")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Critical Analysis of Markov Modeling for the Economic Evaluation of Obesity Interventions: A Systematic Review
Authors Lin Q, Ung COL , Lai Y , Hu H , Jakovljevic M
Received 13 March 2025
Accepted for publication 20 June 2025
Published 28 June 2025 Volume 2025:18 Pages 2169—2187
DOI https://doi.org/10.2147/RMHP.S528064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kubra Kaya
Qiucen Lin,1 Carolina Oi Lam Ung,1– 3 Yunfeng Lai,4 Hao Hu,1– 3 Mihajlo Jakovljevic5– 7
1State Key Laboratory of Quality Research in Chinese Medicine, Institute of Chinese Medical Sciences, University of Macau, Macao, People’s Republic of China; 2Centre for Pharmaceutical Regulatory Sciences, University of Macau, Macao, People’s Republic of China; 3Department of Public Health and Medicinal Administration, Faculty of Health Sciences, University of Macau, Macao, People’s Republic of China; 4School of Public Health and Management, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 5UNESCO-TWAS, The World Academy of Sciences, Trieste, 34100, Italy; 6Shaanxi University of Technology, Hanzhong, 723099, People’s Republic of China; 7Department of Global Health Economics and Policy, University of Kragujevac, Kragujevac, Serbia
Correspondence: Hao Hu, Email [email protected] Mihajlo Jakovljevic, Email [email protected]
Background: Obesity poses significant health and economic burdens globally, with interventions requiring robust cost-effectiveness evaluations. Markov models are widely utilized in economic evaluation of obesity interventions, their structure, assumptions, and related uncertainties have not yet been thoroughly evaluated.
Objective: This study aimed to systematically review the Markov models used for the economic evaluation of anti-obesity interventions, describe their structural characteristics, identify key uncertainties, and provide insights for future research.
Methods: The review was conducted across three databases (PubMed, Embase, the Cochrane Library) and health technology assessment agency websites to identify published Markov model-based full economic evaluations in adults with obesity from their inception to 2 June 2024. Model structure, model uncertainty, and validation were extracted from the included studies. Philips checklist for the methodology quality of modeling studies was performed.
Results: The review included 21 primary publications with 21 unique Markov models. Two modeling approaches regarding the progression of obesity and its impact were identified: direct BMI to cost and utility; and BMI-linked complications, with diabetes and cardiovascular diseases most frequently modeled. Validation practices were inconsistently reported (43% of models), and structural uncertainty (eg, BMI trajectory assumptions) was rarely addressed. Quality assessment revealed moderate rigor (a mean compliance rate of 78% across all criteria), with gaps in transparency and generalizability, particularly for non-Western populations. Probabilistic sensitivity analysis was universal, yet scenario analyses highlighted outcome sensitivity to complication inclusion and time horizons.
Conclusion: While Markov models are commonly utilized in obesity intervention evaluations, methodological heterogeneity and insufficient validation limit comparability and reliability. Future models should prioritize standardized validation (eg, ISPOR guidelines), broader complication spectrum, and diverse population data. Enhancing transparency in structural assumptions and uncertainty analysis is critical for robust policy recommendations.
Keywords: obesity, Markov model, disease progression, economic evaluation
Introduction
Obesity is a complex, progressive, chronic disease characterized by excessive accumulation of body fat that impairs health and is associated with an increased risk of premature morbidity and mortality.1–3 Historically, obesity was rare and associated with affluence in traditional societies, and its global prevalence has more than doubled since 1990, affecting 16% of adults globally in 2022.2,4,5 Notably, substantial increase of obesity was seen among lower- and middle-income countries, which might be driven by reduced physical labor due to technological advancements, urbanization, and reliance on affordable, calorie-dense processed foods.6–10 Recent advances in obesity management include GLP-1 receptor agonists (eg, semaglutide) and dual GLP-1/GIP agonists like tirzepatide, which promote weight loss and metabolic improvements.11 Nevertheless, bariatric surgery has proven to be more effective superior in facilitating weight loss and addressing overall metabolic imbalances for eligible patients, such as those with severe obesity and comorbidities.12
Regarding the scarce healthcare resources and the potentially high cost of such interventions, economic evaluations are increasingly performed to inform decisions by comparatively analyzing their cost and consequence.13 The decision analytic model has increased prominence in economic evaluation, especially for cases like obesity, a chronic relapsing progressive disease process. A review by Bjoern Schwander et al provided a comprehensive overview of published decision models for health economic assessments related to obesity, various methodological approaches were identified and Markov models dominated (85% of studies).14 Similarly, a review of 23 bariatric surgery cost-effectiveness studies reported 70% used state-transition models, including 10 Markov models.15 Cohort-based Markov approaches were also prevalent in pharmacoeconomic evaluations of anti-obesity medications.16
Markov model is particularly well-suited for modeling chronic diseases, in which a hypothetical cohort of individuals resides in a finite number of mutually exclusive health states at every point in time, all transition probabilities are constant or depend only on calendar time (ie, time in model).17,18 It enables analysis of long-term outcomes, time-dependent intervention, and population-level strategies while maintaining transparency and simplicity for decision maker. Moreover, Markov model is relatively simple to develop, debug, communicate, and analyze using user-friendly software.19
Despite the widespread use of Markov models in economic evaluation of obesity interventions, their structure, assumptions, and related uncertainties have not yet been thoroughly evaluated. Therefore, this study aimed to systematically review the Markov models used for the economic evaluation of obesity interventions, describe their structural characteristics, identify key uncertainties, and provide insights for future research.
Methods
Search Strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.20 A search strategy was devised using each database’s specified set of search terms (Supplementary Table S1). In brief, the search was designed to identify published economic modeling studies in adults with obesity. Searches were performed in PubMed, Embase, and the Cochrane Library on 2 June 2024, with no start date restrictions, ensuring coverage of all relevant studies from database inception to the search date. The bibliographies of eligible articles were reviewed to identify any additional relevant publications that could be included in the review.
Additionally, we also searched the websites of the following health technology assessment agencies (HTA): the UK National Institute for Health and Care Excellence (NICE), the Canadian Agency for Drugs and Technologies in Health (CADTH), and the Institute for Clinical and Economic Review (ICER).
Literature Selection
Identified records were downloaded and screened for inclusion based on the predefined inclusion and exclusion criteria (Supplementary Table S2): briefly, only Markov model-based full economic evaluations (including cost-effectiveness, cost-utility, and cost-benefit studies) of anti-obesity interventions in adults with obesity would be included.
Downloaded literature was selected in steps. Firstly, duplicates were removed, and irrelevant records were excluded based on the eligibility criteria during title and abstract screening. Secondly, full-text publications were obtained for the remaining citations, and the screening process was repeated using the eligibility criteria for full-text articles to obtain a final set of included publications. For models described in multiple publications, the most comprehensive journal article (preferred over Health Technology Assessment report) would be included as the primary source for this study, while the remaining publications as secondary sources. The screening process was conducted by two reviewers independently, and any disagreements were resolved through further discussion or by consensus with a third reviewer.
Data Extraction and Analysis
Data extraction was performed using a pre-designed data extraction form. One reviewer performed data extraction, which was checked by two reviewers independently. The following data were extracted from the included studies: (1) General study characteristics, including authors, year of publication, country, intervention, target population, funding sources, conflicts of interest, health outcomes, perspective, and time horizon of analysis; (2) Model characteristics, including graphical representation, health states, cycle length, software used, calibration of parameters, model validation, and types of sensitivity analysis.
