")
Back to Journals » Nature and Science of Sleep » Volume 16
Decreased Memory-Related Regional Cerebral Perfusion in Severe Obstructive Sleep Apnea with a Mild Cognitive Impairment During Wakefulness
Authors Yan X , Liu W, Li D, Huang Q, Wu J, Zhang Q
Received 27 June 2024
Accepted for publication 22 November 2024
Published 3 December 2024 Volume 2024:16 Pages 1869—1880
DOI https://doi.org/10.2147/NSS.S481602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Xiangbo Yan,1,2 Wanqing Liu,3 Danyang Li,1 Qiang Huang,1 Jianlin Wu,1 Qing Zhang1
1Imaging Department, Affiliated Zhongshan Hospital Dalian University, Dalian, People’s Republic of China; 2Faculty of Medicine, Dalian University of Technology, Dalian, People’s Republic of China; 3Department of Radiology, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Qing Zhang, Imaging Department, Affiliated Zhongshan Hospital, Dalian University, Dalian, 116001, People’s Republic of China, Tel +86 15566978288, Email [email protected]
Purpose: Previous studies have found that obstructive sleep apnea (OSA) can induce cognitive impairment (CI). However, the exact mechanisms of CI development in patients with OSA remains unclear. We investigated the neuropathological basis of CI development by examining changes in cerebral blood perfusion.
Patients and Methods: Thirty-five patients with untreated OSA (15 with CI and 20 without CI [NCI]) and 15 good sleepers (GS) diagnosed using polysomnography were recruited. All participants underwent resting state brain scans in a Siemens 3.0 Tesla magnetic resonance imaging scanner with a pulsed arterial spin labeling sequence and completed a battery of neuropsychological tests.
Results: Compared to the regional cerebral blood flow (rCBF) values in the GS group, both the CI and NCI groups exhibited lower rCBF values in the bilateral inferior temporal, left lingual, and right medial and paracingulate gyri, as well as higher rCBF values in the bilateral middle frontal gyrus (p < 0.05 in all cases). Compared to the rCBF values in the NCI group, the CI group had lower rCBF values in the bilateral inferior temporal and left lingual gyri, and higher rCBF values in the right rectus and right middle orbital frontal gyri (p < 0.05 in all cases). In the CI group, rCBF values in the bilateral inferior temporal (right, p = 0.025; left, p = 0.005) and left lingual gyri (p = 0.018) were positively associated with the delayed memory scores, and rCBF values in the left inferior temporal gyrus positively correlated with the attention scores (p = 0.011).
Conclusion: Regions with abnormal perfusion in the NCI and CI groups were mostly memory-related. Blood perfusion in the bilateral inferior temporal and left lingual gyri decreased in the following order: GS > OSA-NCI > OSA-CI. These findings provide blood perfusion-level insights into the neuropathological basis of OSA-CI development.
Keywords: Obstructive sleep apnea, cognitive impairment, cerebral blood flow, memory function, arterial spin labeling
Introduction
Obstructive sleep apnea (OSA) is characterized by recurrent upper airway collapse and obstruction during sleep, leading to hypopnea and breathing-related arousal.1,2 OSA can also induce cognitive impairment (OSA-CI).3 Patients with OSA-CI may experience deficits in attention, memory, executive function, emotion regulation, visuospatial ability, fine coordination, and language skills.4 However, the neuropathological basis of CI development in patients with OSA remains unclear. Therefore, investigating the mechanisms associated with cognitive function in OSA using neuroimaging is crucial for the early clinical prevention and diagnosis of OSA-CI.
In patients with OSA, high levels of sympathetic excitation and delayed vasoconstrictor effects may reduce cerebral blood flow.5,6 Moreover, apnea episodes in patients with OSA can cause cerebral hypoxia, resulting in increased carbon dioxide concentrations and vascular dilation, leading to elevated cerebral blood flow.7,8 Both these factors disrupt the self-regulation mechanism of human cerebral blood flow. The dysfunction of cerebral vascular endothelial cells owing to blood pressure fluctuations in patients with OSA may further contribute to the abnormal cerebral blood flow perfusion in the affected brain areas, ultimately leading to structural9 and functional10,11 brain damage and cognitive function decline.7 This suggests that cerebral blood perfusion may be used as an important indicator of neuropathological mechanisms of OSA-CI. Therefore, in the present study, we employed arterial spin labeling (ASL)8 and examined local cerebral hemodynamic features to investigate neuropathological characteristics of patients with OSA-CI.
Such patients may initially present with decreased memory function. In relevance to this, decreased cerebral blood perfusion in OSA patients has been observed in brain areas related to memory function (eg, bilateral parahippocampal and left lingual gyri).12–14 From the disease comorbidity perspective, OSA contributes to neurological diseases such as mild cognitive impairment (MCI) and Alzheimer’s disease, accompanied by early memory loss.3,15 Temporal brain regions, such as the inferior temporal and parahippocampal gyri, are relatively distal from the main blood vessels, so normal blood oxygen content in these regions is sufficient only for the basic neural activity maintenance.13 Furthermore, the temporal hippocampal gyrus has lower vascular expansion capacity than other brain regions, making it susceptible to insufficient blood supply and oxygen deprivation, which may lead to a decline in memory function.13 Thus, once brain blood perfusion becomes abnormal, it may initially affect blood supply to brain regions distal to large blood vessels, such as the hippocampal gyrus, consequently affecting memory function.
Some neuroimaging studies have found that factors such as age, sex, and global mean brain blood perfusion affect calculation of blood perfusion values in local brain regions.16,17 Therefore, when examining group differences in regional cerebral blood flow (rCBF), it is essential to control for these factors to ensure comparability between groups. In addition, given that OSA severity positively correlates with body mass index (BMI) and sleepiness levels that both could affect cerebral blood perfusion,18,19 it was difficult to control the effects of BMI and sleepiness levels on cerebral blood perfusion between the GS and OSA groups. However, differences in BMI and sleepiness levels between the OSA-NCI and OSA-CI groups were counterbalanced. Therefore, directly comparing differences in rCBF between the OSA-NCI and OSA-CI groups may help mitigate the influence of BMI and drowsiness levels.
