")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Dose-Dependent Effects of Remimazolam on Early Perioperative Neurocognitive Disorders in Elderly Colorectal Cancer Patients Undergoing Laparoscopic Surgery
Authors Liu Z, Zhang X, Wang X, Liu Z, Pang Y
Received 22 November 2024
Accepted for publication 13 June 2025
Published 30 June 2025 Volume 2025:19 Pages 5507—5516
DOI https://doi.org/10.2147/DDDT.S502910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Zhenqi Liu, Xinyu Zhang, Xuebing Wang, Ziyang Liu, Yong Pang
Department of Anesthesiology, Affiliated Hospital of North Sichuan Medical College, Nanchong City, Sichuan Province, People’s Republic of China
Correspondence: Yong Pang, Department of Anesthesiology, Affiliated Hospital of North Sichuan Medical College, Nanchong City, Sichuan Province, People’s Republic of China, Tel +86 18784295942, Email [email protected]
Objective: To study the effect of different doses of remimazolam on the maintenance of anesthesia and its impact on postoperative cognitive function in elderly patients undergoing laparoscopic colorectal surgery.
Methods: A total of 120 elderly patients scheduled for laparoscopic colorectal surgery under general anesthesia (both sexes included, ASA grade (II–III) were randomly assigned to experimental groups (R1-R3) and control group (P), with 30 cases per group. The experimental groups received different remimazolam maintenance doses: R1 (0.5 mg/kg/h), R2 (1.0 mg/kg/h), and R3 (1.5 mg/kg/h), while the control group received propofol for sedation. Perioperative cognitive function was evaluated using MMSE (Mini-Mental State Examination) and MoCA (Montreal Cognitive Assessment) preoperatively, and on postoperative days 3 and 7, to analyze differences in cognitive effects and safety profiles of remimazolam across the four groups.
Results: A total of 117 patients were ultimately included, with 3 excluded due to intraoperative conversion to open surgery. Participants were randomly allocated into four groups according to remimazolam maintenance dosing regimens: 30 in the R1 group, 28 in the R2 group, 30 in the R3 group, and 29 in the P group.There was no statistically significant difference in postoperative cognitive function scores between the R2 and R3 groups, and both groups had scores that were significantly higher than those of the R1 and P groups, with statistically significant differences.
Conclusion: Compared to propofol, remimazolam at medium and high doses can reduce the incidence of perioperative neurocognitive dysfunction in elderly patients. High-dose remimazolam anesthesia maintenance may prolong extubation time, increase the incidence of postoperative shivering, and potentially lead to re-sedation after awakening, so medium-dose remimazolam is more suitable for intraoperative anesthesia maintenance in elderly patients without increasing the incidence of adverse events.
Keywords: remimazolam, general anesthesia, elderly, cognitive function
Introduction
The incidence of PND is between 7% and 26% after non-cardiac surgery,1 and it can be as high as 14% to 60% after cardiac surgery.2 Postoperative cognitive dysfunction is more common in the elderly population aged 65 and older. Reports indicate that the incidence of postoperative cognitive dysfunction one week after surgery in adults over 65 years old ranges from 9% to 54%.3 Advanced age is a recognized risk factor for PND, with causes including changes in brain structure, the development of dementia, lower cognitive reserve, and the depletion of the brain’s limited recovery potential.4 Reducing the incidence of postoperative cognitive dysfunction in elderly patients has become a significant challenge. Several studies suggest that remimazolam, a recently introduced benzodiazepine used in clinical anesthesia, may be beneficial in alleviating postoperative cognitive dysfunction in the elderly compared to traditional intravenous sedatives. However, current research primarily focuses on the effects of remimazolam during anesthesia induction on cognitive function in older adults, and there is a lack of studies on its use as a maintenance anesthetic in this population, particularly regarding the impact of different doses on PND. In the initial clinical applications of remimazolam, the Expert Consensus on the Clinical Application of Remimazolam served as the primary reference. However, this consensus does not specify the recommended maintenance dose range for elderly patients. Leveraging our medical center’s extensive experience in colorectal cancer surgeries (with elderly patients accounting for 75.7% of cases), our research team has summarized substantial clinical practice with remimazolam. Building upon the expert consensus, we have identified three maintenance concentrations as a preliminary exploration of optimal dosing strategies.This study aims to explore the effects of different doses of remimazolam on perioperative neurocognitive dysfunction in elderly patients using Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) as cognitive assessment tools, providing a reference for determining the optimal maintenance dosage for anesthesia in older adults.
