")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Dynamic Changes in ALFF and DC in Subthreshold Depression Before and After ICBT Intervention
Authors Wang Y , Ying Y, Zhu Z, Wang L, Yang Y, Zhang L, Yu W, Liang Y, Zhang H, Ji Y, Pan Y
Received 29 January 2025
Accepted for publication 2 June 2025
Published 7 June 2025 Volume 2025:21 Pages 1161—1172
DOI https://doi.org/10.2147/NDT.S518526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rakesh Kumar
Yu Wang,1,* Yuchen Ying,2,* Zili Zhu,1 Li Wang,2 YiLing Yang,2 Li Zhang,2 Wenquan Yu,1 Yichuan Liang,1 Hui Zhang,1 Yunxin Ji,3 Yuning Pan1
1Department of Radiology, THE First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China; 2Department of Elderly Health Care and Management, Ningbo College of Health Sciences, Ningbo, Zhejiang, 315000, People’s Republic of China; 3Department of Psychosomatic Medicine, The First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuning Pan, Email [email protected] Yunxin Ji, Email [email protected]
Purpose: Subthreshold depression (SD) is a highly prevalent mental health condition and a key precursor in major depressive disorder. Internet-based cognitive behavioral therapy (ICBT) effectively treats SD in clinical settings, but the neuromechanisms behind its success are not fully understood. This study aimed to examine changes in intrinsic brain activity in SD and their further alterations after ICBT intervention.
Patients and Methods: Twenty-five individuals with SD and 25 matched healthy controls (HC) were enrolled. SD underwent the same MRI scans and clinical assessments before and after a five-week ICBT intervention. HC underwent a single MRI scan during enrollment. The amplitude of low-frequency fluctuation (ALFF) and degree centrality (DC) are established analytical techniques in the field of neuroimaging to assess intrinsic brain activity. Two-sample and paired-sample t-tests were employed to examine changes in whole-brain ALFF and DC. Pearson or Spearman correlation analysis was performed to evaluate associations between altered ALFF/DC values and changes in clinical assessment scores in SD.
Results: Compared with HC, decreased DC in the right precuneus (PCUN) and increased ALFF in the right insula (INS) were found in SD before ICBT intervention. After ICBT intervention, ALFF in the left hippocampus (HIP) was increased, and DC in the right medial and paracingulate gyri (DCG) was reduced in SD. Altered ALFF values in the left HIP showed a negative correlation with changes in PHQ-9 scores, and a positive correlation with changes in FATS-ReB scores. Altered DC values in the right DCG were positively correlated with changes in CCTS-TR-BhA scores.
Conclusion: These findings provide new insights into the altered intrinsic brain activities in SD. More importantly, this study found potential changes in intrinsic activity in brain regions associated with ICBT response to SD, which may help further explore the neuropsychological mechanism underlying the efficacy of ICBT in the future.
Keywords: subthreshold depression, internet-based cognitive behavioral therapy, resting-state functional magnetic resonance imaging, amplitude of low-frequency fluctuation, degree centrality
Introduction
Subthreshold depression (SD) is a highly prevalent mental health condition that is considered a significant precursor to and a risk factor for major depressive disorder (MDD).1 While the definition of SD is often considered overly inclusive, several representative studies identify a Center for Epidemiologic Studies Depression Scale (CES-D) score of ≥16 as the meeting criteria for SD.2,3 Core symptoms of SD typically include low mood, anhedonia, sleep disturbances, and decreased energy levels. These symptoms may have a profound impact on subjective well-being, quality of life, and social-psychological functioning.1 The prevalence of SD exceeds that of MDD,4 with a common occurrence among adolescents and emerging adulthood.5,6 SD poses a significant burden on public mental health services, leading to substantial healthcare costs.7 Implementing effective interventions can mitigate the symptoms of SD and potentially impede its evolution into MDD.
Currently, the predominant interventions for SD involve psychological therapies combined with medication. Cognitive behavioral therapy (CBT), a form of offline psychological treatment, has been demonstrated to effectively reduce depressive symptoms in SD and mitigate the risk of MDD.8 CBT skills include attention bias modification (ABM),9 increased cognitive load,10 and behavioral activation (BhA).11 However, individuals with SD frequently avoided seeking professional help and participating in traditional face-to-face psychological interventions due to the perception of mild symptoms, the stigma surrounding the disorder, and the financial burden, resulting in a low rate of consultation within this demographic.12
This limitation has been overcome by online psychological treatments, which present several benefits, including increased accessibility, flexibility in scheduling, reduced reliance on in-person clinical psychologists, enhanced privacy protections, and lower costs.13 At present, internet-based cognitive behavioral therapy (ICBT) is a widespread and highly effective modality. A previous meta-analysis showed that official organizations in numerous countries acknowledged ICBT as a viable alternative to traditional CBT for treating MDD.14 Additionally, a prior randomized controlled trial conducted by our research team demonstrated the efficacy of ICBT in reducing depressive symptoms in SD.15
Magnetic resonance imaging (MRI) studies have identified disruptions in the local synchrony of neural activity and regulatory processes in brain regions linked to the default mode network (DMN) in SD, notably in the medial prefrontal cortex, anterior cingulate cortex (ACC), and hippocampus (HIP).16,17 Several studies have explored the neuroimaging mechanisms underlying the effectiveness of CBT skills in treating SD. After CBT intervention, a reduction in functional connectivity (FC) between the anterior DMN subnetwork and the dorsal ACC was observed in SD.18 Previous research also indicated that BhA enhanced diminished activity in the left lateral prefrontal cortex and angular gyrus of SD.19 Li et al found that ABM training may lead to altered spontaneous brain activity in the right anterior insula (INS) and middle frontal gyrus in young women with SD.9
ICBT and CBT share the same theoretical foundation, while their differences in intervention format and therapist involvement may lead to divergent therapeutic effects and potential neural changes. The studies on ICBT for social anxiety disorder demonstrated that a reduction in left amygdala reactivity following intervention,20 and the BOLD response patterns of the dorsal ACC-amygdala regions was a significant predictor of the long-term efficacy of ICBT.21 A study indicated that a larger volume of the right rostral ACC prior to ICBT intervention significantly predicted greater improvement in depressive symptoms.22 Additionally, another investigation into ICBT for depression revealed that reduced FC between the right anterior insula and the temporoparietal junction, along with increased FC between the right anterior insula and left anterior insula, were associated with improvements in depression.23 The aforementioned studies found alterations in brain function and structure associated with the treatment of anxiety and depression through ICBT. Nevertheless, there is a paucity of neuroimaging research investigating changes in brain activity in SD following ICBT intervention.