Quality Assessment
Quality assessment was performed using the Philips Checklist.21 Philips checklist was a 57-item checklist to evaluate the methodological quality of modeling studies across three dimensions: structure, data, and consistency, as recommended by the National Institute for Health and Care Excellence (NICE).22 Two reviewers assessed the quality of the included studies independently, and any disagreements were resolved through further discussion or by consensus with a third reviewer.
Results
Literature Search Results
We followed PRISMA guidelines (Supplementary Table S3), the flow diagram (Figure 1) outlines study selection. The search yielded 3,561 hits via database search, of which 869 were excluded after removing auto-duplicates (Figure 1). Further 2,562 hits were excluded based on title and abstract screening. We sought to obtain the full text of the remaining 130 hits, and 38 hits with abstract only were excluded. Full publications of 92 hits were assessed, and 30 studies that met our criteria were included. We also searched the websites of HTA agencies; 8 health technology assessment (HTA) reports were identified, and 4 reports were included in the review after full-text screening. As such, a total of 34 studies were identified.
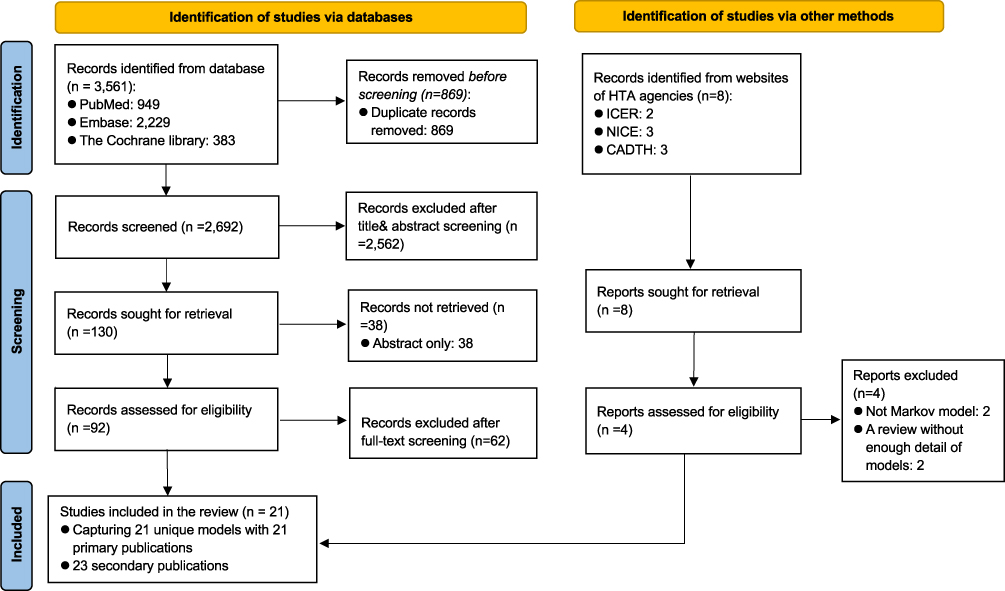 |
Figure 1 PRISMA flowchart of the study selection process. |
Following a detailed review of these 34 publications, 21 unique models with 21 primary publications were included in the current review,23–43 and the remaining 23 publications were documented as secondary sources (Supplementary Table S4). The most frequently applied model was the model by Borisenko O et al, used in seven publications to assess the cost-effectiveness of bariatric surgery in different countries.30 This was followed by the Core Obesity Model (COM),44,45 employed in four publications to evaluate the cost-effectiveness of anti-obesity medications (AOMs). Fifteen other models were described in only one publication.24,25,28,29,31–35,37–42
General Study Characteristics
The main characteristics of the 21 identified Markov-based economic evaluations are summarized in Table 1.
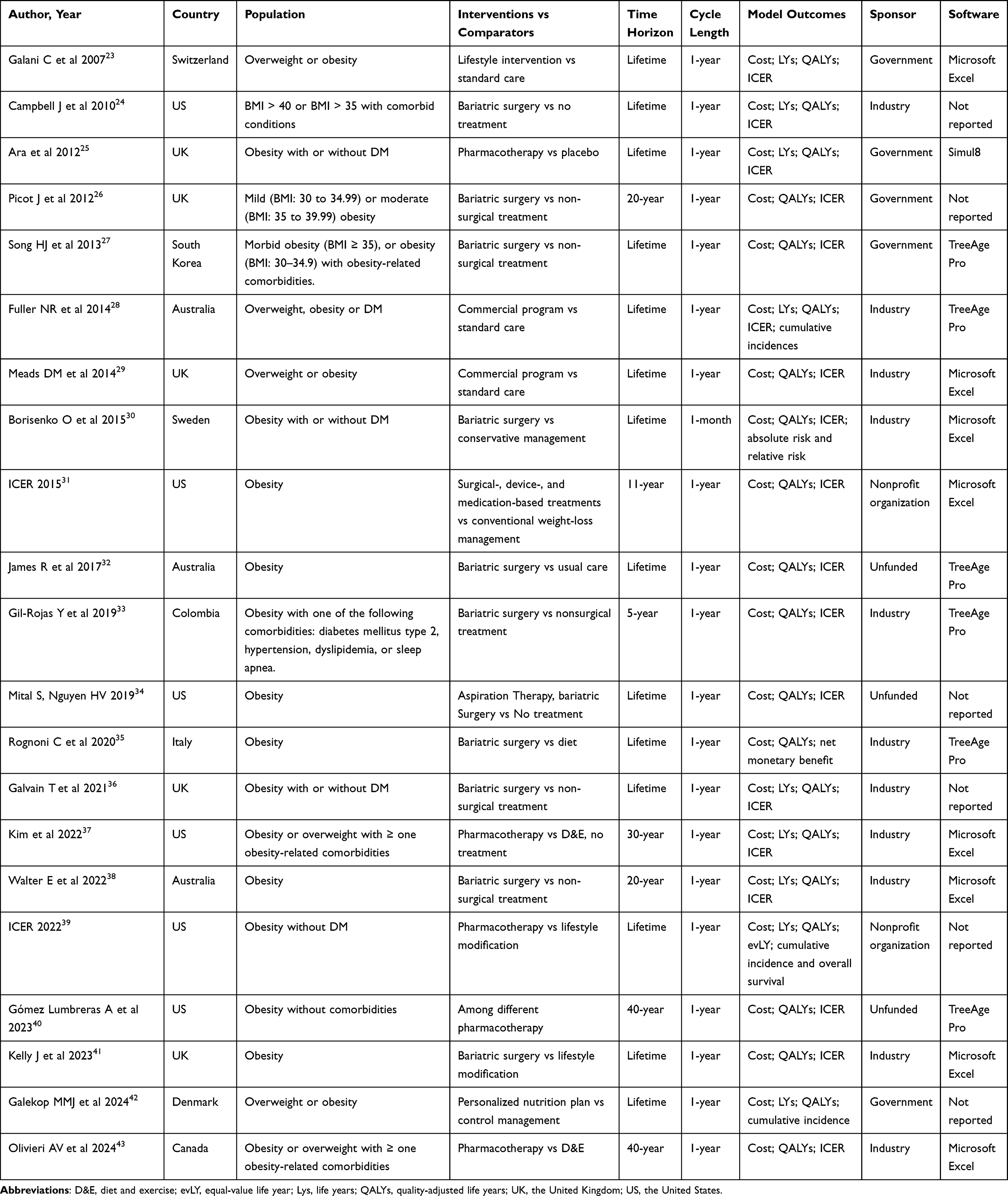 |
Table 1 Main Characteristics of the Markov-Based Modelling Studies |
Regarding time horizon, most included studies applied a lifetime horizon23–25,27–30,32,34–36,39,41,42 or a relatively long-time horizon (ie, 40 years or 30 years).37,40,43 Two studies chose a 20-year time horizon to assess the cost-effectiveness of surgery.26,38 In the Health Technology Assessment issued by the Institute for Clinical and Economic Review (ICER) in 2015, an 11-year time horizon was applied: a one-year time horizon to assess the immediate clinical and economic effects of bariatric surgery, a newer medication, and a newer type of device, and a cost-utility analysis was also conducted over a ten-year time horizon based on assumed trajectories of BMI change after the various surgical, pharmacological, and device interventions.31 A shorter time horizon – 5 years, was applied by Gil-Rojas et al, considered clinically relevant and owing to available efficacy data.33 For the cycle length, all Markov models utilized annual cycles with one exception utilized 1-month cycle length.30
All economic evaluations of obesity interventions have been conducted in western countries, except two studies focusing on Colombia and South Korea seperately.27,33 Most of the studies (52%, 11/21) were funded and sponsored by the industry,24,28–30,33,35–38,41,42 24% (5/21) by government,23,25–27,42 10% (2/21) by the nonprofit organization,31,39 and 14% (3/21) without funding.32,34,40
Apart from cost/LYs/QALYs/ICER, other model outcomes were also considered in the studies reviewed, such as the cumulative incidence of events,28,39,42 and the absolute risk and relative risk of events.30
Among the studies that reported the use of software (n = 15), half of the studies (8/15) used Microsoft Excel (Microsoft Corporation),23,29–31,37,38,41,43 whereas TreeAge (TreeAge Software, Inc.) was used by six studies.27,28,32,33,35,40 One study used software developed by Simul 8 (Simul8 Corporation).25
Model Structure
A model structure is designed to describe the relevant clinical pathways for patients undergoing treatment with the interventions under evaluation. This structure is informed by both the characteristics of the interventions themselves and the established understanding of the natural history of the specific condition in question.18 Additionally, the model structure incorporates insights into how these interventions may influence the progression of the condition. Hence, the natural history of the condition is very important in designing a Markov model given that the model is structured around health states, contributing to our understanding of the disease. The transition probabilities between these health states determine disease progression and must align with current knowledge of the natural history of obesity to ensure their relevance for evaluation purposes.
