")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Defining Reablement in the Dutch Context: A Modified Delphi Study
Authors Buma LE , Mouchaers I , Zwakhalen SM, Vluggen S, Satink T, Metzelthin SF
Received 12 February 2025
Accepted for publication 8 May 2025
Published 23 May 2025 Volume 2025:18 Pages 2859—2873
DOI https://doi.org/10.2147/JMDH.S522161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lise Elisabeth Buma,1– 3 Ines Mouchaers,1,2 Sandra MG Zwakhalen,1,2 Stan Vluggen,1,2,4 Ton Satink,5 Silke F Metzelthin1,2
1Department of Health Services Research, Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; 2Living Laboratory in Ageing and Long-Term Care, Maastricht, the Netherlands; 3Cicero Zorggroep, Brunssum, the Netherlands; 4Academy of Nursing, Zuyd University of Applied Sciences, Heerlen, the Netherlands; 5Research Group Neurorehabilitation – Self-Regulation and Participation, HAN_University of Applied Sciences, Nijmegen, the Netherlands
Correspondence: Lise Elisabeth Buma, Department of Health Services Research, Care and Public Health Research Institute, Maastricht University, P.O. Box 616, Maastricht, 6200 MD, the Netherlands, Tel +31 43 388 2815, Email [email protected]
Introduction: For the past decade, the Netherlands has been developing and implementing reablement programs to promote independence and to empower older adults’ autonomy. However, a key challenge remains the lack of clarity around the definition of reablement and its relations to usual care practices. Existing international definitions lack specificity to account for contextual differences, such as variations in healthcare systems and cultural norms. An operational definition is needed that not only fits the Dutch health and social care system and incorporates context-specific elements. This study extends the original conceptual definition by integrating these elements, offering clearer, more practical guidance for real-world application.
Materials and methods: A modified Delphi study was performed to develop a definition of reablement that fits the Dutch health and social care system, extending beyond conceptual understanding. The study comprised three expert rounds and three Delphi survey rounds.
Results: A total of 139 participants from Dutch health and social care, education, research, and representatives of clients and informal caregivers, participated. They evaluated statements in four sections: the target group, aims, type of care or support, and characteristics of reablement programs. Key discussions during the expert rounds focused mainly on 1) the target group, emphasizing the importance of involving individuals and their families, and 2) the characteristics of reablement, such as coordinating roles, team composition, and size. Input from the Delphi surveys and expert rounds led to the development of an operational definition for the Dutch context, agreed upon by 81% of stakeholders.
Conclusion: The Delphi methodology proved valuable in identifying context-specific elements and incorporating expert perspectives, creating a culturally and contextually sensitive definition. This definition distinguishes itself from the international version by offering practical guidance on areas of application and interventions, with a focus on promoting social participation, well-being, and the involvement of the individual’s social network.
Keywords: restorative care, goal-oriented care, multidisciplinary collaboration, person-centered care
Introduction
The increase in population ageing and high prevalence of chronic conditions are straining healthcare systems.1 Reablement offers a solution by promoting independence and empowering older adults’ autonomy through person-centered support and interventions.2 Currently, more than 15 countries have embraced the reablement approach, either as a national care policy or as a promising care concept. Still, its interpretation and application can vary greatly depending on the country and healthcare system in which it is implemented. To address this ambiguity, Metzelthin et al3 conducted a Delphi study in 2018 with 82 reablement experts from 11 countries to develop a conceptual, consensus-based, international definition of reablement:
Reablement is a person-centered, holistic approach that aims to enhance an individual’s physical and/or other functioning, to increase or maintain their independence in meaningful activities of daily living at their place of residence and to reduce their need for long-term services. Reablement consists of multiple visits and is delivered by a trained and coordinated interdisciplinary team. The approach includes an initial comprehensive assessment followed by regular reassessments and the development of goal-oriented support plans. Reablement supports an individual to achieve their goals, if applicable, through participation in daily activities, home modifications and assistive devices as well as involvement of their social network. Reablement is an inclusive approach irrespective of age, capacity, diagnosis or setting.
The international consensus based definition of reablement has been utilized as a foundation for policy and research in several countries in Western Europe and Asia.4 This definition outlines reablement in a broad, theoretical sense, and highlights its focus on enabling and empowering individuals. Due to contextual differences between and even within countries this conceptual definition lacks the specificity needed for practical application. For example, it requires more specific information about the target group, assessment tools, interventions, and processes. The ReAble Network5 advocates for developing country-specific operational definitions, based on the internationally accepted conceptual definition.6 Developing an operational definition for a specific context ensures that reablement practices are aligned with local needs and resources, such as the availability of trained professionals and cultural attitudes, thereby increasing their relevance and feasibility for practitioners and policymakers.
In the Netherlands, research on reablement has been conducted for over a decade. The focus has been on developing and implementing reablement programs, as well as evaluating their feasibility, stakeholder experiences and effectiveness in terms of client and care professional outcomes, and cost-effectiveness.2,7,8 With the introduction of a national policy program (Living, Support, and Care for the Elderly) by the Dutch Ministry of Health, Welfare, and Sport in 2022, reablement has gained increased national attention. It is presented as a sustainable solution to promote independence among older individuals and thereby reduce pressure on the healthcare system.9 This growing interest has stimulated numerous health and social care providers in the Netherlands to integrate reablement into their daily practices. However, there is ambiguity regarding the definition of reablement and how it relates to usual care practices, with many organizations left to navigate its implementation without clear guidance. An operational definition is needed that not only fits the Dutch health and social care system but also refines and build upon existing definitions of reablement. This study progresses the original conceptual definition by incorporating context-specific elements and drawing input from relevant stakeholders. By doing so, it aims to create a more practical and context-sensitive definition, offering clearer guidance for real-world application. The term “operational definition” in this study refers to guidance for policy and practice that extends beyond a conceptual definition, outlining the operationalization of reablement in practice in terms of its target group, aims, type of care or support, and characteristics. We aimed to develop an operational reablement definition by incorporating the perspectives of various stakeholders across practice, policy, and research.
