")
Back to Journals » Journal of Pain Research » Volume 18
Effect of Bilateral Erector Spinae Plane Block on the Gastrointestinal Function in Patients Undergoing Traumatic Lumbar Spine Fracture surgery: A Retrospective Study
Authors Zhao M, Gao M, Zhang X, Zhou Q, Yu P, Liu C, Song X, Shan X, Dong J, Li Z, Wang Q
Received 21 August 2024
Accepted for publication 2 March 2025
Published 13 March 2025 Volume 2025:18 Pages 1231—1239
DOI https://doi.org/10.2147/JPR.S492380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Meizhu Zhao, Mingyang Gao, Xin Zhang, Qi Zhou, Peixia Yu, Chunxiao Liu, Xueyin Song, Xin Shan, Jianglong Dong, Zhihua Li, Qiujun Wang
Department of Anesthesiology, The Third Hospital of Hebei Medical University, Shijiazhuang, 050051, People’s Republic of China
Correspondence: Zhihua Li, Email [email protected] Qiujun Wang, Email [email protected]
Purpose: This retrospective study aimed to explore the effect of erector spinae plane block (ESPB) on the gastrointestinal function in patients after traumatic lumbar fracture surgery and the effects of different levels of block approach.
Patients and Methods: Clinical data were retrospectively analyzed from electronic medical records of patients who underwent traumatic lumbar spine fracture surgery (September 2022-June 2023). Eligible patients were divided into three groups: group L (bilateral ESPB at L3 level), group T (bilateral ESPB at T12 level) and group C (no block). The primary outcomes were the incidence and the time of occurrence postoperative bloating. We also recorded the time of the first flatus and bowel movement, postoperative nausea and vomiting (PONV), gastrointestinal medications, enema, intraoperative opioid dosage, number of rescue analgesia within 48 h postoperatively, visual analogue scale (VAS) scores at 24 h and 48 h postoperatively, inflammatory mediators, complications and hospital length of stay (LOS).
Results: 145 patients were included, including 32 in group L, 33 in group T and 80 in group C. Patients in group L and T experienced less bloating compared to group C (P < 0.05). Patients in group T presented bloating significantly later than group L (log rank P < 0.0167). Patients in group L and group T had a significantly shorter time to first flatus and bowel movement, lower incidence of PONV, gastrointestinal medications and enema, and a lower dose of opioid and VAS scores at 24 h postoperatively compared to group C (all P < 0.05), the difference between group L and T was not statistically significant.
Conclusion: Bilateral ESPB improved postoperative gastrointestinal function in patients with traumatic lumbar spine fracture, where the T12 level of ESPB was more favorable than the L3 level.
Keywords: erector spinae plane block, postoperative ileus, spine fracture, trauma
Introduction
Postoperative gastrointestinal dysfunction (POGD), or postoperative ileus (POI), frequently occurs after surgery in patients with lumbar spine fracture.1 It typically manifests as transient gastrointestinal dysfunction, resulting in symptoms such as nausea and vomiting, bloating, abdominal pain, and delayed expulsion of gas or faeces.2 Improper management of POGD can impact nutrient intake and absorption, causing delayed wound healing, higher infection risk, increased hospitalization expenses, extended the length of hospital stay and recovery periods, and even potential mortality.3,4 POGD has been linked to autonomic dysfunction, opioid use, surgical traumatic stress, inflammation, and prolonged bedbound.1,3–6 Patients who have suffered from a traumatic lumbar fracture tend to display a greater severity of POGD. This is primarily due to the compression and stimulation of the peripheral sympathetic nerves by the fractured vertebrae and hematoma. Pre-existing bedridden immobility may also contribute to this syndrome.7,8 The administration of stellate ganglion block or adjunctive drugs, including dexmedetomidine, lidocaine, and gastrointestinal medications, for the prevention of POGD following spinal surgery is currently available in clinical practice. However, these interventions pose a risk of causing hemodynamic instability or having a controversial effects.7,9,10
The erector spinae plane block (ESPB) is a regional technique that involves the injection of local anesthetic into the fascial space between the deep surface of the erector spinae muscle and the transverse process of the vertebral body. It is commonly used for postoperative pain management in lumbar spine surgery and facilitates early recovery and improved analgesia.11,12 Recently, ESPB at the T8 level has been shown to improve acute gastrointestinal dysfunction in critically ill patients.13 Zheng et al14 also demonstrated that ESPB at the 2-level of the lumbar spine bilaterally promotes recovery of gastrointestinal function after lumbar fusion. However, it remains unclear whether ESPB facilitates the recovery of gastrointestinal function in patients with traumatic lumbar spine fracture surgery, as no studies have confirmed the optimal level of block.
