")
Back to Journals » Journal of Pain Research » Volume 18
Diagnostic Performance of Infrared Thermography, Quantitative Sudomotor Axonal Reflex Testing, and 3-Phase Bone Scintigraphy for Complex Regional Pain Syndrome Diagnosis: A Retrospective Observational Study
Authors Noh C, Lee J , Choi HY, Park E, Shin YS , Hong B , Ko Y, Oh C, Lee SY
Received 23 April 2024
Accepted for publication 8 October 2024
Published 14 March 2025 Volume 2025:18 Pages 1305—1312
DOI https://doi.org/10.2147/JPR.S474451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael A Ueberall
Chan Noh,1,2,* Jiyong Lee,1,2,* Hye Young Choi,1 Eunhye Park,1 Yong Sup Shin,1,2 Boohwi Hong,1,2 Youngkwon Ko,1,2 Chahyun Oh,1,2 Sun Yeul Lee1,2
1Department of Anesthesiology and Pain Medicine, Chungnam National University Hospital, Daejeon, Korea; 2Department of Anesthesiology and Pain Medicine, College of Medicine, Chungnam National University, Daejeon, Korea
*These authors contributed equally to this work
Correspondence: Sun Yeul Lee; Chahyun Oh, Email [email protected]; [email protected]
Purpose: Complex regional pain syndrome (CRPS) diagnosis poses challenges due to the absence of an objective and definitive test. Although laboratory tests such as infrared thermography, quantitative sudomotor axonal reflex testing (QSART), and 3-phase bone scintigraphy have been considered diagnostic aids, their use remains controversial. This retrospective study aimed to elucidate the diagnostic validity and potential value of these modalities for the diagnosis of CRPS.
Patients and Methods: The Budapest criteria were used to diagnose CRPS, and infrared thermography, QSART, and 3-phase bone scintigraphy were performed as ancillary tests. Diagnostic performance was evaluated using receiver operating characteristic (ROC) curve analysis and measurement of sensitivity, specificity, and positive and negative likelihood ratios.
Results: Of the 41 patients assessed, 26 (63.4%) were diagnosed with CRPS based on these criteria. Among the three tests, only infrared thermography demonstrated significant diagnostic performance (area under the ROC curve, 0.718; 95% confidence interval, 0.569– 0.866; p = 0.003). Infrared thermography revealed a positive and negative likelihood ratio of 2.308 and 0.346, respectively, indicating clinically informative results. The three positive results exhibited the highest specificity (0.933) and positive predictive value (0.917).
Conclusion: Among the three laboratory tests for CRPS, infrared thermography was the most useful. QSART and 3-phase bone scintigraphy did not show a significant diagnostic performance; however, combining the results of all three tests may provide additional diagnostic confidence in certain cases.
Keywords: complex regional pain syndrome, infrared thermography, quantitative sudomotor axonal reflex testing, 3-phase bone scintigraphy
Introduction
Complex regional pain syndrome (CRPS) is characterized by persistent and severe pain, typically triggered by musculoskeletal trauma or surgery. CRPS is characterized by four cardinal signs and symptoms, and is diagnosed based on these clinical manifestations. The diagnostic criteria for CRPS, established by the International Association for the Study of Pain in 1994, have been revised multiple times, and the diagnosis is currently based on the 2007 Budapest criteria.
As the name implies, the condition presents distinctive manifestations, including sensory changes such as allodynia or hyperalgesia, autonomic signs, and trophic changes.1,2 Despite its significant impact on patients’ quality of life due to intense pain and diverse manifestations, the exact pathophysiology and prevention of CRPS remain elusive.3,4 Moreover, beyond the current limited understanding, diagnosis of CRPS is substantially challenging owing to the lack of a validated screening tool or definitive confirmatory test.2,5 Consequently, the standard diagnostic approach relies on clinical evaluation. This creates a dilemma because clinical diagnosis inherently depends on the physicians’ subjective judgements and expertise. Complicating matters include the frequent entanglement of this condition with various legal issues, including compensation claims, following an inciting event.6,7
Currently, laboratory tests that are implemented to assist in the diagnosis of CRPS include, but are not limited to, infrared thermography, plain radiography, 3-phase bone scintigraphy, quantitative sudomotor axonal reflex testing (QSART), and electromyography.
