")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Determinants of Anemia Among Patients with Chronic Kidney Disease: A Systematic Review of Empirical Evidence
Authors Prapaiwong P , Ruksakulpiwat S , Jariyasakulwong P, Kasetkala P, Puwarawuttipanit W, Pongsuwun K
Received 19 April 2025
Accepted for publication 19 June 2025
Published 28 June 2025 Volume 2025:18 Pages 3765—3780
DOI https://doi.org/10.2147/JMDH.S535423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Prapatsinee Prapaiwong, Suebsarn Ruksakulpiwat, Pawitra Jariyasakulwong, Piyoros Kasetkala, Wimolrat Puwarawuttipanit, Kewalin Pongsuwun
Department of Medical Nursing, Faculty of Nursing, Mahidol University, Bangkok, Thailand
Correspondence: Suebsarn Ruksakulpiwat, Department of Medical Nursing, Faculty of Nursing, Mahidol University, 2 Wanglang Road, Siriraj, Bangkok Noi, Bangkok, 10700, Thailand, Email [email protected]
Objective: This systematic review aimed to identify and synthesize empirical evidence regarding determinants of anemia among patients with chronic kidney disease (CKD) to inform clinical management and guide future research.
Methods: A comprehensive search of six electronic databases (PubMed, MEDLINE, ScienceDirect, Scopus, Web of Science, Google Scholar) was conducted for studies published from 2019 to 2024, following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Methodological quality was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklists tailored to each study design, and data synthesis was performed using convergent thematic analysis.
Results: Of 2269 records initially identified, 21 studies met inclusion criteria. Most studies originated from China (33.3%), employed cross-sectional designs (66.6%), and were hospital-based. Overall methodological quality was moderate to high, with JBI scores ranging from 69.23% to 100% (mean = 86.48%); notably, 47.6% of studies achieved a perfect quality score. Seven key themes emerged: 1) demographic and personal characteristics, 2) comorbidities, 3) duration of dialysis treatment, 4) kidney function, 5) biomarkers and metabolic ions, 6) geographic disparities, and 7) stimulation interventions (including stimulating agents, supplements, and exercise). Our review highlights that comorbidity (eg, diabetes mellitus, low BMI), declining kidney function, prolonged dialysis duration, and biomarkers such as calcium, phosphorus, ferritin, and inflammatory markers were significantly associated with anemia. Geographic disparities highlighted greater anemia prevalence in rural populations.
Conclusion: This review underscores multifaceted determinants of anemia in CKD, emphasizing comprehensive assessment and targeted interventions. Future research should explore individualized strategies addressing these diverse factors.
Keywords: chronic kidney disease, anemia, risk factors, comorbidities, dialysis, biomarkers, geographic disparities, systematic review
Background
Chronic kidney disease (CKD) is a growing global health worldwide and affects an estimated 700–850 million people, with the majority of cases occurring in low- and middle-income countries (LMICs).1 Among its most frequent and clinically significant complications is anemia, which develops as diseased kidneys fail to produce sufficient erythropoietin, the hormone driving red blood cell production.2 This condition is clinically relevant because it is not merely a laboratory abnormality but a driver of adverse outcomes: anemia in CKD is associated with significantly heightened risks of cardiovascular morbidity and mortality.3 Inadequate oxygen delivery due to low hemoglobin contributes to cardiac strain and can exacerbate CKD progression, forming a vicious cycle. Thus, anemia is widely recognized as a serious complication of CKD with major implications for patient health.2
Anemia is a common complication of CKD, with prevalence increasing alongside disease severity. Approximately 15% of patients with early-stage CKD are anemic, compared to 41% among those under nephrology care and up to 80% in Stage 5 CKD.4–6 Nearly all patients receiving renal replacement therapy are affected. Geographic and socioeconomic disparities further influence prevalence, with lower-income settings experiencing higher burdens due to limited care access.7–9 As CKD prevalence rises globally, anemia remains a major contributor to its health burden.
The high prevalence of CKD-related anemia translates into significant clinical and public health consequences. Anemic CKD patients suffer profound reductions in functional status and well-being. Untreated anemia also heightens the risk of adverse clinical outcomes, including higher rates of hospitalization, cardiovascular events, and CKD progression.10,11 Anemia in CKD has been linked to secondary complications such as cognitive decline and exacerbation of heart disease.12,13 The healthcare utilization and costs for CKD patients with anemia are substantially higher than for those without anemia.14,15 Importantly, many of these impacts are modifiable; evidence suggests that early identification and treatment of anemia can improve quality of life and slow renal decline.16 Recently, roxadustat, a hypoxia-inducible factor prolyl hydroxylase (HIF-PH) inhibitor, has emerged as a novel treatment for CKD-related anemia. By stabilizing HIFs, it enhances endogenous erythropoietin production, suppresses hepcidin, and improves iron metabolism.17,18 This mechanism offers an innovative approach beyond traditional ESAs. However, existing literature has not adequately addressed the role of HIF-PH inhibitors in regulating iron pathways, representing a key gap. A conceptual model of the HIF pathway may support understanding of this therapeutic innovation.
Despite extensive research, there are notable gaps in synthesized evidence regarding the multifactorial determinants of anemia in CKD. These include biological, clinical, sociodemographic, and behavioral factors. While several individual studies have examined these contributors, findings remain fragmented and vary across regions and study designs. This lack of consolidated evidence represents a critical knowledge gap. Without a clear, holistic understanding of who is most at risk for anemia and why, it is challenging to develop targeted interventions. This underscores the need for a systematic review that integrates the full spectrum of documented factors.
This systematic review is both timely and significant. For clinical nursing practice, it supports early identification of high-risk patients and implementation of proactive care strategies. For patient-centered care, it encourages a holistic approach that considers both biomedical and psychosocial determinants. At the health system level, the findings can inform planning, resource allocation, and the development of equitable, cost-effective strategies. Understanding the determinants of CKD anemia is vital for improving outcomes and reducing the burden on healthcare systems. Moreover, this review addresses a critical knowledge gap by synthesizing empirical evidence on the determinants of anemia in CKD. The findings will provide a comprehensive understanding that can inform clinical decision-making, support patient-centered care, and guide policy and planning. In doing so, it aims to enhance outcomes and quality of life for CKD patients globally.
Objective
To systematically review and synthesize empirical evidence on the determinants of anemia among patients with chronic kidney disease (CKD), to identify key contributing factors and inform clinical management and future research directions.
Methods
Identify Relevant Studies
In this systematic review, we adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework19 to document the process of identifying, screening, excluding, and including studies in a flow diagram. A comprehensive search of six electronic databases—PubMed, MEDLINE, ScienceDirect, Scopus, Web of Science, and Google Scholar—was conducted. This search aimed to locate studies published between 2019 and 2024 that examined factors associated with anemia in patients with chronic kidney disease (CKD). The search strategy utilized the following keywords: (“factor related” AND “chronic kidney disease” AND “anemia”) combined with Boolean operators. Additionally, reference lists from relevant studies were manually reviewed to identify further pertinent literature. All identified references were managed using EndNote.
