")
Back to Journals » Journal of Pain Research » Volume 18
Day-to-Day Risk and Resilience Factors in the Context of Pediatric Post-Surgical Recovery – A Network Analysis of Intensive Longitudinal Data From Adolescents Undergoing Spinal Fusion Surgery and Their Parents
Authors Thorsell Cederberg J, Lavefjord A, Sundström FTA, Bartels SL, Zetterqvist V, Wicksell RK, McCracken L, Goubert L
Received 15 October 2024
Accepted for publication 6 February 2025
Published 24 March 2025 Volume 2025:18 Pages 1545—1561
DOI https://doi.org/10.2147/JPR.S501009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Jenny Thorsell Cederberg,1,2 Amani Lavefjord,1 Felicia TA Sundström,1 Sara Laureen Bartels,2,3 Vendela Zetterqvist,2,4 Rikard K Wicksell,2,5 Lance McCracken,1 Liesbet Goubert6
1Department of Psychology, Uppsala University, Uppsala, Sweden; 2Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden; 3Department of Psychiatry and Neuropsychology, Maastricht University, Maastricht, the Netherlands; 4Department of Medical Sciences, Uppsala University, Uppsala, Sweden; 5Pain Clinic, Capio S:t Göran Hospital, Stockholm, Sweden; 6Department of Experimental-Clinical and Health Psychology, Ghent University, Ghent, Belgium
Correspondence: Jenny Thorsell Cederberg, Department of Psychology, Uppsala University, Von Kraemers allé 1A och 1C, Uppsala, SE-75237, Sweden, Tel +460184710000, Email [email protected]
Objective: Ineffective pediatric post-operative pain management increases the risk of Chronic Post-Surgical Pain (CPSP), affecting around 20% of children undergoing major surgery. Psychological predictors of recovery, in both children and their parents, have been identified. However, how these variables change throughout the recovery process remains unclear. The aim of the present study was to investigate the associations of adolescent and parental risk and resilience variables in everyday life, during post-operative recovery, for adolescents undergoing spinal fusion surgery.
Methods: Participants were adolescents with Idiopathic Scoliosis (AIS), aged 12– 18 years, undergoing spinal fusion surgery, and their parents, recruited at four hospitals in Belgium. Participants completed daily assessments for 7 consecutive days, at 5 time-points, before surgery, and at 3 and 6 weeks, and 6 and 12 months, post-surgery. Diary measures included adolescent and parental pain and recovery variables known to be relevant in the context of pediatric post-operative pain. Network analysis was used to explore correlations between all variables throughout the post-operative recovery process.
Results: The sample comprised N=190 participants. Associations were stronger within adolescent and parent variables, than between them. For adolescents, psychological flexibility was associated with positive mood and activity engagement, and pain intensity with pain catastrophizing and activity avoidance. For parents, higher levels of pain-related fear and catastrophizing were related to more parent-to-child instructions to avoid activities. Regarding adolescent-parent between correlations, parental instructions to avoid activities were associated with adolescent physical complaints and activity avoidance, and parent pain catastrophizing was associated with adolescent pain-related fear and catastrophizing. Generally, networks displayed both similarities and differences across post-operative phases.
Discussion: The study sample was small in relation to the statistical analyses conducted. Even so, the present findings provide a new perspective on psychological predictors at play in everyday life throughout the pediatric post-operative recovery process, indicating important targets, both clinical and for future investigation.
Keywords: post-operative recovery, risk and resilience factors, adolescents, parents, diary data, network analysis
Introduction
Globally, millions of children undergo surgery each year.1 Adequate post-operative pain management improves recovery after surgery and has been the focus of a global health initiative in recent years.2–4 However, many pediatric patients still receive insufficient post-operative care. Ineffective pain management may result in unnecessary patient suffering and poorer recovery, and increases the risk of Chronic Post-Surgical Pain (CPSP).5–7 CPSP is defined as pain that persists longer than the usual period of healing (typically >3 months) and that cannot be explained by any other peri- or post-operative complications. CPSP affects around 20% of pediatric patients undergoing major surgery and is associated with reduced quality-of-life and impaired functioning.7, 8 One example of major surgery is spinal fusion surgery, one of the most invasive pediatric procedures, used for correction of adolescent idiopathic scoliosis (AIS), leading to an increased risk of CPSP and associated long-term health problems for this patient group.9–11
Several psychological mechanisms have been identified as predictors of pediatric post-operative recovery. For instance, anxiety and pain catastrophizing are known risk factors for CPSP, whereas pain coping and pain acceptance represent key resilience factors.7,12,13 Resilience here means the capacity to maintain effective functioning despite the exposure of external and/or internal stressors, such as pain.14,15 The biopsychosocial model can be used to understand the transition from acute pain to CPSP, in which resilience and parental factors are underscored as important targets for future research.16 Parental factors are associated with child pain and functioning in the context of pediatric chronic pain where both parental emotional states and behavior can affect child outcomes.17 In two recent studies investigating parental factors in relation to CPSP, pain catastrophizing and psychological flexibility in parents before surgery, predicted recovery in the children at one-year follow-up.13,18 Yet, more research is needed to further investigate how different psychological processes in the children themselves, and how parental processes, before and after surgery, impact post-operative recovery in children and adolescents.
Most often, nomothetic, or group-based, data collected at a small number of fixed time-points has been used in pain research. During the past years, the need to further refine pain treatments to better meet the needs of the individual has been emphasized with more focus on process-based research.19,20 In line with this ambition, and complementary to more traditional group-level data, Experience Sampling Methods (ESM) and daily diary studies emerge, including repeated high-frequency assessments of persons in their everyday lives.21 These methods allow capturing how persons think, feel and behave in the moment and are particularly suitable for studying change processes during major transitions, such as post-operative recovery following surgery.22 In a diary study investigating parental processes relevant for adolescents with chronic pain, daily parental psychological flexibility was indirectly associated with lower activity avoidance and higher activity engagement in adolescents, via an association with parental protective responses and activity-engagement instructions.23 Moreover, in a 7-day diary study for adults undergoing joint arthroplasty, daily post-surgical catastrophizing was associated with pain intensity during the acute phase and daily emotional distress was associated with pain intensity and interference during the sub-acute phase and with pain interference at 3-month follow-up.24 However, if and how daily psychological processes influence child outcomes in the context of post-operative pain and recovery and how these processes may change throughout the post-operative process remains to be examined further.
Network analysis can be used to explore the partial correlations between multiple variables while indicating which of these variables that may be most influential for changes occurring in the remaining variables.25 In the context of post-operative pain, network analysis can explore the processes at different stages during recovery and potentially point out whether some processes are more prominent than others.
In sum, previous research has shown that psychological processes constitute risk and/or resilience factors for post-surgical recovery in children and adolescents undergoing major surgery and that parents influence their child’s recovery. If and how these positive and/or negative post-surgical recovery variables change throughout the recovery process for children undergoing surgery is unclear. The aim of the present study was to investigate the associations of risk and resilience factors in everyday life, in both adolescents and parents, and daily post-operative recovery variables in adolescents undergoing spinal fusion surgery, throughout the 1-year post-operative recovery process, in an explorative network analysis.
Materials and Methods
This study is part of a larger research project (“Post-operative recovery after spinal fusion (PR-SF) – A prospective study in adolescents with idiopathic scoliosis and their parents”). Research protocol can be found at: http://biblio.ugent.be/publication/8578153. The project has followed the Helsinki Declaration and the guidelines for Good Clinical Practice (ICH/GCP). The study was approved by the Medical Ethical Committee of Ghent University [BC16-1353], with an extended approval from all local ethical committees as for data collection at their respective unit. Data can be accessed from the corresponding author upon reasonable request.
Design
The study applied a longitudinal observational design with participants completing digital diaries during five time-points (or phases), for seven consecutive days during each phase, once daily. There was a pre-determined phase length with no randomization of baseline.
Participants
Participants were recruited to the orthopedic units at the university hospitals in Ghent, Antwerp, and Leuven and at Saint-Jan hospital in Bruges, Belgium, between 2016 and 2018, where patients with Adolescent Idiopathic Scoliosis (AIS), aged 12–18 years, scheduled for spinal fusion surgery, and one of their parents, were offered participation in the study. Exclusion criteria were insufficient language skills (in Dutch), prior spinal fusion surgery, and severe comorbidity. Informed consent was collected from both adolescents and parents. In exchange for participation, participants were offered two movie tickets. Adolescents and parents were recruited in dyads, and only participants with dyadic data were included in the present analyses. One hundred and forty-four adolescents were eligible for study participation, of whom five could not be reached and 139 were invited. Of these, 33 declined and 106 accepted. Six of these dropped out before the study started. Thus, 100 dyads of adolescents-parents were enrolled in the study.
