")
Back to Journals » Journal of Pain Research » Volume 17
Dysmenorrhea, a Narrative Review of Therapeutic Options
Authors Kirsch E , Rahman S, Kerolus K, Hasan R, Kowalska DB, Desai A, Bergese SD
Received 14 January 2024
Accepted for publication 15 June 2024
Published 15 August 2024 Volume 2024:17 Pages 2657—2666
DOI https://doi.org/10.2147/JPR.S459584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Elayna Kirsch,1 Sadiq Rahman,2 Katrina Kerolus,2 Rabale Hasan,1 Dorota B Kowalska,1 Amruta Desai,2 Sergio D Bergese2
1Department of Obstetrics and Gynecology, Stony Brook University Hospital, Stony Brook, NY, USA; 2Department of Anesthesiology, Stony Brook University Hospital, Stony Brook, NY, USA
Correspondence: Sergio D Bergese, School of Medicine, Stony Brook University, Health Science Center, Level 4, Room 060, Stony Brook, NY, 11794, USA, Tel +631444-2979, Fax +631444-2907, Email [email protected]
Abstract: Dysmenorrhea is the most common pathology women of childbearing age face. It is defined as painful uterine cramping associated with menstruation. Primary dysmenorrhea occurs in the absence of an organic cause, whereas secondary dysmenorrhea is pelvic pain associated with an underlying pelvic pathology. The purpose of this review is to discuss the pathophysiology of dysmenorrhea and provide a discussion of pharmacologic and non-pharmacologic treatment options. Prostaglandins play a large role in the pathophysiology of dysmenorrhea by causing myometrial contraction and vasoconstriction. The first-line treatment for dysmenorrhea is with nonsteroidal anti-inflammatory drugs due to the inhibition of cyclooxygenase enzymes, thereby blocking prostaglandin formation, as well as hormonal contraception. Other pharmacologic treatment options include Paracetamol, as well as Gonadotrophic Release Hormone Analogs, which are typically used in the treatment for endometriosis. Non-pharmacologic treatments with strong evidence include heat therapy and physical exercise. There are less evidence-based data behind other modalities for treating dysmenorrhea, such as dietary supplements, acupuncture, and transcutaneous nerve stimulation, and these methods should be used in conjunction with first-line therapy after a discussion of risks and benefits. Lastly, for women who fail medical management, surgical options include endometrial ablation, presacral neurectomy, and laparoscopic uterosacral nerve ablation. Further research is needed to measure the socioeconomic burden of dysmenorrhea on the healthcare system and to evaluate the efficacy of treatment combinations, as a multi-modal approach likely provides the most benefit for women who suffer from this condition.
Keywords: dysmenorrhea, prostaglandin, NSAIDs, hormonal contraception, pelvic pain, pharmacologic management, behavioral interventions, surgical intervention
Two Letters to the Editor have been received and published for this article
Introduction
Dysmenorrhea is the most common pathology faced by women of childbearing age, regardless of race, age, and/or economic status.1 The worldwide prevalence of dysmenorrhea ranges from 45% to 95% in females of reproductive age and 2 to 29% of women experience severe pain.2 Dysmenorrhea is defined as painful uterine cramping associated with menstruation. It has been both underdiagnosed and inadequately treated and can be classified as primary or secondary dysmenorrhea depending on the etiology.1,2
Primary dysmenorrhea is defined as painful cramping in the lower abdomen during the menstrual cycle that begins before or at the onset of menses in the absence of an organic cause. Pain with primary dysmenorrhea has a specific cyclic pattern—it is usually most severe during the first day of menses and can last for several days. Secondary dysmenorrhea is menstrual pain associated with an underlying pelvic pathology.3 This pathology can include endometriosis, chronic pelvic inflammatory disease, adenomyosis, fibroids, endometrial polyps, ovarian cysts, congenital anomalies, and complications from intrauterine contraceptive devices. Pain caused by secondary dysmenorrhea is typically more diffuse, constant and may not always sync with the onset of menses.3
Although dysmenorrhea is widely prevalent among women of childbearing age, many women do not seek treatment. Furthermore, it is imperative that healthcare professionals are well equipped to diagnose dysmenorrhea, and subsequently educate and treat patients in order to improve their quality of life. Here we present an up-to-date, evidence-based perspective on this topic. The goal of this narrative is to educate providers on first-line pharmacologic treatments for dysmenorrhea and discuss the evidence behind non-pharmacologic interventions. We also aim to review the role of surgical interventions in refractory disease.
