")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Dyadic Effects of Stigma and Self-Compassion on Resilience of Schizophrenic Patients and Caregivers During Recovery: An Actor-Partner Interdependence Mediation Model
Authors Feng J , Du C, Xiao Y, Liu J, Chen Q, Liu Y, Zhang Z
Received 19 December 2024
Accepted for publication 21 March 2025
Published 8 April 2025 Volume 2025:21 Pages 775—790
DOI https://doi.org/10.2147/NDT.S507386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Jingyi Feng,1,2 Conglin Du,3 Yanling Xiao,1 Jie Liu,4 Qiuxia Chen,1 Yaping Liu,1 Zhixia Zhang1
1Nursing Department, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2Institute of Nursing Research, Hubei Province Key Laboratory of Occupational Hazard Identification and Control, School of Medicine,Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Urology, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 4Trauma Surgery, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Correspondence: Yaping Liu; Zhixia Zhang, Nursing Department, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China, Email [email protected]; [email protected]
Purpose: In this study, dyadic analysis was used to explore the dyadic effect of stigma on resilience and whether self-compassion plays a mediating role in the dyadic relationship between schizophrenia patients and primary caregivers during recovery.
Methods: A total of 210 patients with schizophrenia and their primary caregivers from a tertiary hospital in Hubei Province were selected as the research objects by convenience sampling method. The investigation was conducted with the General Information Questionnaire, Stigma Scale, Self-Compassion Scale and Connor-Davidson Resilience Scale.
Results: This study found that the mental illness stigma of patients with schizophrenia at the recovery stage was negatively correlated with their self-compassion and resilience, as well as the self-compassion and resilience of their primary caregivers (r=− 0.644, − 0.653, − 0.431, − 0.362, all P< 0.05). The mental illness stigma of primary caregivers of patients with schizophrenia in recovery period was negatively correlated with self-compassion and psychological resilience, and self-compassion and psychological resilience of patients (r=− 0.291, − 0.430, − 0.375, − 0.282, all P< 0.05). The study found that the mental illness stigma of schizophrenia patients and their primary caregivers had a significant subjective impact on their resilience. The stigma of schizophrenia convalescence patients and their primary caregivers has a significant indirect effect on each other’s psychological resilience through self-compassion.
Conclusion: This study found that stigma not only directly affects the resilience of patients with schizophrenia and their primary caregivers, but also plays a mediating role in the resilience of patients themselves and their caregivers through self-compassion. It is recommended that medical staff carry out intervention based on dyadic perspective to help patients and their caregivers improve their ability to recover from difficulties, adapt and grow from adversity and crisis, attach importance to and promote the close relationship and positive interaction between them, so as to jointly cope with disease challenges and help patients return to society.
Keywords: schizophrenia, caregiver, stigma, resilience, self-compassion, actor-partner interdependence model
Introduction
Schizophrenia is a chronic mental disorder characterized by abnormalities in thinking, emotion, and behavior.1 Patients typically experience cyclical deterioration and resolution, which are characterized by volatility.2 Although timely drug treatment can effectively control the disease, it is often difficult to fully recover the cognitive and basic psychological functions of patients, and it takes a long time to recover.3
Approximately 24 million people worldwide are affected by schizophrenia, accounting for 1 in 300 of the population. With the progress of medical treatment and society, the focus of treatment for patients with schizophrenia has shifted to the psychological level. Caregivers face multiple challenges such as physical, emotional, and social support when undertaking the corresponding care responsibilities, which may damage their mental health. Resilience is the relative resistance to adverse experiences,4 which is a protective factor for mental health. Caregivers with higher resilience can more effectively cope with the psychological stress and negative emotions brought by caring for patients with schizophrenia, which is very important for the rehabilitation of mental illness.5 Patients with schizophrenia have a long course of disease and suffer from discrimination for a long time, which may lead to decline in social skills, difficulty in coping with complex social situations, and unwillingness to seek help, leading to reduced resilience, and then encounter more difficulties in physical rehabilitation and social adaptation.6 Studies have shown that the resilience of patients with schizophrenia is significantly lower than that of unaffected people and patients with other mental disorders.7
According to interdependence theory,8 the interaction of individuals in a close relationship, such as patient and caregiver, has a significant impact on the health outcomes of both parties. Patients with schizophrenia rely on caregivers to provide emotional support, daily care, and medical help, while caregivers rely on patients’ feedback to adjust care strategies, and this dependence may affect the resilience of both parties. Therefore, attention to the resilience of patients and caregivers is essential to maintain mental health, relieve disease symptoms, improve quality of life, and reduce the risk of recurrence. Research has shown that resilience has a positive effect on mental health. For patients with schizophrenia during rehabilitation, stigma is an important factor affecting resilience. Patients with high resilience have stronger adaptability and lower stigma.9 On the contrary, patients with higher stigma have lower resilience, which will affect the recovery process of the disease.10
Stigma is a negative emotion caused by social exclusion and discrimination in patients with schizophrenia,11 which is mostly caused by social misunderstanding and prejudice against mental illness. Stigma was divided into “intrinsic stigma” and “extrinsic stigma”.12 Intrinsic stigma diminishes self-esteem, reduces help-seeking behavior, delays diagnosis and treatment. Extrinsic stigma, originating from public discrimination, leads to self-devaluation, treatment avoidance, and even illness concealment.13 The stigma of patients with schizophrenia during rehabilitation not only affects themselves, but also affects the mental health of their caregivers.14 About 90% of patients with schizophrenia in China live with their families.15 While providing social support for patients, caregivers also suffer from social isolation and discrimination, and have high psychological pressure.16 Chinese caregivers of patients with schizophrenia may suffer from more serious stigma due to special social and cultural factors,17 such as the taboo concept of mental illness in traditional culture, the emphasis on the supremacy of imperial power and the concept of family, and the belief that suffering from mental illness will tarry the family honor.18 This is also an important reason for the serious stigma of domestic patients with mental illness and the discrimination of the public against patients with schizophrenia.19
Stigma can increase the individual’s psychological burden, affect the recovery of emotional regulation and adaptability, and reduce psychological resilience. As a positive emotion regulation strategy,20 self-compassion can promote individuals to accept negative emotions with understanding rather than avoiding them.21
People with higher levels of self-compassion are better able to treat themselves in the face of failure or misfortune, and have higher levels of happiness and positive self-evaluation.22 Self-compassion is considered to be a valuable component in the treatment of schizophrenia and an important structure for the mental health of patients with schizophrenia.23 It can directly improve the stigma of patients and alleviate the negative effects caused by social discrimination.24 Studies have shown that self-compassion is related to resilience,25 but there is a lack of research to explore the relationship between self-compassion and resilience in patients with schizophrenia during rehabilitation.
