")
Back to Journals » Patient Related Outcome Measures » Volume 15
Development and Validation of the Self-Management Questionnaire for Patients with Lower Extremity Arterial Disease Who Underwent Endovascular Revascularization
Authors Shi M, Yang X, Song P, Xiong H, Wang D, Quan X, Liu X, Hu X, Zhou J
Received 23 October 2024
Accepted for publication 12 December 2024
Published 21 December 2024 Volume 2024:15 Pages 301—314
DOI https://doi.org/10.2147/PROM.S493159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Meihong Shi,1– 3,* Xi Yang,4,* Pan Song,1 Huarong Xiong,5 Dan Wang,6 Xiaoyan Quan,1 Xinjun Liu,7 Xiuying Hu,3 Jia Zhou8
1School of Nursing, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 2Nursing Department, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 3Innovation Center of Nursing Research, West China Hospital, Sichuan University/Nursing Key Laboratory of Sichuan Province/ West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 4Department of Vascular Surgery, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 5Department of Endocrinology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 6Department of Respiratory and Critical Care Medicine, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, People’s Republic of China; 7Department of Vascular Surgery, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 8School of Humanities and Management Science, Southwest Medical University, Luzhou, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jia Zhou; Xiuying Hu, Email [email protected]; [email protected]
Introduction: To develop and psychometrically validate the Self-management Questionnaire for Patients with Lower Extremity Arterial Disease Patients Who Underwent Endovascular Revascularization (LESQ).
Methods: We developed the LESQ and validated it in a Chinese population. A three-round cross-sectional descriptive survey in six hospitals in China, involving samples of 271, 269, and 623 participants, respectively. The surveys were conducted between February 2021 to March 2022.
Results: The final version of the LESQ, with 22 items, was divided into three domains using exploratory factor analysis: medical management, rehabilitation exercise management, and daily life management. The questionnaire had good internal consistency reliability, with a Cronbach’s α of 0.953 and good retest reliability, with the coefficients of 0.917, respectively. The content validity of the LESQ was 0.939. The three domains of the questionnaire were confirmed by confirmatory factor analysis. The optimal cut-off points were 52 and 70, respectively, using latent profile analysis.
Discussion: The LESQ is a new self-report questionnaire for measuring self-management ability with good reliability and validity through validation.
Keywords: lower extremity arterial disease, endovascular revascularization, self-management, questionnaire, reliability, validity
Introduction
Lower-extremity arterial disease (LEAD) currently affects 200 million patients and is associated with elevated cardiovascular morbidity and mortality.1–3 It has gradually become the third major complication of atherosclerosis after coronary heart disease and stroke, with the aging of the global population, as well as a threat to the health of the elderly. It is estimated that approximately 45.3 million patients experience LEAD in China.4 The overall prevalence of LEAD was 10.0% in the old population.5,6 The number of patients with LEAD continues to increase with age.7 It is estimated that the lifetime risk of LEAD is 19.0%–30.0%.8 LEAD has received less attention,9 with only 21.0–25.0% of people knowing it.10,11 The LEAD manifestation of impaired walking ability is often regarded as a sign of frailty, especially in older patients, leading to a low diagnosis rate and inadequate treatment. When patients seek treatment, their condition has often progressed to a severely ischemic stage that usually requires surgical intervention. Endovascular revascularization (EVR) is a pillar of therapeutic management in patients with LEAD.12 Patients who accepted the EVR was as high as 70.0% to 90.0%.13 However, the high restenosis rate after EVR is problematic for patients and vascular surgeons.14 Restenosis after EVR may lead to symptom recurrence, unhealed ulcers, risk of amputation, and repeated revascularization,15 which places a heavy burden on patients, families, and health care systems.16,17 Comprehensive risk factor control, optimal medical therapy, and appropriate exercise are required in patients with LEAD who undergo EVR to prevent restenosis and other adverse outcomes.
In the past several decades, the vascular community at large has begun to acknowledge the crucial role of self-management in the treatment and management of chronic diseases, to improve patients’ quality of life.18–20 However, only a few studies have reported on the self-management of patients with LEAD or those with LEAD who underwent EVR.
To date, few measures have focused on self-management.21,22 However, the measures concentrate on limited aspects or the traditional domains of self-management, which cannot effectively evaluate the specific self-management of patients with LEAD in other domains (eg, exercise management, pain management, and foot care). Furthermore, no specific self-management questionnaire is available for patients with LEAD who underwent EVR. This study aimed to develop and psychometrically test a self-management questionnaire for patients with LEAD who underwent EVR (LESQ). Healthcare providers can use the LESQ to assess and identify strategies for improving self-management abilities of these patients.
Methods
Sample and Procedures
DeVellis’ guidelines for instrument development incorporating qualitative and quantitative procedures, were used.23 There were three main stages of questionnaire development: (i) Construction of the item pool, (ii) Delphi expert consultation, and (iii) psychometric evaluation. A flow chart of this study is shown in Figure 1.
 |
Figure 1 A flow chart of this study. |
Phase 1: Construction of the Item Pool
Conceptual framework: The self-management conceptual framework of Lorig 24 guided the development of the item pool. Self-management of LEAD in patients who underwent EVR was defined as the ability of patients with LEAD who underwent EVR, with the help of healthcare, to implement medical management, role management and emotional management.
