")
Back to Journals » Journal of Pain Research » Volume 18
Disease Burden of Neck Pain in China from 1990 to 2021 and Its Prediction for 2042: The Global Burden of Disease Study 2021
Authors Wei J, Yang K, Xue J, Luo M, Peng W, Yin X, Sun W, Gao C, Teng G, Yin H, Feng M, Li L, Sun K, Zhang W
Received 3 February 2025
Accepted for publication 2 April 2025
Published 11 April 2025 Volume 2025:18 Pages 1975—1990
DOI https://doi.org/10.2147/JPR.S516118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Jiaming Wei,* Kexin Yang,* Jiarui Xue, MingYi Luo, Wei Peng, Xunlu Yin, Wu Sun, Chunyu Gao, Guangfei Teng, He Yin, Minshan Feng, Luguang Li, Kai Sun, Wei Zhang
Department of SpineII, Wangjing Hospital of China Academy of Chinese Medical Sciences, Beijing, 100102, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xunlu Yin, Email [email protected] Kexin Yang, Email [email protected]
Purpose: This study, aimed to report the rates and trends of the prevalence, incidence, and years lived with disability caused by neck pain in the general population of China from 1990 to 2021 and forecast the incidence, prevalence, and disability-adjusted life Years (DALYs) from 2022 to 2042.
Methods: We used data from the Global Burden of Diseases Study (GBD) 2021. The annual percentage change (APC) and average APC between 1990 and 2021 were calculated using joinpoint regression analysis. An autoregressive integrated moving average (ARIMA) model was used to forecast the incidence, prevalence, and DALYs rates between 2022 and 2042.
Results: From 1990 to 2021, the disease burden of neck pain in China showed a clear upward trend, with age-standardised incidence rate (ASIR), age-standardised prevalence rate (ASPR), and DALYs rates being significantly higher in females than in males. Especially in terms of DALYs, Aging has had the largest impact, contributing 61.88% of the increase, while population growth has accounted for 32.43%. Joinpoint regression analysis showed that the incidence and prevalence of neck pain in China increased gradually from 2000 to 2021. Data from 2021 showed that individuals aged 45– 59 years are the most affected by neck pain, regardless of sex. The prediction results of the ARIMA model indicate that China’s ASIR and ASPR for neck pain are projected to continue increasing over the next 20 years.
Conclusion: Neck pain is a serious public health problem in the general Chinese population. This may be related to changes in people’s lifestyles and work patterns due to improvements in societal well-being and technology. Raising awareness of the risk factors for neck pain in the general population could help reduce the future burden of neck disorders, and neck pain should be a priority for future research on prevention and therapy.
Keywords: neck pain, joinpoint regression analysis, ARIMA models, Burden of disease, prevalence, incidence, disability-adjusted life years
Introduction
Neck pain (NP) is a significant public health challenge and a major concern in contemporary society.1 It is the foremost cause of disability and poses considerable economic and medical burdens in high-income nations while gaining recognition as a pertinent issue in low- and middle-income countries, particularly among middle-aged and older adults.2,3 The Global Burden of Disease (GBD) Study 2021, and research on the epidemiology of NP identified neck and back pain as the fourth leading cause of disability-adjusted life years (DALYs). Based on the existing literature, a particular study estimated the 1-year incidence of NP to range from 10.4% to 21.3%.3 Given the rapid technological advancements and the ageing population in China, the prevalence and incidence of NP are expected to continue to increase. In specific occupational sectors, annual prevalence rates of 54%-76% have been reported.4,5 A comprehensive understanding of the impact of NP on individuals is essential for developing targeted lifestyle interventions across diverse populations and fostering the implementation of effective national health policies.6
Additionally, NP is categorised as a musculoskeletal condition,7 and substantial evidence indicates a correlation between musculoskeletal conditions and chronic diseases.8 Individuals suffering from musculoskeletal conditions exhibit a 17% increased risk of developing chronic diseases.9 On 11 May 2021, China unveiled the main findings of its seventh national population census, which indicated that the total population of the mainland had reached approximately 1.3 billion in 2020, an increase from 1.33972 billion in 2010.10,11 In pursuit of the ambitious objectives outlined in the Healthy China 2030 blueprint,12 it is imperative to incorporate the most recent data concerning the burden of NP from the GBD 2021 estimates.13 This included an examination of the prevalence, incidence, and years lived with disability (YLDs) attributable to NP, as well as the changes observed from 1990 to 2021.14 A comprehensive analysis of these data could significantly enhance our understanding of the current prevalence and impact of NP across various developmental stages in China, thereby providing a valuable basis for etiological research and evaluation of the healthcare system.
The GBD 2021 offer a standardised methodology for evaluating the burden of NP in China.15 This study aimed: (1) to investigate the incidence, prevalence, and YLDs attributable to NP within the general population of China from 1990 to 2021, with stratification by age and sex; (2) to examine the independent influences of age, period, and cohort on the incidence of NP during the same timeframe, including a sex-based analysis of influences; and (3) to apply the autoregressive integrated moving average (ARIMA) model to forecast the overall incidence, prevalence, and DALYs rates from 2022 to 2042. The results of this study may provide valuable insights for health policymakers in China, enhance their understanding of the burden of NP, and facilitate the formulation of timely and effective preventive measures.
Resources and Methods
Overview
The GBD 2021 study offers an extensive analysis of all-cause and cause-specific mortality, in addition to disabilities linked to significant diseases and injuries. This study incorporates data from 204 countries, from 1990 to 2021, categorised by age, sex, and demographic factors. Our investigation specifically focused on the prevalence, incidence, and YLDs of NP in China.16
Definitions and Data Sources
Case definition for NP (ICD-11 code: ME84.2, ICD-10 code: M54.2) was defined as discomfort or pain localised in the cervical spine region, which may radiate to the arms and persist for a minimum duration of 24.4,17
Information regarding the incidence, prevalence, DALYs, and age-standardised rates (ASRs) was obtained from the GBD 2021 study (https://www.healthdata.org/research-analysis/gbd).