A total of twenty-one unique Markov models were included in our review, with substantial variations being observed across the studies, as shown in Table 2. A clear graphical representation of the model structure was provided in most studies, except for two.24,31 The number of health states included in the Markov models ranged from 4 to 19.
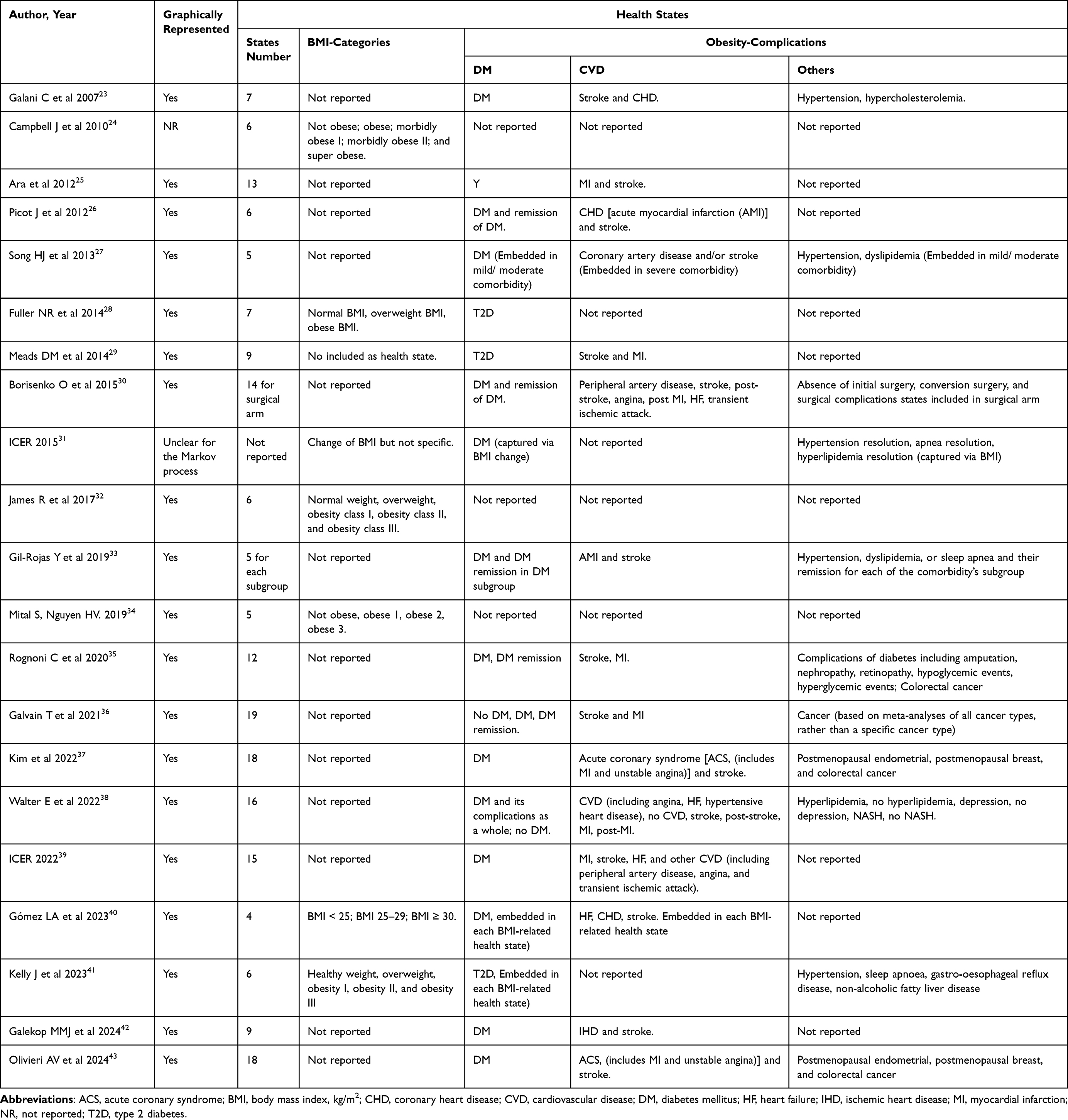 |
Table 2 Summary of Model Structure |
There were two main approaches to modeling the impact of obesity and anti-obesity intervention on cost and health consequence: (1) direct BMI to cost and consequence; (2) BMI change to obesity-related complications.
A much more straightforward approach, BMI change transferred into cost and consequences directly, was employed by four models to assess the cost-effectiveness of bariatric surgery.24,31,32,34 In these models, the natural history of obesity was reproduced and governed by the transition between various BMI categories, eg, not obese (BMI < 30 kg/m2); obese (BMI 30–34.9 kg/m2); morbidly obese I (BMI 35–39.9 kg/m2); morbidly obese II (BMI40-49.9 kg/m2); and super obese (BMI > 50 kg/m2) and death.24
Various BMI categories were utilized as distinct health states within the model; patients transition between Markov states by changing BMI (losing or gaining weight) or dying. Each of these health states was assigned specific cost and utilities. A critical distinction emerged in the methodologies used to assign BMI-specific healthcare costs and health-related quality-of-life (HRQoL) utilities across studies. In two studies, costs and utilities were systematically derived for each BMI category using direct evidence from published sources, such as healthcare expenditures and quality-of-life values specific to BMI categories.24,34 In contrast, two other studies adopted a linear extrapolation method to estimate BMI-related changes in costs and utilities.31,32 Baseline costs and utilities for each health state were extracted from available data, while BMI change-related costs and utilities were estimated via linear extrapolation. Commonly, this approach assumed uniform gains (eg, consistent utility improvements per unit of BMI reduction) to model outcomes.