Qualitative semi-structured interviews: Eleven patients with LEAD who underwent EVR, 10 vascular surgeons, and 11 vascular nurses were interviewed between July and November 2020. The purpose of the interviews was to describe qualitatively how self-management was understood. The questions were as follows: “What do you understand about self-management in patients with LEAD who underwent EVR?” and “What aspects of self-management exist?” Before beginning the interview, the purpose of the interview was explained to the participants and the interview was conducted in a quiet, uninterrupted room. Each participant completed an informed consent form and a demographic survey. The interviews were digitally recorded and transcribed verbatim in 24 h. The transcript also included the participants’ expressions, body language, and other information. The transcript was imported into Nvivo software (version 12.0) and analyzed. Qualitative descriptions and content analyses were used to identify the important themes and potential items.25–27 Through semi-structured interviews, four themes and 18 sub-themes of self-management were extracted. Theme one: Protection motivation is the driving force behind self-management. Theme two: Multiple tasks from the core of self-management. Theme three: Healthcare provider-patient cooperation is the cornerstone of self-management. Theme four: Improvement of the quality of life is the goal of self-management. The process and results of the qualitative semi-interview are presented in Supplementary Tables 1–3.
Based on the definition, tasks, and theory of self-management, related self-management scales or questionnaires were searched and screened to select items. LESQ items from the recommended behaviors in the LEAD guidelines were generated. Using these methods, we obtained 43 items.
Phase 2: Delphi Expert Consultation
In this phase, a panel of 29 experts from 19 different institutions in China was recruited to evaluate the question format and each item. Inclusion standards: (i) Be familiar with the content consulted; (ii) be an expert with a professional title of assistant professor or professor; (iii) work experience ≥10 years; and (iv) experts give informed consent and actively participate in the consultation. All the experts had more than 10 years of experience in the field of vascular diseases or self-management. The mean age of the experts was 44.7±5.7 years, and 58.6% were females. The consultation questionnaire containing the item pool was sent to the experts via e-mail. The experts were required to evaluate and rate the items on their importance to the self-management of patients with LEAD who underwent EVR on a 4-point Likert scale (1= not relevant, 2= somewhat relevant, 3= quite relevant, and 4= highly relevant). The experts also provided written comments on each item. The research team met and evaluated each of these responses and arrived at a consensus on which items to include in the psychometric evaluation of the LESQ. In the two rounds of Delphi consultation, the positive coefficients for experts were 90.6% and 100.0%, respectively. The expert authority coefficient was 0.948 in the first round and 0.946 in the second. We discarded 17 items, reducing the questionnaire from 43 to 26 through a Delphi expert consultation. The results of the Delphi expert consultation are shown in Supplementary Tables 4–7. We submitted a 26-item, unidirectional, 5-point Likert questionnaire for psychometric evaluation.
Phase 3: Psychometric Evaluation of the Items
Participants
Using convenience sampling, participants were recruited from the vascular surgery departments of six hospitals in China. Inclusion criteria: (1) Those who meet the diagnosis criteria of “the diagnosis and treatment guideline of LEAD”28: i) Age> 40 years; ii) clinical manifestations of LEAD; iii) impairment or disappearance of the pulse of the distal arteries of ischemic limbs; iv) ankle brachial index (ABI)≤ 0.9; and v) imaging examination showing the corresponding arterial stenosis or obstruction. (2) Patients who met the indications for endovascular treatment and successfully underwent EVR in the hospital. EVR includes percutaneous balloon angioplasty, drug-coated balloon, cutting balloon, frozen balloon, bare metal stent, drug-eluting stent plaque rotation excision, catheter-directed mechanical thrombectomy, and drug thrombolysis. (3) No psychiatric diseases or cognitive impairment. (4) The patients who understood the content of the questionnaires and answered them independently. Exclusion criteria were as follows: (1) Patients who could not provide written informed consent and (2) who did not complete or refused to complete the questionnaire after explanation.
Sample Size
According to the principles of questionnaire design and measurement, the sample size should be at least 10–20 times the number of items and 5% of invalid questionnaires should be considered.29 Therefore, the smallest sample size of each survey was equal to the number of items x10x (1+0.05).
Pretest
The initial draft of the LESQ was pretested in 30 patients who met the eligibility criteria to check whether the semantics of the items were accurate. In the pretest, five items of the initial draft of the LESQ were semantically adjusted to form the LESQ-I with 26 items.
First-Round Cross-Sectional Survey
In the first-round cross-sectional survey, 271 participants were tested using the 26-item LESQ-I, in which items were selected using the following statistical methods. (i) Correlation coefficient analysis: Any item with a Pearson correlation coefficient < 0.30 with the total score was eliminated, (ii) Dispersion degree analysis: Any item with a standard deviation < 0.75 was eliminated, (iii) Cronbach’s α coefficient method: If the Cronbach’s α coefficient increased substantially after any item deletion, indicating this item should be eliminated, (iv) Critical ratio method: Participants were ranked by the score on the questionnaire to derive high- and low-score groups, comprising 27% of those with the highest and lowest scores, respectively. The score of each item was then compared using the Student’s t-test. Items with no significant difference (P > 0.05) between the groups were eliminated, (v) Exploratory factor analysis: Any item with a factor loading < 0.40 or the factors in two domains > 0.40 was eliminated. After item selection and combination with the expert’s suggestions, four items were discarded (the item selection process is shown in Supplementary Tables 8–11, the results of item selection are seen in Supplementary Table 12). A 22-item LESQ-II was developed for reliability and validity test.
