")
Back to Journals » Clinical Ophthalmology » Volume 19
Demographic and Clinical Factors Associated with Mechanisms of Open Globe Injury in the United States: A Multi-Center Study
Authors Anant S , Casella A, Greenfield JA , Miller SC , Wang KY, Momenaei B, Lee K, Mansour HA, Justin GA , Makhoul KG, Bitar RA, Lorch A, Armstrong GW , Wakabayashi T, Yonekawa Y, Cavuoto KM, Woreta F
Received 19 February 2025
Accepted for publication 28 April 2025
Published 8 May 2025 Volume 2025:19 Pages 1543—1556
DOI https://doi.org/10.2147/OPTH.S520082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shruti Anant,1 Alicia Casella,2 Jason A Greenfield,2 Sarah C Miller,1 Kristine Y Wang,3 Bita Momenaei,3 Karen Lee,3 Hana A Mansour,3 Grant A Justin,4 Kevin G Makhoul,5 Racquel A Bitar,5 Alice Lorch,5 Grayson W Armstrong,5 Taku Wakabayashi,3 Yoshihiro Yonekawa,3 Kara M Cavuoto,2 Fasika Woreta1
1Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Bascom Palmer Eye Institute, University of Miami School of Medicine, Miami, FL, USA; 3Wills Eye Hospital, Thomas Jefferson University, Philadelphia, PA, USA; 4Duke Eye Center, Duke University School of Medicine, Durham, NC, USA; 5Massachusetts Eye and Ear, Harvard Medical School, Boston, MA, USA
Correspondence: Shruti Anant, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 1800 Orleans St, Baltimore, MD, 21287, USA, Tel +1-703-389-3753, Email [email protected]
Purpose: We sought to examine the demographic and clinical risk factors associated with specific mechanisms of open globe injuries (OGIs) and identify predictors of Zone III injuries across multiple tertiary eye care centers.
Patients and methods: 1570 patients with OGIs presenting to the Wilmer Eye Institute, the Bascom Palmer Eye Institute, Massachusetts Eye and Ear, and Wills Eye Hospital between 2018– 2021 were retrospectively reviewed. Multinomial and binomial logistic regression models were used to evaluate associations between demographic and clinical risk factors with injury mechanisms and Zone III injuries.
Results: Among the study population (74.2% male, mean age 48.2 years), falls (21.3%), construction work (16.2%), and assaults (10.0%) were the most common injury mechanisms. Black patients had higher risk of assault-related OGIs (relative risk ratio [RRR], 6.41; 95% confidence interval [CI], 2.06– 19.93; p< 0.001) and elderly patients > 61 years showed increased risk for falls (RRR, 10.45; 95% CI, 2.22– 49.10; p=0.003). Eyelid laceration was significantly associated with assaults (RRR, 5.58; 95% CI, 1.59– 19.65; p=0.007) and falls (RRR, 4.81; 95% CI, 1.61– 14.34; p=0.005), while iris prolapse was associated with assaults (RRR, 3.23; 95% CI, 1.12– 9.32; p=0.03) and construction work injuries (RRR, 1.99; 95% CI, 1.12– 3.52; p=0.02). Zone III injuries were independently associated with eyelid laceration (prevalence ratio [PR], 1.62; 95% CI, 1.20– 2.18; p< 0.001), relative afferent pupillary defect (RAPD) (PR, 2.42; 95% CI, 1.71– 3.43; p< 0.001), and retrobulbar hemorrhage (PR, 2.77; 95% CI, 1.76– 4.36; p< 0.001).
Conclusion: This multi-institutional study identified distinct demographic risk profiles for different OGI mechanisms and clinical predictors of severe injuries. These findings suggest opportunities for targeted prevention strategies and may aid in early identification and triage of severe OGIs.
Plain Language Summary: Open globe injuries (OGIs), traumatic eye injuries that pierce through the eye wall, can lead to permanent vision loss if not treated quickly. Identifying which patient populations are most at risk for OGIs, and the specific factors that increased likelihood of injury, can guide more effective prevention and treatment efforts. Our study aimed to identify the common causes of OGIs and their risk factors by analyzing patient data from four major eye hospitals in the United States.
We reviewed the medical records of 1570 patients who presented to the hospital with OGIs. The most common causes of injury were falls, construction work, and assaults. Different populations faced different risks, such as: Black patients, who had a higher risk of assault-related injuries, and elderly individuals, especially women, who were more likely to be injured from falls. We found that lacerations of the eyelid were linked with assaults and falls, and iris prolapse (when the colored part of the eye is displaced) were linked to assaults and construction work injuries. Additionally, more severe injuries (Zone III injuries, which extend to the back of the eye) were associated with eyelid lacerations, changes in pupil response (relative afferent pupillary defect, or RAPD), and bleeding behind the eye (retrobulbar hemorrhage).
This study provides important insights into which demographic and clinical factors put patients at risk for different mechanisms of OGIs. Our findings may be used to help identify severe cases earlier and guide targeted prevention efforts.
