")
Back to Journals » Infection and Drug Resistance » Volume 18
Deadly Diarrhea Caused by Co-Infection of Clostridium perfringens Type ST-865 and Clostridium difficile: A Case Report and Review of the Literature
Authors Hao Y, Li J , Xie S, Liu Y, Wen H
Received 20 March 2025
Accepted for publication 24 June 2025
Published 1 July 2025 Volume 2025:18 Pages 3231—3236
DOI https://doi.org/10.2147/IDR.S529341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yuyao Hao,1,* Jianhui Li,2,* Shoujun Xie,1 Yanchao Liu,1 Hainan Wen1,3
1Department of Clinical Laboratory, The Affiliated Hospital of Chengde Medical University, Chengde, Hebei, People’s Republic of China; 2Department of Preventive Medicine, Chengde Medical University, Chengde, Heibei, People’s Republic of China; 3Hebei Key Laboratory of Panvascular Diseases, The Affiliated Hospital of Chengde Medical University, Chengde, Heibei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hainan Wen, Email [email protected]
Purpose: There is a paucity of evidence regarding the occurrence of fatalities resulting from diarrhea due to co-infection with C. perfringens and C. difficile. Here, we report a rare case of severe diarrhea caused by a novel ST-865 type of C. perfringens in conjunction with C. difficile to draw the attention of clinicians and microbiology laboratory staff.
Case Descriptions: The patient is male, 69 years old and one month before admission, there was diarrhea without fever. The doctor administered anti-infective treatments such as levofloxacin, ceftriaxone, minocycline, gentamicin and tinidazole, and sent fecal samples for anaerobic culture. Two colonies, Clostridium perfringens and Clostridium difficile, were cultivated and identified by sequencing as type F-Clostridium perfringens of ST-865 and Clostridium difficile carrying toxins A and B.
Conclusion: The case we reported, which involved a severe case of diarrhea caused by a combined infection of ST-865 type F-type Clostridium perfringens and Clostridium difficile carrying both A and B toxins, and resulting in eventual death, is extremely rare. Such cases should draw the attention of clinicians and microbiology laboratory personnel.
Keywords: Clostridium perfringens, Clostridium difficile, diarrhea
Introduction
Clostridium perfringens and Clostridium difficile are anaerobic gram-positive bacilli that form spores that are highly resistant to environmental assaults, thus complicating their treatment. Both bacilli can cause bloodstream infections and diarrhea. C. perfringens is the second leading cause of foodborne bacterial illness in the United States, resulting in approximately one million cases annually;1 the fourth most common in Europe,2 and among the top six in Japan.3 C. difficile causes antibiotic-associated diarrhea (AAD) and severe infectious colitis, resulting in high morbidity and mortality on a global scale. C. difficile has also been associated with gastroenteritis-related mortality in North America and Europe for several decades.4 However, there is a paucity of evidence regarding the occurrence of fatalities resulting from diarrhea due to co-infection with C. perfringens and C. difficile. A novel ST-type C. perfringens strain was recently isolated from the feces of a patient presenting with diarrhea, a condition not previously documented in the medical literature. Here, we report a rare case of severe diarrhea caused by a novel ST-865 type of C. perfringens in conjunction with C. difficile to draw the attention of clinicians and microbiology laboratory staff.
Case Description
A 69-year-old male presented with diarrhea without an identifiable trigger a month prior to admission. Diarrhea was characterized by mucopurulent and bloody stools accompanied by nausea and vomiting but no fever. The patient was admitted to a local hospital 25 days before presentation and was diagnosed with infectious diarrhea. The three stool cultures yielded negative results. An anti-infection regimen of levofloxacin, ceftriaxone, minocycline, gentamicin, and tinidazole was initiated, which notably improved his symptoms. Seven days previously, the patient presented with mucopurulent bloody stools accompanied by abdominal pain and diarrhea. His abdominal discomfort intensified, prompting admission as an outpatient for further treatment of infectious diarrhea.
