")
Back to Journals » Infection and Drug Resistance » Volume 18
Cryosurgery and Next-Generation Sequencing Unravel Talaromycosis Mimicking an Airway Tumor: A Case Report
Authors Zhang Q , Zheng F, Pang Z, Xiang Y, Wang S
Received 8 January 2025
Accepted for publication 10 April 2025
Published 21 April 2025 Volume 2025:18 Pages 1985—1992
DOI https://doi.org/10.2147/IDR.S516461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Qinzhe Zhang,1 Fei Zheng,1 Zongdong Pang,1 Yonghong Xiang,1 Saibin Wang2
1Department of Pulmonary and Critical Care Medicine, Minzu Hospital of Guangxi Zhuang Autonomous Region, NanNing, Guangxi Province, 530000, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, Jinhua Municipal Central Hospital, Jinhua, Zhejiang Province, 321000, People’s Republic of China
Correspondence: Yonghong Xiang, Department of Pulmonary and Critical Care Medicine, Minzu Hospital of Guangxi Zhuang Autonomous Region, No. 232, East Mingxiu Road, NanNing, Guangxi Province, 530000, People’s Republic of China, Email [email protected] Saibin Wang, Department of Pulmonary and Critical Care Medicine, Jinhua Municipal Central Hospital, No. 365, East Renmin Road, Jinhua, Zhejiang Province, 321000, People’s Republic of China, Email [email protected]
Abstract: Tracheobronchial talaromycosis is uncommon in non-HIV infected patients. Reports on tracheobronchial talaromycosis presenting as a tumor-like lesion are also scarce, and the value of bronchoscopic cryosurgery in the treatment of tracheobronchial talaromycosis has not been mentioned. We report a case of tracheobronchial talaromycosis mimicking an airway tumor, which was diagnosed through bronchoscopic cryosurgery, next-generation sequencing(NGS), and tissue culture. The patient presented with neoplastic lesions in the airway and tested positive for anti-interferon-gamma autoantibody(AIGA). Clinical cure was achieved through bronchoscopic cryosurgery followed by a 2-week course of intravenous amphotericin B infusion and atomization induction therapy, along with 3 months of oral voriconazole maintenance therapy. In addition, we collected six reports summarizing the clinical data of tracheobronchial Talaromyces marneffei infection in non-HIV infected patients, including 14 patients with AIGA-positive, and discussed their clinical features. Our research may help increase physicians’ awareness of these types of diseases and provide resources for future diagnosis and treatment.
Keywords: talaromycosis, anti-interferon-gamma autoantibody, airway tumor-like lesions, next-generation sequencing, cryosurgery
Introduction
Talaromycosis is an invasive fungal disease caused by Talaromyces marneffei (T. marneffei) infection, belonging to the group of endemic fungal diseases. The traditional high incidence areas are Southeast Asia and southern China, and it has now spread to 34 countries worldwide.1 The disease primarily affects individuals with HIV, those with anti-interferon-gamma autoantibody(AIGA), patients with primary immunodeficiency disorders, individuals with diabetes mellitus, individuals undergoing cancer treatment or organ transplantation, or those using corticosteroids or immunosuppressants, as well as others with compromised immune function. Anti-interferon-gamma autoantibody-mediated immunodeficiency syndrome is a rare acquired immunodeficiency disorder characterized by the production of autoantibodies against interferon-gamma. These autoantibodies neutralize interferon-gamma activity, impairing STAT-1 phosphorylation and interleukin-12 (IL-12) secretion. Consequently, this results in severe defects in the Th1 cell-mediated immune response and impaired macrophage capacity to eliminate intracellular pathogens. This immunodeficiency predisposes individuals to severe or disseminated opportunistic infections, such as nontuberculous mycobacterial infections, T. marneffei infections, or mixed infections.