We hypothesized that during the progression from no CI to mild CI, memory function in severe OSA deteriorates more significantly than other cognitive functions, and most abnormally perfused brain regions would be associated with memory function. Based on the speculation that the aggravation of cerebral blood perfusion abnormalities triggers CI, we further hypothesized that rCBF in memory-related brain regions would decrease in the following order: GS > OSA-NCI > OSA-CI.
Materials and Methods
Participants
This study was approved by the Ethics Committee of the Affiliated Zhongshan Hospital of Dalian University and included 50 participants who provided written informed consent prior to the study. Considering that patients with OSA need to undergo prolonged abnormal perfusion of cerebral blood to develop cognitive impairment, and previous studies found only abnormal brain perfusion in severe OSA patients,14 we divided the participants into three groups: good sleepers (GS), patients with severe OSA without cognitive impairment (OSA-NCI), and patients with severe OSA with cognitive impairment (OSA-CI). This helped us analyze cerebral blood perfusion dynamics during OSA development from a healthy state to confirmed OSA with mild CI.
Based on the diagnosis of MCI and polysomnography (PSG), the participants were allocated to the GS, OSA-CI, and OSA-NCI groups. The three groups were matched by age, sex, and educational level. The OSA-CI, OSA-NCI, and GS groups comprised 14 untreated OSA patients, 21 untreated OSA patients, and 15 GSs, respectively.
For the OSA group, the study inclusion criteria were as follows: 1) suspected of having OSA and was not treated; 2) between 25 and 60 years of age, right-handed, completed more than 9 years of schooling; 3) the apnea-hypopnea index (AHI) ≥ 15 times/h on overnight PSG. The MCI was diagnosed based on the revised consensus criteria of the International Working Group on MCI.20 For the patients with MCI, the inclusion criteria were as follows: 1) the person was neither normal nor demented; 2) Montreal Cognitive Assessment (MoCA) score below 26, met the criteria for MCI, and subjectively reported significant memory decline; and 3) activities of daily living were preserved, and complex instrumental functions were intact.
The inclusion criteria for the GS group were as follows: 1) hospital and social volunteers whose handedness, age, and education level were matched with those of the OSA group; 2) AHI < 5 times/h on overnight PSG; and 3) no CI. The inclusion criteria for the OSA-NCI group were as follows: 1) the inclusion criteria for OSA were met, 2) the person had no CI, and 3) the MoCA scores of all patients in this group were greater than 26 and not significantly different from those of the GS group. The inclusion criteria for the OSA-CI group were as follows: 1) the inclusion criteria for OSA were met, 2) the inclusion criteria for MCI were met, and 3) the MoCA scores in this group were less than 26 and significantly lower than those in the GS group.
The study exclusion criteria were as follows: 1) respiratory diseases other than OSA; 2) severe hypertension, Alzheimer’s disease, diabetes, and cardiovascular disease; 3) neurological diseases (epilepsy, schizophrenia, and neurodegenerative diseases); 4) intracranial structural lesions (severe white matter lesions, cerebrovascular disease, brain atrophy, brain trauma, cerebral infarction, cerebral hemorrhage, and tumor); 5) a history of alcoholism, use of psychotropic substances within 1 week of study initiation; 6) metal implants, claustrophobia, and other factors that would limit MRI data acquisition.
PSG Assessment
Overnight PSG examinations were conducted in the sleep monitoring room of the Otolaryngology Department at the Zhongshan Hospital of Dalian University. A Philips Alice 6 system was used to record the electroencephalogram (10–20 EEG electrode positions), bilateral electrooculogram, electrocardiogram, mandibular electromyography, chest and abdominal exercises, oronasal airflow, finger pulse oxygen saturation, bilateral leg movements, and body position measurements over an 8-hour period at night. Subsequently, sleep-related parameters, such as AHI (events/h), minimum oxygen saturation (minimum SaO2, %), mean oxygen saturation (mean SaO2, %), oxygen desaturation index (events/h), sleep efficiency (SE, %), total sleep time (TST, min), awake index (events/h), and microarousal index (events/h) were obtained.
Using thermocouple readings, apnea was defined as an airflow reduction of > 90% from baseline for > 10s. Hypopnea was defined as a reduction in the nasal pressure airflow signal by > 30% from baseline for > 10s. In this study, the clinical signs and symptoms in all patients with OSA included excessive daytime sleepiness, insufficient rest despite adequate sleep duration, loud or irregular snoring, and choking or difficulty in breathing while sleeping. OSA severity was classified as light, moderate, or severe according to the 2012 American Academy of Sleep Medicine (AASM) guidelines: mild (5 < AHI < 15 events/hour), moderate (15 ≤ AHI < 30 events/hour), and severe (AHI ≥ 30 events/hour).
Neuropsychological Scale Assessments
All neuropsychological scale assessments were administered prior to the MRI scan. Each participant completed the following scale assessments sequentially: MoCA, the Epworth Sleepiness Scale (ESS), Self-Rating Anxiety Scale (SAS), and Self-Rating Depression Scale (SDS).
MoCA is a widely used scale for screening for cognitive dysfunction that encompasses tests of executive function, immediate recall, word fluency, orientation, calculation, abstraction, delayed recall, visual perception, and nomenclature. Scores range from 0 to 30, with a score of 26 or higher considered normal, and less than 26 indicating cognitive impairment.21
ESS comprises eight self-rated questions with a maximum total score value of 24. A score of 6 indicates sleepiness, 11 indicates excessive sleepiness, and 16 indicates severe sleepiness.22
SAS consists of 20 self-rating questions graded on a scale of 1–4, with a total score ranging from 20 to 80. The anxiety index was calculated as total score × 1.25. A score of < 50 indicates no anxiety, 50–59 — mild anxiety, 60–69 — moderate anxiety, and > 70 — severe anxiety.23
SDS also comprises 20 self-rating questions, with a total score ranging from 20 to 80. The depression index was calculated as follows: total score/80. A depression index of < 0.5 indicates no depression, 0.5–0.59 — mild depression, 0.6–0.69 — moderate depression, and > 0.7 — major depression.24
MRI Data Acquisition
ASL utilizes hydrogen protons in the arterial blood as an endogenous tracer. By labeling blood with an inversion pulse and imaging it after a delay, ASL generates a labeled image containing both labeled blood signals and static tissue signals. Subsequently, an unlabeled image containing only static tissue signals is generated without applying an inversion pulse. Finally, blood perfusion images are obtained by subtracting the unlabeled images from the labeled images.
