")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Fentanyl on Remimazolam-Induced Sedation in Female Patients Undergoing Hysteroscopic Surgery: A Randomized Controlled Trial
Authors Huang XD, Xu L, Zheng CH, Chen MM, Shou HY, Zhou ZF
Received 15 November 2024
Accepted for publication 21 February 2025
Published 27 February 2025 Volume 2025:19 Pages 1393—1401
DOI https://doi.org/10.2147/DDDT.S504189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Xiao-Dong Huang,1 Lan Xu,2 Cai-Hong Zheng,1 Min-Min Chen,1 Hong-Yan Shou,1 Zhen-Feng Zhou1
1Department of Anesthesiology, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital, Hangzhou First People’s Hospital Qianjiang New City Campus, Zhejiang Chinese Medical University), Hangzhou, 310008, People’s Republic of China; 2Department of Anesthesiology, Affiliated Xiaoshan Hospital, Hangzhou Normal University, Hangzhou, 311202, People’s Republic of China
Correspondence: Zhen-Feng Zhou, Department of Anesthesiology, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital, Hangzhou First People’s Hospital Qianjiang New City Campus, Zhejiang Chinese Medical University), Hangzhou, 310008, People’s Republic of China, Email [email protected]
Purpose: Previous studies have reported the recommended dosage of remimazolam alone for achieving loss of consciousness (LoC). However, the effect of analgesics on the dosage of remimazolam for successful sedation remains unclear. This study evaluated the impact of fentanyl on the effective dose of remimazolam-induced sedation in female patients undergoing elective hysteroscopic surgery.
Patients and Methods: Two hundred female patients were randomly allocated into two groups, receiving with or without fentanyl (1ug/kg) during anesthetic induction. Within each group, patients were randomized to receive one of four doses (0.1, 0.2, 0.3, and 0.4 mg/kg) of remimazolam for sedation. Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) was evaluated during anesthetic induction. Success was defined when the patient did not respond to painful trapezius squeeze and no requirement for rescue doses. Estimate of ED50 and ED95 with 95% confidence interval (CI) was performed by probit regression.
Results: The ED50 and ED95 values of remimazolam for patients receiving fentanyl (1 ug/kg) were 0.097 (95% CI, 0.072– 0.120) mg/kg and 0.254 (95% CI, 0.203– 0.345) mg/kg, respectively. For patients not receiving fentanyl, the ED50 and ED95 values of remimazolam were 0.181 (95% CI, 0.149– 0.215) mg/kg and 0.475 (95% CI, 0.377– 0.687) mg/kg, respectively. The estimated relative median potency of remimazolam in patients, with and without fentanyl administration, was determined to be 0.534 (95% CI, 0.327– 0.737).
Conclusion: The administration of fentanyl reduced the effective dose of remimazolam-induced sedation by 50% in female patients undergoing elective hysteroscopic surgery. The recommended ED95 dose for remimazolam-induced sedation was 0.254 mg/kg under the condition of this study.
Trial Number and Registry Url: ChiCTR2400079842; https://www.chictr.org.cn/showproj.html?proj=216480: HUANG, Date of registration: January 15, 2024.