Currently, there have only been reports on the clinical characteristics of tracheobronchial talaromycosis in non-HIV infected patients,2 and there is limited information available regarding the characteristics of airway lesions in patients with AIGA-positive and talaromycosis. We report a case of tracheobronchial talaromycosis mimicking an airway tumor, which was diagnosed through bronchoscopic cryobiopsy, next-generation sequencing (NGS), and tissue culture, along with confirmation of AIGA-positive. The patient achieved clinical resolution through a combination therapy involving endobronchial cryotherapy, intravenous infusion of amphotericin B, atomization induction therapy for 2 weeks, followed by oral voriconazole maintenance therapy. This study was approved by the Ethics Committee of Minzu Hospital of Guangxi Zhuang Autonomous Region. Approval GMYLSTZ[2025] NO.12. And the procedures were conducted according to the principles of the Helsinki Declaration. To our knowledge, there have been no reports on the use of bronchoscopic cryosurgery in tracheobronchial talaromycosis with AIGA-positive. The detailed report is as follows:
Case Presentation
A 45-year-old female patient presented with a two-week history of persistent cough, productive sputum, and fever. Notably absent were dyspnea, hemoptysis, chest tightness, or night sweats. Initial chest CT imaging performed at an external facility demonstrated bilateral lower lobe pulmonary inflammation, prompting recommendation for post-treatment reevaluation. The patient denied any significant medical history or chronic underlying conditions. Physical examination findings were unremarkable. Initial hematological evaluation demonstrated leukocytosis (WBC 14.74 ×10⁹/L) with neutrophilic predominance (NEUT# 11.32 ×10⁹/L), accompanied by mild anemia (Hb 100 g/L) and normal platelet counts (PLT 352 ×10⁹/L). Elevated C-reactive protein (47.1 mg/L) confirmed systemic inflammation, while procalcitonin levels remained within normal limits (0.06 ng/mL). Serological screening returned negative results for HIV antibodies, fungal pathogens (β-D-glucan, galactomannan, cryptococcal antigen), and tumor markers. Hepatic, renal, cardiac, and biochemical profiles remained within normal parameters. Ultrasonographic evaluations of the urinary system, abdomen, and cardiac structures revealed no abnormalities. Repeat chest imaging with contrast-enhanced CT and three-dimensional reconstruction identified two critical findings: (1) an irregular nodule in the right upper lobe (Figure 1A) and (2) a neoplasm in the left main bronchus, causing luminal narrowing (Figure 1B). These imaging modalities were unable to definitively rule out lung cancer. Initial bronchoscopic evaluation identified an obstructive mass within the left main bronchus (Figure 2A). Microbiological analyses, including bacterial cultures, acid-fast bacilli smears, and Mycobacterium tuberculosis PCR, returned negative results. Histopathological examination of biopsied tissue demonstrated chronic mucosal inflammation with focal dysplasia, necrotic debris, and dense inflammatory infiltrates. Immunohistochemical (IHC) profiling demonstrated negative results for neoplastic markers, including Periodic acid-Schiff (PAS), Verhoeff–Van Gieson (VG), iron (Fe), Congo red, and acid-fast staining, while no definitive evidence of microbial pathogens was identified. Given inconclusive histopathology and persistent clinical suspicion of occult malignancy, bronchoscopic cryosurgery was performed under multidisciplinary consensus (Figure 2B). Post-procedural bronchoscopy at 7 days demonstrated near-complete lesion resolution with minimal residual mucosal irregularity (Figure 2C). Concurrently, tissue specimens underwent next-generation sequencing (NGS), The genomic material of T. marneffei was detected with the following parameters: 5 sequence reads, 55.56% relative abundance, and 0.0016% coverage depth. Subsequent sterile tissue cultures confirmed this finding, with the appearance of burgundy-colored colonies formed by T. marneffei (Figure 3), establishing disseminated talaromycosis. Comprehensive immunological evaluation