Previous preliminary studies on self-compassion in caregivers of children with autism have shown that caregivers with a high level of self-compassion have fewer negative emotions such as depression and better psychological health.26 Self-compassion can help caregivers to strengthen their attention and understanding of their own emotional needs in the face of stress and frustration, reduce the accumulation of self-blame and negative emotions, and effectively deal with the negative emotions of caregivers caused by caring for patients with schizophrenia during the recovery period. Cultivating self-compassion of caregivers can not only help to relieve their psychological burden, but also help caregivers to reduce their psychological burden. It also promotes the long-term sustainability and quality of care.27
The actor-object interdependence model is a binary analysis method that is one of the most commonly used models for studying the relationship between patients and caregivers. It is used to assess personal effects (actor effect) and interpersonal effects (partner effect). Individual effects show the influence of individual predictor variables (such as patient stigma) on their outcome variables (such as patient resilience), while interpersonal effects show the influence of individual predictor variables on partner outcome variables (such as caregiver resilience). The Actor-object interdependence mediation model (APIMeM) extends the APIM by adding mediating variables, and can estimate the mediating role of self-compassion in the patient-caregiver relationship.
Previous studies have shown that self-compassion plays a mediating role between stigma and psychological resilience in patients with bipolar disorder.28 However, no research has yet examined the mediating role of self-compassion between stigma and psychological resilience in patients with schizophrenia and their caregivers during the recovery period. Moreover, existing studies have mostly focused on either patients or caregivers individually, often neglecting the mutual interaction and influence between the two in terms of stigma, self-compassion, and psychological resilience. Given that stigma may exacerbate the psychological resilience impairment in patients with schizophrenia, while self-compassion may be a protective factor, it is necessary to further explore the relationship among stigma, self-compassion, and psychological resilience. The relationship between stigma, self-compassion, and psychological resilience in patients and caregivers may vary depending on their respective roles. Considering the interdependence between patients and caregivers, in-depth research on this dual influence model is crucial for understanding the dynamic relationship between stigma and psychological resilience and the mediating role of self-compassion.
This study aims to explore the dual effects of stigma on resilience of patients with schizophrenia and their caregivers during rehabilitation, and the mediating role of self-compassion. The hypotheses of this study include: (1) the stigma of schizophrenia patients and caregivers during recovery is negatively correlated with their own resilience (actor effect); (2) The stigma of schizophrenia patients and caregivers was negatively correlated with the resilience of their partners (partner effect); (3) Self-compassion played a mediating role between stigma and resilience.
Material and Methods
Study Design and Participants
This cross-sectional study was conducted from December 2023 to June 2024, involving the recruitment of patients and their caregivers from the psychiatry department of a tertiary hospital in Wuhan, Hubei Province, China. The sample size was estimated for a medium effect size of 0.2, a two-sided α = 0.05, and power (1-β) =0.80, which are regarded as appropriate to detect actor and partner effects in dyadic data. It was calculated that at least 196 dyads participants would be required. The study initially recruited 215 pairs of schizophrenia patients and their caregivers; after excluding those who withdrew during the questionnaire process and those who completed the questionnaires incorrectly, 210 pairs were included in the final analysis, yielding an effective response rate of 97.67%.
Inclusion and Exclusion Criteria for Patients
The inclusion criteria for patients with schizophrenia are as follows: 1) A diagnosis of schizophrenia that meets the criteria of the International Classification of Diseases (ICD-10). 2) The patient is in the recovery phase, characterized by significant improvement following systematic antipsychotic treatment, with psychiatric symptoms largely resolved and a Brief Psychiatric Rating Scale (BPRS) score of <35. 3) Age between 18 and 65 years. 4) The ability to read and comprehend independently. 5) Informed consent signed by the patient and their guardian.
The exclusion criteria for patients with schizophrenia are as follows: 1) Severe cognitive dysfunction or difficulties in reading, comprehension, or communication. 2) Refusal of conventional psychiatric treatment or poor adherence to care routines. 3) Significant fluctuations in condition during the intervention period leading to a relapse. 4) Voluntary withdrawal from the study by the patient or their guardian. 5) Exclude individuals diagnosed with comorbid psychiatric conditions, including but not limited to depression, bipolar disorder, and anxiety disorders.
Inclusion and Exclusion Criteria for Caregivers
The inclusion criteria for caregivers of patients with schizophrenia are as follows: 1) The individual must be the primary caregiver of the patient during the convalescent phase of schizophrenia, having provided care for more than three months and being well-acquainted with the patient’s condition. 2) No history of mental illness and has basic self-reading and comprehension abilities. 3) Signed informed consent for participation in this study.
The exclusion criteria for caregivers are as follows: 1) Under the age of 18. 2) The primary caregiver is unable to complete the assessment due to hearing or visual impairments or other reasons. 3) The caregiver has a history of cognitive impairment or mental illness, or has recently experienced a major traumatic event or life crisis.
Procedures
This study was conducted in accordance with the principles of the Declaration of Helsinki, and ethical approval was obtained from the ethics Committee of Wuhan University of Science and Technology School of Medicine (2024137). All participants provided written informed consent prior to participation. The investigator provided an overview of the study to the patients and their family members during hospitalization. If patients and caregivers expressed interest in participating, the researcher explained the details, including the study’s purpose, procedures, data confidentiality and security, and participants’ rights. Only those who met the inclusion criteria were allowed to participate. Patients and caregivers were asked to complete questionnaires separately, with no exchange of answers permitted. The questionnaires were collected immediately after completion. The entire survey took approximately 10 to 15 minutes.
Measurements
Internalized Stigma of Mental Illness (ISMI)
Internalized stigma in patients was assessed using the Internalized Stigma of Mental Illness (ISMI) scale,29 which consists of 29 items rated on a Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). The instrument comprises five subscales: alienation, stereotype endorsement, discrimination experience, social withdrawal, and stigma resistance. Total scores range from 29 (indicating no internalized stigma) to 116 (indicating high internalized stigma).
Connor–Davidson Resilience Scale (CD-RISC)
The Connor–Davidson Resilience Scale (CD-RISC) is a widely recognized measure of stress-coping ability. The CD-RISC consists of 25 items, each rated on a 5-point scale ranging from 0 to 4, with higher scores indicating greater resilience. The scale demonstrates high reliability and validity, with a Cronbach’s α of 0.89 for the full scale, indicating good internal consistency.
Self-Compassion Scale (SCS)
The Self-Compassion Scale (SCS) is a 26-item self-report measure using a 5-point Likert scale (1=almost never, 5=almost always) that assesses six dimensions of global self-compassion. These dimensions include “self-kindness” (being understanding and kind towards oneself in difficult times), “self-judgment” (punishing oneself with criticism during suffering), “common humanity” (recognizing that difficulties are part of a shared human experience), “isolation” (feeling isolated by emotional pain and distress), “mindfulness” (being mindful of the present moment by fully accepting feelings, thoughts, and bodily sensations), and “over-identification” (tendency to over-identify with negative experiences). Higher scores indicate greater self-compassion. In the original study,30 the scale demonstrated strong internal consistency, with a Cronbach’s α of 0.92.
