")
Back to Journals » Journal of Pain Research » Volume 18
CT Angiographic Evaluation of Superior Gluteal Artery Branches in Lateral Sacroiliac Joint Fusion: A Pilot Study to Inform Preoperative Surgical Planning and Anatomic Parameters
Authors Mallard CJ , Harned ME, Grider JS
Received 7 February 2025
Accepted for publication 11 June 2025
Published 19 June 2025 Volume 2025:18 Pages 3069—3075
DOI https://doi.org/10.2147/JPR.S514778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Christopher J Mallard, Michael E Harned, Jay S Grider
Department of Anesthesiology, University of Kentucky, Lexington, KY, USA
Correspondence: Christopher J Mallard, University of Kentucky, 2400 Greatstone Point Suite A-100, Lexington, 40504, KY, USA, Email [email protected]
Introduction: The sacroiliac (SI) joint can be a source of low back pain. Surgical techniques for fusion include lateral transiliac, posterolateral, sacro-alar iliac and posterior interpositional fixations. Although these various trajectories are supported by the literature, the lateral transiliac approach is the most extensively studied. However, this technique has been associated with concern for potential injury to branches of the superior gluteal artery (SGA). Currently, no preoperative workup includes the evaluation of SGA and its branches for location and potential injury during lateral fusion. We propose a clinical pathway for the identification and risk stratification of SGA injuries using preoperative CT of the pelvic vasculature and measurements of the proposed transiliac screw sites.
Purpose: To determine whether preprocedural CT angiography (CTA) can identify the course of the SGA and its branches in relation to planned lateral transiliac SI joint fusion trajectories, thereby informing surgical planning and potentially reducing vascular risk.
Patients and Methods: Twenty patients underwent preoperative CTA. Angiographic images were processed to generate a 3D vascular reconstruction. The proposed screw locations were identified, measured, and analyzed using descriptive statistics.
Results: 20 patients’ images were analyzed with the average distance to the nearest SGA branch on the right being 19.0 mm ± 9.4 mm (minimum distance 5.75mm) and 17.3 mm ± 7.9 mm (minimum distance 5.97mm) on the left. Screw placement was altered in 1 of the 10 patients with an average total estimated blood loss (EBL) of 6.5mL ± 2.4mL in surgical patients.
Conclusion: This pilot study suggests that preoperative CTA may aid proceduralists in planning lateral transiliac sacroiliac joint fusion by identifying the course of the SGA and its branches, potentially reducing the risk of vascular injury.
Keywords: superior gluteal artery, sacroiliac joint fusion, lateral transiliac, sacroiliac joint, minimally invasive spine surgery, sacroiliitis
Introduction
The sacroiliac (SI) joint can account for 15%–30% of chronic low back pain. This percentage increases to approximately 40% in patients with a history of lumbar fusion.1–4 The treatment options for chronic SI joint pain include physical therapy, medications, intra-articular injections, radiofrequency ablation and surgical fusion.1 Currently, three trajectories can be utilized for the outpatient fusion of the SI joint (posterior, posterolateral, and lateral).1,2 An algorithm proposed by Falowski et al5 was designed to create a paradigm for SI joint diagnosis and treatment; however, the question of which fusion approach is most efficacious remains. This was addressed in a meta-analysis conducted by Whang et al.1 They suggest that the lateral transiliac approach (LTI) demonstrated superior efficacy compared to the posterolateral transiliac (PLI) fixation or posterior interpositional (PI) approaches for pain and Oswestry Disability Index (ODI) reduction. Moreover, there was less radiographic evidence of lucency with LTI indicative of nonunion compared with PLI.1 Given the evidence, the LTI approach may have an advantage in clinical outcomes over PI or PLI approaches. However, a concern for the LTI approach is injury to the superior gluteal neurovascular complex.4 Knowledge of the course of the SGA and its branches can be helpful in avoiding iatrogenic injuries when considering the use of the LTI approach for SI joint arthrodesis.