Study Selection
We first screened the titles and abstracts to identify potentially relevant studies. Full-text articles were subsequently reviewed to determine their relevance to our research objectives. Studies that met the inclusion criteria were selected, while those that did not align with the review’s focus were excluded based on predefined criteria (Table 1).
 |
Table 1 Inclusion and Exclusion Criteria |
Quality Assessment
The purpose of the quality assessment is to evaluate the methodological rigor of each study and to identify any potential biases in their design, conduct, and analysis. In this review, two researchers independently assessed the quality of the studies using the Joanna Briggs Institute (JBI) critical appraisal tools, specifically developed for systematic reviews.20
Data Extraction
The standardized data extraction chart used for this review (Supplementary Table 1) captured the following information for each study: reference, year of publication, country of origin, study setting, target population, study design, sample size, mean age of participants, quality assessment score, study objectives, factors related to anemia, anemia measurements or indicators used, and the study’s implications or recommendations.
Data Synthesis
For data synthesis in this review, we employed the convergent integrated analysis framework as outlined by the Joanna Briggs Institute (JBI).21,22 This process involved extracting themes from the key findings of the studies by comparing and contrasting their main results. Subsequently, more specific sub-themes were developed based on the detailed aspects of the findings, following a method akin to the thematic analysis used in qualitative research.
Results
Search Results
Following the PRISMA guidelines,23,24 a total of 2269 records were initially identified through database searches, including Scopus (n = 261), ScienceDirect (n = 120), Web of Science (n = 973), PubMed and Medline (n = 504), and Google Scholar (n = 411). After the removal of duplicate records (n = 3), 2266 records remained for title and abstract screening. Of these, 2227 records were excluded based on the predefined inclusion and exclusion criteria (Table 1), resulting in 39 full-text articles sought for retrieval and assessed for eligibility. During the full-text screening phase, 18 reports were excluded due to the following reasons: the study did not investigate factors related to anemia in patients with chronic kidney disease (n = 11), non-English publication (n = 2), being a review article (n = 3), and ongoing studies with no results available (n = 2). Ultimately, 21 studies met the eligibility criteria and were included in the systematic review (Figure 1).
 |
Figure 1 Flow Diagram. Note: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.24 |
Description of Characteristic of Included Studies
Table 2 presents the characteristics of the included studies, categorized by publication year, country of origin, study setting, study design, sample size, target population, and anemia indicators used. The studies were published in 2024 (n = 2, 9.52%), 2023 (n = 5, 23.80%), 2022 (n = 2, 9.52%), 2021 (n = 7, 33.32%), 2020 (n = 3, 14.28%), and 2019 (n = 2, 9.52%). The included studies were conducted in a variety of countries/settings, with the largest proportion from China (n = 7, 33.32%), followed by Japan and Ethiopia (each n = 2, 9.52%). The remaining studies originated from Egypt, Korea, Mexico, the USA, Turkey, Brazil, Pakistan, Spain, Taiwan, and one multinational study covering the United States, South America, Australia, New Zealand, and Asia (each n = 1, 4.76%). In terms of study settings, most were conducted in university hospitals (n = 7, 33.32%) and nephrology units (n = 6, 28.56%), followed by general hospitals (n = 5, 23.80%), an institute of social security (n = 1, 4.76%), a database setting (n = 1, 4.76%), and one study that did not specify the setting (n = 1, 4.76%).
 |
Table 2 Characteristics of Included Studies |
Regarding study design, cross-sectional studies were the most common (n = 14, 66.64%), followed by randomized controlled trials (RCTs) (n = 3, 14.28%), longitudinal studies (n = 2, 9.52%), quasi-experimental studies (n = 1, 4.76%), and cohort studies (n = 1, 4.76%).
The majority of studies (n = 15, 71.40%) had sample sizes ranging from 1 to 500 participants, while a smaller number included more than 1000 participants (n = 5, 23.80%), and only one study (n = 1, 4.76%) had between 501 and 1000 participants. In terms of target populations, over half of the studies focused on patients with chronic kidney disease (CKD) (n = 12, 57.12%). Others targeted patients undergoing hemodialysis (HD) or peritoneal dialysis (PD) (n = 5, 23.80%), patients with CKD stages 3–5 (n = 3, 14.28%), and patients with CKD stages 1–4 (n = 1, 4.76%).
The mean age of participants was between 41 and 60 years in most studies (n = 12, 57.12%). Four studies (n = 4, 19.04%) included participants over 60 years of age, while the remaining studies reported broader age ranges or did not specify. Various anemia indicators were employed across the studies. Hemoglobin was the most frequently used biomarker (n = 18, 39.96%), followed by serum erythropoietin (EPO) levels (n = 5, 11.10%). Other commonly used indicators included hematocrit (n = 2, 4.44%), serum ferritin (n = 2, 4.44%), mean corpuscular hemoglobin (MCH) (n = 2, 4.44%), and the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) criteria (n = 2, 4.44%). Additional indicators used in individual studies (each n = 1, 2.22%) included hepcidin, red blood cell count, mean corpuscular volume (MCV), reticulocyte hemoglobin equivalent (RET-He), serum creatinine (Scr), serum iron (SI), transferrin (TRF), intrinsic factor antibody (IFAb), soluble transferrin receptor (STfR), total iron-binding capacity (TIBC), interleukin-6 (IL-6), Japanese Society for Dialysis Therapy (JSDT) criteria (1 and 2), and the European Best Practice Guidelines (EBPG) criteria.
Assessment of Methodological Quality
The methodological quality of the 21 included studies was assessed using the JBI critical appraisal checklists, tailored to each study design. Overall, the studies demonstrated moderate to high methodological quality, with quality scores ranging from 69.23% to 100%. The average quality score across all studies was 86.48%, indicating that most studies clearly reported essential methodological elements. Notably, ten studies (47.6%) achieved a perfect score of 100%, reflecting strong adherence to quality standards. Detailed quality assessments for each individual study are presented in Supplementary Table 1.
Description of Factors Related to Anemia in Patients with CKD
A summary of the findings on factors associated with anemia among patients with CKD is presented in Table 3, and more details of each included studies have been shown in Supplementary Table 1.25–45 Based on the synthesis of 21 studies, seven major themes were identified: (1) demographic and personal characteristics, (2) comorbidities and chronic illness, (3) duration of dialysis treatment, (4) kidney function, (5) biomarkers and metabolic ions, (6) geography, and (7) stimulation, which includes two subthemes—stimulating agents and supplements, and exercise. The frequency and distribution of these themes across the included studies are summarized below.