Second-Round Cross-Sectional Survey
In the second-round cross-sectional survey, we used the 22-item LESQ-II to investigate 269 patients. Reliability tests included internal consistency reliability (Cronbach’s α coefficient) and test-retest reliability (Pearson’s correlation coefficient and intraclass correlation coefficient [ICC]). The internal consistencies of the instrument and its domains were calculated using Cronbach’s α. Cronbach’s α coefficient was considered appropriate if it was higher than 0.70. To assess test-retest reliability, 30 participants returned four weeks later to complete the same questionnaire. Pearson’s correlation coefficient for test-retest > 0.70 was acceptable. An ICC > 0.50 was deemed appropriate.
The validity of the LESQ-II was tested as follows.(i) Content validity was evaluated using the standard proposed by Polit and Back for the content validity index.30 We used the results of the Delphi expert consultation to calculate the content validity index (CVI). We calculated item-level content validity index (I-CVI) by the percentage of experts who rate the item as “quite relevant” or “highly relevant” in the total number of experts. We considered that an I-CVI ≥ 0.78 was appropriate.29 The average of all the I-CVIs on the scale (S-CVI/Ave) was the average of all the I-CVIs, representing the content validity of the questionnaire. S-CVI/Ave ≥ 0.90 indicates a good content validity.29 (ii) Criterion validity: In this study, we chose the partners in health scale (PIH) as the criterion scale.22,31 The correlation between LESQ-II and PIH was calculated, and Pearson’s correlation coefficient ≥ 0.70 indicated a good criterion validity.29 (iii) Construct validity was tested using principal component analysis, and the Kaiser-Meyer-Olkin (KMO) and Bartlett’s sphere tests were used to determine whether the final items were suitable for principal components analysis. When the KMO value was not less than 0.60, Bartlett’s sphere test with P< 0.01 indicated that it was appropriate for principal components analysis. The common factor is extracted by principal component analysis and maximum variance rotation:29 i) to extract common factors whose eigenvalues are ≥ 129 and ii) to use the parallel analysis method to extract common factors.
Third-Round Cross-Sectional Survey
In the third-round cross-sectional survey, the 22-item LESQ-II was used to assess 639 patients. AMOS 24.0 was used to construct the model to confirm the structure of the LESQ-II by confirmatory factor analysis. Multilevel structural equation modeling (SEM) was employed to examine the factor loadings. The fitness of the model was acceptable as follows. Chi-square value/degree of freedom (χ2/df) < 3 indicates good, and < 5 indicates acceptable. Root-mean-square error of approximation (RMSEA) ≤ 0.50 indicates good, and ≤ 0.8 indicates acceptable. The goodness of fit index (GFI), adjusted goodness of fit index (AGFI), comparative fit index (CFI), normed fit index (NFI), incremental fit index (IFI), and Tucker-Lewis index (TLI) > 0.90 indicate good and > 0.80 indicate acceptable.29 Convergent and discriminant validities were calculated based on a confirmatory factor analysis. The composite reliability (C.R). value of domains > 0.70 and the average variance extracted (AVE) of domains > 0.50 indicated good convergent validity.29 The AVE square root of the domain greater than the correlation coefficient of the domain and other domains showed good discriminant validity.
We also used Vascular Quality of Life Questionnaire-6 (VQ6) to test the quality of life of patients. Then The VQ6 is a disease-specific instrument for peripheral arterial disease.32 Additionally, we calculated the correlation between the LESQ-II and VQ6 to explore the relationship between patients’ self-management abilities and their quality of life.
The potential profile analysis method was used to calculate the robust maximum likelihood value, and a series of classification models were compared to determine the best-fitting model using the Mplus software. The fitting indicators included the Akaike information criterion (AIC), Bayesian information criterion (BIC), adjusted Bayesian information criterion (aBIC), bootstrap likelihood ratio test (BLRT), Lo-Mendell-Rubin test (LMRT), and entropy. The smaller the AIC, BIC, and aBIC, the better the model. The closer the entropy value is to 1, the better the model.33 The BLRT and LMRT indicate whether the current model is statistically significant compared with the reduced classification model, P < 0.05 for significance. The optimal cut-off point was determined according to the posterior classification probability.
Data Collection
The study was conducted between February 2021 and March 2022. We collected data using the LESQ, PIH scale, VQ6 and sociodemographic and medical characteristic questionnaires. The LESQ was used to evaluate the self-management ability applicable of patients with LEAD who underwent EVR. It’s a self-evaluation questionnaire. The recall period shall be “within the past one month”. Using the Likert score of 5, “Cannot do it at all”, “Rarely do it”, “Can do it sometimes”, “Can do it most of the time”, and “Can do it completely” represents 1, 2, 3, 4, and 5 points, respectively. The final version of the LESQ (LESQ-II) consisted of 22 items. The total scores ranged from 22 to 110. The PIH scale was used as a criterion. PIH is a 12-item scale with four domains of disease knowledge, coping style, symptom recognition, and treatment adherence, on a 9-point Likert scale (0–8).22,31 A score of 0 indicated poor self-management, and 8 indicated good self-management. The total scores ranged from 0 to 96. The higher the score, the better was the patients’ self-management ability. The total Cronbach’s α coefficient of the PIH was 0.820. The VQ6 includes six items concern limitation in activities (activity), tiredness in the legs (symptom), walking ability (activity), concerns about poor circulation in the legs (emotional aspects), ability to take part in social activities (social aspects) and discomforts from pain in the leg (pain).32 Each question has a four-point response scale (1 most problems to 4 no problems). Lower scores indicate poorer quality of life. The total Cronbach’s α coefficient of the VQ6 was 0.860. The sociodemographic and medical characteristic questionnaire by self-design consisted of information to be obtained directly from patients or clinical records: age, sex, ethnicity, marital status, family residence, educational level, financial burden, Rutherford category, duration of LEAD (months), postoperative time (months), and comorbidities. Participants were recruited from the vascular surgery departments of six hospitals in China.