Procedure
Patients (ie adolescents) received standard surgical care at their respective hospital. Participants, including both adolescents and parents, were asked to complete daily assessments over a period of seven days at five time-points: two weeks prior to surgery (T0), at three (T1) and six weeks (T2), and six (T3) and 12 (T4) months post-surgery. Hence, 35 daily assessments were expected from each participant. Data were collected via an online survey platform, Limesurvey 2.0. A week prior to each diary period, participants were contacted via telephone and instructed to complete the daily assessment in the evening for seven consecutive days. For each daily assessment, instructions included prompts to complete all items at once. Participants were reminded daily to fill in the diary, via automatic text messages. When there was a non-response, participants were reminded by a research team member the following day and prompted to fill in the diary assessment before 10 am the next day. Demographical data were collected through self-report questionnaires at T0. Biomedical data were retrieved via medical records.
Measures
Two diaries were developed to measure adolescent and parent variables, respectively, and were validated with regard to reliability, validity and variability, showing good psychometric properties.26 For both diaries, all items were rated on a 7-point numerical rating scale, ranging from “0” to “6” (from “not at all true” to “totally true”, if not otherwise specified). The adolescent diary assessed pain intensity, fatigue, physical complaints, pain-related fear, pain catastrophizing, psychological flexibility, activity engagement, activity avoidance, positive and negative affect/mood, general functioning, and pain interference. The parent diary measured: positive and negative affect/mood (parental), pain catastrophizing (about child pain), pain-related fear (regarding child pain), parent instructions towards their child to avoid or engage in activities, and parent protective behaviour. The diaries were developed based upon validated questionnaires measuring constructs related to pediatric pain and function. The Discriminant Content Validity (DCV) procedure was applied.27 Variables, number of items, items, response scales, and sources for development are presented in Table 1 for the adolescent diary and Table 2 for the parent diary.28–39
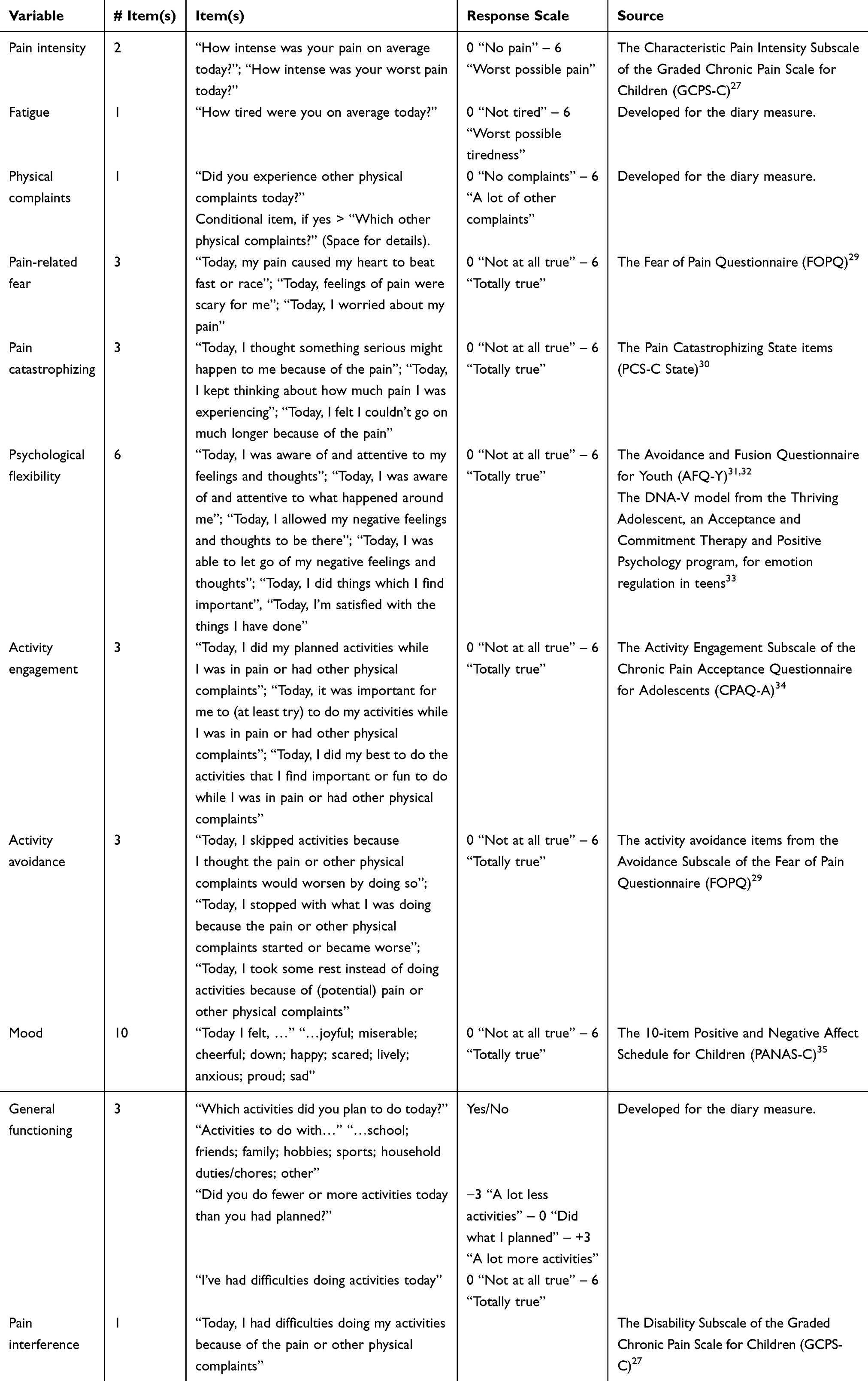 |
Table 1 Variables, Number of Items, Items, Response Scales and Sources for the Adolescent Diary |
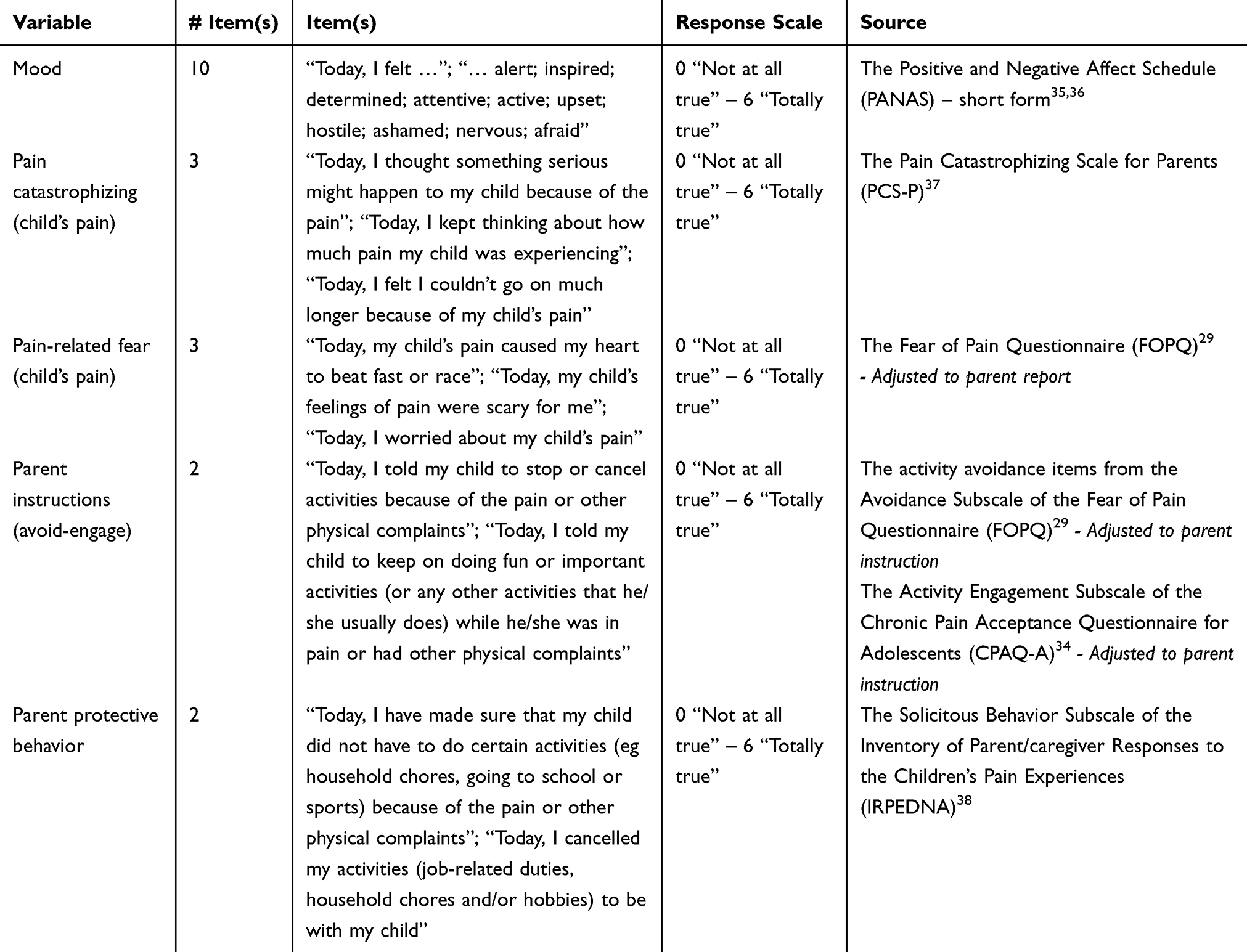 |
Table 2 Variables, Number of Items, Items, Response Scales, and Sources for the Parent Diary |
Data Preparation and Management
In line with the guidelines on management of missing diary data, the cut-off of 33% was applied.40 Consequently, participants with less than 12 data entries were excluded from analyses, which concerned five participants. Diary entries were coded according to time-point (T0-T4) and day (1–7). A diary entry that was completed before 10 am the next day was coded as the previous day (according to the instructions to participants). Missing diary entries were coded as missing data and not imputed. Some participants completed double assessments the same day, in which case the duplicate was removed. When participants filled in diaries for more than the instructed seven days, the seven consecutive days with most data were kept, and the surplus data entries (exceeding seven days) were excluded. For data to correspond best to its current time-point, the seven consecutive days closest to the starting point were prioritized. Only complete dyad data, from both adolescent and parent, were analyzed.