Socio-Demographic and Clinical Characteristics
Socio-demographic and clinical characteristics collected from patients with schizophrenia and their caregivers included age, education level, employment status, gender, place of residence, marital status, occupation, course of illness, impulsive behavior in patients, duration of caregiving, monthly per capita household income of caregivers, the relationship between caregivers and patients, caregivers’ attitudes, and caregivers’ knowledge of the disease.
Data Analysis
Descriptive statistics were calculated as means and standard deviations for continuous variables and as proportions and counts for categorical variables. Pearson correlation analysis was conducted to examine the relationships between stigma, self-compassion, and resilience in patient-caregiver dyads. An independent-samples t-test was performed to assess differences in socio-demographic characteristics and study variables between patients and caregivers. In this study, patient-caregiver dyads were treated as distinguishable individuals. The Actor-Partner Interdependence Mediation Model (APIMeM) was employed to test the hypotheses. Preliminary analyses revealed that patients’ education level, age, and duration of illness, as well as caregivers’ disease understanding and caregiving duration, significantly impacted the resilience of both patients and caregivers. Consequently, education level, age, duration of illness, disease knowledge, and caregiving duration were included as covariates in the final APIMeM. Mediation effects were assessed using bootstrapped 95% confidence intervals with 5000 samples. Model fit was evaluated using several goodness-of-fit indices, including χ²/df (acceptable fit <3), the Root Mean Square Error of Approximation (RMSEA, acceptable fit ≤0.08), the Comparative Fit Index (CFI, acceptable fit ≥0.90), the Tucker–Lewis Index (TLI, acceptable fit ≥0.90), and the Normed Fit Index (NFI, acceptable fit ≥0.90). Data analysis was conducted using SPSS (version 23.0) and AMOS (version 24.0) software. Significance was determined at a two-sided p-value of ≤0.05.
Results
General Statistical Data of Schizophrenia Patients and Their Primary Caregivers During Rehabilitation Period
The proportion of patients with schizophrenia was 51.9% male, and the proportion of patients without impulsive behavior was 82.4%. 53.3% of patients had a disease duration of more than 15 years, 17.1% had a disease duration of 11–15 years, and 17.6% had a disease duration of 6–10 years.
50.5% of the caregivers we surveyed were male, and 51% lived in cities. Most of the caregivers have a high school education level or above, with 9.5% in primary school, 29.5% in junior high school, 50.5% in high school, and 10.5% in university. 66.7% of the caregivers were to diligence care them, and 12.4% were forced to take care of them, the remaining 21% are very willing to take care of them. 58.6% of the caregivers knew a little about schizophrenia, 18.1% had a basic understanding, 15.7% knew completely, and 7.6% did not know. The majority of caregivers were spouses (32.4%), mothers (28.6%), fathers (16.7%), siblings (16.7%), sons (1.9%), and daughters (3.8%). 44.8% of caregivers were between 45 and 65 years old, 43.3% were between 18 and 45 years old, and only 11.9% were older than 66 years. The socio-demographic and clinical characteristics of patient-caregiver dyads are summarized in Table 1.
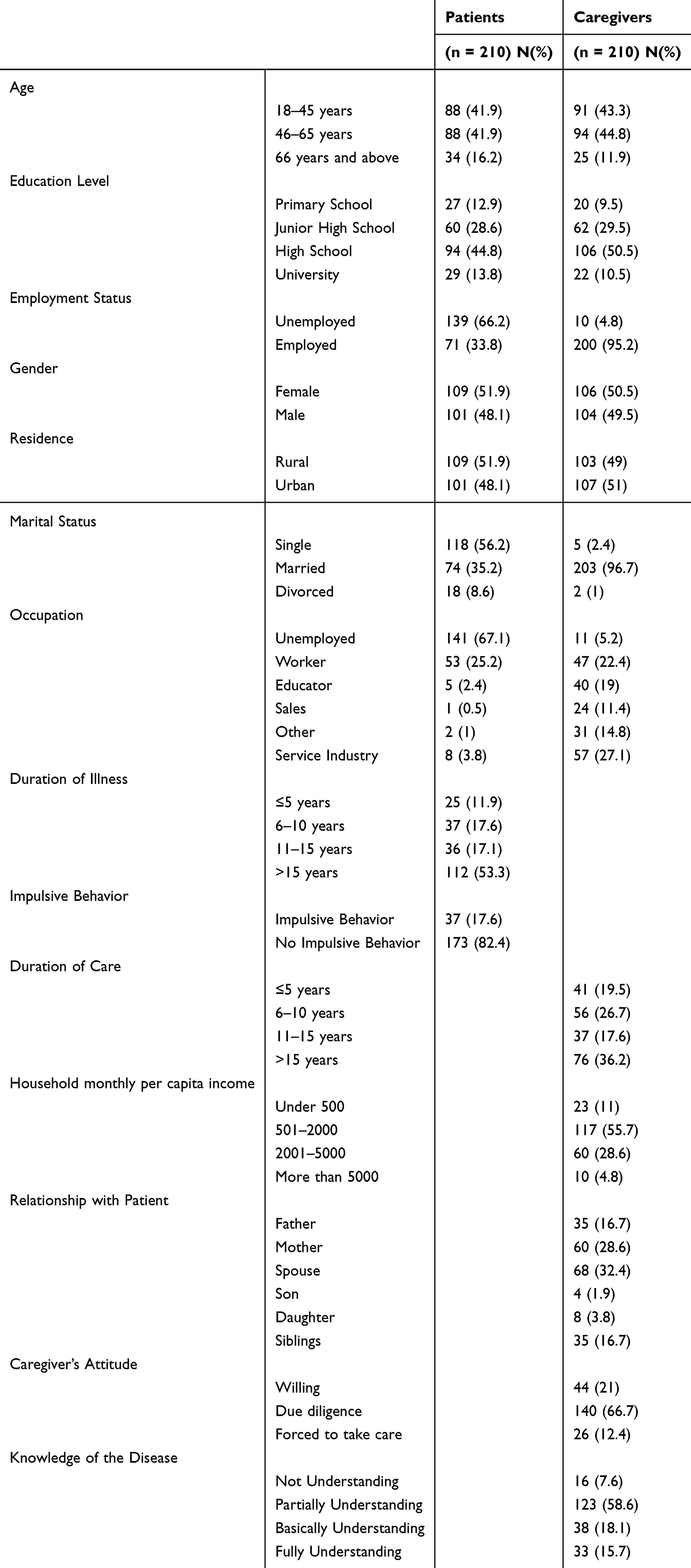 |
Table 1 Sociodemographic Characteristics of the Participants ((N=210 Families) |
Scores of Internalized Stigma, Self-Compassion and Resilience in Patients With Schizophrenia
Differences in patient sociodemographic characteristics and study variables are shown in Table 2. There were statistically significant differences in the scores of stigma, self-compassion and resilience among patients with different work situations, residential areas, ages, education levels, marital status, and specific occupations (all P<0.05). There was a statistically significant stigma score in patients with or without impulsive behavior (P<0.05). There was a statistically significant score of resilience over the duration of the disease (P<0.05).