All participants underwent imaging using a Siemens 3.0T Magnetom Verio system equipped with a 12-channel head coil. The scan sequences included 3D-T1-weighted imaging (3D-T1WI) and pulsed arterial spin labeling (PASL). Participants were positioned supine on the examination bed and wore noise-canceling headphones. Sponge foam was used to secure the sides of the head. Participants were instructed to maintain body stability and keep awake during the scan.
A 3D-T1WI sequence was employed, with parameters including repetition time (TR) of 1900 ms, echo time (TE) of 2.79 ms, 176 slices with a slice thickness of 1 mm, voxel size of 0.7 mm × 0.7 mm × 1.0 mm, matrix size of 384 × 384, field-of-view (FOV) of 259 mm × 259 mm, and flip angle (FA) of 9°. The scan durations were 6 min 27s. Additionally, PASL imaging was utilized, with the following parameters: TR of 2500 ms, TE of 11 ms, FA of 90°, bandwidth of 2790 hz/pixel, label-delay of 1800 ms, FOV of 230 mm × 230 mm, and slice thickness of 6 mm. These sequences were used to gather brain structural information for further analyses.
Image Preprocessing
First, two senior imaging diagnosticians reviewed the T2-FLAIR and T1WI images of each subject to identify and exclude those with poor image quality (owing to false artifacts and/or incomplete images) and parenchymal lesions. The cerebral blood flow perfusion images were preprocessed using the ASLtbx toolkit (available at https://www.cfn.upenn.edu/ASLtbx.php) on the MATLAB 2013b platform. The specific steps were as follows. 1) Format conversion: original DICOM images were converted into NIFTI-format images. 2) Spatial standardization: the registered structural images were spatially standardized using the MNI template. The deformation field generated by this process was used for spatial standardization of the cerebral blood flow perfusion map. 3) Registration: the linear transformation of the T1-weighted anatomical structure image was registered to the cerebral blood flow perfusion image. 4) Generation of the rCBF map: ASLtbx was used to process the spatially standardized images and obtain the whole-brain average rCBF map. 5) Normalization: the average rCBF map was normalized by dividing the rCBF value of each voxel by the whole-brain mean. 6) Smoothing: a 6-mm Gaussian smoothing kernel was used to smooth the normalized images and prepare them for subsequent statistical analysis.
Statistical Analysis
Differences between the three groups were analyzed using the IBM SPSS Statistics software (version 20.0; IBM, Armonk, NY, USA). The demographic statistical parameters, neuropsychological scale scores, and PSG parameters of the OSA-CI, OSA-NCI, and GS groups were normally distributed. Therefore, one-way analysis of variance (ANOVA) was used to compare differences between the three groups. The chi-squared test was used to compare the distribution of sexes in the three groups. Differences and effects were considered significant when p < 0.05.
One-way ANOVA of voxel-level rCBF values was performed in the three groups using SPM (http://www.fil.ion.ucl.ac.uk/spm) based on MATLAB, with sex, age, years of education, BMI values, and global brain gray matter mean CBF values being included as covariates. We used brain regions with statistically significant differences in rCBF values between the three groups as regions of interest and extracted rCBF values of each region of all participants using DPABI software. The independent sample t-test was performed to pairwise compare analysis of rCBF values among the three groups (FDR correction; cluster clumps > 50 voxels).
In addition, by using SPSS 20.0, Pearson’s correlation analysis was performed to determine the relationships between rCBF values in different brain regions of patients in the CI and NCI groups and MoCA scores describing visuospatial/executive memory, attention, language, abstraction, delayed memory, orientation, and naming skills.
Results
Demographic and Clinical Data
The results of participants in the CI, NCI, and GS groups regarding demographic data and results of sleep monitoring and neuropsychological scale assessments of all participants are presented in Table 1. Variables including age, sex, years of education, SAS, SDS, visual space, executive function, orientation, naming, and microarousal index did not statistically differ across the three groups (p > 0.05 for all comparisons). However, participants in the CI and NCI groups exhibited higher BMI, ESS, AHI, and oxygen reduction index values compared to those in the GS group (p < 0.05 for all comparisons). Additionally, the minimum SpO2 was significantly lower in the CI and NCI groups than in the GS group (p < 0.05). Moreover, the OSA-CI participants had lower MoCA scores for attention (−23%), language (−27%), abstract memory (−37%), and delayed memory (−50%) compared to those in the GS group (p < 0.05 in all cases).