Pathophysiology
While the pathophysiology of dysmenorrhea is not completely understood; current research suggests that prostaglandins play a major role.4,5 During menses, endometrial sloughing releases prostaglandins, stimulating myometrial contraction and vasoconstriction. This subsequently causes uterine ischemia, anaerobic metabolite formation, and hypersensitization of nociceptive fibers. Interestingly, women with dysmenorrhea have higher levels of prostaglandin E2 and F2 in menstrual fluid, further supporting the role of prostaglandins in the pathophysiology of dysmenorrhea.5 Additionally, uterine artery dopplers are elevated during menses in women with dysmenorrhea, most likely due to higher resistance blood flow through the uterine arteries.6
Pharmacological Treatment
Analgesia-Based Therapy: Nonsteroidal Anti-Inflammatory Drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line analgesia-based therapy for dysmenorrhea, as the pathophysiology of dysmenorrhea involves prostaglandin release. NSAIDs provide relief by inhibiting cyclooxygenase (COX) enzymes, COX-1 and COX-2, thereby blocking prostaglandin production.7 NSAIDs have been used as a first-line treatment for dysmenorrhea for decades, with evidence supporting its superiority in treating dysmenorrhea compared to placebo. One large metanalysis identified thirty-five publications regarding the efficacy and safety of various NSAIDs, including Naproxen, Ibuprofen, Aspirin, Diclofenac and Ketoprofen, for the treatment of primary dysmenorrhea.8 All five NSAID medications were superior to placebo in relieving pain symptoms from dysmenorrhea. When comparing the efficacy of each medication, Diclofenac provided the most symptom relief, followed by Ibuprofen, Ketoprofen, Naproxen and Aspirin. Ibuprofen and Ketoprofen were considered the safest options with respect to side effects, whereas Diclofenac had the largest side effect profile.8 A Cochrane review that analyzed eighty publications on NSAID use for primary dysmenorrhea similarly found that NSAIDs had significantly greater symptom reduction than placebo for pain relief, though had greater side effects, mostly gastrointestinal upset, than the placebo group. Among the twenty different NSAIDs studied, there was no difference in the effectiveness of treating dysmenorrhea.9
The review additionally compared NSAIDs and Paracetamol (Tylenol), another pharmacologic treatment option for primary dysmenorrhea discussed further below. While this review found that NSAIDs were superior to paracetamol in providing pain relief, the study data was rated as low-quality due to poor reporting methods within the individual journal articles analyzed.9 Additional studies suggest that NSAIDs with fenamate derivatives (ie, mefenamic acid) may work better than NSAIDs with phenyl propionic acid derivatives (ie, Ibuprofen or Naproxen) by blocking both prostaglandin synthesis and action.10 Nonetheless, experts recommend first-line treatment to be with phenyl propionic acid derivates, such as Ibuprofen, with dosages ranging from 400 to 600mg every 4–6 hours or 800mg every 8 hours, with maximum dose of 2400mg daily.11 If this medication class fails to improve symptoms, next-line treatment is with a fenamate derivative, such as Mefenamic acid 500mg followed by 250mg every 6 hours. This pharmacologic treatment is intended to be used for only two to three days at the onset of menses.11
Analgesia-Based Therapy: Paracetamol
Paracetamol (Tylenol) is another analgesic option for primary dysmenorrhea. Paracetamol has been shown to also effect the COX pathway. However, it predominately acts within the central nervous system and has a weak effect on peripheral anti-inflammatory pathways, making it a second-line option for treating primary dysmenorrhea after NSAIDs.12 Within the central nervous system, paracetamol activates descending serotonergic pathways and may influence cannabinoid receptors, mediating its analgesic and antipyretic effects. While paracetamol alone may not be as effective as NSAIDs in reducing pelvic pain, it is a good alternative for women who have contraindications or intolerance to NSAIDs. Furthermore, paracetamol in conjunction with either Pamabrom, a mild diuretic agent, or Caffeine, has been shown to be effective in reducing symptoms of dysmenorrhea with minimal side effects.12,13
Hormonal-Based Therapy: Hormonal Contraception
Another pharmacologic treatment for primary dysmenorrhea is hormonal-based contraception. For women who are agreeable to hormonal treatment and desire contraception in addition to dysmenorrhea treatment, hormonal contraception is a good option. Estrogen prevents the release of FSH, ultimately preventing ovulation. Progesterone causes thinning of the endometrial lining and thickening of cervical mucus, preventing sperm from penetrating. A thin endometrial lining has less arachidonic acid to be used for prostaglandin synthesis, thus reducing both blood flow and contractions during menstruation.14
There are many forms of combined estrogen-progesterone therapies such as oral contraception pills (OCPs), a transdermal patch, or a vaginal ring. A Cochrane review article investigating oral contraceptive use identified twenty-one randomized control trials comparing OCPs with placebo, different dosages of OCPs, and OCPs versus NSAIDs.14 The review found that OCPs reduce pain significantly more than placebo pills in women who suffer from dysmenorrhea. However, OCPs increase the risk of side effects, including irregular bleeding and headaches, and have been known to increase the risk of adverse events, such as blood clots. The data were insufficient to determine if continuous OCPs (no inactive tablets) were superior to the standard regiment of 21 days of hormone pills. There was also insufficient evidence in this review comparing NSAIDs and OCPs. Furthermore, rates of symptom relief were similar with estrogen doses <35mcg or >35mcg.14 There are limited data investigating the use of an estrogen vaginal ring or transdermal patch in the treatment of dysmenorrhea. One review showed evidence that the vaginal ring works as well as OCPs for symptom relief,15 while another randomized trial suggested OCPs have better efficacy than the transdermal patch.16 Nonetheless, the decision to implement estrogen-based therapies and the route of administration should be a shared decision between women and doctor with the women’s medical history taken into consideration.
Progestin-only contraception has also been shown to improve dysmenorrhea. Studies of the levonorgestrel-releasing intrauterine system (LNG-IUS) have shown lower rates of pelvic pain in women with dysmenorrhea from 60% to 29% after 36 months of use.17 The implantable contraceptive device, a single-rod etonogestrel-releasing contraceptive implanted in the upper arm (commonly known as the Nexplanon), is also effective for symptom relief.18 In a small pilot study, the implant reduced dysmenorrhea by 68% after 6 months; another study reported a decrease in dysmenorrhea by 58% after using the injectable contraception medroxyprogesterone acetate (commonly known as Depo-Provera).19 Medroxyprogesterone is associated with weight gain, delayed return to fertility, and should be used with caution for greater than two years as there is a risk of osteoporosis with long-term use.11 Limitations in using progestin-only pills include increased breakthrough bleeding; however, progestin-only contraception is a good alternative for women who have contraindications to estrogen, including hypertension, history of stroke, ischemic heart disease, blood clotting disorders, current breast cancer, liver abnormalities, migraines with aura, and smoking use over age 35.11,17
Hormonal-Based Therapy: Gonadotrophic Releasing Hormone Analogs
Another medication option for dysmenorrhea includes Gonadotrophic Releasing Hormone (GnRH) agonists. GnRH agonists are considered second-line compared to NSAIDs and hormonal contraception. GnRH is naturally produced in the hypothalamus and acts on the pituitary gland to release LH and FSH, causing increased estrogen production from the ovaries. While an initial infusion of GnRH agonists causes an increase in sex hormones, continuous medication treatment causes inhibition of LH and FSH and thus a reduction in estrogen production.20
GnRH analogs are most frequently used as a treatment for dysmenorrhea caused by endometriosis, a disease that occurs when endometrial tissue is located outside of the uterus and thought to be caused by retrograde menstrual flow. One meta-analysis of 11 studies on the use of GnRH analogs for endometriosis found that Relugolix 40mg, Elagolix 400mg and Relugolix 20mg were the most effective treatments for decreasing dysmenorrhea; however, only high-dose treatments were associated with improved quality of life in these women but were also associated with adverse outcomes.21 Most common side effects of GnRH analog treatment include hot-flashes, fatigue, weight gain, fluid retention, decreased libido, and loss of bone density with long-term use.20 GnRH analog therapy may be used empirically for dysmenorrhea in women with persistent dysmenorrhea despite NSAID or hormonal contraception use and who would like to avoid diagnostic laparoscopy assessing for endometriosis, or for women who have persistent pelvic pain despite medical management with a negative diagnostic laparoscopy.11 Women who respond well to GnRH analogs are likely to have an underlying diagnosis of endometriosis contributing to dysmenorrhea. The various pharmacologic options for treating dysmenorrhea are shown in Table 1.