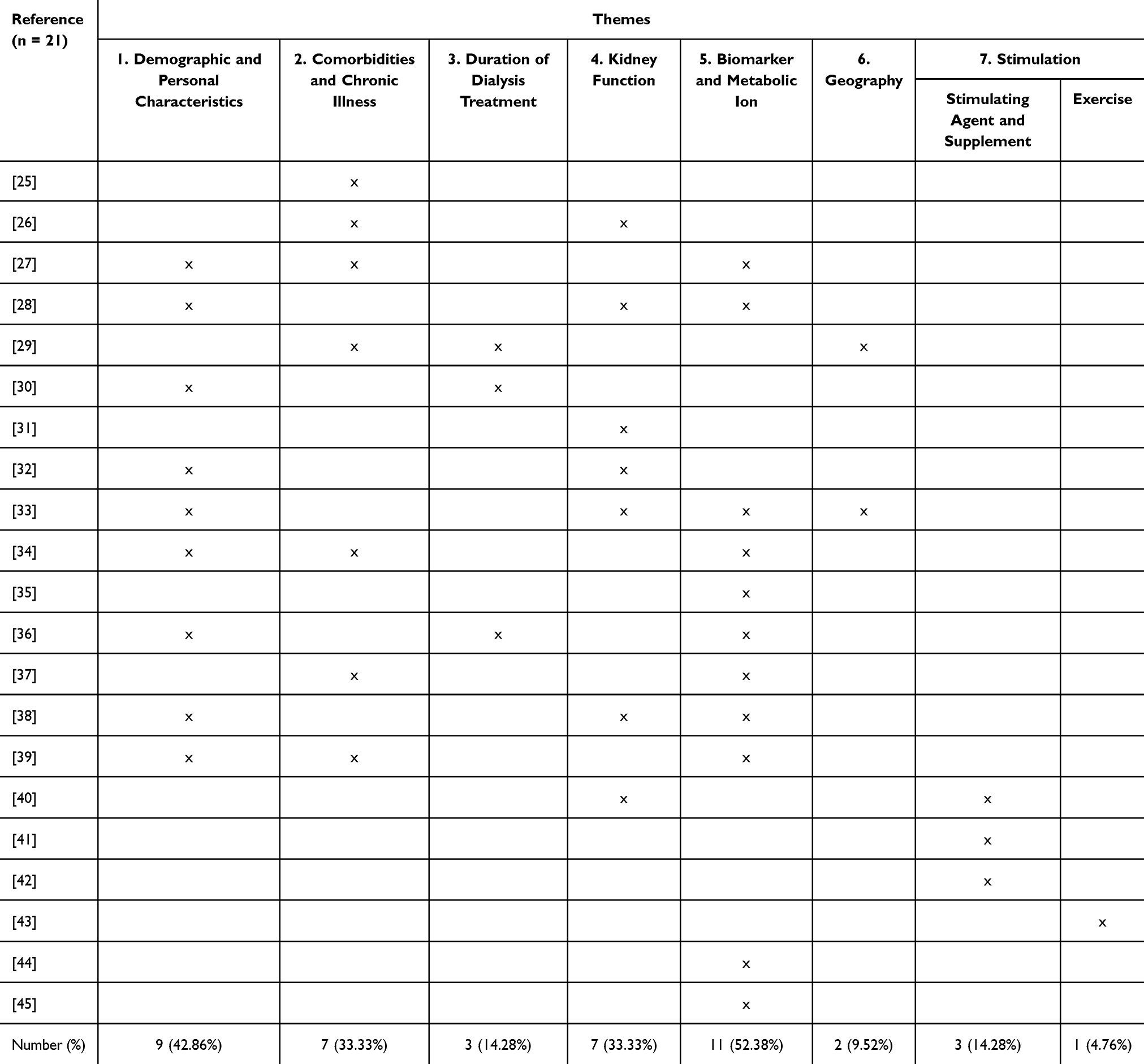 |
Table 3 Factors Related to Anemia Among Patients with Chronic Kidney Disease |
Demographic and Personal Characteristics
Nine included studies27,28,30,32,33,36,38,39 identified demographic and personal characteristics—particularly age and gender—as significant factors associated with anemia among patients with CKD. For instance, Lizardi Gómez et al examined the frequency of achieving optimal hemoglobin and hematocrit levels and the factors associated with suboptimal values in CKD patients undergoing maintenance hemodialysis. Their findings indicated that advanced age was significantly associated with anemia in this population.27 Similarly, Andrade et al reported that increasing age correlated with a higher risk of anemia among CKD patients.34 Moreover, a cross-sectional study by Alagoz et al aimed to determine the prevalence, severity, risk factors, and treatment of anemia in CKD. The results showed that female patients were more likely to experience severe anemia compared to males.33
Comorbidities and Chronic Illness
Seven included studies25–27,29,34,37,39 demonstrated a significant association between comorbidities and anemia in patients with CKD. Among these, diabetes mellitus (DM) emerged as a consistent contributing factor. For instance, Alaidy et al compared three groups—patients with diabetes but no renal abnormalities, patients with diabetic kidney disease (DKD), and healthy controls—and found that decreased erythropoietin (EPO) levels were a significant predictor of anemia in diabetic patients with CKD (AUC = 0.828, p < 0.001).25 Similarly, Lizardi Gómez et al conducted a study in Mexico involving 747 patients receiving maintenance hemodialysis, revealing that diabetes mellitus was a significant predictor of anemia (OR = 1.49, 95% CI = 1.06–2.10, p = 0.022).27 In a retrospective analysis by Andrade et al patients with non-dialytic CKD and diabetes had significantly higher odds of developing anemia compared to non-diabetic patients (OR = 13.038, 95% CI = 1.037–163.879, p = 0.04).34
Abnormal body mass index was another comorbidity-related factor associated with anemia. A retrospective cross-sectional study by Kim et al using data from the Korean National Health and Nutrition Examination Surveys (KNHANES), found that underweight participants had a significantly higher risk of anemia compared to those with normal weight (OR = 2.30, 95% CI = 1.22–4.34, p =0.01).26 Likewise, Adera et al reported that participants with a BMI <18.5 kg/m² and those with BMI between 18.5–24.9 kg/m² had a significantly increased risk of anemia compared to those with obesity (BMI 30–50 kg/m²), with adjusted odds ratios (AORs) of 6.78 (95% CI = 1.32–34.73, p = 0.022) and 5.04 (95% CI = 1.26–20.10, p = 0.022), respectively.29
Duration of Dialysis Treatment
Three studies29,30,36 identified the duration of dialysis treatment as a significant factor associated with anemia in patients with CKD. For instance, Bukhari et al evaluated the prevalence of anemia among CKD patients receiving maintenance hemodialysis and found a significant association between prolonged dialysis duration and increased anemia risk.36 Likewise, Adera et al conducted a cross-sectional study that revealed patients with a history of dialysis treatment were four times more likely to develop anemia compared to those without such a history.29 These findings suggest that extended exposure to dialysis-related physiological changes may contribute to worsening anemia outcomes in CKD populations.