Infrared thermography is performed to objectively verify the difference in body temperature between the affected and unaffected body parts, which is one of the diagnostic criteria for CRPS.8,9 Individuals with CRPS typically experience an initial rise in temperature in the affected extremities, followed by cold and clammy extremities in the later stages.10 Infrared thermography has been widely used in the diagnosis of CRPS because of its easy availability and objective validation of the patient’s subjective symptoms.
QSART evaluate the cholinergic sudomotor function of the sympathetic system,11 which can be useful to evaluate autonomic nervous system disorders and neuropathic pain. The test is performed by stimulating sweat glands with weak electrical stimuli and measuring the quantity of sweat generated by these stimuli.12
Three-phase bone scintigraphy, a diagnostic tool developed in 1988 by Yang et al13 evaluate bone abnormalities by assessing the blood flow and tissue perfusion. The test generates images in three distinct phases: (1) the flow phase, captured immediately after the injection of a radioactive substance, which reflects the blood flow to the area of interest; (2) the pool phase, taken approximately 5 min post-injection, showing the amount of activity that has leaked into the surrounding tissues; and (3) the delayed phase, captured 2–4 h after the injection, which indicates the rate of bone turnover.14 An increased uptake in all three phases is typically observed in CRPS, although variations in patterns may occur.14,15
Unfortunately, studies on the diagnostic value of these laboratory tests have reported inconsistent and/or unsatisfactory results; therefore, the diagnostic utility of these tests is still not definitively established.2,15–17 This study retrospectively evaluated the diagnostic performance of three laboratory tests for CRPS: infrared thermography, QSART, and 3-phase bone scintigraphy. We hypothesized that one modality or a combination of these modalities would demonstrate diagnostic utility. Notably, studies that simultaneously compare all three tests are scarce, highlighting the importance of our investigation.
Materials and Methods
This retrospective observational study was approved by the Institutional Review Board of Chungnam National University Hospital (CNUH 2024-01-078) on March 13, 2024. The requirement for informed consent was waived owing to the retrospective design of the study.
Electronic medical records of all patients who underwent CRPS workups at an outpatient pain clinic in a tertiary hospital (Chungnam National University Hospital) between January 2019 and December 2023 were retrospectively reviewed. During this period, our departmental CRPS workup involved a comprehensive clinical examination using the Budapest criteria (Box 1)18 and three ancillary laboratory tests: infrared thermography, QSART, and 3-phase bone scintigraphy. Patients without test results or definitive diagnoses were excluded. The extracted clinical information included demographic characteristics (age, sex, weight, and height), disease characteristics (symptom onset, affected extremities, and type), and test results.
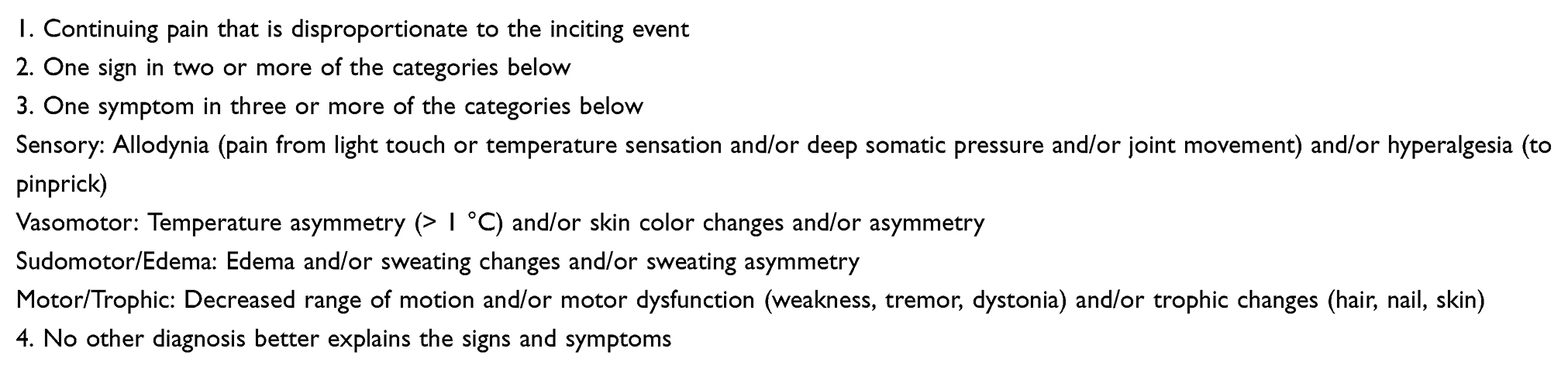 |
Box 1 The Budapest Criteria for Complex Regional Pain Syndrome (CRPS) |
Laboratory Tests
Infrared thermography was conducted by trained physicians.19 To mitigate potential influences on the results, before undergoing infrared thermography, participants were allowed 15 min to adapt to the test room after removing clothes covering the body parts to be imaged. Depending on the area to be examined, images were taken with the patient either standing or sitting. Views were captured from the front, both sides, and back, and the painful region were compared with the opposite limb. The specific shape, size, and location of each region of interest (ROI) were determined at the examiner’s discretion based on the patient’s medical history and the location of pain. A temperature difference between the ROIs of the painful area and the opposite limb was calculated, and a difference > 1.0 °C was considered positive.18