Statistical Analyses
Network analysis was used to explore partial correlations between all variables in the study. Moreover, network analysis provides information about node centrality, reflecting which nodes appear to be the most associated with the other nodes in the network.41 While strength centrality looks at the sum of all edge weights connected to a particular node, closeness centrality examines the indirect connections between a node and other nodes, and betweenness looks at how often a particular node lies between other nodes and connecting them to each other.41 An often customary so-called regularization in network analysis was employed, forcing correlations close to zero to actually become zero, in order to provide a network structure less prone to displaying potentially false connections.42
Cross-sectional, contemporaneous, network analyses for each phase were performed based on the mean value of the seven daily diary entries within each phase. The mean of the seven days – or the mean of the number of days with responses in the case of missing data – was used to capture a representative value for a particular participant in a specific phase. Due to multivariate non-normality in Mardia’s test,43 non-paranormal transformations were performed before conducting the five networks, one for each phase (T0-T4).44,45 The networks were configured using graphical least absolute shrinkage and selection operator regularization with extended Bayesian information criterion model selection (EBICglasso) and plotted in graphs for visualizations.46 Sample size recommendations for network analysis begin at around 100 participants, where larger sample sizes are needed for more complex networks with more nodes.47 For high sensitivity, 250 participants are considered to be optimal. Due to the relatively small sample size in the present study, precautions were taken to assess each generated network for accuracy. As network results can be sensitive to sample size, testing for accuracy involves utilizing bootstrapping to examine how results would differ if the sample was different.42 First, non-parametric bootstrapped confidence intervals (CIs) were estimated around edge-weights, where large CIs around the mean of edge weights in the bootstrapped samples would indicate that edge-weights might change in other samples, and vice versa that the edge-weights would not differ much in another sample if the CIs were smaller. Second, centrality stability was estimated, examining how the centrality indices results would differ if a certain number of cases were dropped from the sample. A so-called Correlation-Stability (CS) Coefficient can be calculated, indicating that the mean percentage can be dropped from the sample while leaving the mean correlation between the sample index value and bootstrapped index values at a particular correlation value, here set to the default value of 0.7. A high CS-coefficient means that sample size can be largely reduced without centrality being much changed, indicating that a sample is not greatly affected by certain sample characteristics. The CS-coefficient should be at least 0.25.42
Network Comparison Test
Networks from each phase were compared to each other using the network comparison test (NCT),48 to test network invariance in terms of differences between edge weights in the networks, and global strength invariance, meaning differences in the absolute sum of edge weights in the different networks. Permutations of 1000 were used, and the permutation seed value was set to “123”.
Software
Descriptive statistical analyses were computed using the IBM SPSS Statistics version 28.49 Network analyses were performed using R version 4.4.0,50 employing the packages “dplyr”,51 “readxl”,52 bootnet,53 “mvnormalTest”,54 “qgraph”,46 “NetworkComparisonTest”,48 and “huge”.55
Results
Sample Characteristics
The sample comprised N=190 participants, n=95 adolescents and n=95 parents. Sample characteristics are presented in Table 3, also reported in Thorsell Cederberg et al (2024).26
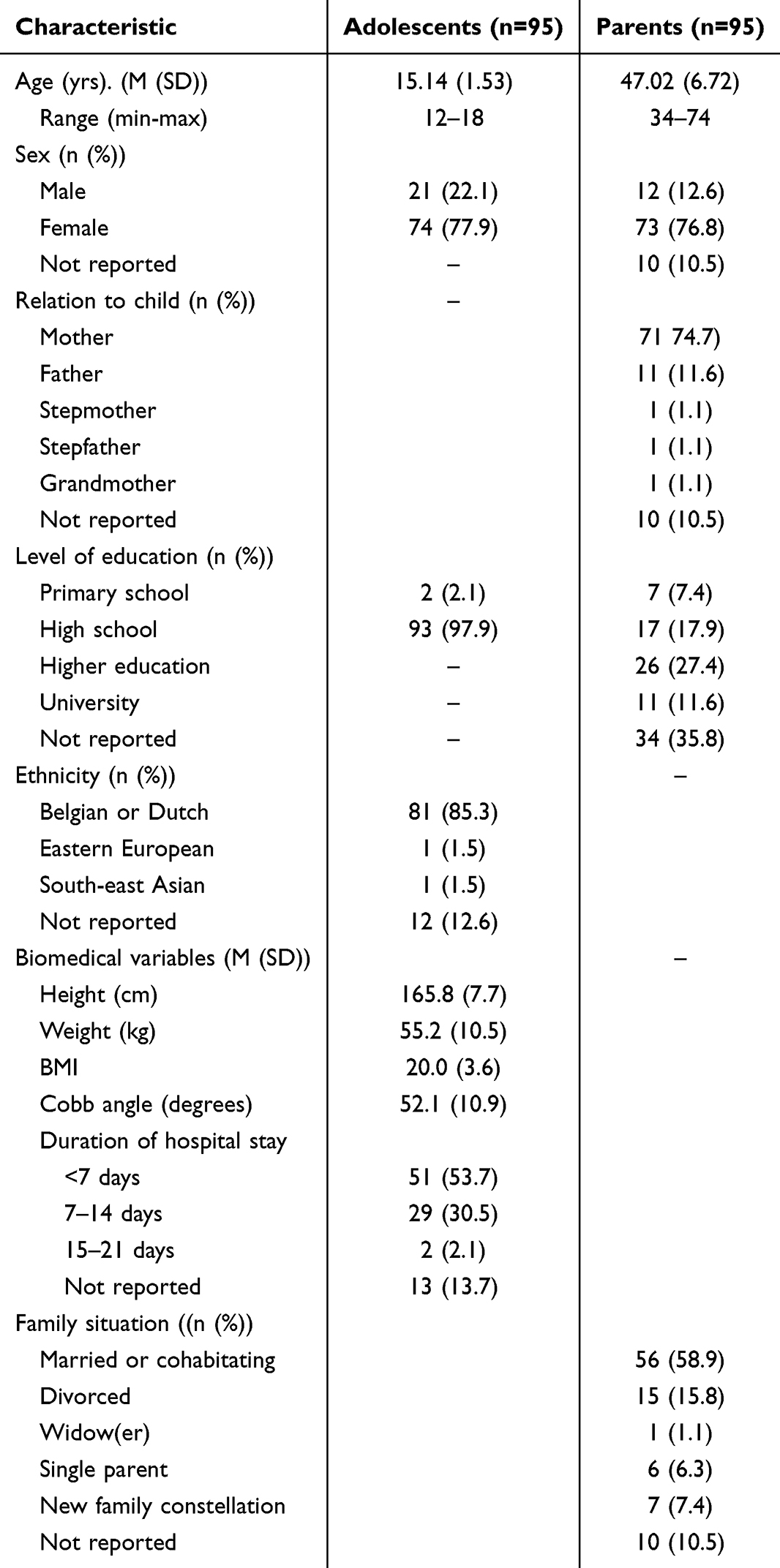 |
Table 3 Sample Characteristics, N=190 |
Network Analyses
Descriptive characteristics of the network analysis are presented in Table 4. Network plots are presented in Figures 1–5. Looking at the strongest edges within the networks for the five phases, some edges appeared consistently strong. For instance, the edge between parental catastrophizing in response to their child’s pain and parental fear of child’s pain was one of the strongest edges in all phases. Some of the edges appeared to be among the strongest in some or most of the phases, but not in all of them. Specifically, adolescent-reported psychological flexibility and positive mood, adolescent-reported pain interference and activity engagement, adolescent-reported pain catastrophizing and pain-related fear, and parental instructions to avoid and displaying protective parent behavior, were among the stronger edges in many of the phases. Details of the strongest edges in each phase are presented in Table 5. Additionally, for adolescents, psychological flexibility and activity engagement, and pain intensity and pain catastrophizing were correlated in Phase 0 and 1. In Phase 1, 2, and 3, pain intensity was correlated with both pain catastrophizing and activity avoidance. In Phase 4, pain intensity was correlated with pain catastrophizing and pain-related fear to activity avoidance. Also, additionally, for parents, parent-reported pain-related fear (regarding child’s pain) was correlated with parental instructions to avoid activities in phase 0. In phase 1 and 2, parental pain-related fear and parental pain catastrophizing (also in phase 4) were correlated with parental instructions to avoid activities. Parental positive mood and parental instructions to engage in activities were correlated in phase 1. Generally, the bootstrapped CIs showed somewhat accurate results for the very strongest edges in the sense that the strongest edges while overlapping with each other, did not overlap, or only overlapped slightly, with weaker edges in the network. Bootstrapped results for each network phase are presented in Figures S1–S5. Thus, it was shown to be likely that these strongest edges would reoccur as strong edges in other samples.