Kidney Function
Seven studies26,28,31–33,38,40 in this review consistently identified kidney function as a significant factor associated with anemia in patients with CKD. For example, Cui et al categorized 225 maintenance hemodialysis (MHD) patients into three groups based on their ultrafiltration rate (UFR): <10 mL/h/kg, 10–13 mL/h/kg, and >13 mL/h/kg. The findings revealed that a higher UFR was associated with lower hemoglobin levels.28 In a cross-sectional cohort study, Sofue et al reported a significantly higher prevalence of anemia among Japanese patients with CKD stages G4 and G5.31 Similarly, a large retrospective study by Lamerato et al conducted in the United States and involving 750,701 patients with CKD stages 3a–5 not on dialysis (estimated glomerular filtration rate <60 mL/min/1.73 m²), demonstrated that advancing CKD stage was strongly associated with anemia. Specifically, the risk of anemia increased with CKD progression (1-year HR = 4.47, 95% CI: 3.73–5.35; 5-year HR = 2.37, 95% CI: 2.22–2.52).32
Biomarkers and Metabolic Ions
Eleven studies27,28,33–39,44,45 identified biomarkers and metabolic ions as significant factors associated with anemia in patients with CKD. For instance, Cui et al analyzed clinical data from hemodialysis (HD) patients to examine the relationship between ultrafiltration rate (UFR), hemoglobin (Hb) levels, and erythropoietin (EPO) responsiveness.28 The findings indicated that various biomarkers—including calcium, phosphorus, albumin, and C-reactive protein (CRP)—were significantly associated with Hb levels. In a multicenter cross-sectional study involving 1066 CKD patients not receiving renal replacement therapy, Alagoz et al assessed the prevalence, severity, and risk factors of anemia across nephrology centers. The study found that biomarkers such as serum ferritin, serum iron, and soluble Fas (sFas) levels were linked to the presence and severity of anemia.33 Similarly, a cross-sectional study conducted in China by Li et al explored the association between bone metabolic markers and anemia in CKD patients and evaluated the impact of parathyroidectomy. The study reported that serum calcium, phosphorus, and intact parathyroid hormone (iPTH) levels were significantly related to anemia status in this population.39
Geography
Two included studies29,33 investigated the role of geographical factors in the prevalence and severity of anemia among patients with CKD. Adera et al assessed the prevalence and associated factors of anemia in CKD patients and found that rural residence was significantly associated with higher rates of anemia.29 Similarly, a multicenter cross-sectional study by Alagoz et al examined anemia across various nephrology centers and analyzed geographic differences in anemia-related parameters. The study revealed significant disparities in the prevalence of severe anemia between centers located within the same geographic region, suggesting that location-specific healthcare infrastructure or resource availability may influence anemia outcomes.33
Stimulation
Stimulating Agent and Supplement
Three studies40–42 examined the effects of stimulating agents and supplements on anemia among patients with CKD. Li et al investigated the association between serum vitamin D₃ levels and anemia in patients with CKD stages 1 to 5 in China, finding that higher vitamin D₃ concentrations were associated with a reduced risk of anemia.40 Two additional studies explored the effectiveness of roxadustat, a hypoxia-inducible factor prolyl hydroxylase inhibitor, in managing anemia.
Coyne et al conducted a multicenter trial across various global regions and demonstrated that roxadustat significantly improved hemoglobin levels compared to placebo in CKD patients.41 Similarly, Hou et al evaluated the efficacy of roxadustat in Chinese patients undergoing peritoneal dialysis. The findings suggested that roxadustat led to greater improvements in hemoglobin levels and higher response rates compared to erythropoiesis-stimulating agents (ESAs), supporting its clinical potential in anemia management among this population.42
Exercise
One included study43 examined the role of exercise as a supportive strategy in managing anemia among patients with CKD undergoing hemodialysis (HD). Torres et al conducted a prospective, non-controlled intervention study in Spain to evaluate the effects of intradialytic exercise training on physical function, nutritional and inflammatory status, and anemia-related parameters. The results demonstrated that participation in exercise programs during HD sessions led to a significant reduction in iron and erythropoietin (EPO) requirements, while hemoglobin and ferritin levels remained stable throughout the study period. The authors highlighted the importance of integrating simple, individualized exercise routines into HD care to improve outcomes and reduce healthcare costs, although further research with controlled study designs is recommended.
Discussion
This systematic review provides a comprehensive synthesis of the multifactorial determinants associated with anemia in patients with CKD, highlighting key factors that span clinical, biochemical, geographic, and therapeutic dimensions. Specifically, our findings underscore the significant role of comorbidities (eg, diabetes mellitus and low body mass index), prolonged dialysis duration, declining kidney function, biochemical disturbances, geographic disparities, and stimulation strategies (pharmacological, nutritional, and exercise-based interventions) in influencing anemia outcomes among CKD patients. Understanding these diverse determinants offers critical insights into anemia’s complex etiology and highlights opportunities for targeted interventions and more personalized management strategies. The following sections discuss these determinants in detail, contextualize their clinical implications, and outline directions for future research to enhance the care and quality of life for CKD patients affected by anemia.
Our review identified comorbidities—particularly diabetes mellitus (DM) and low body mass index (BMI)—as significant factors associated with anemia in patients with chronic kidney disease (CKD).25–27,29,34,37,39 A population-based cohort study in Northern Denmark examined the risk of anemia in adults newly diagnosed with CKD stages 3–5 and found that the incidence of anemia was significantly higher in patients with diabetes compared to those without.46 Similarly, a cross-sectional study of 353 CKD patients at an outpatient clinic in South Africa reported that individuals with diabetes had more than twice the odds of developing anemia compared to non-diabetic patients.47
Low BMI also emerged as a notable risk factor for anemia in CKD. A study conducted in two hospitals affiliated with Kaohsiung Medical University in southern Taiwan assessed the relationship between BMI and renal outcomes in CKD patients (stages 1–5) not receiving renal replacement therapy. The findings revealed a positive association between BMI and hemoglobin levels, suggesting that lower BMI was significantly correlated with lower hemoglobin levels.48 Evidence suggests that anemia in individuals with type 2 diabetes mellitus (T2DM) is often linked to impaired erythropoietin production due to diabetic kidney injury.49 Poor glycemic control further contributes to progressive vascular and renal damage, thereby increasing the risk of anemia.50 Similarly, low BMI is commonly associated with malnutrition and deficiencies in essential nutrients—such as iron, vitamin B12, and folate—which are crucial for red blood cell synthesis.2,51 These deficiencies impair erythropoiesis and contribute to the development and progression of anemia in CKD patients.
Managing these comorbidities is crucial in slowing the progression of anemia in CKD. For individuals with diabetes, effective blood glucose control through adherence to medications and dietary management is essential. In parallel, improving nutritional status and maintaining a healthy BMI can mitigate malnutrition-related anemia. Further research should focus on the development and evaluation of targeted interventions addressing comorbidity management—especially diabetes and nutritional status—as part of an integrated approach to anemia prevention and treatment in CKD populations.