Methods
Study Design
We conducted a modified Delphi study. It deviated from the traditional Delphi method by incorporating additional elements alongside the expert panel, such as the scientific literature and stakeholder input, obtained through open-ended questions.10 The Delphi technique is used to identify the collective opinion of experts and to detect agreement.11 In our Delphi study, three rounds of expert panel meetings and three Delphi survey rounds were conducted between April 2024 and September 2024 following the recommendations for Conducting and Reporting of Delphi Studies (CREDES) to increase robustness.12
Participants and Recruitment
Expert Panel
Purposive sampling13 was used to invite stakeholders to form an expert panel, to provide informed opinions and insights on reablement based on their experiences. The experts were selected based on their expertise in reablement, covering health and social care professionals. Recruitment was conducted through the Dutch reablement network, ensuring the inclusion of professionals from organizations considered frontrunners in reablement implementation. This included four project leaders, a policy advisor for the municipality, members of reablement teams (ie, occupational therapist, physiotherapist, community nurse, and a district linking pin), as well as representatives of clients and informal caregivers. This approach aimed to ensure a panel with relevant knowledge and practical experience in diverse settings with diverse backgrounds.
Survey Participants
Online surveys were used in all three Delphi rounds. For these online survey rounds, a large group of stakeholders across the Netherlands was recruited through word of mouth, email, and social media. This large group included a mix of stakeholders and the members of the expert panel, comprising all individuals involved in reablement or those who have experienced it firsthand – such as clients, informal caregivers, social workers, nursing staff, therapists, management, educators, researchers, and others – without any specific eligibility criteria.
Before the start of the study, all participants were provided an information letter, that stated the study’s background, objectives, and participation information. Informed consent was obtained prior to the start of the study, including publication of anonymized responses/direct quotes.
Data Collection
The surveys were conducted using the online survey program Qualtrics14 Background information such as gender, age, education, job title, primary field of work, work area, working experience, experience with reablement, and knowledge of reablement was collected from all participants. The research team, consisting of the authors LB, IM, SZ, SV, TS, and SM, was responsible for all aspects of the Delphi process, including preparation, execution, analysis, and reporting of the study. Figure 1 shows an overview of the steps of the Delphi process including an overview of the total number of respondents per round.
 |
Figure 1 The modified Delphi process consisting of three online Delphi rounds and three expert panel meetings. |
Expert Round 1 (April - May 2024)
A literature search was conducted to gather existing descriptions of reablement from scientific papers. Drawing on the international conceptual definition by Metzelthin et al3 the research team identified statements related to the target group, aims, characteristics, and components of reablement. These were used to create a preliminary set of statements. Then, an online survey was conducted with the expert panel, who were asked to generate statements about the target group, aims, characteristics, and components of reablement through open-ended questions, without prior knowledge of the literature-based statements. The research team incorporated the experts’ contributions and the findings from the scientific papers and the international Delphi study to refine the statements. The resulting first survey was divided into four sections – target group, aims, type of care or support, and characteristics. The expert panel subsequently reviewed these statements, offering feedback and suggestions. The research team discussed all the feedback, which included recommendations on survey structure, language use, and the inclusion of examples. The final version of the survey included 80 statements.
Delphi Round 1 (May – June 2024)
In the first survey, the participants were asked to evaluate the 80 statements using a nine-point Likert scale, where higher scores corresponded to greater agreement on that the statement was relevant to the question (see Figure 2). The participants were encouraged to suggest additional statements if they felt important topics were missing and were able to respond to the statements through open-ended questions. These additional comments were thoroughly reviewed by two members of the research team (LB and SM). They were subsequently used in round 2 to rephrase and refine specific statements and text and were also incorporated into discussions with the expert panel during round 2. Statements with any ambiguity were reassessed in the subsequent round.
 |
Figure 2 Sample survey questions for the target group prompted the participants to provide their responses based on their ideal scenario for reablement in practice. |
Delphi Round 2 (June – July 2024)
All participants from round 1 were invited for round 2. Two reminders were sent to increase the response rate. The adapted survey included additional statements as suggested by the participants in round 1. In addition, the statements with ambiguity from the first survey were evaluated using a binary response option (include versus do not include in the definition).
After collecting all the responses, the research team created a draft of the definition based on the statements. The text was divided into sections on the aims, target group, the individual’s needs, and characteristics of reablement.
Expert Round 2 (July 2024)
The draft was presented to the expert panel, who provided feedback during a two-hour online meeting led by two members of the research team (LB and SM). During the meeting, the panel was divided into two groups. Each group reviewed the text sections of the definition to refine nuances and to ensure the precision of the wording and terminology used. Notes were taken by the researchers. After both groups had discussed the definition, they reconvened and shared their findings with the other group. During each step, the panel members were allowed to provide clarifications, add nuances, and make further contributions. The outcomes were collectively reviewed afterwards.
The draft was subsequently revised and refined by the research team based on the suggestions of the expert panel. Within the research team, agreement was also sought regarding the use of certain terms or concepts and keeping all of the participants’ suggestions in mind.
Delphi Round 3 (July – September 2024)
In the third round, the refined definition was shared with the participants form Delphi rounds 1 and 2. They were invited to indicate their agreement with the proposed definition or to suggest any modifications if they did not agree. Two reminders were sent to increase the response rate. After collecting all the responses, the research team revised the draft of the definition based on the feedback received. The, the revised draft was shared with the expert panel via email, allowing them to offer any final comments. These were incorporated into the document, resulting in the final version.
