")
Back to Journals » Infection and Drug Resistance » Volume 18
Diagnosis of Mycoplasma Hominis Peritonitis in a CAPD Patient with Metagenomic Next-Generation Sequencing: A Case Report
Authors Deng C, Hong L, Sun D, Miao H, Tang F, Li Z, Liu X
Received 12 January 2025
Accepted for publication 6 May 2025
Published 12 May 2025 Volume 2025:18 Pages 2469—2473
DOI https://doi.org/10.2147/IDR.S510660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Chunfeng Deng, Lei Hong, Dongni Sun, Hui Miao, Fei Tang, Zhaohui Li, Xi Liu
Department of Nephrology, Longgang Central Hospital of Shenzhen, Shenzhen, 518116, People’s Republic of China
Correspondence: Xi Liu, Email [email protected]
Background: Mycoplasma hominis (Mh) is a conditional pathogenic microorganism in humans, typically colonizing the genitourinary tract of adults and causing infections in this system. However, Mh is rarely reported as a causative agent of peritoneal dialysis (PD)-associated peritonitis.
Case Presentation: A 46-year-old woman undergoing maintenance PD presented with abdominal pain and cloudy PD effluent. Her PD modality is continuous ambulatory peritoneal dialysis (CAPD). Cultures of the PD effluent and blood were negative, and empirical antibiotic therapy was ineffective, leading to a diagnosis of refractory peritonitis. Metagenomic next-generation sequencing (mNGS) detected Mh in the PD effluent. Treatment was adjusted to intraperitoneal (IP) clindamycin combined with intravenous drip(ivdrip) moxifloxacin, resulting in complete recovery.
Conclusion: Patients with culture-negative PD-associated peritonitis or refractory peritonitis should be evaluated for potential Mh infection. mNGS enables rapid detection of pathogens that traditional methods may fail to identify. A combination of moxifloxacin and clindamycin is effective for treating PD-associated peritonitis caused by Mh.
Keywords: mycoplasma hominis, peritoneal dialysis-associated peritonitis, metagenomic next-generation sequencing
Introduction
PD is a primary treatment method for patients with end-stage renal disease (ESRD). PD-associated peritonitis is a frequent and severe complication in these patients, contributing to significant morbidity and mortality.1 The incidence of PD-associated peritonitis ranges from 0.26 to 0.40 episodes per person-year.2 Although dialysis effluent culture is the primary diagnostic method, it is limited by a substantial rate of culture-negative results, which account for 13.4% to 40% of all peritonitis cases.1 To date, PD-associated peritonitis caused by Mycoplasma hominis (Mh) has been rarely reported. Infections caused by mycoplasma lack distinctive clinical features, often leading to misdiagnosis. Due to its slow growth rate, the requirement for specialized culture media, and lack of a cell wall, Mh is difficult to identify using traditional culture methods. mNGS is a highly sensitive and specific technique for identifying infectious pathogens.3 We report a case of refractory PD-associated peritonitis caused by Mh, diagnosed using mNGS, with successful resolution following targeted antibiotic therapy.
Case Presentation
A 46-year-old woman with ESRD of unknown etiology was admitted on October 31, 2023, with complaints of abdominal discomfort and cloudy PD effluent for one day. She had been on CAPD for five years, with a regimen of four 2000-mL dialysate exchanges daily.
On admission, her vital signs were as follows: blood pressure 116/81 mmHg, heart rate 98 bpm, respiratory rate 20 cycles/min, and temperature 36.8°C. Cardiopulmonary examination was unremarkable. Abdominal examination revealed diffuse tenderness with a soft abdomen. No erythema or purulent discharge was observed at the PD catheter site, but the PD effluent was cloudy. Symmetrical edema was noted in her lower extremities. Laboratory tests revealed peripheral white blood cell (WBC) count of 10.13 × 10⁹/L, platelet count of 255 × 10⁹/L, hemoglobin of 84 g/L, C-reactive protein (CRP) of 85.13 mg/L, creatinine of 878.7 μmol/L, and urea nitrogen of 20.09 mmol/L. Analysis of the PD effluent showed a WBC count of 3386 × 10⁶/L, with 90% polymorphonuclear leukocytes. Based on these findings, the patient was diagnosed with PD-associated peritonitis.