The other distinct method, change in BMI transferred into the incidence of obesity-related complications that subsequently impact the cost and consequences, stood out as the most widely adopted.23,25–30,33,35–43 In these models, the natural history of obesity was simulated, reflecting the transitions between obesity, obesity-related complications, and death.
Commonly, BMI change was modeled continuously, then the incidence of obesity-related complications and mortality were estimated based on the BMI change with incorporation of additional related risk parameters when appropriate. Nevertheless, three models involved using various BMI categories to define health states in the preceding setting, and BMI categories-related complications were modeled as distinct health states29,40 or implicitly included.41
Regarding the obesity-related complications considered, diabetes mellitus (DM, 15/15) was the most frequently modeled, followed by cardiovascular disease (CVD, 14/15). However, there was notable heterogeneity among the different models in their consideration of DM and CVD.
Most models considered DM alone, while DM-related complications were included as distinct health states in two models as well.35,38 Five models included patients with DM at baseline, explicitly modeling DM remission as a potential benefit of bariatric surgery.26,30,33,35,36
In the modeling of CVD, stroke was the most frequently modeled, followed by myocardial infarction (MI). Secondary CVD event was also considered by three models.25,29,43
Of note, the more recently developed models appear to incorporate a broader range of complications compared to previous models.35–38,43 Among them, cancer was the most frequently considered. However, there was significant heterogeneity among the studies, with one study encompassing all cancer types collectively,36 while others focused on specific types of cancer often encompassing various cancer types within these categories.35,39,43 Additionally, as evidence increasingly highlights the association between BMI, sleep apnea, and knee replacement surgery, three models incorporated the impacts of these conditions, although outside the Markov framework.36,37,43 Furthermore, depression and nonalcoholic steatohepatitis (NASH) were also included in the analysis by Walter E et al.38
In the context of obesity-related complication simulation, a diverse array of approaches was identified. Two studies applied country-specific databases to estimate the relationship between BMI and related complications.25,27 For the other studies, relationships from the published studies are applied. When simulating diabetes mellitus, the most widely adopted approach was BMI-dependent risk estimation via polynomial regression, as proposed by Picot J et al.46 It was used by four models. For cardiovascular disease (CVD), the dominant strategy involved applying the Framingham Heart Study risk equation. 26,30,35,36,39,43 This equation estimates overall 10-year CVD risk by integrating key clinical predictors, including age, total cholesterol, HDL cholesterol, systolic and diastolic blood pressure, smoking status, and diabetes status.47 However, in Markov models focused on obesity, nuanced approaches were employed to account for heterogeneous CVD outcomes, such as myocardial infarction (MI), stroke, and heart failure. This allowed for a more granular estimation of CVD-related morbidity and mortality tied to BMI trajectories.
Model Uncertainty
All models included were able to deal with model uncertainty, which was described in varying levels of detail in the primary publications (Table 3). All included studies conducted probabilistic sensitive analysis (PSA). Deterministic sensitive analysis (DSA) was reported in most studies considering diversity variables, except two.23,35 Among the studies DSA performed, the most frequently reported influential factors were the utility associated with BMI change,26,36,39–41the cost of Type 2 diabetes (T2D) management,26,30,38–40 and time horizon.26,27,31,37,42
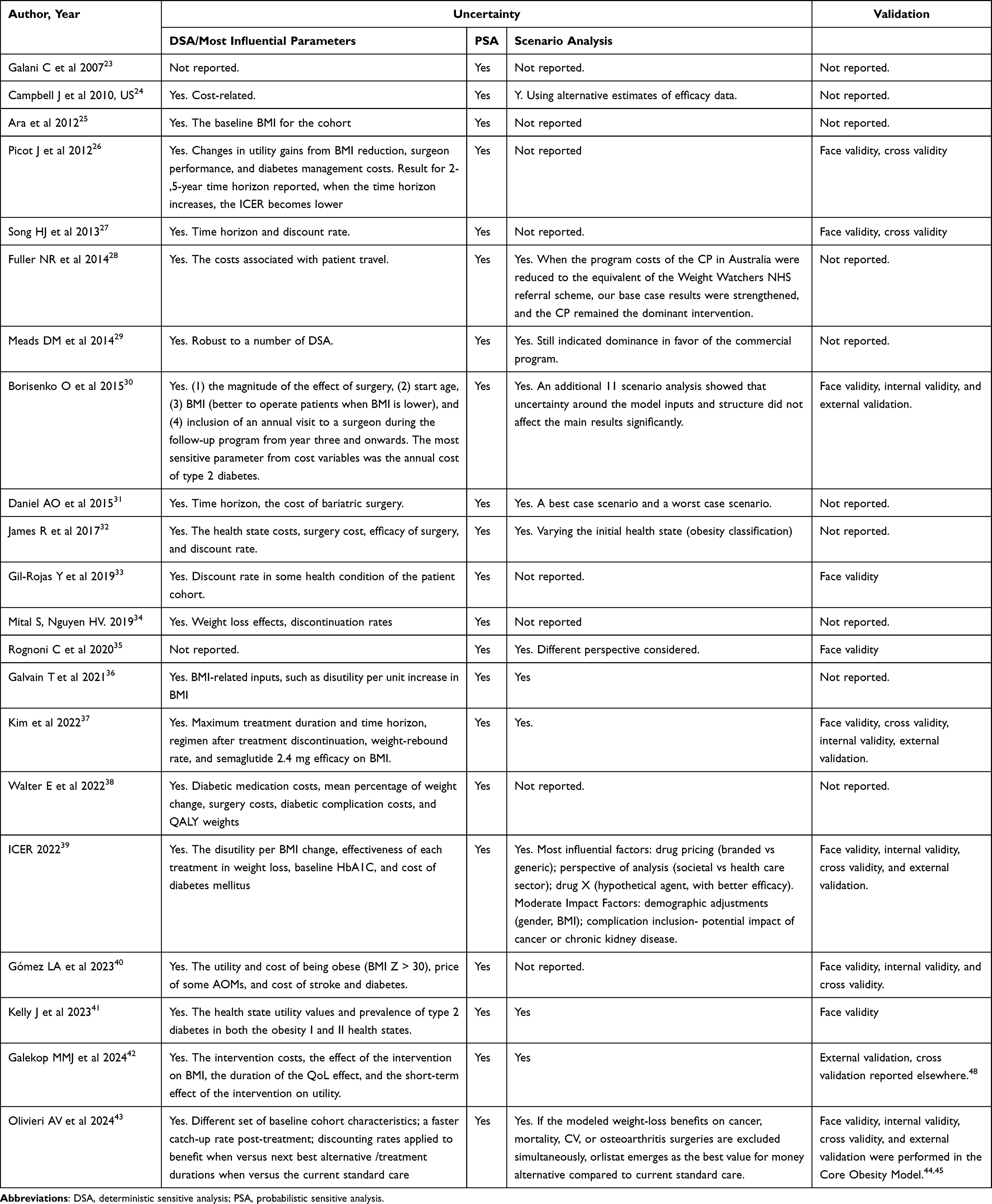 |
Table 3 Uncertainty and Validation |
Additionally, scenario analyses were performed in most studies. In the study of Borisenko O et al, 11 scenario analysis showed that uncertainty around the model inputs and structure did not affect the main results significantly.30 However, the study of Olivieri AV et al found that when the weight-loss benefit on cancer, mortality, cardiovascular disease or osteoarthritis surgeries were excluded simultaneously, orlistat emerged as the best value for the money alternative compared to the current standard care.43 Scenario analysis was also performed in ICER-2022, with the most influential factors including drug price, perspective of analysis, and a hypothetical drug agent with better efficacy; and the moderate impact factors including demographic adjustments, complication inclusion for the potential impact of cancer or chronic kidney disease.39
Model Validation
Model validation is a crucial process that assesses whether a model accurately represents the system it aims to simulate, involving various methods such as face validity (wherein experts evaluate model structure, data sources, assumptions, and results), verification or internal validity (check accuracy of coding), cross validity (comparison of results with other models analyzing the same problem), external validity (comparing model results with real-world results), and predictive validity (comparing model results with prospectively observed events).49
Among the twenty-one unique models, various methods of validation were reported in nine models (43%),26,30,33,37,39–43 and only a small proportion of studies reported internal and external validation processes (Table 3). One model reported conducting internal validity by use of alternative data on complication risks, use of microsimulation analysis instead of Markov cohort analysis, and use of life years as an outcome.34 The study by Galekop MMJ et al,42 which was developed as part of the COMPAR-EU project to estimate the (cost-)effectiveness of self-management interventions for obesity and included partners from five different countries (Germany, Greece, the Netherlands, Spain and the UK) was a part of COMPAR-EU project, the external validity and cross validity was reported elsewhere.48
A comprehensive three-step validation process was employed by the model of Borisenko O.30 First, the face validity of modelling results was assessed. Second, numerous “stress tests” were performed to verify the technical performance of the model. Third, an external validation of the model was performed using three large epidemiological studies (ASCOT-BPLA,50 AHEAD51 and ACCORD52) and the Scandinavian Obesity Surgery Registry annual report-2011.