Physical examination upon admission revealed a body temperature of 36.4°C, respiratory rate of 20 bpm, heart rate of 112 bpm, blood pressure of 111/89 mmHg, flat abdomen, normal respiratory movement, soft abdominal wall, and abdominal pressure without a palpable mass. Laboratory test results indicated a C-reactive protein content of 201.50 mg/L (normal value, 0–8 mg/L), white blood cell count of 1.42 × 109/L (normal value, 4.0–10.0 × 109/L), red blood cell count of 2.63 × 10¹²/L (normal value, 4.0–5.5 × 10¹²/L), absolute neutrophil count of 1.19 × 109/L (normal value, 1.5–7.0 × 109/L), and procalcitonin content of 2.12 ng/mL (normal value, <0.15 ng/mL). The fecal sample was watery and was positive for occult blood and transferrin. These findings suggested the presence of intestinal infection, and a stool sample was sent for culture (Figure 1A). Gram staining of the stool samples revealed the presence of predominantly gram-positive cocci with a minor population of large gram-positive rods (Figure 1B), suggesting an imbalance in the microbial community. After 48 h of aerobic incubation, there was no growth of pathogenic bacteria. However, anaerobic culture yielded two presumptive pathogenic bacterial colonies. The first colony, measuring 2–4 mm in diameter, exhibited a white, round, elevated, smooth surface and a neat edge, with evident hemolysis (Figure 1C). This colony was identified as C. perfringens using mass spectrometry. The second colony, measuring 2–3 mm in diameter, displayed a grayish-white coloration with irregular edges and no hemolysis and was identified as C. difficile by mass spectrometry (Figure 1C). Both bacterial strains were tested for susceptibility to imipenem, metronidazole, meropenem, vancomycin, ceftriaxone, penicillin, and piperacillin/tazobactam using the E-test method. The results demonstrated that C. perfringens was susceptible to antimicrobials, whereas C. difficile was resistant to ceftriaxone and penicillin (Table 1). Bacteriophage DNA was extracted and sequenced, which demonstrated that C. difficile harbors two toxin genes: TcdA and TcdB. Multilocus sequence typing (MLST) identified the strain as ST-81. The