The amplitude of low-frequency fluctuation (ALFF) and degree centrality (DC) are established analytical techniques utilizing brain blood oxygen level-dependent (BOLD) signals obtained during resting-state functional MRI (rs-fMRI). ALFF quantifies the intensity of brain signal fluctuations within the low-frequency range of 0.01–0.08 hz, providing a comprehensive assessment of spontaneous brain activity.24 DC assesses the degree to which a node within a network is interconnected with other nodes, reflecting the intrinsic connectivity of a specific brain region within the larger network of the brain.25 Both methods have been used simultaneously to investigate a range of mental disorders, such as MDD26 and schizophrenia,27 to examine alterations in brain activity.
Therefore, the present study endeavored to examine changes in whole-brain ALFF and DC in SD. In addition, alterations in ALFF and DC in specific brain regions in SD before and after ICBT intervention were investigated. Finally, the relationships between the altered ALFF and DC and psychiatric symptoms, as well as the acquisition and utilization frequency of CBT skills, were also assessed. It was hypothesized that SD exhibit significant differences in brain regions compared with healthy controls (HC), and SD demonstrate altered intrinsic spontaneous brain activities following ICBT intervention. Furthermore, we posited that the brain regions affected by the ICBT intervention are associated with psychiatric symptoms and CBT skills.
Materials and Methods
Participants
Individuals aged 18–23 who were enrolled in college or undergraduate programs in Ningbo City, Zhejiang Province, were recruited between December 2021 and June 2023. The exclusion criteria were as follows: (1) suicidal ideation (with a score for question 9 on the Patient Health Questionnaire-9 (PHQ-9) of >2); (2) a history of neurological or psychiatric disorders; (3) evidence of structural brain abnormalities such as trauma, tumors, or infections; (4) drug or alcohol abuse; and (5) any contraindications for undergoing an MRI scan. The included participants were categorized into two distinct groups based on their total CES-D scores: individuals with a CES-D score of 16 or higher were designated as the SD group, while those with a CES-D score below 16 were assigned to the HC group.
The SD group underwent two MRI scans and two clinical assessments, with the first MRI scan and clinical assessment conducted at the time of recruitment, followed by a five-week ICBT intervention. The second MRI scan and clinical assessment were conducted immediately after the completion of intervention. The HC group only underwent one MRI scan and clinical assessment after enrollment. The SD group comprised solely of patients newly diagnosed with SD. Participants did not receive any psychotherapeutic treatments other than ICBT intervention. After the completion of the study, participants can receive individualized treatment regimens tailored to their specific conditions and medical recommendations.
Two measures were implemented as follows to facilitate participant compliance. (1) The ICBT was developed as a WeChat mini-program tailored specifically for the Chinese population, enhancing its accessibility and convenience for students. Additionally, the research team monitored the completion of participants’ treatment through the program’s backend system and reminded participants to complete treatment tasks on time. (2) The research team was available to address any questions from participants throughout the study. Therapists can comprehensively assess participants’ compliance based on their feedback and platform data.
This study was approved by the Medical Ethics Committee of Ningbo University (NBU-2020-139). All participants were given comprehensive information about the experimental protocols and potential risks, and willingly signed informed consent forms. This study complies with the Declaration of Helsinki. This protocol was retrospectively registered at the Chinese Clinical Trial Register (ChiCTR) on February 22, 2022, with Identifier: ChiCTR2200056884.
ICBT Intervention
Our research team cooperated with a third-party company to develop ICBT software and create a WeChat Mini-Program. This project was based on the Chinese version of the Handbook of Cognitive-Behavioral Therapies,28 including five lessons and corresponding case stories to teach practical skills of CBT. The lesson content encompassed text, images, and videos, with homework assignments provided after the completion of each session. Each lesson lasted about 30 minutes. ICBT lesson content specifications are detailed in our previous study.15 Participants were required to complete five lessons (Lesson 1–5) in order within five weeks following the same treatment schedule. The case stories corresponding to the lessons were drawn from real cases of Chinese patients who had received CBT and recovered from anxiety and depression.
Clinical Measurements
Depressive symptoms were assessed utilizing the Chinese versions of the CES-D and PHQ-9 scales,29,30 and anxiety symptoms were evaluated through the Chinese version of the Generalized Anxiety Disorder-7 (GAD-7) scale.31 These clinical measurement instruments exhibited strong reliability and validity within the Chinese population.
Participants’ acquisition and utilization frequency of CBT skills were assessed using the Competencies of Cognitive Therapy Scale-Therapist Report (CCTS-TR) and the Frequency of Actions and Thoughts Scale (FATS) scales.32,33 The CCTS-TR scale encompasses automatic thoughts (AuT), BhA, and core beliefs (CoB). The FATS scale consists of cognitive restructuring (CoR), social interactions (SoI), rewarding behaviors (ReB), and activity scheduling (AcS). CCTS-TR is a measure administered by raters, where trained CBT therapists evaluate participants’ proficiency in CBT techniques while remaining unaware of other research-related details.
The SD group underwent the same contents of clinical assessments before and after ICBT intervention, to evaluate changes in anxiety and depression levels, as well as the acquisition and frequency of utilization of CBT skills.
MRI Data Acquisition
All MRI data were acquired using a 3T MRI scanner (MAGNETOM Vida, Siemens, USA) equipped with a 64-channel phased-array head coil. Participants were instructed to remain awake, maintain physical stillness, and refrain from engaging in cognitive activities during the scanning procedure, with earplugs provided to mitigate the scanner noise. Participants underwent standard cranial MRI scans, including T1-weighted, T2-weighted, T2-fluid-attenuated inversion recovery (FLAIR), and diffusion-weighted imaging sequences, which were reviewed by a proficient radiologist to rule out any brain structural abnormality. rs-fMR data were acquired using gradient echo planar imaging (GRE-EPI) sequences with the following scan parameters: slice number = 54, field of view (FOV) = 216×216 mm², repetition time (TR) = 2000 ms, echo time (TE) = 30 ms, flip angle (FA) = 90°, matrix size = 72 × 72, slice thickness = 3 mm, voxel size = 3 × 3×3 mm³, and no gap.