Keywords: ocular trauma, epidemiology, demographics, etiology, prevention
Introduction
Over the past two decades, trauma to the eye has been identified as a leading cause of preventable vision loss.1–4 In the United States (US) alone, ocular trauma accounts for one-third of all eye-related emergency department visits.3
Open globe injuries (OGIs), a subset of ocular trauma, are full-thickness defects of the eyewall. Without timely surgical repair, OGIs can cause permanent vision loss. OGIs are classically categorized by type of injury into ruptures, caused by blunt trauma, and lacerations, caused by sharp trauma.5,6 OGIs can also be described by anatomical zone based on extent of injury, from Zone I (limited to the cornea and limbus) to Zone II (extending 5 millimeters [mm] posterior to the limbus) to Zone III (extending beyond 5 mm posterior to the limbus).5,7 The ocular trauma score (OTS) further stratifies OGIs based on injury characteristics, in order to predict visual outcomes and guide management strategies.5,6
The worldwide incidence of OGIs is estimated at 3.5 injuries per 100,000 people, with more than 203,000 cases occurring per year globally.4,8,9 Previous studies have reported on the epidemiology of OGIs. Overall, OGIs most commonly affect young, male patients, with a secondary peak in incidence among elderly individuals 70 years or older.9–11 Assaults, recreational accidents, and occupational work injuries are the most common causes of ocular trauma in younger patients, while falls are the major cause among elderly patients.12–15 Disparities in incidence, apart from age and gender, have also been noted: patients with lower socioeconomic status, patients with residence in the South and West of the US, Black patients, and Hispanic patients are all groups more likely experience OGIs.9,10,16–18
There, however, remains a gap in our knowledge of the demographic and clinical risk factors associated with specific mechanisms of OGIs, as well as risk factors associated with the most severe injuries. Such an understanding can help better characterize and triage OGI mechanisms, delineate mechanisms and exam findings that increase risk for the most severe injuries, and target prevention efforts toward demographics most at risk.
While previous work has reported important data on the epidemiology and demographics of OGIs, these data have been limited to single-center studies,15,19,20 or have used large inpatient databases based on sampling methods, such as the Nationwide Emergency Department Sample (NEDS) or National Inpatient Sample (NIS).9,16,21 One study leveraged the American Academy of Ophthalmology’s Intelligent Research (IRIS) Registry to study the incidence, risk factors, and visual outcomes of open globe repairs, but did not study all patients initially presenting with injury or include information on their mechanisms of injury.10
To our knowledge, there has not been a large, multi-institution retrospective study on the association between granular, clinically relevant OGI characteristics and their specific mechanisms and classifications of injury. In our three-year retrospective chart review of traumatic OGIs across four high-volume eye centers, we investigated (1) the demographic, clinical characteristics, and visual outcomes of open globes presenting to emergency departments in the United States, (2) assessed the demographic and clinical characteristics associated with elevated risk for the most commonly reported mechanisms of injury, and (3) examined the demographic and clinical variables associated with the outcome of Zone III injury.
Methods
Study Population
We conducted a retrospective cohort study using data from patients who presented with OGIs to emergency departments at four tertiary care eye centers: the Wilmer Eye Institute in Baltimore, Maryland, the Bascom Palmer Eye Institute in Miami, Florida, Mass Eye and Ear in Boston, Massachusetts, and Wills Eye Hospital in Philadelphia, Pennsylvania, between January 1st, 2018 and December 31st, 2021. The study was approved by the Institutional Review Boards (IRBs) of all four participating centers (Wilmer Eye Institute: IRB00132759; Bascom Palmer Eye Institute: IRB20200719; Mass Eye and Ear: IRBP002523; Wills Eye Hospital: IRB21E.828) and adheres to the tenets of the Declaration of Helsinki. A waiver of patient consent was granted to review medical records per IRB approval as this research involved no more than minimal risk to subjects. Patient data confidentiality was preserved by ensuring that only approved individuals collected data, and that data was accessed and stored only through secure storage avenues for research data.
Data Collection
All patients with an International Classification of Diseases, Tenth Revision (ICD-10) code for ocular lacerations and ruptures with or without prolapse or penetrating wounds of orbit with or without foreign body (ICD-10 codes: S05.2, S05.20, S05.21, S05.22, S05.3, S05.30, S05.31, S05.32, S05.4, S05.40, S05.41, S05.42, S05.5, S05.50, S05.51, S05.52, S05.6, S05.60, S05.61, S05.62) or a Current Procedural Terminology (CPT) code for open globe repair or intraocular foreign body (codes: 65235, 65,260, 65,265, 65,275, 65,280, 65,285, 65,286, 66,250, 67413) were initially queried from the electronic medical record (Supplement 1).
Inclusion criteria for eyes included in the study were eyes with a documented history of OGI (defined by ICD-10 or CPT codes).
Demographic and Clinical Characteristics
Eyes from patients meeting inclusion criteria were retrospectively reviewed for patient demographics (including age, sex, race, ethnicity, insurance status, and occupational status) and clinical characteristics (including laterality, mechanism of injury, place of injury, type of object, object material, open globe type, laceration type, zone of injury, concomitant injuries, time to surgery, surgical management, and visual acuity).
Sex, race, ethnicity, and insurance status were self-reported by patients in the medical record. Race included standard options of White, Black or African American, Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or “Other” race. Due to a minimal number of patients in categories other than White or Black race, all other reported race categories were condensed into the “Other” race categories for analysis purposes. Ethnicity included standard options of “Hispanic or Latino”, or “Not Hispanic or Latino”. Primary insurance status included standard options of private insurance, Medicaid, Medicare, on uninsured status.
Occupation was obtained from the medical record and grouped based on frequency into the following categories: construction work, industrial work, student, unemployed, or other occupation.
Reported mechanisms of injury were collected and categorized based on frequency into the following categories: assault, motor vehicle accident (MVA), fall, sports, firearms, construction work, or other causes. Visual acuity data was converted to logarithm of the minimum angle of resolution (logMAR) acuity for analysis. In cases where more than one zone of injury was involved, the classification of zone was based on the most posterior extent of the injury. Any demographic, clinical, or visual acuity characteristics not recorded in the medical record were identified and treated as missing observations for analysis purposes.
Demographic and clinical characteristics of the study population were summarized using means and standard deviations for continuous variables and proportions for categorical variables.
Statistical Analysis
Univariable and multivariable multinomial logistic regression models were used to analyze the associations between the most common mechanisms of OGI and demographic and clinical characteristics. Assumptions of the multinomial logistic regression model were verified, as follows. Categories of mechanism of injury were mutually exclusive and each observation was independent of other observations. Lack of multicollinearity between predictor variables was verified. To ensure adequate sample size for each combination of outcome variable categories and predictors, predictor variables with less than ten cases per variable per category were excluded from the model. Demographic and clinical predictor variables that were significant on univariable analysis were included in the final multivariable model.