Ethical Approval
Our study complies with the Declaration of Helsinki. Ethical approval for this study was obtained from the Institutional Review Board of the West China School of Medicine, Sichuan University (approval number 2021–108). Eleven patients with LEAD who underwent EVR, 10 vascular surgeons, and 11 vascular nurses who were interviewed in semi-structured interview received oral information on the purpose of the study. They were informed that the interview would be taped. They signed the informed consent form. All experts in Delphi expert consultation consented to participate in the study. We described the goal of our survey and asked if the candidate participants who met the eligible criterion would be interested in participating in pretest or in the three-round cross-sectional survey. All participants gave their written informed consent and provided their consent for the publication of the manuscript. We also promised to keep the personal information of participants confidential in our study.
Statistical Analysis
IBM SPSS Statistics (version 25.0, IBM Corporation), Amos (version 24.0, IBM Corporation), and Mplus (version 8.0) were used for data analysis. Data screening was the first step in identifying errors and missing data. Continuous data were nonnormally distributed after visual and statistical inspection for normality. Means and standard deviations used to describe normally distributed continuous data. Medians and interquartile ranges were used to describe continuous data were not normally distributed. Frequencies and percentages were calculated for categorical variables. Statistical significance was set at P < 0.05.
Results
Response and Patient Characteristics
The effective completion rates were 93.1% (271/291), 89.1% (269/302), and 90.9% (623/685) in the three rounds of cross-sectional surveys. Three rounds of cross-sectional surveys were conducted to assess the self-management ability of 1163 patients with LEAD who underwent EVR. The average age, duration of LEAD, and postoperative time were 74.8±9.1 years, 20.1±17.1 months, and 18.2±16.8 months, respectively. The sample comprised 67.2% males. Illiteracy and primary school education accounted for 26.7% and 35.3% of the sample, respectively. A total of 47.5% of patients were in the Rutherford 5–6 category; 72.5%, 48.2%, 26.7%, and 22.3% had hypertension, diabetes, coronary heart disease, and cerebrovascular disease, respectively. Detailed characteristics of the participants of the three cross-sectional surveys are shown in Table 1.
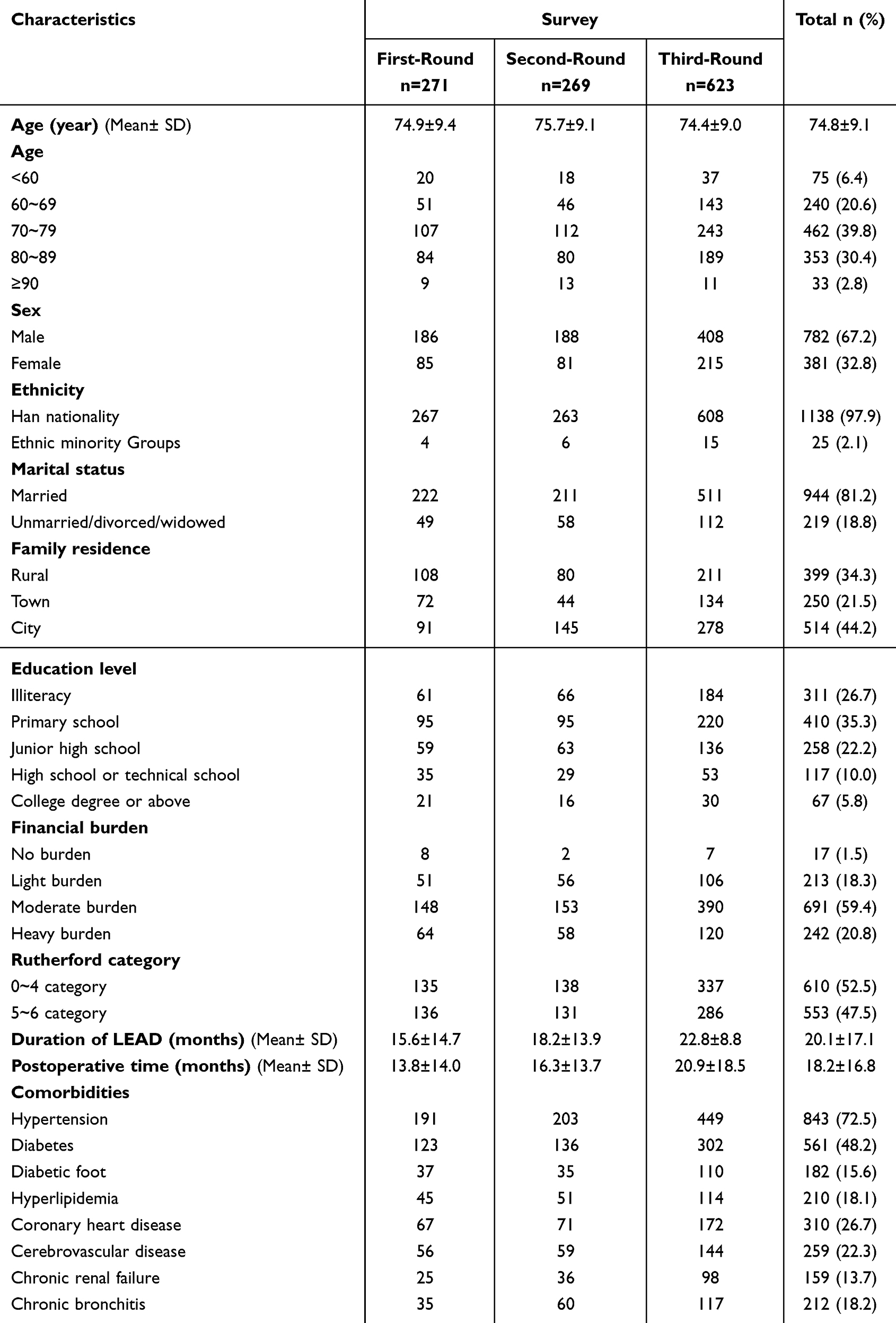 |
Table 1 Participants’ Sociodemographic and Medical Characteristics |
Reliability of the Questionnaire
The LESQ had good internal consistency reliability, with Cronbach’s α coefficients for the total questionnaire, medical management, rehabilitation exercise management, and daily life management were 0.953, 0.940, 0.938 and 0.953, respectively. The Split-half coefficients 0.899. The results showed good retest reliability, with Pearson’s coefficient and intraclass correlation coefficients of 0.917 and 0.911, respectively. The reliability of the questionnaire was good.
Content Validity of the Questionnaire
The content validity of the questionnaire was evaluated based on the results of the second round of expert consultations, and the importance of the 22 items was evaluated. The I-CVI scores of items were between 0.828 and 1.000, and all met the requirements of I-CVI ≥ 0.780. The S-CVI/Ave, which is an indication of the content validity of the LESQ, was 0.939. The value was higher than 0.900, indicating satisfactory content validity of the questionnaire (Supplementary Table 13).
Criterion Validity of the Questionnaire