revealed distinct abnormalities: Total T-lymphocytes accounted for 74.52% (2,117.17 cells/μL) of circulating lymphocytes, with CD4⁺ helper T cells representing 59.41% (1,762.58 cells/μL) and CD8⁺ cytotoxic T cells comprising 14.46% (428.89 cells/μL), yielding an elevated CD4⁺/CD8⁺ ratio of 4.11. Total CD45⁺ lymphocytes measured 2,842.51 cells/μL, while B lymphocytes (CD19⁺) were quantified at 332.04 cells/μL. Humoral immunity profiling showed elevated immunoglobulin levels (IgG: 18.81 g/L; IgA: 3.12 g/L; IgM: 1.68 g/L) with normal complement components (C3: 0.99 g/L; C4: 0.266 g/L). Notably, anti-interferon-gamma autoantibody(AIGA) tested positive via ELISA at high titers (1:100, 1:500, and 1:1000 dilutions). Adjuvant amphotericin B nebulization (10 mg bid) was initiated to enhance local antifungal penetration. Clinical improvement occurred rapidly, with defervescence within 24 hours and resolution of respiratory symptoms by 72 hours. Systemic therapy transitioned to oral voriconazole (200 mg bid) at 2-week follow-up. Three-month post-treatment assessment confirmed anatomical restoration: Chest CT: The mediastinal window shows normal appearance of the left main bronchus (Figure 4A). Surveillance bronchoscopy: Bronchoscopy reveals complete resolution of the mass in the left main bronchus, with a smooth and intact mucosal surface (Figure 4B). Notably, despite clinical resolution, serial AIGA titers demonstrated persistent elevation (1:1000 dilution) without symptomatic recurrence during 6-month follow-up. Whole-body Single-Photon Emission Computed Tomography/Computed Tomography (SPECT/CT) bone metabolic imaging revealed no osseous involvement.
 |
Figure 1 Chest Computed Tomography (CT) and Bronchoscopic Findings. Notes: (A) The chest CT reveals an irregular nodule in the right upper lobe. (B) The Mediastinal window reveals a neoplasm in the left main bronchus, causing luminal narrowing. |
 |
Figure 2 Comparison of the bronchial lumen before and after cryosurgery. Notes: (A) Bronchoscopy shows a mass in the left main bronchus, causing luminal narrowing. (B)Cryosurgery was performed within the bronchial lumen. (C) 1-week follow-up bronchoscopy after cryosurgery shows near-complete resolution of the mass, with slight irregularity at the base. |
 |
Figure 3 Sterile tissue culture media reveals the formation of burgundy-colored colonies. |
 |
Figure 4 3-month post-treatment Follow-up CT and Bronchoscopy Findings. Notes: (A) The mediastinal window shows normal appearance of the left main bronchus. (B) Bronchoscopy reveals complete resolution of the mass in the left main bronchus, with a smooth and intact mucosal surface. |
Discussion
T. marneffei is a dimorphic fungus that exhibits yeast phase growth at 37°C in the medium and hyphal phase growth at 25°C.Bamboo rats and humans are the primary hosts for this pathogen, with human infection believed to occur through inhalation of spores from the environment followed by systemic dissemination. Soil exposure, particularly during the rainy season, plays a critical role in T. marneffei infection. A study conducted in Guangxi, China found a 100% detection rate of T. marneffei infection among captured Bamboos silverstar rats (43 individuals). Other known infected species include Bamboos sinensis, Bamboos greater and Bamboos lesser. Individuals residing or traveling in endemic areas and those exposed to environments inhabited by bamboo rats should be considered as potential cases for diagnosis of T. marneffei infection.
T. marneffei infection is a significant concern that cannot be overlooked. The overall prevalence rate of HIV infection stands at 3.6%, with an alarmingly high mortality rate.1 Moreover, there has been a growing incidence of infections among individuals living with HIV.2 Talaromycosis primarily affects the skin, lungs, and reticuloendothelial system but can also spread to the bones, bone marrow, joints, lymph nodes, pericardium, liver, spleen, mesentery, and even the central nervous system. Common clinical manifestations include fever, weight loss, anemia, lymphadenopathy hepatosplenomegaly respiratory symptoms skin lesions and bone destruction.