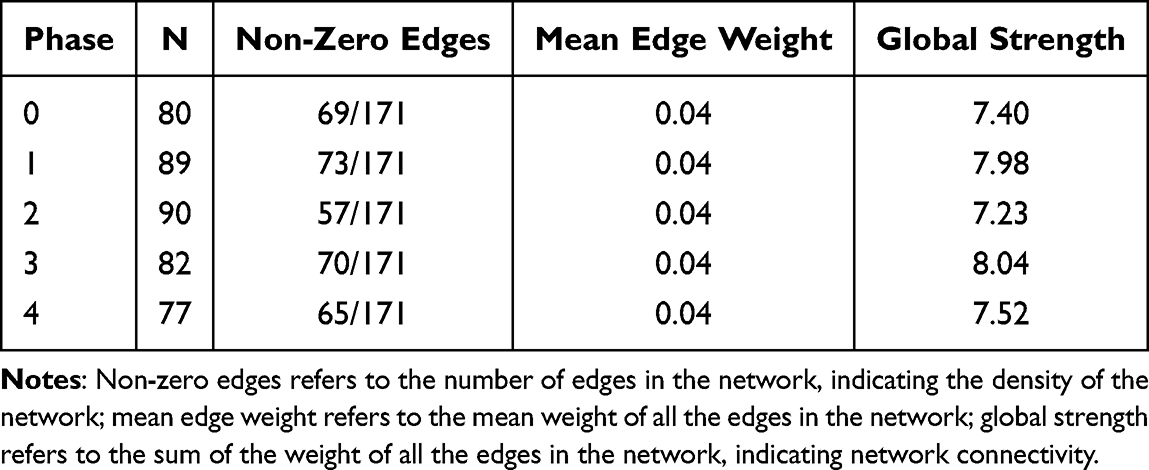 |
Table 4 Descriptive Statistics of the Network for Each Phase |
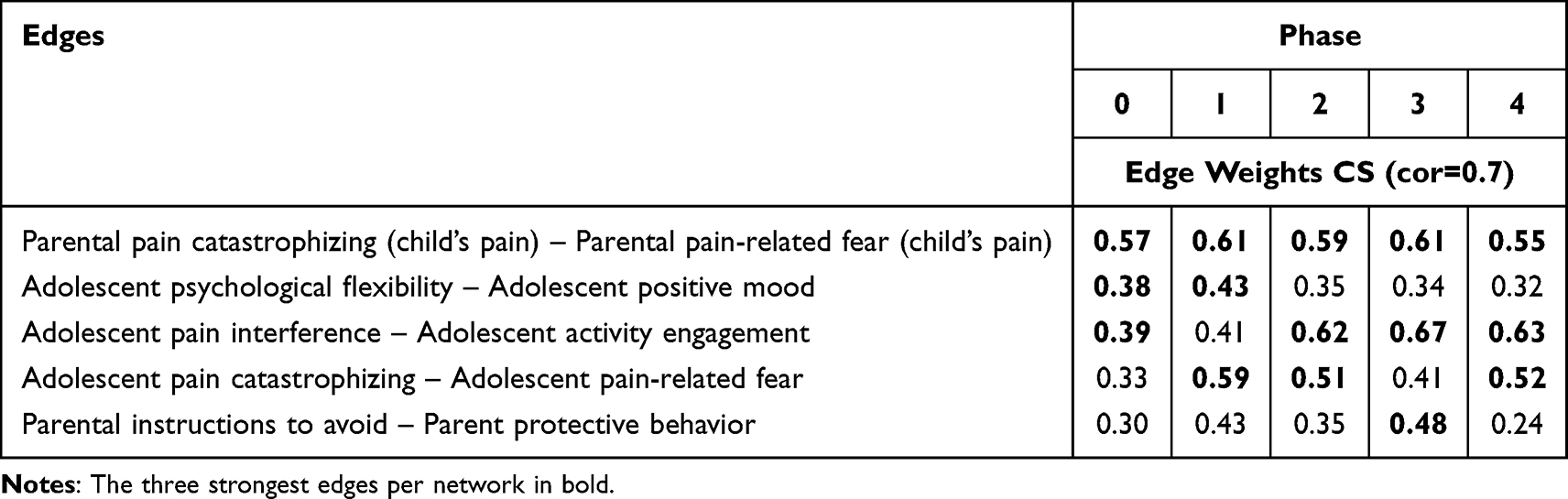 |
Table 5 The Three Strongest Edges for the Network in Each Phase, and Corresponding Edge Weights in the Other Networks |
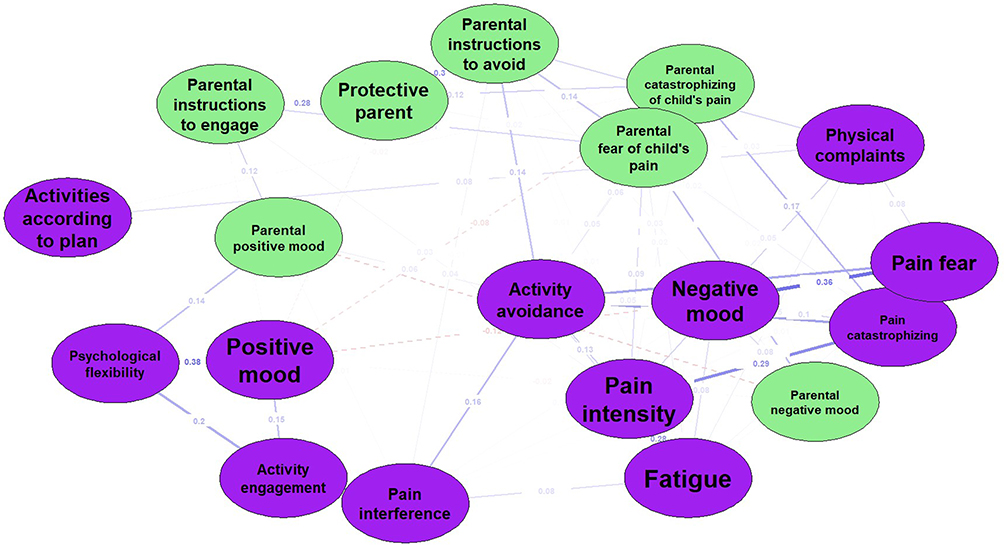 |
Figure 1 Network plot phase 0. Notes: Nodes are presented within circles. Purple nodes are adoloescent rated variables, while reen nodes are parent rated variables. The lines between the circles are the network edges, displaying the edge weights, or correlations, between nodes. A thicker edge indicates a stronger correlation. Red, dashed, lines indicate negative correlations, while blue lines indicate positive correlations. |
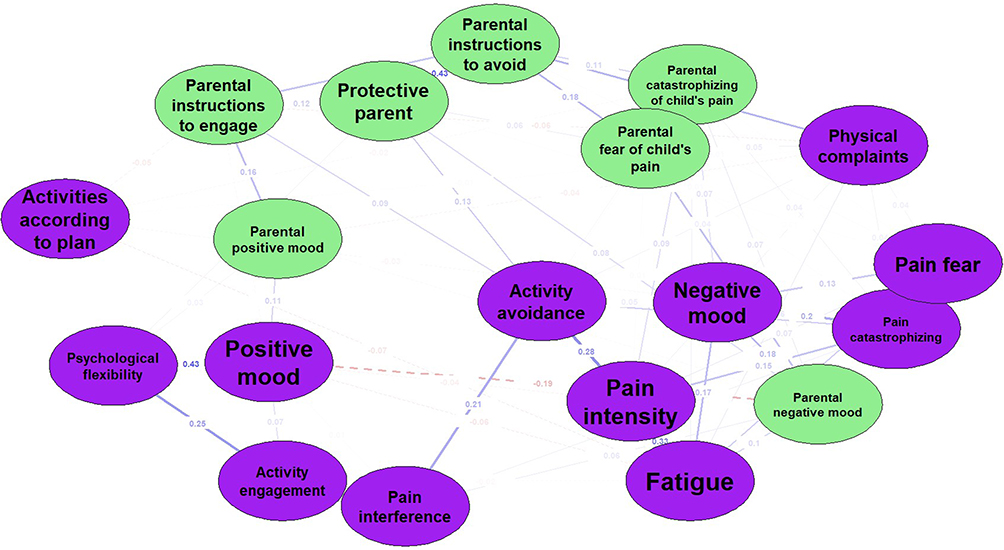 |
Figure 2 Network plot phase 1. Notes: Nodes are presented within circles. Purple nodes are adoloescent rated variables, while reen nodes are parent rated variables. The lines between the circles are the network edges, displaying the edge weights, or correlations, between nodes. A thicker edge indicates a stronger correlation. Red, dashed, lines indicate negative correlations, while blue lines indicate positive correlations. |
 |
Figure 3 Network plot phase 2. Notes: Nodes are presented within circles. Purple nodes are adoloescent rated variables, while reen nodes are parent rated variables. The lines between the circles are the network edges, displaying the edge weights, or correlations, between nodes. A thicker edge indicates a stronger correlation. Red, dashed, lines indicate negative correlations, while blue lines indicate positive correlations. |
 |
Figure 4 Network plot phase 3. Notes: Nodes are presented within circles. Purple nodes are adoloescent rated variables, while reen nodes are parent rated variables. The lines between the circles are the network edges, displaying the edge weights, or correlations, between nodes. A thicker edge indicates a stronger correlation. Red, dashed, lines indicate negative correlations, while blue lines indicate positive correlations. |
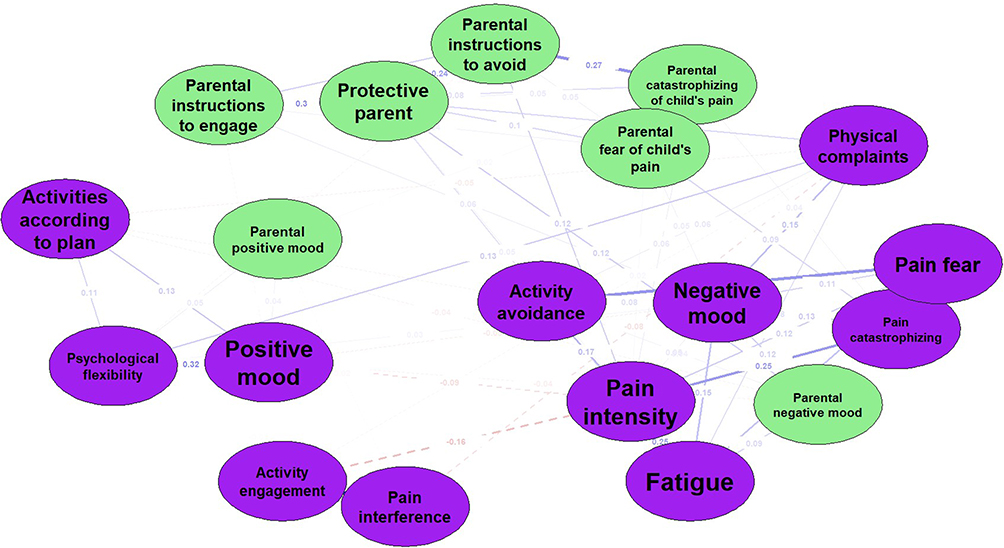 |
Figure 5 Network plot phase 4. Notes: Nodes are presented within circles. Purple nodes are adoloescent rated variables, while reen nodes are parent rated variables. The lines between the circles are the network edges, displaying the edge weights, or correlations, between nodes. A thicker edge indicates a stronger correlation. Red, dashed, lines indicate negative correlations, while blue lines indicate positive correlations. |
Generally, correlations based on the within individual parental and within individual adolescent variables, respectively, were stronger than those based on variance between the parental and adolescent variables. Examining the edges between parental variables and adolescent variables, the correlations appear generally low.