S. perfringens isolate carried two major toxin genes (plc and cpe) and 22 other toxin genes (nagH, nagI, nagJ, nagL, colA, cloSI, entA, entB, entD, pilB, pilM, pilT, pilC, pilN, pilA1, pilA2, fbpA, CBO, CPF, hlyB, virS, and virR). Notably, the sequencing results demonstrated the absence of a corresponding ST type in the public database, indicating that the C. perfringens isolate was a newly discovered ST type. The housekeeping gene sequence was uploaded to the PubMLST database (https://pubmlst.org/multilocus-sequence-typing) and designated ST-865.
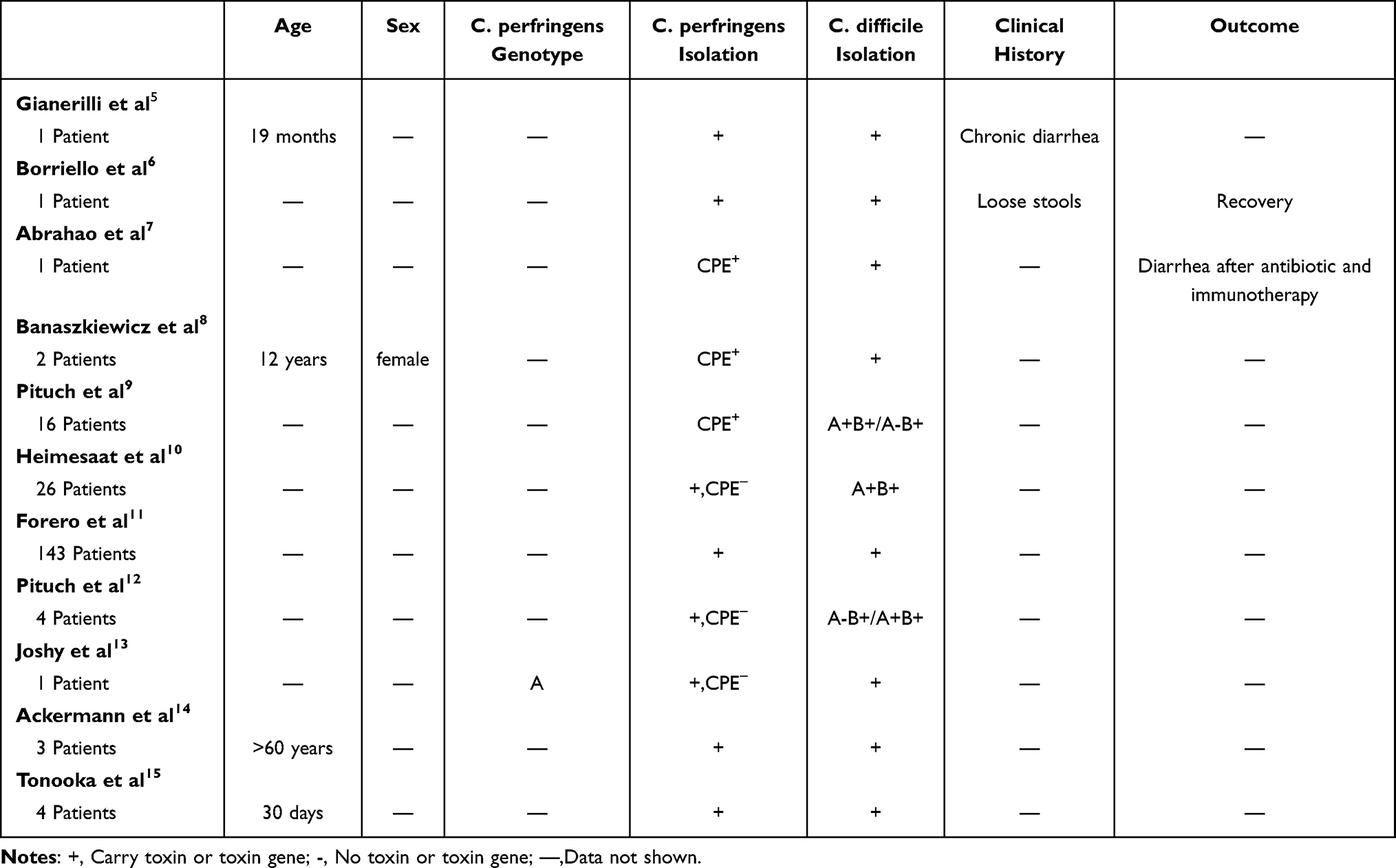 |
Table 1 Details of Simultaneous Detection of C. perfringens and C. difficile as Described in the Literature |
 |
Figure 1 (A) A watery fecal sample. (B) A large number of Gram-positive cocci and a small number of Gram-positive bacilli observed at high magnification of a Gram-stained fecal smear (×1000). (C) Two distinct colonies were observed: one with irregular edges and no hemolysis, identified as C. difficile (white arrow), and a second that was round with a raised, smooth surface, neat edges, and obvious hemolysis, identified as C. perfringens (black arrow). |
During hospitalization, 10 g of human albumin was administered via intravenous drip to treat hypoproteinemia. Acid suppression and rehydration have been used to treat electrolyte disorders. Following admission, cefoperazone sulbactam was administered at 3.0 g every 12 h via an intravenous drip as an anti-infective agent. However, after a 3-day period, there was no improvement, and the patient’s condition deteriorated rapidly, progressing to acute necrotizing enterocolitis 4 days post-admission. On post-admission day 3, in accordance with the stool culture results, penicillin was administered intravenously at 4,000,000 U every 6 h, along with oral vancomycin at 0.125 g every 6 h. On post-admission day 4, the patient’s body temperature was 39.2°C. Thus, aspirin DL-lysine was initiated at 0.9 g as an antipyretic and the anti-infective regimen was continued. However, the patient’s condition did not improve. On the morning of post-admission day 5, the patient was discharged and died 1 day later.