Keywords: remimazolam, fentanyl, effective dose, sedation, side effect
Introduction
The utilization of hysteroscopy for precise and standardized diagnosis and treatment of uterine cavity diseases is currently widely prevalent worldwide.1,2 It offers a brief duration, minimal invasiveness, and rapid turnover. Consequently, day hysteroscopic surgery is characterized by its simplicity and accessibility; however, it also necessitates higher safety and efficiency standards for anesthetic drugs.3 Therefore, the utilization of short-acting anesthetics with appropriate drug combinations and doses is highly valued in outpatient hysteroscopic surgery due to their rapid onset of action and facilitation of prompt postoperative recovery.4
Remimazolam, a relatively novel ultrashort-acting benzodiazepine medication, is increasingly prevalent in the field of general anesthesia for minor operation, such as colonoscopies and bronchoscopies,5–7 due to its non-accumulative properties in the body and independence from hepatic or renal function for metabolism.8 The safety profile of remimazolam has been consistently demonstrated in various populations, including healthy individuals, patients with ASA grade III, and elderly patients.7,9 For dose guiding purpose, Chae et al conducted a study to investigate the optimal dosage and safety of intravenous bolus administration and found that the doses required for achieving loss of consciousness (LoC) were 0.11 mg kg−1 (ED50) and 0.14 mg kg−1 (ED95), whereas the doses associated with respiratory depression were determined as 0.19 mg kg−1 (ED50) and 0.27 mg kg−1 (ED95).10
For elderly patients, a recent study proposed that the median effective dose (ED50) and 95% effective dose (ED95) of remimazolam for anesthesia induction were 0.061–0.088 mg/kg and 0.090–0.118 mg/kg, respectively, based on the MOAA/S score.11 However, the generalizability of these study findings in clinical practice was limited due to the widespread use of low-dose analgesics combined with sedatives for daily anesthesia in many institutions. Studies have shown analgesics may potentially reduce the necessary dosage of other sedatives for achieving LoC.12,13 Our recent study14 found that combined 1 µg/kg of fentanyl significantly decreased the required sedative dose of remimazolam by approximately 30% during induction in elderly patients. However, the dose-response may vary from patient age, therefore, the aim of this study was to investigate the effect of fentanyl on remimazolam-induced sedation in non-elderly female patients undergoing hysteroscopic surgery. Our hypothesis was that fentanyl would decrease the required dose of remimazolam for inducing loss of consciousness.
Materials and Methods
Study Design
This single-center, double-blind, prospective, randomized controlled trial was conducted from February 01, 2024 to March 31, 2024 after obtaining approval from the Ethics Committee of Hangzhou Women’s Hospital (IRB: 2023A-155). This study was conducted in accordance with the principles of the Declaration of Helsinki. Prior to enrolling parturients, we registered this clinical trial with the Chinese Clinical Trial Registry (ChiCTR2400079842; https://www.chictr.org.cn/showproj.html?proj=216480). The principal investigator is XD. Huang and the registration date was January 15, 2024. The written consent of all participants in this study has been duly obtained following comprehensive information disclosure. The inclusive criteria were as follows: (1) Patients aged 18–60 years undergoing elective hysteroscopic surgery; (2) American Society of Anesthesiologists (ASA) class I–II; (3) Body mass index (BMI) between 18 and 30 kg/m2. The exclusive criteria included: (1) Allergy to remimazolam or contraindication to its use; (2) Preoperative impaired consciousness or chronic pain managed with long-term analgesic use, psychiatric medications, or alcohol abuse; (3) Utilization of sedatives, antiemetics, anti-itch medications, or monoamine oxidase inhibitors, or antidepressants within 24 hours prior to the surgery.
Randomization and Blinding
The randomization process was performed by an independent researcher, who was not involved the following procedure, utilizing computer-generated random-number software (Microsoft Excel, Redmond, Washington). Then, the contents were carefully concealed and maintained unbiased throughout the study by placing them in consecutively numbered envelopes with opaque coverings. Subsequently, upon inclusion of each participant, a corresponding envelope was unveiled. A total of 200 patients were randomly allocated into two groups (Group FR and Group R) receiving with or without fentanyl (1μg/kg) during anesthetic induction. Within each group, patients were randomized to receive one of four doses (Group FR1-FR4 and Group R1-R4) to receive remimazolam at doses of 0.1, 0.2, 0.3, and 0.4 mg/kg with or without fentanyl; each group comprised of 25 female participants.