Three-phase bone scintigraphy involved the flow, blood pool, and delayed phases after the systemic administration of technetium-99m methylene diphosphonate. Since no firmly established criteria are available for diagnosing CRPS using 3-phase bone scintigraphy, the following criteria based on previous studies were applied: 1) concordant findings in both the flow and blood pool phases (decreased, increased, or symmetrical), as well as increased uptake in the delayed phase; 2) decreased uptake in all three phases, indicative of the chronic stage; and 3) decreased uptake in both the flow and blood pool phases, with symmetrical uptake in the delayed phase. A result was considered positive if any of these three criteria were met.15,20,21
QSART evaluates postganglionic sympathetic function following a cholinergic challenge. Changes in humidity at the monitoring site were plotted, and the area under the curve was quantified.22 Neurologists interpreted the results and assessed the presence of sudomotor dysfunction.
Outcome Measures
The overall diagnostic performance of each laboratory test was evaluated using the area under the receiver operating characteristic curve (AUROC). Secondary measures included the sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), positive predictive value, and negative predictive value for each test. Among these secondary measures, a PLR > 2.0 and a NLR < 0.5 were considered clinically informative.23
Exploratory Analysis
The diagnostic value of all three modalities (ie, three positive results) combined was evaluated to explore the potential additional benefits of enhancing the diagnostic performance.
Statistical Analyses
The sample size was based on the data available at the time of the study. All statistical analyses were conducted using the R software (version 4.2.2; R Project for Statistical Computing, Vienna, Austria). Continuous variables were analyzed using Student’s t-test or Mann–Whitney U-test depending on data distribution. The data are presented as mean ± standard deviation or median (interquartile range), as appropriate. The diagnostic performance of each laboratory tool was evaluated using the receiver operating characteristic (ROC) curve analysis. The DeLong’s test was used to compare the models. Statistical significance was set at a two-tailed p-value < 0.05, which was deemed statistically significant for all computations.
Results
Forty-one patients were examined, of whom 26 (63.4%) were diagnosed with CRPS. Patients without test results or diagnosis of CRPS (positive or negative) were excluded, and all other patients were included in the final analysis (Figure 1). The clinical characteristics of the patients are summarized in Table 1. Among the patients with CRPS, 17 (65.4%) were diagnosed with CRPS type 1.
 |
Table 1 Clinical Characteristics Stratified by Complex Regional Pain Syndrome (CRPS) Diagnosis |
 |
Figure 1 Flow diagram of patient selection process of this study. Notes: IRT, infrared thermography; QSART, quantitative sudomotor axonal reflex testing; TPBS, 3-phase bone scintigraphy; CRPS, complex regional pain syndrome. |
The laboratory test results are presented in Table 2 and Figure 2. An increasing rate of CRPS diagnosis was observed with more positive laboratory test results; specifically, 91.7% (11/12) of the patients with three positive results were diagnosed with CRPS. The overall performance of the tests is presented in Table 3. Among the three tests, only infrared thermography demonstrated significant diagnostic performance, with an AUROC of 0.718 (95% confidence interval [CI], 0.569–0.866; p = 0.003), whereas QSART and 3-phase bone scintigraphy exhibited AUROC of 0.571 (95% CI, 0.425–0.716; p = 0.846) and 0.560 (95% CI, 0.400–0.721; p = 0.779), respectively. Additionally, infrared thermography revealed a PLR of 2.308 (95% CI, 1.094–4.866) and an NLR of 0.346 (95% CI, 0.157–0.761), indicating clinically informative results.