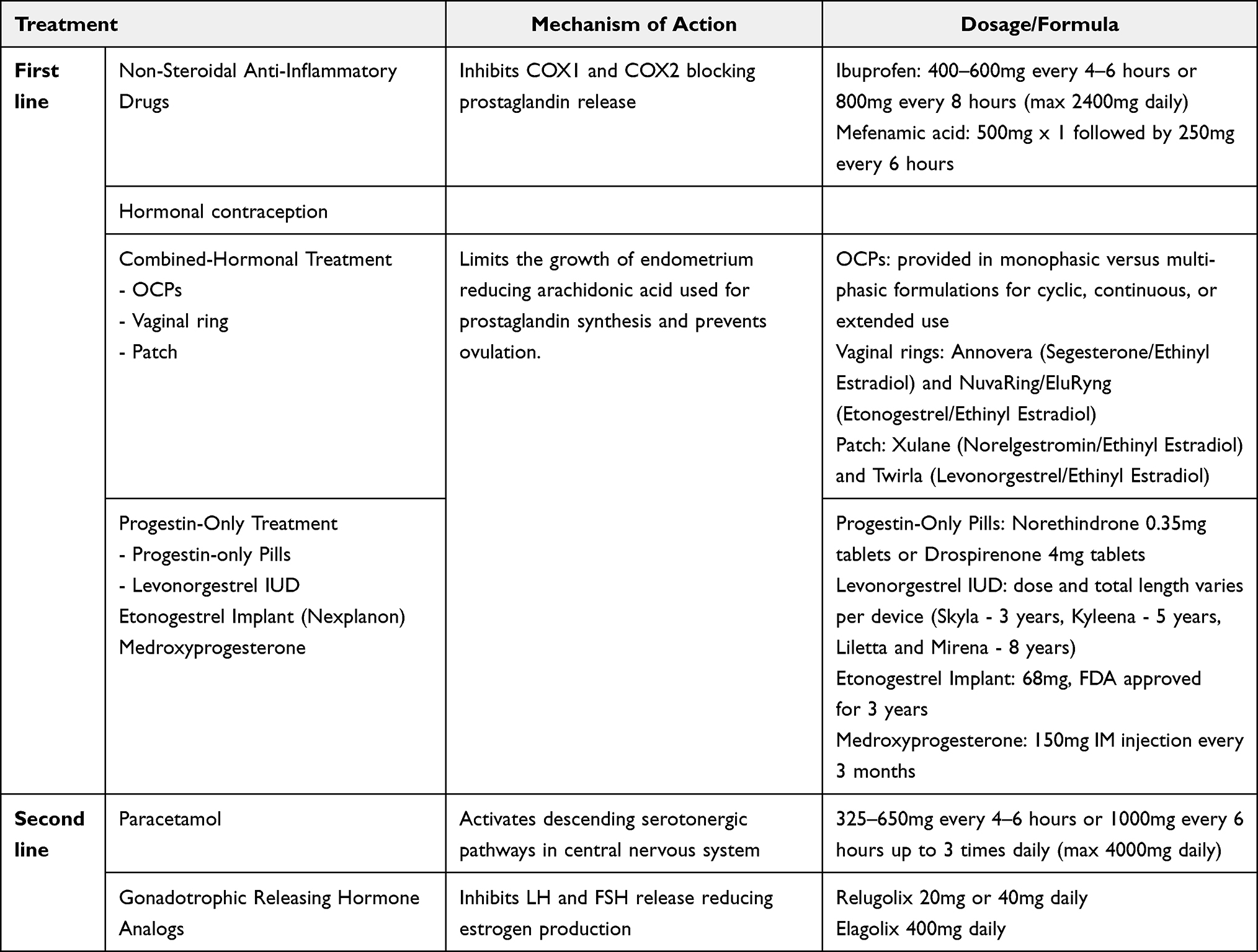 |
Table 1 Pharmacologic Treatment for Primary Dysmenorrhea |
Non-Pharmacological Treatment
Alternative therapies for pharmacologic treatment for dysmenorrhea may be used in place of or in conjunction with medication. All pharmacologic interventions have the potential for side effects, and many women try lifestyle modifications prior to taking medication to avoid unwanted side effects. There is a range of data supporting various non-pharmacologic therapies for dysmenorrhea. In a review that analyzed the most common self-care options for young women, many females rely on rest, heat therapy, herbal medicine or teas, and exercise. In this study, only 11% of females sought care from a physician for their dysmenorrhea. Interestingly, when females used pharmacologic treatment, more women relied on Paracetamol than NSAIDs, even though NSAIDs have greater efficacy.22 Women should be encouraged to discuss non-pharmacologic methods with their providers to allow for counseling of the risks and benefits of less traditional treatment options. The non-pharmacologic treatment options discussed are shown in Table 2.