The GBD database is an extensive repository curated by global health research institutions and spearheaded by the Institute for Health Metrics and Evaluation at the University of Washington.18,19 The GBD 2021 initiative systematically quantifies approximately 369 diseases and injuries across 204 countries from 1990 to 2021. The data are categorised by age, sex, year, and geographical location, thereby facilitating comparisons of disease burden across a diverse array of conditions.20 The research team used the DisMod-MR 2.1 Bayesian meta-regression methodology to estimate the prevalence, incidence, and DALYs outcomes across various age and sex demographics in all provinces of China.21 In our analysis, the incidence and population data were categorised into consecutive 5-year intervals from 1990 to 2021. Age groups were defined by successive 5-year increments, ranging from “<5” years to “95+”, resulting in 20 distinct age categories. This methodological framework enabled a thorough examination of the trends and identification of different risk groups. Additionally, According to Article 32, Items 1 and 2 of Chapter III of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, which was issued by the Central People’s Government of the People’s Republic of China on February 18, 2023, the following types of life science and medical research involving human subjects that utilize human information data or biological samples may be exempted from ethical review if they do not cause harm to human bodies, involve sensitive personal information, or involve commercial interests. This exemption aims to reduce unnecessary burdens on researchers and promote the development of life science and medical research involving human subjects.22
(1) Research conducted using legally obtained public data, or data generated through observation without interfering with public behavior. (2) Research conducted using anonymized information data.
This study relied on publicly accessible data, thus ethical approval was not required.
Research Methods
Prevalence and Disease Burden Analysis of NP
Using data from the GBD 2021 database, the prevalence of NP can be determined using publicly accessible metrics, including incidence rates (crude rates), incidence numbers, prevalence rates (crude rates), and prevalence numbers.23 The burden of NP can be assessed using crude DALY rates,24 which quantify the total years of healthy life lost from the onset of the disease until death. This encompasses the years of life lost (YLLs) attributable to premature mortality and YLDs associated with disease-related impairments. In accordance with the current age classifications in the GBD database, the study segmented the population into 20 distinct 5-year age intervals. The specified age groups are as follows: <5, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90–94, and ≥95 years. This systematic framework enabled a comprehensive analysis of the trends and patterns across various life stages. The overall trend in NP development was assessed using the rate of change and estimated annual percentage change (EAPC).25
The EAPC was derived using a linear regression model using ASRs in conjunction with the calendar year. In contrast to the estimates produced by DisMod-MR 2.1, we included a 95% confidence interval (95% CI) for each EAPC. Correlation analysis was performed using the Spearman rank-order correlation method, with statistical significance at P<0.05.26 Comprehensive data analysis and visualisation were performed using the R software (version 4.3.3) and SPSS Statistics (version 29.0).
ARIMA (p, d, q) Model
The ARIMA model serves as a tool for forecasting future values based on the historical values of the variable.27 This model comprises three primary components: Autoregressive (AR), moving average (MA), and integration (I). Its standard notation is ARIMA (p, d, q), where “p” denotes the order of autoregression, “d” signifies the order of differencing, and “q” represents the order of the moving average.28 The AR (p) model is a p-order autoregressive model, whereas the MA (q) model corresponds to a q-order moving-average process.29 The underlying principle of the ARIMA model is to conceptualise the data generated by the target variable over time as a stochastic sequence. This methodology uses a mathematical framework to characterise the inherent autocorrelation in sequences. By capitalising on the relationship between historical and current values within a sequence, the model endeavours to accurately predict future values.30
Detailed Steps for Building the Model
(1) Conduct stationarity tests on time series data. If a series does not satisfy the conditions for stationarity, differencing transformations were applied to convert it into a stationary series.
(2) The parameters were estimated using graphs of the autocorrelation function (ACF) and partial autocorrelation (PACF). By determining the order of differencing, we obtained the parameters p, d, and q.
(3) The fitting effect was observed using visualisation methods, and the significance of the parameters was assessed.
(4) SPSS software was used for modelling, the results of the fitting parameters were compared, and the final model was selected.
(5) A white-noise test is conducted on the residual sequence of the fitted model.
(6) Predicted data.
Statistical Analysis
The R software (version 4.3.3) was used to analyse and organise the data pertaining to the incidence, prevalence, and DALYs associated with NP, to elucidate the disease burden of NP in China. Joinpoint software (version 4.9.0.1; National Cancer Institute, Rockville, MD, USA) was used to develop the linear statistical models.31 The objective of this study was to identify the optimal model and examine the temporal trends in the disease burden of NP in China, as indicated by the estimation of the average annual percent change (AAPC). Statistical significance was set at P< 0.05. Furthermore, SPSS Statistics (version 29.0) will be used to construct an ARIMA model to project the incidence, prevalence, and DALYs of NP in China from 2022 to 2042, maintaining a significance level of α = 0.05.
Decomposition Analysis
Decomposition analysis was used to provide a visual representation of the contributions of the three factors affecting variations in DALYs from 1990 to 2021, which pertain to the underlying age-and population-adjusted mortality and morbidity rates.32
Results
Overall Burden of NP in China from 1990 to 2021
Disease burden and the trends of NP in China are represented in Tables 1 and 2. In 2021, the number of NP cases in China was 10,292,099 (95% CI: 8062750, 13,039,595), representing a 66.21% increase compared with 1990. The age-standardised incidence rate (ASIR) increased from 558.53 per 100,000 in 1990 to 567.23 per 100,000 in 2021, representing a change rate of 1.56%. The EAPC was 0.08% (0.06, 0.11) (P<0.05). In 2021, there were 48,377,403 (95% CI: 37665090, 60063295) prevalent cases of NP in China, marking an increase of 82.35% since 1990. The age-standardised prevalence rate (ASPR) increased from 2,479.42 per 100,000 in 1990 to 2,549.87 per 100,000 in 2021, representing a change rate of 2.84%. The EAPC was 0.13% (0.10, 0.16) (P<0.05). In 2021, the DALYs for NP in China amounted to 4,807,593 person-years, reflecting an increase of 79.71% compared with 1990. The DALYs rate increased from 248.00 per 100,000 in 1990 to 254.77 per 100,000 in 2021, representing a change rate of 2.36%. EAPC was 0.13% (0.10, 0.16) (P<0.05).