Materials and Methods
Study Design
From April 2024 to July 2024, 120 elderly patients underwent laparoscopic colorectal cancer surgery at the Affiliated Hospital of North Sichuan Medical College. Researchers not involved in perioperative management and data analysis used computer-generated random numbers to assign patients to groups in the order they were enrolled.This anesthesiologist assessed whether patients met inclusion and exclusion criteria one day before the surgery and obtained informed consent for clinical trials from those who met the inclusion criteria (all patients were from the same surgical team). After entering the anesthesia preparation room, the anesthesia nurse retrieved opaque envelopes from the anesthesiologist. Once the patients were grouped and the verification was completed by all parties, routine anesthesia induction was performed. Two infusion pumps were used for intraoperative medication delivery: Pump 1 was managed by the anesthesia nurse (who did not participate in anesthesia management or data collection and analysis), administering different doses of remimazolam while keeping it concealed. Pump 2 was operated by the anesthesiologist to administer propofol and remifentanil, with the infusion rate adjusted based on the BIS values. After all patient information was collected, the blinding was revealed. The blind files were preserved, and emergency letters were prepared, with the grouping information and intervention details disclosed upon trial termination and completion of data analysis (Figure 1).
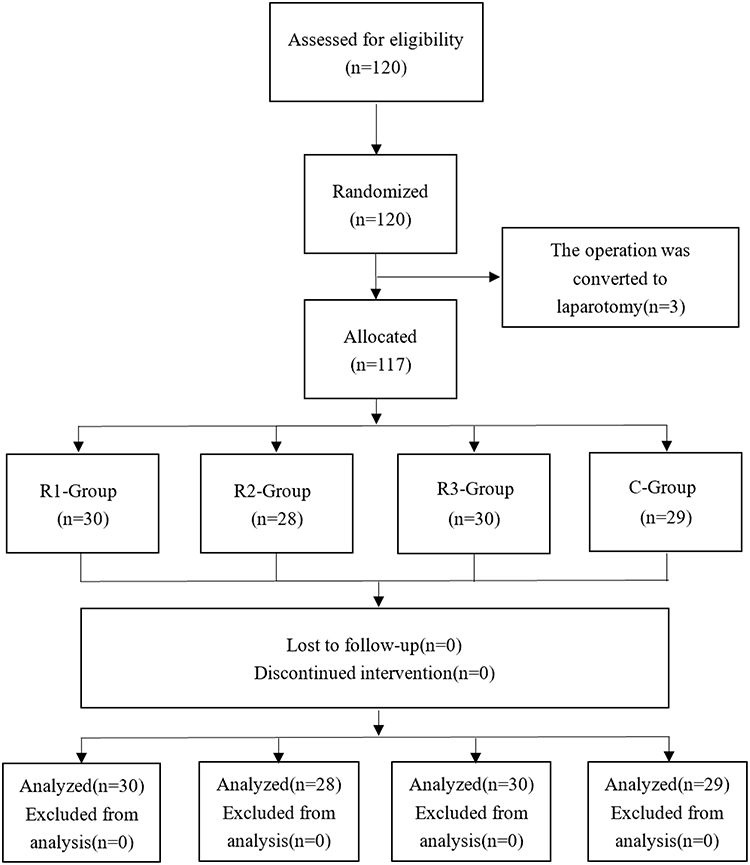 |
Figure 1 The CONSORT Flow Diagram. |
Inclusion Criteria: (a) Patients undergoing elective laparoscopic radical resection for colorectal cancer under general anesthesia, with no restriction on gender; (b) ASA classification: II–III; (c) Age: ≥65 years; (d) Capable of independently completing the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA).
Exclusion Criteria: (a) Preoperative cognitive impairment assessed by Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA) (illiterate preoperative score ≤17, elementary preoperative score ≤20, middle school ≤22, college ≤23); (b) History of cardiac surgery, cerebrovascular accident, or alcoholism; (c) Presence of severe organic diseases, such as liver or kidney dysfunction; (d) Coagulation disorders; (e) Severe visual and hearing impairments that hinder communication; (f) History of mental illness or prolonged use of sedative or antidepressant medications.
Elimination Criteria: (a) Patients who experienced excessive intraoperative bleeding requiring blood transfusion; (b) Patients with adverse reactions to the drugs used or other reasons necessitating premature termination of the study.