The Core Obesity Model was well developed and has undergone thorough validation, with the details of its development and validation process published.44,45 As reported, for most outcomes, the predictions of the COM showed good linear correlation with observed outcomes, as evidenced by the high coefficients of determination (R2 values). The independent validation revealed a degree of underestimation in predictions of cardiovascular (CV) disease and mortality, and type 2 diabetes.
The model developed by ICER for their obesity management report in 2022 was also well-validated and comprehensively reported in their HTA report.39 When they changed their model inputs to resemble the study of Kim et al (ie, higher semaglutide unit cost, utility inputs, two-year treatment, and 30-year time horizon),37 their incremental cost-effectiveness estimate comparing semaglutide to lifestyle modification approached their reported estimate comparing semaglutide to diet and exercise. The remaining difference in these incremental cost-effectiveness estimates could likely be explained by a much shorter 30-year life expectancy in all treatments reported in their model.
Quality Assessment
The results of quality assessment using the checklist by Philips et al21 were presented in Figure 2 and Supplementary Table S5. Quality assessment revealed a mean compliance rate of 78% across all 57 checklist items, with unequal distribution both across studies and quality dimensions (model structure, data, consistency), indicating variability in methodological rigor and transparency. Notably, overall compliance with reporting checklist items improved in recent studies.39,42,43 Meanwhile, quality assessment revealed that the included Markov models were well-suited for their purpose with a clear statement of decision problem and objective. The outcomes of all included models were consistent with their objective of the evaluation.
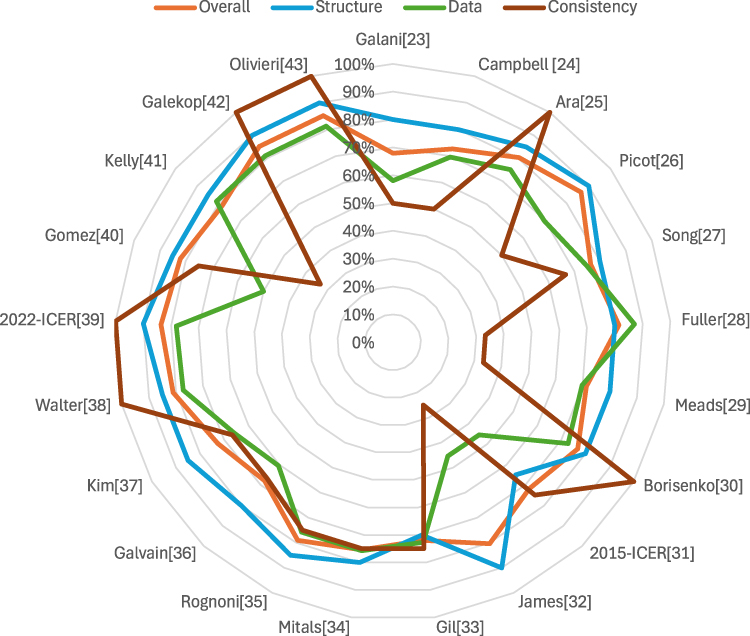 |
Figure 2 Proportion of adequately reporting the Philips checklist item. |
However, given that the models were predominantly intervention-specific, none of the included studies comprehensively evaluated all feasible and practical intervention options within their frameworks. Furthermore, the justification for excluding these viable alternatives was inadequately addressed, which might compromise the validity and generalizability of the findings. Though parameter uncertainty was frequently addressed via deterministic sensitivity analysis and probabilistic sensitivity analysis, few studies comprehensively addressed all of the four principal types of uncertainty—parameter, structural, heterogeneity, and methodological.53
Discussion
Principal Findings
Obesity presents rather unique and complex phenomenon in an array of other “prosperity” or noncommunicable diseases. It is also closely correlated with variety of diabetes, cardiovascular and cerebrovascular events, whose contribution to premature morbidity and preventable mortality remains huge.54–57 Furthermore, specific opportunity cost of obesity is exceptionally high and widely related to the absenteeism and decreased or lost work ability. However, the complexity and costliness of these factors complicate precise quantification of both direct and indirect economic impacts.58–61
In the context of economic evaluations of anti-obesity interventions, Markov models have been widely applied to simulate the progression of obesity and its related health and economic outcomes. This systematic review identified 34 publications describing 21 unique Markov-based economic models evaluating obesity interventions, with 21 primary publications included. The included studies varied significantly in scope, methodological approaches, and reporting quality.
Most models adopted a lifetime or long-term time horizon, reflecting the chronic nature of obesity. However, substantial heterogeneity in the modeling approaches across studies was identified. Two distinct approaches to modeling the progression of obesity and its impact on health outcomes have been observed. The first approach was relatively straightforward, directly translating the changes in body mass index (BMI) into associated costs and health consequences. Commonly, a linear extrapolation method to estimate BMI-related changes in costs and utilities was adopted. For example, a fixed utility gain or cost reduction was systematically applied, irrespective of baseline BMI or individual variability. This approach prioritized simplicity and generalizability but did not account for potential nonlinearities or threshold effects in BMI-related outcomes. It might oversimplify the progression of obesity and underestimate its associated cost and health consequences.
Interestingly, the study by Bjoern Schwander et al raises an important question: does the structure of a health economic model matter?62 Their research found that in severely obese populations, the model’s structure is crucial for accurately predicting clinical events. However, if the goal was simply to compare incremental health economic outcomes, the specific structure might be less significant, as the results tend to be comparable across different models. This suggests that while a well-structured model is essential for precise predictions, it may be less critical when evaluating cost-effectiveness in terms of incremental comparisons.
In contrast, the second and most widely adopted approach-BMI change modelled, and the change in BMI was transferred into the incidence of obesity-related complications that subsequently impact the cost and consequences. Obesity is recognized not only as a disease in its right but also as a significant risk factor for various chronic diseases, including cardiovascular disease, diabetes, and certain cancers63–65 Consequently, when evaluating the impact of obesity and anti-obesity intervention on cost and health consequence, focusing solely on the impact of changes in body mass index (BMI) without considering the associated complications will likely lead to an underestimation of the true impact of obesity. This approach might better reflect the complex nature of obesity and its associated complications, acknowledging the intricate relationships between BMI, health outcomes, and economic implications.