Empirical antibiotic therapy with IP cefazolin and ceftazidime was initiated after collecting a PD effluent sample for culture. On the fourth day, due to a lack of clinical improvement, the antibiotics were upgraded to IP vancomycin. On the fifth day, laboratory tests showed a peripheral WBC count of 14.08 × 10⁹/L and CRP of 139 mg/L. The treatment was adjusted to IP imipenem combined with ivdrip piperacillin-tazobactam, and fluconazole was added to prevent fungal infections. Despite these changes, the patient’s condition continued to deteriorate, with persistent abdominal pain, cloudy PD effluent, and worsening inflammatory markers. On the seventh day the WBC count in the PD effluent was 3415 × 10⁶/L, higher than on admission (Table 1). Based on these findings, the patient was diagnosed with refractory peritonitis.
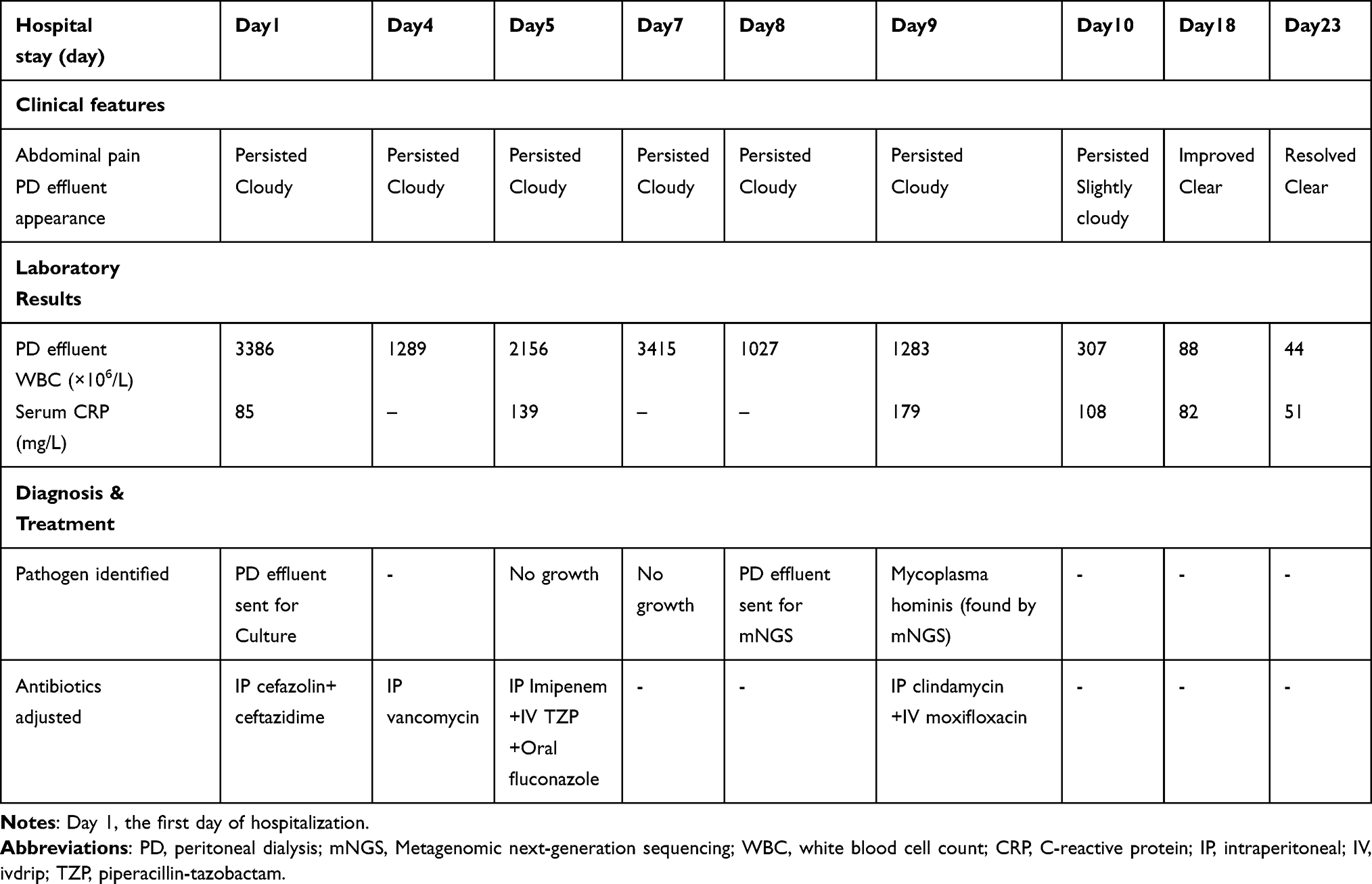 |
Table 1 Summary of Clinical Features, Laboratory Results, and Antibiotic Treatment |
Removal of the PD catheter was recommended, but the patient refused and requested to retain it. The pathogen remained undetermined as PD effluent cultures, blood cultures, fungal D-glucan testing, and a tuberculosis interferon-γ release test were all negative. Subsequently, mNGS of the PD effluent was performed, which identified Mh. The final diagnosis was Mh peritonitis.Based on the mNGS results, the treatment was changed on November 8 to ivdrip moxifloxacin (0.4 g once daily) and IP clindamycin (600 mg QID). A rapid decrease in the WBC count of the PD effluent was observed the following day. On the tenth day after the patient started the new treatment regimen, the effluent WBC count had dropped below 100 × 10⁶/L, and the patient’s abdominal pain had significantly improved. After 14 days of treatment, the PD effluent became clear, and the patient was discharged. Post-discharge, the patient continued oral moxifloxacin for one week. During a three-month follow-up, the patient remained stable, and no recurrence was noted.
