged in suicidal behavior, Groschwitz et al discovered that 76.6% of these patients had suicidal thoughts prior to their suicide.27 The suicidal behavior of individuals with depressive disorder is a significant public health concern that involves a combination of psychology, genetics, neurobiology, and other factors. Currently, neurobiological research on suicide in patients with depressive disorders has evolved from the initial monoamine hypothesis to the neuro-endocrine immune theory.28 Neurobiological research on suicide in patients with depressive disorder is advancing, shedding light on the physiological and pathological mechanisms involved.29 However, a unified understanding of the specific mechanism behind suicidal activities in these patients is still lacking. Some propose that cytokine dysfunction in the body contributes to depressive disorder development and subsequent suicidal behavior.30 On the other hand, some argue that suicidal activity is just one symptom of depressive disorder, potentially triggered by abnormal cytokine function in response to adverse life event.31
The study found that patients with depressive disorder and suicidal ideation exhibited higher levels of inflammation, indicating a close relationship between abnormal inflammation levels and suicidal thoughts. Suicidal ideation may exacerbate psychological stress and despair in these patients, leading to prolonged stress and low mood, which in turn disrupts the immune system and increases inflammation levels.32,33 Moreover, heightened inflammation levels in individuals with depression may lead to the development of suicidal thoughts. Increased levels of inflammation may also affect the functioning of the body’s HPA axis.34 A study on animals found that inflammatory markers such as TNF-α and IL-6 can activate corticotropin-releasing hormone neurons in the hypothalamus, leading to the activation of the HPA axis.35–37 Previous research has established a strong link between depression pathogenesis in patients and dysfunction of the HPA axis. Increased levels of cortisol in depressed individuals disturb the regulation of the HPA axis, leading to changes in mood and cognition.38 The dexamethasone suppression test (DST) is a frequently utilized method to evaluate HPA axis functionality. Studies have shown that depressed individuals exhibiting DST desuppression are at a higher risk of suicide, indicating a close association between HPA axis dysfunction and suicidal behavior in depressed patients. This suggests that HPA axis hyperfunction could be a distinctive feature linked to suicidal tendencies in individuals with depressive disorders.39 Therefore, heightened inflammation levels in patients with depressive disorders may trigger suicidal thoughts by activating HPA axis activity.
The research discovered a notable link between thoughts of suicide and the inflammatory levels within the bodies of individuals diagnosed with depression. Those individuals experiencing thoughts of suicide showed elevated levels of Neutrophil, Platelet, and SII in contrast to those who did not experience such thoughts. Study also introduced SII as a more comprehensive measure of the inflammatory response by incorporating platelet count into the NLR formula, offering a potentially more thorough assessment of suicidal ideation in depressed patients. A higher SII often indicates an elevated inflammatory response and a weakened immune response in patients. Platelets not only are produced due to inflammation but also function as a marker for inflammation. Despite this, definitive biomarkers reflecting inflammation in depression are still lacking. It is essential to conduct routine blood examinations for all hospitalized patients, and calculating the SII using standard blood routine parameters can provide valuable insights.
This study not only provides valuable insights for clinical applications, but also highlights some limitations that should be considered. We focused on MDD patients who were initiating medication for the first time, excluding those who had previously taken antidepressants multiple times in order to enhance the validity of our findings. This decision was based on existing research indicating the impact of antidepressants on immune inflammation levels in the body. Additionally, we controlled for variables such as age, gender, and depression severity, while also excluding patients with a BMI over 30 to further strengthen the reliability of our results.
