")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Development and Validation of a UPLC-MS/MS Detection Method of Baricitinib for Therapeutic Drug Monitoring in COVID-19 Patients
Authors Zhan R , Shen Y , Fu H, Wu H, Chen X , Yu Y, Xu RA
Received 28 November 2024
Accepted for publication 9 May 2025
Published 9 June 2025 Volume 2025:19 Pages 4957—4966
DOI https://doi.org/10.2147/DDDT.S509176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Ruanjuan Zhan,* Yuxin Shen,* Haoxin Fu, Hualu Wu, Xiaohai Chen, Yige Yu, Ren-Ai Xu
Department of Pharmacy, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yige Yu, Email [email protected] Ren-Ai Xu, Email [email protected]
Background: Baricitinib is widely used as a selective Janus kinase (JAK) inhibitor for the treatment of immune-mediated inflammatory diseases in clinic. It is now successfully applied in reducing inflammation and suppressing COVID-19-associated immune dysregulation. As knowledge of the appropriate plasma level of baricitinib in COVID-19 patients is deficient, the measurement of the level of baricitinib in plasma during treatment is necessary and important.
Purpose: The aim of this study was to establish a bioanalytical method to detect the concentration of baricitinib in COVID-19 patients’ plasma by ultra performance liquid chromatography tandem mass spectrometry (UPLC-MS/MS).
Methods: The preparation process of the injected sample was to spike 100 μL of plasma and 10 μL of internal standard (IS, upadacitinib) working solution, then add 1:3 of acetonitrile to obtain the supernatant. The intra-day and inter-day precision and accuracy, matrix effect, recovery, and stability of the established methodology were all required.
Results: The method was established to determine the plasma levels in 22 COVID-19 patients. After taking 2 mg/day or 4 mg/day of baricitinib, the mean plasma concentrations of the patients were 15.36 ng/mL and 12.64 ng/mL, respectively.
Conclusion: This novel UPLC-MS/MS method enables rapid and accurate determination of baricitinib concentrations in human plasma, which is suitable for the therapeutic drug monitoring (TDM) of baricitinib.
Keywords: baricitinib, UPLC-MS/MS, drug monitoring, COVID-19
Introduction
Baricitinib (OlumiantTM) is a small-molecule, orally active Janus kinase (JAK) 1/2 selective inhibitor that could influence immune responses by triggering Janus Kinase-Signal Transducer and Activator of Transcription (JAK-STAT) signaling pathways and regulating transcription in reaction to external cytokines, interferons, and growth factors.1 Baricitinib is already authorized for the treatment of immune-mediated inflammatory conditions like rheumatoid arthritis (RA), alopecia areata (AA), and atopic dermatitis (AD).2–4
Thus, baricitinib has been successfully applied in reducing inflammation and suppressing COVID-19-associated immune dysregulation.5 The FDA approved baricitinib as the first immunomodulatory treatment for COVID-19 in hospitalized adults who require supplemental oxygen, noninvasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO) in 2022.6 Several clinical trials have been implemented to evaluate the efficacy and safety of baricitinib in COVID-19. Baricitinib was shown to reduce 28-day all-cause mortality in both RECOVERY and COV-BARRIER studies.7,8 The ACTT-2 and ACTT-4 study showed that the combination of baricitinib and remdesivir was superior to remdesivir alone or dexamethasone plus remdesivir in shortening recovery time, enhancing clinical status improvement or reducing adverse events in hospitalized patients with COVID-19 requiring supplemental oxygen or noninvasive ventilation.9,10
Research has also demonstrated that baricitinib hinders virus endocytosis and decreases viral assembly by blocking the enzymes AP-2 Associated Protein Kinase 1 (AAK1) and cyclin-G Associated Kinase (GAK) in alveolar type 2 (AT2) cells.11 To put it simply, baricitinib exerts dual antiviral effects by adjusting the inflammatory response through JAK1/2 and blocking viral entry through AAK1 and GAK.