Review and Discussion
A review of the relevant published literature using the keywords “Clostridium perfringens” and “Clostridium difficile” returned 11 articles, but there were no case reports of diarrhea and death due to co-infection with C. perfringens and C. difficile. The retrieved articles are summarized in Table 1. In a report to determine the role of C. difficile in the upper gastrointestinal tract of children, 19 specimens from patients with chronic diarrhea were positive for both bacteria.5 In one case of AAD, both C. perfringens and C. difficile were detected.6 In a prospective study of patients with AAD, 10 fecal specimens were positive for the C. difficile enterotoxin A and one was positive for both the C. perfringens enterotoxin and C. difficile toxin.7 In a study investigating the prevalence of C. perfringens infection in pediatric patients with inflammatory bowel disease, two (2.2%) of 91 stool specimens were positive for both the C. difficile toxin and C. perfringens enterotoxin.8 A pilot study on the clinical correlation between C. difficile toxin and C. perfringens conducted in Poland found that 16 (30.8%) of 52 stool samples were positive for both C. perfringens and C. difficile.9 A prospective study of patients with AAD reported that 26 (3.8%) of 693 stool specimens were positive for C. difficile toxins A and B.10 A study conducted in Bogotá, Columbia, found that 143 (65%) of 220 stool samples were positive for both C. perfringens and C. difficile.11 In a study of 158 patients to explore the role of enterotoxin-producing anaerobes, other than C. difficile, in the etiology of AAD, found that four specimens were positive for both C. perfringens and C. difficile.12 A prospective study conducted in India on the prevalence and characterization of C. perfringens reported that only one (0.07%) of 150 stool specimens was positive for both C. perfringens and C. difficile.13 Another study evaluating the prevalence of different bacteria in the stools of patients with AAD reported that 89 diarrhea specimens were positive for C. perfringens, C. difficile, and Staphylococcus aureus.14 Lastly, an investigation of the prevalence of the genus Clostridium in infants identified both C. perfringens and C. difficile in four (18.2%) of 22 fecal samples.15
A combination of C. perfringens and C. difficile can cause severe intestinal infections. Although both C. perfringens and C. difficile can cause diarrhea, co-infection is uncommon and the underlying mechanisms are distinct. C. perfringens is capable of secreting nearly two dozen different toxins and can be categorized into seven distinct toxin types (A–G) based on the production of six major exotoxins, which include α (CPA), β (CPB), ε (ETX), iota (ITX), enterotoxin (CPE), and necrotizing enteritis B-like (Net-B).16 In the present case, C. perfringens carried two major toxin genes, cpe and plc (also known as cpa), and was therefore classified as type F. This classification is associated with both food poisoning and AAD.16 CPE, the primary toxin produced by C. perfringens, is responsible for gastrointestinal symptoms17 via a mechanism of action that involves binding to the tight junction protein receptor, which is a crucial component of the tight junctions on the surfaces of epithelial and endothelial cells. This binding process not only facilitates the formation of pores in the plasma membrane, but also the removal of claudin proteins from the cell membrane, thereby disrupting the tight junctions between cells, thereby increasing barrier permeability and impairing absorption in the small intestine and colon, leading to diarrhea.18,19 Isolates of the F-type carrying the chromosomal cpe gene are reportedly more likely to cause foodborne gastrointestinal disorders, whereas most isolates of the F-type carrying the plasmid cpe gene are mainly associated with non-foodborne gastrointestinal disorders.20 Furthermore, strains carrying the plasmid cpe gene exhibit greater heat resistance than strains with the chromosomal cpe gene.21 This enhanced heat resistance enables the former to survive in food, thereby increasing the likelihood of food poisoning. Sequencing analysis revealed that the cpe gene of C. perfringens in this case was located on the chromosome, which may provide more favorable conditions for food-borne infection. Furthermore, our findings revealed that this particular strain of C. perfringens contained 22 paratoxin genes, including colA, which has been associated with avian necrotizing enterocolitis and degradation of the extracellular matrix.22 The nagH, nagI, nagJ, and nagL genes have been demonstrated to promote the diffusion of tissue-damaging α-toxins, degrade hyaluronic acid cell surface coatings, and increase the permeability of connective tissues, which collectively elevate the risk of airborne gangrene. Given their destructive impact on the intestine,23,24 we postulate that these toxins may facilitate further invasion of C. difficile and provide favorable conditions for co-infection with C. perfringens and C. difficile, although this hypothesis requires further confirmation. A total of 186 C. perfringens isolates were obtained from nine provinces in China between 2013 and 2021. Human isolates were characterized by four predominant types:25 ST-221, ST-62, ST-408, and ST-493. In a separate study, 195 ST types were identified in 372 isolates from diverse sources. The most common subtypes are ST-147, ST-248, ST80, ST251, and ST-73. However, isolates within these STs tended to share the same toxin type. For instance, 14 F-type isolates obtained from food and human sources in the United States and Italy between 2017 and 2019 were classified as ST-147, while 13 F-type isolates from dogs and horses in Canada and the United States were classified as ST-80.26 Notably, this is the first report of diarrhea caused by the novel ST-865 type. The housekeeping gene sequence of this new ST type was uploaded to the PubMLST database for reference. Although the origin of this strain was not traced in detail, these new typing results may serve to enhance the C. perfringens database and provide a theoretical foundation for future epidemiological investigations of this bacterium.