Binomial logistic regression was used to analyze the relationship between Zone III injuries and demographic and clinical predictor variables. Predictor variables that were significant on univariable analysis were incorporated into a multivariable mode.
Statistical analysis was performed using Stata version 14 (StataCorp). One-tailed and two-tailed p-values < 0.05 were considered statistically significant.
Results
Baseline Study Cohort Characteristics
1570 patients presented with OGIs. Most patients (1165, 74.2%) identified as male. The mean (SD) patient age at presentation was 48.2 (22.8) years. Demographically, most patients (920, 58.6%) identified as White race, 300 (19.1%) identified as Black race, and 32 (2.0%) were categorized as other races. 965 patients (61.5%) identified as not Hispanic or Latino, and 392 (25.0%) identified as Hispanic or Latino. 726 patients (46.2%) were privately insured, 339 (21.6%) were insured through Medicare, 155 (9.9%) were insured through Medicaid, and 272 (17.3%) were uninsured. Most patients’ occupational status was not reported (72.%), 3.9% (N=61) were construction workers, 1.8% (N=29) were industrial workers, 3.9% (N=62) were students, 6.0% (N=94) were unemployed, and 12.4% (N=194) had other occupations. All demographic characteristics of the cohort are summarized in Table 1.
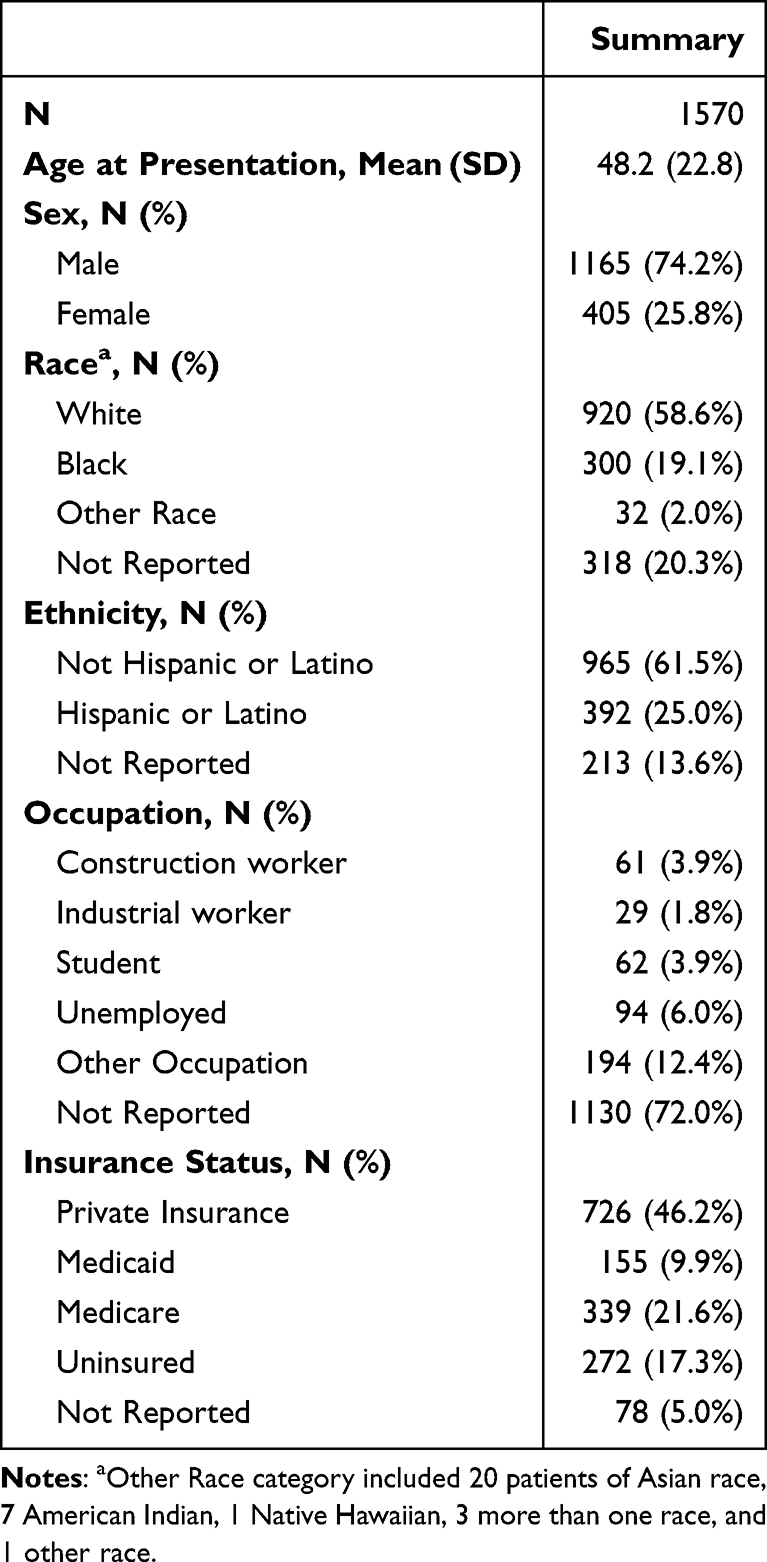 |
Table 1 Demographic Characteristics of Open Globe Injuries |
Most patients (673, 41.8%) were not using any substances at the time of injury, were not using eye protection of any kind (673, 42.9%), and were first seen at a local hospital (954, 60.8%) before presentation to one of the four eye centers included in this study.
The most common mechanisms of injury were falls (334 patients, 21.3%), followed by construction work (255 patients, 16.2%), assaults (157 patients, 10.0%), sports (64 patients, 4.1%), MVAs (60 patients, 3.8%), and firearms (22 patients, 1.4%). Most injuries occurred at home (517, 32.9%) or at the workplace (256, 16.3%).