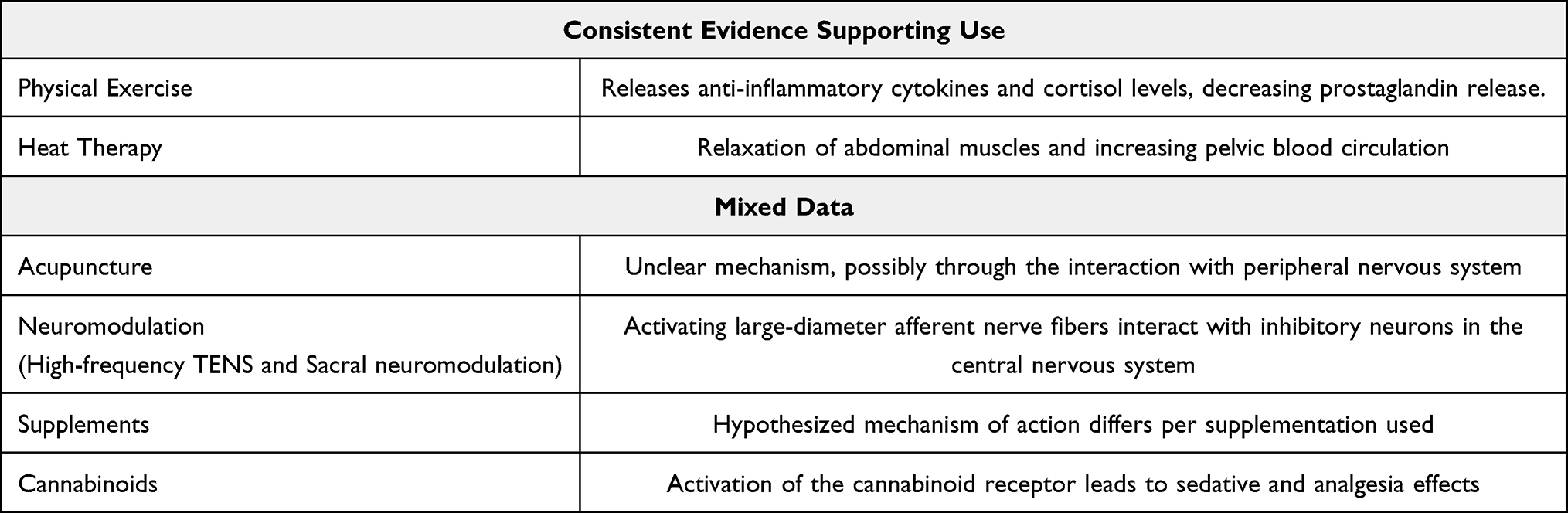 |
Table 2 Nonpharmacologic Treatment for Primary Dysmenorrhea |
Behavioral Interventions
Exercise
Behavioral interventions are the ways in which patients’ actions are altered to improve health. Physical exercise has long been considered a behavioral intervention that improves chronic illnesses, such as diabetes and hypertension. Physical exercise has been postulated as a potential treatment for dysmenorrhea for decades, with the hypothesis that exercise could reduce stress and pain associated with this condition.23 It is thought that exercise causes a release of anti-inflammatory cytokines and cortisol levels, leading to a decrease in prostaglandin release.24,25 A systematic review concluded that therapeutic exercise for eight to twelve weeks produces a decrease in pain intensity of dysmenorrhea and, to a lesser extent, pain duration.26 Given the low-risk side effects associated with physical exercise and the benefit to one’s overall health, exercise in conjunction with other treatment modalities such as NSAIDs or hormonal contraception should be encouraged to help manage menstrual pain.27
Diet
Dietary supplements have also been used by women to treat dysmenorrhea. Supplements can be taken as vitamins, minerals, herbals, enzymes and amino acids and are often easily attainable and self-administered by women. Interventions studied in one review included 12 different herbal medicines (German chamomile, cinnamon, Damask rose, dill, fennel, fenugreek, ginger, guava, rhubarb, uzara, valerian, zataria and five non-herbal supplements [fish oil, melatonin, vitamins B1 and E, and zinc sulphate]) in a variety of formulations and doses. Evidence for dietary supplements in improving pain levels for dysmenorrhea was deemed to be low quality with many limitations including small sample sizes, failure to report methods, and inconsistency.28 While there is limited data to support the efficacy of supplements, the majority of supplements pose little harm to patients and should be reviewed with providers to ensure no interactions with other prescribed medications.
Cannabinoids
Another modality used by patients for pain management is cannabinoids. It is important to note that FDA has not approved cannabinoids for medical use, and in this review, cannabinoids for symptom management will be discussed as “off-label” use. The delta-9-tetrahydrocannabinol (THC) component of cannabinoids has analgesic, anti-inflammatory and sedative properties. Previous research has shown that there are altered levels of endocannabinoids and cannabinoid receptor expression in patients with pelvic pain disorders such as endometriosis and adenomyosis. Endocannabinoids are produced in response to tissue injury and reduce pain by activation of cannabinoid receptors.29 Data-driven evidence for cannabinoids in the treatment for dysmenorrhea is limited; however, one study of over 200 patient reported that 25% used cannabinoids as adjunct treatment, and over 90% of patient reported improvement in pain with the addition of the drug. Patients who used cannabinoids also reported improvement in mood/psychologic symptoms, which plays a large role in patients’ overall pain experiences.30 The variation in legality of cannabinoids has led to challenges for certain populations of patients to access the drug for medicinal use, and there is a lack of oversight in the distribution of cannabinoids, especially if illegally acquired. There is a need for randomized control trials investigating the efficacy of cannabinoids on quality of life and pain in primary dysmenorrhea.
Additional Behavioral Interventions
Other behavioral interventions for the treatment of dysmenorrhea include biofeedback, balneoclimatology (bathing), breathing exercises, hypnotherapy, and relaxation training.31–33 Some data on balneoclimatology suggest aquatic exercises to reduce dysmenorrhea;34 however, specific studies looking at brine and radon baths typically refer to pelvic pain caused by inflammation, such as pelvic inflammatory disease.35 Review articles examining clinical trials studying behavioral interventions for dysmenorrhea determined that there are no strong conclusions to be made due to small sample sizes and variations in quantifying pelvic pain.32 Further studies are needed to better evaluate behavioral interventions for the treatment of dysmenorrhea.