The SGA is the largest terminating branch of the internal iliac artery. It emerges from the pelvis, passing through the lower edge of the greater sciatic notch and upper edge of the piriformis muscle. The SGA then branches to form the deep and superficial branches. The deep branch continues to branch forming an abundance of perforating branches supplying the gluteus medius and the gluteus minimus as it courses between them. The deep branch then further divides into the deep superior and inferior branches. The deep superior branch continues along the upper edge of the gluteus minimus until the anterior superior spine. The deep inferior branch courses through the gluteus minimus to the greater trochanter. The superficial branch goes inward and upward to the upper gluteus maximus and the skin behind the sacrum. The venous drainage is anatomically analogous to the arterial system.6–8 In the orthopedic trauma literature, there has been studies looking at the relation of the SGA and its branches to iliosacral screws (IS) and transsacral screws (TS) down to the third sacral segment. In a cadaver study published by Collinge et al they reported a variable branching pattern of the superior gluteal neurovascular bundle after they exit the greater sciatic notch. 10 of 58 (18%) iliosacral screws that were placed by a single surgeon caused injury to the superior branch of the superior gluteal nerve and vessels; 8 neurovascular bundles were impaled, and 2 others were partly entrapped between the screw head and the ilium.9 In 2017, Collinge and Maslow published risks to the SGA neurovascular bundle using CT angiography and transsacral screws due to the popularity of their insertion access. They evaluated 20 CT angiographies of the pelvis and excluded those with significant pelvic dimorphism as well as those without a safe corridor for the proposed screw trajectory. The reported average distances from the superior gluteal artery to the modeled screws being 25.3 mm (± 9.2) for S1 IS, 12.4 mm (± 9.0) for S1 TS, and 23.6 mm (± 10.7) for S2 TS screws, respectively. Ten S1 TS screws (25%), no S1 IS screws, and no S2 TS screws were projected to have caused injury to the SGA neurovascular bundle (P < 0.001).10 Mahato proposed an alternative method for evaluating neurovascular risk using an anatomical grid system, which was overlaid on cadaver specimens to facilitate measurement. The overlayed grid system found that the superficial branch more frequently encroached upon and traversed the osseous sacral area labeled “D” compared to the deep branch.11 In the 1990’s Routt et al published on the applied anatomy of the sacrum and pelvis regarding iliosacral screw fixation along with a case report of SGA injury during iliosacral screw placement.12,13 He discussed optimizing supine position for surgery, preprocedural planning with CT scans and fluoroscopic intra-procedural anatomy along with noting that the iliac vessels are best appreciated on CT scans performed after angiographic embolization to control hemorrhage.12 In the case report injury to the SGA occurred during insertion of the drill guide through the buttock stab wound after the anterior pelvic ring reductions were secured openly. Diffuse bleeding occurred from the percutaneous wound site resulting in 1 liter of blood loss. This was due to a perforated branch of the left superior gluteal artery which required embolization.13
In contrast to the reported rates of SGA neurovascular injury in the orthopedic trauma literature the reported rate of bleeding requiring procedural intervention during LTI procedures is approximately 0.04%.1 However, the potential risk of injury to the superior gluteal artery and its branches has been cited as a key factor influencing procedural approach selection among non-orthopedic interventionalists.5 The specific aim of this pilot study was to evaluate whether preprocedural CT angiography can identify the course of the SGA and its branches in relation to planned trajectories for lateral transiliac sacroiliac joint fusion (Figure 1). We propose that this approach allows for assessment of individual anatomical variation and consideration of trajectory planning. Although angiographic and cadaver-based studies related to iliosacral and transsacral trajectories have evaluated the SGA and its branches in the orthopedic trauma literature, to our knowledge, no angiographic studies have specifically examined SGA anatomy in the context of preoperative planning for lateral transiliac sacroiliac joint fusion.
 |
Figure 1 3-D CT angiographic reconstruction of the sacroiliac joint demonstrating measurement technique and proposed lateral transiliac screw trajectories relative to the nearest vascular branch. |
Material and Methods
All patients deemed candidates for sacroiliac joint (SIJ) fusion surgery at a single academic medical center between February 2024 and December 2024 were included in this study. This retrospective study was conducted in accordance with the ethical principles of the Declaration of Helsinki and its subsequent amendments. Approval was obtained from the Institutional Review Board at the University of Kentucky prior to data collection and analysis (IRB Protocol #99588). All data was de-identified prior to analysis to protect patient confidentiality. No identifiable personal information has been included in this publication. The study involved no direct contact with patients and posed no more than minimal risk. All data were handled in a manner that protected patient confidentiality. No identifiable personal information was collected or reported. The study posed no more than minimal risk to participants and included no interventions or changes to patient care. Failure of conservative measures prior to surgical discussion included physical therapy, medication trials, two separate selective injections into the sacroiliac joint under fluoroscopy with greater than 75% relief in pain for the duration of the local and no long-term relief with intra-articular steroids. Preoperative imaging consisted of computed tomography angiography (CTA) of the pelvis and CT scan of the bony pelvis. Angiographic images were processed by the Department of Radiology to generate a 3D reconstruction of pelvic vasculature. Using the imaging software eUnity v7.4.4.401 the reconstructed 3-D images provided were rotated in the horizontal axis to provide a true lateral view where we aligned the greater sciatic notches, hip joints and alar lines as possible. Next, using the included liner measurement tool within the software the proposed screw locations were measured to the nearest location of vasculature and recorded. This was performed on both the left and right sides for all patients within the study regardless of the side being treated. For patients who proceeded to surgery, estimated blood loss (EBL) was recorded. In accordance with our preoperative planning workflow, we documented any instances where angiographic findings necessitated changes to the intended screw trajectory. All measurements and surgical data were compiled using Microsoft Excel 16.91. Descriptive statistics, including mean and standard deviation, were calculated for all variables.