This study has several limitations. The control group was small due to strict inclusion criteria and recruitment difficulties, but it was well - matched with the patient group in key variables like age, gender, and BMI. The main aim was to explore inflammatory characteristics of the SA subgroup in depressed patients, not to directly compare patients and healthy individuals. Future multicenter studies can increase the control sample to improve external validity. The exclusion of obese patients (BMI ≥ 30) may limit the generalizability of the results. Obesity is associated with chronic low - grade inflammation, and adipose - derived pro - inflammatory factors (eg, IL - 6, TNF - α) may independently affect SII values. While this exclusion enhanced internal validity, it highlights the need to validate the predictive value of SII for SA in a broader population in future research. We plan to include obese patients in our approved multicenter cohort and analyze the moderating effect of BMI on the SII - SA association. As a retrospective study, we could not establish a causal relationship. We also lacked data on some factors that may influence SII levels, such as detailed dietary and lifestyle information. The relatively small sample size may also limit the generalizability of the results. In future research, we intend to use a prospective design, collect a larger sample, and include more clinical and biological variables to comprehensively explore the relationship between SII and suicidal behavior in MDD patients. We also plan to employ advanced technologies like genomics and proteomics to further investigate the mechanisms underlying the association between SII and inflammatory responses. Future research should consider the characteristics of the SII index and recent advances in inflammatory treatment. Developing targeted inflammatory treatment strategies for the high - SII population and evaluating their effectiveness could provide more effective methods for clinical treatment.
Based on our research findings, it was observed that individuals with first-episode MDD who did not receive any treatment and had a high SII above 515.3 were at a significantly higher risk of developing SA. Additionally, a high SII was identified as an independent risk factor for the recent occurrence of SA. Considering the systemic inflammation levels is vital when assessing the risk of suicide in this specific group. Prior research has shown that it is crucial to identify patient subgroups with both suicidal tendencies and immune system dysregulation. This is necessary for customizing treatment plans to suit individual needs. Thus, analyzing SII levels to detect these specific subgroups can aid healthcare professionals in creating personalized and effective interventions for preventing suicide and managing depression. Focusing on individuals experiencing their first episode of depression, rather than recurrent episodes, can aid in the development of more effective early intervention tactics, which are crucial for suicide prevention.
Data Sharing Statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available because of local ethical restrictions and the protection of the privacy of study participants.
Statement of Ethics
This nationwide research project received ethical approval from the central institution (The First Affiliated Hospital of Wannan Medical College, 2023(69)). Each participant provided a written informed consent.
Acknowledgments
The authors thank the participants who have generously given their time to complete the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by the National Natural Science Foundation of China (Grant No. 81971277, Yonggui Yuan) and the Jiangsu Provincial Key Research and Development Program (Grant No. BE2019748, Yonggui Yuan).
Disclosure
The authors report no conflict of interest.
References
1. Noetel M, Sanders T, Gallardo-Gómez D, et al. Effect of exercise for depression: systematic review and network meta- analysis of randomised controlled trials. BMJ. 2023;384(e075847). doi:10.1136/bmj-2023-075847
2. Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation a mong medical students: a systematic review and meta-analysis. JAMA. 2016;316(21):2214–2236. doi:10.1001/jama.2016.17324
3. Xu Z, Wu X, Xiao C, et al. Observational and genetic analyses of the bidirectional relationship b etween depression and hypertension. J Affect Disord. 2023;348:62–69. doi:10.1016/j.jad.2023.12.028
4. Liu H, Zhang X, Shi P, et al. α7 Nicotinic acetylcholine receptor: a key receptor in the cholinergic anti-inflammatory pathway exerting an antidepressant effect. J Neuroinflammation. 2023;20(1):84. doi:10.1186/s12974-023-02768-z
5. Medeiros AC, Medeiros P, Pigatto GR, Maione S, Coimbra NC, de Freitas RL. Cannabidiol in the dorsal hippocampus attenuates emotional and cogniti ve impairments related to neuropathic pain: the role of prelimbic neoc ortex-hippocampal connections. Prog Neuropsychopharma Biol Psychiatry. 2024;134:111039. doi:10.1016/j.pnpbp.2024.111039
6. Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. 2016;(12):307–330. doi:10.1146/annurev-clinpsy-021815-093204
7. Paljärvi T, Tiihonen J, Lähteenvuo M, Tanskanen A, Fazel S, Taipale H. Taipale H: psychotic depression and deaths due to suicide. J Affect Disord. 2022;321:28–32. doi:10.1016/j.jad.2022.10.035
8. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
9. Choi KW, Kim Y-K, Jeon HJ. Comorbid anxiety and depression: clinical and conceptual consideration and transdiagnostic treatment. Adv Exp Med Biol. 2020;1191:219–235. doi:10.1007/978-981-32-9705-0_14
10. Quan Z, Li H, Quan Z, Qing H. Appropriate macronutrients or mineral elements are beneficial to improve depression and reduce the risk of depression. Int J mol Sci. 2023;24(8):7098. doi:10.3390/ijms24087098
11. Wang G, Zhang H, Sun J, Zhang Y, He F, Zou J. Cyclosporin A impairs neurogenesis and cognitive abilities in brain de velopment via the IFN-γ-Shh-BDNF pathway. Int Immunopharmacol. 2021;96:107744. doi:10.1016/j.intimp.2021.107744
12. Cao C, Wang L, Zhang J, et al. Neuroligin-1 plays an important role in methamphetamine-induced hippoc ampal synaptic plasticity. Toxicol Lett. 2022;361:1–9. doi:10.1016/j.toxlet.2022.03.007
13. Butler MI, Long-Smith C, Moloney GM, et al. The immune-kynurenine pathway in social anxiety disorder. Brain Behav Immun. 2021;99:317–326. doi:10.1016/j.bbi.2021.10.020
14. Tayab MA, Islam MN, Chowdhury KAA, Tasnim FM. Targeting neuroinflammation by polyphenols: a promising therapeutic approach against inflammation-associated depression. Biomed Pharmacother. 2022;147:112668. doi:10.1016/j.biopha.2022.112668
15. Black C, Miller BJ. Meta-analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. BiolPsychiatry. 2014;78(1):28–37. doi:10.1016/j.biopsych.2014.10.014
16. Ganança L, Galfalvy HC, Cisneros-Trujillo S, et al. Relationships between inflammatory markers and suicide risk status in major depression. J Psychiatr Res. 2021;134:192–199. doi:10.1016/j.jpsychires.2020.12.029
17. Tonelli LH, Stiller J, Rujescu D, et al. Elevated cytokine expression in the orbitofrontal cortex of victims of suicide. Acta Psychiatr Scand. 2008;117(3):198–206. doi:10.1111/j.1600-0447.2007.01128.x
18. Melhem NM, Munroe S, Marsland A, et al. Blunted HPA axis activity prior to suicide attempt and increased infla mmation in attempters. Psychoneuroendocrinology. 2017;77:284–294. doi:10.1016/j.psyneuen.2017.01.001
19. Isung J, Aeinehband S, Mobarrez F, et al. Low vascular endothelial growth factor and interleukin-8 in cerebrospinal fluid of suicide attempters. Transl Psychiatry. 2012;2(11):e196. doi:10.1038/tp.2012.123
20. Pandey GN, Rizavi HS, Ren X, et al. Proinflammatory cytokines in the prefrontal cortex of teenage suicide victims. J Psychiatr Res. 2012;46(1):57–63. doi:10.1016/j.jpsychires.2011.08.006
21. Hu B, Yang X-R, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients afte r curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
22. Zhang Y, Chen B, Wang L, Wang R, Yang X. Systemic immune-inflammation index is a promising noninvasive marker t o predict survival of lung cancer: a meta-analysis. Medicine. 2019;98(3):e13788. doi:10.1097/MD.0000000000013788