The sympathetic preganglionic fibres that innervate the gastrointestinal tract from the stomach to the transverse colon have their origins at T5-T12. In theory, the ESPB administered near the level of the thoracic level is more effective in blocking these sympathetic nerves and promote gastrointestinal motility. Given the current availability of ESPB at our institution, and in light of previous researches, we hypothesized that bilateral ESPB may improve postoperative recovery of gastrointestinal function in patients with traumatic lumbar spine fracture and ESPB at the T12 level may show more advantages than ESPB at the L3 level. The purpose of our retrospective study was to analyze and justify this hypothesis.
Materials and Method
Data Collection
This study was approved by the Ethics Committee of the Third Hospital of Hebei Medical University (Review No: Ke 2023–046-1). The need for written informed consent was waived. The selected patients were those who underwent traumatic lumbar vertebral fracture surgery under general anesthesia, of any gender, aged 18–80 years old, with American Society of Anesthesiologists (ASA) grade I to III, and all of them were using a patient-controlled intravenous analgesia (PCIA). The exclusion criteria included the following: preoperative presence of abdominal injury, or combined gastrointestinal functional disorders (ulcerative colitis, Crohn’s disease, irritable bowel syndrome, etc)., body mass index (BMI) ≥40 kg/m2, combined spinal cord injury, tumor, and other causes of pathologic fracture, patients with preoperative use of opioid medication, surgery and injury of more than two segments, and simultaneous combination of other parts of surgery or nerve block. An electronic medical record information system was used to review and obtain relevant data on the patients. Patients were divided into three groups according to whether ESPB block was performed and the level of ESPB block: group L (bilateral ESPB at the level of L3), group T (bilateral ESPB at the level of T12), and group C (no block).
The primary outcomes were the incidence of bloating within 48 hours postoperatively and the time of the first occurrence of bloating based on relevant medical records and nursing notes. Secondary outcomes included the time of the first flatus and bowel movement, the occurrence of postoperative nausea and vomiting (PONV), the use of gastrointestinal medications, and the use of enema, intraoperative opioid dosage, number of rescue analgesia within 48 h postoperatively, VAS scores at 24 and 48 hours after operation and the length of hospital stay (LOS, counted from the first postoperative day to discharge). All opioid dosages, except for remifentanil, were converted to a sufentanil equivalent dose. Additionally, postoperative complications such as delirium, dizziness, fever, and wound infection were recorded. Inflammation mediators, such as white blood cell (WBC) count, neutrophil-to-lymphocyte count ratio (NLR), and C-reactive protein (CRP) were collected on both preoperative and postoperative days. Demographic and surgical characteristics were collected, including gender, age, body mass index (BMI), lumbar spine injury and operative segment, preoperative comorbidities (associated with limbs fractures other than the lumbar spine, hypertension, diabetes mellitus, coronary artery disease, pulmonary complications, etc)., ASA grade, duration of injury to surgery, duration of surgery and anesthesia, intraoperative urine output, bleeding, fluid transfusion and blood transfusion.
Anesthesia Management
Following the anesthesia practice of our institution, patients were admitted to the operating room to establish intravenous access, electrocardiogram, pulse oximetry, and non-invasive blood pressure monitoring. General anesthesia was induced with intravenous midazolam, sufentanil, etomidate and rocuronium bromide for endotracheal intubation. Blood pressure was maintained within a range of 80% to 120% by continuous intravenous infusion of propofol and remifentanil. Neuromuscular blocking drugs were administered during surgery as required. PCIA was performed with 1 ug/kg sufentanil, ramosetron 0.6 mg and 0.9% sodium chloride to 100 mL. The programmes were set with a background dose 2 mL/h, patient-controlled analgesia bolus 2 mL, and locking time interval 15 minutes.
Ultrasound-Guided Bilateral Erector Spinae Block
At our institution, ESPB was performed using two puncture sites located at the L3 and T12 levels, as determined by experienced anesthetists’ preference. The patient was placed in the prone position after induction, and the patient’s anatomical structures such as the spinous processes, transverse processes, and erector spinae muscles were identified using a high-frequency ultrasound transducer. For the ESPB at L3 level, a nerve block needle was inserted at the L2 level and translated cranially to caudally to reach the transverse process of L3. The tip of the translating needle was placed with the bevelled side facing up to reach the tip of the L3 transverse process. Next, 2 mL of saline was injected to ensure diffusion in the fascial plane without intramuscular injection. On each side, 25 mL of 0.375% ropivacaine solution was injected, for a total of 50 mL per patient. For the ESPB at T12 level, the nerve block needle was inserted at the level of T11, translated cranially to caudally to reach the level of T12, and the tip of the needle was placed obliquely upward to reach the tip of the transverse process of T12.The rest of the procedure was performed as in the previous L3 level ESPB.