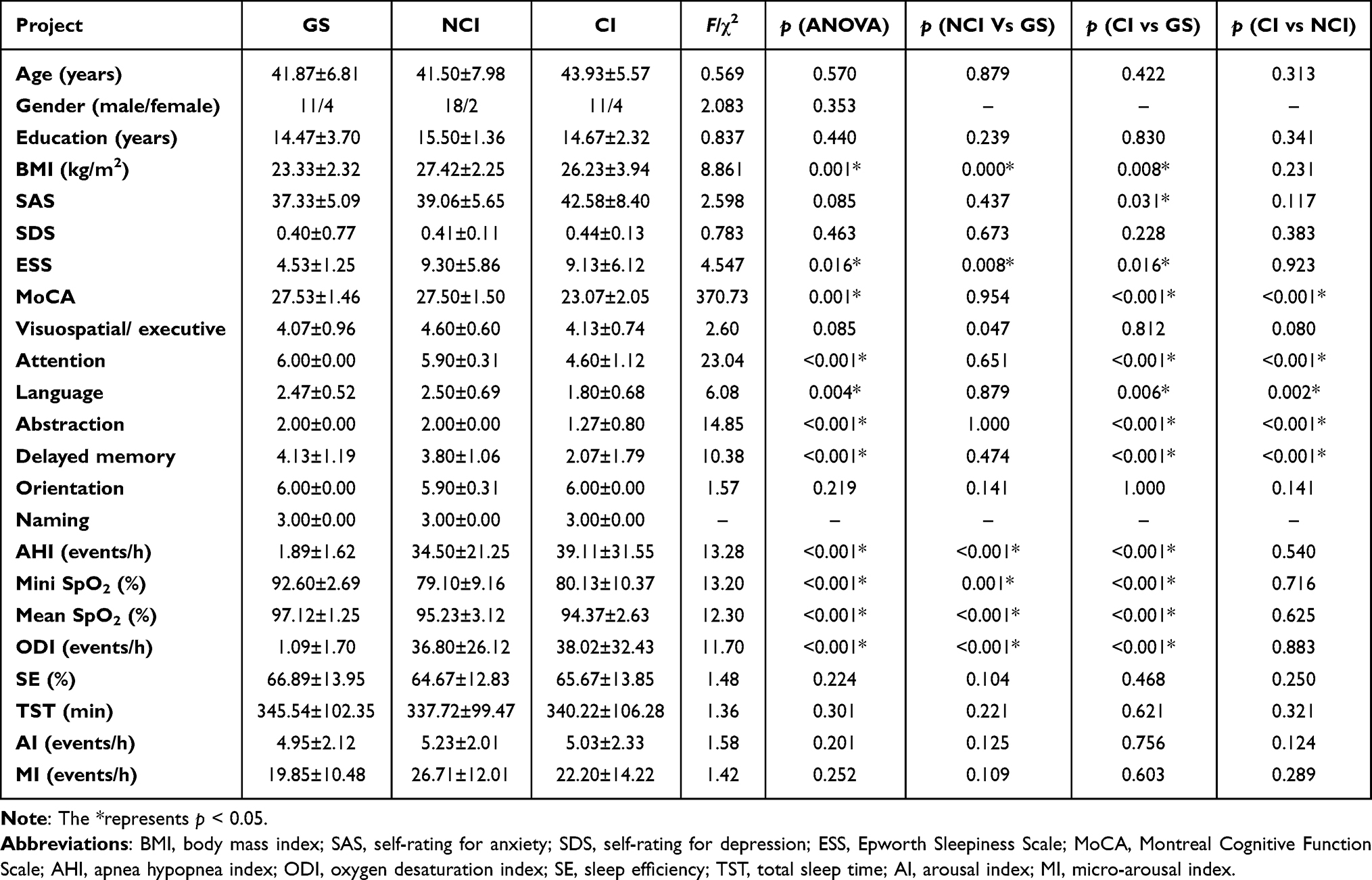 |
Table 1 Results of the Three Groups in Demographic Data, Sleep Monitoring and Neuropsychological Scale Tests |
Comparison of the rCBF Values Among the Three Groups
One-way ANOVA, conducted at the voxel level, revealed significant group differences in rCBF values, primarily localized in the bilateral inferior temporal, left rectus, right orbital inferior frontal, bilateral middle frontal, right angular, right medial, and paracingulate gyri, as well as the right paracentral lobule (p < 0.05, FDR-corrected in all cases; Figure 1). Subsequent post hoc pairwise independent-sample t-tests indicated lower rCBF values in the bilateral inferior temporal, left rectus, left lingual, and right middle orbital frontal gyri in the CI group compared with those in the NCI group (p < 0.05, FDR-corrected in all cases; Table 2; Figure 1). Furthermore, compared with those in the GS group, patients from the NCI group exhibited higher rCBF values in the bilateral middle frontal gyrus, right angular gyrus, and right paracentral lobule, along with decreased rCBF values in the right fusiform, bilateral inferior temporal, left lingual, right middle temporal, right medial, and paracingulate gyri (p < 0.05, FDR-corrected in all cases; Table 3; Figure 1). Similarly, patients with CI displayed higher rCBF values in the bilateral middle frontal gyrus and decreased rCBF values in the bilateral inferior temporal, right lingual, left lingual, right orbital inferior frontal, right medial, and paracingulate gyri compared with those in the GS group (p < 0.05, FDR-corrected in all cases; Table 4; Figure 1).
 |
Table 2 Difference in rCBF Values Between the CI and NCI Groups (p < 0.05, FDR Correction) |
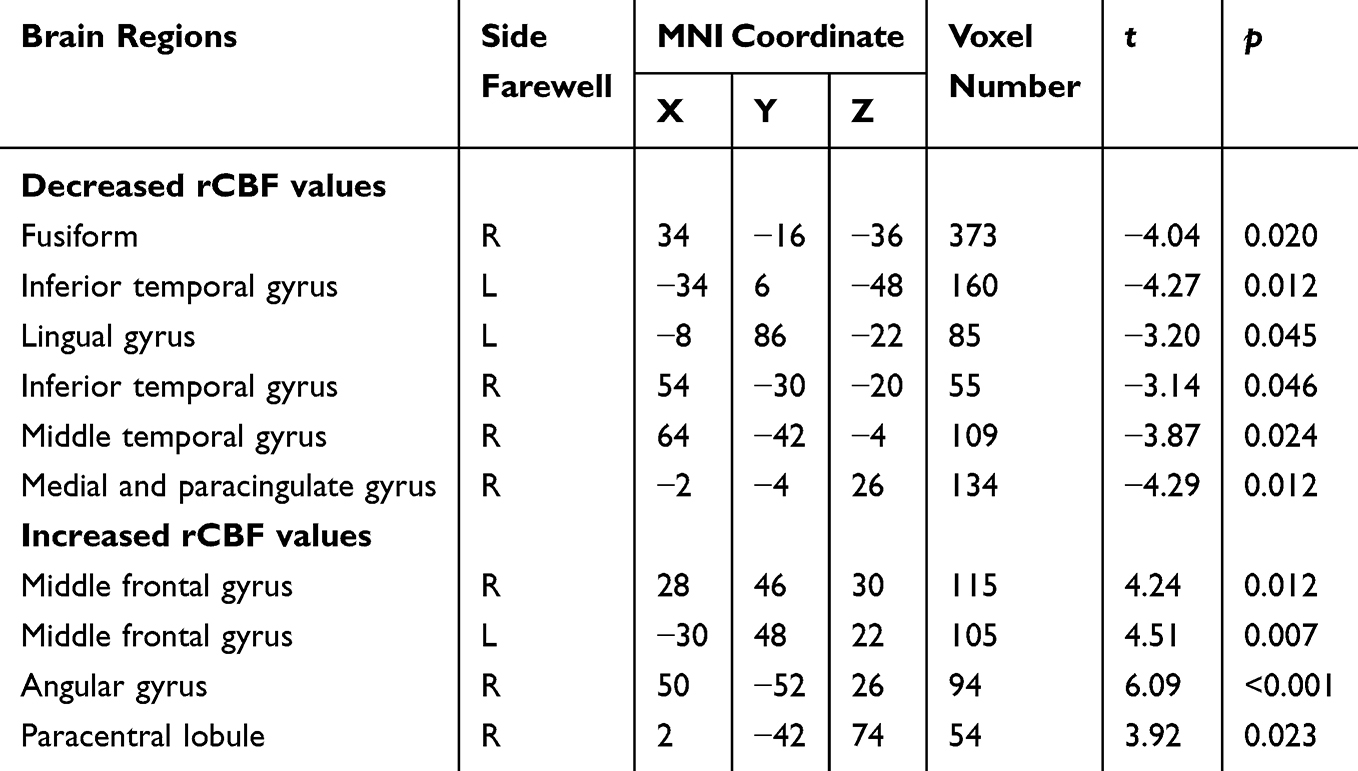 |
Table 3 Difference in rCBF Values Between NCI and GS Groups (p < 0.05, FDR Correction) |
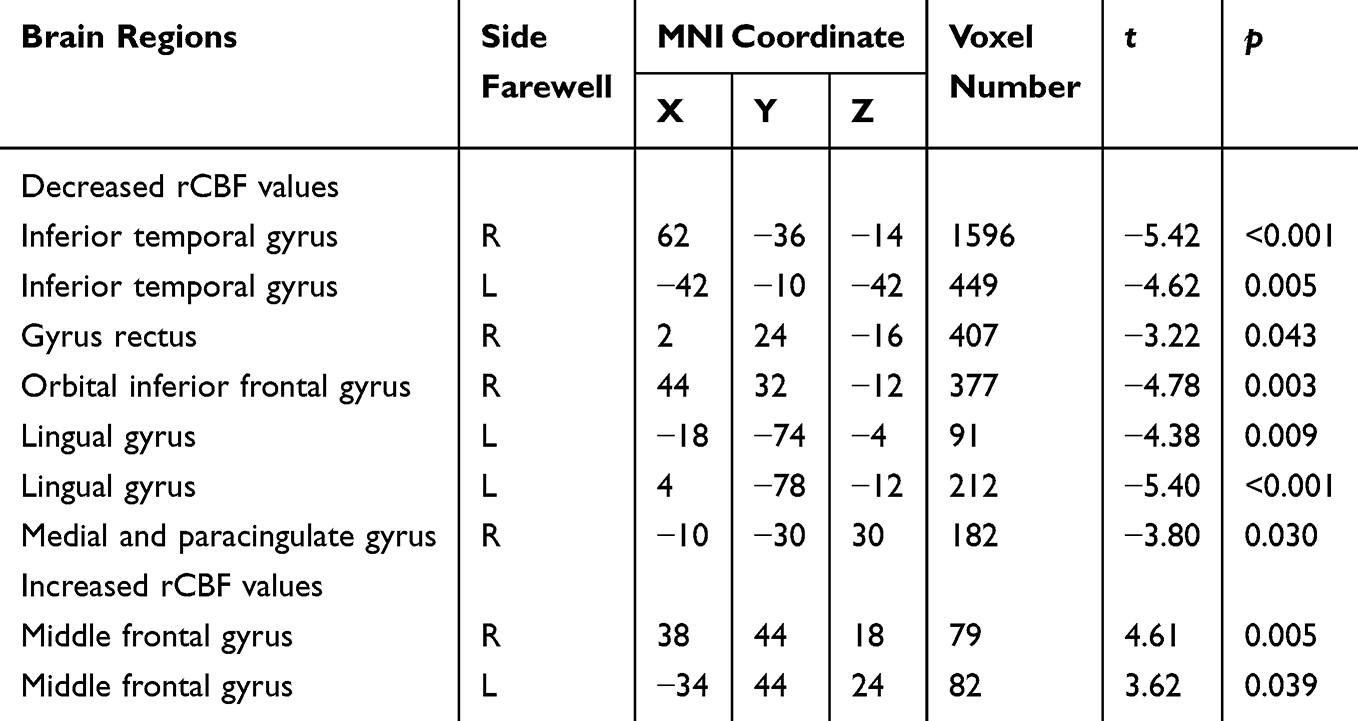 |
Table 4 Difference in rCBF Values Between CI and GS Groups (p < 0.05, FDR Correction) |
 |
Figure 1 Brain regions with divergent rCBF values among the NCI, CI, and GS groups. In this visualization, yellow denotes brain regions exhibiting discrepancies in rCBF values across the three groups as per the one-way ANOVA. Additionally, red indicates brain regions with increased rCBF values, while blue represents brain regions with decreased rCBF values. Abbreviations: rCBF, regional cerebral blood flow; GS, good sleeper; NCI, no cognitive impairment; CI, cognitive impairment. |