MRI Data Preprocessing
On the Matlab R2018b platform, rs-fMRI data were preprocessed using Data Processing Assistant for Resting-State fMRI Advanced (DPARSFA version 5.4, http://rfmri.org/DPARSF) and Statistical Parametric Mapping (SPM version 12, http://www.fil.ion.ucl.ac.uk/spm). The first 10 time points of the images were excluded to accommodate the stabilization of the gradient magnetic field and the participant’s acclimation to scanning noise. Afterward, the remaining 190 images were subjected to slice timing and head motion correction. Participants who met the criteria of maximum translational movement ≤3 mm and rotational angles ≤3° were included. Subsequently, functional images were registered with T1 structural images, subjected to spatial normalization to the Montreal Neurological Institute (MNI) space, and resampled to a voxel resolution of 3 × 3×3 mm³. Finally, nuisance covariates such as white matter signal and cerebrospinal fluid signal were regressed out and linear trends were performed.
Calculation of ALFF and DC
Preprocessed functional images were imported into the DPARSFA software to calculate ALFF and DC. The procedure for computing ALFF was as follows.24 First, a fast Fourier transform was applied to convert the pulse signal from the time domain to the frequency domain, resulting in a power spectrum. Then, the square root was computed at each frequency within the power spectrum. Finally, an average of the square roots which were obtained within the 0.01–0.08 hz range for each voxel was analyzed as ALFF. DC was calculated by summing up the weights of all correlations that exceeded a predefined optimized threshold for a given voxel. The Pearson correlation coefficient was computed between the BOLD time series of every pair of voxels in the brain, with an r threshold set at 0.25.25 Additionally, ALFF and DC data were spatially smoothed with a Gaussian kernel of 4 × 4×4 mm3 full-width at half-maximum.
Statistical Analysis
Statistical analyses of functional images were performed with SPM12. Two-sample t-tests were applied to compare the whole-brain differences in ALFF and DC between HC and SD before ICBT intervention, with age, gender, and mean head motion parameters as nuisance covariates. Paired-sample t-tests were used to determine the whole-brain differences in ALFF and DC in SD before and after ICBT intervention, with the above parameters as nuisance covariates. The Gaussian Random Field (GRF) correction was conducted with the statistical threshold set at two-tailed voxel-level p < 0.01 and cluster-level p < 0.05.34 Brain regions showing significant differences were defined as regions of interest, from which ALFF and DC values were extracted.
A Shapiro–Wilk test was performed to assess the normality of demographic data. A two-sample t-test was applied to compare normally distributed data, with the choice of statistical results depending on the evaluation of homogeneity of variance. Meanwhile, non-normally distributed data were compared using a Mann–Whitney U-test. Gender differences were analyzed using a chi-square test. In addition, a Shapiro–Wilk test was used to check the normality of the altered scores between the two clinical measurements. A paired t-test was employed for normally distributed altered scores to assess the differences in clinical measurements before and after the intervention, whereas a Wilcoxon signed-rank test was utilized for non-normally distributed altered scores. In the SD group, Pearson or Spearman correlation analysis was applied to evaluate the association between the altered ALFF and DC values in significantly different brain regions and the changes in clinical measurement scales (SD after ICBT intervention minus SD before ICBT intervention).
Statistical analyses were conducted utilizing SPSS, version 25.0 (IBM SPSS Statistics for Windows, Armonk, New York, USA) and R software, version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria), with a significance level of p < 0.05.
Results
Participants
Twenty-seven individuals with SD and 25 hC were recruited. In the SD group, one participant did not complete the ICBT intervention and follow-up MRI examination, while another exhibited significant artifacts in the MRI images before ICBT intervention. Finally, these two participants were excluded from the analysis due to the absence of essential MRI data. All participants in the HC group completed the MRI scans. Finally, a total of 25 individuals with SD who completed the entire process and 25 matched HC were included in the analysis. The mean age of the SD and HC groups was 235.20 months and 244.28 months respectively. All participants were right-handed. No statistically significant differences were found between the two groups in terms of age, gender, weight, height, and body mass index (BMI) (p > 0.05). The baseline demographic information of participants is detailed in Table 1. A flowchart is presented in Figure 1.
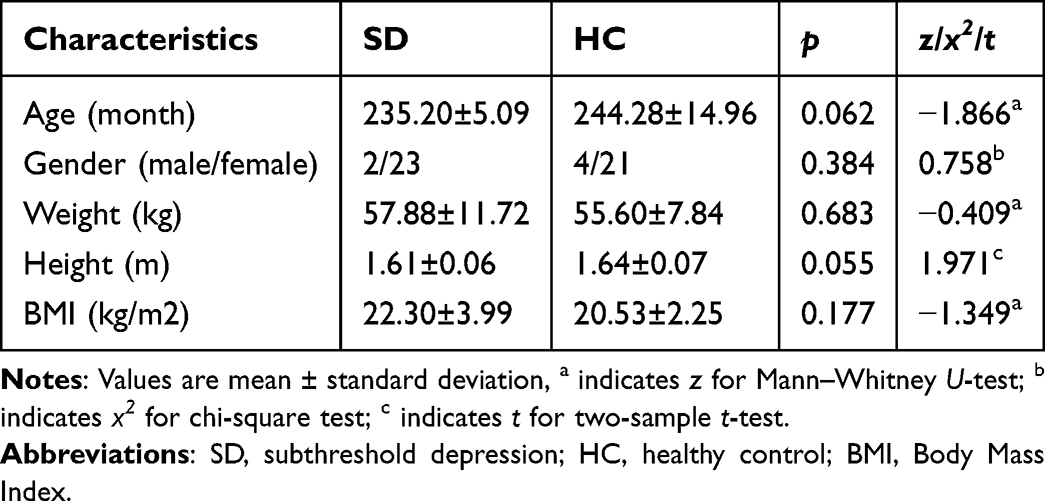 |
Table 1 Demographic Information of Participants |
 |
Figure 1 Study flowchart. Support was provided by Figdraw. Abbreviations: CES-D, Center for Epidemiologic Studies Depression; HC, healthy control; SD, subthreshold depression; MRI, magnetic resonance imaging; rs-fMRI, resting-state functional MRI; ICBT, internet-based cognitive behavioral therapy. |
Changes in Clinical Measurements
The SD group showed a significant decrease in CES-D, PHQ-9, and GAD-7 scores, and a significant increase in FATS-CoR/SoI/ReB and CCTS-TR-AuT/BhA/CoB scores after ICBT intervention (p < 0.05). However, no significant difference was found in FATS-AcS scores in the SD group before and after ICBT intervention (p > 0.05). Further details on the changes in clinical measurements in the SD group before and after ICBT intervention are provided in Table 2.