Statistical Analysis
The statistical analyses were performed on SPSS software version 26.0 (IBM Corp, Armonk, NY, USA). Continuous variables were expressed as mean ± SD (x ± s) or median (IQR), while frequencies and percentages described qualitative variables using the chi-squared test or Fisher’s exact probability method. Normally distributed data were tested using one-way analysis of variance (ANOVA) and comparisons between groups were made using the Bonferroni test. Non-normally distributed data were tested using the Kruskal–Wallis H rank sum test. A Log Rank test was performed to determine the time of occurrence of postoperative abdominal distension. Kaplan-Meier survival curves were plotted, and between-group comparisons were corrected using the Bonferroni test. The difference was considered statistically significant at P < 0.0167 after correction. All other statistical tests were performed using the two-sided test, and the difference was considered statistically significant at P < 0.05.
Results
A total of 145 patients were included in the present study for analysis out of 163 patients who underwent surgery for traumatic lumbar spine fracture. 16 patients were excluded based on the inclusion and exclusion criteria (3 with 3-segment lumbar spine injuries, 5 with spinal cord injuries, 3 with extra-lumbar spine surgeries, 3 with abdominal injuries, and 2 without PCIA). There were 32 patients in group L, 33 patients in group T, and 80 patients in group C (Figure 1). There was no statistically significant difference among the three groups in terms of demographic and surgical characteristics, all P > 0.05 (Table 1).
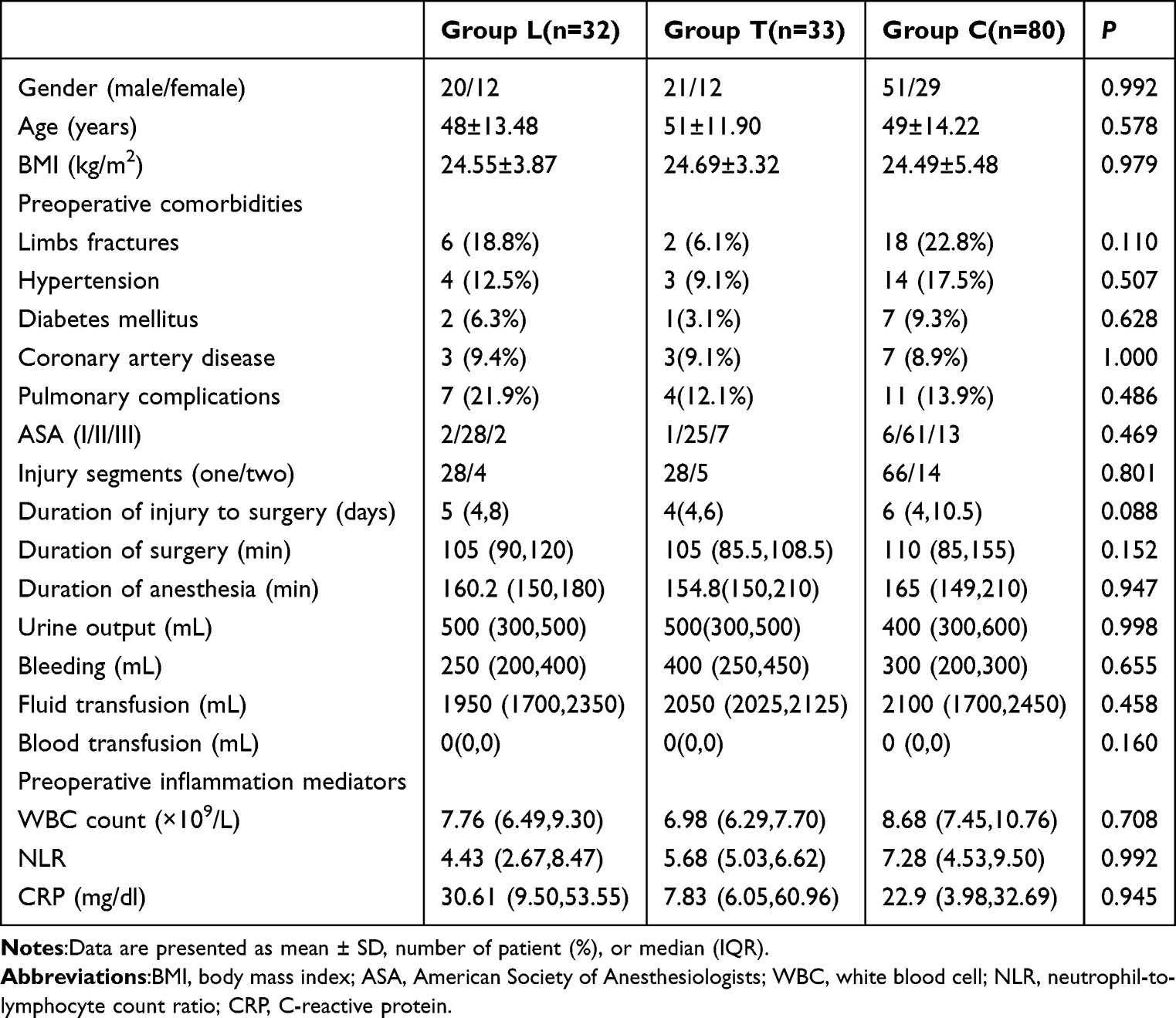 |
Table 1 Demographic and Surgical Characteristic |
 |
Figure 1 Flow diagram demonstrating patients included for study analysis. |
The incidence of bloating within 48 hours after operation was lower in group L and group T compared to group C (40.6%, 18.2%, 68.8%, P < 0.05), and the difference between patients in group L and group T was not statistically significant. Survival analysis of the time of occurrence of bloating in the three groups was performed, and the Kaplan-Meier survival curves showed that the time of occurrence of bloating was significantly later in groups L and T than in group C (Log Rank P < 0.001). And the time of occurrence of bloating was later in group T than in group L, P < 0.0167 (Figure 2). The time to first flatus and bowel movement after operation in groups L and T were earlier compared to group C, all P > 0.05. The difference between the patients in groups L and T was not statistically significant. The incidence of PONV, gastrointestinal medications use, and postoperative enema in groups L and T were lower than in group C, all P < 0.05. There was no statistically significant difference between patients in group L and group T regarding the time to first flatus and bowel movement, incidence of PONV, use of gastrointestinal medications, and enema, all P > 0.05 (Table 2).