There was considerable variability in the obesity-related complication addressed across the different models included in the analysis. For instance, the model developed by Fuller et al assessed only type 2 diabetes, as it was the sole condition for which baseline prevalence rates were available and because the link between BMI and type 2 diabetes is well established.28 For studies only interested in diabetes mellitus as an outcome, this modeling approach would be suitable. However, for studies modeling interventions for people with obesity, other obesity-related complications would be relevant. As the authors noted, incorporating additional obesity-related diseases into the model would likely enhance the robustness of their existing conclusions.28
In line with this, the review revealed that among the models examined, diabetes mellitus and cardiovascular diseases, particularly MI and stroke, were the most frequently included obesity-related complications. This finding is consistent with the previous systematic review14,66 and recommendations from an expert panel,67 which suggested that models should incorporate at least three key comorbidities: coronary heart disease, type 2 diabetes, and stroke. According to a comprehensive report from the World Health Organization, there is substantial evidence—either strong or moderate—supporting the association of these conditions with obesity.68 These conditions significantly affect health-related quality of life (HRQoL), life expectancy, and the utilization of healthcare resources and costs.68,69 Furthermore, they are known to be influenced by weight management interventions.
Moreover, a broader range of obesity-related complications has been incorporated into the recently developed models. As reported by Olivieri AV et al, when the weight-loss benefit on cancer, mortality, cardiovascular disease or osteoarthritis surgeries was excluded simultaneously, orlistat emerged as the best value for the money alternative compared to the current standard care.43 This finding underscores the necessity of comprehensively incorporating obesity-related complications in cost-effectiveness analyses to ensure accurate assessments of intervention value.
BMI categories were utilized in seven studies, with six focusing on the cost-effectiveness of bariatric surgery,24,31,32,41 while one study concentrated on anti-obesity medications.40 When evaluating the cost-effectiveness of anti-obesity medications using BMI categories approach, all treatments yielded similar quality-adjusted life years (QALYs).40 The amount of weight loss with these medications was often insufficient to facilitate a transition from one BMI category to another, resulting in only modest differences in QALYs. In contrast, modeling BMI as a continuous variable rather than categorically would enhance the model’s flexibility in simulating the effects of interventions on BMI reductions.48
Regarding the relationship between BMI and obesity-related complications, the process of identifying studies reporting the association was often poorly described and rarely based on systematic or structured reviews. Moreover, existing Markov-based health economic models predominantly derived from Western populations—rely on data specific to Caucasian cohorts, which limits its generalizability to diverse ethnic or geographic groups. Introducing new data or calibrating existing risk equations could enhance the accuracy of decision-making in this context.70
With respect to the uncertainty, parameter uncertainty was consistently addressed via probabilistic sensitivity analysis (PSA) in most studies. Despite the critical importance underscored by established modeling guidelines, which necessitate the exploration of implications arising from alternative plausible assumptions,71 structural uncertainty, particularly regarding assumptions about BMI trajectories, complication risks, and treatment effect durability, remains insufficiently addressed in current scholarly investigations. Addressing uncertainty in the model is not merely a technical step but a critical foundation for robust decision-making, substantial efforts must be devoted to systematically evaluating and mitigating it.
Validation practices were inconsistently reported and only a small proportion of studies reported internal or external validation processes. As trust and confidence are foundational to the success of health economic models, rigorous validation is imperative to ensure their reliability in informing policy and clinical decisions. There is an urgent need for concerted efforts to align validation practices with the 2012 ISPOR guidelines.49
Quality assessment of the 21 models was carried out by using the Philips checklist. Overall, the reviewed models achieved a mean proportion of 78% that adequately fulfilled across all criteria, indicating moderate methodological adequacy. However, stratified analysis revealed significant disparities between the structure section and data section, with models consistently more adequately reporting in structural design than in data handling and transparency. Most models failed to address structural uncertainty, such as assumptions about sustained treatment effects or its extrapolation methods, and omitted sensitivity analyses to test these assumptions. Furthermore, transparency gaps were evident in insufficient documentation of excluded interventions and incomplete consideration of uncertainty types (eg, parameter, structural, heterogeneity). These findings highlight critical limitations in methodological rigor, particularly the underassessment of structural uncertainty and data-driven assumptions, which may undermine the reliability of cost-effectiveness conclusions in obesity intervention evaluations.
Limitations
This systematic review has several limitations that should be acknowledged. Firstly, the review was restricted to literature published in English, which may have resulted in the exclusion of relevant studies published in other languages, limiting the comprehensiveness of our findings. Secondly, the focus was solely on Markov models, excluding potentially valuable insights from non-Markov modeling approaches that could enhance understanding of the natural history of obesity and its related comorbidities. This focus may also lead to structural uncertainty, as variability in model assumptions and disease progression pathways can influence outcomes and cost-effectiveness conclusions. Thirdly, the Philips checklist,21 a tool for evaluating the methodological quality of health economic models, exhibits limitations when applied to obesity-related studies. Many criteria assessments under this framework rely on subjective interpretations and lack specificity for modeling chronic, multifactorial conditions such as obesity. For instance, the checklist’s generalized criteria may inadequately address the complexity of obesity dynamics, including long-term weight trajectories, behavioral heterogeneity, and interactions with comorbidities, thereby limiting its utility in ensuring methodological rigor for obesity-specific models.
Recommendations for Future Research
Future studies should prioritize enhancing methodological rigor in health economic models for obesity interventions by systematically addressing structural uncertainty through advanced sensitivity analyses, and adhering to standardized validation frameworks to ensure robust internal and external validation. Efforts must focus on improving transparency in data sourcing, justifying excluded interventions, and integrating diverse population data to enhance generalizability across ethnic and geographic cohorts. Additionally, models should incorporate a broader spectrum of obesity-related complications using evidence synthesized from systematic reviews, while refining quality assessment tools to better capture chronic, complex disease dynamics. Calibrating risk equations to reflect non-linear BMI-outcome relationships and contextual factors (eg, socioeconomic disparities) will further strengthen the validity of cost-effectiveness conclusions.
Conclusion
This systematic review of Markov models in economic evaluation of obesity intervention underscores significant methodological heterogeneity, particularly in addressing structural uncertainty, validating assumptions, and generalizing findings beyond Western populations. Within Markov frameworks, the accuracy and reliability of modeling the impact of obesity and its interventions depend critically on methodological rigor, such as explicitly defined health states, the evidence-based transition probabilities, generalizable simulations of long-term outcomes, and comprehensive uncertainty analyses—particularly those addressing structural assumptions. Adherence to standardized validation frameworks (eg, ISPOR guidelines) is critical to ensure models reliably inform obesity-related reimbursement decisions. Future research should prioritize these frameworks alongside advanced uncertainty analyses and population-specific risk calibrations to strengthen cost-effectiveness evidence.
Data Sharing Statement
All the data has been included in the manuscript.
Acknowledgments
We would like to thank the Editor and two anonymous reviewers for their comments that have much contributed to improve the final version of this paper.