Diarrhea caused by C. difficile is a direct consequence of the disruption of the intestinal flora following antibiotic administration. In this case, the C. difficile infection produced two toxins, A and B, which are encoded by tcdA and tcdB, respectively, within the pathogenicity locus. The pathogenesis of diarrhea caused by C. difficile is primarily driven by the activity of enterotoxin A and cytotoxin B, which are internalized by intestinal epithelial cells, resulting in the glycosylation of small Rho proteins in the cell membrane, ultimately leading to cell death and a loss of intestinal barrier function.4,27 Furthermore, the host immune response intensifies the symptoms of infection, including an acute intestinal inflammatory response and neutrophil infiltration, which exacerbate damage to epithelial cells.28 A number of studies have demonstrated that individuals who are particularly susceptible to C. difficile infection include those who are hospitalized and have recently undergone antibiotic exposure, as well as those aged ≥65 years.29 The risk factors for C. difficile infection in these individuals include the elimination of protective gut flora by antibiotics29–31 and a diminished immune response to C. difficile due to age and medical comorbidities.32,33 In this case, the patient was aged ≥65 years and had been treated with antibiotics, including tinidazole, gentamicin, and minocycline, at the onset of diarrhea, which markedly elevated the likelihood of C. difficile infection.
Search Strategy and Selection Criteria
Articles were retrieved from the MEDLINE (PubMed), SPRINGER NATURE LINK, Web of Science, and EBSCO databases until December 29, 2024, with the key words “Clostridium perfringens” and “Clostridium difficile”, and no restrictions on language, in additional to the reference lists of the retrieved publications.
Conclusion
We postulated that our patient had a diet-induced C. perfringens infection, and that the extensive use of antimicrobials during treatment resulted in intestinal flora dysbiosis and C. difficile co-infection, which ultimately progressed to severe hemorrhagic necrotizing enterocolitis. Despite our best efforts to identify the causative pathogen, the patient’s condition ultimately deteriorated, resulting in his demise 1 day after the administration of penicillin for C. perfringens and vancomycin for C. difficile. To the best of our knowledge, this is the first reported death caused by a co-infection with C. perfringens and C. difficile. In particular, an ST-865 type C. perfringens was identified. It remains unclear whether the large number of toxin genes carried by this F-type strain is associated with the severe symptoms observed in this patient. Furthermore, it is unclear whether this strain is more likely to occur with C. difficile. These research avenues warrant further investigation.
Ethical Approval
This report has been approved by The Affiliated Hospital of Chengde Medical University’s ethics committee to publish the case details and conducted in accordance with the ethical principles for medical research involving human subjects, as described in the Declaration of Helsinki. Written informed consent to have the case details published has been provided by the patient’s family.
Acknowledgment
We would like to thank the patient’s family for their consent.
Funding
This study was supported by the 2023 Clinical Medical Excellent Talent Cultivating Program of Hebei (grant no. ZF2023248).
Disclosure
The authors declare no competing interests in this work.