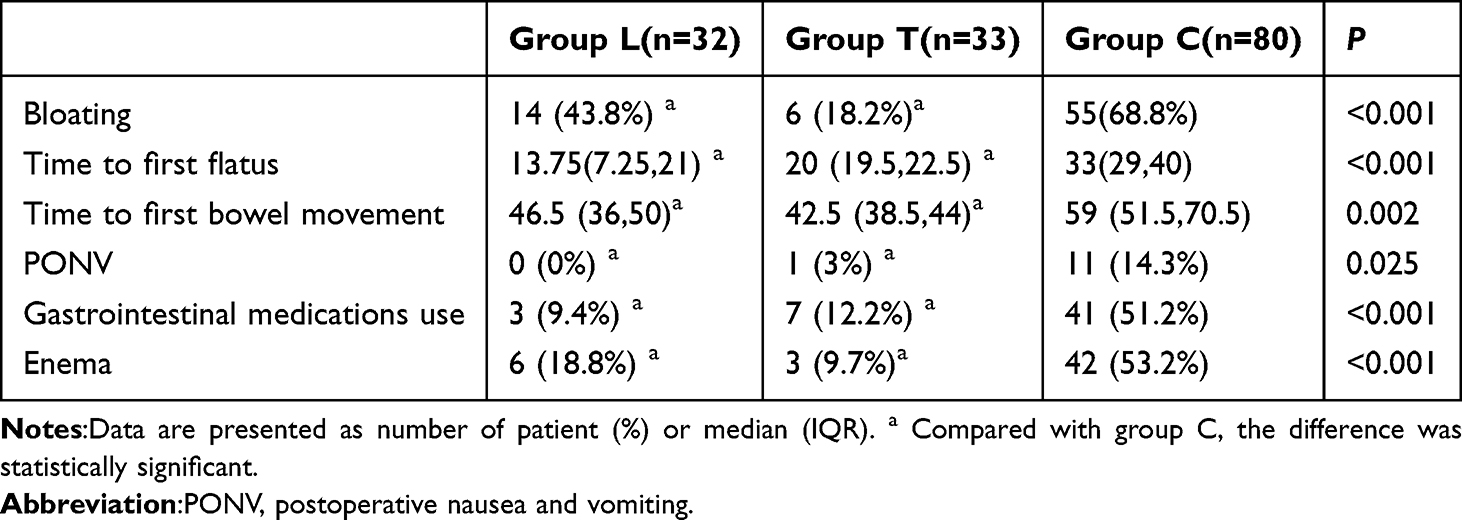 |
Table 2 Operative Gastrointestinal Function |
 |
Figure 2 Kaplan-Meier survival curves for time of the first occurrence of bloating among three groups. |
Compared to group C, patients in groups L and T received lower intraoperative remifentanil dosages and reported lower 24 h postoperative VAS scores (P < 0.05). The differences between patients in groups L and T were not statistically significant (P > 0.05). There were no statistically significant differences in the intraoperative dosage of sufentanil, VAS scores at 48 h postoperatively, number of analgesic remedies used in the 48 h postoperative period, postoperative inflammation mediators, postoperative complications, hospital length of stay among the three groups, all P > 0.05 (Table 3).
