")
Back to Journals » Infection and Drug Resistance » Volume 18
Detection of Klebsiella Pneumoniae and Antibiotic Resistance in Burn Wards in China From 2019 to 2023
Received 15 January 2025
Accepted for publication 17 March 2025
Published 24 March 2025 Volume 2025:18 Pages 1595—1604
DOI https://doi.org/10.2147/IDR.S505514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sandip Patil
Xu Sun,1,* Rui Li,2,* Jun Xiang1
1Department of Burn, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2School of Medicine, Nankai University, Tianjin, 300071, People’s Republic of China
* These authors contributed equally to this work
Correspondence: Jun Xiang, Department of Burn, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected]
Introduction: The rise of antimicrobial resistance in Klebsiella pneumoniae, especially carbapenem-resistant strains (CRKP), presents a major challenge in burn care. This study aimed to examine the detection trends and resistance patterns of K. pneumoniae in burn wards over five years (2019– 2023) and analyze the clinical characteristics of patients with CRKP infections during the last three years.
Methods: A retrospective study was conducted on K. pneumoniae isolates from burn wards, collecting data on bacterial detection and antimicrobial resistance over five years (2019– 2023). Clinical records of CRKP-infected patients from the last three years were analyzed, focusing on age, total burn area, third-degree burn area, and prognosis. Statistical analyses assessed resistance trends and correlations between infection outcomes and clinical variables.
Results: The detection rate of Klebsiella pneumoniae and its resistance to common antibiotics have increased annually, particularly for carbapenem-resistant strains (CRKP). Polymyxin resistance among CRKP isolates has also risen. Wound secretions were the primary infection source, accounting for 75.9% of K. pneumoniae isolates, followed by the respiratory tract at 15.2% and blood/venous catheter samples at 8.9%. There was a significant rise in bloodstream CRKP detection rates during the study period. Clinically, CRKP infections were associated with a larger total burn area (mean: 45.3% vs 28.7% in non-CRKP cases) and more extensive third-degree burns (mean: 22.1% vs 12.4%). Mortality rates were higher in patients with CRKP infections compared to those with carbapenem-susceptible infections (34.6% vs 18.2%).
Conclusion: The drug-resistant phenomenon of Klebsiella pneumoniae in the burn ward of our hospital was serious, especially the number of carbapenem-resistant antimicrobial drugs of Klebsiella pneumoniae increased significantly, which should be strengthened to monitor and guide the rational use of drugs in the clinic.
Keywords: burn, klebsiella pneumoniae, drug resistance, antibiotic, antimicrobial
Introduction
Unlike other patients, burn patients have a compromised natural skin barrier, leading to increased capillary permeability. This makes it easier for pathogenic microorganisms to penetrate through the broken skin or damaged intestinal mucosa, invading the organism. Additionally, burn wounds are accompanied by a large number of necrotic tissues and inflammatory exudate, which activate pro-inflammatory and anti-inflammatory signaling pathways. This dysregulation of the innate and adaptive immune response ultimately results in a high incidence of infections in burn patients.1–3 The incidence of infection in burn patients remains high, with potential consequences including delayed healing, scar tissue proliferation, bacteremia, sepsis, and multiple organ dysfunction syndrome once the pathogen invades the subdermal tissue layer.4 In fact, infection is the most common complication in burn patients and one of the leading causes of death among those with severe burns (accounting for about 42%-65% of burn deaths).5–7
In recent years in China, there has been an increasing trend in detecting Klebsiella pneumoniae (especially Carbapenem-Resistant Klebsiella Pneumoniae (CRKP) strains) and its resistance to various types of drugs among burn patients. It has become one of the main causative organisms of hospital-acquired infections. Two factors have contributed to the increasing risk and threat posed by CRKP. One underlying factor is the growing genetic diversity of Klebsiella pneumoniae.8 Another significant factor is the presence of a wide array of virulence factors. Four specific virulence factors—capsular, lipopolysaccharide, fimbrium, and ferrierite—have been widely recognized as critical contributors to virulence. Isolates that possess these virulence factors are associated with higher mortality rates compared to those that do not carry such factors.9 It has been reported that in patients with extremely severe burns treated at single-center burn units in China, the mortality rate associated with bloodstream infections caused by Klebsiella pneumoniae is approximately 20–30%.10 Furthermore, according to a meta-analysis conducted by Solomon et al,11 the mortality rate among patients infected with carbapenem-resistant Klebsiella pneumoniae (CRKP) was found to be twice that of patients who were sensitive to carbapenem antibiotics. Additionally, the average length of hospital stay for CRKP-infected patients was significantly prolonged compared to their carbapenem-sensitive counterparts. A retrospective cohort study examining bloodstream infections caused by carbapenem -producing Klebsiella pneumoniae in critically ill patients revealed a 14-day mortality rate of 26.3% among 384 cases of CPKP bacteremia.12 Due to geographical differences in bacterial resistance and changing trends over time, dynamic bacterial epidemiologic data can contribute to treating clinically resistant bacteria and rationally applying antimicrobial drugs. This study presents preliminary retrospective statistics and analysis on the source of Klebsiella pneumoniae as well as drug resistance and clinical characteristics among burn patients infected with CRKP at our hospital from 2019–2023.