Data Analysis
All analyses were performed using SPSS Statistics version 28.0.1.1.15 Descriptive statistics were used to analyze the background characteristics of the participants (ie, frequencies, percentages, means, and standard deviations [SDs]). For the questions employing the Likert-scale in Delphi rounds 1 and 2, median scores and inter-quartile ranges (IQR) were used to assess relevance and the level of consensus, respectively. Statements were deemed relevant if they achieved a median score of 7–9 and an IQR of ≤2.16 Statements with a median score of 1–3 and an IQR of ≥2 were considered to be less relevant and lacking consensus and were subsequently excluded.16 The remaining statements were considered uncertain. For questions employing a binary response option (include versus do not include in the definition, agree versus disagree with the definition draft), a threshold of 75% was established to determine agreement.12 This threshold was chosen based on established Delphi methodology in healthcare research, balancing inclusivity with methodological rigor.17 Responses were not weighted by experience or primary field of work; all panel members’ inputs were equally considered to ensure broad representativeness.
The notes taken during various steps of the process were reviewed and discussed by the research team, and then thematically summarized to identify key messages and insights. In addition, to capture changes in expert opinion and identify evolving themes, qualitative analysis was applied to responses, key insights were reviewed by the research team. This allowed us to capture and interpret significant topics and themes, providing a deeper understanding of the data evolving consensus on the definition, particularly given the challenges of direct statistical comparisons across rounds in Delphi studies.18
Ethical Considerations
The study was reviewed and approved by the Faculty of Health, Medicine & Life Sciences (FHML) Research Ethics Committee of Maastricht University in the Netherlands, under approval number FHML-REC/2024/014. The study was not subject to the Dutch Medical Research Involving Human Subjects Act (WMO). All participants received information about the study’s purposes, provided informed consent, and had the right to withdraw from the study at any moment. All data were pseudo-anonymized and stored on the research server of Maastricht University and only accessible to the members of the research team.
Results
In total, 139 participants across the Netherlands participated in round 1 of the Delphi study; of these, 105 (75.5%) participated in round 2, and 108 (77.6%) participated in round 3. An overview of the participants’ background information is presented in Table 1. Of the participants, 81.3% were primarily employed in healthcare, 7.2% within social care, 4.3% in education or research, and 7.2% in other sectors (eg, health insurer, client, and caregiver representatives). Additionally, 37.4% held management-related positions (eg, manager, policy advisor, project leader), while 54% were practitioners within health and social care (eg, registered nurses, occupational therapists, and social workers). The participants had an average of 8.3 years (SD 7.8) of work experience in their current occupation, an average of 2.8 years (SD 4.2) of experience with reablement and self-rated their knowledge of reablement with an average 7.1 out of 10 (SD 1.5).
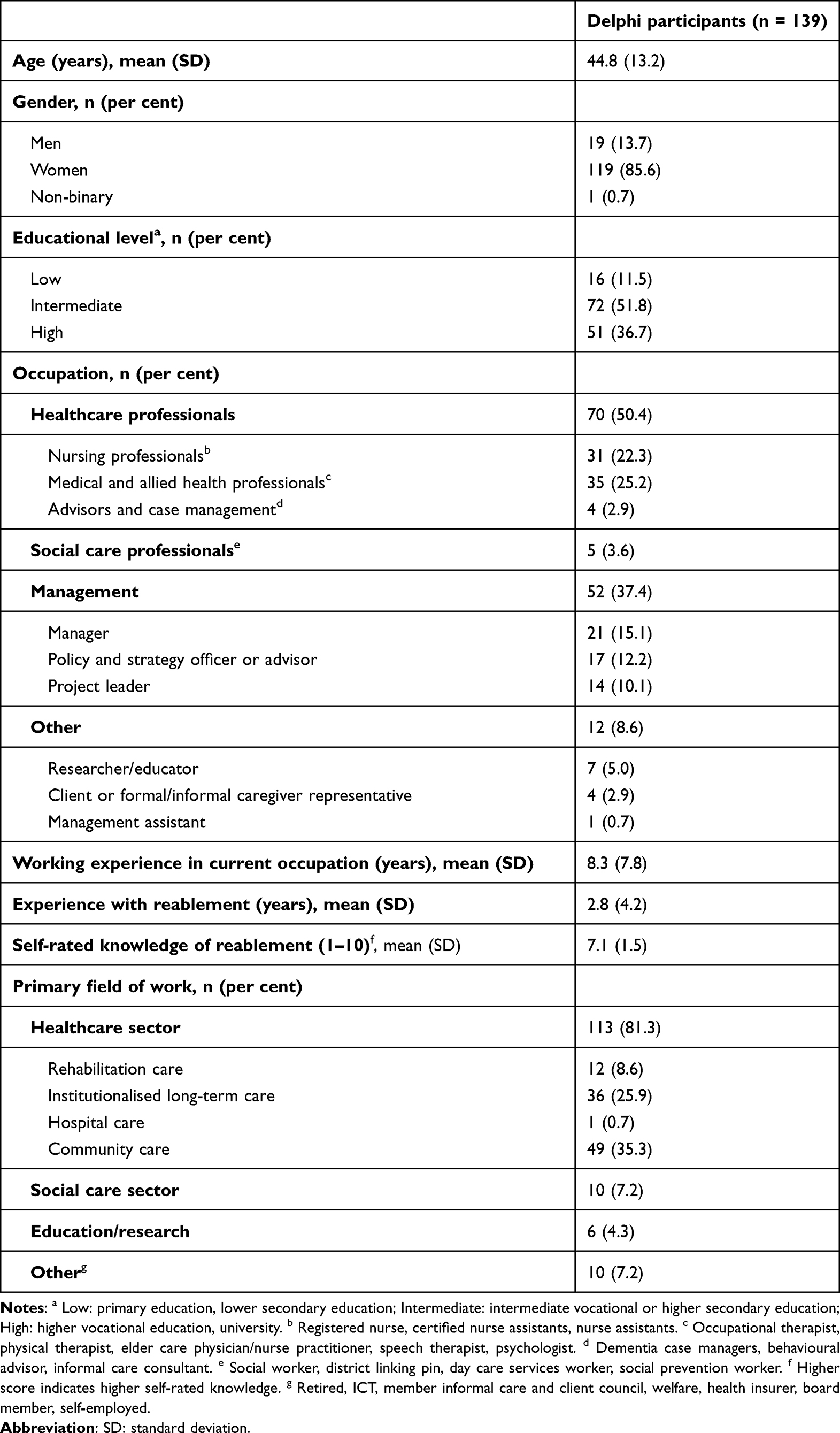 |
Table 1 Background Information of the Participants (n = 139) |
In the following sections, we present the findings and participant discussions for each part of the definition on reablement (ie, the target group, aims, type of care or support needed, and characteristics) and present the final phrasing of each section. Figure 3 shows the proportion of statements related to each part of the definition that did or did not reach agreement in the Delphi rounds. A scoring summary of all statements of Delphi rounds 1 and 2 is provided in Appendix 1.