A few edges were somewhat stronger than others: in phase 0, the two strongest edges were between parental instructions to avoid activities and adolescent-reported activity avoidance and between parental pain catastrophizing of child pain and adolescent-reported pain catastrophizing. In phase 1, the strongest edges were between parental instructions to avoid activities and adolescent-reported physical complaints and a negative correlation between parent-reported negative mood and adolescent-reported positive mood. In Phase 2, the strongest edges were between parental instructions to avoid activities and adolescent-reported physical complaints and between parent-reported and adolescent-reported negative mood. In Phase 3, the strongest edges were between parent-reported pain catastrophizing (child’s pain) and adolescent-reported pain-related fear and between parent-reported negative mood and adolescent-reported fatigue. Additionally, parent instructions to engage in activities were negatively associated with adolescent activity avoidance in phase 3. Lastly, in phase 4, the strongest edges were between parent-reported and adolescent reported negative mood, and between parent-reported protective behavior and adolescent-reported physical complaints. Details of the strongest edges between adolescent and parental variables are presented in Table 6.
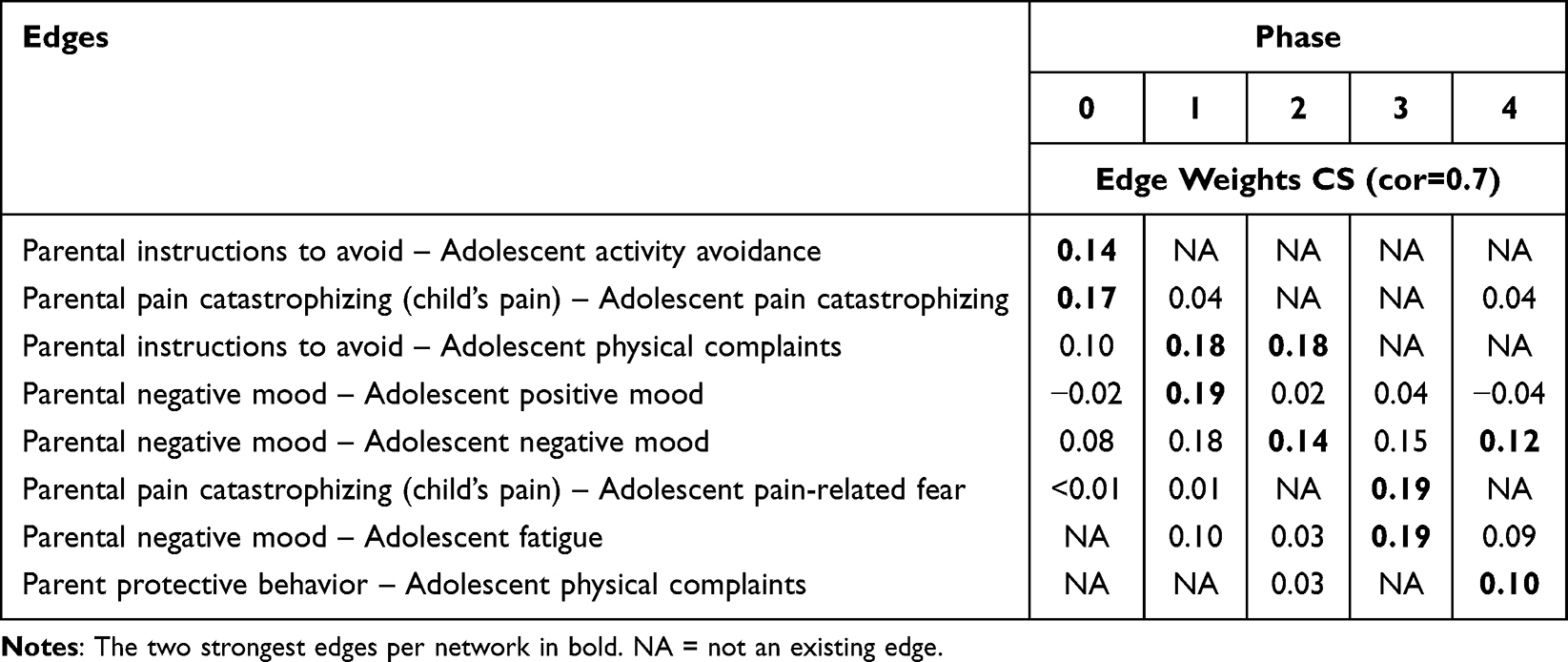 |
Table 6 The Two Strongest Edges Between Parental and Adolescent Variables for the Network in Each Phase, and Corresponding Edge Weights in the Other Networks |
Centrality Indices
In phase 0, parental pain-related fear (of child’s pain) was the most central variable, followed by adolescent-reported pain catastrophizing. In phase 1, adolescent-reported pain catastrophizing was the most central, followed by parental pain-related fear (of child’s pain). In phases 2 and 4, adolescent-reported pain intensity was the most central variable, followed by parental pain-related fear of child’s pain. In phase 3, adolescent-reported pain intensity was again the most central variable, this time followed by adolescent-reported pain catastrophizing. Inspecting centrality accuracy, it should be mentioned that the CS-coefficients were overall low, meaning that these centrality results may not be replicated in other samples. However, CS-coefficients for strength centrality were the highest ones compared to betweenness and closeness centrality, which is why strength centrality index is the one being presented here. The CS-coefficients (cor = 0.7) were 0.2 in phase 0 and 1, 0.37 in phase 2, 0.21 in phase 3, and 0.13 in phase 4. Thus, strength centrality seemed accurate in phase 2 with the CS-coefficient being above the recommended cut-off of 0.25, and approaching accuracy in phases 1 and 2. However, the strength centrality was deemed inaccurate for phase 4. Output on centrality is presented in Figure S6.