Heat Therapy
Another non-pharmacologic remedy for dysmenorrhea includes heat therapy. A systematic review found that heat therapy consistently decreases menstrual pain in women with primary dysmenorrhea compared to placebo therapy. The mechanism behind symptom relief with heat therapy includes relaxation of abdominal muscles and increased pelvic blood circulation, thereby diminishing pelvic congestion, swelling, vasospasm and ischemia.36 Superficial heat via heat packs/bottles typically treats to 1cm in depth, while deep heat through shortwave or microwave diathermy treats 2–5cm in depth. Few studies have investigated the use of deep heat. One randomized control trial specifically comparing the use of microwave diathermy with transcutaneous electrical nerve stimulation (TENS) found that deep thermotherapy improved pain scores after 10min, 110min and 24hrs after treatment compared to TENS and placebo.37 Limitations in using microwave or shortwave diathermy includes risks of skin burns, risk of excessive heat in subcutaneous fat layer for patients with high BMI, and contraindications to use in patients with metal implants. Patients should first try application of superficial heat, but if no relief is found, shared decision-making should occur in discussing deep heat therapy. While heat therapy is a low-budget and low-risk addition to dysmenorrhea treatment, there is a need for studies to compare short-term and long-term outcomes as well as cost-effectiveness of heat therapy in comparison to other treatment modalities.38
Acupuncture
Acupuncture is a traditional Chinese practice that has been around for more than 3000 years. This practice involves piercing the skin with thin needles throughout different flow points of the body referred to as “Qi” that make up different channels known as “meridians”. Although its exact mechanism has not been well defined, acupuncture treatment has demonstrated efficacy for a wide range of indications.39–41 It is hypothesized that acupuncture interacts with peripheral nerves and modulates neurotransmission in the spinal cord. Additionally, functional MRI studies have demonstrated that acupuncture may influence the activity of various brain regions not directly associated with tactile sensation.42–46 Nonetheless, in a Cochrane review consisting of 42 randomized controlled trials comparing acupuncture to placebo, medication therapy, or alternative treatments for dysmenorrhea, there was no consistent evidence suggesting that acupuncture was superior. While acupuncture may provide a small benefit for pelvic pain, it should not replace conventional treatment or be used as a first-line treatment for dysmenorrhea.47
Neuromodulation
Transcutaneous Electrical Nerve Stimulation (TENS) uses electrical currents through the skin to provide pain relief. Its proposed mechanism of action is through activation of large-diameter afferent nerve fibers. These afferent nerve fibers excite inhibitory neurons at the spinal cord, ventral medulla, and periaqueductal gray, preventing pain modulation via the gate control theory.48 TENS can be provided at two frequency levels: low (2–10 Hz) and high (50–100 Hz). High-frequency TENS was more effective in pain relief than placebo, while low-frequency TENS did not show significance in pain relief for dysmenorrhea.49 It is also believed that TENS causes vasodilation, increases blood flow, and alters menstrual fluid prostaglandins, which is particularly therapeutic for primary dysmenorrhea.49
A more invasive form of neuromodulation than TENS that may be used in treating pelvic pain is sacral neuromodulation. This includes the electrical stimulation of sacral nerve roots through percutaneously implanted electrodes. Sacral nerve stimulation is typically used in refractory cases of chronic pelvic pain, when other treatment modalities, including pharmacologic and non-invasive non-pharmacologic methods, do not alleviate pain. In a meta-analysis investigating the effect of sacral neuromodulation on pelvic pain, there was a significant benefit of sacral neuromodulation in improving pain for up to 2 years. This meta-analysis reported improvement in pain that varied from 40% to 53%.50 Further research is needed on sacral neuromodulation to support these findings.
Surgical Management
Most cases of dysmenorrhea are managed with non-pharmacologic and pharmacologic treatments; however, if unable to provide relief, surgical management is an alternative option (Table 3).50 For women who do not desire future fertility and have associated heavy menstrual bleeding, endometrial ablation may be a good option. One study of women treated with endometrial ablation for heavy menses who also had pelvic pain, approximately half had significant reduction in pelvic pain.51 Presacral neurectomy (PN) and Laparoscopic Uterosacral Nerve Ablation (LUNA) have also been used as an alternative surgical intervention for chronic pelvic pain. Both methods involve transecting sensory nerve fibers. During a Presacral Neurectomy, the somatic pain fibers from the uterus that course within the superior hypogastric plexus are interrupted. The surgery involves incising the pelvic peritoneum over the sacrum and transecting the sacral nerve plexus. Success rates of this procedure range from 60% to 75%; however, long-term postoperative constipation and urinary retention are common side effects, and further research is needed studying the long-term effect of PN on dysmenorrhea.52 LUNA involves transecting the nerve plexuses in the uterosacral ligaments, the structural tissue that connects the junction of the uterus and cervix to the sacrum. This method has had mixed data in regard to the success of treating pelvic pain. One study showed no significant reduction in pain than patients that underwent diagnostic laparoscopy without nerve ablation; however, this study included patients that had chronic pelvic pain from various etiology, including mild endometriosis, pelvic adhesions and pelvic inflammatory disease. Other studies show improvement in pain overtime and improvement in quality of life.53,54 Lastly, hysterectomy would be the definitive surgical treatment for chronic pelvic pain refractory to medications. Hysterectomy is typically reserved for patients with secondary dysmenorrhea, such as endometriosis, who fail more conservative measurements. However, it may be considered as a last-resort-measure for patients with no alternative reason for pelvic pain and who failed non-pharmacologic and pharmacologic management.11,55 The American College of Obstetrics and Gynecology (ACOG) recommends against treating adolescents with dysmenorrhea with hysterectomy.56
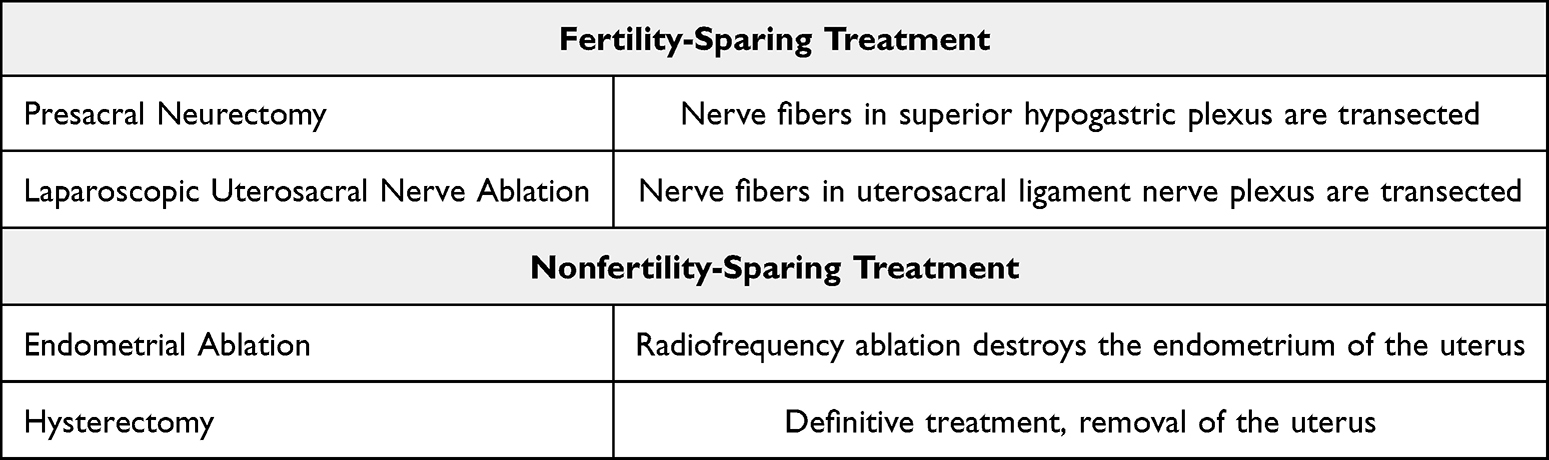 |
Table 3 Surgical Interventions for Primary Dysmenorrhea |
Discussion
This paper has reviewed recent literature on the rates, pathophysiology and treatment modalities for dysmenorrhea, the most common gynecologic condition affecting women of reproductive age. Dysmenorrhea prevalence rates in females or reproductive age have been estimated to be from 45% to 95% worldwide, and there is a considerable impact on quality of life, including school and work productivity.1 Here, we aim to provide a clinical framework for patient care.