Author Contributions
QCL, COLU, and HH conceptualized the study. QCL, COLU, and HH conducted the collection and analysis. All authors participated in the result interpretation. QCL drafted the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process. A position statement of the world obesity federation. Obesity Reviews. 2017;18(7):715–723. doi:10.1111/obr.12551
2. World Health Organization. Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
3. BMIMC G, Di Angelantonio E, N BS, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–786. doi:10.1016/s0140-6736(16)30175-1
4. Hojjat TA. Income and wealth inequality and obesity. The Economics of Obesity. 2021;53–70.
5. Goda ET, Boshera TD, Aredo MK. Examining the relationship between urban household food insecurity and under-five mortality in Lideta Sub-city, Addis Ababa, Ethiopia. Global Health Economics and Sustainability. 2024;2(1):1682. doi:10.36922/ghes.1682
6. Żukiewicz-Sobczak W, Wróblewska P, Zwoliński J, et al. Obesity and poverty paradox in developed countries. Annals of Agricultural and Environmental Medicine. 2014;21(3):590–594. doi:10.5604/12321966.1120608
7. Jakovljevic M, Liu Y, Cerda A, et al. The global south political economy of health financing and spending landscape–history and presence. Journal of Medical Economics. 2021;24(sup1):25–33. doi:10.1080/13696998.2021.2007691
8. Amarra MS, de Los Reyes F. Assessment of the intake and sources of total sugar among Filipino children and adolescents based on national consumption data. Global Health Economics and Sustainability. 2024;2(1):2060. doi:10.36922/ghes.2060
9. Jakovljevic M, Cerda AA, Liu Y, et al. Sustainability challenge of Eastern Europe—historical legacy, belt and road initiative, population aging and migration. Sustainability. 2021;13(19):11038. doi:10.3390/su131911038
10. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9(6):373–392. doi:10.1016/s2213-8587(21)00045-0
11. Gudzune KA, Kushner RF. Medications for Obesity: a Review. JAMA. 2024;332(7):571–584. doi:10.1001/jama.2024.10816
12. Roomy MA, Hussain K, Behbehani HM, et al. Therapeutic advances in obesity management: an overview of the therapeutic interventions. Front Endocrinol. 2024;15:1364503. doi:10.3389/fendo.2024.1364503
13. Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes.
14. Schwander B, Hiligsmann M, Nuijten M, Evers S. Systematic review and overview of health economic evaluation models in obesity prevention and therapy. Expert Review of Pharmacoeconomics & Outcomes Research. 2016;16(5):561–570. doi:10.1080/14737167.2016.1230497
15. Alsumali A, Al-Hawag A, Samnaliev M, Eguale T. Systematic assessment of decision analytic models for the cost-effectiveness of bariatric surgery for morbid obesity. Surgery for Obesity and Related Diseases. 2018;14(7):1041–1059. doi:10.1016/j.soard.2018.03.005
16. Xue Y, Zou H, Ruan Z, et al. Pharmacoeconomic evaluation of anti-obesity drugs for chronic weight management: a systematic review of literature. Front Endocrinol. 2023;14:1254398. doi:10.3389/fendo.2023.1254398
17. Sonnenberg FA, Beck JR. Markov models in medical decision making: a practical guide. Medical Decision Making. 1993;13(4):322–338. doi:10.1177/0272989x9301300409
18. Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford University Press. 2006.
19. Siebert U, Alagoz O, Bayoumi AM, et al. State-transition modeling: a report of the ISPOR-SMDM modeling good research practices task force-3. Value in Health. 2012;15(6):812–820. doi:10.1016/j.jval.2012.06.014
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. Philips Z, Ginnelly L, Sculpher M, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. Health Technol Assess. 2004;8(36):1–158. doi:10.3310/hta8360
22. National Institute of Health Clinical Excellence. Developing NICE guidelines: the manual. National Institute for Health and Clinical Excellence. Available from: https://www.nice.org.uk/process/pmg20.
23. Galani C, Schneider H, Rutten FF. Modelling the lifetime costs and health effects of lifestyle intervention in the prevention and treatment of obesity in Switzerland. Int J Public Health. 2007;52(6):372–382. doi:10.1007/s00038-007-7014-9
24. Campbell J, McGarry LA, Shikora SA, Hale BC, Lee JT, Weinstein MC. Cost-effectiveness of laparoscopic gastric banding and bypass for morbid obesity Article. The American Journal of Managed Care. 2010;16(7):e174–187.
25. Ara R, Blake L, Gray L, et al. What is the clinical effectiveness and cost-effectiveness of using drugs in treating obese patients in primary care? A systematic review. Health Technol Assess. 2012;16(5):1–195. doi:10.3310/hta16050
26. Picot J, Jones J, Colquitt JL, Loveman E, Clegg AJ. Weight loss surgery for mild to moderate obesity: a systematic review and economic evaluation. Review. Obesity Surgery. 2012;22(9):1496–1506. doi:10.1007/s11695-012-0679-z
27. Song HJ, Kwon JW, Kim YJ, Oh SH, Heo Y, Han SM. Bariatric surgery for the treatment of severely obese patients in South Korea--is it cost effective?. Obes Surg. 2013;23(12):2058–2067. doi:10.1007/s11695-013-0971-6
28. Fuller NR, Carter H, Schofield D, et al. Cost effectiveness of primary care referral to a commercial provider for weight loss treatment, relative to standard care: a modelled lifetime analysis. Article. International Journal of Obesity. 2014;38(8):1104–1109. doi:10.1038/ijo.2013.227
29. Meads DM, Hulme CT, Hall P, Hill AJ. The cost-effectiveness of primary care referral to a UK commercial weight loss programme. Clin Obes. 2014;4(6):324–332. doi:10.1111/cob.12077
30. Borisenko O, Adam D, Funch-Jensen P, et al. Bariatric surgery can lead to net cost savings to health care systems: results from a comprehensive European Decision Analytic Model. Article. Obesity Surgery. 2015;25(9):1559–1568. doi:10.1007/s11695-014-1567-5
31. Ollendorf DA, Shore KK, Cameron C, et al. Controversies in obesity management: a technology assessment; final evidence report. Institute for Clinical and Economic Review. Available from: https://icer.org/wp-content/uploads/2020/10/CTAF_OM_Final_Report_081015.pdf.
32. James R, Salton RI, Byrnes JM, Scuffham PA. Cost-utility analysis for bariatric surgery compared with usual care for the treatment of obesity in Australia. Article. Surg for Obes Related Diseases. 2017;13(12):2012–2020. doi:10.1016/j.soard.2016.12.016
33. Gil-Rojas Y, Garzón A, Lasalvia P, Hernández F, Castañeda-Cardona C, Rosselli D. Cost-effectiveness of bariatric surgery compared with nonsurgical treatment in people with obesity and comorbidity in Colombia. Value Health Reg Issues. 2019;20:79–85. doi:10.1016/j.vhri.2019.01.010
34. Mital S, Nguyen HV. incremental cost-effectiveness of aspiration therapy vs bariatric surgery and no treatment for morbid obesity. Am J Gastroenterol. 2019;114(9):1470–1477. doi:10.14309/ajg.0000000000000359
35. Rognoni C, Armeni P, Tarricone R, Donin G. Cost-benefit analysis in health care: the case of bariatric surgery compared with diet. Clin Ther. 2020;42(1):60–75.e7. doi:10.1016/j.clinthera.2019.12.001
36. Galvain T, Patel S, Kabiri M, Tien S, Casali G, Pournaras DJ. Cost-effectiveness of bariatric and metabolic surgery, and implications of COVID-19 in the United Kingdom. Surg Obes Relat Dis. 2021;17(11):1897–1904. doi:10.1016/j.soard.2021.07.009
37. Kim N, Wang J, Burudpakdee C, et al. Cost-effectiveness analysis of semaglutide 2.4 mg for the treatment of adult patients with overweight and obesity in the United States. J Manag Care Spec Pharm. 2022;28(7):740–752. doi:10.18553/jmcp.2022.28.7.740
38. Walter E, Langer FB, Beckerhinn P, Hoffer F, Prager G. Impact of metabolic surgery on cost and long-term health outcome: a cost-effectiveness approach. Surg Obes Relat Dis. 18(2):260–270. doi:10.1016/j.soard.2021.10.012
39. Atlas SJ, Kim K, Beinfeld M, et al. Medications for obesity management: effectiveness and value; final evidence report. Institute for Clinical and Economic Review. Available from: https://icer.org/assessment/obesity-management-2022/.