Materials and Methods
Collection of Strains
Klebsiella pneumoniae isolates obtained from the burn unit of Ruijin Hospital between January 2019 and December 2023 were analyzed. This included specimens from trauma cases, blood samples, arteriovenous intubation, tracheal intubation, and sputum. Additionally, drug susceptibility results were collected. Clinical data (including age, sex, total body surface area burned [TBSA], prognosis, etc) for patients infected with Klebsiella pneumoniae (TBSA ≥ 30%) were also gathered.
The exclusion criteria for this study were as follows: (1) repeated isolates from the same anatomical site in the same patient were excluded; (2) patients who died within 24 hours of admission; (3) patients who abandoned treatment on the same day; (4) patients with incomplete clinical data; and (5) patients with underlying conditions such as severe diabetes mellitus, heart failure, or renal insufficiency.
Isolation, identification and drug sensitivity testing of bacterial strains.
The collected clinical strains were isolated and purified, and then the ATB automated bacterial identifier (bioMérieux, France) was used for strain identification, and the Kirby-Bauer diffusion method (K-B method) or the dilution method (automated instrumentation) developed by the American Society for Clinical and Laboratory Standardization in 2017 was used for testing, and the antimicrobial drugs selected included ampicillin, piperacillin, cefoperazone/ sulbactam, ampicillin/sulbactam, piperacillin/tazobactam, cefazolin, cefoperazone, cefuroxime, ceftazidime, ceftazidime, cefotaxime, cefepime, amitrazine, imipenem, meropenem, amikacin, gentamicin, ciprofloxacin, mucosaminoglycosides, and tigecycline. The quality control bacteria were Escherichia coli ATCC8739 (provided by Shanghai Clinical Laboratory Center), and the results were judged as drug-resistant, intermediate and sensitive. CRKP was defined as those who were resistant to any of meropenem, ertapenem, or imipenem.
Statistical Analysis
Data were described and statistically analyzed using WHONET 5.6 and SPSS (version: 26.0), and statistical plots were drawn using GraphPad Prism 8. Measurements were described as mean ± standard deviation (x ± s) for normally distributed data and (median (interquartile spacing)) for non-normally distributed data. The count data are described in terms of frequency. For statistical tests, independent samples t-test was used for normally distributed data, Wilcoxon’s rank sum test was used for non-normally distributed data, and X2 test was used for count data, with P < 0.05 representing a statistical difference.
Results
Detection of Strains and Source Composition
A total of 332 clinical isolates of Klebsiella pneumoniae were identified in the burn ward from January 2019 to December 2023, with CRKP strains accounting for 64.76% (215/332) of the total. The clinical detection rates of Klebsiella pneumoniae in the burn wards over the five-year period were as follows: 16.6% (59/356) in 2019; 9.4% (49/519) in 2020; and 15.2% (87/573) in 2021,12.5% (84/672) in 2022, and finally, a decrease to 6.94% (53/764) in year-end of year-end data for year end-2023.
The primary source of Klebsiella pneumoniae in burn wards was found to be the wound (70.7%), followed by the respiratory tract (13.1%), hematogenous sources including deep venous catheters (15.4%), and other specimens. Specific bacterial sources and compositions corresponding to each year are detailed further within Table 1.
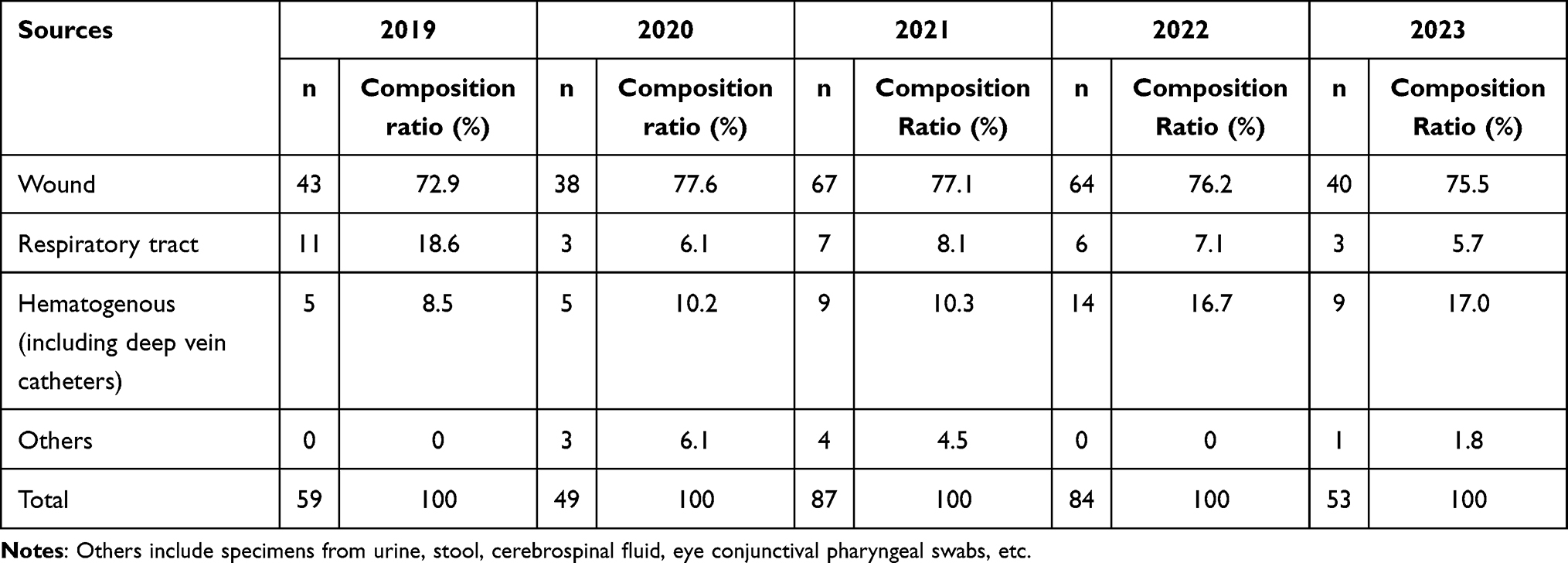 |
Table 1 Distribution of Detected Sources of Klebsiella Pneumoniae in Burn Wards From 2019 to 2023 |
Analysis of Resistance of Klebsiella Pneumoniae to Commonly Used Antimicrobial Drugs
As illustrated in Figure 1, the period from 2019 to 2023 witnessed a consistent resistance of all Klebsiella pneumoniae strains isolated from burn wards to ampicillin. Furthermore, there was an escalating trend in the resistance rates to commonly used antibiotics such as cefepime, gentamicin, ciprofloxacin, minocycline, and piperacillin/tazobactam over the years. By 2023, the resistance rate to phosphomycin had surged to 77.1%, while carbapenem antibiotics (meropenem and imipenem) exhibited a resistance rate exceeding 70%. Additionally, the resistance rate to tigecycline showed a steady increase over three years, reaching 41.1% by 2023. Notably, there was also a decline in sensitivity to polymyxin from 98.4% in 2019 to 85.8% in 2023.