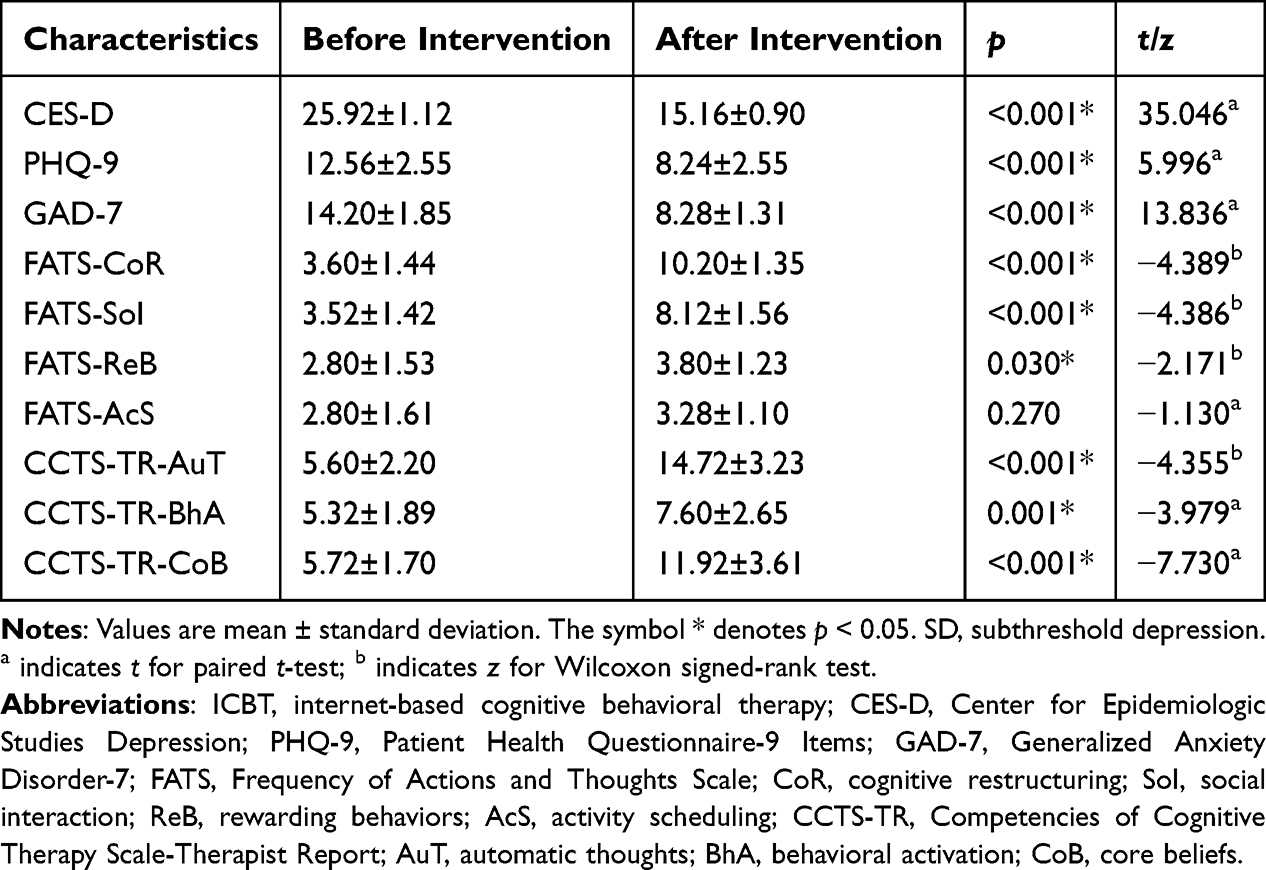 |
Table 2 Changes in Clinical Measurements in the SD Group Before and After ICBT Intervention |
Altered ALFF and DC
Compared to HC, increased ALFF in the right INS and decreased DC in the right precuneus (PCUN) were found in SD before ICBT intervention (corrected p < 0.05, Table 3 and Figure 2). After ICBT intervention, ALFF in the left HIP was increased, and DC in the right medial and paracingulate gyri (DCG) was reduced in SD (corrected p < 0.05, Table 4 and Figures 3A and 4A).
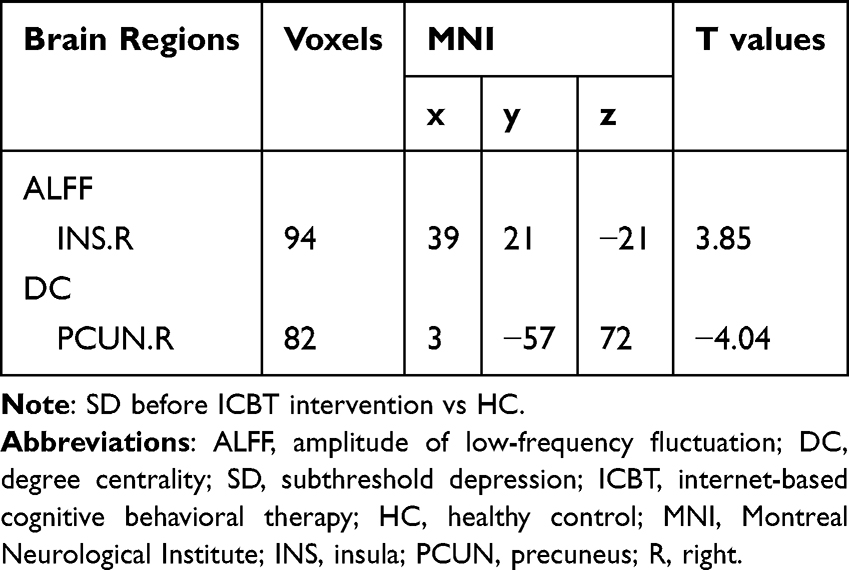 |
Table 3 Brain Regions Showing Significant Differences in ALFF/DC Between SD Before ICBT Intervention and HC |
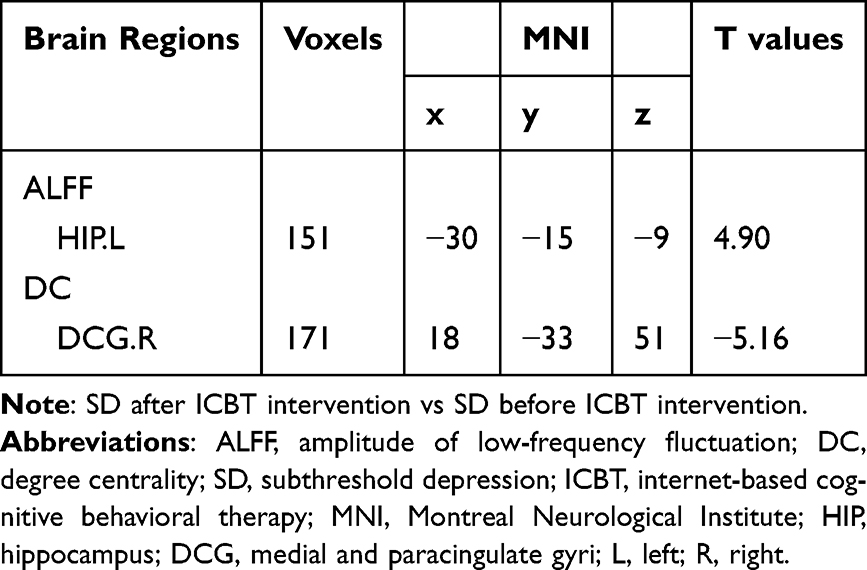 |
Table 4 Brain Regions Showing Significant Differences in ALFF/DC in SD Before and After ICBT Intervention |
 |
Figure 2 Comparison of ALFF and DC between SD before ICBT intervention and HC. Compared with HC, increased ALFF in the right INS and decreased DC in the right PCUN were found in SD before ICBT intervention (two-tailed voxel-level p < 0.01 and cluster-level p < 0.05, GRF correction). Abbreviations: ALFF, amplitude of low-frequency fluctuation; DC, degree centrality; SD, subthreshold depression; ICBT, internet-based cognitive behavioral therapy; HC, healthy control; INS, insula; PCUN, precuneus; GRF, Gaussian Random Field. |
 |
Figure 3 (A) Comparison of ALFF in SD before and after ICBT intervention. Increased ALFF in the left Hip was found in SD after ICBT intervention (two-tailed voxel-level p < 0.01 and cluster-level p < 0.05, GRF correction). (B) Correlations among the altered ALFF values and clinical measurement scores. Altered ALFF values in the left HIP were negatively correlated with changes in PHQ-9 scores, and positively correlated with changes in FATS-ReB scores. Abbreviations: ALFF, amplitude of low-frequency fluctuation; SD, subthreshold depression; ICBT, internet-based cognitive behavioral therapy; HIP, hippocampus; GRF, Gaussian Random Field; PHQ-9, Patient Health Questionnaire-9 Items; FATS, Frequency of Actions and Thoughts Scale; ReB, rewarding behaviors. |
 |
Figure 4 (A) Comparison of DC in SD before and after ICBT intervention. Decreased DC in the right DCG was found in SD after ICBT intervention (two-tailed voxel-level p < 0.01 and cluster-level p < 0.05, GRF correction). (B) Correlations among the altered DC values and clinical measurement scores. Altered DC values in the right DCG were positively correlated with changes in CCTS-TR-BhA scores. Abbreviations: DC, degree centrality; SD, subthreshold depression; ICBT, internet-based cognitive behavioral therapy; DCG, medial and paracingulate gyri; GRF, Gaussian Random Field; CCTS-TR, Competencies of Cognitive Therapy Scale-Therapist Report; BhA, behavioral activation. |
Correlations Between Altered ALFF/DC and Clinical Measurement Scores
Altered ALFF values in the left HIP showed a significant negative correlation with changes in PHQ-9 scores (r = −0.442, p = 0.027), and a significant positive correlation with changes in FATS-ReB scores (r = 0.448, p = 0.025) (Figure 3B). Altered DC values in the right DCG were positively correlated with changes in CCTS-TR-BhA scores (r = 0.455, p = 0.022) (Figure 4B).
Discussion