Correlation Between rCBF Values and Cognitive Scores in Patients with CI
We nominated brain regions with statistically different rCBF values between the CI and NCI groups as regions of interest and calculated coefficients of Pearson correlation of rCBF values of these regions and cognitive scores in patients with OSA-CI. Specifically, rCBF values in the right inferior temporal gyrus showed a significant positive correlation with delayed recall scores (r = 0.574, p = 0.025). In addition, rCBF values in the left inferior temporal gyrus significantly and positively correlated with delayed recall (r = 0.685, p = 0.005) and attention scores (r = 0.634, p = 0.011). Furthermore, rCBF values in the left lingual gyrus positively correlated with delayed recall scores (r = 0.601, p = 0.018; Figure 2).
 |
Figure 2 Correlation between rCBF values in abnormal brain regions and delayed memory and attention scores in the CI group. (A) a scatter plot of the correlation between delayed memory scores and rCBF values in right inferior temporal gyrus. (B) a scatter plot of the correlation between delayed memory scores and rCBF values in left inferior temporal gyrus. (C) a scatter plot of the correlation between delayed memory and rCBF values in left lingual gyrus. (D) a scatter plot of the correlation between attention scores and rCBF values in left inferior temporal gyrus. Abbreviation: rCBF, regional cerebral blood flow. |
Discussion
In this study, the ASL technique was employed for the quantitative rCBF assessment in patients with OSA differentiated by the presence of CI. Patients in both the CI and NCI groups exhibited higher rCBF values in the bilateral middle frontal gyrus compared with those in the GS group, whereas lower rCBF values were observed in the bilateral inferior temporal, left lingual, right medial, and paracingulate gyri in patients with OSA. These findings are consistent with previous studies of rCBF in regions such as the temporal gyrus and frontal lobes.12 However, we identified additional regions with abnormal rCBF values, namely the lingual and cingulate gyri. This previously unreported observation may be attributed to the previously overlooked confounding factors, such as sex, age, education, and total gray matter mean CBF values. These factors may have masked altered rCBF values associated with OSA in previous studies, which highlights the importance of comprehensive control of confounding variables in neuroimaging research.