Our review identified the duration of dialysis treatment as a significant determinant of anemia in CKD patients, consistent with findings from previous studies.29,30,36 Extended exposure to dialysis therapy was consistently associated with increased anemia risk. For instance, Bukhari et al reported a significant link between prolonged dialysis duration and higher prevalence of anemia in patients receiving maintenance hemodialysis.36 Similarly, Adera et al found that CKD patients with dialysis histories were four times more likely to experience anemia compared to those without such treatment.29 These results align with existing literature suggesting that chronic dialysis may exacerbate anemia through mechanisms such as inflammation,52 oxidative stress,53 ongoing blood loss during dialysis sessions,54 and impaired iron metabolism.55 Clinically, these findings underscore the importance of vigilant anemia monitoring and proactive management strategies in patients undergoing long-term dialysis. Future research should explore targeted interventions aimed at reducing dialysis-related anemia burden, potentially by optimizing dialysis procedures and adjunct therapies that mitigate treatment-related complications.
This review consistently identified kidney function as a critical determinant of anemia in patients with CKD, supported by findings from seven included studies.26,28,31–33,38,40 The relationship between declining renal function and anemia was demonstrated across various stages of CKD. For instance, Cui et al showed that higher ultrafiltration rates among maintenance hemodialysis patients were associated with lower hemoglobin levels, reflecting impaired fluid and metabolic management associated with advanced CKD.28 Similarly, Sofue et al found significantly increased anemia prevalence among patients with advanced CKD (stages G4 and G5).31 A large retrospective cohort by Lamerato et al further illustrated a clear progression-dependent association, indicating markedly increased anemia risk as kidney function deteriorated over time.32 These results align with existing literature highlighting the crucial role of declining renal function in diminishing erythropoietin production, increasing inflammation, and disrupting iron metabolism—factors known to worsen anemia severity.2,56,57 Clinically, this underscores the necessity of regular and systematic anemia screening at earlier CKD stages and proactive intervention strategies tailored to CKD progression. Future research should focus on longitudinal studies examining early intervention effectiveness, particularly emphasizing preventative strategies to manage anemia in earlier CKD stages.
This review highlights the role of biomarkers and metabolic ions as important determinants of anemia in CKD. Several studies consistently identified associations between anemia and alterations in biochemical markers such as calcium, phosphorus, albumin, C-reactive protein, serum ferritin, iron, and intact parathyroid hormone (iPTH).27,28,33–39,44,45 These findings support the multifactorial nature of anemia in CKD, where inflammation, nutritional status, and mineral bone disorder contribute to impaired erythropoiesis. Clinically, this underscores the need for comprehensive biochemical monitoring and individualized management strategies that go beyond hemoglobin and iron indices alone.
These findings are consistent with previous evidence indicating that anemia in CKD is not solely attributable to erythropoietin deficiency but is also influenced by metabolic and inflammatory disturbances.52,55 Elevated CRP may impair erythropoiesis and reduce responsiveness to erythropoiesis-stimulating agents (ESAs),58 while imbalances in calcium-phosphorus metabolism and elevated iPTH contribute to bone marrow dysfunction. Furthermore, disruptions in iron regulation, such as functional iron deficiency, are common and may occur despite normal iron stores.59,60
Clinically, these insights emphasize the importance of comprehensive biochemical assessment in anemia management. Beyond routine hemoglobin and iron testing, clinicians—particularly nephrology nurses and dietitians—should consider inflammation, nutritional status, and bone mineral metabolism. Incorporating these parameters into routine evaluation may support more personalized and effective anemia care. Future research should investigate the utility of multi-marker panels to enhance risk stratification and guide tailored interventions for anemia in CKD.
Geographic factors were consistently identified in our review as contributors to anemia among patients with chronic kidney disease (CKD).29,33 Supporting this, a recent study by Bishaw et al demonstrated that rural residence was significantly associated with anemia among CKD patients, with an adjusted odds ratio (AOR) of 2.5 (95% CI: 1.002–6.53).61 Similarly, a cross-sectional observational study by Singh et al highlighted marked differences in anemia prevalence between rural and urban CKD populations, reporting higher rates in rural areas (86.3% vs 77%).62 These disparities may be attributed to socioeconomic challenges, including lower purchasing power and limited access to iron-rich foods in rural settings. Furthermore, Kant et al noted that misconceptions about dietary causes of anemia also play a role in limiting appropriate nutritional intake.63 Taken together, these findings suggest a need for targeted interventions and policies addressing anemia among rural CKD populations. Future research should prioritize strategies that improve dietary education, enhance food security, and address socioeconomic inequalities. Addressing these upstream determinants could contribute meaningfully to reducing the burden of anemia in underserved CKD populations.
Our review identified stimulation strategies—including pharmacological agents, nutritional supplements, and physical exercise—as significant factors in managing anemia among patients with CKD. Three studies evaluated the effectiveness of stimulating agents and supplements.40–42 For instance, Li et al demonstrated that higher serum vitamin D₃ concentrations were associated with a reduced risk of anemia in patients with CKD stages 1 to 5, highlighting the potential role of vitamin D₃ in erythropoiesis regulation.40 Additionally, two studies41,42 evaluated roxadustat—a hypoxia-inducible factor prolyl hydroxylase inhibitor—as a promising alternative to conventional erythropoiesis-stimulating agents (ESAs). Both studies consistently reported that roxadustat significantly improved hemoglobin levels and treatment responsiveness compared to placebo and traditional ESAs, reinforcing its potential clinical utility. Furthermore, the supportive role of exercise interventions was highlighted in a study by Torres et al, which found that intradialytic exercise training significantly reduced the requirements for iron supplementation and erythropoietin therapy among hemodialysis patients. Importantly, this occurred without compromising hemoglobin and ferritin levels, underscoring exercise as a feasible, safe, and cost-effective supportive strategy.43 These findings align with broader evidence suggesting that integrating non-pharmacological approaches such as individualized exercise regimens into dialysis care could enhance anemia management and patient outcomes.64,65
Collectively, these findings emphasize the importance of a comprehensive approach to anemia management in CKD patients, combining pharmacological innovations, nutritional supplementation, and physical activity. Future research should focus on rigorously designed trials to further clarify optimal strategies for integrating stimulation therapies into standard CKD care pathways, aiming to achieve improved and sustained anemia control.
Study Limitations
While this review offers important insights into the determinants of anemia in patients with CKD, some limitations must be acknowledged. First, the review was limited to studies published between 2019 and 2024 and restricted to the English language. As a result, relevant studies published outside this time frame or in other languages may have been excluded, potentially narrowing the scope of evidence. Future reviews could expand the inclusion criteria to incorporate studies from a broader temporal range and include non-English literature to capture more diverse perspectives, particularly from underrepresented regions.
Second, although the review included a variety of study designs—such as cross-sectional, randomized controlled trials, cohort, and quasi-experimental studies—most included studies were cross-sectional in nature. This limits the ability to draw causal inferences regarding the identified associations. Future systematic reviews or meta-analyses should consider placing greater emphasis on longitudinal and interventional studies to better evaluate temporal relationships and intervention effectiveness.