The study drug was prepared exclusively by a designated anesthesiology assistant, who remained blinded to the patients’ allocation throughout the process. According to the study protocol, fentanyl 0.1 mg or blank saline was diluted into a 10 mL syringe of identical specifications for slow intravenous injection, while remimazolam was diluted into a 20 mL syringe of identical specifications. The anesthesiologist in charge of administering general anesthesia was solely responsible for the induction process and had no involvement in any other aspects of the study. Furthermore, they were intentionally kept unaware of the specific drug being utilized for research purposes. Another independent anesthesiologist, who was not aware of the grouping responsible for data collection, participated in the study. The grouping of patients was not disclosed to any of the participants in all experimental conditions.
Anesthesia Procedure
No sedative premedication was administered on surgery day. On arriving in operating room, a standard monitoring, including non-invasive blood pressure measurement, pulse oximetry and 5-lead electrocardiography, was applied to evaluate patients’ vital signs. We used an 18 G intravenous cannula to establish peripheral venous access by insertion into a vein in the upper limb. The preoxygenation technique was implemented prior to anesthesia induction by administering oxygen for a duration of five minutes through the gentle placement of a mask over the patient’s face.
Patients were randomized to receive one of four remimazolam doses (0.1, 0.2, 0.3, and 0.4 mg/kg) according to the allocation protocol, administered 2 minutes after the administration of fentanyl at a dose of 1 ug/kg or an equivalent volume of saline.
The primary outcome of this study was the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score,15 which ranged from 0 to 5. The Modified Observer’s Assessment of Alertness and Sedation (MOAA/S) score assessed sedation levels as follows: a score of 5 indicated the patient is fully awake and responds promptly to their name; a score of 4 indicated a sluggish response to their name; a score of 3 indicated response after repeated loud calls of their name; a score of 2 indicated response only to gentle shaking or pushing; a score of 1 indicated response only to pain stimulation (trapezius squeeze); and a score of 0 indicated no response to pain stimulation (trapezius squeeze). A “successful sedation” is defined as achieving a sedation level with an MOAA/S score of 0, indicating the absence of response to painful trapezius squeeze within 5 minutes following intravenous administration of remimazolam.11 If the MOAA/S score remained ≥ 1 within the initial 5 minutes following intravenous administration of remimazolam, the sedation was considered unsuccessful, and a rescue dose of propofol (1 mg/kg) was administered, repeated at 3-minute intervals as necessary until achieving a successful sedation status. The anesthesiologists’ assessment determined the subsequent strategy for sedation and analgesia maintenance. Secondary outcomes included remimazolam injection pain, hypotension, respiratory depression and hiccup. The intensity of injection pain was evaluated using a 4-point verbal rating scale, encompassing scores ranging from 0 (absence of pain) to 3 (severe pain). The definition of respiratory depression was established as a respiratory rate below 10 breaths per minute for more than 1 minute and/or a decrease in SpO2 to less than 90%. The respiratory depression observed during anesthesia induction was effectively managed by ensuring airway patency and delivering high-pressure oxygen via a facial mask.8 Hypotension was defined as a systolic blood pressure below 90 mmHg or a reduction of 20% from the baseline, and treated it with a bolus of intravenous phenylephrine (50 μg), repeated if necessary. In cases of bradycardia with a heart rate < 50 beats/min, intravenous administration of 0.5 mg atropine was employed for treatment. Outcome measures and vital signs were recorded both before and at predetermined time intervals following the intravenous administration of remimazolam, specifically at 1 minute (T1), 2 minutes (T2), 3 minutes (T3), 4 minutes (T4), and 5 minutes (T5) post-administration.
Sample Size Calculation
Sample size was determined using the PASS software (version 11; NCSS, LLC, Kaysville, Utah) with the Cochran-Armitage test for trend in proportions. According to our preliminary internal pilot data, the proportions of successful sedation were observed at 0.2, 0.5, 0.6, and 0.8 for patients receiving remimazolam doses of 0.1, 0.2, 0.3, and 0.4 mg/kg respectively. A minimum total sample size of 56 subjects (14 per dosage group) was required to achieve a statistical power of 90% at a significance level of 0.05, using a two-sided Z test with continuity correction, in order to detect a linear trend. To account for potential dropouts (estimated at 20%) and to achieve narrower confidence intervals, a total of 200 subjects were included in the study, with an equal distribution of 100 subjects in each group (25 per dosage group).