847 (53.9%) of patients presented with lacerations of the globe versus 691 (44.0%) who presented with globe ruptures. Further classifying open globes caused by lacerations, 638 (40.6%) were penetrating injuries with no exit wound, 36 (2.3%) were perforating injuries with both an entrance and exit wound, and 166 (10.6%) resulted in intraocular foreign bodies (IOFBs).
Most OGIs were Zone I injuries (779, 49.6%), followed by Zone II (418, 26.6%), and less commonly, Zone III (287, 18.3%). Iris prolapse, hyphema, relative afferent pupillary defect (RAPD), eyelid laceration, and orbital fracture were the most frequent concomitant injuries.
At presentation, most patients (818 patients, 52.1%) had visual acuity (VA) worse than 20/600, 267 patients had VA better than 20/100 to 20/600, 55 patients (3.5%) had VA better than 20/60 to 20/100, and 166 had VA between 20/20 and 20/60. By last follow-up, a majority of patients (982 patients, 62.5%) had improved to VA between 20/20 and 20/60, 66 patients (4.2%) had VA better than 20/60 to 20/100, 164 had VA better than 20/100 to 20/600, and 337 patients still had VA worse than 20/600. 1145 patients (72.9%) received primary surgical repair within 24 hours. Most patients (1547, 98.5%) underwent primary surgical repair, eight patients (0.5%) had self-sealing wounds, and three patients (0.2%) underwent enucleation of the injured eye. Clinical characteristics of the cohort are summarized in Table 2.
 |
Table 2 Clinical Characteristics of Open Globe Injuries |
Risk Factors for Most Common Mechanisms of Injury
Multinomial logistic regression examined associations between common mechanisms of injury and potential demographic and clinical risk factors (Table 3). Univariable multinomial logistic regression analysis revealed that sex, age at presentation, race, ethnicity, open globe type, zone of injury, eyelid laceration, hyphema, RAPD, iris prolapse, and VA at presentation were variables associated with assaults, falls, and construction work mechanisms of injury.
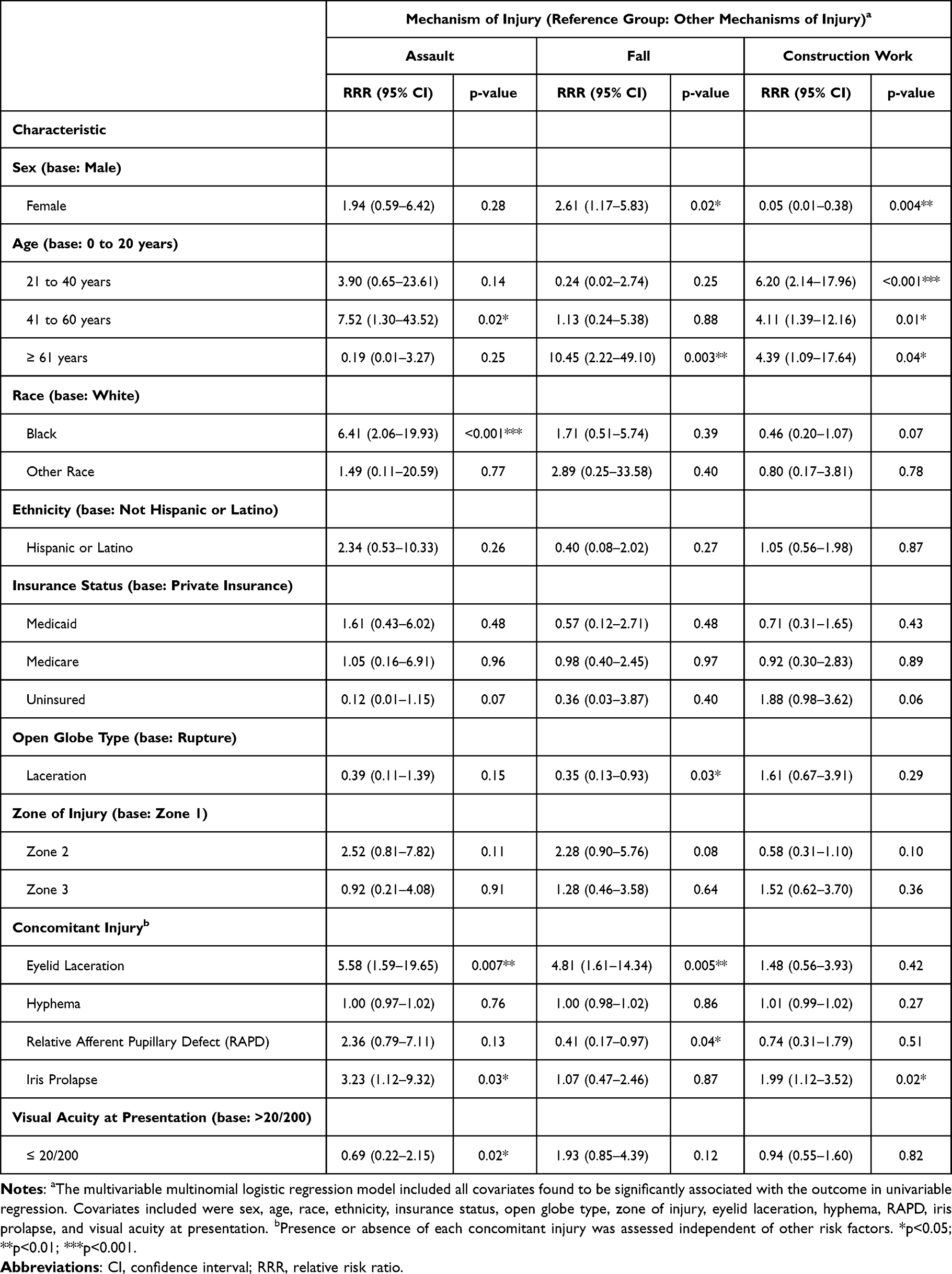 |
Table 3 Multinomial Logistic Regression of Mechanism of Injury by Demographic and Clinical Characteristics |
In an adjusted multivariable multinomial logistic regression model, age 41 to 60 years (relative risk ratio [RRR], 7.52 [95% confidence interval [CI], 1.30–43.52]; p=0.02), Black race (RRR, 6.41 [95% CI, 2.06–19.93]; p<0.001), eyelid laceration (RRR, 5.58 [95% CI, 1.59–19.65]; p=0.007), iris prolapse (RRR, 3.23 [95% CI, 1.12–9.32]; p=0.03), and VA at presentation ≤ 20/200 (RRR, 0.69 [95% CI, 0.22–2.15]; p=0.02) remained risk factors for assault. Female sex (RRR, 2.61 [95% CI, 1.17–5.83]; p=0.02), age 61 years and older (RRR, 10.45 [95% CI, 2.22–49.10]; p=0.003), globe lacerations (RRR, 0.35 [95% CI, 0.13–0.93]; p=0.03), eyelid laceration (RRR, 4.81 [95% CI, 1.61–14.34]; p=0.005), RAPD (RRR, 0.41 [95% CI, 0.17–0.97]; p=0.04) remained associated with falls. Female sex (RRR, 0.05 [95% CI, 0.01–0.38]; p=0.004), age 21 to 40 years (RRR, 6.20 [95% CI, 2.14–17.96]; p<0.001), age 41 to 60 years (RRR, 4.11 [95% CI, 1.39–12.16]; p=0.01), age 61 years and older (RRR, 4.39 [95% CI, 1.09–17.94]; p=0.04), and iris prolapse (RRR, 1.99 [95% CI, 1.12–3.52]; p=0.02) were risk factors for construction work injuries.