Results
Twenty patients who were identified as SI joint fusion candidates in this pilot study underwent preoperative CT angiography of the pelvis. 30% of the patients were male (6/20) and 70% were female (14/20), with a mean age of 56 ± 13 years (min 36 years, max 76 years) and an average body mass index (BMI) of 32 ± 6 (min 20.8, max 46.82). The average Preoperative Visual Analog Scale (VAS) score was 6/10 ± 2/10 (min 2/10, max 8/10), and preoperative Oswestry Disability Index (ODI) was 42% ± 16% (min 11%, max 35%). 25% of the patients (5/20) were on opioids, with an average morphine milligram equivalent (MME) of 25 ± 9 (min 0, 33.75 max) (Table 1).
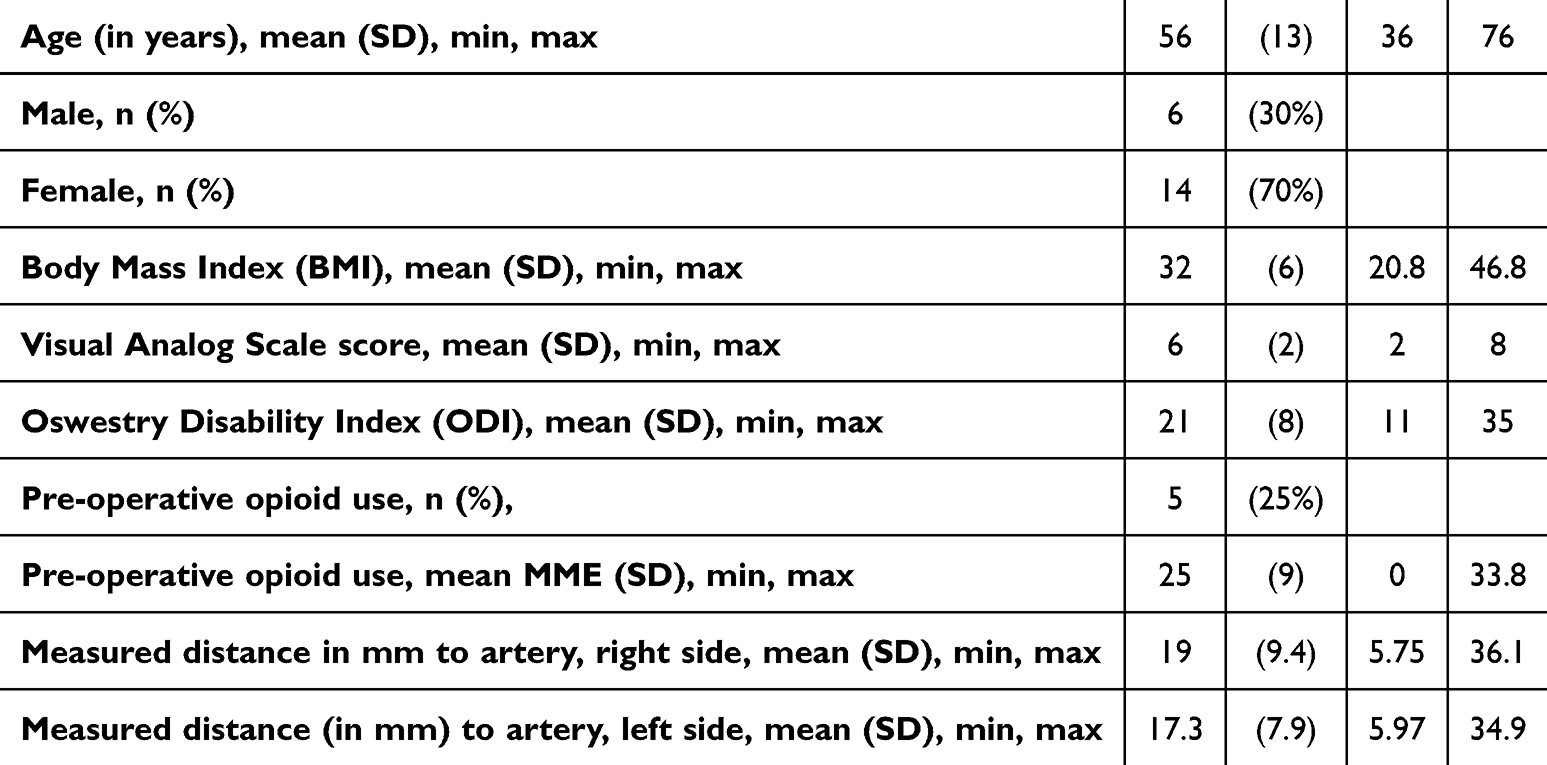 |
Table 1 Participant Demographics and Baseline Characteristics (n=20) |
The average distance to the superior gluteal artery (SGA) on the right was 19.0 mm ± 9.4 mm (min 5.75 mm, max 36.1 mm) (Figure 2). The average distance to the SGA on the left was 17.3 mm ± 7.9 mm (min 5.97 mm, max 34.9 mm) (Figure 3). The intended conventional screw placement was changed because of the preoperative CTA results in 1 of the 10 (10%) cases who underwent surgery to be slightly more posterior than the standard. This was due to the proposed conventional location being deemed too close anatomically by the treating physician, however the conventional location would not have violated the SGA. The estimated blood loss (EBL) for the completed 10 cases was 6.5mL ± 2.4mL (min 5mL, max 10mL) (Table 2).
 |
Table 2 Surgical Characteristics (n=10) |
 |
Figure 2 Distance from nearest branch of the right superior gluteal artery branch to fixation point by patient (n=20). |
 |
Figure 3 Distance from nearest branch of the left superior gluteal artery branch to fixation point by patient (n=20). |
Discussion
The current pilot study utilized three-dimensional CTA to map the surgical field for pre-procedure planning and to determine the distance from the closest arthrodesis fixation point to the SGA and its branches. The arterial distance from the most ventral fixation point was approximately 18 mm, suggesting that proximity to the SGA was not a major consideration in this cohort of patients. Further, while the standard deviation was 9.4 mm (right) and 7.8 mm (left), a branch of the SGA in one patient did impact the surgical procedure by slightly altering the placement of the second fixation screw more dorsal by approximately 1–2 mm. However, it should be noted that in this patient the conventional location would not have violated the superficial branch of the SGA. Regarding outcomes, while being a secondary consideration in this study we report a minimal estimated blood loss (range 5mL–10mL) in the 10 patients who underwent surgical fusion.