In addition, within the CI group, patients exhibited even lower rCBF values in the bilateral inferior temporal gyrus and left lingual gyrus, along with decreased values in the right rectus gyrus and right middle orbital frontal gyrus, compared with those in the NCI group. Notably, in the CI group, rCBF values in the bilateral inferior temporal gyrus and left lingual gyrus positively correlated with delayed recall scores, whereas those in the left inferior temporal gyrus showed a positive correlation with attentional scores. The observation of these relationships may be attributed to comprehensive considerations of potential influencing factors, including sex, age, years of education, BMI, drowsiness, anxiety, depression, AHI, minimum SpO2, oxygen minus index, and total gray matter mean CBF value, when comparing the CI and NCI groups. This meticulous approach enhanced the stability and reliability of our findings.
Notably, we observed that rCBF values in the bilateral inferior temporal gyrus and left lingual gyrus in all groups changed in the following group order: GS > OSA-NCI > OSA-CI. These findings suggest that with the ongoing accumulation of brain damage owing to OSA, cerebral blood perfusion abnormalities intensify, culminating in CI detectable by neuropsychological assessments and ultimately leading to a clinical diagnosis of MCI.
Regions of Abnormal Blood Perfusion and Their Significance
Within the temporal lobe, the inferior temporal gyrus (with the hippocampal gyrus situated in its medial aspect) is crucial for semantic memory processing.25 We revealed significantly lower bilateral rCBF values in both the CI and NCI groups compared with those in the GS group. Importantly, we also observed a further reduction of rCBF values in the bilateral inferior temporal gyrus in the CI group compared with those in the NCI group. This is consistent with previous findings of structural26 and functional27 abnormalities in the inferior temporal gyrus of patients with OSA. This underscores the likelihood that lower rCBF values in the bilateral inferior temporal gyrus may be as a crucial factor of CI onset in patients with OSA.
The lingual gyrus lies posterior to the occipital pole and is close to the parahippocampal gyrus. Previous studies linked the lingual gyrus to memory function,28 suggesting a potential association between the lingual gyrus and hippocampal region.29 In our study, we observed lower rCBF values in the left lingual gyrus in the CI group than in the NCI group. Therefore, as in the case with the bilateral inferior temporal gyrus, low rCBF values in the left lingual gyrus may indicate onset of memory impairment in patients with OSA.
The frontal lobe is pivotal for executive function and integration of long-term memory in the brain. Previous longitudinal MRI studies showed improved functional connectivity in the right middle frontal gyrus and cognitive function following 3 months of continuous positive airway pressure therapy in patients with OSA,30 suggesting a potential link between the middle frontal gyrus and cognitive function. In our study, we observed elevated rCBF values in the bilateral middle frontal gyrus in patients with OSA in both the CI and NCI groups compared with those in the GS group, possibly indicating a compensatory increase in cerebral blood flow. Nonetheless, rCBF values in the right middle orbital frontal gyrus were significantly lower in the CI group than in the NCI group. This shows that low rCBF values in the right middle orbitofrontal gyrus may also be indicative of the developing CI in patients with OSA.
The cingulate gyrus encircles the frontal lobe and extends toward the temporal lobe directly above the corpus callosum. Activity in this area is associated with emotional processing, learning, and memory formation.31 Previous studies documented cortical atrophy,32,33 white matter integrity impairment,34,35 decreased functional connectivity,36 and reduced node properties in the structural networks14 within the cingulate gyrus of patients with OSA. Those reports are consistent with our findings of abnormal blood perfusion in this region. Collectively, these data suggest that abnormalities in cingulate gyrus cerebral blood flow perfusion among patients with OSA may disrupt information transmission within the limbic system and thereby contribute to CI development.
Although the precise function of the rectus gyrus remains elusive, prior neuroimaging investigations have documented gray matter volume atrophy and cortical thickness reduction in in this region in patients with OSA.30,36 We observed lower rCBF values in the right rectus gyrus of patients with OSA-CI compared with those in patients with OSA-NCI, suggesting that there may be abnormal alterations in both the structure and function of the right rectus gyrus in the former group.
In summary, brain areas in which abnormal perfusion was noted in patients with OSA and CI were mostly related to memory function, except for the rectus gyrus.
Relationship Between rCBF Values and Cognitive Scores
Our study identified a positive correlation between delayed memory scores and rCBF values in the bilateral inferior temporal gyrus and left lingual gyrus within the CI group. Given the association of both the inferior temporal and lingual gyri with memory function,25,28 we speculate that lower rCBF values in these brain regions may be related to reduced delayed memory scores.
During word memorization, individuals allocate attentional resources to facilitate word perception, recognition, and subsequent encoding into short-term memory.37–39 The left temporal lobe is implicated in speech perception, recognition, and memory processes.40,41 In our study, we revealed a positive correlation between rCBF values in the left inferior temporal gyrus and attention scores in patients with OSA-CI, suggesting that lower rCBF values in this region are associated with diminished attentional capacity. Impaired attentional function in patients with OSA-CI may adversely affect memory quality, resulting in reduced delayed recall. Therefore, the positive correlation between rCBF values in the left inferior temporal gyrus and attention scores may be related to a decrease in delayed memory scores.