 |
Table 2 Laboratory Test Results Stratified by the Diagnosis of Complex Regional Pain Syndrome (CRPS) |
 |
Table 3 Diagnostic Performances of Laboratory Tests and Their Combined Result (Three Positives, +++) |
 |
Figure 2 Diagnosis of complex regional pain syndrome (CRPS) stratified by counts of positive results from laboratory tests. |
Table 3 presents the results of exploratory analyses. The overall diagnostic performance of the three positive results did not show a significant improvement in diagnostic performance compared with that of infrared thermography alone (p = 0.681). However, it exhibited the highest specificity of 0.933 (95% CI, 0.807–1.000), positive predictive value of 0.917 (95% CI, 0.760–1.000), and PLR of 6.346 (95% CI, 0.906–44.428).
Discussion
In this study, the diagnostic performances of three laboratory tests (infrared thermography, QSART, and 3-phase bone scintigraphy) were retrospectively evaluated in patients with suspected CRPS. Among these, only infrared thermography exhibited significant diagnostic performance, with an AUROC of 0.718, which was further supported by a PLR and NLR of 2.308 and 0.346, respectively, indicating its clinical utility. In contrast, QSART and 3-phase bone scintigraphy did not show significant independent diagnostic performances, as reflected by their insignificant AUROC values. Although combining the results of all three tests did not significantly enhance the overall diagnostic performance compared with infrared thermography alone, it did improve the specificity and positive predictive value, suggesting that a multimodal approach may provide additional diagnostic confidence in certain cases.
One of the key challenges in the diagnosis of CRPS is the subjective nature of the symptoms and difficulty in standardizing clinical assessments. Physicians often rely on patient descriptions of their pain and associated symptoms, which are inherently difficult to objectively evaluate. This creates variability in diagnosis, with inter-rater agreement (kappa) between 0.43 and 0.78 as reported in previous studies.24 Pursuing various diagnostic aids, as demonstrated in the current study, are essential for a more comprehensive understanding and accurate diagnosis of CRPS.
Among these tests, infrared thermography is a particularly useful and commonly employed diagnostic tool owing to its ability to objectively confirm temperature differences between the affected and unaffected body parts, which is one of the hallmark signs of CRPS.2,18 Our findings reinforce the diagnostic utility of infrared thermography, as it was the only test in our study to demonstrate significant diagnostic performance. Although previous studies have suggested that factors such as the duration of the condition and the setting of ROIs may affect the results, this remains a highly useful non-invasive diagnostic method.2,19
Despite being a component of the criteria for the clinical diagnosis of CRPS, the diagnostic validity and accuracy of QSART remain controversial. A recent retrospective study with a similar setting demonstrated a limited diagnostic utility of QSART, and the results of the present study aligns with these findings.17 Previous studies on 3-phase bone scintigraphy for CRPS diagnosis have reported varied performance, and its utility remains controversial.14,25 A retrospective study evaluating the diagnostic performance of 3-phase bone scintigraphy in a similar setting concluded that a positive 3-phase bone scintigraphy result has a low diagnostic value.15 A meta-analysis, using the Budapest criteria as reference, demonstrated a sensitivity of 0.551 and specificity of 0.935.26 Despite some potential prognostic value of 3-phase bone scintigraphy when considering treatment options,2 the findings of our study support the reported low diagnostic value of 3-phase bone scintigraphy.