Studies have demonstrated that the primary etiology of T. marneffei infection in HIV-negative individuals is attributed to the presence of AIGA-positive.3 In a recent publication,2 it was reported that 57.9% (11 out of 19) non-HIV patients with tracheobronchial T. marneffei infection exhibited elevated levels of AIGA. A prospective cohort study4 further indicated that patients with AIGA-positive and talaromycosis were predisposed to systemic dissemination, heightened inflammatory response, increased susceptibility to other intracellular pathogens, and had a poorer prognosis.
Tracheobronchial talaromycosis involvement is uncommon in non-HIV infected patients. As early as 2012, a case report5 described a non-HIV patient presenting with an airway tumor-like mass and obstructive pneumonia. In 2014, another case report6 documented a disseminated talaromycosis in a 28-year-old non-HIV male patient. Bronchoscopy revealed uneven protrusion in the subglottic airway wall. Subsequently, in 2015, bronchoscopy findings of multiple submucosal nodules at the left end of the trachea were reported7 in another non-HIV patient. In 2021, it was reported3 that a case of talaromycosis, associated with AIGAs-positive and co-infected with Burkholderia cepacia, exhibited nodular changes in the left upper and lower lobes of the bronchus during bronchoscopy examination. Furthermore, In 2023, a diagnosis of AIGA-positive T. marneffei infection was confirmed through ultrasound-guided transbronchial needle aspiration (TBNA) and metagenomic next-generation sequencing (mNGS) in a patient presenting with left bronchial stenosis and obstruction. Imaging revealed a proliferative lesion at the orifice of the left upper lobe bronchus and a peanut-sized nodular lesion in the lower lobe bronchus, mimicking neoplastic pathology.8 No subsequent case reports have been published since then; most previous reports describe diffuse proliferative nodular lesions that are more frequently observed among males. The latest report,2 which includes data from our department on 19 cases of non-HIV tracheobronchial T. marneffei infection (57.9% male), describes intratumor tumor-like lesions causing obstruction similar to those previously reported by Simon A Joosten in 2012. However, no AIGA were detected in this particular patient’s case. The patient described in our paper exhibited AIGA-positive, and the etiological diagnosis was obtained through tissue culture and next-generation sequencing (NGS) following bronchoscopic cryobiopsy. The induction treatment involved bronchoscopic cryosurgery combined with local amphotericin B intravenous drip and atomization therapy, along with oral voriconazole maintenance therapy for a duration of 2 weeks. In seven studies (Table 1), the age range of patients with HIV-negative tracheobronchial T. marneffei infection disease was 28–62 years, with a median age of 52 years. The majority of patients were male. The cases were predominantly from the Guangxi region in China. Common symptoms included fever, cough, sputum production, fatigue, weight loss, and lymphadenopathy. The most common imaging findings were patchy shadows, consolidation, bronchial stenosis/obstruction, mediastinal lymphadenopathy, and pleural effusion. Mucosal congestion and edema, nodular protrusions, and purulent secretions were observed in bronchoscopy findings. In the 14 cases that were positive for AIGA, the clinical characteristics were similar to the overall cohort but with more prominent weight loss and pleural effusion. Imaging findings more frequently revealed mass-like lesions, bronchial stenosis, and mediastinal lymphadenopathy. Bronchoscopy findings in these AIGA-positive cases primarily showed mucosal hyperplasia, thickening, nodular occlusion of the airway, and necrotic tissue attachment. The imaging and bronchoscopy features in AIGA-positive cases were more complex, warranting heightened awareness of opportunistic infections. These patients were more likely to receive combination therapy, and their mortality rate was higher than the overall cohort, potentially due to co-infections or extensive disease involvement. Our case reported in this study showed a left main bronchus mass on bronchoscopy, with imaging indicating a tumor-like lesion. Multiple routine bronchoscopy biopsies failed to make a diagnosis. However, frozen biopsy followed by next-generation sequencing (NGS) of tumor tissue eventually led to a definitive diagnosis. This highlights the diagnostic value of frozen biopsy and tissue NGS in tumor-like diseases. The patient responded well to treatment, possibly due to early intervention and the absence of co-infections.