This study was authorized by the Ethics Committee of the Affiliated Hospital of North Sichuan Medical College, with ethics approval number [2024ER196-1]. All patients provided informed consent by signing a comprehensive consent form. The trial has been registered with the Chinese Clinical Trial Registry [(ChiCTR2400083122)]. The study protocol adheres to CONSORT guidelines and operates within the scope of relevant guidelines.
Anesthesia Protocol
Upon entering the operating room, standard monitoring is applied, including five-lead electrocardiography (ECG), non-invasive blood pressure (NIBP), heart rate (HR), oxygen saturation (SpO2), and bispectral index (BIS) monitoring for anesthesia depth. A peripheral venous access is established under local anesthesia with 1% lidocaine, and the radial artery is cannulated.
Anesthesia Induction
Following comprehensive preoperative preparation, oxygen is administered by face mask for denitrogenation. Anesthesia is induced sequentially with sufentanil at 0.4 μg/kg, etomidate at 0.1–0.4 mg/kg, and cisatracurium besylate at 0.15 mg/kg. After 3–5 minutes following the administration of cisatracurium besylate, once the BIS value reaches 40–60 and muscle relaxation is adequate for intubation, tracheal intubation is performed. An additional dose of sufentanil at 0.2 μg/kg is given at the time of skin incision. The PETCO2 is maintained at 35–45 mmHg by adjusting tidal volume and respiratory rate.
Anesthesia Maintenance
R1 Group (low-dose group): Continuous infusion of remimazolam tosylate at 0.5 mg/kg/h and remifentanil at 0.05–0.2 μg/kg/min.R2 Group (medium-dose group): Continuous infusion of remimazolam tosylate at 1 mg/kg/h and remifentanil at 0.05–0.2 μg/kg/min.R3 Group (high-dose group): Continuous infusion of remimazolam tosylate at 1.5 mg/kg/h and remifentanil at 0.05–0.2 μg/kg/min.P Group: Continuous infusion of propofol at 1–10 mg/kg/h and remifentanil at 0.05–0.2 μg/kg/min.
Administer vasoactive drugs intraoperatively based on circulatory fluctuations (blood pressure deviation exceeding 20% of the baseline), and adjust the propofol infusion dosage to maintain a BIS value between 40 and 60. Discontinue sedative infusion 10 minutes before the end of surgery. Administer 0.2 mg of flumazenil at the end of surgery. If the patient’s consciousness has not recovered after 1 minute, administer an additional 0.1 mg of flumazenil. If necessary, continue to administer additional doses at intervals until a maximum total dose of 1 mg is reached.
Postoperative Analgesia Protocol
Ten minutes before the end of the surgery, 5 μg of sufentanil is administered as an analgesic bridge. Upon transfer to the Post-Anesthesia Care Unit (PACU), patient-controlled intravenous analgesia (PCIA) is provided with a mixture of sufentanil 100 μg and ondansetron 32 mg.
Observational Indicators
Primary Indicators
Assess patients’ cognitive function using the MMSE and MoCA scales on the day before surgery (T0) and on the 3rd day (T5) and 7th day (T6) after surgery, recording both preoperative and postoperative scores. Calculate the standard deviation of the preoperative MMSE and MoCA scores; if the difference between preoperative and postoperative scores decreases by ≥1 standard deviation from the preoperative standard deviation, cognitive impairment is diagnosed.
Secondary Indicators
Hemodynamic parameters include heart rate (HR) and mean arterial pressure (MAP) changes recorded at the following times: the day before surgery (T0), skin incision (T1), one hour after the start of surgery (T2), at the end of surgery (T3), and upon entering the PACU (T4). Other indicators include intraoperative remifentanil and propofol dosages, extubation time post-surgery, PACU stay duration, and postoperative opioid usage. Pain levels on postoperative days 3 (T5) and 7 (T6) are assessed using the Visual Analog Scale (VAS). Monitor and record any adverse reactions within 48 hours post-surgery in the four groups, such as respiratory depression, hypotension, bradycardia, drowsiness, and nausea or vomiting.
Statistical Methods
Data analysis was conducted using SPSS 26.0 statistical software, and graphs were created with Origin 2021 software. Data with normal or approximately normal distribution are presented as mean ± standard deviation, followed by multi-sample mean-variance analysis. Comparisons of measurements at different time points were performed using repeated measures ANOVA. Data not following a normal distribution are described by median and interquartile range, and comparisons of group means were conducted using the rank-sum test. For count data, n (%) was employed, with either the chi-square test or Fisher’s exact test. A P-value of < 0.05 was considered statistically significant.