Risk Factors for Zone III Injury
Finally, binomial logistic regression was used to analyze associations between potential demographic and clinical risk factors and risk for Zone III injury (Table 4). Univariable logistic regression revealed that Hispanic or Latino ethnicity (prevalence ratio [PR], 0.67 [95% confidence interval [CI], 0.50–0.89]; p=0.005), uninsured patients (PR, 0.59 [95% CI, 0.41–0.84]; p=0.004), metal objects of injury (PR, 0.77 [95% CI, 0.59–1.00]; p=0.05), lacerations (PR, 0.53 [95% CI, 0.43–0.66]; p<0.001), penetrating injuries (PR, 0.52 [95% CI, 0.40–0.66]; p<0.001), intraocular foreign bodies (IOFBs) (PR, 0.46 [95% CI, 0.30–0.72]; p<0.001), traumatic cataract (PR, 0.29 [95% CI, 0.18–0.47]; p<0.001), and time to primary surgical repair greater than 24 hours (PR, 0.48 [95% CI, 0.35–0.67]; p=0.004) were negatively associated with Zone III injury. Substance use during injury (PR, 2.29 [95% CI, 1.63–3.22]; p<0.001), assault mechanisms of injury (PR, 2.36 [95% CI, 1.74–3.19]; p<0.001), expulsion of the lens (PR, 1.94 [95% CI, 1.46–2.56]; p<0.001), eyelid laceration (PR, 2.80 [95% CI, 2.27–3.45]; p<0.001), hyphema (PR, 2.65 [95% CI, 2.07–3.40]; p<0.001), RAPD (PR, 3.26 [95% CI, 2.56–4.14]; p<0.001), orbital fracture (PR, 2.79 [95% CI, 2.21–3.53]; p<0.001), retrobulbar hemorrhage (PR, 2.77 [95% CI, 1.76–4.36]; p<0.001), and VA greater than 20/60 to 20/100 (PR, 3.45 [95% CI, 1.31–9.08]; p=0.012) or less than 20/600 at presentation were positively associated with Zone III injury (PR, 5.48 [95% CI, 2.62–11.44]; p<0.001).
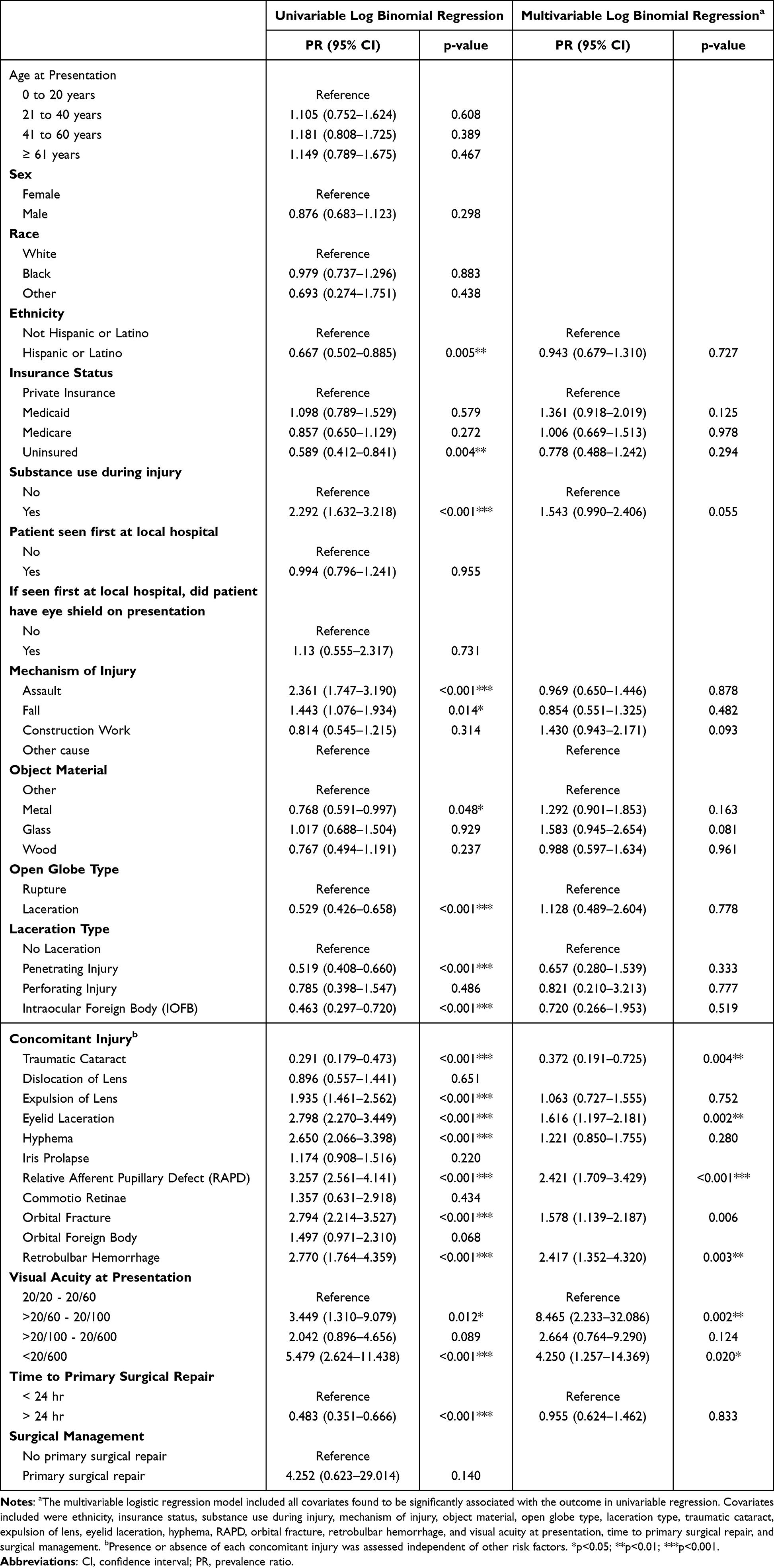 |
Table 4 Demographic and Clinical Risk Factors Associated With Zone III Open Globe Injury |
In a multivariable logistic regression including variables significant on univariable regression, traumatic cataract remained negatively associated with Zone III injury (PR, 0.37 [95% CI, 0.19–0.73]; p=0.004), and eyelid laceration (PR, 1.62 [95% CI, 1.20–2.18]; p=0.002), RAPD (PR, 2.42 [95% CI, 1.71–3.43]; p<0.001), retrobulbar hemorrhage (PR, 2.77 [95% CI, 1.76–4.36]; p<0.001), and presenting VA greater than 20/60 to 20/100 (PR, 8.47 [95% CI, 2.23–32.09]; p=0.002) or less than 20/600 (PR, 4.25 [95% CI, 1.26–14.37]; p=0.02) remained positively associated with Zone III injury.
Discussion
We used a large retrospective cohort of patients with open globe injuries to examine the association between demographic and clinical risk factors and specific open globe injury mechanisms, as well as to investigate risk factors for severe Zone III open globe injuries. We found that demographic factors including middle age (41 to 60 years) and Black race were associated with assault injuries, female sex and old age (61 years and older) were associated with falls, and working age (21 to 40 years), middle age, and old age were associated with construction work injuries. Further, we found that eyelid laceration was associated with assaults and falls, while iris prolapse was associated with assaults and construction work injuries. Poorer presenting VA (≤ 20/200) was associated with assault OGIs. In examining variables associated with Zone III injury, eyelid laceration, RAPD, and retrobulbar hemorrhage were key risk factors for Zone III injury.
The demographic profile of our cohort aligns with prior research showing that OGIs largely affect males and have a bimodal age distribution, with peaks in young adults and elderly individuals.9,16 However, our analysis reveals associations between specific mechanisms and demographic factors. Construction work injuries, which are an understudied mechanism of injury, showed a male predominance (95% lower risk in females compared to males) and peaked in working age adults, compared to those 20 years or younger, likely reflecting workforce demographics and corroborating current literature.22–24 Females had an over two times higher risk of fall-related OGI compared to males and elderly patients 61 years and older had a greater than ten-fold risk of falling compared to those 0 to 20 years. This is consistent with previous studies showing that elderly females are especially likely to sustain OGIs from falls.11,25,26