23. Arteaga-Henríquez G, Simon MS, Burger B, et al. Low-grade inflammation as a predictor of antidepressant and anti-infla mmatory therapy response in MDD patients: a systematic review of the l iterature in combination with an analysis of experimental data collect ed in the EU-MOODINFLAME consortium. Front Psychiatry. 2019;10:458. doi:10.3389/fpsyt.2019.00458
24. Howard DM, Adams MJ, Shirali M, et al. Genome-wide association study of depression phenotypes in UK Biobank i dentifies variants in excitatory synaptic pathways. Nat Commun. 2018;9(1):1470. doi:10.1038/s41467-018-03819-3
25. Réus GZ, Manosso LM, Quevedo J, Carvalho AF. Major depressive disorder as a neuro-immune disorder: origin, mechanis ms, and therapeutic opportunities. Neurosci Biobehav Rev. 2023;155:105425. doi:10.1016/j.neubiorev.2023.105425
26. Zhang Y-X, Zhang X-T, Li H-J, et al. Antidepressant-like effects of helicid on a chronic unpredictable mild stress-induced depression rat model: inhibiting the IKK/IκBα/NF-κB pa thway through NCALD to reduce inflammation. Int Immunopharmacol. 2021;93:107165. doi:10.1016/j.intimp.2020.107165
27. Groschwitz RC, Kaess M, Fischer G, et al. The association of non-suicidal self-injury and suicidal behavior acco rding to DSM-5 in adolescent psychiatric inpatients. Psychiatry Res. 2015;228(3):454–461. doi:10.1016/j.psychres.2015.06.019
28. Yin Q, Wu Y-J, Pan S, et al. Activation of cholinergic anti-inflammatory pathway in peripheral immune cells involved in therapeutic actions of α-mangostin on collagen-induced arthritis in rats. Drug Des Devel Ther. 2020;14:1983–1993. doi:10.2147/DDDT.S249865
29. Chen X, Zhang B, Yuan S, et al. Pre-treatment functional connectivity of the cingulate cortex predicts anti-suicidal effects of serial ketamine infusions. Eur Psychiatry. 2023;66(1):e31. doi:10.1192/j.eurpsy.2023.19
30. Whale R, Fialho R, Field AP, et al. Factor analyses differentiate clinical phenotypes of idiopathic and in terferon-alpha-induced depression. Brain Behav Immun. 2019;80:519–524. doi:10.1016/j.bbi.2019.04.035
31. Yan S, Wu X, Jiang J, et al. Dupilumab improves clinical symptoms in children with Netherton syndro me by suppressing Th2-mediated inflammation. Front Immunol. 2022;3:1054422. doi:10.3389/fimmu.2022.1054422
32. Serafini G, Costanza A, Aguglia A, et al. The role of inflammation in the pathophysiology of depression and Suicidal behavior: implications for treatment. Med Clin North Am. 2023;107(1):1–29. doi:10.1016/j.mcna.2022.09.001
33. Huang M-H, Chen M-H, Hsu J-W, et al. Inflammation, cognitive dysfunction, and suicidal ideation among patie nts with major depression. CNSSpectr. 2022;27(6):724–730. doi:10.1017/S1092852921000729
34. Wang Y, Wu H, Han Z, et al. Guhong injection promotes post-stroke functional recovery via attenuat ing cortical inflammation and apoptosis in subacute stage of ischemic stroke. Phytomedicine. 2022;99:154034. doi:10.1016/j.phymed.2022.154034
35. Ben-Azu B, Adebayo OG, Moke EG, et al. Geraniol attenuates behavioral and neurochemical impairments by inhibitions of HPA-axis and oxido-inflammatory perturbations in mice exposed to post-traumatic stress disorder. J Psychiatr Res. 2023;168:165–175. doi:10.1016/j.jpsychires.2023.10.057
36. Zhang X-S, Lu Y, Li W, et al. Astaxanthin ameliorates oxidative stress and neuronal apoptosis via SI RT1/NRF2/Prx2/ASK1/p38 after traumatic brain injury in mice. Br J Pharmacol. 2021;178(5):1114–1132. doi:10.1111/bph.15346
37. Ma W-X, Li L, Kong L-X, et al. Whole-brain monosynaptic inputs to lateral periaqueductal gray glutama tergic neurons in mice. CNS Neurosci Ther. 2023;29(12):4147–4159. doi:10.1111/cns.14338
38. Zajkowska Z, Gullett N, Walsh A, et al. Cortisol and development of depression in adolescence and young adulth ood - a systematic review and meta-analysis. Psychoneuroendocrinology. 2021;136:105625. doi:10.1016/j.psyneuen.2021.105625
39. Mayer SE, Peckins M, Kuhlman KR, et al. The roles of comorbidity and trauma exposure and its timing in shaping HPA axis patterns in depression. Psychoneuroendocrinology. 2020;120:104776. doi:10.1016/j.psyneuen.2020.104776
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.