The lateral transiliac (LTI) approach represents the most commonly used technique for sacroiliac (SI) joint fusion. It evolved from the original open approach described by Smith-Petersen in 1921 and was later influenced by the development of iliosacral screw fixation techniques in pelvic trauma, as described by Dr. Routt in the 1990s. As a result, the LTI approach has historically been performed by surgeons. However, as technology has evolved from both an imaging and a minimally invasive procedural aspect, the arrival of posterior-lateral transiliac (PLI) and posterior interpositional (PI) approaches has opened the treatment of SI joint pain to interventionalists from other disciplines. Given the prevalence of SI joint pain in the population and its relative underdiagnosis in previous decades, the demand for SI joint evaluation and treatment will certainly increase. Similarly, as the rate of lumbar spinal fusion increases, the incidence of SI joint pain also increases concomitantly, resulting in a patient’s demographic need for evaluation and management. As procedural technology and safety have continued to progress, interventionalists now have the capability to perform LTI; however, the looming question is of possible damage to the SGA and its branches.2
The present pilot study suggests that this risk can potentially be further mitigated through proper pre-procedural evaluation. The ability to plan the trajectory with CT angiography would also allow a given patient who might be identified as having arterial structures in the cannulation pathway to be offered PI or PLI, should these structures be identified. This assurance of safety is welcome, as the efficacy of the LTI fixation approach has data suggesting superiority over conventional medical management in terms of both VAS and ODI. When compared with PLI and PI, we are unaware of any studies with an experimental design that directly compare the LTI approach to posterior approaches from an efficacy or safety standpoint. The studies regarding PLI and PI approaches that have been performed are largely case reviews, case series, or retrospective in nature, with one relatively large-scale prospective observational study with 171 subjects that demonstrated improvement in the ODI and McGill scores. The study performed by Fuchs and Ruhl reported a lower than expected SI joint fusion rate, as demonstrated on CT scans (31%).14 Taken together, this data suggests that, while the posterior approach has clinical efficacy, it may do so with a lesser degree of radiographic joint fusion. The results of this pilot study highlight the need for larger, prospective studies to more fully characterize the clinical implications of these findings. However, our results suggest that preprocedural planning with CT angiography may help reduce the risk of injury to the SGA and its branches during lateral transiliac sacroiliac joint fusion.