In this study, the clinical utility of combining the results of the three laboratory tests to diagnose CRPS was investigated. As illustrated in Figure 2, a noticeable increasing trend was observed in the probability of a CRPS diagnosis as the number of positive findings in the tests increased. This trend is plausible, given that CRPS is not characterized by a single symptom or sign; it presents as a constellation of various manifestations. Consequently, individuals with multiple positive findings were more likely to be diagnosed with CRPS. Conversely, < 50% of cases with only one or no positive results were diagnosed with CRPS. Moreover, there is the potential to explore alternative methods to combine these results. This may involve differential weighting of the results or generation of a numeric index using logistic models. However, these approaches require extensive datasets and rigorous validation to ensure their effectiveness and reliability.
This study has some limitations. First, the sample size was not predetermined through power calculations for ROC analysis; instead, all available data were utilized owing to the infrequency of CRPS. Second, the cases included primarily represented patients who were referred to a tertiary hospital for the evaluation of unspecified chronic pain or a CRPS diagnosis. Although this reflects a common clinical scenario in tertiary care centers in Korea, its generalizability to other clinical settings may be limited.
Conclusion
The findings suggest that among the three laboratory tests for CRPS, infrared thermography is the most useful diagnostic aid. It demonstrated a significant diagnostic performance, with the highest PLR and the lowest NLR in the diagnosis of CRPS. QSART and 3-phase bone scintigraphy did not show a significant diagnostic performance; however, combining the results of all three tests may provide additional diagnostic confidence in certain cases.
Data Sharing Statement
Raw data supporting the conclusions of this study will be made available by the corresponding author upon reasonable request.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Chungnam National University Hospital (CNUH 2024-01-078) on March 13, 2024.
Informed Consent Statement
Patient consent was waived owing to the retrospective design of the study. To ensure confidentiality, the patients’ medical records (registration numbers) and pathology numbers were stored in a separate file under the corresponding author’s supervision. Identifiers were coded or anonymized to prevent subject identification. All study-related documents were encrypted and saved as password-protected files that were accessible only to the researchers. These files were securely stored in the corresponding author’s personal laboratory, equipped with a lock.
Acknowledgments
The authors thank In-Sun Kwon, Ph.D. (Chungnam National University Hospital).
Author Contributions
All authors made a significant contribution to the reported work, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval for the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was funded by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science, ICT, and Future Planning (NRF-2020R1C1C1005423). The funders had no role in the design of the study; collection, analyses, or interpretation of data; writing of the manuscript; or decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bruehl S. Complex regional pain syndrome. BMJ. 2015;351:h2730. doi:10.1136/bmj.h2730
2. Shim H, Rose J, Halle S, Shekane P. Complex regional pain syndrome: a narrative review for the practising clinician. Br J Anaesth. 2019;123(2):e424–e433. doi:10.1016/j.bja.2019.03.030
3. Schasfoort FC, Bussmann JB, Zandbergen AM, Stam HJ. Impact of upper limb complex regional pain syndrome type 1 on everyday life measured with a novel upper limb-activity monitor. Pain. 2003;101(1–2):79–88. doi:10.1016/s0304-3959(02)00298-1
4. van Velzen GAJ, Perez R, van Gestel MA, et al. Health-related quality of life in 975 patients with complex regional pain syndrome type 1. Pain. 2014;155(3):629–634. doi:10.1016/j.pain.2013.12.017
5. Mesaroli G, Hundert A, Birnie KA, Campbell F, Stinson J. Screening and diagnostic tools for complex regional pain syndrome: a systematic review. Pain. 2021;162(5):1295–1304. doi:10.1097/j.pain.0000000000002146
6. Shin S, Jang SG, Min K, Lee W, Kim SY. The Legal Doctrine on the Liability of Physicians in Medical Malpractice Lawsuits Involving Complex Regional Pain Syndrome. J Korean Med Sci. 2018;33(9):e46. doi:10.3346/jkms.2018.33.e46
7. Bae H-M. Study of Legal Issues on Complex Regional Pain Syndrome (CRPS)-Focusing on issues in damage compensation lawsuit; 2010. Available from: https://koreascience.kr/article/JAKO201026359283952.page.