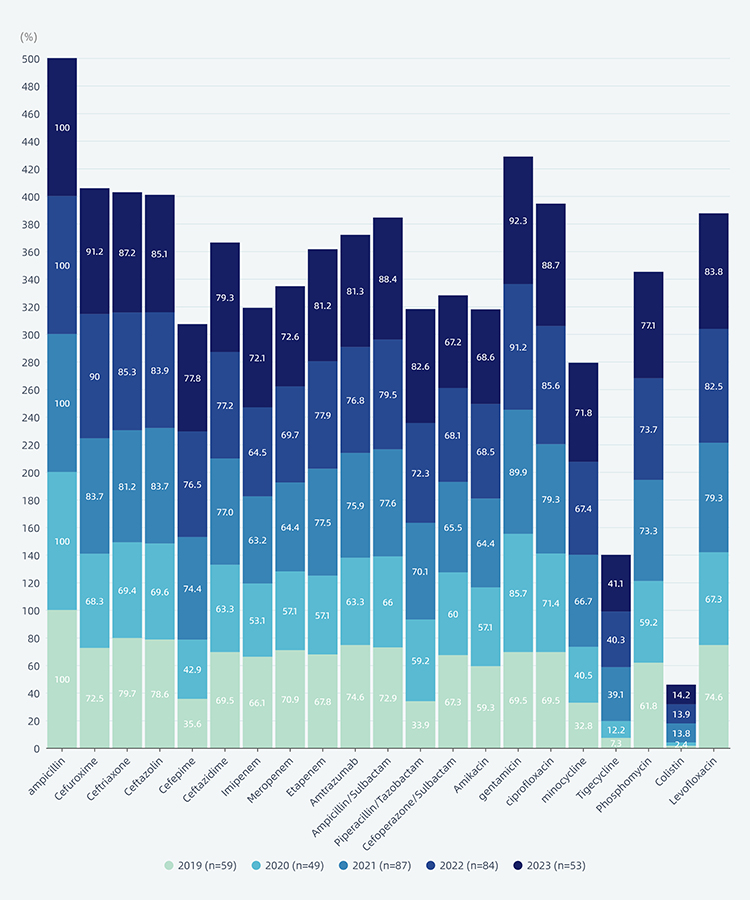 |
Figure 1 Analysis of resistance changes of Klebsiella pneumoniae to commonly used antibiotics in burn wards from 2019 to 2023. |
Analysis of Changes in CRKP Resistance to Commonly Used Antimicrobial Drugs
During the five-year period, a total of 215 CRKP strains were isolated from the burn ward, with detection rates of 67.8% (40/59), 57.1% (28/49), and 64.4% (56/87) in consecutive years. Additionally, detection rates were recorded at 71.4% (60/84) and 58.5% (31/53) for subsequent years. Of the 215 CRKP strains identified, the majority originated from wounds (152) accounting for 70.7%, followed by respiratory tract sources (28) at 13.0%, and blood-borne infections including deep venous catheters contributing to 15.3% (shown in Table 2). Over the course of five years, resistance rates of CRKP strains to cephalosporins, amitraz and quinolones remained consistently high at 100%. Furthermore, there was an observed increase in resistance rates to other antimicrobial drugs each year as indicated in Figure 2. The resistance rate of CRKP strains to tigecycline increased from 10% in 2019 to 51.8% in 2021 while the resistance rate to polymyxin also rose from 14.3% in 2021 to 71% in 2023.