mNGS Analysis
The PD effluent sample was sent to Dinfectome Inc. (Nanjing, China) for unbiased pathogen detection. DNA was extracted using the TIANamp Magnetic DNA Kit (Tiangen), and a metagenomic library was prepared with the Hieff NGS C130P2 OnePot II DNA Library Prep Kit for MGI (Yeasen Biotechnology). Sequencing was conducted on the BGI MGISEQ-200 platform. Human host sequences were removed, and unmapped reads were analyzed against a microbial genome database. The analysis specifically identified Mh, with 605 specific reads detected. The relative abundance of Mh was 29.98%, and the genome coverage rate was 4.48% (Figure 1).
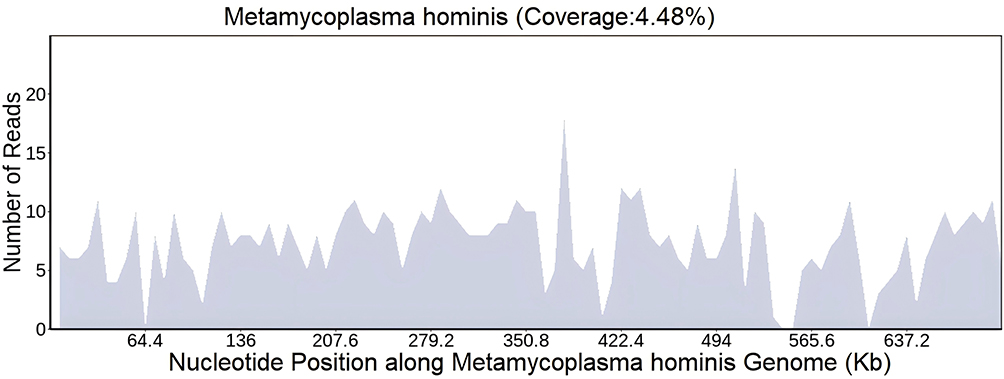 |
Figure 1 mNGS result. |
Discussion
Peritonitis is a common complication in PD patients and a leading cause of PD failure. Refractory peritonitis is defined as a condition in which, after five days of appropriate antibiotic treatment, the PD effluent remains cloudy.1 Common pathogens in PD-associated peritonitis include coagulase-negative Staphylococcus, Enterobacteriaceae, non-fermenting Gram-negative bacilli, and Staphylococcus aureus,4 while Mh is rare. Peritoneal dialysate culture is a key method for identifying pathogens, but detecting mycoplasma is challenging because it grows slowly in vitro and often requires specialized culture media. Studies have shown that Mh can take over a week to form identifiable colonies, which may evade detection by systems like the Bact/ALERT 3D fully automated bacterial/mycobacterial culture monitoring system.5 Additionally, due to its lack of a cell wall, Mh cannot be identified through standard staining methods.6 These limitations make conventional cultivation methods unreliable for detecting Mh in PD effluent.