Although baricitinib is effective in treating patients with COVID-19, it still carries potential risks. Currently, baricitinib is administered at a fixed dose 4 mg once daily orally, accounting for limited between-subject variability (BSV) such as renal impairment or cytopenias.12 Most pharmacokinetic profiles are derived from studies conducted on healthy volunteers, patients of other disease, whereas limited data are available for COVID-19 patients.13 Baricitinib has also been associated with elevated liver enzymes, thrombocytosis, increased creatine phosphokinase levels, neutropenia, deep vein thrombosis, pulmonary embolism, and urinary tract infection (UTI) in COVID-19 patients.12 Therapeutic drug monitoring (TDM) can be a valuable method to ensure the safe and effective use of baricitinib in managing COVID-19, improving the treatment’s risk/benefit ratio. In this study, a well-established methodology was developed and used to determine the plasma concentration of baricitinib in patients infected with COVID-19.
Materials and Methods
Chemicals and Reagents
Baricitinib (Figure 1A) and upadacitinib (internal standard, IS, Figure 1B) were provided by Beijing Sunflower Technology Development Co., Ltd (Beijing, China). Methanol and acetonitrile were HPLC grades supplied by Merck (Darmstadt, Germany). Formic acid was obtained from Anaqua Chemicals Supply (ACS, American). Ultrapure water (MS grade water) was supplied by the Milli-Q pure water system (Millipore, Bedford, USA).
 |
Figure 1 Fragmentation pattern and product ion spectra of baricitinib (A) and IS (B) in this study. |
UPLC-MS/MS Conditions
UPLC-MS/MS analysis included a Waters Xevo TQ-S triple quadrupole tandem mass spectrometer and a Waters Acquity UPLC I-Class system (Milford, MA, USA). An Acquity BEH C18 column (2.1 mm × 50 mm, 1.7 μm; Milford, MA, USA) was used to chromatographic separation of baricitinib and IS at 40°C with acetonitrile (solution A) and 0.1% formic acid (solution B) as the mobile phase. The mobile phase in gradient elution was as follows: 0–0.5 min at 90% B, 0.5–1.0 min at 90–10% B, 1.0–1.4 min at 10% B, 1.4–1.5 min at 10–90% B. And, the entire run time was 2.0 min.
Mass spectrometry measurements were conducted using a Waters Xevo TQ-S triple quadrupole tandem mass spectrometer in positive ion mode with electrospray ionization (ESI). The ion transitions of baricitinib and IS in the mass spectrometry monitored by multiple reaction monitoring (MRM) were m/z 372.44 → 250.97 and m/z 380.90 → 255.99, respectively. The parameters optimized for mass spectrometry of baricitinib and IS included cone voltages of 20 V and 30 V, and collision energies of 30 eV and 25 eV, respectively.
Standard Curves and Stock Solution
Prior to preparing the quality control (QC) and standard curves, baricitinib and IS were each dissolved in methanol at a concentration of 1.00 mg/mL. Subsequently, each concentration of the working solution for the calibration was diluted with methanol from the above stock solution of baricitinib. The concentration points of the standard curve were 1, 2, 5, 10, 20, 50, 75 and 100 ng/mL. The working solution of IS was diluted with methanol to form the concentration of 200 ng/mL. QC samples had four different concentrations with lower limit of quantification (LLOQ) levels (1 ng/mL), low (LQC, 2 ng/mL), medium (MQC, 40 ng/mL) and high (HQC, 80 ng/mL). Finally, all stock solutions were stored in a −80°C freezer, while the working solutions were kept in a 4°C refrigerator for subsequent quantitative analysis.
Human Samples
The retrospective study enrolled adult patients who were infected with COVID-19 and received baricitinib during treatment. The inclusion criteria: (1) age ≥18 years old; (2) hospitalized with laboratory outcome and CT confirmed SARS-CoV-2 infection; (3) requiring supplemental oxygen, noninvasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO); (4) baricitinib’s dosage was 2 mg or 4 mg once daily. The exclusion criteria: (1) A different dosage as 2 mg twice or three times daily; (2) Death, expected discharge or transfer within 48 hours after diagnosis.