There a several limitations of the current study. First, we include a small sample size and is thus under powered to make any accurate conclusion regarding variation in the location of the SGA and its branches based on ethnicity or other demographic factors. Secondly, a single investigator performed all the measurements as they use the technique for preoperative planning of all LTI surgeries. Measurements from other investigators could be beneficial from an interobserver reliability standpoint but could also introduce variability and error. Thirdly, the use of CT angiography itself represents a potential limitation of this approach. As part of our workflow, patients with contraindications to iodinated contrast, such as contrast allergy or impaired renal function, would have been excluded; however, no such cases were encountered during the time frame of this pilot study. Nonetheless, CTA does involve additional radiation exposure beyond standard CT imaging of the bony pelvis. It also introduces added healthcare costs, increased procedural time, and logistical considerations that may impact patient access. While a comprehensive cost-benefit analysis is beyond the scope of this manuscript, these trade-offs are important considerations when evaluating the potential utility of CTA in preoperative planning for SI joint fusion.
Given that the current study is a pilot designed to demonstrate the feasibility of preoperative mapping of the SGA and its branches, larger studies are necessary to more definitively characterize the proximity of surgical trajectories to the SGA and its branches during lateral transiliac SI joint fusion. Prior studies in the orthopedic trauma literature, such as those by Zhao et al15 and Routt et al12 have evaluated SGA vascular anatomy in patients with pelvic trauma, which may not reflect typical anatomy in elective SI joint fusion candidates. Collinge and Maslow10 used CT angiography in their assessment of iliosacral and transsacral screw fixation, but excluded patients with significant pelvic dimorphism or those lacking a safe osseous corridor for screw placement, potentially limiting generalizability to the elective SI joint fusion candidates. In contrast, Eastman et al16 evaluated a random population of patients who presented to the emergency department requiring CT angiography of the pelvis without pelvic trauma, but their analysis focused on the S3 segment, an anatomical region too caudal to be relevant to conventional LTI approaches to SI joint fusion. Zhao et al8 in their 2018 study also analyzed vascular anatomy relative to iliosacral fixation and reported that in 45.1% of cases, the deep superior branch of the SGA passed through the defined “safe area” near the S1 entrance point, with the shortest distance between the artery and bone measuring 0.86 ± 0.84 cm. While similar in technique, their findings are different from what we present here which further supports the need for larger studies. Mahato’s11 cadaveric study used an anatomical grid system to overlay surgical zones and found that the superficial branch of the SGA more frequently encroached on the proposed surgical area compared to the deep branch. These findings underscore the variability of SGA anatomy and support the need for individualized vascular assessment, particularly in elective fusion procedures. Given that the current study is a pilot to demonstrates the feasibility of mapping the SGA and its branches, larger studies are required to determine with certainty the proximity of the procedural field to the SGA and its branches. However, the current report does provide a framework to act as a springboard to these discussions.
Conclusion
This pilot study aims to demonstrate the feasibility of using CT angiography as a preoperative planning tool to assess the course of the superior gluteal artery and its branches in relation to the proposed trajectory of lateral transiliac screws for sacroiliac joint fusion. Although the sample size is limited to 20 patients, our findings suggest that this imaging-based approach may help proceduralists further minimize the risk of vascular injury when employing the LTI technique. Notably, in 1 of 20 cases (5%), the planned screw trajectory was altered based on angiographic findings to reduce the risk of superior gluteal artery injury (although the conventional placement would not have violated the SGA branches). Larger, prospective studies are needed to validate these preliminary findings and to better characterize anatomic variability relevant to surgical planning.