SD is a prevalent mental health condition that has the potential to develop into MDD over time. ICBT has been recognized as an effective therapeutic approach for SD in the clinical setting. The current study aimed to utilize ALFF and DC rs-fMRI metrics to explore the abnormalities of brain activity in SD and significantly different brain regions before and after ICBT intervention. We hypothesized that SD would exhibit altered intrinsic brain activity compared to HC, and that these individuals would demonstrate further changes in intrinsic brain activity following ICBT intervention. It was found that compared with HC, ALFF in the right INS was increased and DC in the right PCUN was decreased in SD before ICBT intervention. After ICBT intervention, increased ALFF in the left HIP and decreased DC in the right DCG were found in SD. Furthermore, correlation analyses revealed a negative relationship between altered ALFF values in the left HIP and changes in PHQ-9 scores, and a positive relationship with changes in FATS-ReB scores. Meanwhile, altered DC values in the right DCG were positively correlated with changes in CCTS-TR-BhA scores. The results of our study supported the hypothesis posited in this research.
Our study revealed a decrease in DC of the right PCUN in the SD compared with HC groups. The PCUN, an integral component of the DMN, is involved in processes such as mentalizing, self-referential thinking, scene construction, and episodic memory subsystem linked to visual-spatial imagery.35,36 Evidence has shown that the PCUN serves as a highly interconnected core hub with high energy demands due to its involvement in cognition and emotion.36 A previous rs-fMRI study found that college students with SD exhibited altered ALFF and regional homogeneity (ReHo) in the right PCUN compared with HC.37 Li et al reported increased gray matter volume in the PCUN in young women with SD.38 Another study related to MDD revealed widespread disruption in FC networks involving the PCUN, which was associated with the manifestation of depressive symptoms.39
The INS plays a significant role in attention and working memory, specifically in social judgments, empathy processes, and accurate internal perception.40,41 The current study found that compared with the HC group, ALFF in the right INS was increased in the SD group, consistent with previous research indicating elevated ALFF in the right anterior INS in SD.9 Additionally, a previous rs-fMRI study found abnormal FC between the INS and dorsolateral prefrontal cortex in SD, which was associated with impaired cognitive control and emotion processing.42 Philippi et al reported that decreased FC between the anterior INS and anterior subgenual ACC was correlated with increased severity of depressive symptoms in SD.43
Our data also revealed that the SD group showed increased ALFF in the left HIP after ICBT intervention. The HIP is essential in modulating mood, cognition, and memory consolidation. It also influences behavior in response to emotional or threatening stimuli, displaying heightened sensitivity to stress and negative affect.44,45 Several neuroimaging studies found a significant improvement in hippocampal function following CBT intervention for MDD. A positron emission tomography (PET) study further revealed that CBT resulted in improved clinical symptoms and increased HIP metabolism, whereas paroxetine, a commonly used antidepressant, was associated with decreased HIP metabolism.46 These findings suggested that distinct therapeutic approaches were employed between CBT and pharmacotherapy in treating MDD. In addition, a separate task-based functional MRI study reported heightened arousal responses in the HIP of patients with MDD following CBT intervention.47 A neuroimaging study of ICBT intervention for social anxiety suggested that the effective mechanism of ICBT may be similar to that of traditional CBT.20 ICBT and CBT are both constructed based on the cognitive-behavioral theory, with similar overall treatment goals and therapeutic processes, yet they differ in their format of delivery.