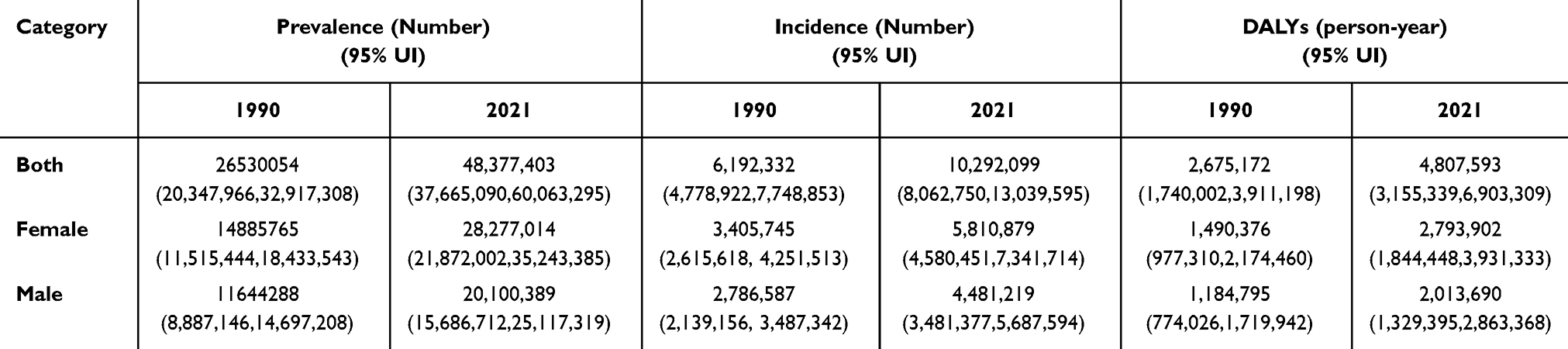 |
Table 1 Disease Burden of Neck Pain in China, 1990–2021 |
 |
Table 2 Disease Burden and the Trends of Neck Pain in China, 1990–2021 |
The Disease Burden of NP Among Different Sexes in China from 1990 to 2021
When comparing males and females in 1990 vs 2021 (Tables 1 and 2), or when comparing males and females at either study time point, we observed a gradual increase in age-standardised incidence and prevalence rates. Furthermore, the number of incident cases, prevalent cases, incidence rates, and prevalence rates among females from 1990 to 2021 were significantly higher than those among males. The detailed analysis is as follows.
In 2021, the number of NP incident cases among males in China was 4,481,219 (95% CI: 3481377,5,687,594), representing an increase of 60.81% compared with 1990. The ASIR increased from 491.91 per 100,000 in 1990 to 495.84 per 100,000 in 2021, with a change rate of 0.80%. The EAPC was 0.06% (P<0.05). In 2021, the number of NP- predominant cases among men in China was 20,100,389 (95% CI: 15686712, 25,117,319), representing an increase of 72.62% compared with 1990. The ASIR increased from 2123.91 per 100,000 in 1990 to 2148.84 per 100,000 in 2021, representing a change rate of 1.18%. The EAPC was 0.07% (P<0.05). In 2021, the DALYs for NP among men in China totalled 2,013,690 person-years, reflecting an increase of 69.96% compared with 1990. The DALYs rate increased from 214.03 per 100,000 in 1990 to 216.09 per 100,000 in 2021, resulting in a change rate of 0.93%. The EAPC was 0.07% (P<0.05), Figures 1 and 2.
 |
Figure 1 Age-standardized Incidence (per 100,000 population) and number of prevalent cases of females and males in China from 1990 to 2021. |
 |
Figure 2 Age-standardized prevalence (per 100000 population) and number of prevalent cases of females and males in China from 1990 to 2021. |
In 2021, the number of NP incidence cases among females in China was 5,810,879 (95% CI: 4580451, 7,341,714), representing an increase of 70.62% compared with 1990. The ASIR increased from 630.29 per 100,000 in 1990 to 641.37 per 100,000 in 2021, representing a change rate of 1.76%. The EAPC was 0.09% (P<0.05). In 2021, the number of NP prevalent cases among females in China was 28,277,014 (95% CI: 21872002,35,243,385), marking an increase of 89.96% compared with 1990. The ASPR increased from 2855.52 per 100,000 in 1990 to 2957.42 per 100,000 in 2021, representing a change rate of 3.57%. The EAPC was 0.16% (P<0.05). In 2021, the DALYs for NP among males in China was 2,793,902 person-years, reflecting an increase with 87.46% compared to 1990. The DALYs rate increased from 284.09 per 100,000 in 1990 to 294.19 per 100,000 in 2021, resulting in a change rate of 3.52%. The EAPC was 0.16% (P<0.05), Tables 1 and 2.
The Disease Burden of NPs Across Different Age Groups in China from 1990 to 2021
Figure 3 shows the prevalence, incidence numbers, and ASRs of NP among different age groups in 2021. The national age-standardised incidence of NP initially increased from the 30–34 age group to the 55–59 age group before declining in the older age groups in 2021. NP is more prevalent among individuals aged 30–34 years and shows a rapid increase between 30 and 49 years. Similar trends were observed regarding the incidence, with a significant increased observed after 30 years of age. The highest incidence peaks occurred between 45 and 59 years of age. Women exhibited higher prevalence rates, incidence rates, and numbers of both incident and prevalent cases than men.
 |
Figure 3 (A) 2021 Age-specific incidence number. (B) 2021 Age-standardized incidence rate. (C) 2021 Age-specific prevalence number. (D) 2021 Age-standardized prevalence rate. |
In 2021, the incidence rate of NP in China reached its peak at 1,129.81 per 100,000 individuals aged 55–59 years. This figure indicates an 11.9% increase for this cohort compared with data from 1990. The EAPC for this age group was 0.42% (P<0.05). In the same year, the prevalence of NP in China reached its highest level of 5,901.49 per 100,000 individuals aged 60–64. This indicates a significant increase of 15% for this age group compared with 1990, with an EAPC of 0.57% (P<0.05). Additionally, in 2021, the DALYs rate of NP in China peaked at 576.69 per 100,000 for the age group of 60–64 years, This represents an increase in this age group compared with 1990, with a change rate of 15%. The EAPC was 0.56 (P<0.05), Tables 3.