Disclosure
Christopher J. Mallard and Michael E. Harned have received institutional grants from Medtronic. Christopher J. Mallard is a consultant for Johnson and Johnson. The authors report no other conflicts of interest in this work.
References
1. Whang PG, Patel V, Duhon B, et al. Minimally Invasive SI Joint Fusion Procedures for Chronic SI Joint Pain: systematic Review and Meta-Analysis of Safety and Efficacy. Int J Spine Surg. 2023;17(6):794–808. doi:10.14444/8543
2. Lee DW, Patterson DG, Sayed D. Review of Current Evidence for Minimally Invasive Posterior Sacroiliac Joint Fusion. Int J Spine Surg. 2021;15(3):514–524. doi:10.14444/8073
3. Polly DW, Swofford J, Whang PG, et al. Two-Year Outcomes from a Randomized Controlled Trial of Minimally Invasive Sacroiliac Joint Fusion vs Non-Surgical Management for Sacroiliac Joint Dysfunction. Int J Spine Surg. 2016;10:28. doi:10.14444/3028
4. Calodney A, Azeem N, Buchanan P, et al. Safety, Efficacy, and Durability of Outcomes: results from SECURE: a Single Arm, Multicenter, Prospective, Clinical Study on a Minimally Invasive Posterior Sacroiliac Fusion Allograft Implant. J Pain Res. 2024;17:1209–1222. doi:10.2147/JPR.S458334
5. Falowski S, Sayed D, Pope J, et al. A Review and Algorithm in the Diagnosis and Treatment of Sacroiliac Joint Pain. J Pain Res. 2020;13:3337–3348. doi:10.2147/jpr.S279390
6. Gabryszuk K, Gliwa J, Dziedzic M, et al. The superior gluteal artery and the posterior division of the internal iliac artery: an analysis of their complete anatomy. Folia Morphologica. 2023. doi:10.5603/fm.96695
7. Aj P, Zwirner J, Doyle T, Hammer N. A Systematic Review of the Normal Sacroiliac Joint Anatomy and Adjacent Tissues for Pain Physicians. Pain Physician. 2019;22(4):E247–E274.
8. Zhao Y, You L, Lian W, et al. Anatomical relation between S1 sacroiliac screws’ entrance points and superior gluteal artery. J Orthopaedic Surg Res. 2018;13(1):1–6. doi:10.1186/s13018-018-0713-5
9. Collinge C, Coons D, Aschenbrenner J. Risks to the Superior Gluteal Neurovascular Bundle During Percutaneous Iliosacral Screw Insertion: an Anatomical Cadaver Study. J Orthop Trauma. 2005;19(2):96–101. doi:10.1097/00005131-200502000-00005
10. Maslow J, Collinge CA. Risks to the superior gluteal neurovascular bundle during iliosacral and transsacral screw fixation: a computed tomogram arteriography study. J Orthop Trauma. 2017;31(12):640–643. doi:10.1097/BOT.0000000000000996
11. Mahato NK. Topographic localization of the sacroiliac joint and superior gluteal artery branches on the posterolateral ilium. Clin Anat. 2023;36(7):971–976. doi:10.1002/ca.24005
12. Routt Jr MC, Simonian PT, Inaba J. Iliosacral screw fixation of the disrupted sacroiliac joint. Tech Orthopaedics. 1994;9(4):300–314. doi:10.1097/00013611-199400940-00010
13. Altman DT, Jones CB, Mlcj R. Superior Gluteal Artery Injury During Iliosacral Screw Placement. J Orthop Trauma. 1999;13(3):220–222. doi:10.1097/00005131-199903000-00011
14. Fuchs V, Ruhl B. Distraction arthrodesis of the sacroiliac joint: 2-year results of a descriptive prospective multi-center cohort study in 171 patients. Eur Spine J. 2018;27(1):194–204. doi:10.1007/s00586-017-5313-2
15. Zhao P, Wang X, Chen X, Guan J, Wu M. Preoperative CT simulation of iliosacral screws for treating unstable posterior pelvic ring injury. BMC Musculoskeletal Disord. 2022;23(1):220. doi:10.1186/s12891-022-05155-6
16. Eastman JG, Kuse QA, Routt MLC, Shelton TJ, Adams MR. Superior gluteal artery injury risk from third sacral segment transsacral screw insertion. Eurn J Orthop Surg Traumatol. 2022;32(5):965–971. doi:10.1007/s00590-021-03073-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.