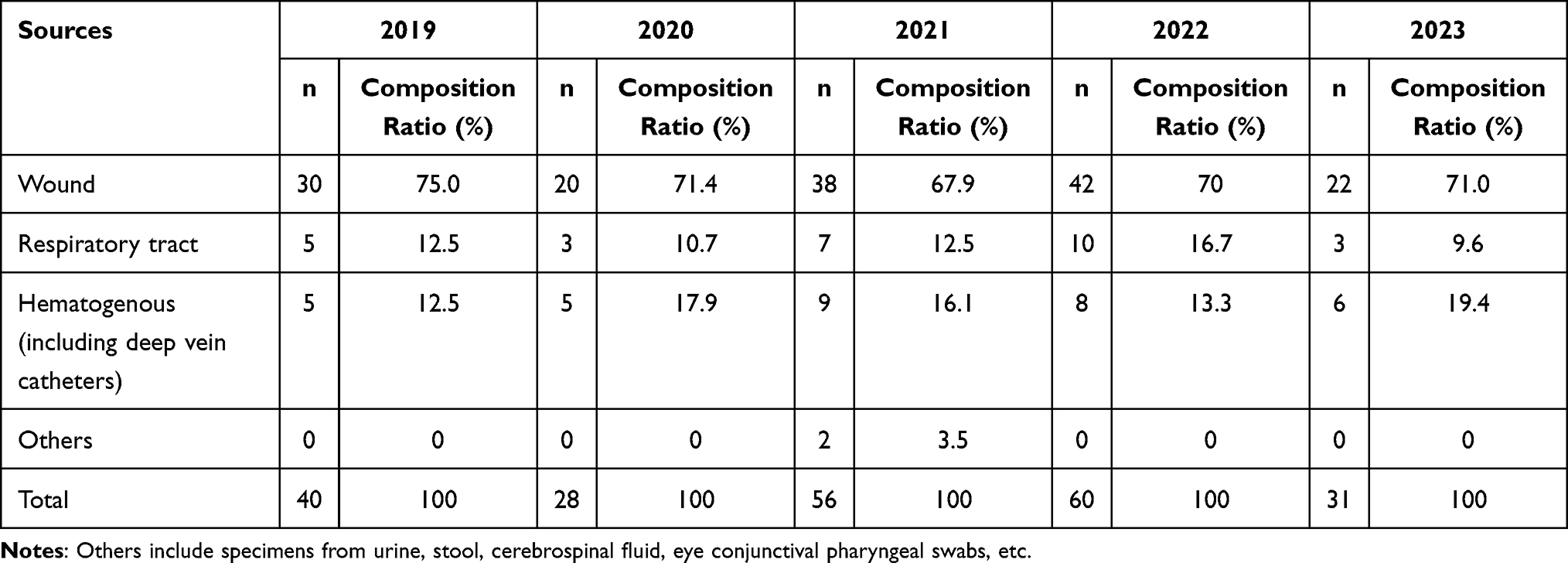 |
Table 2 Distribution of Detected Sources of CRKP in Burn Wards From 2019 to 2023 |
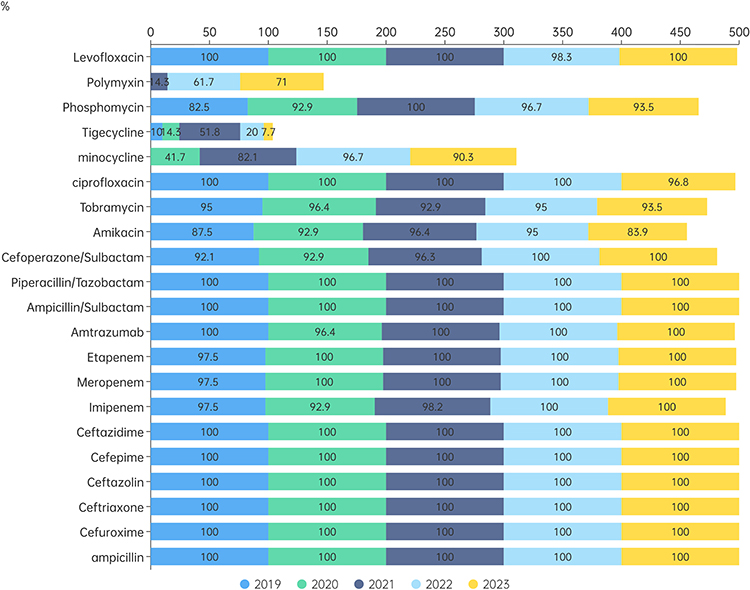 |
Figure 2 Analysis of resistance changes of CRKP in burn wards to commonly used antibiotics from 2019 to 2023. |
Analysis of Clinical Data
A total of 171 clinical isolates of Klebsiella pneumoniae were identified in our department from January 2021 to December 2023. A total of 102 patients infected with Klebsiella pneumoniae were included in the retrospective study and analyzed based on a selection criteria of TBSA≥ 30% of the total burned area. Of these patients, there were 78 males and 24 females, with a mean age of (50.29±8.30) years, a mean total burned surface area (TBSA) of (69.10±14.87) %, and a mean third-degree burned surface area of (45.20±12.10) %. Therefore, it was observed that Klebsiella pneumoniae infections in burn wards were common among older patients aged 50 and above, and that those with larger total burned areas and III-degree burns were more susceptible. The patients were divided into two groups: CRKP group (n=86) and non-CRKP group (n=16), based on whether they were infected with CRKP or not. It was found that compared to the non-CRKP group, patients in the CRKP group had larger total areas of burns and third-degree burns, with a statistically significant difference noted (P < 0.05). Additionally, within the non-CRKP group, it was observed that strains originated primarily from trauma and respiratory tract sources; however, out of the 23 strains originating from blood samples, 19 were identified as CRKP strains as shown in Table 3.