In addition to conventional culture methods, alternative diagnostic approaches, such as polymerase chain reaction (PCR) and mNGS, are available. PCR is characterized by high sensitivity and specificity. It can yield results within hours and is cost-effective. Nevertheless, PCR is a targeted detection method, which restricts its application in detecting unknown pathogens. PCR assays necessitate the design of specific primers or probes for microbial pathogens, thereby limiting its pathogen-detection ability. The existing literature suggests that PCR is not suitable for the rapid identification of bacteria in PD effluent.7 In contrast, mNGS excels in detecting uncommon, novel, and coinfecting pathogens without the need for prior knowledge.8 mNGS is an advanced nucleic acid-based technology that extracts all microbial DNA or RNA directly from clinical samples without requiring culture. It uses genomic research strategies to analyze the genetic composition and function of microbial communities. This high-throughput sequencing method can comprehensively analyze the microbiome in clinical samples, including bacteria, fungi, viruses, parasites, mycoplasma, and chlamydia. In this case, the patient was diagnosed with refractory peritonitis. Repeated PD effluent cultures yielded negative results, and multiple adjustments to empirical antibiotic regimens proved ineffective. Considering the unpredictable nature of the causative pathogen, we employed mNGS, which ultimately identified Mh as the infectious agent. Similarly, there was a report that mNGS detected Mh, Ureaplasma parvum, and Ureaplasma urealyticum in the PD effluent of patients with recurrent “culture-negative” PD-associated peritonitis.9 mNGS is especially useful for PD-associated peritonitis undiagnosed by conventional methods and offers a fast and reliable approach for detecting Mh, although it is expensive.
The main types of mycoplasma that infect humans are Mh, Ureaplasma urealyticum, and Mycoplasma pneumoniae. Mh commonly colonizes the urogenital tract and can cause infections such as urinary tract infections and bacterial vaginosis.10 It is also associated with extragenital infections, including meningitis,11 arthritis,12 and endocarditis.13 However, reports of Mh causing PD-associated peritonitis are rare. Previous studies have found Mh in both PD fluid and urine or cervical smears,14,15 suggesting that it may spread from the urogenital tract to the abdominal cavity. In this case, the patient was unmarried, had no sexual history, and was anuric, so urine and cervical secretions were not collected for testing. Notably, the patient fell ill during the peak season of Mycoplasma pneumoniae pneumonia in China, but whether there is a correlation between the two remains unclear. Studies, however, have suggested a potential seasonal association with peritonitis.16
Due to the lack of a cell wall in Mh, most antibiotics are ineffective, which likely contributed to the failure of initial empiric treatments. According to the 2022 Recommendations of the International Society for PD (ISPD), this patient met the criteria for refractory peritonitis, and removal of the PD catheter was recommended.1 Fortunately, Mh was identified using mNGS. Following the ISPD 2022 guidelines for the prevention and treatment of PD-associated peritonitis, IP clindamycin combined with ivdrip moxifloxacin was administered, resulting in rapid clinical improvement.
Conclusion
The clinical symptoms of PD-associated peritonitis caused by Mh appear nonspecific, presenting as abdominal pain, abdominal tenderness, cloudy PD effluent, and increased WBC count in the effluent. These symptoms are similar to those caused by common pathogens.