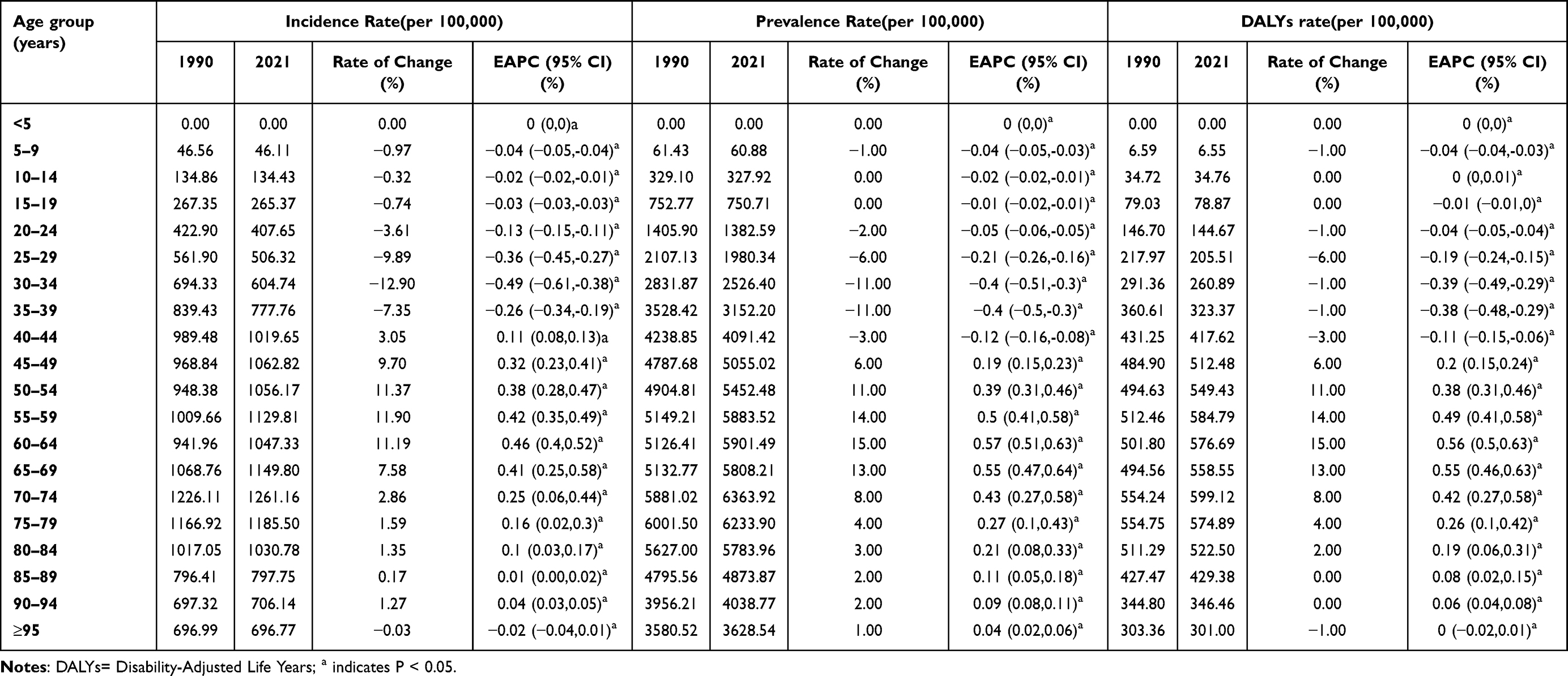 |
Table 3 Disease Burden and the Trends of Neck Pain in Different Age Groups in China, 1990–2021 |
Joinpoint Regression Analysis
The joinpoint regression analysis of the sex-specific age-standardized incidence and prevalence rates of NP in China from 1990 to 2021 is shown in Figure 4. During this timeframe, both male and female populations exhibited a rapid increase in the ASIR of NP between 2006 and 2009, with an annual percentage change (APC) of 0.80 (95% CI: 0.76, 0.83) for males and 0.75 (95% CI: 0.74, 0.76) for females. Significant changes were observed in 2006. Following 2009, the incidence trend showed a moderate for both sexes (Figure 4A–C). Nevertheless, the incidence continued to rise annually, and the prevalence rates exhibited a similar upward trajectory (Figure 4D–F). The AAPC for males and females from 1990 to 2021 was calculated to be 0.03 (95% CI: 0.02, 0.03) and 0.06 (95% CI: 0.05, 0.06), respectively, as represented in Table 4.
 |
Table 4 Joinpoint Regression Analysis: Trends in Age-Standardized Incidence, Prevalence Rates (per 100,000 Persons) Among Both Sexes, Males, and Females in China, 1990–2021 |
 |
Figure 4 Joinpoint regression analysis of the sex-specific age-standardized incidence rate and prevalence rate for NP in China from 1990 to 2019. (A) Age-standardized incidence rate for females. (B) Age-standardized incidence rate for males. (C) Age-standardized incidence rate for both. (D) Age-standardized prevalence rate for females. (E) Age-standardized prevalence rate for males. (F) Age-standardized prevalence rate for both. |
Figure 4 illustrates the AAPC in the incidence and prevalence rates of NP over 3 decades. From 1990 to 2021, age-standardised incidence and prevalence rates of NP in China increased by 0.05 (95% CI: 0.04, 0.05) and 0.09 (95% CI: 0.08, 0.09), respectively. It is noteworthy that females displayed higher AAPC incidence and prevalence rates than males.