Baricitinib was given at a standard dose of 4 mg once daily orally, with adjustments made for cytopenias (interrupt medication, absolute lymphocyte count <200 cells/μL or absolute neutrophil count <500 cells/μL), hepatic impairment (interrupt medication, drug-induced liver injury), or renal impairment (2 mg once daily, eGFR between 30 and <60 mL/min/1.73m2; 1 mg once daily, eGFR between 15 and <30 mL/min/1.73m2), according to the pharmaceutical instructions of baricitinib.12 Blood samples were collected at a steady state plasma concentration. Plasma was separated from peripheral blood sampled in EDTA K3 anticoagulant tubes by centrifugation at 4000 × g for 8 min and stored at −80°C until analysis.
All patient data used in this study were handled with strict confidentiality and in compliance with the ethical principles outlined in the Declaration of Helsinki. The study protocol was approved by the Ethics Committee in Clinical Research of the First Affiliated Hospital of Wenzhou Medical University (Approval number: KY2024-R037). The Ethics Committee granted a waiver for the requirement for written informed consent due to the retroactive nature of the study.
Samples Preparation
All plasma samples were precipitated with acetonitrile after the addition of the IS working solution. The 100 μL plasma sample was added to an Eppendorf (EP) tube containing 10 μL of the IS working solution (200 ng/mL concentration). After the above mixing, acetonitrile was added in a ratio of 1:3 to precipitate plasma proteins. After vortexing, the samples were centrifuged at 13,000 × g for 10 min at 4°C. A 100 μL supernatant was injected into the UPLC-MS/MS system for analysis.
Method Validation
Method validation was conducted according to the FDA’s “Guidance for Industry: Bioanalytical Method Validation”.14
Selectivity and Specificity
The selectivity and specificity of the analytical method were investigated by analyzing the chromatographic profile of blank plasma (Figure 2A), baricitinib and IS added in blank plasma (Figure 2B) as well as in plasma of patients treated with baricitinib (Figure 2C) to check for endogenous interference at the retention times of the analyte and IS.
 |
Figure 2 Representative chromatograms of baricitinib and IS in human plasma: (A) blank plasma; (B) blank plasma spiked with analyte at LLOQ and IS; (C) human plasma sample after oral dose of 4 mg baricitinib. |
Calibration Curve and LLOQ
The concentration range of the standard curve for baricitinib was 1–100 ng/mL. At least 8 concentration points were set up in this range to fit linearity. Each calibration standard needed to be accurate within ±20% of the nominal concentration at the LLOQ and within ±15% at other levels. LLOQ was defined as the lowest concentration of the calibration curve.
Precision and Accuracy
Intra-day precision and accuracy were measured at the same day with 4 different levels of QC samples. Inter-day precision and accuracy were calculated by analyzing 6 QC samples for 3 consecutive days. Accuracy is expressed as the percentage difference between the mean value of the measurement and the standard value. Precision is expressed as a percentage of the sample variance versus the mean. Except for the LLOQ, where ±20% was acceptable, accuracy and precision needed to be within ±15% at each concentration level.
Matrix Effect and Extraction Recovery
In this study, the recovery and matrix effects were calculated as follows:
Recovery = peak area of extract sample/peak area of blank extract spiked with neat solution.
Matrix effect = peak area of blank extract spiked with neat solution/peak area of neat solution.
It was recommended to test a minimum of six samples.
Stability
The stability test of baricitinib was carried out under different experimental conditions, and the detection accuracy and precision of baricitinib in samples were calculated. The test was conducted under the following different conditions: 1. Leave at room temperature for 2 h; 2. Autosampler 10°C for 4 h; 3. Three complete freeze–thaw cycles (−80°C to room temperature); 4. Leave at −80°C for 5 weeks. According to the requirements, the accuracy and precision of each sample should be within ± 15% at each concentration level.