8. Bruehl S, Lubenow TR, Nath H, Ivankovich O. Validation of thermography in the diagnosis of reflex sympathetic dystrophy. Clin J Pain. 1996;12(4):316–325. doi:10.1097/00002508-199612000-00011
9. Wasner G, Schattschneider J, Baron R. Skin temperature side differences--A diagnostic tool for CRPS? Pain. 2002;98(1–2):19–26. doi:10.1016/s0304-3959(01)00470-5
10. Birklein F, Riedl B, Claus D, Neundorfer B. Pattern of autonomic dysfunction in time course of complex regional pain syndrome. Clin Auton Res. 1998;8(2):79–85. doi:10.1007/BF02267817
11. Hooshang H, Masood H. Complex regional pain syndrome. Reflex sympathetic dystrophy syndrome. Diagnosis and therapy-A review of 824 patients Abstract and summary; 1999. Available from: https://www.rsdrx.com/RSD-Articles/Opiates_and_CRPS.pdf.
12. Novak P. Quantitative autonomic testing. J Vis Exp. 2011;53:e502.
13. Yang DC, Gould L, Yee WK, Patel D, Maghazeh P, Giovanniello J. Intravenous radionuclide total body arteriography: a new technique. Clin Nucl Med. 1988;13(10):696–700. doi:10.1097/00003072-198810000-00003
14. Shin SH, Kim SJ. Bone scintigraphy in patients with pain. Korean J Pain. 2017;30(3):165–175. doi:10.3344/kjp.2017.30.3.165
15. Moon JY, Park SY, Kim YC, et al. Analysis of patterns of three-phase bone scintigraphy for patients with complex regional pain syndrome diagnosed using the proposed research criteria (the ‘Budapest Criteria’). Br J Anaesth. 2012;108(4):655–661. doi:10.1093/bja/aer500
16. Jeon SG, Choi EJ, Lee PB, et al. Do severity score and skin temperature asymmetry correlate with the subjective pain score in the patients with complex regional pain syndrome? Korean J Pain. 2014;27(4):339–344. doi:10.3344/kjp.2014.27.4.339
17. Lee HJ, Kim SE, Moon JY, Shin JY, Kim YC. Analysis of quantitative sudomotor axon reflex test patterns in patients with complex regional pain syndrome diagnosed using the Budapest criteria. Reg Anesth Pain Med. 2019;44(11):1026–1032. doi:10.1136/rapm-2019-100415
18. Harden RN, Bruehl S, Stanton-Hicks M, Wilson PR. Proposed new diagnostic criteria for complex regional pain syndrome. Pain Med. 2007;8(4):326–331. doi:10.1111/j.1526-4637.2006.00169.x
19. Choi E, Lee PB, Nahm FS. Interexaminer reliability of infrared thermography for the diagnosis of complex regional pain syndrome. Skin Res Technol. 2013;19(2):189–193. doi:10.1111/srt.12032
20. Kwon HW, Paeng JC, Nahm FS, et al. Diagnostic performance of three-phase bone scan for complex regional pain syndrome type 1 with optimally modified image criteria. Nucl Med Mol Imag. 2011;45(4):261–267. doi:10.1007/s13139-011-0104-x
21. Cheon M, Kang HJ, Do KH, Yang HS, Han EJ, Yoo J. Diagnostic Performance of Three-Phase Bone Scintigraphy and Digital Infrared Thermography Imaging for Chronic Post-Traumatic Complex Regional Pain Syndrome. Diagnostics. 2021;11(8):1459. doi:10.3390/diagnostics11081459
22. Suh BC. Quantitative sudomotor axon reflex test (QSART) as a diagnostic tool of small fiber neuropathy. Ann Clin Neurophysiol. 2022;24(1):1–6. doi:10.14253/acn.2022.24.1.1
23. Jaeschke R, Guyatt GH, Sackett DL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA. 1994;271(9):703–707. doi:10.1001/jama.271.9.703
24. de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129(1–2):12–20. doi:10.1016/j.pain.2006.09.008
25. Fournier RS, Holder LE. Reflex sympathetic dystrophy: diagnostic controversies. Semin Nucl Med. 1998;28(1):116–123. doi:10.1016/s0001-2998(98)80022-6
26. Wertli MM, Brunner F, Steurer J, Held U. Usefulness of bone scintigraphy for the diagnosis of Complex Regional Pain Syndrome 1: a systematic review and Bayesian meta-analysis. PLoS One. 2017;12(3):e0173688. doi:10.1371/journal.pone.0173688
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.