 |
Table 2 Scores of Internalized Stigma, Self-Compassion and Resilience in Patients With Schizophrenia |
Scores of Internalized Stigma, Self-Compassion and Resilience in Caregiver With Schizophrenia
Differences in caregiver socio-demographic characteristics and study variables are shown in Table 3. There were statistically significant differences in the scores of patients with different work situations, monthly household income, caring attitudes, marital status, stigma, self-compassion and resilience (all P<0.05). There were statistically significant differences in the self-compassion scores of caregivers with different ages, residential areas, education levels, care time, disease understanding, and patient relationships (P<0.05). There were statistically significant differences in the resilience scores of caregivers with different education levels, disease duration, and disease understanding (P<0.05).
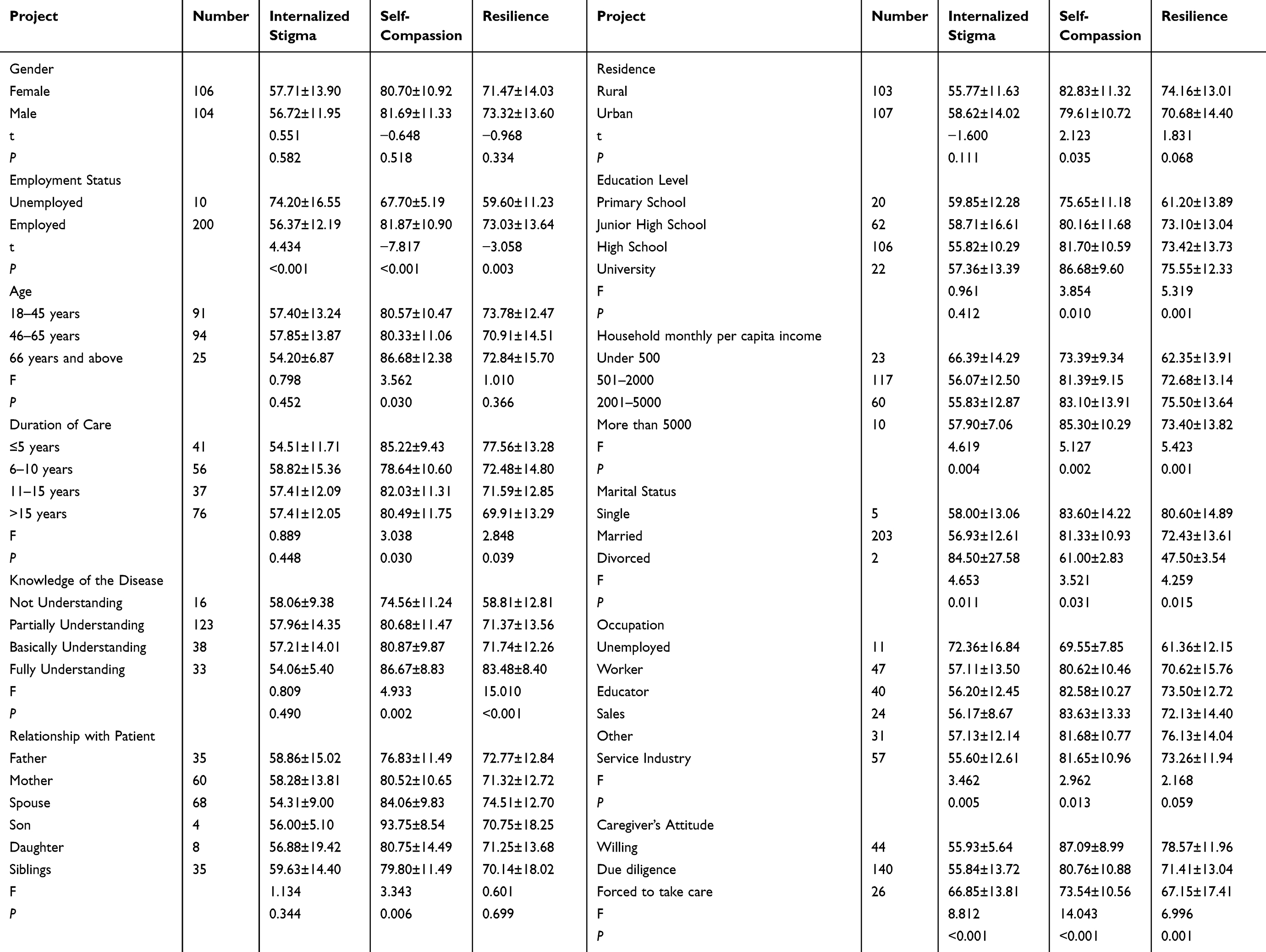 |
Table 3 Scores of Internalized Stigma, Self-Compassion and Resilience in Caregiver With Schizophrenia |
Table 4 Displays the means, standard deviations, and intercorrelations between the study variables. Correlation analyses found that patients’ and caregivers’ Internalized stigma (r=0.202, P<0.01), self-compassion (r=0.548, P<0.01) and Resilience (r=0.500, P<0.01) were significantly related, indicating non-independence in the patient-caregiver dyads. Patients’ resilience was significantly associated with stigma and self-compassion as well as stigma and self-compassion for caregivers. Caregivers’resilience was significantly associated with stigma and self-compassion. Paired samples t-tests indicated no significant differences in self-compassion within patient-caregiver dyads. Moreover, patients (48.20±13.97) had lower resilience than that of their caregivers (72.39±13.82).
 |
Table 4 Inter-Correlations, Means, and SDs of the Study Variables for Patient-Caregiver Dyads (N = 210 Dyads) |
The APIMeM is displayed in Figure 1. The final APIMeM model examining dyadic effects of internalized stigma, self-compassion on resilience produced excellent model fit (χ2/df=1.847, RMSEA=0.064, CFI=0.984, TLI=0.942, NFI=0.968). The results of direct effects and indirect effects of internalized stigma on resilience are displayed in Table 5.
 |
Table 5 Standardized Total Effects, Indirect Effects, and Direct Effects of Patients’ and Caregivers’ Internalized Stigma on Resilience via Self-Compassion in the APIMeM |
 |
Figure 1 APIMeM results of Patient Internalized stigma, Self-compassion on Resilience. Note: APIMeM: Actor-partner interdependence mediation model. Values are unstandardized coefficients. |
Direct Effects of stIgma on Resilience
As shown in Table 5, there is a significant participant effect of Internalized stigma on resilience for patients (β=−0.301; 95% CI, −0.491 to-0.129) and caregivers (β=−0.256; 95% CI, −0.404 to −0.130), suggesting that higher levels of Internalized stigma are often associated with poorer resilience. For patients and caregivers, Internalized stigma has no significant direct partner effect on resilience.