Results
Method Development
A comparison and analysis of solid-phase extraction, liquid–liquid extraction, and protein precipitation method was conducted to improve the practicality and convenience of sample preparation. The protein precipitation method was more in line with the purpose of this study, with good recovery, small matrix effects, and fast analysis. Acetonitrile had a lower matrix effect and higher sensitivity response than methanol and was ultimately selected as the precipitation solvent for protein precipitation.
In order to produce a good analytical chromatogram for baricitinib by UPLC-MS/MS, the chromatographic conditions, and the collision energy of the mass spectrometry had been carefully explored. We tested two types of columns for baricitinib with Acquity BEH C18 column (2.1 mm × 50 mm, 1.7 μm; Milford, MA, USA) and Acquity BEH C18 column (2.1 mm × 100 mm, 1.7 μm; Milford, MA, USA). After observing the parameters and symmetry of the peak shape, we selected the first column for chromatographic analysis, which also had a short retention time. In addition, acetonitrile and 0.05% trifluoroacetic acid as the mobile phase was used and eluted at a flow rate of 0.4 mL/min, but the sensitivity was poor and the peak pattern was distorted. Therefore, we made a new choice of acetonitrile and 0.1% formic acid as the mobile phase, and the results shown in Figure 2 were obtained.
The transition of ion energy in a mass spectrometer is critical for the detection intensity of parent ion and daughter ion. If the collision energy is too low, the parent ion cannot form a daughter ion; if the collision energy is too high, the daughter ion may broken into smaller ions. Finally, under our groping, the cone voltages for baricitinib and IS were 20 V and 30 V, and the collision energy were 30 eV and 25 eV, respectively. Baricitinib and IS generated protonated molecular ions in positive ion mode. The most abundant fragment ions in MRM were m/z 372.44→250.97 for baricitinib and m/z 380.90→255.99 for IS, respectively (Figure 1).
Method Validation
Selectivity
Figure 2 presented typical chromatograms under three distinct conditions: a sample from blank plasma (A; without analyte or IS), a sample from blank plasma spiked with the target analyte at LLOQ concentration and IS (B), and a genuine human sample acquired after oral administration of 4 mg baricitinib (C). From the Figure 2, the retention time of both baricitinib and IS in the chromatogram was 1.15 min. The detection of baricitinib and IS in human plasma showed that there was no interference, and it showed strong detection signal and good peak shape. Therefore, the method had good selectivity for baricitinib in this study.
Calibration Curve and LLOQ
The linear regression equation of baricitinib for the calibration curve obtained in this study was y = (0.00343954*x + 0.00411251, r2 = 0.994). The LLOQ was 1 ng/mL for baricitinib. In addition, the intra-day precision (RSD%) and accuracy (RE%) were 3.2% and 14.6%, respectively, while the inter-day precision and accuracy were 6.3% and 11.4%, respectively (Table 1).