Statistical Analysis
The normality of continuous data was assessed using the Kolmogorov–Smirnov test. Continuous variables, which exhibited a normal distribution, such as patients’ demographic data, were presented as means ± SD and analyzed for significance using one-way analysis of variance (ANOVA), with post-Bonferroni tests for pairwise comparisons. Non-normally distributed data, including MOAA/S scores and pain-intensity scores, were presented as medians (interquartile range) and analyzed using the Kruskal–Wallis test, with Dunn’s tests for post hoc pairwise comparisons. The categorical variables were presented as absolute numbers and percentages. Categorical data, such as the incidence of side effects, were analyzed using the Fisher exact test. In case of a significant overall difference among groups, pairwise comparisons were conducted using chi-square tests. The P-trend value was calculated by the chi-square test for trend.
The ED50 and ED95 of remimazolam for inducing loss of consciousness (successful sedation) were estimated using probit regression analysis. The Pearson goodness-of-fit chi-square test was employed to assess the adequacy of the regression model in fitting the data. Statistical analyses were conducted using IBM SPSS Statistics for Windows version 22.0 (IBM Corp, Armonk, NY) and GraphPad Prism version 8.0 (GraphPad Software Inc., San Diego, CA). A p-value < 0.05 (two-sided) was considered statistically significant.
Results
The Consort Flow is shown in Figure 1. A total of 212 patients were initially assessed for eligibility. Among them, eight were excluded due to non-compliance with the inclusion criteria, while four declined participations. Ultimately, a cohort of 200 patients was recruited and included in the final analysis. All included patients had no pre-existing severe hypertension or arrhythmia, there was not significantly different in the demographic data among groups, Table 1.
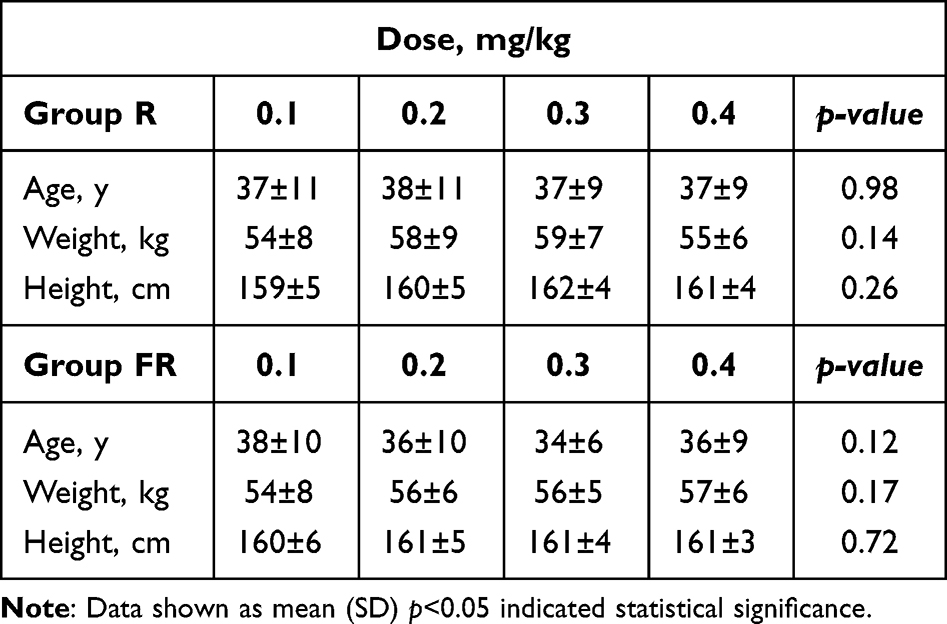 |
Table 1 Patient Characteristics |
 |
Figure 1 CONSORT flow diagram. |
The incidence of successful sedation for different doses of remimazolam is depicted in Figure 2. The ED50 and ED95 values of remimazolam for patients receiving fentanyl were 0.097 (95% CI, 0.072–0.120) mg/kg and 0.254 (95% CI, 0.203–0.345) mg/kg, respectively. For patients not receiving fentanyl, the ED50 and ED95 values of remimazolam were 0.181 (95% CI, 0.149–0.215) mg/kg and 0.475 (95% CI, 0.377–0.687) mg/kg, respectively. The Pearson goodness-of-fit chi-square test demonstrated the model’s adequacy in accurately fitting the observed data (P=0.248). The dose–response curve obtained is illustrated in Figure 3. The estimated relative median potency of remimazolam in patients, with and without fentanyl administration, was determined to be 0.534 (95% CI, 0.327–0.737).