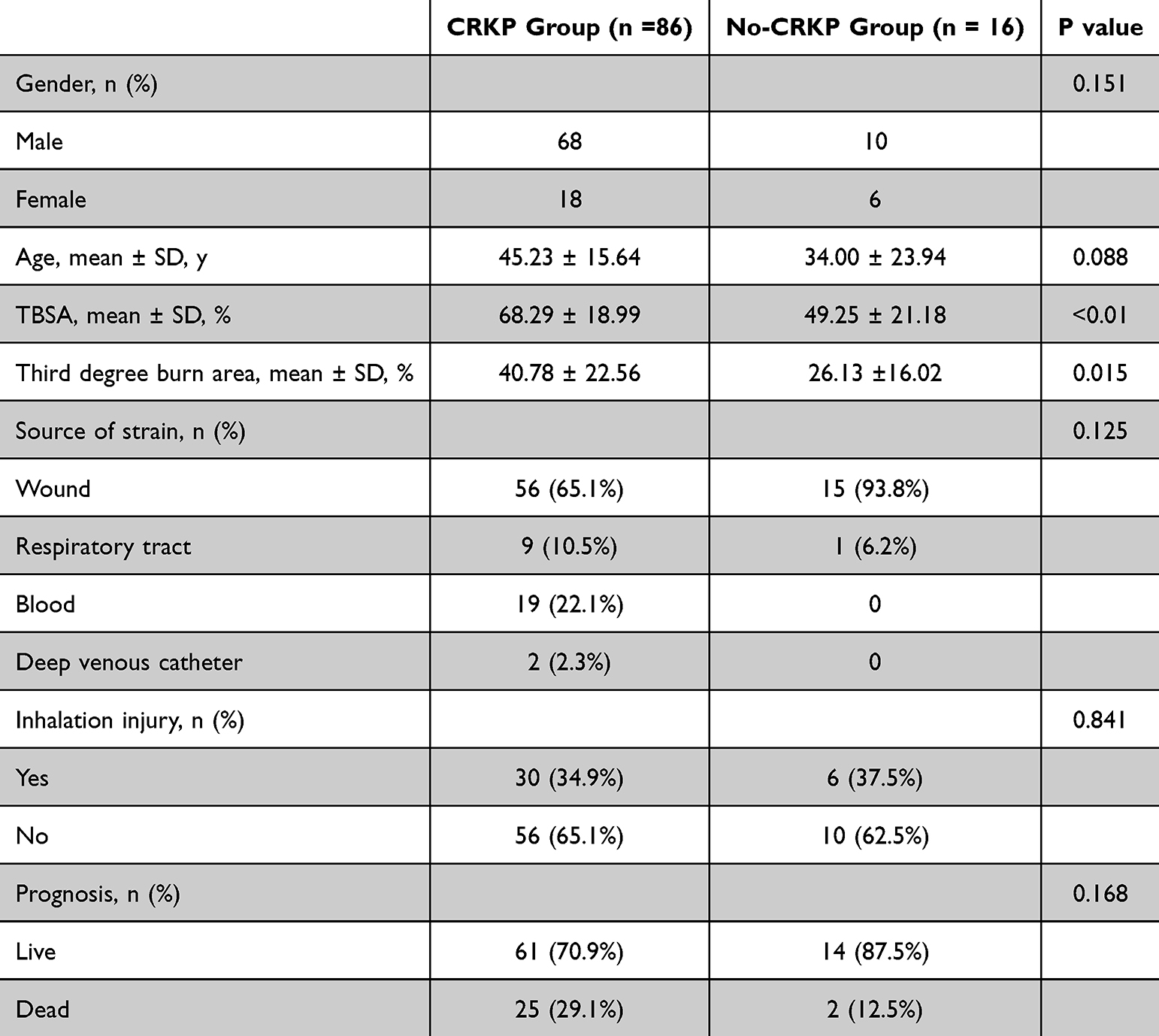 |
Table 3 Comparison of Clinical Data of Different Groups With Patients Klebsiella Pneumoniae Infected (TBSA≥30%) in Burn Ward From 2021 to 2023 |
Discussion
Currently, infection remains the most common complication and one of the leading causes of death in burn patients. Severe burns contribute to the development of oxidative stress, followed by a systemic inflammatory response, and the prolonged hypermetabolic state of the body ultimately leading to an increased risk of secondary muscle content loss, multifunctional organ failure, sepsis, and death. According to the results of CHINET China Drug Resistance Monitoring,13 the ratio of Gram-negative bacilli to Gram-positive cocci in clinical isolates from tertiary hospitals in China is 7:3. The resistance rate to commonly used antibiotics is increasing. It is worth noting that the detection rate of CRKP has significantly increased in recent years, rising from 3% to 10.9% between 2005 and 2019.14 Klebsiella pneumoniae is an opportunistic pathogen widely distributed in the normal environment or colonizing the human oral cavity, skin, respiratory tract, and gastrointestinal tract. It often causes a range of illnesses including urinary tract infections, pyogenic liver abscesses (PLA), and pneumonia in both normal and immunocompromised patients.15 In some general hospitals, Klebsiella pneumoniae prevalence is relatively concentrated and mostly manifests as multi-drug-resistant strains, it is one major Gram-negative strain causing nosocomial infections. In this study, we conducted a retrospective analysis of the distribution and drug resistance of Klebsiella pneumoniae isolated from clinical specimens in the burn ward of our hospital from 2019 to 2023. The aim was to provide a basis for clinicians to formulate a reasonable and scientific antimicrobial treatment plan. The numbers of CRKP strains isolated from our hospital in 2019, 2020, 2021, 2022, and 2023 were as follows: 292, 272, and 342; then decreased slightly to299and335 respectively. Their detection ratios were approximately between 22%to 28%, which is consistent with relevant national reports.16 A total of 332 clinical Klebsiella pneumoniae strains were collected in our burns ward during the same period. Among them 215 were identified as CRKP strains, resulting in an average detection rate of 64.8%. This rate was significantly higher than the data reported by CHINET.16 This discrepancy may be attributed to the distinct immunocompromised status of burn patients, prolonged use of invasive devices (eg, mechanical ventilation for 10 days), and previous exposure to carbapenems. These factors have been identified as independent risk factors for colonization and infection by CRKP.17
The skin barrier is compromised following severe burns, leading to the presence of a large amount of necrotic tissue at the wound site and a weakened systemic immune response. These conditions create an environment conducive to local bacterial proliferation and invasion into the body, increasing the risk of traumatic sepsis in patients with extensive burns. Additionally, the barrier function of the intestinal mucosa is impaired after severe burns, resulting in increased permeability that can facilitate bacterial translocation and subsequent bloodstream infections complicating sepsis. During patient treatment, invasive catheter placement (such as deep venous catheters, arterial catheterization, tracheal intubation) is often necessary to maintain circulation and respiration. However, these procedures may pass through or near burn wounds, serving as potential pathways for bacterial invasion and posing a high risk for drug-resistant bacterial infections. In cases of bloodstream infections