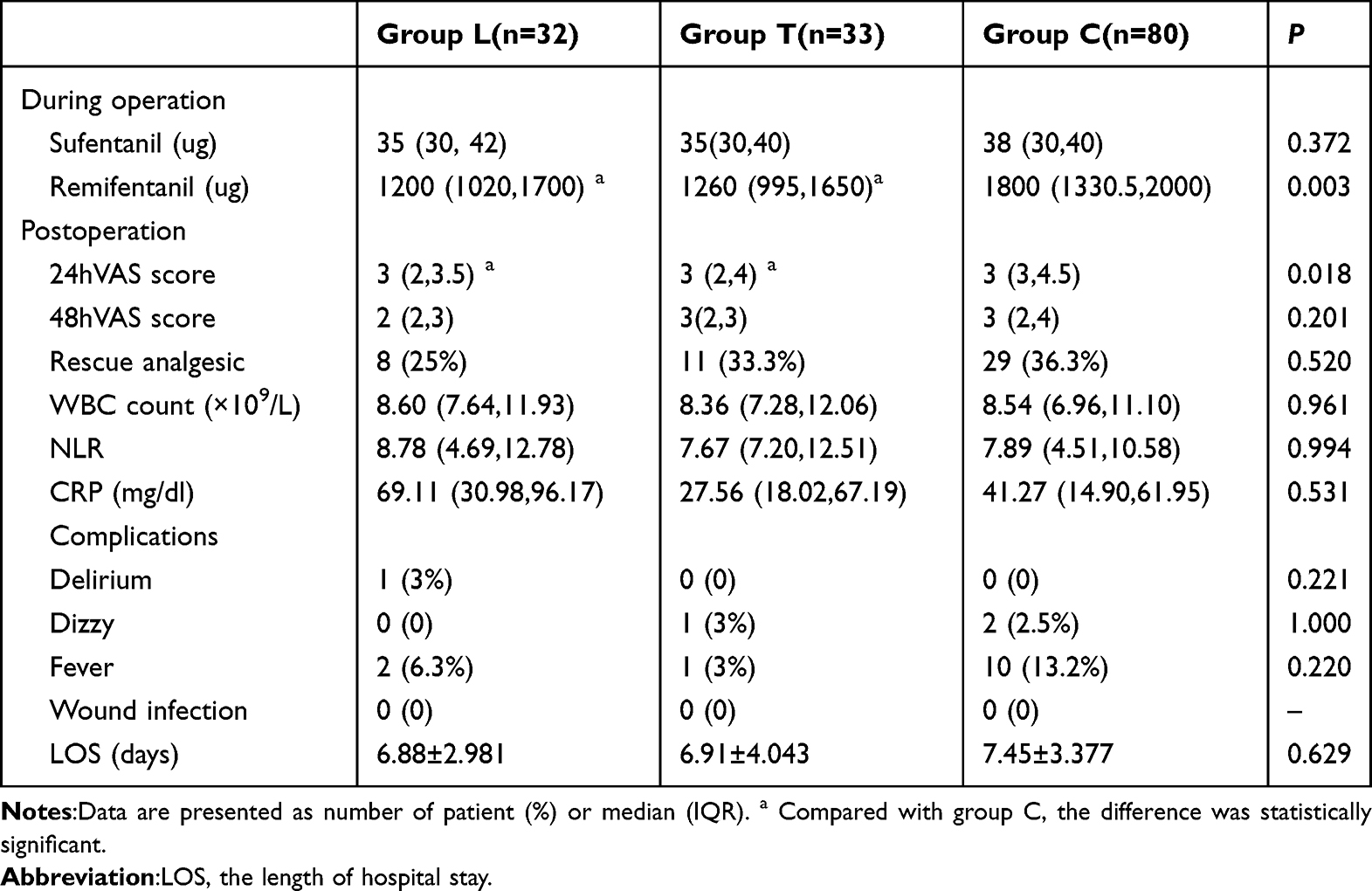 |
Table 3 Other Variables |
Discussion
ESPB, a popular fascial plane block technique, has been employed in recent years for the management of perioperative analgesia in patients undergoing spinal surgery. To our knowledge, this study focused for the first time on patients undergoing lumbar spine fracture surgery who may have more severe postoperative gastrointestinal dysfunction. The reduced total dosage of ropivacaine in this study led to a lower incidence of local anesthetic toxicity compared to the results reported in a previous study conducted by Zheng et al.14 Furthermore, it is the first to compare the differences in the effects of different block levels on postoperative gastrointestinal function. The results of this study indicated that bilateral erector spinae block accelerated postoperative recovery of gastrointestinal function, reduced postoperative pain, and decreased opioid dosage in patients with traumatic lumbar fracture compared to those who did not receive ESPB. ESPB at the level of the transverse process of T12 may enhance postoperative gastrointestinal recovery more than L3.