The DCG belongs to the cingulate gyrus, which has been identified as a crucial element in higher cognitive functions, emotional circuits, and internal sensory adaptation.48 Several studies have reported that abnormal DCG function is associated with depression. A rs-fMRI study showed elevated ALFF in the right DCG of adolescents with MDD who engaged in non-suicidal self-injury.49 Another study found that the FC between the right precentral gyrus and right DCG was enhanced and positively correlated with Edinburgh Postpartum Depression Scale (EPDS) scores in postpartum depression.50 Other studies noted that anterior cingulate cortex played an important role in the intervention of depression with ICBT.22,51 The present study observed a significantly decreased DC in the right DCG in the SD group after ICBT intervention.
ICBT was constructed based on the cognitive-behavioral theory. ICBT aims to equip individuals with essential cognitive and behavioral skills to identify and modify negative cognitions, address depressogenic biases in information processing, engage in behavioral activation, and implement effective problem-solving strategies.52 Building on our group’s prior research,15 this study necessitated that the team utilize the program’s backend system to monitor and remind participants to complete their treatment tasks punctually. SD participants who were ultimately included in the analysis adhered to an identical treatment process and schedule. The HIP and DCG play a vital role in controlling and regulating cognition and emotion. Our findings revealed that an increase in ALFF in the left HIP was associated with the improvement of depressive symptoms and the frequency of participating in ReB in the SD group, consistent with the findings of previous neuroimaging studies suggesting that structural or functional improvements in the HIP may be linked to symptom alleviation in depressive symptoms,53,54 and CBT-related skills.55,56 Moreover, decreased DC in the right DCG was positively correlated with improved BhA skills but not with depressive/anxiety symptoms. The correlation results suggested that ICBT in this study may improve the negative emotion and cognition of SD by helping them to increase the mastery or use frequency of BhA and ReB. This finding implied that future studies should focus on improving the functions of ICBT related to engaging in BhA and ReB skills to enhance the intervention effect of ICBT in SD population.
Nonetheless, this study has several limitations. First, although this is a longitudinal study, only one round of MRI scans and psychological assessments was conducted after the ICBT intervention, preventing us from tracking long-term effects. Future research should include long-term follow-ups to observe the sustained effects of ICBT and changes in brain structure and function over time. Second, the sample size in this study was relatively small. Although our findings preliminarily identify target brain regions for ICBT efficacy in SD, large-scale studies are needed for further validation. Lastly, this study lacked an intervention control group, which may limit the accuracy of our findings since we cannot definitively attribute the observed brain region improvements to the ICBT intervention versus the natural remission of depressive symptoms. Therefore, future research should incorporate a waitlist control group and an offline CBT group.
Conclusions
In summary, this study has demonstrated that SD exhibited alterations in ALFF in the HIP and DC in the DCG after ICBT intervention. These changes were correlated with depressive symptoms, ReB, and BhA. Additionally, ALFF in the INS and DC in the PCUN were altered in SD compared with HC. These findings exhibit a degree of consistency with prior neuroimaging research on SD or ICBT. More significantly, this study concentrated on the alterations in ALFF and DC within SD, as well as the impact of ICBT on these variables. Our findings indicate that the alterations in intrinsic brain activity associated with SD, as well as the specific brain regions targeted by the short-term effects of ICBT, are linked to cognitive and emotional processes. These insights may facilitate future exploration of the neuropsychological mechanisms underlying the efficacy of ICBT.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee of Ningbo University (NBU-2020-139). All participants were given comprehensive information about the experimental protocols and potential risks, and willingly signed informed consent forms.
Funding
This work was supported by the Zhejiang Provincial Natural Science Foundation of China (LGF21H090004), the Zhejiang Provincial Philosophy and Social Sciences Planning Project (24NDQN137YBM, 23GXSZ027YB), the Medical Health Science and Technology Project of Zhejiang Province (2021KY976), the Ningbo Key Research and Development Plan Project (2023Z197), the Ningbo Science and Technology Public Welfare Project (2022S26, 2022S133), and the Ningbo Clinical Research Center for Medical Imaging (2022LYKEYB03).
Disclosure
This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-4285302/v1. The authors report no conflicts of interest in this work.