Our finding that Black patients faced an over six-fold higher risk of assault-related OGIs compared to White patients highlights disparities that warrant further investigation. While prior studies have documented racial disparities in ocular trauma,10,16,27 including that Black and Hispanic patients are at higher overall risk for OGIs, our results specifically ties these disparities in Black patients to assault mechanisms. This suggests a need for targeted education and prevention strategies within vulnerable communities.
The clinical characteristics associated with each mechanism of injury, including vision and concomitant injuries, offer insights for emergency triage and management. Assault-related OGIs showed higher rates of eyelid laceration and iris prolapse, suggesting more extensive periocular trauma and direct impact to the globe. Construction injuries frequently involved iris prolapse but had better VA on presentation, possibly due to smaller, focused impact from construction materials or equipment. Prior studies support the relative severity and poor visual outcomes associated with assault injury mechanisms,18,24 and the association of construction work injuries with concomitant injuries including retinal detachments, vitreous hemorrhage, hyphema, and traumatic cataracts.24,28
Our analysis of risk factors for posterior, Zone III OGIs, where some of the most severe complications of OGIs can occur, showed that eyelid laceration, RAPD, and retrobulbar hemorrhage were concomitant injuries independently associated with elevated risk for Zone III injuries. The presence of these concomitant injuries with Zone III injury likely reflects the severity and extent of globe injury. Lid trauma can be an indicator of high-energy mechanisms of injury or a trajectory of an injuring object that involves both extraocular and intraocular structures. RAPD may signal significant posterior segment involvement or optic nerve compromise, both of which are markers of severe ocular trauma. Finally, retrobulbar hemorrhage can occur emergently with blunt or penetrating OGIs, and is a marker of severe injury. In addition, as expected, severely decreased presenting vision was associated with Zone III injuries. Importantly, none of the mechanisms of injury delineated in our analysis were independent predictors of Zone III injury. Our results are consistent with and build on previous work showing that poor presenting vision is a prognostic factor for Zone III injury and that Zone III OGIs are overall associated with worse presenting vision, blunt trauma, traumatic cataract, hyphema, and RAPD, amongst other poor outcomes.29–31
Our study is subject to certain limitations. The retrospective nature of the data collection may have led to patients being omitted if they were not categorized under the appropriate billing codes (ICD-10 or CPT codes) for open globe injury or open globe repair. Categorization of the variables included in data collection are limited to records available within patient charts, which can be subject to nonreporting or reporting inaccuracies. For example, collection of variables such as use of eye protection or mechanism of OGI is not standardly reported across patients, and variables such as race, ethnicity, and occupation were often not reported. Additionally, while our multi-center design can improve generalizability over single-center studies and may be applicable to other urban, referral centers for eye trauma, it is not largely generalizable to the greater US population. Our cohort may include patients with a greater severity of injury, due to referrals from outside facilities, and likely underrepresents OGIs that occur in more rural settings. Furthermore, the timing of data collection (2018–2021) may have influenced the observed distribution of injuries. The COVID-19 pandemic, and associated lockdowns and lifestyle changes, could have decreased the frequency and types of injuries among patients presenting during our study period, and this temporal factor is an important consideration in interpreting the results presented here.