Indirect Effects of Stigma on Resilience
The stigma of patients (β=−0.568; 95% CI, −0.696 to −0.415) and caregivers (β=−0.183; 95% CI, −0.298 to −0.028) was significantly negative for the actor effect of self-compassion, indicating that stigma negatively predicted patients’ resilience. In addition, the self-compassion of patients (β=0.476; 95% CI, 0.267–0.705) and caregivers (β=0.269; 95% CI, 0.077–0.452) directly positively predicts their own resilience. There was a significant partner effect between patients and caregivers. The higher the patient’s stigma, the lower the caregiver’s self-compassion (β=−0.380; 95% CI, −0.491 to −0.264); The greater the stigma of the caregiver, the lower the patient’s self-compassion (β=−0.214; 95% CI, −0.323 to −0.093). The higher the self-compassion of the patients, the better the resilience of the caregivers (β=0.356; 95% CI, 0.145–0.578); and the higher the self-compassion of the caregivers, the better the resilience of the patients (β=0.183; 95% CI, 0.012–0.365).
Discussion
Most of the previous studies only focused on the subject effect between stigma and resilience. This study extends this by using a dyadic approach to explore the actor and partner effects of stigma on resilience, and using APIMeM to analyze and examine whether self-compassion mediates these relationships between schizophrenia patients and caregivers during recovery. To the best of our knowledge, this is the first study to examine the effects of stigma and self-compassion on the resilience of schizophrenian-caregiver dyads during recovery.
Consistent with the findings of Tantawi SA,31 the stigma of patients with schizophrenia during recovery was significantly higher than that of their caregivers and was directly related to the patients’ resilience. Biserka Sedic et al found that patients with schizophrenia in the rehabilitation period usually show higher stigma and lower resilience,32 and this stigma and resilience will affect their rehabilitation process. The heavier the stigma, the longer the rehabilitation time.33 Therefore, we should pay attention to reducing the stigma of patients and improving their resilience, so as to provide a solid guarantee for their long-term rehabilitation.
During the rehabilitation period, patients with schizophrenia often have strong self-criticism and shame due to the illness, which leads to the decline of self-esteem. Studies have shown that self-esteem can effectively alleviate the negative effects of stigma.34 Self-compassion and self-esteem are closely related, and both represent a positive attitude to cope with complex life events.35 However, while self-esteem is often based on the achievement of personal goals, self-compassion focuses on acceptance of life discontents and is therefore more stable Self-compassion helps patients reduce stigma by making them more tolerant of their illness and by actively seeking emotional support from caregivers and society.36
The results of this study suggest that self-compassion is positively associated with resilience in patients with schizophrenia during recovery. Numerous studies have confirmed that self-compassion promotes resilience,37,38 as a regulatory mechanism between positive mental health and psychopathology,39 play a protective role in patients’ mental health. The higher the level of self-compassion in patients with schizophrenia during the rehabilitation period, the healthier the mental state and the symptoms are alleviated accordingly, thereby improving their resilience.
The stigma of patients with schizophrenia during the rehabilitation period can affect their resilience through their own self-compassion. As a positive internal psychological resource, self-compassion can help patients reduce self-critical emotions caused by stigma, enhance confidence in coping with disease challenges, face difficulties and setbacks in life more actively, and reduce social withdrawal. By improving the quality of interaction between patients and their caregivers and the public, self-compassion contributes to the construction and maintenance of social support networks. Social support is a patient’s subjective perception of external support,40 which is essential for the rehabilitation process. Studies have shown that the perceived social support of patients with schizophrenia can effectively relieve their psychological pressure, prevent them from falling into excessive negative emotions, and reduce negative emotions such as depression, so as to enhance resilience and promote mental health and rehabilitation process.
According to the interdependence theory, there is a dynamic interdependence between patients and their caregivers.41 In this relationship, the behaviors and emotions of the two affect each other, especially in the patient-caregiver situation. Patients and caregivers form a community of mutual support when coping with the challenges of the disease together.42 Patients rely on caregivers to provide physical and emotional support. Patients’ emotional fluctuations and disease progression directly affect the behavior and psychological state of caregivers, and vice versa. Therefore, in-depth research on the mechanism of this interaction is of great significance for improving the quality of care of caregivers and improving the prognosis of patients.
This study found that caregivers’ stigma directly affected their resilience. As a chronic disease, caregivers of schizophrenia need to bear long-term care responsibilities, which may lead to their alienation from family and friends and limit their ability to maintain normal social relationships. Caregivers may experience discrimination and isolation from society when interacting with others.43 At the same time, due to the capacity of the patient’s condition, caregivers may feel hopeless and helpless, leading to increased stigma, which weakens their adaptability, causes psychological pain,44 and reduces their resilience. Noriya Watanabe et al explained the mechanism of resilience from the perspective of neurophysiological dynamics,45 and believed that when individuals face stress, their brain and body adapt and adjust through the activation of the autonomic nervous system and immune system to help individuals restore balance. Stigma, as a source of psychological stress, can weaken caregivers’ resilience and reduce their ability to restore physical and mental balance through these mechanisms. Therefore, the government and relevant medical and health departments should pay attention to the mental health of caregivers and develop respite care services, such as encouraging community health institutions to provide on-site services. Professional medical staff can help caregivers to scientifically arrange rest and adjust psychological stress in the process of care, so as to reduce stigma.
The long-term and complex nature of schizophrenia not only brings stress to patients, but also has a significant impact on the lives and physical and mental health of their caregivers. The results of this study showed that the stigma of caregivers of patients with schizophrenia during the rehabilitation period was negatively correlated with self-compassion. Caregivers of patients with schizophrenia during recovery often face emotional repression, but often pretend to be strong in order to support their sick loved ones.46 If this depression is not regulated in time, it will lead to emotional exhaustion, which will affect mental health. Caregivers’ stigma mainly stems from social prejudice against schizophrenia and doubts about their own care ability. These negative emotions are easy to cause alienation, loneliness and self-blame, and reduce their self-compassion ability. Self-compassion can help caregivers to be more resilient in the face of stress and challenges, help them realize that pain is not unique to individuals, thereby enhancing the sense of connection with others and reducing loneliness. Providing self-compassion interventions for caregivers, such as Compassion-Focused Therapy (CFT) based on cognitive-behavioral therapy, can be beneficial. CFT integrates insights from affective neuroscience, social and developmental psychology, and mindfulness practices. This approach encourages caregivers to express their genuine thoughts, enhances emotional regulation, fosters self-compassion, alleviates stigma, and ultimately improves the quality of care they provide.