In summary, Mh is proven difficult to detect via conventional PD effluent culture. Regarding patients presenting with culture-negative PD-associated peritonitis and demonstrating poor response to empirical antibiotic therapy, Mh infection should be included in the clinical suspicion. It is recommended to apply mNGS in such a patient group to achieve more accurate pathogen identification. This not only enables more targeted antimicrobial therapy but also helps prevent avoidable catheter-related interventions.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Longgang Central Hospital of Shenzhen (2025ECPJO41), and the patient consented for publication of her clinical data.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Acknowledgments
We sincerely express our gratitude to the patient for her kind approval of this paper. Her cooperation has been of great significance to the completion of this research.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Li PK, Chow KM, Cho Y, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Perit Dial Int. 2022;42(2):110–153. doi:10.1177/08968608221080586
2. Perl J, Fuller DS, Bieber BA, et al. Peritoneal dialysis-related infection rates and outcomes: results from the peritoneal dialysis outcomes and practice patterns study (PDOPPS). Am J Kidney Dis. 2020;76(1):42–53. doi:10.1053/j.ajkd.2019.09.016
3. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788.doi. doi:10.1093/cid/cix881
4. Gupta S, Muralidharan S, Gokulnath, et al. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in southern India using an automated blood culture system to culture peritoneal dialysate. Nephrology. 2011;16(1):63–67. doi:10.1111/j.1440-1797.2010.01355.x
5. Waites KB, Canupp KC. Evaluation of BacT/ALERT system for detection of Mycoplasma hominis in simulated blood cultures. J Clin Microbiol. 2001;39(12):4328–4331. doi:10.1128/JCM.39.12.4328-4331.2001
6. Xiao N, Gai W, Hu WG, et al. Next-generation-sequencing technology used for the detection of Mycoplasma hominis in renal cyst fluid: a case report. Infect Drug Resist. 2019;23(12):1073–1079. doi:10.2147/IDR.S198678
7. Szeto CC, Ng JK, Fung WW, et al. Polymerase chain reaction/ electrospray ionization-mass spectrometry (PCR/ESI-MS) is not suitable for rapid bacterial identification in peritoneal dialysis effluent. Perit Dial Int. 2021;41(1):96–100. doi:10.1177/0896860820917845
8. Han D, Li Z, Li R, et al. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol. 2019;45(5–6):668–685. doi:10.1080/1040841X.2019.1681933
9. Wang C, Wang J, Yan J, et al. Mycoplasma hominis, Ureaplasma parvum, and Ureaplasma urealyticum: hidden pathogens in peritoneal dialysis-associated peritonitis. Int J Infect Dis. 2023;131:13–15. doi:10.1016/j.ijid.2023.03.032
10. Margarita V, Fiori PL, Rappelli P. Impact of symbiosis between Trichomonas vaginalis and Mycoplasma hominis on vaginal dysbiosis: a mini review. Front Cell Infect Microbiol. 2020;10:179. doi:10.3389/fcimb.2020.00179
11. Zhou ML, Wang P, Chen S, et al. Meningitis in a Chinese adult patient caused by Mycoplasma hominis: a rare infection and literature review. BMC Infect Dis. 2016;16(1):557. doi:10.1186/s12879-016-1885-4
12. Smith BJ, Crowe A, Comahig J, et al. A 27-year-old woman with an unusual cause of periprosthetic joint infection. Clin Infect Dis. 2016;62(11):
13. Cohen JI, Sloss LJ, Kundsin R, et al. Prosthetic valve endocarditis caused by Mycoplasma hominis. Am J Med. 1989;86(6Pt2):819–821. doi:10.1016/0002-9343(89)90479-8
14. Diekman MJM, Kuipjer EJ, Boeschoten EW. Isolation of Mycoplasma hominis from peritoneal effluent of a CAPD patient. Perit Dial Int. 1991;11:84–85. doi:10.1177/089686089101100118
15. van der Bijl AE, Kamper AM, de Fijter JW, et al. Mycoplasma hominis peritonitis after renal transplantation. Nephron. 2000;86(4):541–542. doi:10.1159/000045862
16. Zeng Y, Jiang X, Feng S, et al. The influence of seasonal factors on the incidence of peritoneal dialysis-associated peritonitis. Ren Fail. 2020;42(1):807–817. doi:10.1080/0886022X.2020.1804401
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnosis of Mycoplasma hominis Meningitis with Metagenomic Next-Generation Sequencing: A Case Report
Dong Y, He Y, Zhou X, Lv X, Huang J, Li Y, Qian X, Hu F, Zhu J
Infection and Drug Resistance 2022, 15:4479-4486
Published Date: 12 August 2022