 |
Figure 2 Success rate of remimazolam at different doses. |
 |
Figure 3 Dose–response curves for remimazolam in each group derived from probit analysis using MOAA/S monitoring. Dashed line indicates the position of the estimate of ED95. The ED95 with and without fentanyl, was determined to be 0.254 and 0.475 mg/kg. |
Secondary outcomes were summarized in Table 2 and Table 3. There was no significant difference in the incidence of respiratory depression in patients with or without intravenous administration of fentanyl, (P = 0.059). The incidence of hiccups was significantly higher in the group of patients not receiving fentanyl compared to those receiving fentanyl (P = 0.037). The incidence of hypotension, injection pain or bradycardia did not exhibit any significant differences in the two groups.
 |
Table 2 Side Effects During Induction Period Between Two Groups |
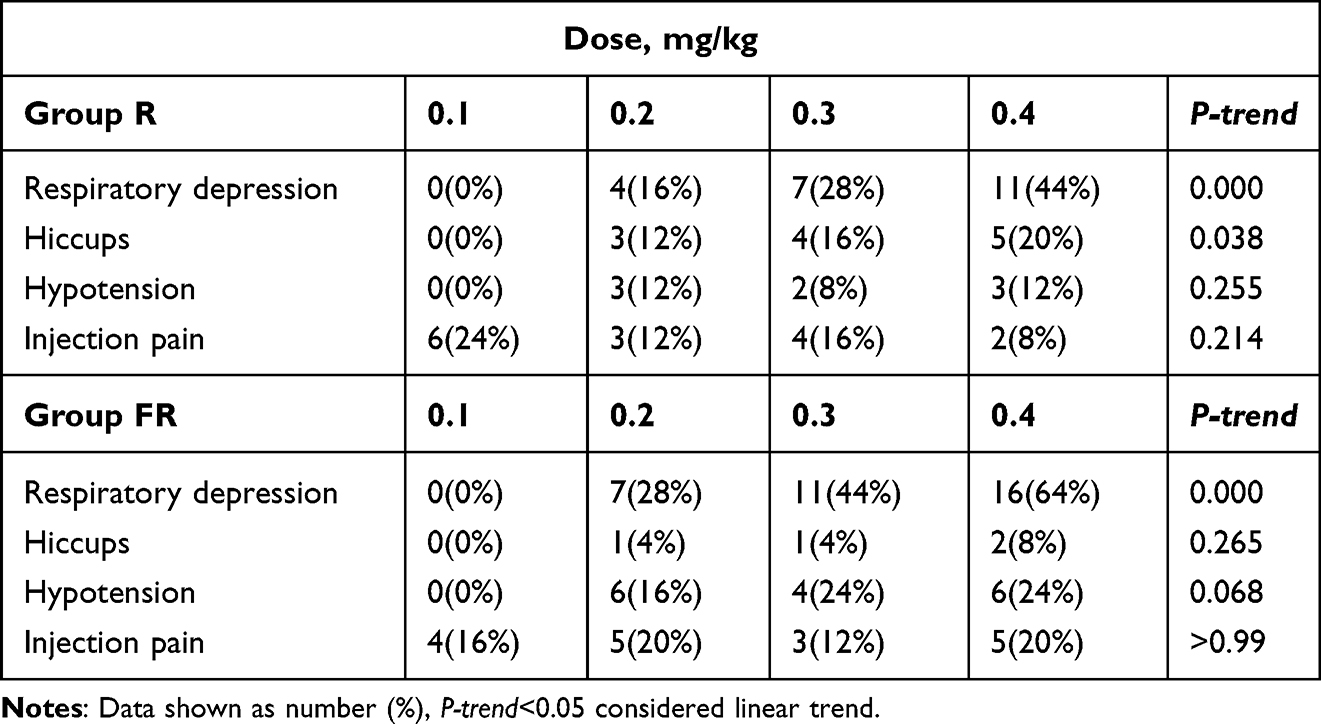 |
Table 3 Trend Comparison of the Incidence of Respiratory Depression, Hiccups, Hypotension, Injection Pain Among the Four Dose Groups |
The incremental dose of remimazolam use was related with an increased risk of respiratory depression; there was a trend toward higher risk with increasing dose of use (two groups, both P-trend = 0.000) in Table 3. In Group R, the incidence of hiccups increased linearly with dosage. Nevertheless, there was no linear-by-linear correlation with remimazolam dose in Group FR while fentanyl was present. The incidence of hypotension or injection pain did not exhibit linear association with remimazolam dose among the four groups.
Discussion
In the current dose-finding study, the effective doses (ED50 and ED95) of intravenous remimazolam for inducing loss of consciousness were determined to be 0.097 and 0.254 mg/kg when administered with fentanyl, respectively; whereas without fentanyl, the corresponding doses were found to be 0.181 and 0.475 mg/kg. Our findings suggest a lower dosage requirement of intravenous remimazolam in combination with 1 μg/kg of intravenous fentanyl for achieving loss of consciousness. In addition, the combination of remimazolam and fentanyl during anesthesia induction was found to significantly reduce the incidence of hiccups compared to the use of remimazolam alone.