Results
General Information
There were no statistically significant differences among the four groups in terms of age, gender, BMI, years of education, surgery duration, ASA classification, or preoperative comorbidities (Table 1).
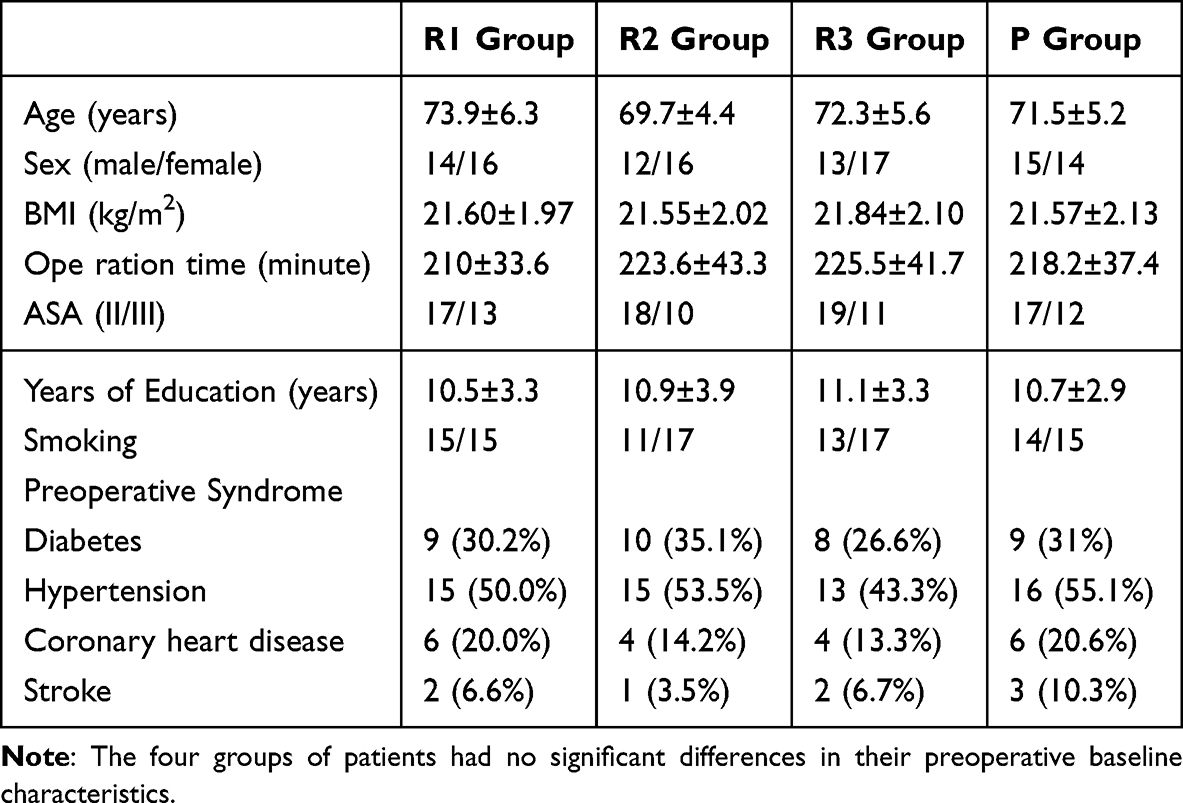 |
Table 1 Preoperative Characteristics of Patients |
Hemodynamic Parameters
At time points T1, T2, and T3, the HR and MAP of patients in groups R2 and R3 were significantly higher than those in groups R1 and P (p < 0.05), with no significant difference between groups R2 and R3. The incidence of intraoperative hypotension was highest in group P and lowest in group R3 (p < 0.05) (Figure 2).
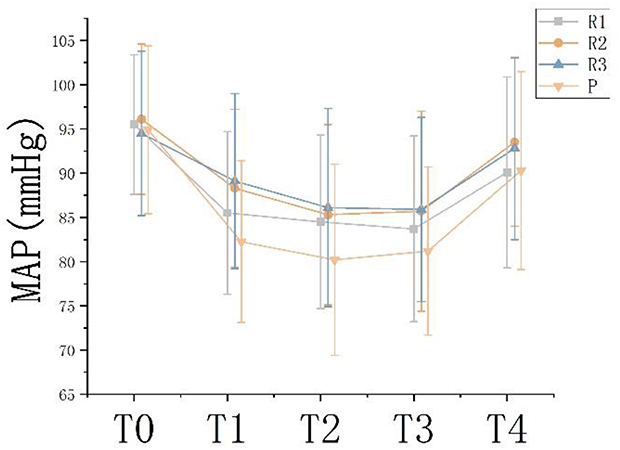 |
Figure 2 MAP at different times. Notes: Data is presented as a Line chart displaying mean ± standard deviation. At time points T1, T2, and T3, the MAP of patients in groups R2 and R3 were significantly higher than those in groups R1 and P. the day before surgery (T0), skin incision (T1), one hour after the start of surgery (T2), at the end of surgery (T3), and upon entering the PACU (T4). |
Anesthesia Indicators
There was no difference in extubation time among the R1, R2, and P groups postoperatively, with all showing significantly shorter times compared to the R3 group. There was no statistically significant difference in PACU stay time among the four groups (p > 0.05), and the intraoperative remifentanil dosage did not differ significantly among the four groups (p > 0.05) (Table 2).