caused by drug-resistant bacteria, sepsis or septic shock can rapidly develop. Our analysis revealed that Klebsiella pneumoniae strains in the burn ward were primarily sourced from traumatic secretions (average 70.7%), with blood sources including deep venous catheters accounting for 15.4%. The distribution of CRKP sources in the burn ward showed similar trends: traumatic secretions accounted for over 70%, followed by blood sources (including deep venous catheters) at 15.3%. The proportion of Klebsiella pneumoniae from wound sources is consistent with most domestic reports.18,19 ALfadli et Al19 analyzed the pathogens of burn wounds in Al-Babtain Burn and Plastic Center in 2017, and the detection rate of Klebsiae pneumoniae was 19.51%, which was significantly different from that in this study. This may be related to factors such as the distribution of bacteria and the use of antibiotics in domestic and foreign environments. Furthermore, the high percentage of blood as a source is concerning because clinical management becomes very challenging in cases of bloodstream infections.
Currently, for drug-resistant Klebsiella pneumoniae infections in severe burns, the treatment relies heavily on systemic application of sensitive antibiotic therapy in addition to surgical wound treatment. The resistance rate of Klebsiella pneumoniae to all types of antibiotics detected in burn wards has been steadily increasing from 2010 to 2017, with the most significant rise seen in resistance to meropenem and imipenem. Tigecycline, which was previously more sensitive, has shown a rapid increase in resistance in recent years. Currently, CRKP is only sensitive to polymyxin.20–22 Our study’s drug sensitization results also indicated that the majority of Klebsiella pneumoniae strains originating from burn wards maintained a resistance rate of over 70% to third- and fourth-generation cephalosporins during the three-year period. Additionally, there was a 60–70% resistance rate to piperacillin/tazobactam and an even higher degree of resistance to quinolones, significantly surpassing the results reported in CHINET.16 For an extended period, carbapenem antibiotics have been the preferred choice for treating Klebsiella pneumoniae infections due to their increased resistance to β-lactamase hydrolysis and significant clinical therapeutic effects compared to other antibiotics. However, with the widespread use of carbapenem antibiotics in clinical settings, there has been a gradual emergence of CRKP, which has shown an epidemic trend. Drug sensitivity results over five years have indicated that the resistance of Klebsiella pneumoniae to carbapenem antibiotics such as imipenem and meropenem was approximately 60%, significantly higher than the rates reported by CHINET (25%, 23.7%). Furthermore, CRKP strains demonstrated high resistance to most antibiotics except for polymyxin, to which they exhibited high sensitivity. It is worth noting that while the resistance rate of CRKP to tigecycline was only 10% in 2019, it had increased to 51.8% by 2021. Additionally, sensitivity to polymyxin decreased from 85.7% to 29%. These findings reflect global trends in local antibiotic selection pressure and the evolution of carbapenem-resistant Klebsiella pneumoniae (CRKP). Genomic studies have elucidated the acquisition of resistance to CRKP through horizontal gene transfer of plasmids harboring blaKPC or blaNDM, alongside chromosomal mutations that enhance virulence and environmental adaptation.23,24 For instance, ST15 and ST11 clones, which are notorious for disseminating the carbapenemase gene, have predominated hospital outbreaks in Europe and Asia. This suggests that similar clonal transmission may underlie the epidemiology observed in our hospitals.