 |
Figure 3 Proportion of statements related to each section of the definition that did or did not reach agreement after rounds 1 and 2 of the Delphi study. The numbers indicate the number of statements. |
Target Group
Delphi Rounds
In round 1, six target group–related statements were identified as relevant. Five were rated as uncertain (median score 6–7, IQR ≥2: prognosis, cognitive functioning, psychological functioning, learning ability, and motivation) and re-evaluated in round 2 (see Appendix 1). Agreement was reached for “cognitive functioning” (75.2%), while the other four were excluded. The participants also suggested two new statements (“cultural background/ethnicity” and “social support availability”), both of which were included after round 2 scoring. Feedback from open-ended questions during round 1 highlighted nuances, such as using the term “diagnosis” and addressing both the individual and their family:
The individual and their family are the center of the treatment, and everything revolves around them. – Participant survey, round 1
Expert Panel Rounds
During each expert panel meeting in round 2, the target group for reablement was a key focus. Stakeholder suggestions were discussed alongside considerations about the intended population and the optimal wording to describe them. While the panel explored the characteristics of an ideal target group, the experts found it challenging to define this group precisely, resulting in a lack of clear criteria. They noted that eligibility is often determined by a combination of factors:
Reablement is fundamentally always an option. It often involves a combination of factors that may render reablement no longer feasible; a single factor does not provide sufficient information on the matter. – Client and informal caregiver representative
In round 2, the expert panel discussed the term “care avoiders”, deeming it inappropriate as it relates more to willingness to engage with reablement. They emphasised that this group requires a different approach and excluded it from the definition. The panel also stressed the importance of considering individuals and their social network as a unit in the definition. They noted that learning ability should not determine eligibility for reablement if the social network can provide support. Additionally, they emphasised that reablement requires the target group to identify a specific goal or support need, recommending this be included under characteristics. Motivation, viewed as a defining factor for the success of reablement, was included in the definition under the type of care or support needed.
Final Definition of the Target Group
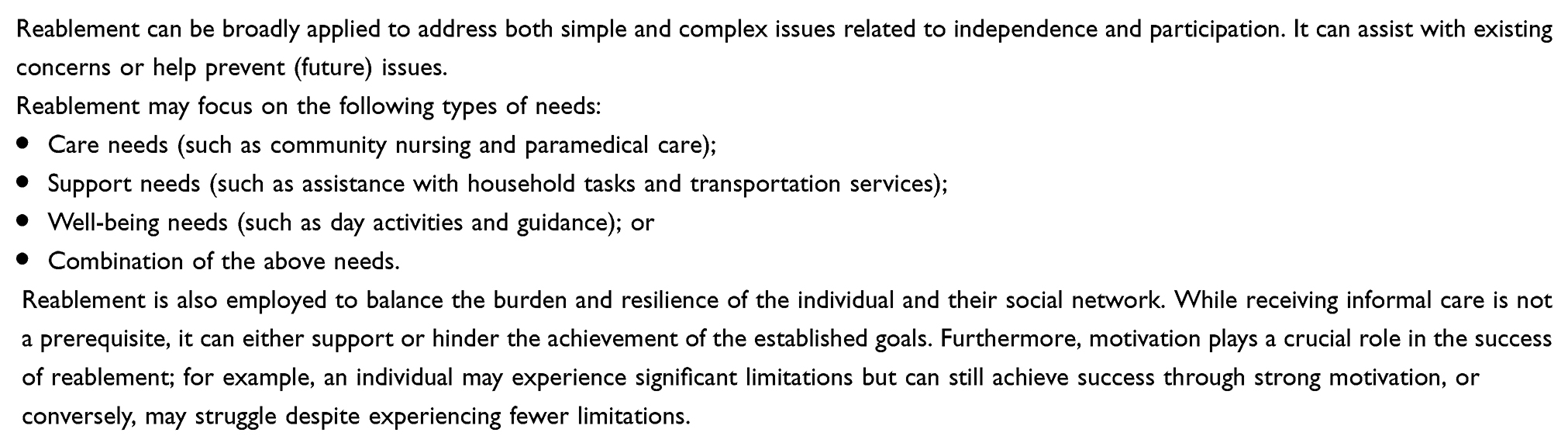
The final text regarding the target group, as agreed upon following the surveys and expert panel meetings, is shown in Box 1.
 |
Box 1 Final Definition Text for the Target Group for Reablement in the Netherlands |
Aims
Delphi Rounds
In round 1, 22 statements related to the aims were identified as relevant to the definition. Three were rated as uncertain (median score 5–8, IQR ≥3: “reducing health and social care costs”, “facilitating discussions about the future”, and “enhancing informal caregivers’ confidence”) and re-evaluated in round 2 (see Appendix 1). Agreement was reached for including “facilitating discussions about the future” (86.7%) and “enhancing informal caregivers’ confidence” (79.0%), while the remaining uncertain statement was excluded. The participants in round 1 suggested a new statement – “deploying professional assistance where it is most needed” – but it was not included after round 2 scoring. Feedback from open-ended questions in round 1 offered further suggestions, such as removing certain statements or clarifying nuances. For example, some participants found the statement “reducing health and social care costs” to be framed too negatively and noted that some questions were difficult to assess.