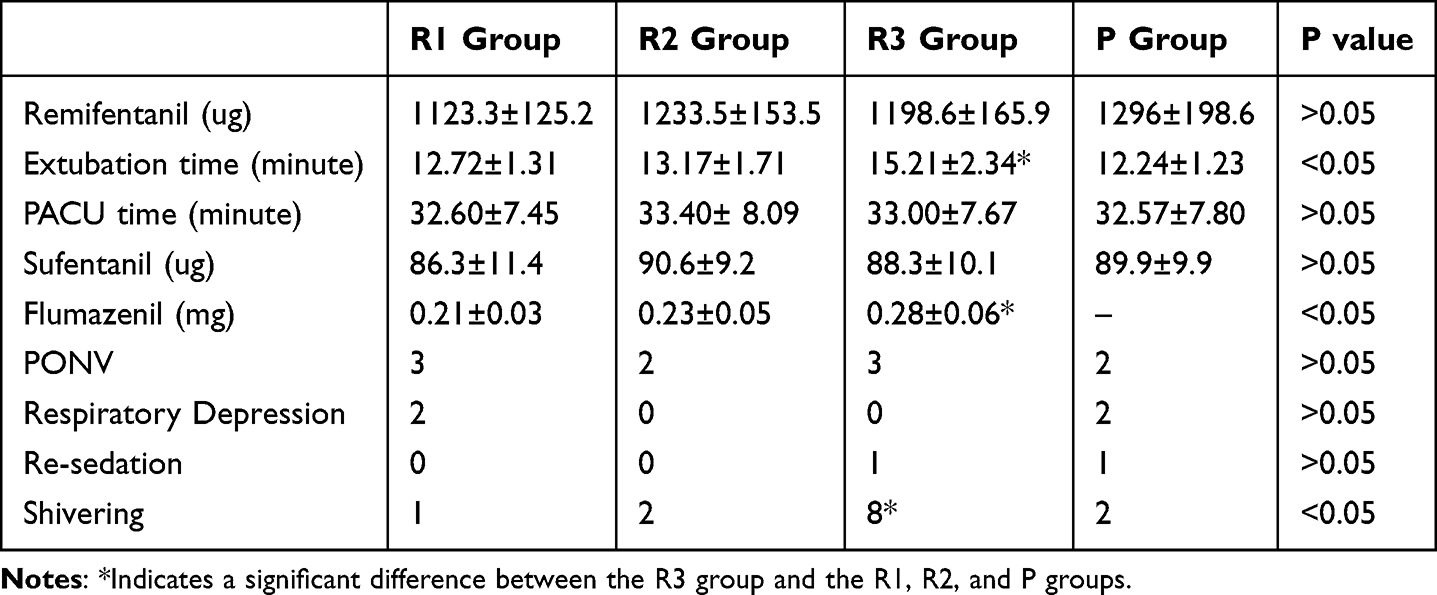 |
Table 2 Secondary Outcome |
Cognitive Function
On the preoperative day (T0), there was no statistically significant difference in MMSE and MoCA scores among the three groups (p > 0.05). At postoperative days 3 (T5) and days 7 (T6), MMSE and MoCA scores for groups R2 and R3 showed no statistically significant difference (p > 0.05), but both groups scored significantly higher than groups R1 and P (p < 0.05) (Figures 3 and 4).
 |
Figure 3 MMSE Scores at different times. Notes: Data is presented as a bar chart displaying mean ± standard deviation.*R2 and R3 groups scored significantly higher than groups R1 and P.preoperative day (T0);postoperative days 3 (T5); postoperative days 7 (T6). |
 |
Figure 4 MoCA Scores at different times. Notes: Data is presented as a bar chart displaying mean ± standard deviation. *R2 and R3 groups scored significantly higher than groups R1 and P.preoperative day (T0); postoperative days 3 (T5); postoperative days 7 (T6). |
Comparison of Postoperative Pain and Adverse Reactions During Recovery
On postoperative days 3 (T5) and 7 (T6), the VAS scores and opioid consumption were compared among the four groups. The incidence of postoperative adverse events was lowest in group R2 and highest in group R3 (Table 2).