Additionally, the variability in anemia definitions, measurement indicators, and population characteristics across studies may have contributed to heterogeneity in findings. Despite efforts to synthesize themes through a structured convergent integrated approach, the diversity in clinical settings, biomarkers, and outcome metrics may limit the generalizability of some conclusions. Standardizing outcome measures and reporting criteria across studies will be important for enabling more robust comparisons in future research.
Third, 71.4% of the included studies had sample sizes below 500 participants, and 33.3% originated from China. This concentration may introduce potential biases related to sample representativeness and geographic overrepresentation. For example, differences in erythropoietin responsiveness among Asian populations may limit the applicability of findings to other populations. Future research should aim to include larger, more geographically diverse samples to improve external validity.
Lastly, while the methodological quality of the included studies was generally high, not all studies achieved full scores, indicating some risk of bias or incomplete reporting. Future primary research should continue to strengthen design rigor and transparency, especially in areas such as sampling procedures, confounding control, and the use of validated measurement tools.
Despite these limitations, this review provides a valuable foundation for understanding the multifactorial contributors to anemia in CKD. Addressing these limitations in future work will enhance the comprehensiveness and applicability of evidence to support clinical decision-making and policy development.
Implementation in Nursing Care and Future Research
The findings of this systematic review highlight several critical factors—ranging from demographic and comorbid profiles to biomarkers, kidney function, dialysis duration, and stimulating agents—that contribute to anemia in patients with CKD. These insights offer actionable implications for nursing care and identify directions for future research. From a clinical nursing perspective, individualized anemia care plans should incorporate routine assessments of risk factors such as age, gender, comorbidities (eg, diabetes mellitus, low BMI), and biomarkers (eg, hemoglobin, ferritin, phosphorus, iPTH). Nurses play a pivotal role in monitoring these parameters, educating patients on anemia-related risks, and collaborating with multidisciplinary teams to optimize anemia management, especially among high-risk groups.
In addition, findings related to stimulating agents, vitamin D, and intradialytic exercise suggest opportunities for nurses to engage in supportive interventions. For instance, nurses can promote safe exercise programs during dialysis sessions, which have been shown to reduce pharmacological treatment needs while maintaining hemoglobin levels. Nurses should also advocate for nutrition assessment and supplement management, particularly in patients with poor nutritional status or residing in rural areas with limited access to care.
Future research should focus on longitudinal and interventional studies to examine the causal relationships among the identified factors and anemia progression. More controlled trials are needed to evaluate the effectiveness of non-pharmacological interventions, including exercise and nutrition, across diverse CKD populations. Additionally, studies exploring the impact of geographic and healthcare access disparities on anemia outcomes may inform targeted public health strategies. Integrating these findings into clinical guidelines, nurse-led protocols, and patient education materials will enhance the quality of anemia management and contribute to better overall outcomes for patients with CKD.
Conclusion
This systematic review synthesized empirical evidence on the determinants of anemia in patients with CKD. The findings reflect a range of contributing factors, including biological indicators (eg, hemoglobin, ferritin), clinical conditions (eg, comorbidities, dialysis duration), sociodemographic characteristics (eg, age, sex, geographic context), and therapeutic interventions (eg, medications, supplementation, intradialytic exercise). These factors demonstrate the multifaceted nature of anemia in CKD and underline the importance of personalized care strategies. The review also identifies opportunities for future research to explore causal pathways and intervention effectiveness across diverse populations.
Funding
This review received no specific grant from any funding agency.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ameh OI, Ekrikpo UE, Kengne AP. Preventing CKD in low- and middle-income countries: a call for urgent action. Kidney Int Rep. 2020;5(3):255–262. doi:10.1016/j.ekir.2019.12.013
2. Badura K, Janc J, Wąsik J, et al. Anemia of chronic kidney disease—a narrative review of its pathophysiology, diagnosis, and management. Biomedicines. 2024;12(6):1191. doi:10.3390/biomedicines12061191
3. Kawai K, Ishii M, Kokado Y, Horikawa T, Hoshino J. Outcomes of early versus delayed anemia treatment in nondialysis-dependent CKD. Kidney Int Rep. 2024;9(7):2056–2066. doi:10.1016/j.ekir.2024.04.030
4. Kim D, Lee J, Toyama T, et al. Prevalence and treatment patterns of anaemia in individuals with chronic kidney disease across Asia: a systematic review and meta-analysis. Nephrology. 2025;30(2):e70002. doi:10.1111/nep.70002
5. Stauffer ME, Fan T. Prevalence of anemia in chronic kidney disease in the United States. PLoS One. 2014;9(1):e84943. doi:10.1371/journal.pone.0084943
6. Chu F, Ji J, Ma Y, et al. Global burden of renal anemia in 204 countries and territories, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. medRxiv. 2024:
7. Canney M, Induruwage D, Tang M, et al. Regional variation in hemoglobin distribution among individuals with CKD: the ISN International Network of CKD Cohorts. Kidney Int Rep. 2023;8(10):2056–2067. doi:10.1016/j.ekir.2023.07.032
8. Hanna RM, Streja E, Kalantar-Zadeh K. Burden of anemia in chronic kidney disease: beyond erythropoietin. Adv Ther. 2021;38(1):52–75. doi:10.1007/s12325-020-01524-6
9. Zeng X, Liu J, Tao S, Hong HG, Li Y, Fu P. Associations between socioeconomic status and chronic kidney disease: a meta-analysis. J Epidemiol Community Health. 2018;72(4):270–279. doi:10.1136/jech-2017-209815
10. Palaka E, Grandy S, van Haalen H, McEwan P, Darlington O. The impact of CKD anaemia on patients: incidence, risk factors, and clinical outcomes—a systematic literature review. Int J Nephrol. 2020;2020:7692376. doi:10.1155/2020/7692376
11. Vondenhoff S, Schunk SJ, Noels H. Increased cardiovascular risk in patients with chronic kidney disease. Herz. 2024;49(2):95–104. doi:10.1007/s00059-024-05235-4
12. Blasco-Colmenares E, Farag YMK, Zhao D, Guallar E, Finkelstein FO. Anemia, CKD, and cognitive function: the national health and nutrition examination survey. Kidney360. 2024;5(6):895–899. doi:10.34067/KID.0000000000000354
13. Buliga-Finis ON, Ouatu A, Tanase DM, et al. Managing anemia: point of convergence for heart failure and chronic kidney disease? Life. 2023;13(6):1311. doi:10.3390/life13061311
14. Zhang J, Diwan V, Wang Z, et al. The impact of anaemia on outcomes, admissions, and costs in patients with chronic kidney disease in two public nephrology practices in Queensland: a CKD.QLD registry study. Int J Nephrol. 2023;2023:8720293. doi:10.1155/2023/8720293
15. Wittbrodt E, James G, Kumar S, et al. PUK6 cost and healthcare resource use in patients with anemia in CKD using linked US claims and electronic health records. Value Health. 2020;23:S378. doi:10.1016/j.jval.2020.04.1465
16. Finkelstein FO, Finkelstein SH. The impact of anemia treatment on health-related quality of life in patients with chronic kidney disease in the contemporary era. Adv Chronic Kidney Dis. 2019;26(4):250–252. doi:10.1053/j.ackd.2019.04.003
17. Gupta N, Wish JB. Hypoxia-inducible factor prolyl hydroxylase inhibitors: a potential new treatment for anemia in patients with CKD. Am J Kidney Dis. 2017;69(6):815–826. doi:10.1053/j.ajkd.2016.12.011
18. Fishbane S, El-Shahawy MA, Pecoits-Filho R, et al. Roxadustat for treating anemia in patients with CKD not on dialysis: results from a randomized phase 3 study. J Am Soc Nephrol. 2021;32(3):737–755. doi:10.1681/ASN.2020081150
19. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Reprint—preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89(9):873–880. doi:10.1093/ptj/89.9.873
20. JBI. Critical appraisal tools. The Joanna Briggs Institute, Faculty of Health and Medical Sciences, The University of Adelaide; 2024 [cited 2024]. Available from: https://jbi.global/critical-appraisal-tools.
21. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Joanna Briggs Institute Reviewer’s Manual. Vol. 5. The Joanna Briggs Institute; 2017.
22. JBI manual for evidence synthesis [Internet]. JBI. 2024. Available from: https://synthesismanual.jbi.global.
23. David M, Alessandro L, Jennifer T, Douglas GA. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
25. Alaidy IMM, Hasan FH, Ibrahim ESA, Alkhrsawy AMA. Serum erythropoietin hormone measurement for evaluation of anemia and red cell parameters in diabetes mellitus and diabetic kidney disease patients. Int J Med Arts. 2024;6(5):4426–4435. doi:10.21608/ijma.2024.282217.1954
26. Kim T-G, Lee S-H, Shin S, Cho J-H, Kim K-W, Ha I-H. Sex-related associations among anemia, body mass index, and kidney function in Koreans: a cross-sectional study with propensity analysis. Medicine. 2021;100(4):e23990. doi:10.1097/MD.0000000000023990
27. Lizardi Gómez L, Reyes Sánchez I, Guerrero Soto J, Rivera Antolin J, Muñoz Menjivar C, Venegas Vera A. Factors related to the presence of anemia in patients with chronic kidney disease in hemodialysis. Ann Hematol Oncol. 2021;8(1):1326.
28. Cui L, Zhang L, Li J, et al. Correlation between ultrafiltration rate and hemoglobin level and erythropoietin response in hemodialysis patients. Renal Failure. 2024;46(1):2296609. doi:10.1080/0886022X.2023.2296609
29. Adera H, Hailu W, Adane A, Tadesse A. Prevalence of anemia and its associated factors among chronic kidney disease patients at University of Gondar Hospital, Northwest Ethiopia: a hospital-based cross sectional study. Int J Nephrol Renov Dis. 2019;Volume 12:219–228. doi:10.2147/IJNRD.S216010
30. Alemu B, Techane T, Dinegde NG, Tsige Y. Prevalence of anemia and its associated factors among chronic kidney disease patients attending selected public hospitals of Addis Ababa, Ethiopia: institutional-based cross-sectional study. Int J Nephrol Renov Dis. 2021;Volume 14:67–75. doi:10.2147/IJNRD.S296995
31. Sofue T, Nakagawa N, Kanda E, et al. Prevalence of anemia in patients with chronic kidney disease in Japan: a nationwide, cross-sectional cohort study using data from the Japan Chronic Kidney Disease Database (J-CKD-DB). PLoS One. 2020;15(7):e0236132. doi:10.1371/journal.pone.0236132
32. Lamerato L, James G, van Haalen H, et al. Epidemiology and outcomes in patients with anemia of CKD not on dialysis from a large US healthcare system database: a retrospective observational study. BMC Nephrol. 2022;23(1):166. doi:10.1186/s12882-022-02778-8
33. Alagoz S, Dincer MT, Eren N, et al. Prevalence of anemia in predialysis chronic kidney disease: is the study center a significant factor? PLoS One. 2020;15(4):e0230980. doi:10.1371/journal.pone.0230980
34. Andrade JF, Dalboni MA, Clemente OC, et al. A retrospective view of the relationship of soluble Fas with anemia and outcomes in chronic kidney disease. PLoS One. 2023;18(6):e0286854. doi:10.1371/journal.pone.0286854
35. Gao Z, Hu Y, Gao Y, Ma X, Hu Z. The association of hepcidin, reticulocyte hemoglobin equivalent and anemia-related indicators on anemia in chronic kidney disease. Medicine. 2023;102(17):e33558. doi:10.1097/MD.0000000000033558
36. Bukhari H, Ahmad A, Noorin A, et al. Association of anemia with parathyroid hormone levels and other factors in patients with end‐stage renal disease undergoing hemodialysis: a cross‐sectional, real‐world data study in Pakistan. Int J Clin Pract. 2023;2023(1):7418857. doi:10.1155/2023/7418857
37. Deng Y, Liu H, Lin N, Ma L, Fu W. Influence of dry weight reduction on anemia in patients undergoing hemodialysis. J Int Med Res. 2019;47(11):5536–5547. doi:10.1177/0300060519872048
38. Kato K, Nakashima A, Ohkido I, Kasai K, Yokoo T. Association between serum phosphate levels and anemia in non-dialysis patients with chronic kidney disease: a retrospective cross-sectional study from the Fuji City CKD Network. BMC Nephrol. 2023;24(1):244. doi:10.1186/s12882-023-03298-9
39. Li F, Ye X, Yang G, et al. Relationships between blood bone metabolic biomarkers and anemia in patients with chronic kidney disease. Renal Failure. 2023;45(1):2210227. doi:10.1080/0886022X.2023.2210227
40. Li M, Xu J, Wan Q, et al. Relationship between serum vitamin D3 concentration and anaemia in patients with chronic kidney disease in China. J Int Med Res. 2021;49(5):03000605211012231. doi:10.1177/03000605211012231
41. Coyne DW, Roger SD, Shin SK, et al. Roxadustat for CKD-related anemia in non-dialysis patients. Kidney Int Rep. 2021;6(3):624–635. doi:10.1016/j.ekir.2020.11.034
42. Hou Y-P, Mao X-Y, Wang C, et al. Roxadustat treatment for anemia in peritoneal dialysis patients: a randomized controlled trial. J Formos Med Assoc. 2022;121(2):529–538. doi:10.1016/j.jfma.2021.06.004
43. Torres E, Aragoncillo I, Moreno J, et al. Exercise training during hemodialysis sessions: physical and biochemical benefits. Ther Apher Dial. 2020;24(6):648–654. doi:10.1111/1744-9987.13469
44. Yu P-H, Lin M-Y, Chiu Y-W, et al. Low serum iron is associated with anemia in CKD stage 1–4 patients with normal transferrin saturations. Sci Rep. 2021;11(1):8343. doi:10.1038/s41598-021-87401-w
45. Zhang C, Wang J, Xie X, Sun D. Low serum vitamin D concentration is correlated with anemia, microinflammation, and oxidative stress in patients with peritoneal dialysis. J Transl Med. 2021;19:1–9. doi:10.1186/s12967-021-03077-w
46. Vestergaard SV, Uffe H-J, Heleen VH, et al. Risk of anemia in patients with newly identified chronic kidney disease – a population-based cohort study. Clin Epidemiol. 2020;12:953–962. doi:10.2147/CLEP.S259648