This study found that in the process of caring for patients with schizophrenia during recovery, the self-compassion of caregivers was significantly and positively correlated with resilience. Caring for patients with schizophrenia can cause damage to the mental health of caregivers,47 while self-compassion helps their emotional regulation and enables them to maintain a stable emotional state in the face of challenges.48 At the same time, self-compassion can improve caregivers’ understanding and acceptance of themselves, encourage them to adopt positive coping strategies, so as to effectively manage their emotions and stress, adapt to environmental changes, reduce the risk of anxiety and depression, and improve resilience.
In the process of caring for patients with schizophrenia during the rehabilitation period, caregivers’ stigma can indirectly affect their resilience through self-compassion. Stigma often leads to caregivers’ negative evaluation of themselves, and lack of self-compassion can weaken their self-understanding ability and adaptability to cope with stress, and reduce their resilience. Self-compassion can help caregivers improve their emotional regulation ability, enhance self-care, reduce negative emotions, and make them more resilient in the face of setbacks. In addition, caregivers with a higher level of self-compassion are more likely to establish an effective social support network, which can help them cope with difficulties in care and further enhance their resilience.49 The findings of this study highlight the need to enhance caregivers’ resilience by cultivating their self-compassion.
The study analysis found that the education level, age, course of disease, understanding of the disease and care time of the patients with schizophrenia and their caregivers during the rehabilitation period all had an impact on their resilience. Therefore, these factors were included as covariates in the final APIMeM model. Studies have shown that patients and caregivers with higher education levels generally have stronger cognitive and problem-solving abilities,50 and are able to flexitively employ effective coping strategies and timely regulate emotions when facing mental illness related stress and challenges, thereby enhancing resilience. On the contrary, patients with longer duration of illness or caregivers with longer duration of care may face more negative emotions.51 Long-term care may cause caregivers to neglect their own emotional and physical health, lack the necessary psychological resources and energy, and reduce their resilience. Previous studies have found that the older the patient is, the higher the resilience is.32 At the same time, the more caregivers know about the patient’s disease, especially the etiology, symptoms, and treatment options of schizophrenia, helps them to set reasonable recovery expectations, reduce anxiety, fear, and uncertainty, and thus improve their resilience.
The results of mediation analysis showed that the stigma of patients and caregivers only indirectly affected each other’s resilience through each other’s self-compassion, but did not directly affect each other’s resilience. This may be related to several potential buffering mechanisms: the first is correct medication and stable medication adherence of the patient. It has been documented that patients with schizophrenia can cope well with the disease by taking prescription drugs regularly, reduce the recurrence and poor prognosis of the disease, reduce the negative impact of stigma, and feel comfortable in normal daily activities with high psychological resilience.52 The second is the coping strategies of patients. If patients or caregivers can adopt effective coping strategies, they may take a more constructive way to deal with the stigma, rather than letting it directly weaken psychological resilience. By pursuing spiritual well-being, to create a sense of belonging that enables them to deal with difficult situations due to stigma and gives them the strength to move on.
As a positive psychological regulation mechanism, self-compassion can help reduce the negative impact of stigma and improve the resilience of both sides. The interaction between patients and caregivers is often affected by each other’s emotional state. When the patient’s stigma is heavy, it is difficult for the caregiver to understand the emotional plight of the other party and become confused, unable to provide support with a sympathetic attitude, which increases the psychological burden of the patient. However, when the stigma of caregivers is heavy, patients will feel more shame and isolation,53 which will lead to negative emotions and withdrawal behavior, and even worsen the condition. In addition, when caregivers perceive that the patient’s condition is deteriorating, they may reduce emotional support due to anxiety and worry, further affecting the patient’s resilience.
Self-compassion can improve the quality of communication between patients and caregivers. Self-compassion enables convalescent patients and caregivers of schizophrenia to better accept each other’s suffering and promote mutual understanding and emotional empathy.54 People with high levels of self-compassion often communicate in an open and non-judgmental manner. This kind of good communication helps reduce misunderstandings and conflicts, thereby improving the resilience of both parties.
Finally, self-compassion helps build a healthy social support network. As caregivers live with patients with schizophrenia during recovery, they supervise patients to take their medications on time and assist in treatment activities, and such interactions help build relationships of trust and increase the availability of social support. Social support is considered to be an important factor to improve resilience.55 It provides emotional, information and material help for caregivers, helps caregivers better regulate stress, and then provides care for patients more effectively, and improves patients’ compliance and treatment effect.
In summary, the stigma of convalescence schizophrenia patients and their caregivers can not only affect their own resilience through their own self-compassion, but also affect the resilience of the other person through their own self-compassion. This interdependent relationship emphasizes the importance of establishing a good emotional connection and understanding in the process of caring and being cared for. In the future intervention and support plans, we should focus on the stigma of both sides, learn to effectively alleviate stigma and improve resilience by cultivating self-compassion, so as to provide a solid foundation for the rehabilitation of patients with schizophrenia.
Nonetheless, it is imperative to acknowledge certain limitations to facilitate a more balanced interpretation of the findings. Firstly, this study utilized cross-sectional data, which constrained our ability to establish causal relationships between individual variables. In the future, longitudinal research design will be considered for implementation. For instance, by conducting long-term follow-up on the same patients and caregivers, we can explore how stigma, psychological resilience and self-compassion change over time, thereby increasing the depth and breadth of the data.
Secondly, reliance on self-reported data introduces a certain degree of subjectivity, which may lead to reporting bias. Future research will introduce multi-dimensional measurement tools, such as psychophysiological indicators measurement, behavioral observation, and long-term data collection and observation through smart devices, etc. At the same time, it encourages participants to report their true situations, thereby reducing potential bias and enhancing the authenticity of the data.
Third, this study was conducted in only one tertiary hospital, and the generalizability of the findings may be limited by regional culture. Future studies will expand the scope of sample collection from a single hospital or region to multiple medical centers or different regions to improve the representativeness and external validity of the research conclusions.
Fourth, this study only proposed interventions to enhance self-compassion to reduce the impact of stigma on resilience and was not specifically implemented, and given the interdependent nature of patients and caregivers, incorporating these interventions into a dyadic framework may optimize outcomes by fostering more supportive environments. Future studies should explore the efficacy and feasibility of these interventions in schizophrenia populations, considering both short-term and long-term impacts.
Conclusion
Our findings suggest that the stigma of schizophrenia patients and caregivers in recovery can affect their own resilience through their own self-compassion and also through the self-compassion of others. The stigma of patients with schizophrenia and their caregivers can directly affect their own psychological resilience. However, the stigma of patients with schizophrenia during rehabilitation does not directly affect the resilience of caregivers, and so does the resilience of caregivers.