Clinical Significance
Previous studies showed that cerebral hemodynamic abnormalities manifest prior to structural brain changes in patients with OSA,9,34 which means that abnormal blood perfusion may predict the occurrence of structural brain damage. In our study, we observed lower rCBF values in the bilateral inferior temporal, left lingual, and right medial and paracingulate gyri in patients with OSA (both the CI and NCI groups) compared with the respective values in the GS group. These findings imply that upon abnormal blood perfusion, these brain regions may be predisposed to structural damage. This insight has practical significance for clinicians, as timely imaging may predict the potential occurrence of organic lesions in these brain regions, and appropriate therapeutic measures may be taken to mitigate the progression of structural brain damage.
Limitations and Future Studies
From a study design perspective, the disproportionately higher representation of male participants reflects the significantly higher incidence of OSA in men, along with the inherent challenges associated with the recruitment of female participants. Nonetheless, future studies should strive to achieve more balanced sex representation.
In this study, we adopted a cross-sectional design. Future longitudinal investigations could track the progression of OSA-CI longitudinally, allowing for within-patient comparisons before and after treatment.
Finally, most brain regions with abnormal blood perfusion identified in this study were associated with memory function, as evidenced by significantly lower memory scores. However, the generalizability of this result may be limited by the sample size because individual differences between the participants cannot be excluded. Moreover, the insufficient sample size precludes a strong conclusion about the relationship between decreased rCBF in the above-mentioned regions and CI. Therefore, future studies should employ larger cohorts of participants to address these issues.
Our results showed that patients with OSA-NCI had abnormal cerebral blood perfusion but normal MoCA scores. This neuropsychological scale was likely insufficiently sensitive to detect functional brain deficits caused by OSA. More sensitive psychological tests (eg, behavioral testing based on reaction time and accuracy as indicators) may allow better detection of early signs of impaired brain function in patients with OSA, facilitating timely identification and intervention by healthcare professionals.
Conclusion
Abnormal perfusion in the groups of patients with OSA (with or without CI) was noted mostly in memory-related brain regions, such as the bilateral inferior temporal, left lingual, and cingulate gyri, as well as the frontal lobe. Furthermore, the extent of the delayed memory deficit in patients with OSA-CI was greater than that in patients with OSA but without CI and individuals with good sleep. In particular, rCBF values in the bilateral inferior temporal gyrus and left lingual gyrus positively correlated with delayed memory scores and changed in the following order in these three groups: GS > OSA-NCI > OSA-CI. These findings support the notion that progressive aggravation of hemodynamic abnormalities in these brain regions in patients with OSA is associated with a gradual decline in memory function.
Ethical Statement
All procedures were in accordance with the Measures for the Ethical Review of Biomedical Research Involving Humans issued by the National Health and Family Planning Commission (National Health Commission Order No.11), the World Medical Association Declaration of Helsinki, and International Ethical Guidelines for Biomedical Research Involving Human Subjects issued by The Council for International Organizations of Medical Sciences. Informed consent was obtained from all subjects included in the study.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (General Project No. 82071911), and Dalian Medical Science Research Plan (Project No. 20181811107). We have reserved a DOI for the description of our protocol (private link for reviewers: https://www.protocols.io/private/CA5B72AD23B511EF92520A58A9FEAC02). This link will be disabled before the publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bixler EO, Vgontzas AN, Ten Have T. et al. Effects of age on sleep apnea in men: i. Prevalence and severity. Am J Respir Crit Care Med. 1998;157(1):144–148. doi:10.1164/ajrccm.157.1.9706079
2. Bixler EO, Vgontzas AN, M LH, et al. Association of hypertension and sleep-disordered breathing. Arch Intern Med. 2000;160(15):2289–2295. doi:10.1001/archinte.160.15.2289
3. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. doi:10.1513/pats.200709-155MG
4. Bucks RS, Olaithe M, Eastwood P. Neurocognitive function in obstructive sleep apnoea: a meta-review. Respirology. 2013;18(1):61–70. doi:10.1111/j.1440-1843.2012.02255.x
5. Gulbenkian S, Uddman R, Edvinsson L. Neuronal messengers in the human cerebral circulation. Peptides. 2001;22(6):995–1007. doi:10.1016/S0196-9781(01)00408-9
6. Narkiewicz K, Somers VK. The sympathetic nervous system and obstructive sleep apnea: implications for hypertension. J Hypertens. 1997;15(12 Pt 2):1613–1619. doi:10.1097/00004872-199715120-00062
7. Liu W, Cao C, Hu B, et al. Topological regularization of networks in adult patients with moderate-to-severe obstructive sleep apnea-hypopnea syndrome: a structural MRI study. Nat Sci Sleep. 2020;12:333–345. doi:10.2147/NSS.S248643
8. Williams DS, Detre JA, Leigh JS, et al. Magnetic resonance imaging of perfusion using spin inversion of arterial water. Proc Natl Acad Sci U S A. 1992;89(1):212–216. doi:10.1073/pnas.89.1.212
9. Cao CL, Liu WQ, Zhang Q. Progress in MRI research on brain gray matter structure in obstructive sleep apnea hypopnea syndrome. Radiol Practice. 2019;34(04):125–130. doi:10.13609/j.cnki.1000-0313.2019.04.021
10. Tahmasian M, Rosenzweig I, Eickhoff SB, et al. Structural and functional neural adaptations in obstructive sleep apnea: an activation likelihood estimation meta-analysis. Neurosci Biobehav Rev. 2016;65:142–156. doi:10.1016/j.neubiorev.2016.03.026