The mechanism behind the promotion of postoperative recovery of gastrointestinal function in patients undergoing lumbar spine fracture surgery by bilateral ESPB remains unclear. The gastrointestinal tract is innervated by both sympathetic and parasympathetic nerves, sympathetic excitation inhibits gastrointestinal motility and secretion, while parasympathetic nerves do the opposite. Preganglionic sympathetic fibres originating from the lateral horn of the spinal cord in the T5-T12 level enter the paravertebral sympathetic trunk via the white traffic branch, and are distributed to the stomach, small intestine, ascending and transverse colons following commutation of the abdominal ganglia and superior mesenteric ganglia. Sympathetic preganglionic fibres from the lateral horn of the spinal cord at T12-L3 enter the paravertebral sympathetic trunk via the white traffic branch and innervate the descending colon, sigmoid colon and rectum after ganglionic commutation in the mesenteric subperitoneal plexus and the infra-abdominal plexus.15 The erector spinae plane block acts mainly through the physical diffusion of local anesthetic into the neural structures within the fascial plane. According to previous autopsy and clinical experience, local anesthetic can diffuse longitudinally at 3–5 levels, with 25 mL of local anesthetic injected at the level of L3 diffusing to L1-L5, and at the level of T12 diffusing more broadly to T8-L5.16 The use of the erector spinae muscle plane block in thoracic and abdominal surgical analgesia provided clinical evidence of the anterior diffusion of local anesthetics.17–22 Schwartzmann et al23 also found local anesthetic diffusion deep into the erector spinae muscle, paravertebral and circumferential epidural under magnetic resonance imaging. Therefore, the most likely mechanism explains that bilateral ESPB can promote gastrointestinal motility through local anesthetic diffusion into the paravertebral and epidural spaces, thus blocking the dorsal and ventral branches and sympathetic nerves innervating the gastrointestinal tract. In this study, we also found that patients who received ESPB at the T12 level experienced bloating later than those who received ESPB at the L3 level. This is because the anatomical location of the T12 level is closer to the sympathetic nerves of the gastrointestinal tract, and the transverse processes of the thoracic vertebrae are 2–3 cm in length, while those of the lumbar vertebrae can be up to 4–6 cm in length and the muscles of the lumbar back are more compact.24 These anatomical features make the T12 level ESPB have a relatively wide spread of local anesthetics and the sympathetic nerve block is relatively adequate. The reason for no difference in the incidence of abdominal distension and postoperative defecation time between the two groups at the T12 level and the L3 level may be due to the sample size limitation received.
We found that bilateral erector spinae plane block can reduce intraoperative opioid dosage and pain levels at 24 hours after operation. The ESPB at the lumbar level has been demonstrated to have an analgesic effect in lumbar spine surgery. Similar to our results, ESPB performed at the T12 level provided effective analgesia and the block effect was safe and stable at the T9-L5 level in lumbar spine surgeries.16,25 The opioid-sparing effect of ESPB at the L3 level and T12 level also provides an advantage in facilitating the recovery of postoperative gastrointestinal function. Opioids have the potential to inhibit gastrointestinal motility and cause opioid-induced constipation (OIC).24 The intestinal intermuscular plexus and submucosal plexus contain a significant number of peripheral μ-receptors. The activation of these receptors by opioids can delay gastric emptying and slow down the movement of food in the intestinal tract. And opioids can also cause anal sphincter dysfunction, which hinders the defecatory reflex.26,27 On the other hand, the pain relieved by the ESPB reduces the stress response. Therefore, we propose that bilateral ESPB can promote postoperative gastrointestinal function recovery by providing optimal analgesia and reducing opioid use.6,28–30 There were no significant differences in the postoperative 48 h VAS scores or the rescue analgesic within 48 hours among the three groups. This lack of difference may be related to the time it takes for the ESPB to subside.30
Inflammatory process also plays an essential role in the developing of POGD.31 However, no statistical differences were found among the three groups in this study for postoperative inflammatory mediators such as white blood cell (WBC) count, neutrophil-to-lymphocyte count ratio (NLR), and C-reactive protein (CRP). Sympathetic activation can lead to the release of endogenous catecholamines, causing an increase in neutrophils and a decrease in lymphocytes, so NLR is often used as a judge of early stress and inflammation levels.32 Additionally, CRP is a pro-inflammatory mediator that is released early in response to stress. Zheng et al14 found that 2- level of bilateral ESPB reduced stress and postoperative inflammatory mediators, such as CRP, in patients undergoing lumbar spine surgery. The disparity between the findings of this study and those of previous studies may be attributed to the fact that the patients selected for this study had traumatic lumbar spine fractures, which may be combined with fractures other than those of the spine, and the trauma of the fracture itself can increase the stress response of the organism.8 On the other hand, the inflammation of the patient was related to the patient’s use of antibiotics, the magnitude of the trauma of the operation, and infection control, and many other factors, and this study did not control for these confounding factors. In addition, this study was a retrospective study and only routine hematological indicators already present in the cases could be used, while WBC, NLR, and CRP lacked specificity as mediators of inflammation for assessing gastrointestinal function. ESPB did not reduce the hospital length of stay after operation in this study, the possible reasons for this may be that the patients collected were from different supervising physicians, and the differences in the standard of postoperative management and the combination of treatment modalities such as gastrointestinal medications and enema made an impact on the length of hospitalization.