References
1. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta psychiatrica Scandinavica. 2004;109(5):325–331. doi:10.1111/j.1600-0447.2004.00301.x
2. Buntrock C, Ebert DD, Lehr D, et al. Effect of a web-based guided self-help intervention for prevention of major depression in adults with subthreshold depression: a randomized clinical trial. JAMA. 2016;315(17):1854–1863. doi:10.1001/jama.2016.4326
3. Jiang X, Luo Y, Chen Y, et al. Comparative efficacy of multiple therapies for the treatment of patients with subthreshold depression: a systematic review and network meta-analysis. Front Behav Neurosci. 2021;15:755547. doi:10.3389/fnbeh.2021.755547
4. Cuijpers P, Huibers M, Ebert DD, Koole SL, Andersson G. How much psychotherapy is needed to treat depression? A metaregression analysis. J Affective Disorders. 2013;149(1–3):1–13. doi:10.1016/j.jad.2013.02.030
5. van Aubel E, Bakker JM, Batink T, et al. Blended care in the treatment of subthreshold symptoms of depression and psychosis in emerging adults: a randomised controlled trial of acceptance and commitment therapy in daily-life (ACT-DL). Behav Res Ther. 2020;128:103592. doi:10.1016/j.brat.2020.103592
6. Fergusson DM, Horwood LJ, Ridder EM, Beautrais AL. Subthreshold depression in adolescence and mental health outcomes in adulthood. Arch Gen Psychiatry. 2005;62(1):66–72. doi:10.1001/archpsyc.62.1.66
7. Cuijpers P, Smit F, Oostenbrink J, de Graaf R, Ten Have M, Beekman A. Economic costs of minor depression: a population-based study. Acta psychiatrica Scandinavica. 2007;115(3):229–236. doi:10.1111/j.1600-0447.2006.00851.x
8. Cuijpers P, Koole SL, van Dijke A, Roca M, Li J, Reynolds CF. Psychotherapy for subclinical depression: meta-analysis. British J Psychiatry. 2014;205(4):268–274. doi:10.1192/bjp.bp.113.138784
9. Li H, Wei D, Browning M, Du X, Zhang Q, Qiu J. Attentional bias modification (ABM) training induces spontaneous brain activity changes in young women with subthreshold depression: a randomized controlled trial. Psychological Med. 2016;46(5):909–920. doi:10.1017/s003329171500238x
10. Hu Y, Wu X, Chen X, Maguire P, Wang D. Can increased cognitive load help people with subthreshold depression to forget negative information? J Affective Disorders. 2021;283:384–394. doi:10.1016/j.jad.2021.01.062
11. Takagaki K, Okamoto Y, Jinnin R, et al. Behavioral activation for late adolescents with subthreshold depression: a randomized controlled trial. Eur Child Adolesc Psychiatry. 2016;25(11):1171–1182. doi:10.1007/s00787-016-0842-5
12. Zhou T, Li X, Pei Y, Gao J, Kong J. Internet-based cognitive behavioural therapy for subthreshold depression: a systematic review and meta-analysis. BMC Psychiatry. 2016;16(1):356. doi:10.1186/s12888-016-1061-9
13. Andersson G, Titov N, Dear BF, Rozental A, Carlbring P. Internet-delivered psychological treatments: from innovation to implementation. World Psychiatry. 2019;18(1):20–28. doi:10.1002/wps.20610
14. Andrews G, Basu A, Cuijpers P, et al. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. J Anxiety Disord. 2018;55:70–78. doi:10.1016/j.janxdis.2018.01.001
15. Ying Y, Ji Y, Kong F, et al. Efficacy of an internet-based cognitive behavioral therapy for subthreshold depression among Chinese adults: a randomized controlled trial. Psychological Med. 2023;53(9):3932–3942. doi:10.1017/s0033291722000599
16. Hwang JW, Xin SC, Ou YM, et al. Enhanced default mode network connectivity with ventral striatum in subthreshold depression individuals. J Psychiatr Res. 2016;76:111–120. doi:10.1016/j.jpsychires.2016.02.005
17. Zhou HX, Chen X, Shen YQ, et al. Rumination and the default mode network: meta-analysis of brain imaging studies and implications for depression. NeuroImage. 2020;206:116287. doi:10.1016/j.neuroimage.2019.116287
18. Yokoyama S, Okamoto Y, Takagaki K, et al. Effects of behavioral activation on default mode network connectivity in subthreshold depression: a preliminary resting-state fMRI study. J Affective Disorders. 2018;227:156–163. doi:10.1016/j.jad.2017.10.021
19. Mori A, Okamoto Y, Okada G, et al. Behavioral activation can normalize neural hypoactivation in subthreshold depression during a monetary incentive delay task. J Affective Disorders. 2016;189:254–262. doi:10.1016/j.jad.2015.09.036
20. Månsson KN, Carlbring P, Frick A, et al. Altered neural correlates of affective processing after internet-delivered cognitive behavior therapy for social anxiety disorder. Psychiatry Res. 2013;214(3):229–237. doi:10.1016/j.pscychresns.2013.08.012
21. Månsson KN, Frick A, Boraxbekk CJ, et al. Predicting long-term outcome of Internet-delivered cognitive behavior therapy for social anxiety disorder using fMRI and support vector machine learning. Transl Psychiatry. 2015;5(3):e530. doi:10.1038/tp.2015.22
22. Webb CA, Olson EA, Killgore WDS, Pizzagalli DA, Rauch SL, Rosso IM. Rostral anterior cingulate cortex morphology predicts treatment response to internet-based cognitive behavioral therapy for depression. Biol Psych. 2018;3(3):255–262. doi:10.1016/j.bpsc.2017.08.005
23. Thai M, Olson EA, Nickels S, et al. Neural and behavioral markers of inhibitory control predict symptom improvement during internet-delivered cognitive behavioral therapy for depression. Transl Psychiatry. 2024;14(1):303. doi:10.1038/s41398-024-03020-9
24. Zang YF, He Y, Zhu CZ, et al. Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 2007;29(2):83–91. doi:10.1016/j.braindev.2006.07.002
25. Buckner RL, Sepulcre J, Talukdar T, et al. Cortical hubs revealed by intrinsic functional connectivity: mapping, assessment of stability, and relation to Alzheimer’s disease. J Neurosci. 2009;29(6):1860–1873. doi:10.1523/jneurosci.5062-08.2009
26. Li X, Yu R, Huang Q, et al. Alteration of whole brain ALFF/fALFF and degree centrality in adolescents with depression and suicidal ideation after electroconvulsive therapy: a resting-state fMRI study. Front Hum Neurosci. 2021;15:762343. doi:10.3389/fnhum.2021.762343
27. Lu XB, Zhang Y, Yang DY, et al. Analysis of first-episode and chronic schizophrenia using multi-modal magnetic resonance imaging. Eur Rev Med Pharmacol Sci. 2018;22(19):6422–6435. doi:10.26355/eurrev_201810_16055
28. Dobson KS, Li Z. Chinese Version of Handbook of Cognitive behavioral Therapies (3rd Ed.). People’s Medical Publishing House; 2015.