Discussion
Various risk factors associated with PND have been previously reported. First, advanced age is the most common precipitating factor. A randomized study reported that, among patients over and under the age of 70, the incidence of postoperative cognitive dysfunction in the first week after major non-cardiac surgery was 29% and 23%, respectively. For those aged 60 to 69, the incidence was 36%, while the overall incidence rate was between 2–3%.5 It is essential to adopt effective anesthesia strategies to prevent PND in elderly patients. Researchers hope to find breakthroughs in anesthetic drugs to prevent PND. Studies on commonly used inhalational and intravenous general anesthetics indicate that volatile anesthetics have a greater impact on cognitive function compared to propofol.6 The newly applied, water-soluble, ultra-short-acting benzodiazepine drug remimazolam has demonstrated effectiveness comparable to that of propofol in clinical practice. It features a high clearance rate, small volume of distribution, short half-life, rapid onset, and quick deactivation.7,8 Unlike propofol, remimazolam is metabolized by tissue esterases and eliminated through first-order pharmacokinetics, making it less likely to accumulate or prolong effects even with high single doses, prolonged infusion, or administration to patients with liver or kidney impairment.9,10 Additionally, the sedative effect of remimazolam can be rapidly reversed by flumazenil, greatly enhancing the controllability of anesthesia.11
Previous studies have shown that remimazolam exhibits excellent cognitive protection. In a retrospective analysis of 98 TAVI patients, the incidence of PND within 3 days post-surgery was significantly lower in the remimazolam group compared to the propofol group (8% vs 26%).12 Compared to sevoflurane anesthesia maintenance in elderly patients, the incidence of delirium on postoperative day 3 was significantly lower in the remimazolam group.13 In addition to improvements in subjective scoring, perioperative inflammatory markers were notably reduced in the remimazolam group compared to the propofol group. In elderly patients undergoing hip surgery, remimazolam use resulted in significantly lower postoperative serum cortisol and norepinephrine levels compared to the propofol group.14 Similar to the aforementioned studies, cognitive function scores in the R2 and R3 groups in this study were significantly higher than those in the R1 and P groups postoperatively. In surgeries involving elderly patients, the use of remimazolam appears to be more beneficial for early postoperative cognitive function recovery compared to propofol. Among the four patient groups, the primary intraoperative difference was in hemodynamic changes, with a lower incidence of hypotension in the remimazolam groups. During the peri-anesthesia period, prolonged intraoperative hypotension can increase the risk of postoperative cognitive dysfunction in elderly patients. Intraoperative hypotension may reduce cerebral blood flow, so avoiding hypotension can help maintain effective cerebral perfusion in elderly patients and reduce the risk of PND and other perioperative neurocognitive disorders.15,16 A multicenter retrospective cohort study involving over 300,000 non-cardiac surgery patients indicated that the incidence of postoperative cognitive and functional impairment is directly proportional to the duration of MAP < 55 mmHg, especially in patients undergoing prolonged surgeries.17,18 In addition to the frequency and duration of hypotension, the degree of intraoperative blood pressure fluctuations during the perioperative period is still significantly associated with POD in elderly patients undergoing non-cardiac surgery.19 Therefore, reducing perioperative hypotension and maintaining hemodynamic stability in elderly patients are important measures for decreasing postoperative cognitive dysfunction. In this study, patients in the R2 and R3 groups demonstrated more stable intraoperative blood pressure and a lower incidence of hypotension compared to those in the R1 and P groups. Additionally, mean arterial pressure during surgery was significantly higher in the remimazolam groups than in the propofol group, which may be one of the key reasons why remimazolam more effectively reduces postoperative cognitive dysfunction compared to propofol.