Chinese social population has serious prejudice against patients with schizophrenia during rehabilitation. Previous interventions to improve resilience only focused on patients and ignored the partner effect of caregivers. The stigma and self-compassion of caregivers can affect the resilience of patients with schizophrenia during rehabilitation, and then affect their treatment effect and rehabilitation process. The results of this study help medical staff to understand the effects of stigma and self-compassion on resilience of patients with schizophrenia during recovery from the dyad level. Therefore, medical staff should regard patients and caregivers as inseparable units, identify the combination with severe stigma, especially the combination with poor self-compassion of caregivers, guide the two sides to support each other and cooperate, enhance individual adaptability, and take targeted measures to reduce stigma. To develop interventions focused on self-compassion to improve dyadic resilience of people with schizophrenia and their caregivers during recovery.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Millier A, Schmidt U, Angermeyer MC. et al. Humanistic burden in schizophrenia: a literature review. J Psychiatr Res. 2014;54:85–93. doi:10.1016/j.jpsychires.2014.03.021
2. Berenbaum H. Classification and psychopathology research. J Abnorm Psychol. 2013;122(3):894–901. doi:10.1037/a0033096
3. Thai ML, Andreassen AK, Bliksted V. A meta-analysis of executive dysfunction in patients with schizophrenia: different degree of impairment in the ecological subdomains of the Behavioural Assessment of the Dysexecutive Syndrome. Psychiatry Res. 2019;272:230–236. doi:10.1016/j.psychres.2018.12.088
4. Rutter M. Implications of resilience concepts for scientific understanding. Ann N Y Acad Sci. 2006;1094:1–12. doi:10.1196/annals.1376.002
5. Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392(10157):1553–1598. doi:10.1016/S0140-6736(18)31612-X
6. Crowe A, Averett P, Glass JS. Mental illness stigma, psychological resilience, and help seeking: what are the relationships? Mental Health Prev. 2016;4(2):63–68. doi:10.1016/j.mhp.2015.12.001
7. Wambua GN, Kilian S, Ntlantsana V, Chiliza B. The association between resilience and psychosocial functioning in schizophrenia: a systematic review and meta-analysis. Psychiatry Res. 2020;293:113374. doi:10.1016/j.psychres.2020.113374
8. Hansen DA. INTERPERSONAL-RELATIONS - A THEORY OF INTERDEPENDENCE - KELLEY,HH, THIBAUT,JW. J Marriage Family. 1982;44(1):246–248. doi:10.2307/351281
9. Bishop M, Greeff AP. Resilience in families in which a member has been diagnosed with schizophrenia. J Psychiatric Mental Health Nursing. 2015;22(7):463–471. doi:10.1111/jpm.12230
10. Rossi A, Galderisi S, Rocca P, et al. Personal resources and depression in schizophrenia: the role of self-esteem, resilience and internalized stigma. Psychiatry Res. 2017;256:359–364. doi:10.1016/j.psychres.2017.06.079
11. Lien YJ, Chang HA, Kao YC, Tzeng NS, Lu CW, Loh CH. Insight, self-stigma and psychosocial outcomes in Schizophrenia: a structural equation modelling approach. Epidemiol Psychiatr Sci. 2018;27(2):176–185. doi:10.1017/s2045796016000950
12. Scambler G. Stigma and disease: changing paradigms. Lancet. 1998;352(9133):1054–1055. doi:10.1016/s0140-6736(98)08068-4
13. Phelan JC, Bromet EJ, Link BG. Psychiatric illness and family stigma. Schizophrenia Bulletin. 1998;24(1):115–126. doi:10.1093/oxfordjournals.schbul.a033304
14. Corrigan PW, Watson AC, Barr L. The self-stigma of mental illness: implications for self-esteem and self-efficacy. J Social Clinical Psychol. 2006;25(8):875–884. doi:10.1521/jscp.2006.25.8.875
15. Ran MS, Chui CHK, Wong IYL, et al. Family caregivers and outcome of people with schizophrenia in rural China: 14-year follow-up study. Social Psychiatry Psychiatric Epidemiol. 2016;51(4):513–520. doi:10.1007/s00127-015-1169-0
16. Corrigan PW, Miller FE. Shame, blame, and contamination: a review of the impact of mental illness stigma on family members. J Ment Health. 2004;13(6):537–548. doi:10.1080/09638230400017004
17. Ran MS, Hall BJ, Su TT, et al. Stigma of mental illness and cultural factors in Pacific Rim region: a systematic review. BMC Psychiatry. 2021;21(1):8. doi:10.1186/s12888-020-02991-5
18. Haraguchi K, Maeda M, Mei YX, Uchimura N. Stigma associated with schizophrenia: cultural comparison of social distance in Japan and China. Psych Clin Neurosci. 2009;63(2):153–160. doi:10.1111/j.1440-1819.2009.01922.x
19. Ng CH. The stigma of mental illness in Asian cultures. Aust N Z J Psychiatry. 1997;31(3):382–390. doi:10.3109/00048679709073848
20. Neff K. Self-Compassion: an Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self and Identity. 2003;2(2):85–101. doi:10.1080/15298860309032
21. Neff KD. Self-Compassion: theory, Method, Research, and Intervention. Annual Review of Psychology. 2023;74:193–218. doi:10.1146/annurev-psych-032420-031047
22. Gutíerrez-Hernández ME, Fanjul LF, Díaz-Megolla A, et al. COVID-19 Lockdown and Mental Health in a Sample Population in Spain: the Role of Self-Compassion. Int J Environ Res Public Health. 2021;18(4):2103. doi:10.3390/ijerph18042103
23. MacBeth A, Gumley A. Exploring compassion: a meta-analysis of the association between self-compassion and psychopathology. Clinic Psychol Rev. 2012;32(6):545–552. doi:10.1016/j.cpr.2012.06.003
24. Heath P, Brenner R, Lannin D, Vogel D. Self-Compassion Moderates the Relationship of Perceived Public and Anticipated Self-Stigma of Seeking Help. Stigma and Health. 2016;3(1):65–68. doi:10.1037/sah0000072
25. Pérez-Aranda A, García-Campayo J, Gude F, et al. Impact of mindfulness and self-compassion on anxiety and depression: the mediating role of resilience. Int J Clin Health Psychol. 2021;21(2):100229. doi:10.1016/j.ijchp.2021.100229
26. Neff KD, Faso DJ. Self-Compassion and Well-Being in Parents of Children with Autism. Mindfulness. 2015;6(4):938–947. doi:10.1007/s12671-014-0359-2
27. Tan EY, Yip VT, Rolles-Abraham KL. Benefit-finding and self-compassion promote psychological well-being in caregivers of individuals with mental illness: a cross-sectional study. medRxiv. 2021;2021:2021–2027. doi:10.1101/2021.07.14.21260546
28. Mackali Z, Çetinkaya S, Ay N. The mediating role of self-compassion in the relationship between internalized stigma and psychological resilience in bipolar disorder. Psychol Psychother. 2023;96(4):952–966. doi:10.1111/papt.12488
29. Ritsher JB, Phelan JC. Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Res. 2004;129(3):257–265. doi:10.1016/j.psychres.2004.08.003
30. Neff KD. The Development and Validation of a Scale to Measure Self-Compassion. Self and Identity. 2003;2(3):223–250. doi:10.1080/15298860390209035
31. Tantawi SA, Kamaleddine AN, Alhajj LA, et al. Social Stigma Toward Individuals with Schizophrenia in a Lebanese Population. Neuropsychiatr Dis Treat. 2024;20:561–570. doi:10.2147/ndt.S450385
32. Sedić B, Štrkalj Ivezić S, Petrak O, Ilić B. Differences in Resilience, Self-Stigma and Mental Health Recovery between Patients with Schizophrenia and Depression. Psychiatry Danub. 2021;33(Suppl 4):518–528.