I find it somewhat challenging to fill in. For example, I don’t think the goal is to relieve either professional care or family members, but that this can be a beneficial side effect. – Participant, round 1
Expert Panel Rounds
During the expert panel meetings, stakeholder suggestions were reviewed alongside considerations regarding the aims, focusing primarily on the precise wording of statements and the final text. For example, “participation” was revised to “social and community participation”. Some phrases were found to be too negative or insufficiently precise and were adjusted in consultation with the panel across all three rounds. The experts highlighted that the initial draft in round 2 did not sufficiently differentiate reablement from usual care in its aims. This was addressed in the final version, emphasizing the importance of focusing on meaningful activities, relationships, and participation, among other changes. The expert panel also stressed the importance of the social network and social care, noting that early drafts in round 2 were predominantly oriented towards health care, leaving these aspects underrepresented. Furthermore, they indicated the significance of prevention as a key component of reablement, recommending its explicit inclusion in the definition. These adjustments were incorporated into the aims and integrated across other sections of the text.
Final Definition of the Aims of Reablement
The final text regarding the aims, as agreed upon following the surveys and expert panel meetings, is shown in Box 2.
 |
Box 2 Final Definition Text for the Aims of Reablement in the Netherlands |
Type of Care or Support Needed
Delphi Rounds
In round 1, ten statements regarding the type of care or support needed were deemed to be relevant to the definition. Two statements – related to “care avoiders” and “acute needs” – were rated as uncertain (median score 6–7, IQR =3) and re-evaluated in round 2 (see Appendix 1). Both were ultimately scored not relevant for inclusion by 60.0% and 67.6% of participants, respectively. Additionally, a new statement suggested in round 1 – concerning short-term residence in institutions such as hospitals, care homes, or rehabilitation centers – was included following round 2 scoring. During round 1, a participant provided feedback on the type of care or support needed, indicating that they did not give maximum scores on the Likert scale because it strongly depends on the implementation of reablement.
It [regarding the type of need for which reablement is implemented] strongly depends on how reablement is implemented. I believe that some needs do not necessarily require an interdisciplinary team with various healthcare professionals, as that might be excessive. – Participant, round 1
Expert Panel Rounds
During the expert panel meetings, stakeholder suggestions were reviewed alongside considerations about the type of care and support needed. Discussions also focused on refining the wording of specific statements and the final text, including examples related to “support needs”, “well-being needs”, and “preventive needs”. A key topic in round 2 was identifying the types of needs suitable for reablement, although no clear consensus emerged. For example, there was debate about whether reablement is only appropriate for complex needs and how such needs should be classified as complex. The panel also discussed the roles of individuals and their social networks, concluding that while individuals should lead the process, their networks – often overburdened – must be considered as well. This reinforced the view that individuals and informal caregivers should be regarded as a unit. The panel emphasised that reablement must integrate the perspectives of both individuals and their informal caregivers. To reflect this, adjustments were made across multiple sections of the text in rounds 2 and 3 to ensure this emphasis was clearly conveyed in the final definition.
Final Definition of Type of Care
The final text regarding the type of care or support needed, as agreed upon following the surveys and expert panel meetings, is shown in Box 3.
 |
Box 3 Final Definition Text for the Type of Care or Support Needs Eligible for Reablement in the Netherlands |
Characteristics
Delphi Rounds
In round 1, 22 statements about the characteristics of reablement were deemed relevant to the definition. Nine statements were rated as uncertain (median score 4–8, IQR ≥3), including those addressing the programme’s end, the core team, and the role of the individual and their social network, and were re-evaluated in round 2 (see Appendix 1). Four statements – “it stops when the individual’s goals have been achieved”, “a coordinator is designated within the core team”, “the individual is part of the core team”, and “the individual appoints someone from their social network to be part of the core team” – were deemed relevant for inclusion, while the other five were excluded. In round 1, the participants also suggested four new statements related to characteristics: “it can be monodisciplinary”, “the core team specifies which expertise is needed to achieve the goals”, “the individual takes on a coordinating role (possibly with professional support)”, and “the informal caregiver takes on a coordinating role (possibly with professional support)”, as well as “the individual is monitored even after goal attainment”. Among these, only “the core team specifies which expertise is needed to achieve the goals” was included following round 2 scoring. Feedback from the open-ended questions during round 1 raised questions about who should hold the coordinating role within the core team. Additionally, one participant highlighted the importance of regular evaluations with the individual to ensure sustained results.
A key component of the program is that after achieving the goals, there should be monthly check-ins to assess progress, with evaluation, adjustment, and follow-up being essential. After all, circumstances in the individual’s life and their environment are always changing. Restarting the process does not seem like a viable option. Someone from social care must remain closely involved, with a clear mandate for observation. – Participant, round 1
Expert Panel Rounds
During the expert panel meetings, stakeholder suggestions from each round were reviewed, with particular attention to the wording of specific statements and the final text (eg, “behavior change” can have a negative connotation). In round 2, discussions focused on the operationalization of reablement and the characteristics essential for its implementation. The experts highlighted the importance of a comprehensive intake process that accounts for well-being and participation. They also stressed the significance of involving the individual as the owner of the process and aligning interventions with the individual’s capabilities. The panel also discussed the value of providing tailored care and support, noting that achieving reablement goals does not always require a large, multidisciplinary team. These considerations were incorporated into the final text, with adjustments made in rounds 2 and 3 to ensure these principles were clearly reflected.
Final Definition of the Characteristics of the Approach
The final text regarding the characteristics, as agreed upon following the surveys and expert panel meetings, is shown in Box 4.