Decomposition Analysis of Age-Standardized DALY Rates
Over the past 3 decades, there has been a significant increase in the number of DALYs in China, with the most substantial increase being observed in the female population. Aging has had the largest impact, contributing 61.88% of the increase, where population growth has accounted for 32.43%, as illustrated in Table 5 and Figure 5. The effect of epidemiological changes increase in DALYs was 5.96%, with a more significant effect observed in females, reaching 6.83%.
 |
Table 5 Changes in DALYs Number According to Population-Level Determinants and Causes From 1990 to 2019 |
 |
Figure 5 Changes in neck pain DALYs according to population-level determinants of population growth, ageing, and epidemiological change from 1990 to 2021 in China. The black dot represents the overall value of change contributed by all three components. The magnitude of a positive value indicates a corresponding increase in neck pain DALYs attributed to the component. |
Results and Test of the Forecasting Model
The results of the Augmented Dickey-Fuller (ADF) test conducted on the time series data for NP in both male and female participants revealed that all series were nonstationary. Consequently, the time series of NP must be differentiated to obtain a steady-state sequence. According to the ADF test results (using the Unit root-test function), the incidence and prevalence of NP after applying a first-order difference, were stable in both male and female participants (male participants, P<0.001; female participants, P<0.001; both participants, P<0.001). This suggests that d=1 for both sexes.
The ACF and PACF were used to estimate other parameters. The ARIMA (2, 1, 1), ARIMA (3, 1, 0), and ARIMA (2, 1, 1) models were identified as optimal for forecasting the trend of NP incidence in both male and female individuals, the model parameters are detailed in the Supplementary Tables S1–S3 and Supplementary Figures S1–S9. Similarly. the ARIMA (2, 1, 1), ARIMA (3, 1, 0), and ARIMA (2, 1, 1) models were deemed optimal for forecasting trends in NP prevalence in both male and female individuals, the model parameters are detailed in the Supplementary Tables S4–S6 and Supplementary Figures S10–S18.
The P-values associated with the parameters were <0.05. The values fitted and predicted according to the ARIMA (2, 1, 1) and ARIMA (3, 1, 0) models are shown in Figure 6. The forecasting outcomes for 2022–2042 are represented in Table 6. From 2021 to 2042, the incidence and prevalence rates of NP will exhibit upward trends across all individuals. According to the predicted results, female individuals experienced rapid increases, whereas only slight increases were observed in male individuals. The ASIR of NP in female individuals is expected to rise to 647.49 per 100,000, whereas that in male individuals is expected to reach 497.47 per 100,000 by 2042. The ASPR of NP in female individuals is anticipated to rise to 3,020.40 per 100,000, whereas that in male individuals is projected to reach 2,161.46 per 100,000 by the same year.
 |
Table 6 Prediction of NP Incidence and Prevalence in China for the Next 20 years According to ARIMA Models With 95% Confidence Interval (per 100,000 Population) |
 |
Figure 6 Forecast of neck pain incidence and prevalence rates (per 100,000) from 2020–2030 through ARIMA. (A) Neck pain incidence in both individuals; (B) Neck pain incidence in male individuals; (C) Neck pain incidence in female individuals; (D) neck pain prevalence in both individuals; (E) neck pain prevalence in male individuals; (F) neck pain prevalence in female individuals. |
Discussion
This study examined the trends associated with the prevalence of NP in China over the past 3 decades. To our knowledge, this is the first analysis of the epidemiological trends of NP in China, using joinpoint analysis combined with the APC model, which was used fit the rate of patients with NP from 1990 to 2021 and to predict the rate of patients with NP in China from 2022 to 2042. NP poses a significant public health challenge to the general Chinese population and has demonstrated an upward trajectory over the last 30 years. The findings indicate that both the number and incidence rates of patients with NP in China have been increasing since 1990, particularly among middle- aged and young adults, specifically those aged 35–60 years, across both sexes. This study illustrates that the incidence of NP in 2021 exhibited a general increase with advancing age in males and females. The ASIR of NP was higher in females than in males. Additionally, in all age groups, the incidence of NP was higher in females than in males, corroborating the findings of previous research.33
As shown in Figures 1 and 2, the disparity in incidence and prevalence rates between men and women has increased significantly between 1990 and 2021. In 2021, the incidence rate of neck pain among Chinese women was 29.4% higher than that of men, with a 27.3% higher prevalence rate. Multiple factors may contribute to this disparity. Women exhibit a greater cervical spine range of motion, however, their neck muscles typically have a smaller cross-sectional area, weaker strength, and lower endurance compared to men, resulting in reduced cervical stability.34 Research indicates that women with a forward head posture exceeding 20° face a 2.19-fold higher risk of neck pain compared to men (OR = 2.19). Postmenopausal estrogen decline accelerates bone loss and intervertebral disc degeneration in women.35 Chinese women have a high labor force participation rate, primarily in the education and healthcare sectors,36 where prolonged neck flexion or repetitive movements are required. Additionally, Chinese women spend significantly more time daily on household chores than men, maintaining their neck muscles in a tense state. They also experience heightened social and psychological stress stemming from the dual pressures of career advancement and family responsibilities, accompanied by more pronounced anxiety and depression symptoms. Psychological stress exacerbates muscle tension by activating the sympathetic nervous system.37 However, women are more likely to seek medical treatment proactively, while men tend to rely on non-medical methods (such as massage and rest) to relieve symptoms, which may contribute to the observed statistical disparities.
Joinpoint regression analysis showed that the incidence and prevalence rates of NP sharply increased from 2005 to 2009, followed by a gradual deceleration in this growth trend. Several factors may have contributed to this observation. First, with the implementation of the reform and opening-up policy in China, there has been a significant increase in mechanisation and automation. During this period, the Chinese population experienced increased income levels and heightened health awareness, which resulted in a preference for less physically demanding occupations. This transition may explain the rapid decline in the incidence of NP in China between 1995 and 2000. Second, as China’s economy has developed and transformed, a growing proportion of the working-age population spends most of their time in front of computers,38 frequently looking down at electronic mobile devices and maintaining sustained postures. This trend contributes to the increased incidence of NP. Third, many individuals begin working with their cervical spine in flexion for prolonged periods. The most affected occupations include those that require continuous work with the hands above the head or elbows above the shoulders, such as teachers, dentists, and painters. Long-term desk work, such as that performed by office and computer workers; and high-intensity jobs that place stress on the cervical spine, such as pilots and competitive athletes. Additionally, obesity, sleep problems, lifestyle choices, psychosocial stress, awkward or sustained postures, psychological factors (including stress, anxiety, and cognitive issues),39 and poor overall healthcare risk factors for NP.