The Pearson correlation coefficient of the LESQ and PIH was 0.854 (P < 0.001), indicating that the LESQ had good criterion-related validity.
Construct Validity of the Questionnaire
An exploratory factor analysis was conducted based on the second round of the survey. Prior to the exploratory factor analysis, the KMO value was 0.934 and Bartlett’s sphere was P < 0.001. Three common factors with eigenvalues ≥1 were extracted by principal component analysis, and the cumulative contribution rate of variance of the three common factors was 80.092%. The factor loadings of the items on their domains range from 0.65 to 0.88, with none of the items exhibiting multiple loadings. The questionnaire was divided into three domains according to three factors: medical management (6 items), rehabilitation exercise management (4 items), and daily life management (12 items) (Table 2).
 |
Table 2 Three Domains and the Factor Loading of Each Item |
Construct validity was further tested by confirmatory factor analysis based on the third round of the survey using the IBM SPSS Amos (version 24.0). The model fitted well with χ2/df=4.498, RMSEA = 0.075, GFI = 0.906, AGFI = 0.847, NFI = 0.969, IFI = 0.976, CFI = 0.976, and TLI = 0.964 (Figure 2).
 |
Figure 2 Structure diagram of confirmatory factor analysis model. The Structure diagram of confirmatory factor analysis model indicates that item 1 to 6 correspond to medical management, item 7 to 10 correspond to rehabilitation exercise management, and the item 11 to 22 correspond to daily life management. |
Convergent and Discriminant Validities
The convergent validity test showed that all C.R. values > 0.70 and all AVE values > 0.50 for all three domains, indicating good convergent validity of the questionnaire (see Supplementary Table 14). The result of the discriminant validity test showed that all three domains of the questionnaire had acceptable discriminant validity (Supplementary Table 15).
The Pearson correlation coefficient of the LESQ and Vascular Quality of Life Questionnaire-6 was 0.285 (P < 0.001), which shows weak correlation with self-management ability and quality of life. This suggests that the LESQ primarily assesses self-management abilities rather than the content of quality of life.
Optimal Cut-off Point for the Questionnaire
The optimal cut-off point for the questionnaire was determined based on the results of the third survey round. The potential profile analysis compared the results of one to four classifications (Table 3). The results of AIC, BIC and aBIC of the three classifications were better than those of the two classifications. The LMRT and BLRT for the three classifications showed P < 0.05. Considering these proportions, the three classifications are relatively balanced. Based on the above, the results of this study were divided into three categories (Figure 3). Through a posterior classification query, the optimal cut-off points were determined to be 52 and 70. Scores ≥ 70, 52–69, and ≤ 51 indicated high (18.2%), moderate (38.0%), and low (43.8%) self-management abilities.
 |
Table 3 The Classifications by Potential Profile Analysis (n=623) |
 |
Figure 3 Three categories outcome of latent profile analysis diagram. The Diagram illustrates the three categories of self-management. The green line represents the high self-management ability group, the blue represents the moderate self-management ability group, the red line represents the low self-management ability group. |
The total LESQ score of the patients with LEAD who underwent EVR was 56 (41, 69), which was moderate. Rehabilitation exercise management had the lowest score among the three self-management domains, with a score of 8 (6, 12). The LESQ scores were 39 (34, 45), 62 (58, 66), and 76 (72, 81.5) in the low, moderate, and high self-management groups, respectively (Table 4).