We do acknowledge the limitations of this study. This is a retrospective study, limited to the analysis of available case data. Representative indicators of gastrointestinal inflammation and hormone levels were not obtained for analysis. As only bilateral ESPB at the L3 and T12 levels are currently performed at our institution, the optimal level of block and the concentration of the blocking drug need to be confirmed in prospective randomized controlled. Intra-operative intra-abdominal pressure was not measured in this study to control for the effect of pressure on the abdomen caused by different operators, which may have influenced the study results.
Conclusion
In conclusion, ultrasound-guided bilateral erector spinae block can reduce the incidence of gastrointestinal dysfunction after traumatic lumbar fracture surgery, promote the recovery of gastrointestinal function, and reduce the use of opioids while providing analgesic effects. The ESPB at T12 level was found to help recover postoperative gastrointestinal function more than L3 level. However, further large-sample prospective studies are needed to confirm these findings.
Ethics Approval and Informed Consent
The study was approved by the medical ethics review committee of the he Third Hospital of Hebei Medical University (protocol code: Ke 2023-046-1, date of approval: 1 September 2023). Due to anonymous, retrospective nature of the data collection, the requirement for informed consent was waived. All data collected for this study were anonymized, and patient information was maintained in strict confidence. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 helsinki declaration and its later amendments or comparable ethical standards.
Consent for Publication
All authors contributed to the intellectual content of this manuscript and read and approved the final manuscript.
Acknowledgments
We express our gratitude to department of trauma emergency surgery and the department of spine surgery from The Third Hospital of Hebei Medical University. Furthermore, we appreciate all the anonymous patients who participated in our study.
Funding
This study was approved by the Institutional Review Board at our institution and was not supported by any external sources of funding.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Mandl LA, Sasaki M, Yang J, Choi S, Cummings K, Goodman SM. Incidence and risk of severe ileus after orthopedic surgery: a case-control study. HSS Journal ®. 2020;16(S2):272–279. doi:10.1007/s11420-019-09712-z
2. Mazzotta E, Villalobos-Hernandez EC, Fiorda-Diaz J, Harzman A, Christofi FL. Postoperative ileus and postoperative gastrointestinal tract dysfunction: pathogenic mechanisms and novel treatment strategies beyond colorectal enhanced recovery after surgery protocols. Front Pharmacol. 2020;11:583422. doi:10.3389/fphar.2020.583422
3. Fineberg SJ, Nandyala SV, Kurd MF, et al. Incidence and risk factors for postoperative ileus following anterior, posterior, and circumferential lumbar fusion. Spine J. 2014;14(8):1680–1685. doi:10.1016/j.spinee.2013.10.015
4. Deng WW, Lan M, Peng AF, et al. The risk factors for postoperative ileus following posterior thoraco-lumbar spinal fusion surgery. Clin Neurol Neurosurg. 2019;184:105411. doi:10.1016/j.clineuro.2019.105411
5. Kim MJ, Min GE, Yoo KH, Chang SG, Jeon SH. Risk factors for postoperative ileus after urologic laparoscopic surgery. J Korean Surg Soc. 2011;80(6):384. doi:10.4174/jkss.2011.80.6.384
6. Hendrickson NR, Zhang Y, Amoafo L, et al. Risk factors for postoperative ileus in patients undergoing spine surgery. Global Spine J. 2022:219256822210750. doi:10.1177/21925682221075056
7. Chen M, Wu D, Chen F, Li J, Wu J, Shangguan W. Intravenous lidocaine simultaneously infused with sufentanil to accelerate gastrointestinal function recovery in patients after thoracolumbar surgery: a prospective, randomized, double-blind controlled study. Eur Spine J. 2023;32(1):313–320. doi:10.1007/s00586-022-07456-9
8. Meng S, Fan M, Qian J, et al. An innovative model of
9. Peng K. Ultrasound-guided stellate ganglion block improves gastrointestinal function after thoracolumbar spinal surgery. Clin Ther.
10. Li M, Wang T, Xiao W, Zhao L, Yao D. Low-dose dexmedetomidine accelerates gastrointestinal function recovery in patients undergoing lumbar spinal fusion. Front Pharmacol. 2019;10:1509. doi:10.3389/fphar.2019.01509
11. Zhang Q, Wu Y, Ren F, Zhang X, Feng Y. Bilateral ultrasound-guided erector spinae plane block in patients undergoing lumbar spinal fusion: a randomized controlled trial. J Clin Anesth. 2021;68:110090. doi:10.1016/j.jclinane.2020.110090
12. Oh SK, Lim BG, Won YJ, Lee DK, Kim SS. Analgesic efficacy of erector spinae plane block in lumbar spine surgery: a systematic review and meta-analysis. J Clin Anesth. 2022;78:110647. doi:10.1016/j.jclinane.2022.110647
13. Cai J, Wang Y, Guo Z, et al. Erector spinae plane block ameliorates acute gastrointestinal injury. Intensive Care Med. 2023;49(3):357–359. doi:10.1007/s00134-023-06995-z
14. Zheng S, Xu L, Zhou Y, et al. General anesthesia combined with bilateral 2-level erector spinae plane block may accelerate postoperative gastrointestinal function recovery and rehabilitation process in patients undergoing posterior lumbar surgery: a randomized controlled trial. Surgery. 2023;174(3):647–653. doi:10.1016/j.surg.2023.05.032