40. Gómez Lumbreras A, Tan MS, Villa-Zapata L, Ilham S, Earl JC, Malone DC. Cost-effectiveness analysis of five anti-obesity medications from a US payer’s perspective. Nutrition, Metabolism and Cardiovascular Diseases. 2023;33:1268–1276. doi:10.1016/j.numecd.2023.03.012
41. Kelly J, Menon V, O’Neill F, et al. UK cost-effectiveness analysis of endoscopic sleeve gastroplasty versus lifestyle modification alone for adults with class II obesity. Article. International Journal of Obesity. 2023;47(11):1161–1170. doi:10.1038/s41366-023-01374-6
42. Galekop MMJ, Uyl-de Groot C, Redekop WK. Economic evaluation of a personalized nutrition plan based on omic sciences versus a general nutrition plan in adults with overweight and obesity: a modeling study based on trial data in Denmark. Pharmacoecon Open. 2024;8(2):313–331. doi:10.1007/s41669-023-00461-8
43. Olivieri AV, Muratov S, Larsen S, et al. Cost-effectiveness of weight-management pharmacotherapies in Canada: a societal perspective. Int J Obes. 2024;48(5):683–693. doi:10.1038/s41366-024-01467-w
44. Lopes S, Johansen P, Lamotte M, McEwan P, Olivieri AV, Foos V. External validation of the core obesity model to assess the cost-effectiveness of weight management interventions. Pharmacoeconomics. 2020;38(10):1123–1133. doi:10.1007/s40273-020-00941-3
45. Lopes S, Meincke HH, Lamotte M, Olivieri AV, Lean MEJ. A novel decision model to predict the impact of weight management interventions: the Core Obesity Model. Obesity Science and Practice. 2021;7(3):269–280. doi:10.1002/osp4.495
46. Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Review. Health Technology Assessment. 2009;13(41):ix–214. doi:10.3310/hta13410
47. Wilson PW, RB D, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998;97(18):1837–1847. doi:10.1161/01.cir.97.18.1837
48. Hoogendoorn M, Galekop M, van Baal P. The lifetime health and economic burden of obesity in five European countries: what is the potential impact of prevention?. Diabetes, Obesity & Metabolism. 2023;25(8):2351–2361. doi:10.1111/dom.15116
49. Eddy DM, Hollingworth W, Caro JJ, et al. Model transparency and validation: a report of the ISPOR-SMDM modeling good research practices task force-7. Medical Decision Making. Sep-Oct. 2012;32(5):733–743. doi:10.1177/0272989x12454579
50. Dahlöf B, Sever PS, Poulter NR, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ascot-bpla): a multicentre randomised controlled trial. Lancet. 9489;366:895–906. doi:10.1016/s0140-6736(05)67185-1
51. Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. New England Journal of Medicine. 2013;369(2):145–154. doi:10.1056/NEJMoa1212914
52. Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. New England Journal of Medicine. 2010;362(17):1575–1585. doi:10.1056/NEJMoa1001286
53. Briggs AH, Weinstein MC, Fenwick EAL, et al. Model parameter estimation and uncertainty: a report of the ISPOR-SMDM modeling good research practices task force-6. Value in Health. Sep-Oct. 2012;15(6):835–842. doi:10.1016/j.jval.2012.04.014
54. Papantoniou P, Papageorgiou A. Short-term cost-effectiveness of oral semaglutide versus empagliflozin, sitagliptin, and liraglutide in the treatment of Type 2 diabetes in Greece. Global Health Economics and Sustainability. 2024;2(4):3032. doi:10.36922/ghes.3032
55. de Souza Rezende P, Franceschet CT, Schmidt MM, Peringer V, Eibel B. Utilizing the REDCap platform in a cardiac rehabilitation service. Global Health Economics and Sustainability. 2024;2(1):1755. doi:10.36922/ghes.1755
56. Hutson J, Hutson P. Neuroinclusive workplaces and biophilic design: strategies for promoting occupational health and sustainability in smart cities. Global Health Economics & Sustainability. 2023;1(1):0549. doi:10.36922/ghes.0549
57. Jakovljevic M, Jakab M, Gerdtham U, et al. Comparative financing analysis and political economy of noncommunicable diseases. Journal of Medical Economics. 2019;22(8):722–727. doi:10.1080/13696998.2019.1600523
58. Hutson P, Hutson J. Enhancing flow states in neurodivergent individuals through cognitive network integration. Global Health Economics and Sustainability. 2024:4345. doi:10.36922/ghes.4345
59. Samantha CS, Mark PA, Jed M. Assessing chronic community health needs through a pharmacy improvement project. Global Health Economics and Sustainability. 2023;1(2):1030. doi:10.36922/ghes.1030
60. Antoniadou C, Vlastos DD, Theofilou P. Investigation of job satisfaction, work-related burnout, and their impact on the general health of individuals active in the catering industry. Global Health Economics and Sustainability. 2024;2(1):1852. doi:10.36922/ghes.1852
61. Collins L, Ross L, Preston M. Cost-effectiveness of promoting population health management through education, seminars, and participatory learning for individuals diagnosed with chronic diseases. Global Health Economics and Sustainability. 2024;3089.
62. Schwander B, Kaier K, Hiligsmann M, Evers S, Nuijten M. Does the structure matter? An external validation and health economic results comparison of event simulation approaches in severe obesity. Pharmacoeconomics. 2022;40(9):901–915. doi:10.1007/s40273-022-01162-6
63. Abdelaal M, le Roux CW, Docherty NG, le Roux CW. Morbidity and mortality associated with obesity. Ann Transl Med. 2017;5(7):161. doi:10.21037/atm.2017.03.107
64. De Pergola G, Silvestris F. Obesity as a major risk factor for cancer. J Obes. 2013;2013:291546. doi:10.1155/2013/291546
65. Gentile S, Guarino G, Satta E, Strollo F. Treatment of insulin-induced skin lipohypertrophy: costs and sustainability of liposuction and education. Global Health Economics and Sustainability. 2024;2(2):2424. doi:10.36922/ghes.2424
66. Schwander B, Nuijten M, Hiligsmann M, Evers S. Event simulation and external validation applied in published health economic models for obesity: a systematic review. Expert Review of Pharmacoeconomics & Outcomes Research. 2018;18(5):529–541. doi:10.1080/14737167.2018.1501680
67. Schwander B, Nuijten M, Hiligsmann M, et al. Identification and expert panel rating of key structural approaches applied in health economic obesity models. Health Policy and Technology. 2020;9(3):314–322. doi:10.1016/j.hlpt.2020.03.005
68. World Health Organization. Obesity: preventing and managing the global epidemic: report of a WHO consultation. 2000.;
69. Petrou S, Jakovljevic M. Reimagining the relationship between economics and health–WHO ‘Health for all’provisions. Cost Effectiveness and Resource Allocation. 2024;22(1):5. doi:10.1186/s12962-024-00512-9
70. Taieb AB, Roberts E, Luckevich M, et al. Understanding the risk of developing weight-related complications associated with different body mass index categories: a systematic review. Diabetology & Metabolic Syndrome. 2022;14(1):186. doi:10.1186/s13098-022-00952-4
71. Bojke L, Claxton K, Sculpher M, Palmer S. Characterizing structural uncertainty in decision analytic models: a review and application of methods. Value Health. 2009;12(5):739–749. doi:10.1111/j.1524-4733.2008.00502.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.