DALYs are widely recognised as the standard metric for assessing the burden of disease, which is determined by aggregating YLLs due to premature mortality and YLDs. Given the absence of evidence indicating that mortality is directly attributable to NP, we opted to use YLDs to measure the burden of NP. The ASPR of NP exhibited only a modest increase, from 2479.42 per 100,000 in 1990 to 2549.87 per 100,000 in 2021, representing a change rate of 2.84%; however, the population increase and ageing contributed to the growth of YLDs. Specifically, the YLDs associated with NP increased by 79.71%, from 2675.17×103 (95% UI: 1740.00, 3911.20) in 1990 to 4807.59×103 (95% UI: 3155.34, 6903.31) in 2021.
Decomposition analysis was performed to assess the impact of population growth, ageing, and epidemiological transitions on the burden of disease. In China, it was reported that 32.43% of the increase in DALYs was attributed to population growth, whereas population aging accounted for 61.88%, and epidemiological changes contributed 5.96%. Population growth and ageing are the two primary drivers of changes in DALYs. Females exhibit greater vulnerability to the effects of ageing than males. Menstrual cycle-related biological fluctuations and hormonal factors may significantly influence the aetiology and pathophysiology of various musculoskeletal degenerative diseases. However, women in China have a considerably longer life expectancy than men.40,41
NP is a significant personal and socioeconomic burden in society. Unlike fatal diseases, such as cancer, diabetes, and cardiovascular diseases, NP is non-fatal. NP does not directly lead to death; 42 however, it significantly affects the YLD. In China, NP remains a pressing public health concern. Achieving a thorough understanding of the epidemiological trends and influencing factors related to the burden of NP in China, as well as accurately forecasting its future trajectory, can serve as a valuable reference for health departments conducting epidemiological research on conditions such as NP. Furthermore, it can provide essential data to support the formulation of prevention and control strategies for NP in China, while offering theoretical support for proactive prevention and control efforts.
The ARIMA model forecasts that both the incidence and prevalence of NP among female and male individuals in China will increase over the next 20 years. This represents the inaugural application of the ARIMA model for forecasting the incidence and prevalence of NP in China, thereby rendering direct comparisons with previous studies infeasible. Nevertheless, the actual incidence curve has thus far aligned with the predicted curve, with all observed values remaining within the 95% CI of the forecast figures. This alignment indicated that the chosen models exhibited a strong fit and were suitable for predicting the incidence of NP in China over the next 20 years. The findings imply an increased risk of NP.
Medical insurance policies and healthcare-seeking behaviors are interrelated factors that jointly influence the prevalence and incidence of neck pain. Following the launch of the “Healthy China 2030” initiative in 2016, basic medical insurance coverage for urban and rural residents increased from 89% to 97%. Neck pain was classified as both a chronic disease and a condition prioritized for traditional Chinese medicine (TCM) interventions. Concurrently, outpatient reimbursement rates rose from 50% to 70%, reaching 80% in eastern provinces. These measures reduced financial barriers to healthcare access, thereby improving the diagnosis rate of neck pain.
The majority of existing research has concentrated on the diagnosis and treatment of NP and related musculoskeletal disorders; however, with a relative scarcity of studies addressing preventive measures for NP. Recently, a three-arm cluster randomised controlled trial demonstrated that interventions aimed at increasing active breaks or postural shifts significantly reduced the incidence of new-onset NP in high-risk office workers.43 According to a systematic review and meta-analysis of randomised controlled trials, exercise interventions can effectively reduce NP risk within 12 months.
Improving people’s awareness of taking physical activity is an important part of Healthy China 2030 plan.44 Physical Activity Guidelines for Chinese People (2021)45 provide detailed guidance on the types and time of exercises for different groups of people.
To prevent neck pain, a multidimensional “socioecological-behavioral-psychological-biomechanical” intervention framework should be established. First, the vicious cycle of sedentary lifestyles and musculoskeletal compensation must be disrupted. Implementing active workstations (including standing desks and intermittent neck-shoulder stretches) can help limit daily sitting time to under six hours. Second, precision health strategies should be prioritized. For women experiencing neck muscle hypertonicity linked to anxiety, redirecting stressors through music therapy and group sports is recommended. Collaborative efforts between teachers and parents are needed to improve adolescents’ reading/writing postures and electronic device ergonomics. Older adults should focus on strengthening deep cervical stabilizers through resistance training (such as elastic band exercises). Employers must optimize workplace ergonomics by minimizing prolonged repetitive tasks and excessive physical strain. Additionally, they should provide training on proper biomechanical techniques and tailor work tasks to individual capabilities through adaptive exercises. Notably, combining sleep environment modifications (such as cervical curvature-supporting pillows) with cognitive-behavioral interventions synergistically alleviates chronic neck muscle strain. Targeted neck-strengthening regimens, including cervical stabilization exercises, yoga, and Pilates, can improve muscular strength and biomechanical stability. This study underscores that multi-sectoral collaboration—spanning families, schools, healthcare systems, employers, and governments—is essential to transition public health strategies from “pain management” to “proactive prevention”, thereby advancing population-wide cervical health literacy.
This study describes the most extensive estimates of the prevalence, incidence, and DALYs associated with NP in China; however, it has certain limitations. First, the data used in this study were obtained from the GBD 2021, with some findings derived from the models rather than direct measurements of the original data. Second, the analysis predominantly focused on population-level trends, which may have resulted in ecological fallacies when interpreting individual-level outcomes. Third, our study only provide a statistical description of the burden of NP in China and did not provide comparative analyses with other countries and provinces. For instance, comparisons between Chinese and European individuals are insufficient because focusing solely on the NP when addressing spinal pain is inadequate. Besides what’s mentioned above, it’s necessary to think about Limitations of predictive models, The current ARIMA model, relying solely on historical population structure data, may fail to account for structural shifts (such as government policy interventions and accelerated population aging), leading to potential overestimation of long-term trends. Future studies should adopt multivariate predictive frameworks (such as ARIMAX or machine learning-based time series models) incorporating covariates such as medical insurance penetration rates, aging indices, and GDP per capita growth rates to improve prediction accuracy.
Future research should aim to fill this gap and develop more effective NP prevention strategies.