First-line treatment of dysmenorrhea should include NSAIDs, as prostaglandins are thought to play the largest role in the pathophysiology of dysmenorrhea. While some data point to Diclofenac providing the maximal analgesia, other studies did not find superiority amongst various types of NSAIDs.8 Ibuprofen was shown to have the best safety profile from the list of NSAIDs reviewed, and the most common side effects to discuss with patients is gastrointestinal upset.9 Another first-line pharmacologic option for patients is hormonal contraception, including combined OCPs and progestin-only contraceptives. There is a lack of studies comparing NSAID use to OCPs for dysmenorrhea, and both options should be offered to patients for maximum analgesia. If patients have contra-indications to estrogen, then progestin-based contraception, including the levonorgestrel IUD or progestin-only pills, are good options for patients.17 With regard to non-pharmacologic treatment, substantial data exists to support behavioral modifications such as exercise, as well as heat therapy, and should be encouraged by providers.
A second-line medication option for dysmenorrhea is Paracetamol, which can be used in combination with NSAIDs or as an alternative therapy for females with contraindications to NSAIDs.12 GnRH analogues are additional hormonal therapy that can be offered to women and are particularly effective for women who have menstrual pain secondary to endometriosis.21 Nonetheless, the utility of GnRH analogs for women with primary dysmenorrhea refractory to NSAIDs and OCPs needs further investigation. If patients continue to have severe symptoms with both NSAID/Paracetamol and hormonal contraceptive use, then patient should be further evaluated for secondary causes of dysmenorrhea, including endometriosis, fibroids, and ovarian cysts. Non-pharmacological treatments for dysmenorrhea that have mixed data include cannabinoid use, dietary supplements, TENS, and acupuncture. While cannabinoid use may have benefits in mitigating pelvic pain, patients should be aware of the legal ramifications of cannabis and providers should discuss with patients who inquire about medicinal cannabinoid use the risk of contamination with other illicit drugs and the fact that its medical use is not FDA approved. Furthermore, while there is no consistent evidence for practices such as dietary supplements, acupuncture, and TENS in effectively treating dysmenorrhea, these are low-cost and low-risk practices that should be considered as additional treatment options for medical management.
Lastly, pelvic pain refractory to pharmacological/non-pharmacologic treatment may require more invasive intervention. For women desiring future fertility, presacral neurectomy or laparoscopic uterosacral nerve ablation are possible surgical interventions that work by transecting pelvic nerve plexuses.52 For women who do not desire future fertility, endometrial ablation may be a good, minimally invasive option for patients. Lastly, hysterectomy is the most definitive surgical treatment but should be reserved for patients who are done with child-bearing and who have exhausted more conservative treatment options.11,55
Conclusion
In this narrative review, we have highlighted the epidemiology, pathophysiology, and treatment options for primary dysmenorrhea. NSAIDs and hormonal contraception are first-line treatments for primary dysmenorrhea. Surgical interventions should be reserved for women who fail medical management or for women who desire definitive treatment. While many non-pharmacologic interventions have minimal data behind their use, low-risk behaviors should be encouraged. Further research with sufficient sample sizes and high-quality methodology is needed measuring the socioeconomic impact primary dysmenorrhea has on the healthcare system. Additionally, given that the treatment of dysmenorrhea is typically multi-modal, further research is needed to evaluate the efficacy of different combinations of pharmacologic and non-pharmacologic treatment methods.
Acknowledgments
Authors would like to acknowledge Dr. Jin Zhaosheng for his input.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harlow SD, Campbell OM. Epidemiology of menstrual disorders in developing countries: a systematic review. BJOG. 2004;111(1):6–16. doi:10.1111/j.1471-0528.2004.00012.x
2. Mendiratta V, Lentz GM. 35 - Primary and secondary dysmenorrhea, premenstrual syndrome, and premenstrual dysphoric disorder: etiology, Diagnosis, Management. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, editors. Comprehensive Gynecology.