Nowadays, CRKP has emerged as a significant causative agent of infection in patients with extensive burns.25,26 It has been noted in the literature27 that bloodstream infections (including catheter-associated infections) caused by CRKP often lead to rapid onset of sepsis and septic shock, resulting in high mortality rates. Our current study also indicated that trabecular secretions and hematogenous origin were the two primary sources of CRKP infection. Clinical data revealed that patients infected with CRKP had larger total burn areas and a higher proportion of third-degree burns compared to non-CRKP-infected patients (P < 0.05). Furthermore, our findings showed that out of 19 patients with CRKP bloodstream infections (including deep venous catheters), the mortality rate was 63.16% (12/19), consistent with previous reports. In addition to surgical interventions for wound treatment, individuals with severe burn CRKP infections often require sensitive antibiotic therapy. Current recommendations primarily advocate for polymyxin-based antimicrobial drug combinations, such as polymyxin combined with tigecycline, aminoglycoside antibiotics, or carbapenem antibiotics.21,28 The literature has demonstrated29 that the use of polymyxins alone to treat CRKP infections resulted in a success rate of only 27%. However, combination therapy increased the success rate by 44%. Another study indicated that antibiotic combination therapy reduced the 30-day morbidity and mortality rate in patients with CRKP bloodstream infections (OR=0.11, P=0.01, 95% CI (0.02–0.69)).20,30 This study reported a morbidity and mortality rate of 54.3% for polymyxin alone, compared to 34.1% for combination therapy. Specifically, the combination of polymyxin and tigecycline had a case-fatality rate of 30.4%, which was further reduced to 12.5% with the addition of meropenem to this combination treatment strategy. QURESHI et al31 also utilized combination antibiotics in treating patients infected with CRKP and documented the various patient outcomes. Their findings revealed that out of the seven patients treated with a combination therapy of polymyxin (one with quinolones, one with tigecycline, and five with carbapenems), only 14.3% experienced a case fatality rate, whereas four deaths occurred in patients treated solely with polymyxin. Therefore, stringent antibiotic management and infection control measures are crucial in effectively preventing further CRKP epidemics.
For patients with severe burns, it is imperative to recommend strict nosocomial infection control measures along with regular and timed bacteriological monitoring of burn wounds, sputum, various inserted catheters, blood samples, as well as ward environment samples. Once it is determined that a patient is infected or colonized by CRKP, isolation from contact is essential along with implementing effective disinfection measures for their medical and living supplies to prevent the spread of CRKP.
Conclusion
The drug-resistant phenomenon of Klebsiella pneumoniae in the burn ward is a serious issue. In particular, there has been a significant increase in the number of carbapenem-resistant antimicrobial drugs of Klebsiella pneumoniae, which requires strengthened monitoring and guidance for the rational use of drugs in clinical settings.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Shanghai Ruijin Hospital affiliated with Shanghai Jiaotong University, School of Medicine (2023-334).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent To Participate
Written informed consent has been obtained from all the patients.
Funding
There is no funding to report.
Disclosure
The authors declare no potential conflict of interests.
References
1. Neely CJ, Kartchner LB, Mendoza AE, et A. Flagellin treatment prevents increased susceptibility to systemic bacterial infection after injury by inhibiting anti-inflammatory IL-10+ IL-12-neutrophil polarization. PLoS One. 2014;9(1):e85623. doi:10.1371/journal.pone.0085623
2. Hidalgo F, Mas D, Rubio M, Garcia-Hierro P. Infections in critically ill burn patients. Medicina intensiva. 2016;40(3):179–185. doi:10.1016/j.medin.2016.02.001
3. Tang YY, Lou GX, He WF. (2021). Sichuan da xue xue bao. Yi Xue Ban = J Sichuan Univ Med Sci. 52(1):16–21.
4. Manning J. Sepsis in the burn patient. Crit Care Clin N Am. 2018;30(3):423–430. doi:10.1016/j.cnc.2018.05.010
5. Krishnan P, Frew Q, Green A, Martin R, Dziewulski P. Cause of death and correlation with autopsy findings in burns patients. Burns. 2013;39(4):583–588. doi:10.1016/j.burns.2012.09.017
6. Bloemsma GC, Dokter J, Boxma H, Oen IM. Mortality and causes of death in a burn centre. Burns. 2008;34(8):1103–1107. doi:10.1016/j.burns.2008.02.010
7. Lopes MCBT, de Aguiar Júnior W, Whitaker IY. The association between burn and trauma severity and in-hospital. Complications Burns. 2020;46(1):83–89.
8. Liqiang L, Jiuxin Q. Toward our understanding of carbapenem-resistant Klebsiella pneumoniae. Chin.Sci Bull. 2025;70(2):148–150.
9. Paczosa MK, Mecsas J. Klebsiella pneumoniae: going on the offense with a strong defense. Microbiol mol Biol Rev. 2016;80(3):629–661. doi:10.1128/MMBR.00078-15
10. Epidemiological characteristics and risk factors of sepsis development and death in patients with extremely severe burns. Chin J Burns. 2023;39(6):558–564.
11. Solomon SL, Oliver KB. Antibiotic resistance threats in the United States: stepping back from the brink. Am Fam Physician. 2014;89(12):938–941.
12. Papadimitriou-Olivgeris M, Bartzavali C, Georgakopoulou A, et al. External validation of INCREMENT-CPE score in a retrospective cohort of carbapenemase-producing Klebsiella pneumoniae bloodstream infections in critically ill patients. Clin Microbiol Infect. 2021;27(6):
13. Fupin H, Yan G, Demei Z, et al. Bacterial resistance surveillance in CHINET tertiary hospitals in 2019. Chin J Infect Chemother. 2020;20(03):233–243.
14. Qiao F, Wenzhi H, Zhiyong Z. Significance and development trend of multi-drug resistant bacteria infection prevention and control. Chin Nurs Manage. 2019;19(8):6.