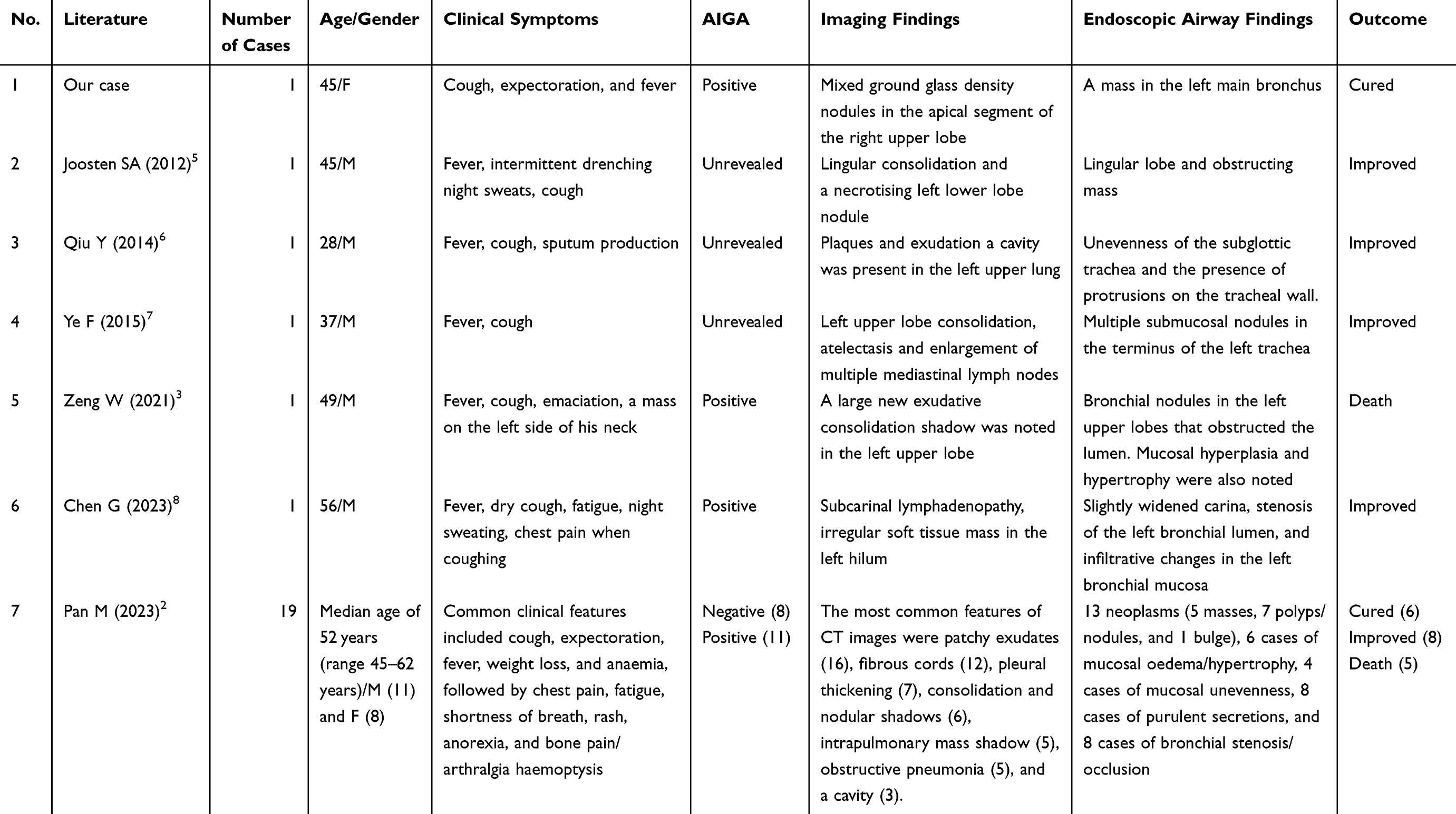 |
Table 1 Clinical Characteristics of Patients with Non-HIV Infection of Tracheobronchial T. marneffei Infection and 14 Patients with AIGAs-Positive |
Conclusion
Talaromycosis airway involvement, though rare, poses significant diagnostic challenges due to its propensity to mimic malignancy radiologically and endoscopically. Early bronchoscopic biopsy with fungal culture and Next-Gen Sequencing is critical in endemic areas. In such cases, The acquisition of sizable specimens can be achieved through transbronchial cryobiopsy, while next-generation sequencing can provide etiological results. Apart from the conventional standard drug treatment, Cryosurgery offers distinct advantages in managing benign airway diseases, including minimal damage, reduced complications, and evident therapeutic efficacy. Combined with systemic antifungals, this approach offers a paradigm for managing complex airway infections.