Conclusions
NP has emerged as a significant public health concern in the general Chinese population. From 1990 to 2021, there was a consistent increase in the age-standardised prevalence, incidence rates, and DALYs associated with NP. Population growth and ageing are the two primary factors driving changes in DALYs. The findings suggest that the relative burden of NP has increased over the last 3 decades. Therefore, NP should be prioritized in future research focusing on its prevention and treatment, particularly considering the increasingly ageing population in China.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Informed Consent
There are no human participants in this article and informed consent is not required.
Acknowledgments
We extend our sincere appreciation to the collaborators of the Global Burden of Disease Study 2021 for their invaluable contributions and unwavering dedication. Their efforts have substantially enhanced our understanding of disease burden and laid a solid foundation for formulating effective strategies to address neck pain in China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 82305280 and 82205152]; Capital’s Funds for Health Improvement and Research [grant number 2022-2-4163]; Science and Technology Innovation Project of China Academy of Chinese Medical Sciences [grant number CI2021A02004]; Construction Project of Key Traditional Chinese Medicine Specialty (Orthopedics and Traumatology) in Chaoyang District, Beijing.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. Wu A, Dong W, Zeng X, et al. Neck pain is the leading cause of disability burden in China: findings from the global burden of disease study 2017. Ann Transl Med. 2021;9(9):777. doi:10.21037/atm-20-6868
2. Qiu Y, Li H, Yang Z, et al. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: results from the China health and retirement longitudinal study. BMC Health Serv Res. 2020;20(1). doi:10.1186/s12913-020-05461-6
3. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783–792. doi:10.1016/j.berh.2011.01.019
4. Li Y, Zhang S, Shu P. Global burden of neck pain in 204 countries from 1990–2019. Arch Med Sci. 2023;19(6):1811–1821. doi:10.5114/aoms/170962
5. Williams FMK, Sambrook PN. Neck and back pain and intervertebral disc degeneration: role of occupational factors. Best Pract Res Clin Rheumatol. 2011;25(1):69–79. doi:10.1016/j.berh.2011.01.007
6. Shin DW, Shin JI, Koyanagi A, et al. Global, regional, and national neck pain burden in the general population, 1990–2019: an analysis of the global burden of disease study 2019. Front Neurol. 2022;13:955367. doi:10.3389/fneur.2022.955367
7. Gill TK, Mittinty MM, March LM. Global, regional, and national burden of other musculoskeletal disorders, 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(11):e670–e682. doi:10.1016/S2665-9913(23)00232-1
8. Zhu K, Devine A, Dick IM, Prince RL. Association of back pain frequency with mortality, coronary heart events, mobility, and quality of life in elderly women. Spine. 2007;32(18):2012–2018. doi:10.1097/BRS.0b013e318133fb82
9. Williams A, Kamper SJ, Wiggers JH, et al. Musculoskeletal conditions may increase the risk of chronic disease: a systematic review and meta-analysis of cohort studies. BMC Med. 2018;16(1):167. doi:10.1186/s12916-018-1151-2
10. Tu WJ, Zeng X, Liu Q. Aging tsunami coming: the main finding from China’s seventh national population census. Aging Clin Exp Res. 2022;34(5):1159–1163. doi:10.1007/s40520-021-02017-4
11. Akimov AV, Gemueva KA, Semenova NK. The seventh population census in the PRC: results and prospects of the country’s demographic development. Her Russ Acad Sci. 2021;91(6):724–735. doi:10.1134/S1019331621060083
12. Lancet T. The best science for achieving healthy China 2030. Lancet. 2016;388(10054):1851. doi:10.1016/S0140-6736(16)31842-6
13. Murray CJL. Findings from the global burden of disease study 2021. Lancet. 2024;403(10440):2259–2262. doi:10.1016/S0140-6736(24)00769-4
14. Kazeminasab S, Nejadghaderi SA, Amiri P, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23(1):26. doi:10.1186/s12891-021-04957-4
15. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Lond Engl. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
16. Ferreira ML, de Luca K, Haile LM. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(6):e316–e329. doi:10.1016/S2665-9913(23)00098-X
17. Guzman J, Hurwitz EL, Carroll LJ, et al. A new conceptual model of neck pain: linking onset, course, and care: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine. 2008;33(Supplement):S14–S23. doi:10.1097/BRS.0b013e3181643efb
18. Cj M, Ad L. Global mortality, disability, and the contribution of risk factors: global burden of disease study. Lancet Lond Engl. 1997;349(9063). doi:10.1016/S0140-6736(96)07495-8
19. Charles Mock MD, Nathan CM. The global burden of musculoskeletal injuries: challenges and solutions. Clin Orthop. 2008;466(10). doi:10.1007/s11999-008-0416-z
20. Steinmetz JD, Culbreth GT, Haile LM. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the global burden of disease study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
21. Minghelli B. Musculoskeletal spine pain in adolescents: epidemiology of non-specific neck and low back pain and risk factors. J Orthop Sci off J Jpn Orthop Assoc. 2020;25(5):776–780. doi:10.1016/j.jos.2019.10.008
22. National Health Commission of the People’s Republic of China, Ministry of Education of the People’s Republic of China, Ministry of Science and Technology of the People’s Republic of China, National Administration of Traditional Chinese Medicine of the People’s Republic of China. Measures for ethical review of life science and medical research involving human participants. 2023. Available from: https://www.gov.cn/zhengce/zhengceku/2023-02/28/content_5743658.htm.