References
1. Scallan E, Hoekstra RM, Angulo FJ, et al. Foodborne illness acquired in the United States--major pathogens. Emerg Infect Dis. 2011;17(1):7–15. doi:10.3201/eid1701.P11101
2. Mahamat Abdelrahim A, Radomski N, Delannoy S, et al. Large-scale genomic analyses and toxinotyping of Clostridium perfringens implicated in foodborne outbreaks in France. Front Microbiol. 2019;10:777. doi:10.3389/fmicb.2019.00777
3. Komatsu H, Inui A, Sogo T, Fujisawa T. Clostridium perfringens. Nihon Rinsho. 2012;70(8):1357–1361.
4. Burke KE, Lamont JT. Clostridium difficile infection: a worldwide disease. Gut Liver. 2014;8(1):1–6. doi:10.5009/gnl.2014.8.1.1
5. Gianerilli P, Luzzi I, Occhionero M, Capano G, Guarino A, Guandalini S. Clostridium difficile and Clostridium perfringens in upper gut of infants with protracted diarrhoea. J Clin Pathol. 1985;38(10):1196. doi:10.1136/jcp.38.10.1196-a
6. Borriello SP, Welch AR, Larson HE, Barclay F. Diarrhoea and simultaneous excretion of Clostridium difficile cytotoxin and C perfringens enterotoxin. Lancet. 1984;2(8413):1218. doi:10.1016/S0140-6736(84)92778-8
7. Abrahao C, Carman RJ, Hahn H, Liesenfeld O. Similar frequency of detection of Clostridium perfringens enterotoxin and Clostridium difficile toxins in patients with antibiotic-associated diarrhea. Eur J Clin Microbiol Infect Dis. 2001;20(9):676–677. doi:10.1007/s100960100571
8. Banaszkiewicz A, Kadzielska J, Gawronska A, et al. Enterotoxigenic Clostridium perfringens infection and pediatric patients with inflammatory bowel disease. J Crohns Colitis. 2014;8(4):276–281. doi:10.1016/j.crohns.2013.08.018
9. Pituch H, Obuch-Woszczatynski P, Wultanska D, van Belkum A, Meisel-Mikolajczyk F, Luczak M. Laboratory diagnosis of antibiotic-associated diarrhea: a Polish pilot study into the clinical relevance of Clostridium difficile and Clostridium perfringens toxins. Diagn Microbiol Infect Dis. 2007;58(1):71–75. doi:10.1016/j.diagmicrobio.2006.12.007
10. Heimesaat MM, Granzow K, Leidinger H, Liesenfeld O. Prevalence of Clostridium difficile toxins A and B and Clostridium perfringens enterotoxin A in stool samples of patients with antibiotic-associated diarrhea. Infection. 2005;33(5–6):340–344. doi:10.1007/s15010-005-5067-3
11. Forero AJ, Munoz M, Camargo M, et al. High frequency of toxigenic Clostridium difficile and Clostridium perfringens coinfection among diarrheic patients at health care facility-onset (HCFO) and community-onset (CO) centers in Bogota, Colombia. Gut Pathog. 2019;11(1):27. doi:10.1186/s13099-019-0308-7
12. Pituch H, van den Braak N, van Belkum A, et al. Characterization of Clostridium perfringens strains isolated from Polish patients with suspected antibiotic-associated diarrhea. Med Sci Monit. 2002;8(3):BR85–BR88.