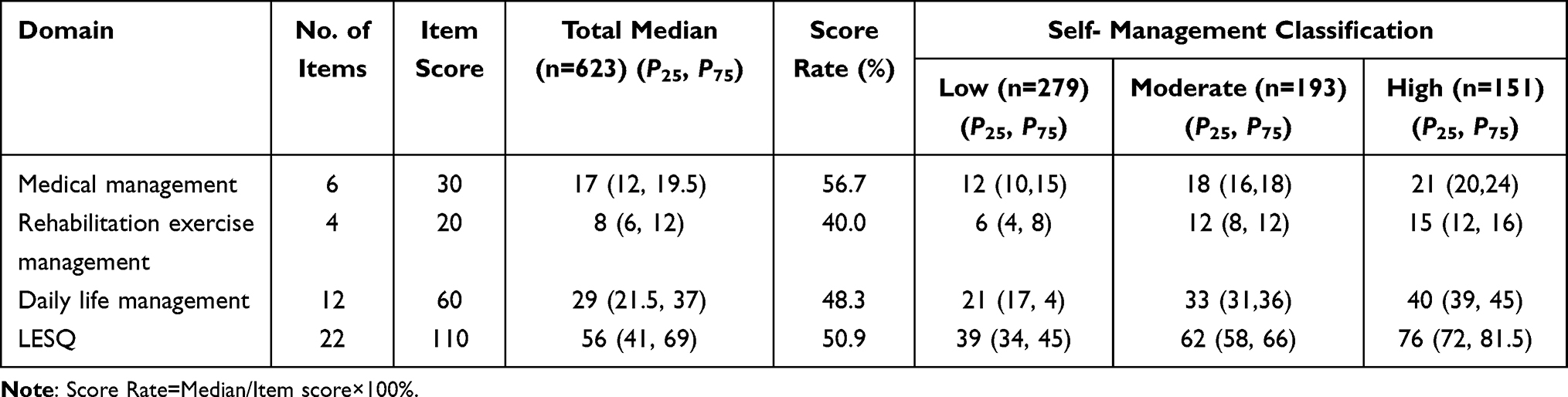 |
Table 4 The Domain’s Score of the LESQ |
Discussion
Characteristics of the LESQ
This study described the development and validation of a self-management questionnaire for patients with LEAD who underwent EVR. The final version of the LESQ was the LESQ- II, with 22 items. The total scores ranged from 22 to 110. The higher the score, the better was the patient’s self-management ability. The Cronbach’s α coefficient and test-retest reliability of the LESQ were good (0.953 and 0.917, respectively). The content validities of the LESQ was 0.939. The following three domains were determined using exploratory factor analysis: medical management (6 items), rehabilitation exercise management (4 items), and daily life management (12 items). A confirmatory factor analysis confirmed that the three domains constructed with the SEM were acceptable. The three LESQ domains also showed good convergent and discriminant validities. The LESQ is a specific questionnaire for patients with LEAD who undergo EVR and differ from other self-management instruments. Medical management included setting management goals (items 1–3) and medical management (items 4–6). Rehabilitation exercise management included item 7–10. Daily life management included lifestyle management (items 11–13), foot care (items 14-18), pain management (item 19), emotional management (items 20–21), and gaining support (item 22). The results showed that the LESQ developed in this study had good reliability and validity throughout the test.
Criterion Validity of LESQ
We use the partners in health scale (PIH) as the criterion scale. The PIH is a general-purpose self-assessment questionnaire for chronic disease self-management. It was first developed by scholars Battersby et al in 31 It has been translated into multiple languages and is widely used across various countries for assessing the self-management of patients with chronic diseases.34 The correlation coefficient between LESQ and PIH was 0.854 shows the LESQ is a self-management tool with good criterion validity. We also calculated the correlation coefficient between LESQ and Vascular Quality of Life Questionnaire-6 (VQ6), which yielded a result of 0.285, indicating a weak correlation between self-management ability and quality of life. This reflects that the LESQ focuses more on self-management abilities rather than the content of quality of life. The results indicate that better self-management ability is associated with a higher quality of life. Previous study has suggested that effective chronic disease self-management can yield significant benefits for patients, including improvements in quality of life.35 Consequently, it is imperative for healthcare providers to promote self-management among patients, as it serves as an indirect strategy to enhance their quality of life.
Classification of Patients with LEAD Who Underwent EVR
Based on the latent profile analysis, the optimal cut-off point for LESQ was determined. Latent profile analysis is a model-based approach for determining the optimal cut-off point of a scale or questionnaire for the classification of continuous variables that identify unobserved heterogeneity in a population based on their response to continuous scoring variables, and classifies individuals with similar response patterns.33 The patients were classified into three groups using the latent profile analysis as follows: patients with scores ≥ 70, 52–69, ≤ 51 were in the high, moderate, and low self-management groups. The health care providers can implement self-management improvement strategies by assessing the patients’ self-management abilities. In our study, 43.8% patients had low self-management. Previous studies have also shown the self-management deficit of patients with LEAD.36,37 This could be related to the age and level of education. In the three rounds cross-sectional survey of 1163 patients, the mean age of the participants was 74.8±9.1 years, 26.7% of them were illiterate, and 35.3% were primary school educated. This could lead to a lack of awareness of the risk factors for disease,38 lower ability to access information and learn, fewer resources, and, therefore, low self-management ability. The lowest score in the rehabilitation exercise management domain was 40.0%, followed by daily life management (48.3%) and medical management (56.7%). These results indicated that rehabilitation exercise management and daily life management should be improved.