15. Hsieh PF, Lin TL, Lee CZ, Tsai SF, Wang JT. Serum-induced iron-acquisition systems and TonB contribute to virulence in Klebsiella pneumoniae causing primary pyogenic liver abscess. J Infect Dis. 2008;197(12):1717–1727. doi:10.1086/588383
16. Fupin H, Yan G, Demii Z, et al. 2020 CHINET China Bacterial Drug Resistance Monitoring [J]. Chin J Infect Chemother. 2021;21(04):377–387.
17. Bian W, Chen W, Gu X, et al. Analysis of related factors of carbapenem resistant Klebsiella pneumoniae infection in patients with artificial airway. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(11):1324–1330. doi:10.3760/cma.j.cn121430-20200601-00431
18. Jing W, et al. Analysis of related factors of pathogenic bacterial infection in burn wound [J]. Chin J Nosocomial Infectiology. 2017;27(2):345–347.
19. Junying Y, Min L, Wandong P, et al. Analysis of pathogenic bacteria distribution and related risk factors of wound infection in burn patients. Chin J Med. 2022;45(09):950–956.
20. Tumbarello M, Viale P, Viscoli C, et A. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. 2012;55(7):943–950.
21. Lee GC, Burgess DS. Treatment of Klebsiella pneumoniae carbapenemase (KPC) infections: a review of published case series and case reports. Ann Clin Microbiol Antimicrob. 2012;11(32).
22. Albur M, Noel A, Bowker K, MacGowan A. Bactericidal activity of multiple combinations of tigecycline and colistin against NDM-1-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2012;56(6):3441–3443. doi:10.1128/AAC.05682-11
23. David S, Reuter S, Harris SR, et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat Microbiol. 2019;4(11):1919–1929. doi:10.1038/s41564-019-0492-8
24. Wyres KL, Lam MMC, Holt KE. Population genomics of Klebsiella pneumoniae. Nat Rev Microbiol. 2020;18(6):344–359. doi:10.1038/s41579-019-0315-1
25. Huan J. Controlling infection and spread of carbapenems-resistant Klebsiella pneumoniae among burn patients. Chin J Burns. 2015;31(1):4.
26. Xiaoling L, Daizhi P, Liang X, Shu W-T, Zhou X, Liu J. Drug resistance phenotype and homology analysis of Klebsiella pneumoniae in burn patients. Chin J Burns. 2012;28(2):96–100.
27. Jun X, Jingning H. Further understanding of carbapenem antibiotics and antimicrobial treatment strategies for Klebsiella pneumoniae infection in burn patients. Chin J Burns. 2018;34(11):6.
28. Yamamoto M, Pop-Vicas AE. Treatment for infections with carbapenem-resistant Enterobacteriaceae: what options do we still have? Critical Care. 2014;18(3):229. doi:10.1186/cc13949
29. Hirsch EB, Tam VH. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): an emerging cause of multidrug-resistant infection. J Antimicrob Chemother. 2010;65(6):1119–1125.
30. Keeney D, Ruzin A, Bradford PA. RamA, a transcriptional regulator, and AcrAB, an RND-type efflux pump, are associated with decreased susceptibility to tigecycline in Enterobacter cloacae.. Microb Drug Resist. 2007;13(1):1–6. doi:10.1089/mdr.2006.9990
31. Qureshi ZA, Paterson DL, Potoski BA, et A. Treatment outcome of bacteremia due to KPC-producing Klebsiella pneumoniae: superiority of combination antimicrobial regimens. Antimicrobial Agents Chemother. 2012;56(4):2108–2113. doi:10.1128/AAC.06268-11
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology, Drug Resistance, and Risk Factors for Mortality Among Hematopoietic Stem Cell Transplantation Recipients with Hospital-Acquired Klebsiella pneumoniae Infections: A Single-Center Retrospective Study from China
Liu YF, Liu Y, Chen X, Jia Y
Infection and Drug Resistance 2022, 15:5011-5021
Published Date: 30 August 2022
Long Term Characteristics of Clinical Distribution and Resistance Trends of Carbapenem-Resistant and Extended-Spectrum β-Lactamase Klebsiella pneumoniae Infections: 2014–2022
Wang N, Zhan M, Wang T, Liu J, Li C, Li B, Han X, Li H, Liu S, Cao J, Zhong X, Lei C, Zhang W, Zhang Z
Infection and Drug Resistance 2023, 16:1279-1295
Published Date: 4 March 2023
Antibacterial Activity Against Multidrug-Resistant Clinical Isolates of Nine Plants from Chencha, Southern Ethiopia
Manilal A, Sabu KR, Tsefaye A, Teshome T, Aklilu A, Seid M, Kayta G, Ayele AA, Idhayadhulla A
Infection and Drug Resistance 2023, 16:2519-2536
Published Date: 27 April 2023
Antibiotic Use, Awareness of Antimicrobial Resistance and Residue in Veterinary Professionals and Farmers in Selected Districts of Kellem Wollega Zone, Ethiopia
Ragassa S, Berhanu G
Veterinary Medicine: Research and Reports 2023, 14:159-175
Published Date: 26 September 2023
The Biological and Regulatory Role of Type VI Secretion System of Klebsiella pneumoniae
Liu W, Li M, Cao S, Ishaq HM, Zhao H, Yang F, Liu L
Infection and Drug Resistance 2023, 16:6911-6922
Published Date: 30 October 2023