Since the widespread adoption of remimazolam in clinical anesthesia across Asian countries in 2021, most studies have focused on its effects during anesthesia induction on perioperative outcomes. To explore the optimal maintenance dose of remimazolam for elderly patients, we examined its effects on postoperative cognitive function using different maintenance dosages. Sequential methods are often used in clinical trials to determine the optimal dose. However, as remimazolam is a relatively new drug in clinical practice, we based our study on limited clinical experience and safety data to compare the effects of three commonly used maintenance doses (low, medium, and high) on early postoperative cognitive function in elderly patients. Additionally, since a single neurological scale cannot adequately assess cognitive changes in elderly patients, we recognize that the widely used MMSE has low sensitivity and specificity for diagnosing moderate cognitive impairment,20 to overcome the limitations of the MMSE, we used both the MMSE and MoCA scales together to assess patients’ postoperative cognitive function.21 This study demonstrated that the medium-high dose groups exhibited significantly higher postoperative cognitive function scores compared to both the low-dose and propofol-based groups, alongside a marked reduction in the incidence of postoperative cognitive dysfunction among these cohorts.Similar to the propofol group, the low-dose group had a higher incidence of intraoperative hypotension and greater intraoperative blood pressure fluctuations, which may have contributed to the differences in postoperative cognitive function among the three groups. There was no significant difference in postoperative cognitive scores between the medium- and high-dose groups, and their perioperative hemodynamic changes were similar. However, it is worth noting that one patient in the high-dose group experienced re-sedation approximately 30 minutes after receiving flumazenil antagonism upon awakening and transfer to the PACU. The patient entered a drowsy state again, requiring immediate flumazenil administration, and regained consciousness within five minutes. We speculate that factors such as patient age and comorbidities may have reduced the clearance rate of remimazolam, resulting in a high residual concentration after drug discontinuation. When the competitive antagonism of flumazenil weakened, re-sedation occurred. Additionally, the incidence of postoperative shivering was significantly higher in the high-dose group than in the medium-dose group. Previous studies have shown that flumazenil use is associated with an increased incidence of postoperative shivering.22,23 In this experiment, the significantly increased use of flumazenil in the high-dose group appears to support this view. The study results indicate that maintenance with medium- to high-dose remimazolam, compared to propofol and low-dose remimazolam, can significantly reduce the incidence of postoperative cognitive dysfunction in elderly patients. Additionally, the medium-dose group experienced fewer postoperative complications, suggesting that using a medium dose of remimazolam for anesthesia maintenance is safer for elderly patients and helps protect their perioperative cognitive function.
This study has the following limitations. First, other potential adverse effects of remimazolam, such as liver function deterioration, hematologic changes, and possible long-term adverse events, were not adequately considered. The primary evaluation metrics focused on cognitive function scores.Owing to staffing limitations, the present investigation did not evaluate remimazolam’s long-term neurocognitive sequelae in elderly patients or its extrapolation to geriatric populations beyond colorectal surgery. Subsequent phases will extend recruitment to diverse surgical cohorts (eg, orthopedic, urologic) and employ multidimensional metrics (eg, the Quality of Recovery-40 scale), to establish dose-response relationships across heterogeneous demographics.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. For any inquiries regarding the data presented in this study, please contact the corresponding author via email.
Institutional Review Board Statement
This study was authorized by the Ethics Committee of the Affiliated Hospital of North Sichuan Medical College, with ethics approval number [2024ER196-1] and conducted in compliance with the Declaration of Helsinki.
Acknowledgement
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moller JT, Cluitmans P, Rasmussen LS, et al. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet. 1998;351(9106):857–861. doi:10.1016/S0140-6736(97)07382-0