Network Comparison Test (NCT)
Using NCT to check for network differences statistically, the networks between phase 0 and phase 3 differed significantly from each other in terms of differences between edge weights, although this difference was not found in post hoc analyses using Bonferroni-Holm correction. Overall, NCT analyses showed that the networks generally did not seem to differ between phases, neither on particular edge weights nor global strength. This means that correlations between the variables seemed to be similar across different stages in relation to surgery, although there may be a potential difference between phase 0 and phase 3. The results from the NCT are presented in Table 7.
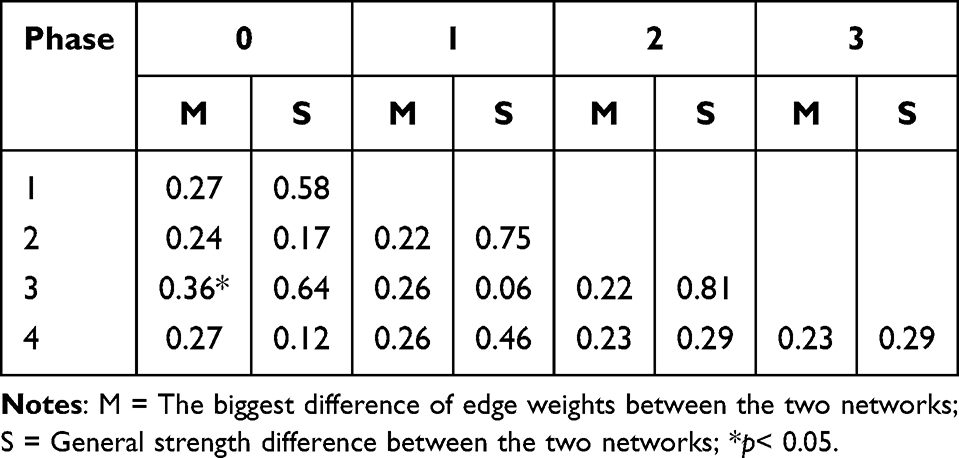 |
Table 7 Comparisons of Edge Differences and Strength Differences Between the Phases |
Discussion
The aim of this study was to investigate the associations of risk and resilience factors in everyday life, in both adolescents and parents, and daily post-operative recovery variables in adolescents undergoing spinal fusion surgery, throughout the post-operative recovery process, in an explorative network analysis. As expected, the results showed that the network edges within adolescent and parent variables, respectively, were stronger than the edges between adolescent and parent variables.
Networks Within Adolescent Variables
Within the adolescents, the strongest edges were found between psychological flexibility and positive mood in phases 0 and 1, ie before surgery and three weeks after surgery, pain interference and activity engagement in phases 0, 2, 3, and 4, ie before surgery, and at six weeks, and six and 12-month post-surgery, and pain catastrophizing and pain-related fear in phase 1, 2 and 4. The association between psychological flexibility and positive mood is worth noting and supported in research beyond the post-operative pain context.33 Psychological flexibility, conceptualized as a process, predictor, or mediating variable, was also related to activity engagement, generally conceptualized as an outcome or recovery variable, in phase 0 (pre-surgery) and 1 (3-week post-surgery), which is in line with previous research showing that psychological flexibility before surgery and the theoretically connected variable pain acceptance after surgery were associated with better recovery at follow-up.13,56 As for the positive association between pain interference and activity engagement found in this study, this may seem surprising. However, pain interference measures whether the respondent perceives difficulties in doing activities due to pain (or other physical complaints), whereas the activity engagement items measure whether the respondent actually pursued, or did their best to pursue, activities in the presence of pain, during the day. The strong edges throughout the post-operative phases between these two variables indicate that the adolescents experienced some struggle in carrying out activities while in pain. At the same time, pain interference was also positively associated with activity avoidance in phase 0 and 1, ie before surgery and 3-week post-surgery, which illustrates that this struggling due to pain while doing activities, may also, in another scenario or for other persons, results in avoidance of activities, or vice versa (that avoidance precedes interference). Determining causality, however, was not part of these exploratory analyses and requires further investigation. The results reflecting strong edges between pain catastrophizing and pain-related fear are not surprising given the conceptual overlap of these two concepts. Also, pain intensity was associated with both pain catastrophizing in the short term (ie, 3- and 6-week), as well as long term (ie, 6- and 12-month post-surgery) and activity avoidance short and intermediate term (ie, from 3-week up to 6-month post-surgery). Activity avoidance is generally conceptualized as an outcome variable, and the results are therefore in line with previous research indicating pain intensity as a predictor of pediatric post-operative recovery.7 This highlights, as in the previous research,16 the importance of proper pain management, and the need to support adolescents struggling with pain to mobilize and engage in daily life activities. In phase 4, at 12-month post-surgery, pain-related fear was also associated with activity avoidance, which is in line with previous research of pain-related fear and pain catastrophizing as predictors of recovery,13 further emphasizing the need to address these psychological variables in adolescents undergoing major surgery, to prevent long-term negative health-related consequences.
Networks Within Parent Variables
Within parents, the strongest edges were observed between parental pain catastrophizing and parental pain-related fear (of child’s pain) and parental instructions to avoid activities and parent-reported protective behavior, which is unsurprising given their conceptual correspondence. However, the relationships of parental pain-related fear and parental pain catastrophizing, respectively, with parent-to-child instructions to avoid activities are of particular interest. Pain-related fear and pain catastrophizing in parents are known predictors of adolescent post-operative recovery,7,13 and parental responses and instructions to avoid or engage in daily life activities have been associated with levels of avoidance in adolescents with chronic pain.23 The results of the present study add to the knowledge of parental processes in the context of pediatric post-operative pain, showing an association between parental pain-related fear and pain catastrophizing, and parental instructions towards their child in pain, which, in turn, have been shown to be associated with child recovery in pediatric chronic pain.23 Furthermore, the result showing an association between parental positive mood and parental instructions to engage in activities shortly after surgery (in phase 1, ie 3-week post-surgery) is also of particular interest in the light of previous research in pediatric chronic pain showing that both parental emotional responses and behavior predict child recovery. These processes, therefore, warrant future investigation in the context of CPSP, eventually, to develop timely interventions.
Networks Between Adolescent-Parent Variables
Regarding the network edges based on variance between adolescent and parent variables, the results showed that parent instructions to avoid activities were associated with adolescent activity avoidance, while parental pain catastrophizing was associated with adolescent pain catastrophizing, before surgery, and with adolescent pain-related fear at 6-month after surgery. These results highlight the need to support parents before and after their child’s surgery to promote recovery in adolescents. Furthermore, the results showed that parental and adolescent mood were associated in phases 1, 2, and 4, ie 3- and 6-week as well as 12-month post-surgery, and that parental mood and adolescent-reported fatigue were associated in phase 3, ie at 6-month post-surgery, which may be unsurprising but still adds to the research that parents’ emotional states may affect child outcomes across the recovery journey.17 Also, among the strongest edges were adolescent-reported physical complaints and parent-reported instructions to avoid activities, at 3- and 6-week post-surgery, and protective behavior, at 12-month post-surgery. It seems logical that a parent would display protective behavior towards their child and encourage avoidance of activities if the child seemed affected by and complained about physical symptoms. However, this may be more functional at an early acute post-operative phase, rather than at a later phase, such as months post-surgery. There is also a possibility that parent protective behavior affects the adolescents to focus more on physical symptoms, increasing the risk of hypervigilance, a process known to be associated with poor pain outcomes.57,58 The results further illustrate the need to support parents to promote resilience for their children after surgery. Additionally, parent instructions to engage were associated with adolescent activity avoidance in phase 3, at 6-month post-surgery, which may seem counter-intuitive at first but may be logical during inter-mediate recovery, where parents may be particularly prone to attempt to encourage their child to activities if the adolescent is still avoiding daily life activities after surgery. Overall, the results are in line with previous research in the context of pediatric post-operative pain, the influence of parental processes,13 and on the impact of parental behavior on adolescent daily pain-related behavior in the context of pediatric chronic pain.17 Yet, the results of the present study extend the knowledge by combining the research from different pediatric pain contexts to include parental factors in everyday life, and their association with adolescent recovery variables, throughout the pediatric post-operative recovery process.