33. Hsu LKG, Wan YM, Chang H, Summergrad P, Tsang BYP, Chen HT. Stigma of Depression Is More Severe in Chinese Americans than Caucasian Americans. Psychiatry. 2008;71(3):210–218. doi:10.1521/psyc.2008.71.3.210
34. Degnan A, Berry K, Humphrey C, Bucci S. The relationship between stigma and subjective quality of life in psychosis: a systematic review and meta-analysis. Clinic Psychol Rev. 2021;85. doi:10.1016/j.cpr.2021.102003.
35. Neff KD, Vonk R. Self-Compassion Versus Global Self-Esteem: two Different Ways of Relating to Oneself. J Personality. 2009;77(1):23–50. doi:10.1111/j.1467-6494.2008.00537.x
36. Lavi-Rotenberg A, Frishman N, Igra L, Gilboa-Schechtman E, Hasson-Ohayon I. Beyond One’s Attitude Toward the Self. J Nerv Ment Dis. 2024;212(1):28–32. doi:10.1097/nmd.0000000000001724
37. Neff KD, McGehee P. Self-compassion and Psychological Resilience Among Adolescents and Young Adults. Self and Identity. 2010;9(3):225–240. doi:10.1080/15298860902979307
38. Joy GV, Alomari AMA, Singh K, et al. Nurses’ self-esteem, self-compassion and psychological resilience during COVID-19 pandemic. Nursing Open. 2023;10(7):4404–4412. doi:10.1002/nop2.1682
39. Trompetter HR, de Kleine E, Bohlmeijer ET. Why Does Positive Mental Health Buffer Against Psychopathology? An Exploratory Study on Self-Compassion as a Resilience Mechanism and Adaptive Emotion Regulation Strategy. Cognit Ther Res. 2017;41(3):459–468. doi:10.1007/s10608-016-9774-0. [published Online First: 20160409].
40. Wang LY, Li MZ, Jiang XJ, et al. Mediating Effect of Self-Efficacy on the Relationship Between Perceived Social Support and Resilience in Patients with Recurrent Schizophrenia in China. Neuropsychiatr Dis Treat. 2022;18:1299–1308. doi:10.2147/ndt.S368695
41. Streck BP, Wardell DW, LoBiondo-Wood G, Beauchamp JES. Interdependence of physical and psychological morbidity among patients with cancer and family caregivers: review of the literature. Psycho-Oncology. 2020;29(6):974–989. doi:10.1002/pon.5382
42. Stusiński J, Merk W, Lew-Starowicz M. Dyadic relationships of people with schizophrenia. Związki diadyczne osób chorujących na schizofrenię. Psychiatr Pol. 2022;56(4):861–876. doi:10.12740/PP/138743
43. Ergetie T, Yohanes Z, Asrat B, Demeke W, Abate A, Tareke M. Perceived stigma among non-professional caregivers of people with severe mental illness, Bahir Dar, northwest Ethiopia. Ann General Psychiatry. 2018;17(1). doi:10.1186/s12991-018-0212-4
44. Krupchanka D, Kruk N, Murray J, et al. Experience of stigma in private life of relatives of people diagnosed with schizophrenia in the Republic of Belarus. Social Psychiatry Psychiatric Epidemiol. 2016;51(5):757–765. doi:10.1007/s00127-016-1190-y
45. Watanabe N, Takeda M. Neurophysiological dynamics for psychological resilience: a view from the temporal axis. Neurosci Res. 2022;175:53–61. doi:10.1016/j.neures.2021.11.004
46. Hou RJ, Wong SY, Yip BH, et al. The effects of mindfulness-based stress reduction program on the mental health of family caregivers: a randomized controlled trial. Psychother Psychosom. 2014;83(1):45–53. doi:10.1159/000353278. [published Online First: 20131119].
47. Martinez A, Baumgartner JN, Kaaya S, et al. Hopefulness among individuals living with schizophrenia and their caregivers in Tanzania: an actor-partner interdependence model. Bmc Psychiatry. 2023;23(1). doi:10.1186/s12888-023-04990-8
48. Zhang ZJ, HHM L, Ng SM, et al. The Effects of a Mindfulness-Based Family Psychoeducation Intervention for the Caregivers of Young Adults with First-Episode Psychosis: a Randomized Controlled Trial. Int J Environ Res Public Health. 2023;20(2). doi:10.3390/ijerph20021018
49. Sin J, Gillard S, Spain D, Cornelius V, Chen T, Henderson C. Effectiveness of psychoeducational interventions for family carers of people with psychosis: a systematic review and meta-analysis. Clinic Psychol Rev. 2017;56:13–24. doi:10.1016/j.cpr.2017.05.002
50. Lök N, Bademli K. The Relationship Between the Perceived Social Support and Psychological Resilience in Caregivers of Patients with Schizophrenia. Community Mental Health J. 2021;57(2):387–391. doi:10.1007/s10597-020-00665-w
51. Velelekou A. Factors influencing the duration of hospitalization of patients with schizophrenia. Med Pharm Rep. 2022;95(3):290–299. doi:10.15386/mpr-2144
52. Commey IT, Ninnoni JPK, Ampofo EA. Coping with personal care and stigma: experiences of persons living with schizophrenia. BMC Nurs. 2022;21(1):107. doi:10.1186/s12912-022-00891-5
53. Shi Y, Shao YP, Li HH, et al. Correlates of affiliate stigma among family caregivers of people with mental illness: a systematic review and meta-analysis. J Psychiatric Mental Health Nursing. 2019;26(1–2):49–61. doi:10.1111/jpm.12505
54. Murfield J, Moyle W, Jones C, O’Donovan A. Self-Compassion, Health Outcomes, and Family Carers of Older Adults: an Integrative Review. Clinical Gerontologist. 2020;43(5):485–498. doi:10.1080/07317115.2018.1560383
55. Chen XY, Mao YX, Kong LH, et al. Resilience moderates the association between stigma and psychological distress among family caregivers of patients with schizophrenia. Pers Individ Dif. 2016;96:78–82. doi:10.1016/j.paid.2016.02.062
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.