13. Joshy L, Chaudhry R, Dhawan B, Kumar L, Das BK. Incidence and characterization of Clostridium perfringens isolated from antibiotic-associated diarrhoeal patients: a prospective study in an Indian hospital. J Hosp Infect. 2006;63(3):323–329. doi:10.1016/j.jhin.2005.12.015
14. Ackermann G, Thomalla S, Ackermann F, Schaumann R, Rodloff AC, Ruf BR. Prevalence and characteristics of bacteria and host factors in an outbreak situation of antibiotic-associated diarrhoea. J Med Microbiol. 2005;54(2):149–153. doi:10.1099/jmm.0.45812-0
15. Tonooka T, Sakata S, Kitahara M, et al. Detection and quantification of four species of the genus Clostridium in infant feces. Microbiol Immunol. 2005;49(11):987–992. doi:10.1111/j.1348-0421.2005.tb03694.x
16. Rood JI, Adams V, Lacey J, et al. Expansion of the Clostridium perfringens toxin-based typing scheme. Anaerobe. 2018;53:5–10. doi:10.1016/j.anaerobe.2018.04.011
17. Freedman JC, Shrestha A, McClane BA. Clostridium perfringens enterotoxin: action, genetics, and translational applications. Toxins. 2016;8(3):73. doi:10.3390/toxins8030073
18. Eichner M, Augustin C, Fromm A, et al. In colon epithelia, Clostridium perfringens enterotoxin causes focal leaks by targeting claudins which are apically accessible due to tight junction derangement. J Infect Dis. 2017;217(1):147–157. doi:10.1093/infdis/jix485
19. Sonoda N, Furuse M, Sasaki H, et al. Clostridium perfringens enterotoxin fragment removes specific claudins from tight junction strands: evidence for direct involvement of claudins in tight junction barrier. J Cell Biol. 1999;147(1):195–204. doi:10.1083/jcb.147.1.195
20. Wang B, Dong W, Ma L, et al. Prevalence and genetic diversity of Clostridium perfringens isolates in hospitalized diarrheal patients from central China. Infect Drug Resist. 2021;14:4783–4793. doi:10.2147/IDR.S338593
21. Sparks SG, Carman RJ, Sarker MR, McClane BA. Genotyping of enterotoxigenic Clostridium perfringens fecal isolates associated with antibiotic-associated diarrhea and food poisoning in North America. J Clin Microbiol. 2001;39(3):883–888. doi:10.1128/JCM.39.3.883-888.2001
22. Van Damme L, Cox N, Callens C, et al. Protein truncating variants of colA in Clostridium perfringens type G strains. Front Cell Infect Microbiol. 2021;11:645248. doi:10.3389/fcimb.2021.645248
23. Hynes WL, Walton SL. Hyaluronidases of Gram-positive bacteria. FEMS Microbiol Lett. 2000;183(2):201–207. doi:10.1111/j.1574-6968.2000.tb08958.x
24. Canard B, Garnier T, Saint-Joanis B, Cole ST. Molecular genetic analysis of the nagH gene encoding a hyaluronidase of Clostridium perfringens. Mol Gen Genet. 1994;243(2):215–224. doi:10.1007/BF00280319
25. Zhong JX, Zheng HR, Wang YY, et al. Molecular characteristics and phylogenetic analysis of Clostridium perfringens from different regions in China, from 2013 to 2021. Front Microbiol. 2023;14:1195083. doi:10.3389/fmicb.2023.1195083
26. Camargo A, Guerrero-Araya E, Castaneda S, et al. Intra-species diversity of Clostridium perfringens: a diverse genetic repertoire reveals its pathogenic potential. Front Microbiol. 2022;13:952081. doi:10.3389/fmicb.2022.952081
27. Etienne-Manneville S, Hall A. Rho GTPases in cell biology. Nature. 2002;420(6916):629–635. doi:10.1038/nature01148
28. Kelly CP, Kyne L. The host immune response to Clostridium difficile. J Med Microbiol. 2011;60(Pt 8):1070–1079. doi:10.1099/jmm.0.030015-0
29. Edlund C, Nord CE. Effect of quinolones on intestinal ecology. Drugs. 1999;58(Suppl 2):65–70. doi:10.2165/00003495-199958002-00013
30. Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect. 2009;58(6):403–410. doi:10.1016/j.jinf.2009.03.010
31. Pepin J, Saheb N, Coulombe M, et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a cohort study during an epidemic in Quebec. Clin Infect Dis. 2005;41(9):1254–1260. doi:10.1086/496986
32. Kyne L, Warny M, Qamar A, Kelly CP. Asymptomatic carriage of Clostridium difficile and serum levels of IgG antibody against toxin A. N Engl J Med. 2000;342(6):390–397. doi:10.1056/NEJM200002103420604
33. Kyne L, Warny M, Qamar A, Kelly CP. Association between antibody response to toxin A and protection against recurrent Clostridium difficile diarrhoea. Lancet. 2001;357(9251):189–193. doi:10.1016/S0140-6736(00)03592-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.