Our recent study14 demonstrated that administering 1 µg/kg of fentanyl significantly decreased the required sedative dose of remimazolam by approximately 30% during induction in elderly patients. Moreover, this fentanyl dosage did not increase the risk of adverse effects such as hypotension, respiratory depression or hiccups. In contrast, the present study observed that fentanyl reduced the effective dose of remimazolam by about 50% in female patients undergoing elective hysteroscopic surgery. Additionally, this combination reduced the incidence of hiccups during remimazolam-induced sedation. The key differences between these findings and those of our previous study likely stem from patient age. While our previous study involved patients aged 65–80 years, the current study focused on patients aged 18–60 years. Furthermore, the experimental design differed; the previous study employed an up-down sequential method, whereas our study utilized a randomized approach, with patients assigned to two groups and further subdivided into four remimazolam dosage subgroups, resulting in a nested grouping strategy.
The optimal initial loading dose for inducing loss of consciousness during anesthesia induction remains a subject of ongoing debate in the literature. Chae et al10 conducted a study to evaluate the efficacy and safety of intravenous bolus remimazolam for anesthesia induction, and recommended optimal doses of 0.25–0.33 mg/kg, 0.19–0.25 mg/kg, and 0.14–0.19 mg/kg for patients aged under 40 years, between 60–80 years old, and over 80 years old respectively based on age-specific estimated ED95 values. In a recent study by Tan et al,16 a dose-response investigation was conducted to evaluate the efficacy of remimazolam for intravenous sedation during day-surgery hysteroscopy in patients aged 20–45 years. He study findings revealed that when combined with sufentanil 0.1µg/kg, the ED50 and ED95 values of remimazolam were determined as 0.09 (0.08−0.11) mg/kg and 0.21 (0.16–0.35) mg/kg, respectively, which is significantly lower than the results reported by Chae et al, suggesting a reduced requirement of remimazolam when co-administered with opioids for inducing loss of consciousness. In this study, probit regression was employed to determine and compare the ED50 and ED95 of remimazolam for sedation with or without fentanyl administration. Our findings provide direct evidence supporting the ability of opioids to reduce remimazolam consumption for sedation.