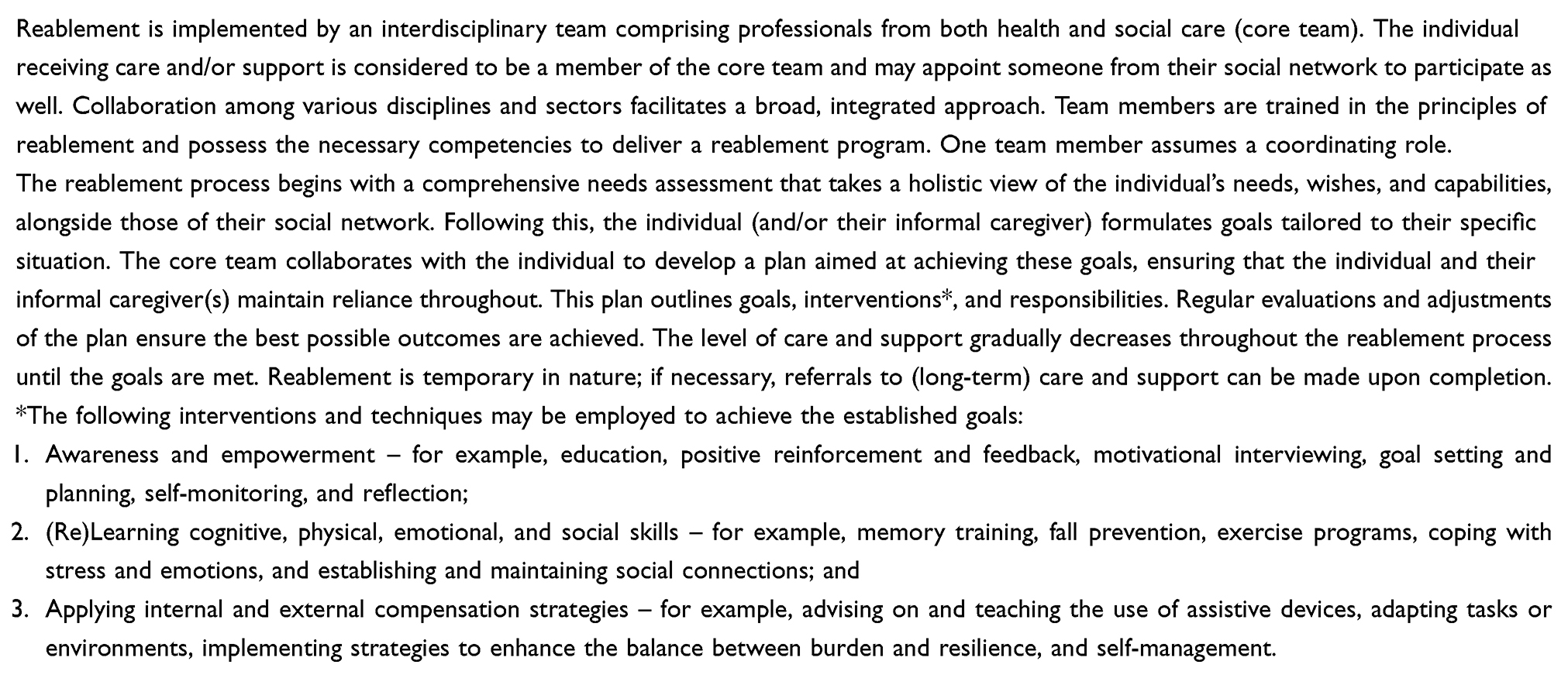 |
Box 4 Final Definition Text for the Characteristics of Reablement in the Netherlands |
Refining the Definition
After drafting the initial complete definition text, 88 (81.5%) of the 108 participants in round 3 agreed with the first draft (see Appendix 2). The 20 participants (18.5%) who did not agree with the definition were given the chance to refine the text. Their comments addressed aspects such as language use, the rationale, and the focus of reablement. Table 2 provides details on the suggestions made and how they were incorporated into the final version of the text.
 |
Table 2 Comments Given by Participants During Delphi Round 3 That Led to Adjustments in the Definition |
Some experts’ feedback focused more on the reablement mindset rather than the specific content of reablement as a program. Additional suggestions led to a restructuring of the text to improve the readability. After the research team revised the text, it was forwarded to the expert panel for a final review. Three experts provided additional remarks, primarily focused on readability and word choice (eg, “needs assessment” instead of “intake”, with one expert suggesting the addition of more examples to improve operationalization). In response, the research team further refined the text to ensure a more concise and polished formulation, resulting in the final definition presented in Appendix 3.
Discussion
The expert and Delphi rounds led to the development of the operational definition of reablement in the Netherlands presented in Appendix 3, which was agreed upon by 81.5% of the stakeholders. The key discussions focused on the target group, such as the importance of involving individuals and their families, and the characteristics of reablement, including the coordinating role, team composition, and size.
The operational definition closely aligns with the international definition by Metzelthin et al3 when considering the scope and focus of both definitions. While international definitions of reablement often emphasize short-term, goal-oriented support aimed at improving independence in daily functioning,19–21 the Dutch definition distinguishes itself by offering more detailed and practical guidance on the implementation of elements such as areas of application and interventions that can be used to reach the clients’ goals. Notably, in line with the international definition3 no specific target group was identified, highlighting the broad applicability of the approach. Moreover, the Dutch definition particularly focuses on social participation and connection, expanding its focus beyond independence to the individual’s social network and well-being. This reflects a move from individual autonomy to “meaningful functioning”, offering a more holistic and person-centred interpretation of goals. This aligns with trends in Dutch healthcare that focus on integrated care, prevention, and person-centered approaches to support older adults in living fulfilling, independent lives while participating in society.9,22 The focus on social connectedness and participation further positions the Dutch reablement definition as especially relevant within today’s policy context, reflecting a shift towards more holistic care that integrates formal services with community and social support to enhance overall well-being and resilience. These trends highlight that care-related challenges do not always need to be solved solely through formal care; they can also be addressed through social care and the support of the individual’s social network. The evolution of the concept and operationalization of reablement towards the social domain and well-being is evident globally, as seen in the development of reablement practices over time. Initially, reablement was more focused on functional recovery from a biomedical perspective – for example, “reabling” individuals back to work – and often aimed at specific conditions such as arthritis or cerebral palsy.23 However, over the years, the importance of social care and overall well-being has emerged more often in the reablement literature. This is not surprising, given the shifts in broader perspectives on health throughout the world, such as the World Health Organization’s concept of “Healthy Ageing”.24 Healthy Ageing is defined as the process of promoting and preserving functional ability to support well-being in later life. It focuses on enhancing an individual’s capacity to engage in activities that are meaningful to them, enabling them to “be” and “do” what they value.24
Our data also revealed a distinction between reablement as a mindset and reablement as an intervention, with the participants discussing that fostering this reablement mindset is a prerequisite for successful implementation of the intervention. The distinction between mindset and intervention has also emerged within the reablement literature, with Metzelthin et al25 also making a distinction between grounded service models and time-limited intervention programs in reablement principles. They argued that reablement service models aim to build capacity and foster environments enabling professionals to assist individuals in engaging in meaningful activities, thereby cultivating a reablement mindset rather than delivering time-limited interdisciplinary reablement interventions. This distinction influences the intended recipients and providers of reablement – for example, in how providers are trained, or services are structured, it reflects a move from “doing reablement” as a programmatic intervention to “being reablement” as a holistic, integrated approach within care systems. Moreover, Vluggen et al26 highlighted the importance of first cultivating the right mindset before implementing the program with clients. Attempting to implement the program without focusing on the right mindset risks reducing it to a mere checklist, where the core principles of reablement are not fully realized. Conversely, focusing only on mindset without offering adequate descriptions and guides of the approach for its implementation and sustainability may fail to achieve lasting change.