47. Nalado AM, Mahlangu JN, Waziri B, et al. Ethnic prevalence of anemia and predictors of anemia among chronic kidney disease patients at a tertiary hospital in Johannesburg, South Africa. Int J Nephrol Renovasc Dis. 2019;12:19–32. doi:10.2147/IJNRD.S179802
48. Hung -C-C, Yu P-H, Niu S-W, et al. Association between body mass index and renal outcomes modified by chronic kidney disease and anemia: the obesity paradox for renal outcomes. J Clin Med. 2022;11(10):2787. doi:10.3390/jcm11102787
49. Thomas MC. The high prevalence of anemia in diabetes is linked to functional erythropoietin deficiency. Semin Nephrol. 2006;26(4):275–282. doi:10.1016/j.semnephrol.2006.05.003
50. Antwi-Bafour S, Hammond S, Adjei JK, Kyeremeh R, Martin-Odoom A, Ekem I. A case–control study of prevalence of anemia among patients with type 2 diabetes. J Med Case Rep. 2016;10(1):110. doi:10.1186/s13256-016-0889-4
51. Portolés J, Martín L, Broseta JJ, Cases A. Anemia in chronic kidney disease: from pathophysiology and current treatments, to future agents. Front Med. 2021;8. doi:10.3389/fmed.2021.642296
52. Matsuoka T, Abe M, Kobayashi H. Iron metabolism and inflammatory mediators in patients with renal dysfunction. Int J Mol Sci. 2024;25(7):3745. doi:10.3390/ijms25073745
53. Ling XC, Kuo K-L. Oxidative stress in chronic kidney disease. Ren Replace Ther. 2018;4(1):53. doi:10.1186/s41100-018-0195-2
54. Vaziri ND. Understanding iron: promoting its safe use in patients with chronic kidney failure treated by hemodialysis. Am J Kidney Dis. 2013;61(6):992–1000. doi:10.1053/j.ajkd.2012.10.027
55. Gluba-Brzózka A, Franczyk B, Olszewski R, Rysz J. The influence of inflammation on anemia in CKD patients. Int J Mol Sci. 2020;21(3):725. doi:10.3390/ijms21030725
56. Bissinger R, Schaefer L, Bohnert BN, et al. GFR is a key determinant of red blood cell survival in anemia associated with progressive CKD. Kidney Int Rep. 2025;10(3):730–742. doi:10.1016/j.ekir.2024.12.023
57. Daimon S. Reconsideration of the anemia management strategy for chronic kidney disease and dialysis patients. Ren Replace Ther. 2025;11(1):16. doi:10.1186/s41100-025-00612-z
58. Bradbury BD, Critchlow CW, Weir MR, Stewart R, Krishnan M, Hakim RH. Impact of elevated C-reactive protein levels on erythropoiesis- stimulating agent (ESA) dose and responsiveness in hemodialysis patients. Nephrol Dial Transplant. 2009;24(3):919–925. doi:10.1093/ndt/gfn543
59. Hruska KA, Sugatani T, Agapova O, Fang Y. The chronic kidney disease—Mineral bone disorder (CKD-MBD): advances in pathophysiology. Bone. 2017;100:80–86. doi:10.1016/j.bone.2017.01.023
60. NIDDK. Mineral & bone disorder in chronic kidney disease. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); 2021 [cited 2025]. Available from: https://www.niddk.nih.gov/health-information/kidney-disease/mineral-bone-disorder#:~:text=3-,Slowed%20bone%20growth%20and%20bone%20deformities,calcium%20can%20harm%20your%20bones.
61. Bishaw F, Belay Woldemariam M, Mekonen G, Birhanu B, Abebe A. Prevalence of anemia and its predictors among patients with chronic kidney disease admitted to a teaching hospital in Ethiopia: a hospital-based cross-sectional study. Medicine. 2023;102(6):e31797. doi:10.1097/MD.0000000000031797
62. Singh PP, Patel PS, Krishna A, Kuntal S, Kumar S, Kumar O. Epidemiology and clinical characteristics of chronic kidney disease in Bihar: a cross-sectional study from a single center. Cureus. 2024;16(7):e64719. doi:10.7759/cureus.64719
63. Kant S, Kumar R, Malhotra S, Kaur R, Haldar P. Prevalence and determinants of anemia among adult males in a rural area of Haryana, India. J Epidemiol Glob Health. 2019;9(2):128–134. doi:10.2991/jegh.k.190513.001
64. Battaglia Y, Baciga F, Bulighin F, et al. Physical activity and exercise in chronic kidney disease: consensus statements from the Physical Exercise Working Group of the Italian Society of Nephrology. J Nephrol. 2024;37(7):1735–1765. doi:10.1007/s40620-024-02049-9
65. Correa HL, Rosa TS, Santos RL, et al. The impact of different exercise modalities on chronic kidney disease: an umbrella review of meta-analyses. Front Physiol. 2025;15:1444976. doi:10.3389/fphys.2024.1444976
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anaemia, Morphological Classification and Its Associated Risk Factors Among Lactating Mothers at Mbarara City Council Health Centre IV, Southwestern Uganda
Clinton O, Micheal K, Namyalo Angella K, Mary M, Mike M, Muwanguzi E, Okongo B, Wagubi R
Journal of Blood Medicine 2022, 13:473-481
Published Date: 2 September 2022
Clinical Evaluation of Dapagliflozin in the Management of CKD: Focus on Patient Selection and Clinical Perspectives
Nashar K, Khalil P
International Journal of Nephrology and Renovascular Disease 2022, 15:289-308
Published Date: 1 November 2022
Exploring the Agreement Between Self-Reported Medication Adherence and Pharmacy Refill-Based Measures in Patients with Kidney Disease
Murali KM, Mullan J, Roodenrys S, Cheikh Hassan HI, Lonergan MA
Patient Preference and Adherence 2022, 16:3465-3477
Published Date: 30 December 2022
Exploration of the Risk Factors of Anemia in Patients with Tuberculous Meningitis in South China
Wen A, Leng EL, Cao WF, Xiang ZB, Rao W, Cai W, Zhou YL, Hu F, Wu LF, Zhang P, Liu SM
Neuropsychiatric Disease and Treatment 2023, 19:369-377
Published Date: 16 February 2023
Real-Life Anemia Management Among Patients with Non-Dialysis-Dependent Chronic Kidney Disease in Three European Countries

Fliser D, Mata Lorenzo M, Houghton K, Ainsworth C, Blogg M, González de Antona Sánchez E, Portoles J
International Journal of Nephrology and Renovascular Disease 2023, 16:115-129
Published Date: 13 April 2023