3. Bernardi M, Lazzeri L, Perelli F, Reis FM, Petraglia F. Dysmenorrhea and related disorders. F1000Res. 2017;6:1645. doi:10.12688/f1000research.11682.1
4. Guimaraes I, Povoa AM. Primary Dysmenorrhea: assessment and Treatment. Revista Brasileira de Ginecologia e Obstetrícia / RBGO Gynecology and Obstetrics. 2020;42(8):501–507. doi:10.1055/s-0040-1712131
5. Powell AM, Chan WY, Alvin P, Menstrual-PGF2 Alpha LIF. PGE2 and TXA2 in normal and dysmenorrheic women and their temporal relationship to dysmenorrhea. Prostaglandins. 1985;29(2):273–290. doi:10.1016/0090-6980(85)90208-4
6. Dmitrovic R. Transvaginal color Doppler study of uterine blood flow in primary dysmenorrhea. Acta Obstet Gynecol Scand. 2000;79(12):1112–1116. doi:10.1034/j.1600-0412.2000.0790121112.x
7. Cashman JN. The mechanisms of action of NSAIDs in analgesia. Drugs. 1996;52 Suppl 5(Supplement 5):13–23. doi:10.2165/00003495-199600525-00004
8. Nie W, Xu P, Hao C, Chen Y, Yin Y, Wang L. Efficacy and safety of over-the-counter analgesics for primary dysmenorrhea: a network meta-analysis. Medicine. 2020;99(19):e19881. doi:10.1097/MD.0000000000019881
9. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;2015(7):CD001751. doi:10.1002/14651858.CD001751.pub3
10. Feng X, Wang X. Comparison of the efficacy and safety of non-steroidal anti-inflammatory drugs for patients with primary dysmenorrhea: a network meta-analysis. Mol Pain. 2018;14:1744806918770320. doi:10.1177/1744806918770320
11. SRK AM. Dysmenorrhea in adult females: treatment. In: Eckler RLBK, editor UpToDate. 2023.1:1.
12. Di Girolamo G, Sánchez AJ, Los Santos AR D, González CD. Is Acetaminophen, and its combination with pamabrom, an effective therapeutic option in primary dysmenorrhoea? Expert Opin Pharmacother. 2004;5(3):561–570. doi:10.1517/14656566.5.3.561
13. Ali Z, Burnett I, Eccles R, et al. Efficacy of a paracetamol and caffeine combination in the treatment of the key symptoms of primary dysmenorrhoea. Curr Med Res Opin. 2007;23(4):841–851. doi:10.1185/030079907x182239
14. Schroll JB, Black AY, Farquhar C, Chen I. Combined oral contraceptive pill for primary dysmenorrhoea. Cochrane Database Syst Rev. 2023;7(7):CD002120. doi:10.1002/14651858.CD002120.pub4
15. Roumen FJ. The contraceptive vaginal ring compared with the combined oral contraceptive pill: a comprehensive review of randomized controlled trials. Contraception. 2007;75(6):420–429. doi:10.1016/j.contraception.2007.01.013
16. Audet MC, Moreau M, Koltun WD, et al. Evaluation of contraceptive efficacy and cycle control of a transdermal contraceptive patch vs an oral contraceptive: a randomized controlled trial. JAMA 2001.;285(18):2347–2354. 10.1001/jama.285.18.2347.
17. Baldaszti E, Wimmer-Puchinger B, Loschke K. Acceptability of the long-term contraceptive levonorgestrel-releasing intrauterine system (Mirena): a 3-year follow-up study. Contraception. 2003;67(2):87–91. doi:10.1016/s0010-7824(02)00482-1
18. Niu X, Luo Q, Wang C, Zhu L, Huang L. Effects of Etonogestrel implants on pelvic pain and menstrual flow in women suffering from adenomyosis or endometriosis: results from a prospective, observational study. Medicine. 2021;100(6):e24597. doi:10.1097/MD.0000000000024597
19. Walch K, Unfried G, Huber J, et al. Implanon versus medroxyprogesterone acetate: effects on pain scores in patients with symptomatic endometriosis--A pilot study. Contraception. 2009;79(1):29–34. doi:10.1016/j.contraception.2008.07.017
20. Gonadotropin Releasing Hormone (GnRH) Analogues. LiverTox. 2012;1:1.
21. Yan H, Shi J, Li X, et al. Oral gonadotropin-releasing hormone antagonists for treating endometriosis-associated pain: a systematic review and network meta-analysis. Fertil Steril. 2022;118(6):1102–1116. doi:10.1016/j.fertnstert.2022.08.856
22. Armour M, Parry K, Al-Dabbas MA, et al. Self-care strategies and sources of knowledge on menstruation in 12,526 young women with dysmenorrhea: a systematic review and meta-analysis. PLoS One. 2019;14(7):e0220103. doi:10.1371/journal.pone.0220103
23. Metheny WP, Smith RP. The relationship among exercise, stress, and primary dysmenorrhea. J Behav Med. 1989;12(6):569–586. doi:10.1007/BF00844826
24. Pascoe MC, Thompson DR, Ski CF. Yoga, mindfulness-based stress reduction and stress-related physiological measures: a meta-analysis. Psychoneuroendocrinology. 2017;86:152–168. doi:10.1016/j.psyneuen.2017.08.008
25. Febbraio MA. Exercise and inflammation. J Appl Physiol. 2007;103(1):376–377. doi:10.1152/japplphysiol.00414.2007
26. Carroquino-Garcia P, Jimenez-Rejano JJ, Medrano-Sanchez E, de la Casa-Almeida M, Diaz-Mohedo E, Suarez-Serrano C. Therapeutic Exercise in the Treatment of Primary Dysmenorrhea: a Systematic Review and Meta-Analysis. Phys Ther. 2019;99(10):1371–1380. doi:10.1093/ptj/pzz101
27. Armour M, Ee CC, Naidoo D, et al. Exercise for dysmenorrhoea. Cochrane Database Syst Rev 2019.;9(9):Cd004142. 10.1002/14651858.CD004142.pub4.
28. Pattanittum P, Kunyanone N, Brown J, et al. Dietary supplements for dysmenorrhoea. Cochrane Database Syst Rev 2016.;3(3):CD002124. 10.1002/14651858.CD002124.pub2.
29. Sinclair J, Abbott J, Proudfoot A, Armour M. The Place of Cannabinoids in the Treatment of Gynecological Pain. Drugs. 2023;83(17):1571–1579. doi:10.1007/s40265-023-01951-z
30. Carrubba AR, Ebbert JO, Spaulding AC, DeStephano D, DeStephano CC. Use of Cannabis for Self-Management of Chronic Pelvic Pain. J Womens Health. 2021;30(9):1344–1351. doi:10.1089/jwh.2020.8737
31. Denney DR, Gerrard M. Behavioral treatments of primary dysmenorrhea: a review. Behav Res Ther. 1981;19(4):303–312. doi:10.1016/0005-7967(81)90051-6
32. Proctor ML, Murphy PA, Pattison HM, Suckling J, Farquhar CM. Behavioural interventions for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. 2007;(3):CD002248. doi:10.1002/14651858.CD002248.pub3
33. Lewis RJ, Wasserman E, Denney NW, Gerrard M. The etiology and treatment of primary dysmenorrhea: a review. Clinic Psychol Rev. 1983;3(3):371–389. doi:10.1016/0272-7358(83)90020-X
34. Rezvani S, Taghian F, Valiani M. The effect of aquatic exercises on primary dysmenorrhoea in nonathlete girls. Iran J Nurs Midwifery Res. 2013;18(5):378–383.