While studies have proposed an optimal initial bolus dose for sedation, it is imperative to acknowledge the potential inter-individual variability in responses to remimazolam. The different response of side effects observed among individuals exposed to this drug serves as a pertinent illustration of such individual responsiveness. Therefore, in this study, we have not only provided the ED50 value as the minimum effective dose and the ED95 as an initial loading dose but also presented a comprehensive dose-response curve to offer clinical practitioners with extensive information for reference. What have to interpret is that the inconsistent recommended dose can be attributed to variations in individual physiological responses to the drug, divergent definitions of successful sedation, diverse statistical methodologies employed, and different combinations of drugs among studies. For a comprehensive overview of the distinctions between our study and similar ones, we have provided a summary in Supplemental Appendix1.
Given its recent introduction into clinical practice, healthcare providers should remain vigilant regarding the potential adverse effects associated with remimazolam, especially with large dose. In this study, we observed a dose-dependent respiratory depression of remimazolam in the induction of loss of consciousness (LoC), particularly when administered with fentanyl at a dosage of 1 µg/kg. Hiccups is a common side effect of intravenous remimazolam.16,17 However, the mechanisms for drug-induced hiccups are still unknown.18 Interestingly, our findings demonstrate a reduction in the incidence of hiccups upon fentanyl administration, suggesting that fentanyl’s mechanism of action involves potentiation of GABA-mediated central inhibitory effects, thereby attenuating the release of excitatory neurotransmitters within the central nervous system. The interactive effects of opioids and remimazolam remain to be elucidated. The potential interactions between opioids and remimazolam necessitate further investigation, aiming to optimize their compatibility and strike a delicate balance between therapeutic efficacy and adverse effects.
Although no patients experienced cough during the injection of fentanyl or saline prior to remimazolam administration, we designed the protocol with patients allocated into different dose subgroups to further ensure the implementation of a double-blind approach. Therefore, we believe the shortcomings in blinding of the coughing associated with fentanyl would not have significantly impacted the results of our study due to the double methods mentioned above. Although no additional side effects were observed when fentanyl was added to remimazolam in this study, it is important to acknowledge that respiratory depression remains an inherent risk associated with fentanyl administration, particularly in elderly patients and young children. Therefore, this consideration should be taken into account when selecting drug combinations for clinical use.
Limitations
Several limitations of this study must be acknowledged. First, the recruitment of patients was based on strict inclusion and exclusion criteria, which limits the generalizability of the findings, particularly for patients with comorbid conditions. Future research should explore the use of remimazolam in individuals with specific risk factors, such as ASA III–IV status, obesity, and advanced age. Second, this study focused exclusively on the induction phase, and further investigations are necessary to assess its application during the intraoperative maintenance phase.
Conclusions
The administration of fentanyl resulted in a significant 50% reduction in the effective dose of remimazolam-induced sedation among female patients undergoing elective hysteroscopic surgery. The recommended ED95 dose for remimazolam-induced sedation was 0.254 mg/kg under the condition of this study.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding author if reasonable.
Ethics Approval and Consent to Participate
This study was approved by The Ethics Committee of Hangzhou Women’s Hospital (IRB: 2023A-155) and written informed consent was obtained from all subjects participating in the study.