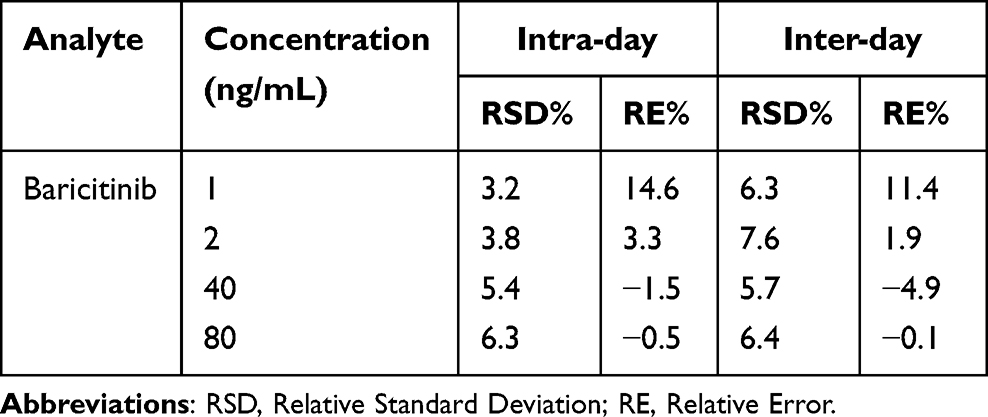 |
Table 1 The Precision and Accuracy of Baricitinib in Human Plasma (n = 6) |
Accuracy and Precision
The precision and accuracy of the method were calculated by measuring the concentrations of QC samples for three consecutive days, including intra-day and inter-day precision and accuracy. The QC sample concentrations were 1, 2, 40, and 80 ng/mL, respectively (n = 6). The results were shown in Table 1. Intra-day precision ranged from 3.2% to 6.3%, and accuracy covered from −1.5% to 14.6%; inter-day precision ranged from 5.7% to 7.6%, and accuracy covered from −4.9% to 11.4%. According to the requirements of −15% < RE < 15% and RSD <15%, the method met the requirements.
Recovery and Matrix Effect
The average recovery of baricitinib ranged from 101.1% to 103.8%, and the matrix effect of baricitinib ranged from 99.5% to 108.2% for QC samples at 2, 40 and 80 ng/mL (Table 2).
 |
Table 2 Recovery and Matrix Effect of Baricitinib in Human Plasma (n = 6) |
Stability
In order to explore the stability of baricitinib in human plasma, we performed the test under the following different conditions: 1. Leave at room temperature for 2 h; 2. Autosampler 10°C for 4 h; 3. Three complete freeze–thaw cycles (−80°C to room temperature); 4. Leave at −80°C for 5 weeks. The results are shown in Table 3, and they were considered stable after data analysis.
 |
Table 3 Stability Results of Baricitinib in Plasma Under Different Conditions (n = 6) |
Analysis of Human Samples
A total of 22 COVID-19 patients were treated with baricitinib, and plasma concentration of baricitinib was measured throughout the study. The median detecting time point was 7–8 days after once-daily baricitinib administration. The mean plasma concentration of patients was 15.36 ng/mL at 2 mg/day and 12.64 ng/mL at 4 mg/day (Table 4).
 |
Table 4 Individualized Monitoring of Baricitinib in 22 COVID-19 Patients |
Discussion
TDM is a strategy for maximizing drug effectiveness and lowering the incidence of adverse drug effects (ADRs) across different drug categories, especially in cases where pharmacokinetics is influenced by physiological or pathological factors.15 In healthy volunteers, the pharmacokinetics of baricitinib follow a linear pattern, showing a dose-proportional rise in systemic exposure within the therapeutic dose range.13 When administered orally, baricitinib is absorbed rapidly, achieving a median peak time of roughly 1 hour, with an 80% absolute bioavailability, and is predominantly spread throughout tissues.12 A population pharmacokinetic (popPK) analysis in 18 adult and pediatric patients with rheumatoid arthritis shows the average area under the concentration–time curve (AUC) was 1.83 times greater than that of baricitinib in adult patients at therapeutic doses.16 Thus Cafaro et al presented an LC-MS/MS approach for the TDM of baricitinib, intended to support refining therapy in children.17 Massart found that there was notable variability among patients and relatively low trough concentrations and AUC in critically ill COVID-19 patients taking the standard 4 mg/day dose of baricitinib.18 Another research showed that in a critically ill COVID-19 patient undergoing continuous venovenous haemodialysis (CVVHD), a 2-mg dose of baricitinib results in a Cmax similar to that in healthy individuals, although total clearance is reduced to approximately 20%.19 Consequently, reliable techniques for measuring drug levels in patient plasma are vital for advancing TDM practices and detailing the pharmacokinetic/pharmacodynamic characteristics of baricitinib.