Abbreviations
NGS, next-generation sequencing; AIGA, anti-interferon-gamma autoantibody; SPECT/CT, Single-Photon Emission Computed Tomography/Computed Tomography; T. marneffei, Talaromyces marneffei; IHC, Immunohistochemical.
Data Sharing Statement
The datasets used in the case are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Minzu Hospital of Guangxi Zhuang Autonomous Region. Approval GMYLSTZ[2025] NO.12. Institutional approval to publish the case details was also secured from the Ethics Committee of Minzu Hospital of Guangxi Zhuang Autonomous Region. And the procedures were conducted according to the principles of the Helsinki Declaration.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying figure.
Acknowledgments
We would like to express our heartfelt gratitude to the Science and Technology Department of Guangxi Zhuang Autonomous Region for their invaluable support and funding of this research project (No. 2023GXNSFAA026291).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wang F, Han R, Chen S. An overlooked and underrated endemic mycosis-talaromycosis and the pathogenic fungus Talaromyces marneffei. Clin Microbiol Rev. 2023;36:e0005122. doi:10.1128/cmr.00051-22
2. Pan M, Fang G, Zheng F, et al. Clinical characteristics of tracheobronchial Talaromyces marneffei infection in non-HIV-infected patients in South China. Ann Med. 2023;55.
3. Zeng W, Qiu Y, Tang M, et al. Talaromyces marneffei and Burkholderia cepacia co-infection in a HIV-uninfected patient with anti-interferon-γ autoantibodies. Infect Drug Resist. 2021;14:2173–2177. doi:10.2147/IDR.S312042
4. Chen Z-M, Li Z-T, Li S-Q, et al. Clinical findings of Talaromyces marneffei infection among patients with anti-interferon-γ immunodeficiency: a prospective cohort study. BMC Infect Dis. 2021;21:21. doi:10.1186/s12879-020-05633-z
5. Joosten SA, Hannan L, Heroit G, Boerner E, Irving L. Penicillium marneffei presenting as an obstructing endobronchial lesion in an immunocompetent host. Eur Respir J. 2012;39:1540–1543. doi:10.1183/09031936.00156911
6. Qiu Y, Zhang J, Liu G, et al. A case of Penicillium marneffei infection involving the main tracheal structure. BMC Infect Dis. 2014;14:242. doi:10.1186/1471-2334-14-242
7. Ye F, Luo Q, Zhou Y, et al. Disseminated penicilliosis marneffei in immunocompetent patients: a report of two cases. Indian J Med Microbiol. 2015;33:161–165. doi:10.4103/0255-0857.148433
8. Chen G, Ma N, Zhu D, et al. Accurate diagnosis of bronchopulmonary Talaromyces marneffei infection in an anti-IFN-γ autoantibodies positive patient assisted by endobronchial ultrasound-guided TBNA and mNGS: a case report. Front Cell Infect Microbiol. 2023;13.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.