Conclusion
In conclusion, our large, multi-institutional study compiled demographic and etiological data on open globe injury, and identified significant demographic and clinical risk factors for OGI mechanisms and their severity. To our knowledge, it is one of the largest cohorts to study OGIs with relevant clinical and patient-level data. Assault injuries showed markedly higher risk among middle-aged adults and Black patients. Elderly patients and females were predominantly affected by falls, and construction injuries were associated with working-age adults. Clinical markers including eyelid laceration, iris prolapse, and poor presenting vision were mechanism-specific predictors that may help aid in early identification and triage of severe OGIs. Zone III injuries were strongly associated with poor prognostic indicators including RAPD and retrobulbar hemorrhage, highlighting the importance of careful posterior segment evaluation.
Future studies should evaluate targeted prevention programs for groups at increased risk for OGIs, evaluate risk assessment tools based on demographic and clinical variables to help stratify OGIs, and investigate the factors contributing to increased risk for certain mechanisms of injuries amongst demographic groups. Our findings suggest that such programs could include mandatory and enforced use of protective eyewear in high-risk occupations such as construction and industrial work, public awareness campaigns promoting awareness of fall risk and fall prevention safety measures among elderly populations, and community-based initiatives focused on reducing assault-related trauma, particularly in urban areas where interpersonal violence is a significant contributor to OGIs.
This study highlights key demographic and clinical risk factors associated with different mechanisms of injury. Our findings provide a foundation for the development of risk assessment tools that incorporate variables such as occupation, insurance status, and mechanism of injury to stratify OGI risk. Such tools could be implemented in emergency or primary care settings to guide screening, counseling, and referral. Future work should continue to explore these disparities, with the goal of developing more comprehensive, objective, and equity-informed interventions for OGIs.
Abbreviations
OGI, open globe injury.
Funding
There are no external funding sources for this work.
Disclosure
Dr Grayson Armstrong is a consultant to Ocular Technologies Inc, Kriya Therapeutics, Optomed, Xenon-VR, Chart Biopsy, McKinsey & Company, and Dynamed, and receives grants from the American Macular Degeneration Foundation, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Parver LM. Eye trauma: the neglected disorder. Arch Ophthalmol. 1986;104(10):1452–1453. doi:10.1001/archopht.1986.01050220046022
2. Acar U, Tok OY, Acar DE, Burcu A, Ornek F. A new ocular trauma score in pediatric penetrating eye injuries. Eye. 2011;25(3):370–374. doi:10.1038/eye.2010.211
3. Ramirez DA, Porco TC, Lietman TM, Keenan JD. Ocular injury in United States emergency departments: seasonality and annual trends estimated from a nationally representative dataset. Ame J Ophthalmol. 2018;191:149–155. doi:10.1016/j.ajo.2018.04.020
4. Négrel AD, Thylefors B. The global impact of eye injuries. Ophthal Epidemiol. 1998;5(3):143–169. doi:10.1076/opep.5.3.143.8364
5. Kuhn F, Morris R, Witherspoon CD, Heimann K, Jeffers JB, Treister G. A standardized classification of ocular trauma. Ophthalmology. 1996;103(2):240–243. doi:10.1016/s0161-6420(96)30710-0
6. Kuhn F, Morris R, Mester V, Witherspoon CD. Terminology of mechanical injuries: the Birmingham eye trauma terminology (BETT). Ocular Traumatology. 2008;3–11. doi:10.1007/978-3-540-33825-3_1
7. Pieramici DJ, Sternberg P, Aaberg TM, et al. A system for classifying mechanical injuries of the eye (globe). The ocular trauma classification group. Am J Ophthalmol. 1997;123(6):820–831. doi:10.1016/s0002-9394(14)71132-8
8. Blanch RJ, McMaster D, Patterson TJ. Management of open globe injury: a narrative review. Eye. 2024;38(16):3047–3051. doi:10.1038/s41433-024-03246-3
9. Mir TA, Canner JK, Zafar S, Srikumaran D, Friedman DS, Woreta FA. Characteristics of open globe injuries in the United States from 2006 to 2014. JAMA Ophthalmol. 2020;138(3):268–275. doi:10.1001/jamaophthalmol.2019.5823
10. Tomaiuolo M, Woreta FA, Li A, et al. Open-globe injury repairs in the American Academy of Ophthalmology IRIS® registry 2014 - 2018: incidence, risk factors, and visual outcomes. Ophthalmology. 2023;130(8):812–821. doi:10.1016/j.ophtha.2023.03.002
11. Andreoli MT, Andreoli CM. Geriatric traumatic open globe injuries. Ophthalmology. 2011;118(1):156–159. doi:10.1016/j.ophtha.2010.04.034
12. Klopfer J, Tielsch JM, Vitale S, See LC, Canner JK. Ocular trauma in the United States. Eye injuries resulting in hospitalization, 1984 through 1987. Arch Ophthalmol. 1992;110(6):838–842. doi:10.1001/archopht.1992.01080180110037
13. May DR, Kuhn FP, Morris RE, et al. The epidemiology of serious eye injuries from the United States Eye Injury Registry. Graefes Arch Clin Exp Ophthalmol. 2000;238(2):153–157. doi:10.1007/pl00007884
14. Kim JH, Ryoo HW, Kim JY, et al. Causative activities and prognostic factors of open-globe injury: a registry-based city-wide multicentre study. Ophthalmic Epidemiol. 2024:1–8. doi:10.1080/09286586.2024.2372051.