23. Uthman OA. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet Lond Engl. 2016;388(10053):1603–1658. doi:10.1016/S0140-6736(16)31460-X
24. Kassebaum NJ, Smith AGC, Bernabé E, et al. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96(4):380–387. doi:10.1177/0022034517693566
25. Dong Y, Peng R, Kang H, et al. Global incidence, prevalence, and disability of vertebral fractures: a systematic analysis of the global burden of disease study 2019. Spine J off J North Am Spine Soc. 2022;22(5):857–868. doi:10.1016/j.spinee.2021.12.007
26. Ding W, Hu S, Wang P, et al. Spinal cord injury: the global incidence, prevalence, and disability from the global burden of disease study 2019. Spine. 2022;47(21):1532–1540. doi:10.1097/BRS.0000000000004417
27. Newbold P. ARIMA model building and the time series analysis approach to forecasting. J Forecast. 1983;2(1):23–35. doi:10.1002/for.3980020104
28. Jian Y, Zhu D, Zhou D, et al. ARIMA model for predicting chronic kidney disease and estimating its economic burden in China. BMC Public Health. 2022;22(1):2456. doi:10.1186/s12889-022-14959-z
29. Lou HR, Wang X, Gao Y, Zeng Q. Comparison of ARIMA model, DNN model and LSTM model in predicting disease burden of occupational pneumoconiosis in Tianjin, China. BMC Public Health. 2022;22(1):2167. doi:10.1186/s12889-022-14642-3
30. Chaurasia V, Pal S. COVID-19 pandemic: ARIMA and regression model-based worldwide death cases predictions. SN Comput Sci. 2020;1(5):288. doi:10.1007/s42979-020-00298-6
31. Zhang Y, Liu J, Han X, et al. Long-term trends in the burden of inflammatory bowel disease in China over three decades: a joinpoint regression and age-period-cohort analysis based on GBD 2019. Front Public Health. 2022;10:994619. doi:10.3389/fpubh.2022.994619
32. Xie Y, Bowe B, Mokdad AH, et al. Analysis of the global burden of disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567–581. doi:10.1016/j.kint.2018.04.011
33. Chiang PH, Ju PC, Chiang YC, Wei JC. Correspondence on “incidence trend of five common musculoskeletal disorders from 1990 to 2017 at the global, regional and national level: results from the global burden of disease study 2017. Ann Rheum Dis. 2023;82(2). doi:10.1136/annrheumdis-2020-219522
34. Monticone M, Simone Vullo S, Lecca LI, Meloni F, Portoghese I, Campagna M. Effectiveness of multimodal exercises integrated with cognitive-behavioral therapy in working patients with chronic neck pain: protocol of a randomized controlled trial with 1-year follow-up. Trials. 2022;23(1):425. doi:10.1186/s13063-022-06340-7
35. Wright VJ, Schwartzman JD, Itinoche R, Wittstein J. The musculoskeletal syndrome of menopause. Climacteric J Int Menopause Soc. 2024;27(5):466–472. doi:10.1080/13697137.2024.2380363
36. Czępińska A, Zawadka M, Wójcik-Załuska A, Rzezak-Siwiec A, Gawda P. Association between pain intensity, neck disability index, and working conditions among women employed in horticulture. Ann Agric Environ Med AAEM. 2023;30(3):531–535. doi:10.26444/aaem/162028
37. Moon KY, Shin D. Correlation between psychosocial stresses, stress coping ability, pain intensity and degree of disability in patients with non-specific neck pain. Physiol Behav. 2024;275:114433. doi:10.1016/j.physbeh.2023.114433
38. Derakhshanrad N, Ms Y, Mehrdad R, Saberi H. Neck pain associated with smartphone overuse: cross-sectional report of a cohort study among office workers. Eur Spine J off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. 2021;30(2):461–467. doi:10.1007/s00586-020-06640-z
39. Clair D, Edmondston S, Allison G. Variability in pain intensity, physical and psychological function in non-acute, non-traumatic neck pain. Physiother Res Int J Res Clin Phys Ther. 2004;9(1). doi:10.1002/pri.299
40. Wáng YXJ, Wáng JQ, Káplár Z. Increased low back pain prevalence in females than in males after menopause age: evidences based on synthetic literature review. Quant Imaging Med Surg. 2016;6(2):19906. doi:10.21037/qims.2016.04.06
41. Wang YXJ. Menopause as a potential cause for higher prevalence of low back pain in women than in age-matched men. J Orthop Transl. 2016;8:1–4. doi:10.1016/j.jot.2016.05.012
42. Muscari A, Bianchi G, Forti P, et al. Inverse association between neck pain and all-cause mortality in community-dwelling older adults. Pain Med. 2018;19(12):2377–2386. doi:10.1093/pm/pnx306
43. Waongenngarm P, van der Beek AJ, Akkarakittichoke N, Janwantanakul P. Effects of an active break and postural shift intervention on preventing neck and low-back pain among high-risk office workers: a 3-arm cluster-randomized controlled trial. Scand J Work Environ Health. 2021;47(4):306–317. doi:10.5271/sjweh.3949
44. Dai J, Menhas R. Sustainable development goals, sports and physical activity: the localization of health-related sustainable development goals through sports in China: a narrative review. Risk Manag Healthc Policy. 2020;13:1419–1430. doi:10.2147/RMHP.S257844
45. Composing and Editorial Board of Physical Activity Guidelines for Chinese. physical activity guidelines for Chinese (2021). Zhonghua Yu Fang Yi Xue Za Zhi. 2022;56(1):7–8. doi:10.3760/cma.j.cn112150-20211119-01070
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Characteristics of Chronic Viral Hepatitis in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019
Ashimkhanova A, Syssoyev D, Gusmanov A, Yesmembetov K, Yespotayeva A, Abbay A, Nurpeissova A, Sarria-Santamera A, Gaipov A
Infection and Drug Resistance 2022, 15:3333-3346
Published Date: 27 June 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Association of Triglyceride Glucose Index with Prevalence and Incidence of Diabetic Retinopathy in a Singaporean Population
Neelam K, Aung KCY, Ang K, Tavintharan S, Sum CF, Lim SC
Clinical Ophthalmology 2023, 17:445-454
Published Date: 2 February 2023
Use of Linked Nordic Registries for Population Studies in Hematologic Cancers: The Case of Multiple Myeloma
Abildgaard N, Freilich J, Anttila P, Bent-Ennakhil N, Ma Y, Lassenius M, Ørstavik S, Toppila I, Waage A, Turesson I, Hansson M
Clinical Epidemiology 2023, 15:987-999
Published Date: 18 September 2023
Type 2 Diabetes, the Epidemic: Trends in Prevalence and Incidence, 2004-2020
Overbeek JA, Nijpels G, Swart KMA, Blom MT, Elders PJM, Herings RMC
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1503-1509
Published Date: 28 March 2024