Funding
This work was supported by Medical Empowerment and Talent Development Plan of Medical Empowerment Public Welfare Special Fund, Chinese Red Cross Foundation (2022-468).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fagioli R, Vitagliano A, Carugno J, Castellano G, De Angelis MC, Di Spiezio Sardo A. Hysteroscopy in postmenopause: from diagnosis to the management of intrauterine pathologies. Climacteric. 2020;23(4):360–368. doi:10.1080/13697137.2020.1754387
2. Neveu ME, Debras E, Niro J, Fernandez H, Panel P. Standardizing hysteroscopy teaching: development of a curriculum using the Delphi method. Surg Endosc. 2017;31(12):5389–5398. doi:10.1007/s00464-017-5620-z
3. Clark TJ. Virtual pain relief for outpatient hysteroscopy. BJOG. 2021;128(1):96. doi:10.1111/1471-0528.16391
4. Ma T, Readman E, Hicks L, et al. Response to Outpatient hysteroscopy. Aust N Z J Obstet Gynaecol. 2017;57(5):E10. doi:10.1111/ajo.12663
5. Pambianco DJ, Borkett KM, Riff DS, et al. A phase IIb study comparing the safety and efficacy of remimazolam and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2016;83(5):984–992. doi:10.1016/j.gie.2015.08.062
6. Pastis NJ, Yarmus LB, Schippers F, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155(1):137–146. doi:10.1016/j.chest.2018.09.015
7. Liu X, Ding B, Shi F, et al. The efficacy and safety of remimazolam tosilate versus etomidate-propofol in elderly outpatients undergoing colonoscopy: a prospective, randomized, single-blind, non-inferiority trial. Drug Des Devel Ther. 2021;15:4675–4685. doi:10.2147/DDDT.S339535
8. Lu Z, Zhou N, Li Y, Yang L, Hao W. Up-down determination of the 90% effective dose (ED90) of remimazolam besylate for anesthesia induction. Ann Palliat Med. 2022;11(2):568–573. doi:10.21037/apm-22-89
9. Zhang X, Li S, Liu J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: single-centre randomized controlled trial. BMC Anesthesiol. 2021;21(1):156. doi:10.1186/s12871-021-01373-y
10. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesth. 2022;129(1):49–57. doi:10.1016/j.bja.2022.02.040
11. Liu M, Sun Y, Zhou L, Feng K, Wang T, Feng X. The median effective dose and bispectral index of remimazolam tosilate for anesthesia induction in elderly patients: an up-and-down sequential allocation trial. Clin Interv Aging. 2022;17:837–843. doi:10.2147/CIA.S364222
12. Smith C, McEwan AI, Jhaveri R, et al. The interaction of fentanyl on the Cp50 of propofol for loss of consciousness and skin incision. Anesthesiology. 1994;81(4):820–26A. doi:10.1097/00000542-199410000-00008
13. Kazama T, Ikeda K, Morita K. Reduction by fentanyl of the Cp50 values of propofol and hemodynamic responses to various noxious stimuli. Anesthesiology. 1997;87(2):213–227. doi:10.1097/00000542-199708000-00007
14. Huang XD, Chen JB, Dong XY, Wang WL, Zhou J, Zhou ZF. The impact of fentanyl on the effective dose of remimazolam-induced sedation in elderly female patients: an up-and-down sequential allocation trial. Drug Des Devel Ther. 2024;18:3729–3737. doi:10.2147/DDDT.S473662
15. Antonik LJ, Goldwater DR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled Phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part I. Safety, efficacy, and basic pharmacokinetics. Anesth Analg. 2012;115(2):274–283. doi:10.1213/ANE.0b013e31823f0c28
16. Tan H, Lou AF, Wu JE, Chen XZ, Qian XW. Determination of the 50% and 95% effective dose of remimazolam combined with propofol for intravenous sedation during day-surgery hysteroscopy. Drug Des Devel Ther. 2023;17:1753–1761. doi:10.2147/DDDT.S406514
17. Huang Q, Zou Y, Kong G. Hiccup, a neglected side-effect of remimazolam bolus? Minerva Anestesiol. 2022;88(3):193–194. doi:10.23736/S0375-9393.21.16086-9
18. Liu CC, Lu CY, Changchien CF, Liu PH, Perng DS. Sedation-associated hiccups in adults undergoing gastrointestinal endoscopy and colonoscopy. World J Gastroenterol. 2012;18(27):3595–3601. doi:10.3748/wjg.v18.i27.3595
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.