The quantitative detection of baricitinib in plasma established in this study has certain advantages. Protein precipitation technology is a popular purification method and is widely used as a rapid sample preparation technique for bioanalysis. Veeraraghavan’s study reported a 7.5 min run time for quantifying the concentration of baricitinib in plasma using protein precipitation.20 Tachet J developed and validated a 7 min analytical run time assay in plasma of 6 major currently used JAKi in patients with polycythemia vera (PV).21 Koller D used microelution-solid phase extraction in protein precipitation and applied it to the simultaneous monitoring of 11 tyrosine kinase inhibitors (TKIs) in human plasma.22 Ezzeldin E extracted baricitinib from plasma by liquid–liquid extraction for observation of baricitinib in rat plasma and applied it in a pharmacokinetic study.23 Compared to those study, the analysis time of baricitinib was reduced to 2.0 min with more simplified processing steps. Compared with liquid–liquid extraction, the protein precipitation technology of acetonitrile as precipitant used in this study had a good recovery and matrix effect, and had obvious advantages in the sample preparation process, with simple process operation and small precipitant dosage. Therefore, the methodology established in this study is a high-efficiency detection method.
The outcome of human samples showed that there was no difference in gender, age, BMI, eGFR, urine output, concomitant use of antiviral drugs, steroids, or traditional Chinese medicine between the 2 mg and 4 mg groups. We also observed a lower plasma concentration of baricitinib at a dose of 4 mg/day compared to the 2 mg dose. This may be due to the underlying conditions in the 2 mg group, which included renal insufficiency, post-liver/renal transplant, or post-allogeneic hematopoietic stem cell transplantation, making them more complicated than those in the 4 mg group. And the number of patients was small and the sample collection time points between the two groups were not even, which was a limitation of this study. In addition, concomitant medications may affect the outcome of baricitinib plasma concentration.
Conclusion
We developed a novel and accurate UPLC-MS/MS method to measure plasma levels of baricitinib in COVID-19 patients. Furthermore, monitoring the plasma levels of baricitinib in COVID-19 patients helps in developing personalized treatment strategies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Philips RL, Wang Y, Cheon H, et al. The JAK-STAT pathway at 30: much learned, much more to do. Cell. 2022;185(21):3857–3876. doi:10.1016/j.cell.2022.09.023
2. Szekanecz Z, Buch MH, Charles-Schoeman C, et al. Efficacy and safety of JAK inhibitors in rheumatoid arthritis: update for the practising clinician. Nat Rev Rheumatol. 2024;20(2):101–115. doi:10.1038/s41584-023-01062-9
3. Messenger A, Harries M. Baricitinib in alopecia areata. N Engl J Med. 2022;386(18):1751–1752. doi:10.1056/NEJMe2203440
4. Bieber T. Atopic dermatitis: an expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. 2022;21(1):21–40. doi:10.1038/s41573-021-00266-6
5. Stebbing J, Sánchez Nievas G, Falcone M, et al. JAK inhibition reduces SARS-CoV-2 liver infectivity and modulates inflammatory responses to reduce morbidity and mortality. Sci Adv. 2021;7:eabe4724. doi:10.1126/sciadv.abe4724
6. Rubin R. Baricitinib is first approved COVID-19 immunomodulatory treatment. JAMA. 2022;327(23):2281.
7. RECOVERY Collaborative Group. Baricitinib in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial and updated meta-analysis. Lancet. 2022;400(10349):359–368. doi:10.1016/S0140-6736(22)01109-6
8. Marconi VC, Ramanan AV, de Bono S, et al; COV-BARRIER Study Group. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled Phase 3 trial. Lancet Respir Med. 2021;9(12):1407–1418. doi:10.1016/S2213-2600(21)00331-3
9. Kalil AC, Patterson TF, Mehta AK, et al; ACTT-2 Study Group Members. Baricitinib plus remdesivir for hospitalized adults with covid-19. N Engl J Med. 2021;384(9):795–807. doi:10.1056/NEJMoa2031994
10. Wolfe CR, Tomashek KM, Patterson TF, et al; ACTT-4 Study Group. Baricitinib versus dexamethasone for adults hospitalised with COVID-19 (ACTT-4): a randomised, double-blind, double placebo-controlled trial. Lancet Respir Med. 2022;10(9):888–899. doi:10.1016/S2213-2600(22)00088-1
11. Stebbing J, Phelan A, Griffin I, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20(4):400–402. doi:10.1016/S1473-3099(20)30132-8
12. European Medicines Agency (EMA). Olumiant. 2023. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/olumiant#product-information-section.