11. Chen LT, Fan XL, Li HJ, et al. Disrupted small-world brain functional network topology in male patients with severe obstructive sleep apnea revealed by resting-state fMRI. Neuropsychiatr Dis Treat. 2017;13:1471–1482. doi:10.2147/NDT.S135426
12. Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: mild cognitive impairment: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. 2018;90(3):126–135. doi:10.1212/WNL.0000000000004826
13. Shaw K, Bell L, Boyd K, et al. Neurovascular coupling and oxygenation are decreased in hippocampus compared to neocortex because of microvascular differences. Nat Commun. 2021;12(1):3190. doi:10.1038/s41467-021-23508-y
14. Innes CR, Kelly PT, Hlavac M, et al. Decreased regional cerebral perfusion in moderate-severe obstructive sleep apnoea during wakefulness. Sleep. 2015;38(5):699–706. doi:10.5665/sleep.4658
15. Reutrakul S, Mokhlesi B. Obstructive sleep apnea and diabetes: a state of the art review. Chest. 2017;152(5):1070–1086. doi:10.1016/j.chest.2017.05.009
16. Liu Y, Zhu X, Feinberg D, et al. Arterial spin labeling MRI study of age and gender effects on brain perfusion hemodynamics. Magn Reson Med. 2012;68(3):912–922. doi:10.1002/mrm.23286
17. Poudel GR, Innes CRH, Jones RD. Cerebral perfusion differences between drowsy and non-drowsy individuals following acute sleep restriction. Sleep. 2012;35(8):1085–1096. doi:10.5665/sleep.1994
18. Ancoli-Israel S, Kripke DF, Mason WJ, Mason WJ, Fell R, Kaplan O. Sleep-disordered breathing in community-dwelling elderly. Sleep. 1991;14(6):486–495. doi:10.1093/sleep/14.6.486
19. Chen JJ, Rosas HD, Salat DH. Age-associated reductions in cerebral blood flow are independent from regional atrophy. NeuroImage. 2011;55(2):468–478. doi:10.1016/j.neuroimage.2010.12.032
20. Winblad B, Palmer K, Kivipelto M; Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment, et al. J. Intern Med. 2004;256:240–246. doi:10.1111/j.1365-2796.2004.01380.x
21. Smith T, Gildeh N, Holmes C. The Montreal cognitive assessment: validity and utility in a memory clinic setting. Can J Psychiatry. 2007;52(5):329–332. doi:10.1177/070674370705200508
22. Chung KF. Use of the Epworth Sleepiness Scale in Chinese patients with obstructive sleep apnea and normal hospital employees. J Psychosom Res. 2000;49(5):367–372. doi:10.1016/S0022-3999(00)00186-0
23. Samakouri M, Bouhos G, Kadoglou M, et al. Standardization of the Greek version of Zung’s Self-rating Anxiety Scale (SAS). Psychiatriki. 2012;23(3):212–220.
24. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515. doi:10.1001/archpsyc.1965.01730060026004
25. Cabeza R, Nyberg L. Imaging cognition II: an empirical review of 275 PET and fMRI studies. J Cogn Neurosci. 2000;12(1):1–47. doi:10.1162/08989290051137585
26. Joo EY, Tae WS, Lee MJ, et al. Reduced brain gray matter concentration in patients with obstructive sleep apnea syndrome. Sleep. 2010;33(2):235–241. doi:10.1093/sleep/33.2.235
27. Li H, Li L, Shao Y, et al. Abnormal intrinsic functional hubs in severe male obstructive sleep apnea: evidence from a voxel-wise degree centrality analysis. PLoS One. 2016;11(10):e0164031. doi:10.1371/journal.pone.0164031
28. Leshikar ED, Duarte A, Hertzog C. Task-selective memory effects for successfully implemented encoding strategies. PLoS One. 2012;7(5):e38160. doi:10.1371/journal.pone.0038160
29. Cho S, Metcalfe AW, Young CB, et al. Hippocampal-prefrontal engagement and dynamic causal interactions in the maturation of children’s fact retrieval. J Cogn Neurosci. 2012;24(9):1849–1866. doi:10.1162/jocn_a_00246
30. Dalmases M, Sole-Padulles C, Torres M, et al. Effect of CPAP on cognition, brain function, and structure among elderly patients with OSA: a randomized pilot study. Chest. 2015;148(5):1214–1223. doi:10.1378/chest.15-0171
31. Critchley HD, Mathias CJ, Josephs O, et al. Human cingulate cortex and autonomic control: converging neuroimaging and clinical evidence. Brain. 2003;126(Pt 10):2139–2152. doi:10.1093/brain/awg216
32. Joo EY, Jeon S, Kim ST, et al. Localized cortical thinning in patients with obstructive sleep apnea syndrome. Sleep. 2013;36(8):1153–1162. doi:10.5665/sleep.2876
33. Macey PM, Henderson LA, Macey KE, et al. Brain morphology associated with obstructive sleep apnea. Am J Respir Crit Care Med. 2002;166(10):1382–1387. doi:10.1164/rccm.200201-050OC
34. Chen HL, Huang CC, Lin HC, et al. White matter alteration and autonomic impairment in obstructive sleep apnea. J Clin Sleep Med. 2020;16(2):293–302. doi:10.5664/jcsm.8186
35. Kumar R, Chavez AS, Macey PM, et al. Altered global and regional brain mean diffusivity in patients with obstructive sleep apnea. J Neurosci Res. 2012;90(10):2043–2052. doi:10.1002/jnr.23083
36. Chou PS, Chen CJ, Hsu CY, et al. Compensatory neural recruitment for error-related cerebral activity in patients with moderate-to-severe obstructive sleep apnea. J Clin Med. 2019;8(7):1077. doi:10.3390/jcm8071077
37. Awh EK, Vogel EK, Oh SH. Interactions between attention and working memory. Neuroscience. 2006;139(1):201–208. doi:10.1016/j.neuroscience.2005.08.023
38. Gazzaley A, Nobre AC. Top-down modulation: bridging selective attention and working memory. Trends Cognit Sci. 2012;16(2):129–135. doi:10.1016/j.tics.2011.11.014
39. Fu Y, Zhou Y, Zhou J, et al. More attention with less working memory: the active inhibition of attended but outdated information. Sci Adv. 2021;7(47):eabj4985. doi:10.1126/sciadv.abj4985
40. Jeneson A, Squire LR. Working memory, long-term memory, and medial temporal lobe function. Learn Mem. 2011;19(1):15–25. doi:10.1101/lm.024018.111
41. Kiernan JA. Anatomy of the temporal lobe. Epilepsy Res Treat. 2012;2012:176157. doi:10.1155/2012/176157
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COMT Val158Met Polymorphism Influences the Cerebral Blood Flow Changes Related to Psychomotor Retardation in Major Depressive Disorder
Yin Y, Xie C, Zhang H, Zhang H, Zhang Z, Yuan Y
Neuropsychiatric Disease and Treatment 2022, 18:2159-2169
Published Date: 25 September 2022