29. Jiang L, Wang Y, Zhang Y, et al. The reliability and validity of the center for epidemiologic studies depression scale (CES-D) for Chinese university students. Front Psychiatry. 2019;10:315. doi:10.3389/fpsyt.2019.00315
30. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the patient health questionnaire (PHQ-9) in the general population. General Hospital Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
31. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archiv Internal Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
32. Strunk DR, Hollars SN, Adler AD, Goldstein LA, Braun JD. Assessing patients’ cognitive therapy skills: initial evaluation of the competencies of cognitive therapy scale. Cognitive Ther Res. 2014;38(5):559–569. doi:10.1007/s10608-014-9617-9
33. Terides MD, Dear BF, Fogliati VJ, et al. Increased skills usage statistically mediates symptom reduction in self-guided internet-delivered cognitive-behavioural therapy for depression and anxiety: a randomised controlled trial. Cognitive Behav Ther. 2018;47(1):43–61. doi:10.1080/16506073.2017.1347195
34. Tong Y, Huang X, Qi CX, Shen Y. Altered functional connectivity of the primary visual cortex in patients with iridocyclitis and assessment of its predictive value using machine learning. Front Immunol. 2021;12:660554. doi:10.3389/fimmu.2021.660554
35. Jitsuishi T, Yamaguchi A. Posterior precuneus is highly connected to medial temporal lobe revealed by tractography and white matter dissection. Neuroscience. 2021;466:173–185. doi:10.1016/j.neuroscience.2021.05.009
36. Power JD, Schlaggar BL, Petersen SE. Studying brain organization via spontaneous fMRI signal. Neuron. 2014;84(4):681–696. doi:10.1016/j.neuron.2014.09.007
37. Zhang B, Qi S, Liu S, Liu X, Wei X, Ming D. Altered spontaneous neural activity in the precuneus, middle and superior frontal gyri, and hippocampus in college students with subclinical depression. BMC Psychiatry. 2021;21(1):280. doi:10.1186/s12888-021-03292-1
38. Li H, Wei D, Sun J, Chen Q, Zhang Q, Qiu J. Brain structural alterations associated with young women with subthreshold depression. Sci Rep. 2015;5(1):9707. doi:10.1038/srep09707
39. Peng D, Liddle EB, Iwabuchi SJ, et al. Dissociated large-scale functional connectivity networks of the precuneus in medication-naïve first-episode depression. Psychiatry Res. 2015;232(3):250–256. doi:10.1016/j.pscychresns.2015.03.003
40. Augustine JR. Circuitry and functional aspects of the insular lobe in primates including humans. Brain Res Brain Res Rev. 1996;22(3):229–244. doi:10.1016/s0165-0173(96)00011-2
41. Paulesu E, Frith CD, Frackowiak RS. The neural correlates of the verbal component of working memory. Nature. 1993;362(6418):342–345. doi:10.1038/362342a0
42. Hwang JW, Egorova N, Yang XQ, et al. Subthreshold depression is associated with impaired resting-state functional connectivity of the cognitive control network. Transl Psychiatry. 2015;5(11):e683. doi:10.1038/tp.2015.174
43. Philippi CL, Motzkin JC, Pujara MS, Koenigs M. Subclinical depression severity is associated with distinct patterns of functional connectivity for subregions of anterior cingulate cortex. J Psychiatr Res. 2015;71:103–111. doi:10.1016/j.jpsychires.2015.10.005
44. Strange BA, Dolan RJ. Anterior medial temporal lobe in human cognition: memory for fear and the unexpected. Cognitive Neuropsychiatr. 2006;11(3):198–218. doi:10.1080/13546800500305096
45. Bremner JD, Randall P, Vermetten E, et al. Magnetic resonance imaging-based measurement of hippocampal volume in posttraumatic stress disorder related to childhood physical and sexual abuse--a preliminary report. Biol Psychiatry. 1997;41(1):23–32. doi:10.1016/s0006-3223(96)00162-x
46. Goldapple K, Segal Z, Garson C, et al. Modulation of cortical-limbic pathways in major depression: treatment-specific effects of cognitive behavior therapy. Arch Gen Psychiatry. 2004;61(1):34–41. doi:10.1001/archpsyc.61.1.34
47. Ritchey M, Dolcos F, Eddington KM, Strauman TJ, Cabeza R. Neural correlates of emotional processing in depression: changes with cognitive behavioral therapy and predictors of treatment response. J Psychiatr Res. 2011;45(5):577–587. doi:10.1016/j.jpsychires.2010.09.007
48. Zhu W, Tang W, Liang Y, et al. Aberrant functional connectivity of sensorimotor network and its relationship with executive dysfunction in bipolar disorder type I. Front Neurosci. 2021;15:823550. doi:10.3389/fnins.2021.823550
49. Huang Q, Xiao M, Ai M, et al. Disruption of neural activity and functional connectivity in adolescents with major depressive disorder who engage in non-suicidal self-injury: a resting-state fMRI study. Front Psychiatry. 2021;12:571532. doi:10.3389/fpsyt.2021.571532
50. Chen C, Li B, Zhang S, et al. Aberrant structural and functional alterations in postpartum depression: a combined voxel-based morphometry and resting-state functional connectivity study. Front Neurosci. 2023;17:1138561. doi:10.3389/fnins.2023.1138561
51. Hanuka S, Olson EA, Admon R, et al. Reduced anhedonia following internet-based cognitive-behavioral therapy for depression is mediated by enhanced reward circuit activation. Psychological Med. 2023;53(10):4345–4354. doi:10.1017/s0033291722001106
52. Webb CA, Rosso IM, Rauch SL. Internet-based cognitive-behavioral therapy for depression: current progress and future directions. Harvard Rev Psychiatry. 2017;25(3):114–122. doi:10.1097/hrp.0000000000000139
53. Deckersbach T, Peters AT, Shea C, et al. Memory performance predicts response to psychotherapy for depression in bipolar disorder: a pilot randomized controlled trial with exploratory functional magnetic resonance imaging. J Affective Disorders. 2018;229:342–350. doi:10.1016/j.jad.2017.12.041
54. Li H, Sagar AP, Kéri S. Translocator protein (18kDa TSPO) binding, a marker of microglia, is reduced in major depression during cognitive-behavioral therapy. Prog Neuro Psychopharmacol Biol Psychiatry. 2018;83:1–7. doi:10.1016/j.pnpbp.2017.12.011
55. Yang S, Jiang C, Ye H, et al. Effect of integrated cognitive therapy on hippocampal functional connectivity patterns in stroke patients with cognitive dysfunction: a resting-state FMRI study. Evidence-Based Complementary Alternative Med. 2014;2014:962304. doi:10.1155/2014/962304
56. Matsuda Y, Makinodan M, Morimoto T, Kishimoto T. Neural changes following cognitive remediation therapy for schizophrenia. Psych Clin Neurosci. 2019;73(11):676–684. doi:10.1111/pcn.12912
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.