13. Shi JG, Chen X, Lee F, et al. The pharmacokinetics, pharmacodynamics, and safety of baricitinib, an oral JAK 1/2 inhibitor, in healthy volunteers. J Clin Pharmacol. 2014;54:1354–1361. doi:10.1002/jcph.354
14. U.S. Department of Health and Human Services Food and Drug Administration (FDA), Center for Drug Evaluation and Research (CDER), Center for Veterinary Medicine (CVM), Bioanalytical Method Validation Guidance for Industry, Center for Drug Evaluation and Research. 2018. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry.
15. Barco S, Mesini A, Barbagallo L, et al. A liquid chromatography-tandem mass spectrometry platform for the routine therapeutic drug monitoring of 14 antibiotics: application to critically ill pediatric patients. J Pharm Biomed Anal. 2020;186:113273. doi:10.1016/j.jpba.2020.113273
16. Kim H, Brooks K, Tang C, et al. Pharmacokinetics, pharmacodynamics, and proposed dosing of the oral JAK1 and JAK2 inhibitor baricitinib in pediatric and young adult CANDLE and SAVI patients. Clin Pharmacol Ther. 2018;104(2):364–373. doi:10.1002/cpt.936
17. Cafaro A, Baiardi G, Pigliasco F, et al. A novel LC-MS/MS method for therapeutic drug monitoring of baricitinib in plasma of pediatric patients. Ther Drug Monit. 2024;46(1):67–72. doi:10.1097/FTD.0000000000001128
18. Massart N, Fillatre P, Lemaitre F, Mari A, Tron C. Pharmacokinetics of baricitinib in critically ill COVID-19 patients. Clin Biochem. 2023;118:110601. doi:10.1016/j.clinbiochem.2023.110601
19. Palmer ME, Belcher RM, Engeleit A, Wenzler E, Bulman ZP, Benken ST. Pharmacokinetics and dialytic clearance of baricitinib during in vivo continuous venovenous haemodialysis in a patient with COVID-19. Int J Antimicrob Agents. 2023;62(3):106920. doi:10.1016/j.ijantimicag.2023.106920
20. Veeraraghavan S, Thappali SR, Viswanadha S, Vakkalanka S, Rangaswamy M. Simultaneous quantification of baricitinib and methotrexate in rat plasma by LC-MS/MS: application to a pharmacokinetic study. Sci Pharm. 2016;84(2):347–359. doi:10.3797/scipharm.1510-08
21. Tachet J, Versace F, Mercier T, et al. Development and validation of a multiplex HPLC-MS/MS assay for the monitoring of JAK inhibitors in patient plasma. J Chromatogr B Analyt Technol Biomed Life Sci. 2023;1230:123917. doi:10.1016/j.jchromb.2023.123917
22. Koller D, Vaitsekhovich V, Mba C, et al. Effective quantification of 11 tyrosine kinase inhibitors and caffeine in human plasma by validated LC-MS/MS method with potent phospholipids clean-up procedure. Application to therapeutic drug monitoring. Talanta. 2020;208:120450. doi:10.1016/j.talanta.2019.120450
23. Ezzeldin E, Iqbal M, Asiri YA, et al. A hydrophilic interaction liquid chromatography-tandem mass spectrometry quantitative method for determination of baricitinib in plasma, and its application in a pharmacokinetic study in rats. Molecules. 2020;25(7):1600. doi:10.3390/molecules25071600
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.