2. Keizer AM, Hijman R, Kalkman CJ, Kahn RS, van Dijk D. The incidence of cognitive decline after (not) undergoing coronary artery bypass grafting: the impact of a controlled definition. Acta Anaesthesiol Scand. 2005;49(9):1232–1235. doi:10.1111/j.1399-6576.2005.00835.x
3. Evered L, Scott DA, Silbert B, Maruff P. Postoperative cognitive dysfunction is independent of type of surgery and anesthetic. Anesthesia Analg. 2011;112(5):1179–1185. doi:10.1213/ANE.0b013e318215217e
4. Keage HA, Smith A, Loetscher T, Psaltis P. Cognitive Outcomes of Cardiovascular Surgical Procedures in the Old: an Important but Neglected Area. Heart Lung Circulation. 2016;25(12):1148–1153. doi:10.1016/j.hlc.2016.09.002
5. Laalou FZ, Carre AC, Forestier C, Sellal F, Langeron O, Pain L. Pathophysiology of post-operative cognitive dysfunction: current hypotheses. J Chirurgie. 2008;145(4):323–330. doi:10.1016/S0021-7697(08)74310-2
6. Zhang Y, Shan GJ, Zhang YX, et al. Propofol compared with sevoflurane general anaesthesia is associated with decreased delayed neurocognitive recovery in older adults. Br J Anaesth. 2018;121(3):595–604. doi:10.1016/j.bja.2018.05.059
7. Lee A, Shirley M. Remimazolam: a Review in Procedural Sedation. Drugs. 2021;81(10):1193–1201. doi:10.1007/s40265-021-01544-8
8. Antonik LJ, Goldwater DR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled Phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part I. Safety, efficacy, and basic pharmacokinetics. Anesthesia Analg. 2012;115(2):274–283. doi:10.1213/ANE.0b013e31823f0c28
9. Stöhr T, Colin PJ, Ossig J, et al. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Br J Anaesth. 2021;127(3):415–423. doi:10.1016/j.bja.2021.05.027
10. Wesolowski AM, Zaccagnino MP, Malapero RJ, Kaye AD, Urman RD. Remimazolam: pharmacologic Considerations and Clinical Role in Anesthesiology. Pharmacotherapy. 2016;36(9):1021–1027. doi:10.1002/phar.1806
11. Chen X, Sang N, Song K, et al. Psychomotor Recovery Following Remimazolam-induced Sedation and the Effectiveness of Flumazenil as an Antidote. Clin Ther. 2020;42(4):614–624. doi:10.1016/j.clinthera.2020.02.006
12. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
13. Fujimoto D, Obata N, Mizobuchi S. Effectiveness of remimazolam in preventing postoperative delirium in elderly patients with proximal femoral fractures. J Anesthesia. 2024;38(4):475–482. doi:10.1007/s00540-024-03339-z
14. Sun Y, Zhang J, Feng S. Remimazolam Supplemented to General Anesthesia Alleviates Stress and Cognitive Impairment in Elder Patients After Hip Surgery. Psychiatry Invest. 2023;20(5):481. doi:10.30773/pi.2022.0323e
15. Scholz AF, Oldroyd C, McCarthy K, Quinn TJ, Hewitt J. Systematic review and meta-analysis of risk factors for postoperative delirium among older patients undergoing gastrointestinal surgery. Br J Surg. 2016;103(2):e21–28. doi:10.1002/bjs.10062
16. Wang J, Li Z, Yu Y, Li B, Shao G, Wang Q. Risk factors contributing to postoperative delirium in geriatric patients postorthopedic surgery. Asia-Pacific Psychiatry. 2015;7(4):375–382. doi:10.1111/appy.12193
17. Wachtendorf LJ, Azimaraghi O, Santer P, et al. Association Between Intraoperative Arterial Hypotension and Postoperative Delirium After Noncardiac Surgery: a Retrospective Multicenter Cohort Study. Anesthesia Analg. 2022;134(4):822–833. doi:10.1213/ANE.0000000000005739
18. Maheshwari K, Ahuja S, Khanna AK, et al. Association Between Perioperative Hypotension and Delirium in Postoperative Critically Ill Patients: a Retrospective Cohort Analysis. Anesthesia Analg. 2020;130(3):636–643. doi:10.1213/ANE.0000000000004517
19. Hirsch J, DePalma G, Tsai TT, Sands LP, Leung JM. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery. Br J Anaesth. 2015;115(3):418–426. doi:10.1093/bja/aeu458
20. Ciesielska N, Sokołowski R, Mazur E, Podhorecka M, Polak-Szabela A, Kędziora-Kornatowska K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatria polska. 2016;50(5):1039–1052. doi:10.12740/PP/45368
21. Wang Q, Zhou M, Zhou Y, Ji J, Raithel D, Qiao T. Effects of Carotid Endarterectomy on Cerebral Reperfusion and Cognitive Function in Patients with High Grade Carotid Stenosis: a Perfusion Weighted Magnetic Resonance Imaging Study. Eur J Vasc Endovasc Surg. 2015;50(1):5–12. doi:10.1016/j.ejvs.2015.03.032
22. Eisenried A, Schüttler J, Lerch M, Ihmsen H, Jeleazcov C. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: part II. Pharmacodynamics of Electroencephalogram Effects. Anesthesiology. 2020;132(4):652–666. doi:10.1097/ALN.0000000000003102
23. Lee B, Kim MH, Kong HJ, et al. Effects of Remimazolam vs. Sevoflurane Anesthesia on Intraoperative Hemodynamics in Patients with Gastric Cancer Undergoing Robotic Gastrectomy: a Propensity Score-Matched Analysis. J Clin Med. 2022;11(9):1.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.