Our study presents several important insights with implications for both practice and research. First, while the operational definition provides a guide outlining the operationalization of reablement in practice, it does not provide information on how it relates to existing forms of care, which is necessary to clarify reablement’s value and to receive the necessary resources and support to implement reablement into standard care. To achieve this, it is important to compare reablement with existing interventions such as traditional home care or outpatient rehabilitation. One example of how this comparison can be made is through patient journeys, which could illustrate key differences in outcomes and approaches.27 This comparison can highlight both the differences and similarities, helping to clarify reablement’s value and its potential to become part of standard care. Second, while the conceptual international definition helps to anchor what reablement is in a broad, theoretical sense, the operational definition describes reablement in practice by outlining specific actions, interventions, and processes. Together, these definitions offer both a theoretical understanding of reablement and practical guidance for its application. For policymakers, these definitions ensure consistent and clear guidance that can support the creation of policy aligned with the principles of reablement. For practitioners, they provide a tangible structure for defining roles, responsibilities, and measurable outcomes, helping to translate theory into effective practice. For example, the definition can inform the development of outcome sets aligned with core reablement goals—such as meaningful functioning, social participation, and self-efficacy in daily activities—measured through validated instruments and narrative tools. It may also guide the selection of process indicators, including goal-setting quality, interdisciplinary collaboration, and client involvement, to assess feasibility and implementation. Third, the results of our study suggest that future reablement research should focus on outcomes related to well-being and social connectedness, as these areas are underexplored to capture the benefits of reablement and are often emerging themes in qualitative research.28 This could provide a valuable addition to the existing outcome measures used within reablement, as there are often doubts as to whether these measures fully capture the impact of reablement.29 Fourth, a critical consideration for future studies is to evaluate the real-world applicability of the definition across different healthcare settings. Qualitative research could assess how well the Dutch definition translates to different contexts and its level of adoption in practice. Our study provides a valuable example for other countries facing difficulties in aligning reablement practices due to conceptual ambiguity arising from varying interpretations. Our study can offer a blueprint for countries looking to develop their own context-sensitive definition, allowing them to view it through their own lens and take cultural differences and variations in healthcare systems into account. By systematically engaging diverse stakeholders – for example, through the Delphi method – it is possible to generate context-sensitive insights into reablement’s goals, target group, core characteristics, and interventions. This process can help to bridge gaps in understanding and align practices with the broader philosophy of reablement. In doing so, it strengthens the foundation for effective implementation, collaboration, and robust evaluation of reablement services.
A major strength of our study is its robustness: we followed the CREDES guidelines for conducting and reporting our research.12 Additionally, the Delphi methodology allowed for an iterative process to continuously refine and clarify the definition, incorporating data triangulation through expert and survey input to ensure a well-considered outcome. By engaging with a large group of stakeholders, we enhanced the applicability and relevance of our findings. The Delphi approach also ensured the definition was sensitive to the specific cultural and contextual aspects of the Dutch healthcare system. However, our study is also subject to certain limitations. For example, selection bias may have occurred, as most participants were from the healthcare sector and had a higher education, with a relatively small number from social care and those with lower levels of education. Consequently, the recommendations and conclusions drawn from the study might be less applicable or generalizable to these underrepresented populations and may not produce the same results in a in a future study with a comparable sample. Finally, reablement is a relatively new concept in the Netherlands, as confirmed by the average of 2.8 years of experience reported by participants. This may have affected the depth of understanding and the overall generalizability of our findings, as reablement does not have an established standard in the Dutch healthcare system.
Conclusions
In conclusion, our study developed an operational definition of reablement in the Dutch healthcare context using the modified Delphi methodology. This approach proved to be a valuable tool for identifying context-specific elements and incorporating the experiences of experts, facilitating the creation of operational definitions that are both culturally and contextually sensitive. The developed definition serves as a guide for operationalizing reablement in practice, extending beyond a conceptual definition to offer concrete, actionable guidance. By engaging with a diverse group of experts, we sought to capture context-specific insights that could clarify key characteristics and offer practical guidance for its implementation. Future research should examine the adoption of the definition, assess its applicability across diverse healthcare settings, and identify barriers to its widespread implementation. Despite some limitations, the definition may contribute to both the theoretical and practical understanding of reablement. It could serve as a foundation for further research and policy development, helping to standardize and support the integration of reablement in the Netherlands and provide an example for other countries aiming to develop context-sensitive definitions.
Abbreviations
CREDES, Conducting and Reporting of Delphi Studies;12 SD, Standard deviation; IQR, Inter-quartile range.
Data Sharing Statement
The data supporting the findings of this study are available upon request from the corresponding author.
Acknowledgments
We thank all experts for their participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Dutch Organization for knowledge and innovation in health, healthcare, and well-being (ZonMw): 10830022310002.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lee R, Mason A. Cost of aging. Fin Dev. 2017;54(1):7–9.