Methodological Considerations and Limitations
A considerable limitation of the study was a small sample in relation to the number of data entries. It would have been preferable considering the design of study, with one daily assessment during seven consecutive days, to have a larger sample size. Alternatively, additional assessments, possibly twice or even more often daily, and/or for a longer time period, would have yielded more data entries for the analyses. This reflection is an important note for future research, and a priori sample size calculations might be useful. In the present study, most data entries were gathered in phase 2, at 6-week post-surgery, which generated most robust results based on strength centrality accuracy. Due to restrictions of power, the data did not permit to examine temporal networks (which would allow exploration of correlations of all variables also between phases, and not only across phases). Hence, the networks of the study are contemporaneous and should be interpreted as such. Even so, the relatively small sample size in the study means that there may be associations missed in the networks due to insufficient sensitivity to all potential associations. While network accuracy was tested thoroughly in order not to over-interpret unstable results, it is possible that a larger sample would have provided a clearer result and revealed stronger associations (provided they existed in the population). A small sample may also be skewed and indicate sample-specific associations not present in a larger sample. Still, the present results constitute the first evidence of day-to-day recovery processes in pediatric post-operative pain and may be seen as preliminary evidence calling for further exploration of larger samples to ensure generalizability. Future studies wishing to examine contemporaneous networks should, thus, include more participants. Future studies may also wish to include more repeated measures for generating temporal networks and, thereby, exploring moment-to-moment changes between variables. However, respondent burden should be carefully considered to avoid attrition. Although this was addressed in the present study, the risk of response fatigue cannot be excluded.
Moreover, adolescent general functioning (ie the extent to which adolescents had difficulties to do activities or did fewer or more activities than planned) did not correlate with the other variables, with no edge 6-weeks post-surgery and only weak edges in all other networks. It seems implausible that the level of function would not be associated with the rest of the variables in the study, both with regard to the associations between activity engagement and activity avoidance (as outcomes) and the other variables in the present study and also based on previous research identifying functioning as a target variable in pediatric pain.17,59 It seems more plausible that the diary items of the study simply did not capture the level of general functioning, as planned. Another result of the study was that the edges were generally lower in phase 4, indicating that the variables did not affect each other as much at one year after surgery.
Regarding the finding of stronger edge weights in some phases than in others, it is possible that both within adolescent and parent variables, respectively, and between adolescent-parent variables have different weights of impact during different phases of the post-operative recovery process. This would mean that certain interventions to support adolescents and parents to promote resilience would be more effective at different post-operative phases. However, the NCT test did not support significant differences between phases, apart from possibly between phase 0, ie before surgery, and 3, ie 6-month post-surgery. Alternatively, restrictions in power may have reduced the study’s capacity to detect certain associations between variables in some of the phases. In fact, some edges display weaker correlations, and should be interpreted with caution due to large bootstrapped confidence intervals around many of the weaker edges. Consequently, the order of strength of these weaker correlations might not be replicated in other samples, with edges close to zero in some phases. Nonetheless, it might be noteworthy that some edges appear to show meaningful connections between variables in some phases and may very well reoccur as strong edges in other samples. Altogether, this is indeed an empirical question to be investigated further.
Conclusion
The present results provide insights into adolescent and parental psychological risk and resilience factors in everyday life throughout the pediatric post-operative recovery process. Findings warrant further investigation and indicate important targets for post-operative pain treatments. Pain catastrophizing and pain-related fear, in both adolescents and parents, parent protective behavior and parent instructions towards their child to engage or avoid in daily life activities as well as adolescent psychological flexibility, and activity engagement and avoidance seem to be particularly important targets. The results are also essential in the light of the current under-treatment of pediatric post-operative pain. Finally, interventions may be needed to target different mechanisms at different moments during the recovery process as dynamics within and between adolescents and parents appear to vary over time.
Acknowledgment
We would like to thank all adolescents and parents participating in the study as well as the staff involved in the recruitment. In particular, we would like to thank the orthopaedic surgeons at each hospital, ie, prof. Dr. Plasschaert, prof. Dr. Michielsen, Dr. Moens and Dr. Schelfaut.
Funding
The study was supported by a postdoctoral placement grant [TJ2018-0101] and a project grant [PR2018-0103] by the Swedish Childhood Cancer Fund to Jenny Thorsell Cederberg and a grant by the Special Research Fund of Ghent University to Liesbet Goubert (BOF15/24j/017).
Disclosure
We declare no conflicts of interest.
References
1. Mullapudi B, Grabski D, Ameh E, et al. Estimates of number of children and adolescents without access to surgical care. B World Health Organ. 2019;97(4):254. doi:10.2471/BLT.18.216028
2. Meara J, Greenberg S. The lancet commission on global surgery global surgery 2030: evidence and solutions for achieving health, welfare and economic development. Surgery. 2015;157(5):834–835. doi:10.1016/j.surg.2015.02.009
3. Botman M, Meester RJ, Voorhoeve R, et al. The Amsterdam declaration on essential surgical care. World J Surg. 2015;39(6):1335–1340. doi:10.1007/s00268-015-3057-x
4. Landrum K, Cotache-Condor CF, Liu Y, et al. Global and regional overview of the inclusion of paediatric surgery in the national health plans of 124 countries: an ecological study. BMJ Open. 2021;11(6):e045981. doi:10.1136/bmjopen-2020-045981
5. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–540. doi:10.1213/01.ANE.0000068822.10113.9E
6. Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014;30(1):149–160. doi:10.1185/03007995.2013.860019
7. Rabbitts JA, Fisher E, Rosenbloom BN, Palermo TM. Prevalence and predictors of chronic postsurgical pain in children: a systematic review and meta-analysis. J Pain. 2017;18(6):605–614. doi:10.1016/j.jpain.2017.03.007
8. Dugan MQ, Delgado JR, De Souza E, Anderson TA. Pediatric chronic post-surgical pain prevalence, pain scores, and quality-of-life: results of an exploratory patient survey at a single-center tertiary care children’s hospital. J Anesth. 2022;36(5):606–611. doi:10.1007/s00540-022-03089-w
9. Connelly DM, Fulmer ER, Prohaska EJ, et al. Predictors of Postoperative Pain Trajectories in Adolescent Idiopathic Scoliosis. Spine. 2014;39(3):E174–E181. doi:10.1097/BRS.0000000000000099
10. Landman Z, Oswald T, Sanders J, Diab M. Prevalence and predictors of pain in surgical treatment of adolescent idiopathic scoliosis. Spine. 2011;36(10):825–829. doi:10.1097/BRS.0b013e3181de8c2b
11. Wong GTC, Yuen VMY, Chow BFM, Irwin MG. Persistent pain in patients following scoliosis surgery. Eur Spine J. 2007;16(10):1551–1556. doi:10.1007/s00586-007-0361-7
12. Chieng YJS, Chan WCS, Klainin‐Yobas P, He HG. Perioperative anxiety and postoperative pain in children and adolescents undergoing elective surgical procedures: a quantitative systematic review. J Adv Nurs. 2014;70(2):243–255. doi:10.1111/jan.12205
13. Thorsell Cederberg J, Bartels SL, Thulin M, Beeckman M, Wicksell RK, Goubert L. Child and parent risk and resilience factors as predictors of long-term recovery in youths undergoing spinal fusion surgery. Clin J Pain. 2024;40(5):278–287. doi:10.1097/AJP.0000000000001200
14. Sturgeon JA, Zautra AJ. Resilience: a new paradigm for adaptation to chronic pain. Curr Pain Headache R. 2010;14(2):105–112. doi:10.1007/s11916-010-0095-9
15. Goubert L, Trompetter HR. Towards a science and practice of resilience in the face of pain. Eur J Pain. 2017;21(8):1301–1315. doi:10.1002/ejp.1062
16. Rabbitts JA, Palermo TM, Lang EA. A conceptual model of biopsychosocial mechanisms of transition from acute to chronic postsurgical pain in children and adolescents. J Pain Res. 2020;13:3071–3080. doi:10.2147/JPR.S239320
17. Donnelly TJ, Palermo TM, Newton-John TRO. Parent cognitive, behavioural, and affective factors and their relation to child pain and functioning in pediatric chronic pain: a systematic review and meta-analysis. Pain. 2020;161(7):1401–1419. doi:10.1097/j.pain.0000000000001833
18. Kerr J, Abraham E, Vandewint A, et al. Predicting health-related quality of life outcomes following major scoliosis surgery in adolescents: a latent class growth analysis. Global Spine J. 2024;14(3):902–913. doi:10.1177/21925682221126451
19. McCracken LM, Yu L, Vowles KE. New generation psychological treatments in chronic pain. BMJ. 2022;376:e057212. doi:10.1136/bmj-2021-057212
20. Hayes SC, Hofmann SG, Stanton CE, et al. The role of the individual in the coming era of process-based therapy. Behav Res Ther. 2019;117:40–53. doi:10.1016/j.brat.2018.10.005
21. Horstmann K. Experience sampling and daily diary studies: basic concepts, designs and challenges. In: Rauthmann JF, editor. The Handbook of Personality Dynamics and Processes. Academic Press; 2020.