15. Innervation of the Gastrointestinal Tract.pdf.
16. Zhang JF, Zhang WW, Wang J, Guo H, Wang T. Distribution of the T12 erector spinal muscle plane block in the dorsal region guided by ultrasound. J Orthop Surg Res. 2021;16(1):48. doi:10.1186/s13018-020-02195-3
17. Cai Q, Qing LG, Sheng HL, et al. Effects of erector spinae plane block on postoperative pain and side-effects in adult patients underwent surgery: a systematic review and meta-analysis of randomized controlled trials. Int j Surg. 2020;80:107–116. doi:10.1016/j.ijsu.2020.05.038
18. Aponte A, Sala-Blanch X, Prats-Galino A, Masdeu J, Moreno LA, Sermeus LA. Anatomical evaluation of the extent of spread in the erector spinae plane block: a cadaveric study. Can J Anaesth. 2019;66(8):886–893. doi:10.1007/s12630-019-01399-4
19. Saadawi M, Layera S, Aliste J, Bravo D, Leurcharusmee P, Tran DQ. Erector spinae plane block: a narrative review with systematic analysis of the evidence pertaining to clinical indications and alternative truncal blocks. J Clin Anesth. 2021;68:110063. doi:10.1016/j.jclinane.2020.110063
20. Altıparmak B, Korkmaz Toker M, Uysal AI, Kuşçu Y, Gümüş Demirbilek S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: randomized, controlled trial. J Clin Anesth. 2019;57:31–36. doi:10.1016/j.jclinane.2019.03.012
21. Viderman D, Aubakirova M, Abdildin YG. Erector spinae plane block in abdominal surgery: a meta-analysis. Front Med. 2022;9:812531. doi:10.3389/fmed.2022.812531
22. Kamel AAF. Bilateral ultrasound-guided erector spinae plane block versus transversus abdominis plane block on postoperative analgesia after total abdominal hysterectomy. Pain Phys. 2020;23:375–382. doi:10.36076/ppj.2020/23/375
23. Schwartzmann A, Peng P, Maciel MA, Forero M. Mechanism of the erector spinae plane block: insights from a magnetic resonance imaging study. Can J Anaesth. 2018;65(10):1165–1166. doi:10.1007/s12630-018-1187-y
24. Bahk JH, Kim YH, Park HY, Min HK, Kim SI, Ha KY. Incidence and risk factors of gastrointestinal and hepatobiliary complications after spinal fusion surgery: a retrospective cohort study. J Korean Med Sci. 2020;35(40):e345. doi:10.3346/jkms.2020.35.e345
25. Mistry T, Chaudhari NP, Sekar C, Senthilkumar B. Ultrasound-guided low thoracic erector spinae plane block for perioperative analgesia in an elderly patient undergoing emergency lumbar spine surgery. J Clin Anesth. 2021;71:110202. doi:10.1016/j.jclinane.2021.110202
26. Guay J, Nishimori M, Kopp SL. Epidural local anesthetics versus opioid-based analgesic regimens for Postoperative gastrointestinal paralysis, vomiting, and pain after abdominal surgery: a Cochrane review. Cochrane Database Syst Rev 2016;123(6).
27. Dunn LK, Thiele RH, Lin MC, et al. The impact of alvimopan on return of bowel function after major spine surgery – a Prospective, randomized, double-blind study. Neurosurgery. 2019;85(2):E233–E239. doi:10.1093/neuros/nyz005
28. Lin H, Guan J, Luo S, Chen S, Jiang J. Bilateral erector spinae plane block for quality of recovery following posterior lumbar interbody fusion: a randomized controlled trial. Pain Ther. 2022;11(3):861–871. doi:10.1007/s40122-022-00395-9
29. Changes of opioid consumption after lumbar fusion using ultrasound-guided lumbar erector spinae plane block: a randomized controlled trial. Pain Phys. 2021;E161–E168. doi:10.36076/ppj.2021.24.E161-E168
30. Yayik AM, Cesur S, Ozturk F, et al. Postoperative analgesic efficacy of the ultrasound-guided erector spinae plane block in patients undergoing lumbar spinal decompression surgery: a randomized controlled study. World Neurosurg. 2019;126:e779–e785. doi:10.1016/j.wneu.2019.02.149
31. Stakenborg N, Wolthuis AM, Gomez-Pinilla PJ, et al. Abdominal vagus nerve stimulation as a new therapeutic approach to prevent postoperative ileus. Neurogastroenterol Motil. 2017;29(9):e13075. doi:10.1111/nmo.13075
32. Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune SYSTEM and diseases. Int J mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.