Limitation
This study had some limitation. This cross-sectional study was conducted at six hospitals in Sichuan Province, China. Therefore, further nationwide surveys should be conducted. Due to resource limitation, convenience sampling was used instead of random sampling. These results may have been affected by a selection bias. Despite these limitations, to the best of our knowledge, this is the first study to develop and test a self-management questionnaire for patients with LEAD who underwent EVR.
Conclusion
The LESQ is a promising evaluation tool for self-management with good reliability and validity for patients with LEAD who undergo EVR. To the best of our knowledge, this is the first self-management questionnaire for patients with PAD who undergo EVR. Healthcare providers can use this instrument to evaluate the patients with LEAD who undergo EVR and identify strategies for improving self-management abilities and health-related outcomes.
Research Highlight
This cross-sectional descriptive study developed the Self-management Questionnaire for Patients with Lower Extremity Arterial Disease Who Underwent Endovascular Revascularization (LESQ). This is a new self-management questionnaire specifically designed to assess the self-management ability of patients with lower extremity arterial disease (LEAD) who undergo endovascular revascularization (EVR).
The final version of the LESQ with 22 items, was divided into three domains: medical management (6 items), rehabilitation exercise management (4 items), and daily life management (12 items). The results of the psychometric validation showed good internal consistency and retest reliabilities, and content, criterion-related, and construct validities.
The optimal cut-off point was determined using the potential profile analysis. There were 18.2%, 38.0%, and 43.8% of patients with high (≥70), moderate (52–69), and low (≤51) self-management abilities.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the project of Southwest Medical University (Grant No. 2021ZKMS003), Foundation of Nursing Key Laboratory of Sichuan Province (Grant No. HLKF2023(Y)-3), Luzhou Science and Technology Program (Grant No. 2023RQN182), the Education and Teaching Reform Project of Southwest Medical University (08/02323012), and Sichuan Science and Technology Program (Grant No. 2024NSFSC1605).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roijers JP, Rakke YS, Hopmans CJ, et al. A mortality prediction model for elderly patients with critical limb ischemia. J Vasc Surg. 2020;71:2065–2072. doi:10.1016/j.jvs.2019.08.245
2. Mueller L, Engelbertz C, Reinecke H, et al. Secondary prevention in lower extremity artery disease patients: lipid-lowering therapy and long-term guideline adherence. J Clin Med. 2022;11:1–14. doi:10.3390/jcm11226838
3. Spannbauer A, Chwała M, Ridan T, et al. Intermittent claudication in physiotherapists’ practice. Biomed Res Int. 2019;2019:2470801. doi:10.1155/2019/2470801
4. Song P, Rudan D, Zhu Y, et al. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: an updated systematic review and analysis. Lancet Glob Health. 2019;7:e1020–e1030. doi:10.1016/S2214-109X(19)30255-4
5. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33:S5–S75. doi:10.1016/j.ejvs.2006.09.024
6. Urbano L, Portilla E, Munoz W, Hofman A, Sierra-Torres CH. Prevalence and risk factors associated with peripheral arterial disease in an adult population from Colombia. Arch Cardiol Mex. 2018;88:107–115. doi:10.1016/j.acmx.2017.02.002
7. Kieback AG, Gähwiler R, Thalhammer C. PAD screening: why? whom? when? how? - A systematic review. VASA Z Gefasskrankheiten. 2021;50:85–91. doi:10.1024/0301-1526/a000897
8. Matsushita K, Sang Y, Ning H, et al. Lifetime risk of lower-extremity peripheral artery disease defined by ankle-brachial index in the United States. J Am Heart Assoc. 2019;8:e012177. doi:10.1161/JAHA.119.012177
9. Hardman RL, Jazaeri O, Yi J, Smith M, Gupta R. Overview of classification systems in peripheral artery disease. Seminars Interventional Radiology. 2014;31:378–388.
10. Criqui MH, Matsushita K, Aboyans V, et al. Lower extremity peripheral artery disease: contemporary epidemiology, management gaps, and future directions: a scientific statement from the American Heart Association. Circulation. 2021 144:E171–E191.