22. Bolger N, Davis A, Rafaeli E. Diary methods: capturing life as it is lived. Annu Rev Psychol. 2003;54(1):579–616. doi:10.1146/annurev.psych.54.101601.145030
23. Beeckman M, Simons LE, Hughes S, Loeys T, Goubert L. Investigating how parental instructions and protective responses mediate the relationship between parental psychological flexibility and pain-related behavior in adolescents with chronic pain: a daily diary study. Front Psychol. 2019;10:2350. doi:10.3389/fpsyg.2019.02350
24. Giusti EM, Lacerenza M, Gabrielli S, et al. Psychological factors and trajectories of post-surgical pain: a longitudinal prospective study. Pain Pract. 2022;22(2):159–170. doi:10.1111/papr.13074
25. Robinaugh DJ, Hoekstra RHA, Toner ER, Borsboom D. The network approach to psychopathology: a review of the literature 2008-2018 and an agenda for future research. Psychol Med. 2020;50(3):353–366. doi:10.1017/S0033291719003404
26. Thorsell Cederberg J, Zetterqvist, V, Wicksell, R, Goubert, L, Bartels, SL. Preliminary validation of a diary approach to monitor daily adolescent and parental predictors of post-operative recovery: a longitudinal diary study in adolescents undergoing spinal fusion surgery. World Neurosurg. 2014. doi: 10.1016/j.wneu.2025.123744
27. Johnston M, Dixon D, Hart J, Glidewell L, Schröder C, Pollard B. Discriminant content validity: a quantitative methodology for assessing content of theory-based measures, with illustrative applications. Brit J Health Psychol. 2014;19(2):240–257. doi:10.1111/bjhp.12095
28. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133–149. doi:10.1016/0304-3959(92)90154-4
29. Vervoort T, Logan DE, Goubert L, De Clercq B, Hublet A. Severity of pediatric pain in relation to school-related functioning and teacher support: an epidemiological study among school-aged children and adolescents. Pain. 2014;155(6):1118–1127. doi:10.1016/j.pain.2014.02.021
30. Simons LE, Sieberg CB, Carpino E, Logan D, Berde C. The fear of pain questionnaire (FOPQ): assessment of pain-related fear among children and adolescents with chronic pain. J Pain. 2011;12(6):677–686. doi:10.1016/j.jpain.2010.12.008
31. Durand H, Birnie KA, Noel M, et al. State versus trait: validating state assessment of child and parental catastrophic thinking about children’s acute pain. J Pain. 2017;18(4):385–395. doi:10.1016/j.jpain.2016.11.012
32. Greco LA, Lambert W, Baer RA. Psychological inflexibility in childhood and adolescence: development and evaluation of the avoidance and fusion questionnaire for youth. Psychol Assess. 2008;20(2):93–102. doi:10.1037/1040-3590.20.2.93
33. Livheim F, Tengström A, Bond FW, Andersson G, Dahl J, Rosendahl I. Psychometric properties of the avoidance and fusion questionnaire for youth: a psychological measure of psychological inflexibility in youth. J Contextual Behav Sci. 2016;5(2):103–110. doi:10.1016/j.jcbs.2016.04.001
34. Hayes LL, Ciarrochi J. The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Context Press; 2015.
35. McCracken LM, Gauntlett-Gilbert J, Eccleston C. Acceptance of pain in adolescents with chronic pain: validation of an adapted assessment instrument and preliminary correlation analyses. Eur J Pain. 2009;14(3):316–320. doi:10.1016/j.ejpain.2009.05.002
36. Ebesutani C, Regan J, Smith A, Reise S, Higa-McMillan C, Chorpita BF. The 10-item positive and negative affect schedule for children, child and parent shortened versions: application of item response theory for more efficient assessment. J Psychopathol Behav. 2012;34(2):191–203. doi:10.1007/s10862-011-9273-2
37. Thompson ER. Development and validation of an internationally reliable short-form of the positive and negative affect schedule (PANAS). J Cross Cult Psychol. 2007;38(2):227–242. doi:10.1177/0022022106297301
38. Goubert L, Eccleston C, Vervoort T, Jordan A, Crombez G. Parental catastrophizing about their child’s pain. The parent version of the pain catastrophizing scale (PCS-P): a preliminary validation. Pain. 2006;126(1–3):123. doi:10.1016/j.pain.2006.06.026
39. Huguet A, Miró J, Nieto R. The inventory of parent/caregiver responses to the children’s pain experience (IRPEDNA): development and preliminary validation. Pain. 2008;134(1):128–139. doi:10.1016/j.pain.2007.04.004
40. Delespaul P. Assessing Schizophrenia in Daily Life: The Experience Sampling Method. Maastricht: Maastricht University; 1995.
41. Robinaugh DJ, Millner AJ, McNally RJ. Identifying highly influential nodes in the complicated grief network. J Abnorm Psychol. 2016;125(6):747–757. doi:10.1037/abn0000181
42. Epskamp S. Network psychometrics. Psychology Research Institute: University of Amsterdam; 2017.
43. Mardia KV. Measures of multivariate skewness and kurtosis with applications. Biometrika. 1970;57(3):519–530. doi:10.1093/biomet/57.3.519
44. Liu H, Han F, Yuan M, Lafferty J, Wasserman L. High-dimensional semiparametric gaussian copula graphical models. Ann Stat. 2012;40(4):2293–2326. doi:10.1214/12-AOS1037
45. Zhao T, Liu H, Roeder K, Lafferty J, Wasserman L. The huge Package for High-dimensional undirected graph estimation in R. J Mach Learn Res. 2012;13:1059–1062.
46. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Software. 2012;48(4). doi:10.18637/jss.v048.i04
47. Constantin MA. Sample size recommendations for estimating cross-sectional network models. Available from: https://arno.uvt.nl/show.cgi?fid=149724.
48. Van Borkulo CD, van Bork R, Boschloo L, et al. Comparing network structures on three aspects: a permutation test. Psychol Methods. 2023;28(6):1273–1285. doi:10.1037/met0000476
49. IBM. SPSS Statistics. Version 28. Armonk: IBM Corporation; 2021.
50. R. A Language and Environment for Statistical Computing_.R Foundation for Statistical Computing. Vienna: R Core Team; 2024.
51. Wickham H, François R, Henry L, Müller K, Vaughan D. _dplyr: a grammar of data manipulation_. R package version 1.1.4. Available from: https://cran.r-project.org/web/packages/dplyr/index.html.
52. Wickham H, Bryan J, Kalincinski M, et al. _readxl: read excel files_. R package version 1.4.3. Available from: https://cran.r-project.org/web/packages/readxl/index.html.
53. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
54. Zhang Y, Zhou M, Shao Y. _mvnormalTest: powerful tests for multivariate normality_. R package version 1.0.0. Available from: https://cran.r-project.org/web/packages/mvnormalTest/index.html.
55. Jiang H, Fei X, Liu H, et al. _huge: high-dimensional undirected graph estimation_. R package version 1.3.5. Available from: https://cran.r-project.org/web/packages/huge/huge.pdf.
56. Beeckman M, Hughes S, Van der Kaap-Deeder J, et al. Risk and resilience predictors of recovery after spinal fusion surgery in adolescents. Clin J Pain. 2021;37(11):789–802. doi:10.1097/AJP.0000000000000971
57. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
58. Linton SJ. Do psychological factors increase the risk for back pain in the general population in both a cross-sectional and prospective analysis? Eur J Pain. 2005;9(4):355. doi:10.1016/j.ejpain.2004.08.002
59. Wicksell RK, Kanstrup M, Kemani MK, Holmström L. Pain interference mediates the relationship between pain and functioning in pediatric chronic pain. Front Psychol. 2016;7:1978. doi:10.3389/fpsyg.2016.01978
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Interrelations of Family Relationship, Illness Cognition of Helplessness and Perceived Barriers to Medication Adherence: A Study of Adolescent and Emerging Adult Kidney Recipients and Their Parents
Hamama-Raz Y, Frishberg Y, Ben-Ezra M, Levin Y
Adolescent Health, Medicine and Therapeutics 2023, 14:205-215
Published Date: 30 October 2023