15. Beshay N, Keay L, Dunn H, Kamalden TA, Hoskin AK, Watson SL. The epidemiology of open globe injuries presenting to a tertiary referral eye hospital in Australia. Injury. 2017;48(7):1348–1354. doi:10.1016/j.injury.2017.04.035
16. Ojuok E, Uppuluri A, Langer PD, Zarbin MA, Thangamathesvaran L, Bhagat N. Demographic trends of open globe injuries in a large inpatient sample. Eye. 2021;35(8):2270–2276. doi:10.1038/s41433-020-01249-4
17. Chen V, Pharr C, Junn S, et al. Baltimore pediatric ocular trauma study: health disparities and outcomes in pediatric and adolescent open globe trauma. Injury. 2023;54(2):533–539. doi:10.1016/j.injury.2022.11.013
18. Schulz M, Bonnell AC, Chee YE, Feng S, Chen PP, Bojikian KD. Associations between socioeconomic status and open globe injury. Eye. 2025;39:986–991. doi:10.1038/s41433-024-03537-9
19. Kıvanç SA, Akova Budak B, Skrijelj E, Tok Çevik M. Demographic characteristics and clinical outcome of work-related open globe injuries in the most industrialised region of Turkey. Turk J Ophthalmol. 2017;47(1):18–23. doi:10.4274/tjo.81598
20. Tabatabaei SA, Khameneh EA, Soleimani M, Baramaki A. Open globe injuries in children under 7 years referred to a tertiary center in Iran from 2006 to 2016. Eye. 2021;35(4):1235–1239. doi:10.1038/s41433-020-1023-9
21. Siddiqui N, Chen EM, Parikh R, et al. Epidemiology of United States inpatient open globe injuries from 2009-2015. Ophthalmic Epidemiol. 2021;28(6):469–478. doi:10.1080/09286586.2021.1875008
22. Kanoff JM, Turalba AV, Andreoli MT, Andreoli CM. Characteristics and outcomes of work-related open globe injuries. Am J Ophthalmol. 2010;150(2):265–269.e2. doi:10.1016/j.ajo.2010.02.015
23. Zhou B, Uppuluri A, Zarbin MA, Bhagat N. work-related ocular trauma in the United States: a national trauma databank study. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):2081–2088. doi:10.1007/s00417-023-05983-9
24. Kolomeyer AM, Shah A, Bauza AM, Langer PD, Zarbin MA, Bhagat N. Nail gun-induced open-globe injuries: a 10-year retrospective review. Retina. 2014;34(2):254–261. doi:10.1097/IAE.0b013e3182979e0b
25. Halawa O, Mitchell W, Zebardast N. Fall-related eye injury among older adults in the United States. Am J Ophthalmol. 2021;229:82–89. doi:10.1016/j.ajo.2021.03.063
26. Morikawa S, Okamoto F, Okamoto Y, et al. Clinical characteristics and visual outcomes of work-related open globe injuries in Japanese patients. Sci Rep. 2020;10(1):1208. doi:10.1038/s41598-020-57568-9
27. Mike EV, Brandsdorfer A, Parsikia A, Mbekeani JN. Disparities associated with discharge patterns in firearm-associated ocular trauma. JAMA Ophthalmology. 2023;141(6):564–571. doi:10.1001/jamaophthalmol.2023.1467
28. Ilhan C, Citirik M, Uzel MM, Bagli S. Characteristics of work-related eye trauma in construction and manufacturing industries. Clin Exp Optom. 2022;105(5):546–551. doi:10.1080/08164622.2021.1952842
29. Bleicher ID, Tainsh LT, Gaier ED, Armstrong GW. Outcomes of zone 3 open globe injuries by wound extent: subcategorization of zone 3 injuries segregates visual and anatomic outcomes. Ophthalmology. 2023;130(4):379–386. doi:10.1016/j.ophtha.2022.10.027
30. Agrawal R, Ho SW, Teoh S. Pre-operative variables affecting final vision outcome with a critical review of ocular trauma classification for posterior open globe (zone III) injury. Indian J Ophthalmol. 2013;61(10):541–545. doi:10.4103/0301-4738.121066
31. Knyazer B, Levy J, Rosen S, Belfair N, Klemperer I, Lifshitz T. Prognostic factors in posterior open globe injuries (zone-III injuries). Clin Exp Ophthalmol. 2008;36(9):836–841. doi:10.1111/j.1442-9071.2009.01922.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Incidence and Characteristics of Orbital Hemorrhages in the United States from 2006 to 2018
Jensen AD, Taneja K, Ahmad MT, Woreta FA, Rajaii F
Clinical Ophthalmology 2022, 16:3369-3380
Published Date: 12 October 2022
Viral and Atypical Pathogen’s Epidemiology of a Large Cohort of Patients with Acute Respiratory Tract Infections in Shaanxi Province, Northwest China
Liu X, Li M, Yang T, He R, Guo X, Chen M
International Journal of General Medicine 2023, 16:1671-1679
Published Date: 5 May 2023