11. Hirsch AT, Murphy TP, Lovell MB, et al. Gaps in public knowledge of peripheral arterial disease - the first national PAD public awareness survey. Circulation. 2007;116:2086–2094. doi:10.1161/CIRCULATIONAHA.107.725101
12. Stella J, Stausberg J, Lichtenberg M, Hoffmann U, Malyar NM. Clinical characteristics and current practice of endovascular revascularization in aorto-iliac, femoropopliteal and infra-popliteal lower extremity artery disease-insights from the RECCORD registry. J Clin Med. 2022;11:1–12. doi:10.3390/jcm11206074
13. Frank U, Nikol S, Belch J, et al. ESVM guideline on peripheral arterial disease. Vasa. 2019;48:7–79. doi:10.1024/0301-1526/a000834
14. Nowakowski T, Malinowski KP, Nizankowski R, Iwaniec T, Undas A. Restenosis is associated with prothrombotic plasma fibrin clot characteristics in endovascularly treated patients with critical limb ischemia. J Thromb Thrombolysis. 2019;47:540–549. doi:10.1007/s11239-019-01826-9
15. Mahoney EM, Wang K, Keo HH, et al. Vascular hospitalization rates and costs in patients with peripheral artery disease in the United States. Circ Cardiovasc Qual Outcomes. 2010;3:642–651. doi:10.1161/CIRCOUTCOMES.109.930735
16. Sharma A. Current review with evolving management strategies in critical limb ischemia. Indian J Radiol Imaging. 2019;29:258–263. doi:10.4103/ijri.IJRI_208_19
17. Berger A, Zhao Q, Murphy B, Leeper NJ, Ting W, Berger JS. Patterns of utilization and cost of health care among patients with chronic coronary artery disease and/or peripheral arterial disease in clinical practice: analyses of a large us integrated claims-emr database. Circulation. 2018;138. 138.
18. Groessl EJ, Sklar M, Laurent DD, Lorig K, Ganiats TG, Ho SB. Cost-effectiveness of the hepatitis C self-management program. Health Educ Behav. 2017;44:113–122. doi:10.1177/1090198116639239
19. Basu R, Ory MG, Towne SD Jr, Smith ML, Hochhalter AK, Ahn S. Cost-effectiveness of the chronic disease self-management program: implications for community-based organizations. Front Public Health. 2015;3:1–8. doi:10.3389/fpubh.2015.00027
20. Kaambwa B, Bryan S, Jowett S, et al. Telemonitoring and self-management in the control of hypertension (TASMINH2): a cost-effectiveness analysis. Eur J Prev Cardiol. 2014;21:1517–1530. doi:10.1177/2047487313501886
21. Golledge J, Drovandi A, Rowbotham S, Velu R, Quigley F, Jenkins J. Control of modifiable risk factors and major adverse cardiovascular events in people with peripheral artery disease and diabetes. World J Diabetes. 2021;12;883.
22. Petkov J, Harvey P, Battersby M. The internal consistency and construct validity of the partners in health scale: validation of a patient rated chronic condition self-management measure. Qual Life Res. 2010;19:1079–1085. doi:10.1007/s11136-010-9661-1
23. D RF. Scale Development: Theory and Application.
24. Lorig KR, Holman HR. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26:1–7. doi:10.1207/S15324796ABM2601_01
25. Sullivan-Bolyai S, Bova C, Harper D. Developing and refining interventions persons with health disparities: the use of qualitative description. Nurs Outlook. 2005;53:127–133. doi:10.1016/j.outlook.2005.03.005
26. Neergaard MA, Olesen F, Andersen RS, Sondergaard J. Qualitative description - The poor cousin of health research? BMC Med Res Methodol. 2009;9. doi:10.1186/1471-2288-9-52
27. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23:334–340. doi:10.1002/1098-240X(200008)23:4<334::AID-NUR9>3.0.CO;2-G
28. Aboyans V, Ricco J-B, Bartelink ML, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39:301–302.
29. Wm R. Questionnaire Statistical Analysis Practice – SPSS Operation and Application. Chongqing: Chongqing Publishing House; 2010.
30. Polit DF. Nursing Research: Generating and Assessing Evidence for Nursing Practice.
31. W Battersby M, Ask A, M Reece M, J Markwick M, P Collins J. The partners in health scale: the development and psychometric properties of a generic assessment scale for chronic condition self-management. Aust J Prim Health. 2003;9:41–52. doi:10.1071/PY03022
32. Kumlien C, Nordanstig J, Lundstrom M, Pettersson M, Kasprowicz M, Hermanowski T. Validity and test retest reliability of the vascular quality of life questionnaire-6: a short form of a disease-specific health-related quality of life instrument for patients with peripheral arterial disease. Health Qual Life Outcomes. 2017;15:15. doi:10.1186/s12955-017-0587-y
33. Fu H, Si L, Guo R. What is the optimal cut-off point of the 10-item center for epidemiologic studies depression scale for screening depression among Chinese individuals aged 45 and over? An exploration using latent profile analysis. Front Psychiatry. 2022;13:820777. doi:10.3389/fpsyt.2022.820777
34. Smith D, Harvey P, Lawn S, Harris M, Battersby M. Measuring chronic condition self-management in an Australian community: factor structure of the revised Partners in health (PIH) scale. Qual Life Res. 2017;26:149–159. doi:10.1007/s11136-016-1368-5
35. Cao X, Feng M, Ge R, Wen Y, Yang J, Li X. Relationship between self-management of patients with anxiety disorders and their anxiety level and quality of life: a cross-sectional study. PLoS One. 2023;18;e0284121.
36. Cao X, Feng M, Ge R, Wen Y, Yang J, Li X, Application of continuous nursing in interventional treatment of lower limb arteriosclerosis obliterans. Chin Med Pharm. 2017;7:82–85.
37. Ran Y W H Influence evaluation of motor function and prognosis after continuous nursing in interventional treatment of lower limb arteriosclerosis obliterans. Electronic J Practical Clin Nurs Sci. 2019;4:143–144.
38. Builyte IU, Baltrunas T, Butkute E, et al. Peripheral artery disease patients are poorly aware of their disease. Scand Cardiovasc J. 2019;53:373–378. doi:10.1080/14017431.2019.1645350
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.