35. Malgorzata Wojcik KP. APPLICATION PHYSIOTHERAPY AND BALNEOCLIMATOLOGY IN GYNAECOLOGY. Acta Balneol. 2022;LXV(176):253–262. doi:10.36740/ABAL202304110
36. Ke Y-M, Ou M-C, Ho C-K, Lin Y-S, Liu H-Y, Chang W-A. Effects of somatothermal far-infrared ray on primary dysmenorrhea: a pilot study. Evid Based Complement Alternat Med. 2012;2012:240314. doi:10.1155/2012/240314
37. Machado AFP, Perracini MR, Rampazo ÉP, Driusso P, Liebano RE. Effects of thermotherapy and transcutaneous electrical nerve stimulation on patients with primary dysmenorrhea: a randomized, placebo-controlled, double-blind clinical trial. Complement Ther Med. 2019;47:102188. doi:10.1016/j.ctim.2019.08.022
38. Jo J, Lee SH. Heat therapy for primary dysmenorrhea: a systematic review and meta-analysis of its effects on pain relief and quality of life. Sci Rep. 2018;8(1):16252. doi:10.1038/s41598-018-34303-z
39. Mu J, Furlan AD, Lam WY, Hsu MY, Ning Z, Lao L. Acupuncture for chronic nonspecific low back pain.Cochrane Database Syst Rev. 2020;12(12):CD013814. doi:10.1002/14651858.CD013814
40. Cheong KB, Zhang J-P, Huang Y, Zhang Z-J, Baradaran HR. The Effectiveness of Acupuncture in Prevention and Treatment of Postoperative Nausea and Vomiting - A Systematic Review and Meta-Analysis. PLoS One. 2013;8(12):e82474. doi:10.1371/journal.pone.0082474
41. Yuan QL, Wang P, Liu L, et al. Acupuncture for musculoskeletal pain: a meta-analysis and meta-regression of sham-controlled randomized clinical trials. Sci Rep 2016.;6(1):30675. 10.1038/srep30675.
42. Chae Y, Chang DS, Lee SH, et al. Inserting needles into the body: a meta-analysis of brain activity associated with acupuncture needle stimulation. J Pain. 2013;14(3):215–222. doi:10.1016/j.jpain.2012.11.011
43. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/s0166-2236(02)00006-1
44. Karatay S, Okur SC, Uzkeser H, Yildirim K, Akcay F. Effects of Acupuncture Treatment on Fibromyalgia Symptoms, Serotonin, and Substance P Levels: a Randomized Sham and Placebo-Controlled Clinical Trial. Pain Med. 2018;19(3):615–628. doi:10.1093/pm/pnx263
45. Parrish TB, Schaeffer A, Catanese M, Rogel MJ. Functional magnetic resonance imaging of real and sham acupuncture. Noninvasively measuring cortical activation from acupuncture. IEEE Eng Med Biol Mag. 2005;24(2):35–40. doi:10.1109/memb.2005.1411346
46. Zhang RX, Lao L, Wang L, et al. Involvement of opioid receptors in electroacupuncture-produced anti-hyperalgesia in rats with peripheral inflammation. Brain Res 2004.;1020(1–2):12–17. 10.1016/j.brainres.2004.05.067.
47. Smith CA, Armour M, Zhu X, Li X, Lu ZY, Song J. Acupuncture for dysmenorrhoea. Cochrane Database Syst Rev 2016. 4(4):CD007854. doi:10.1002/14651858.CD007854.pub3
48. Johnson M. Transcutaneous Electrical Nerve Stimulation: mechanisms, Clinical Application and Evidence. Rev Pain. 2007;1(1):7–11. doi:10.1177/204946370700100103
49. Elboim-Gabyzon M, Kalichman L. Transcutaneous Electrical Nerve Stimulation (TENS) for Primary Dysmenorrhea: an Overview. Int J Womens Health. 2020;12:1–10. doi:10.2147/IJWH.S220523
50. Greig J, Mak Q, Furrer MA, Sahai A, Raison N. Sacral neuromodulation in the management of chronic pelvic pain: a systematic review and meta-analysis. Neurourol Urodyn Apr. 2023;42(4):822–836. doi:10.1002/nau.25167
51. Wyatt SN, Banahan T, Tang Y, Nadendla K, Szychowski JM, Jenkins TR. Effect of Radiofrequency Endometrial Ablation on Dysmenorrhea. J Minim Invasive Gynecol. 2016;23(7):1163–1166. doi:10.1016/j.jmig.2016.08.825
52. Chen FP, Soong YK. The efficacy and complications of laparoscopic presacral neurectomy in pelvic pain. Obstet Gynecol. 1997;90(6):974–977. doi:10.1016/s0029-7844(97)00484-5
53. Daniels J, Gray R, Hills RK, et al. Laparoscopic uterosacral nerve ablation for alleviating chronic pelvic pain: a randomized controlled trial. JAMA. 2009;302(9):955–961. 10.1001/jama.2009.1268.
54. Proctor ML, Latthe PM, Farquhar CM, Khan KS, Johnson NP. Surgical interruption of pelvic nerve pathways for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. 2005;(4):CD001896. doi:10.1002/14651858.CD001896.pub2
55. Itani R, Soubra L, Karout S, Rahme D, Karout L, Khojah HMJ. Primary Dysmenorrhea: pathophysiology, Diagnosis, and Treatment Updates. Korean J Fam Med. 2022;43(2):101–108. doi:10.4082/kjfm.21.0103
56. ACOG. Dysmenorrhea and Endometriosis in the Adolescent. ACOG Committee Opinion. 2018;132(6):e249–e258. doi:10.1097/AOG.0000000000002978
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.