2. Rostgaard T, Parsons J, Tuntland H. Reablement in Long-Term Care for Older People: International Perspectives and Future Directions. Policy Press; 2023:248.
3. Metzelthin SF, Rostgaard T, Parsons M, Burton E. Development of an internationally accepted definition of reablement: a Delphi study. Ageing Soc. 2022;42(3):703–718. doi:10.1017/S0144686x20000999
4. Parsons J, Burton E, Graff L, Metzelthin SF, O’Connell H, Tuntland HK. Reablement as an evolution in home care: a comparison of implementation across five countries. In: Rostgaard T, Parsons J, Tuntland H, editors. Reablement in Long-Term Care for Older People: International Perspectives and Future Directions. Policy Press; 2023:68–92:chap4.
5. ReAble Network. Reablement or restorative home support | ReAble Network; 2024,
6. Parsons J, Tuntland HK, Nelson M, Westendorp RG, Rostgaard T. A cross-country reflection on empirical and theoretical learnings, challenges, and the way forward for reablement. In: Rostgaard T, Parsons J, Tuntland H, editors. Reablement in Long-Term Care for Older People: International Perspectives and Future Directions. Policy Press; 2023:238–247:chap11.
7. Rooijackers TH. Supporting older adults to STAY ACTIVE AT HOME: Process, Effect and Economic Evaluation of a Reablement Training Program for Homecare Staff [PhD dissertation]. Maastricht University; 2022.
8. Mouchaers I. Managing Everyday Life: Exploring the Essential Components of Reablement and User Experiences [PhD dissertation]. Maastricht University and KU Leuven; 2024.
9. Programma Wonen, Ondersteuning en Zorg voor Ouderen (WOZO) (Ministerie van Volksgezondheid, Welzijn en Sport); 2022.
10. Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. 2021;11(4):116–129. doi:10.5662/wjm.v11.i4.116
11. Fitch K, Bernstein SJ, Aguilar MD, et al. The RAND/UCLA Appropriateness Method User’s Manual. RAND Corporation; 2001.
12. Jünger S, Payne S, Brine J, Radbruch L, Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684–706. doi:10.1177/0269216317690685
13. Etikan I. Comparison of convenience sampling and purposive sampling. Am J Theoretic Appl Stat. 2016;5(1):1. doi:10.11648/j.ajtas.20160501.11
14. Qualtrics XM. Version April-September, 2024. Qualtrics; 2024. Available from: https://www.qualtrics.com/.
15. IBM SPSS Statistics for Windows. Version 28.0.1.1. IBM Corp; 2021.
16. Jünger S, Payne S, Brearley S, Ploenes V, Radbruch L. Consensus building in palliative care: a Europe-wide Delphi study on common understandings and conceptual differences. J Pain Symptom Manage. 2012;44(2):192–205. doi:10.1016/j.jpainsymman.2011.09.009
17. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
18. von der Gracht HA. Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc Change. 2012;79(8):1525–1536. doi:10.1016/j.techfore.2012.04.013
19. Aspinal F, Glasby J, Rostgaard T, Tuntland H, Westendorp RG. New horizons: reablement - supporting older people towards Independence. Age Ageing. 2016;45(5):572–576. doi:10.1093/ageing/afw094
20. Doh D, Smith R, Gevers P. Reviewing the reablement approach to caring for older people. Ageing Soc. 2019;40(6):1371–1383. doi:10.1017/s0144686x18001770
21. Sims-Gould J, Tong CE, Wallis-Mayer L, Ashe MC. Reablement, reactivation, rehabilitation and restorative interventions with older adults in receipt of home care: a systematic review. J Am Med Dir Assoc. 2017;18(8):653–663. doi:10.1016/j.jamda.2016.12.070
22. Ouder Worden 2040. Een transformatieagenda voor een ouder wordende samenleving. 2021:289. Available from: https://www.ouderworden2040.nl/wp-content/uploads/2021/05/Publicatie-Ouder-Worden-2040.pdf.
23. Clotworthy A, Kusumastuti S, Westendorp RGJ. Reablement through time and space: a scoping review of how the concept of ‘reablement’ for older people has been defined and operationalised. BMC Geriatr. 2021;21(1):61. doi:10.1186/s12877-020-01958-1
24. Beard JR, Officer A, de Carvalho IA, et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387(10033):2145–2154. doi:10.1016/s0140-6736(15)00516-4
25. Metzelthin SF, Thuesen J, Tuntland H, et al. Embracing reablement as an essential support approach for dementia care in the 21st century: a position paper. J Multidisciplin Healthcare. 2024;17:5583–5591. doi:10.2147/jmdh.S484069
26. Vluggen S, Heinen M, Metzelthin S, Huisman-de Waal G, Bleijlevens M, de Lange W. Lessons Learned and implications of function focused care based programs of various nursing care settings: a thematic synthesis. Ann Nurs Res Pract. 2021;6(2).
27. Davies EL, Pollock D, Graham A, et al. Reporting of patient journey mapping in current literature: a scoping review protocol. JBI Evidence Synth. 2022;20(5):1361–1368. doi:10.11124/jbies-21-00226
28. Mulquiny L, Oakman J. Exploring the experience of reablement: a systematic review and qualitative evidence synthesis of older people’s and carers’ views. Health Soc Care Commun. 2022;30(5):e1471–e1483. doi:10.1111/hsc.13837
29. Lewin G, Parsons J, O’Connell H, Metzelthin S. Does reablement improve client-level outcomes of participants? An investigation of the current evidence. In: Rostgaard T, Parsons J, Tuntland H, editors. Reablement in Long-Term Care for Older People. Policy Press; 2023:93–117:chap5.
 © 2025 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2025 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Recommended articles
Exploring Goal-Setting and Achievement Within Reablement: A Comparative Case Study of Three Countries
Buma LE, Tuntland H, Parsons M, Zwakhalen S, Metzelthin SF
Journal of Multidisciplinary Healthcare 2024, 17:1203-1218
Published Date: 19 March 2024