")
Back to Journals » Nature and Science of Sleep » Volume 17
Effect of General Anesthesia Combined with Transversus Abdominis Plane Block on Postoperative Sleep Disorders in Elderly Patients Undergoing Gastrointestinal Tumor Surgery: A Prospective, Randomized Controlled Trial
Authors Pu J, Guo C, Xiao Y, Cao Y, Liu Z, Jin Y, Hu Y
Received 17 July 2024
Accepted for publication 7 December 2024
Published 7 January 2025 Volume 2025:17 Pages 17—25
DOI https://doi.org/10.2147/NSS.S486711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Jie Pu,1 Chendong Guo,1 Yue Xiao,2 Yanan Cao,1 Zhenhua Liu,3 Yuzhong Jin,3 Yimin Hu4
1Department of Anesthesiology, The Second People’s Hospital of Changzhou, Nanjing Medical University, Changzhou, 213003, People’s Republic of China; 2Department of Anesthesiology, Sichuan Cancer Hospital, Chengdu, 100062, People’s Republic of China; 3Changzhou Wujin Hospital of Traditional Chinese Medicine, Changzhou, 213161, People’s Republic of China; 4Department of Anesthesiology, Hospital for Skin Diseases (Institute of Dermatology), Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, 210042, People’s Republic of China
Correspondence: Yimin Hu, Department of Anesthesiology, Hospital for Skin Diseases (Institute of Dermatology), Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, 210042, People’s Republic of China, Tel +86 18951767577, Email [email protected]
Purpose: The aim of this study was to investigate the effect of general anesthesia combined with transversus abdominis plane block on postoperative sleep disorders in elderly patients undergoing gastrointestinal tumor surgery.
Methods: For elderly patients with gastrointestinal malignant tumors, we recruited 94 patients, aged 65– 80, who were scheduled for radical laparoscopic surgery. Using the random number table method, the patients were randomly divided into two groups, the general anesthesia group (group GA) and the general anesthesia combined with transversus abdominis plane block group (group GT). The group GA received the sedation-aspiration complex general anesthesia regimen, while the group GT underwent bilateral transversus abdominis plane blocks (TAPB) after the same induction of anesthesia. Group GA was injected bilaterally with equal amounts of saline in the same way. Sleep was monitored using wearable devices on the first day before surgery (P1) and the first and third day after surgery (D1 and D3). The Pittsburgh Sleep Quality Index(PSQI) scale was used to assess sleepiness and the occurrence of postoperative sleep disorders (POSD) on P1, D1 and D3 nights, respectively.
Results: Compared to the group GA, the group GT showed a significant decrease in remifentanil use during surgery (P< 0.05). At D1, the group GT showed an increase in the ratio of deep sleep to rapid eye movement sleep (REM), along with a significant decrease in the number of wakefulness (P< 0.05). At D3, the proportion of REM continued to increase and PSQI scores were significantly lower at both D1 and D3 (P< 0.05). In addition, the incidence of POSD and the visual analog scores (VAS) at 0.5h and 6h postoperative activity in D1 showed a decreasing trend (P< 0.05). However, no significant differences were observed between the two groups in general condition, intraoperative condition, remedial analgesia and number of analgesic pump presses (P> 0.05).
Conclusion: General anesthesia combined with transversus abdominis plane block reduces the dosage of opioids in abdominal surgery, especially gastrointestinal surgery, alleviates postoperative pain in elderly gastrointestinal oncology patients, improves sleep quality, and reduces the incidence of sleep disorders.
Keywords: transversus abdominis plane block, sleep disorders, elderly, gastrointestinal tumors, Pittsburgh sleep quality index
Introduction
Sleep is an integral part of human life activities and is a physiological phenomenon that is actively produced and regulated by the brain.1,2 With age, the amplitude of circadian oscillations of bodily functions, including sleep, as well as melatonin levels, gradually decreases, and the efficiency of the suprachiasmatic nucleus of the hypothalamus decreases, a situation that can result in altered sleep patterns with age, which in the elderly population manifests itself in the following ways Increased percentage of light sleep time (N1 and N2), sleep fragmentation, and forward phase shift of circadian rhythms, etc. Also opioids, depression, chronic pain, and neurodegenerative changes can lead to predisposition to sleep disorders in elderly patients.3,4 POSD is a common clinical phenomenon in surgical patients, which manifests itself as an abnormal quality of sleep for at least one day postoperatively or as behavioral abnormalities, such as sleep fragmentation, frequent nocturnal awakenings, difficulty falling asleep, sleep deprivation, early awakening, and sleep rhythm disorders.5,6 Factors triggering POSD are manifold, mainly surgical trauma, pain, use of anaesthetics, age, environmental factors, preoperative comorbidities and type of surgery. Age is an important preoperative factor in perioperative sleep disorders, and its influence is mainly reflected in the changes in sleep structure during aging and the diminished ability to adaptively regulate sleep in response to environmental changes.5 Therefore, based on the special needs and challenges of perioperative management of elderly patients, as well as the high prevalence of postoperative sleep disorders and the statistical significance of their associated complications in this age group, we chose the elderly patient population as the study population.
TAPB is performed by injecting local anesthetic drugs into the fascial space between the transversus abdominis muscle and the internal oblique muscle and blocking the abdominal wall nerves that travel in this plane.7 To achieve analgesia and anesthesia in the abdominal wall region, an ideal block and dosing regimen can produce analgesia for 15–20 hours.
Previous studies have shown that general anesthesia combined with TAPB significantly reduces intraoperative opioid use and improves patient prognosis.8 However, its effectiveness in improving postoperative sleep quality in elderly patients has yet to be thoroughly investigated. In this study, we propose to evaluate the effect of general anesthesia combined with TAPB on patients’ POSD in elderly patients undergoing gastrointestinal oncology surgery, with the aim of providing a valuable reference basis for clinical anesthesia.
Methods
Study Design and Participants
This single-center, prospective, double-blind, randomized controlled trial was formally approved by the Medical Ethics Committee of the Second People’s Hospital of Changzhou Affiliated to Nanjing Medical University (No. 2023YLJSA030), and registered in the China Clinical Trial Registry (Registration No. ChiCTR2300075329). All patients and their families participating in the study have signed an informed consent form to ensure that each patient and their family fully understand the study and agree to participate in this study.
From August 2023 to March 2024, this study included elderly patients who were to undergo laparoscopic radical surgery for gastrointestinal malignant tumors at the Changzhou Second People’s Hospital affiliated with Nanjing Medical University, with an age range of 65–80 years old, American Society of Anesthesiologists (ASA) classification I to II, body mass index (BMI) of 18–30 kg/m², and no restriction on gender. Patients who met the following criteria were excluded from the study: (1) preoperative PSQI scores higher > 7, (2) sleep apnea syndrome, (3) severe cardiac, cerebral, hepatic, and renal diseases, (4) long-term application of narcotic analgesics or sedatives, (5) patients with history of psychiatric disorders, such as anxiety and depression. During the course of the study, we excluded participants who changed surgical methods, had incomplete follow-up data, withdrew midway, failed or developed complications from TAPB treatment, and were transferred to the ICU after surgery.
Randomization and Blinding
All enrolled patients underwent laparoscopic radical surgery for gastrointestinal malignancies. Patient eligibility was assessed by a two-step screening with final enrollment and randomization. Initial screening, recruitment, final enrollment, and randomization were performed 1 day before surgery. Patients were assigned to either the group GA or the group GT by a computer-generated table of random numbers. Group assignments were sealed in sequentially numbered opaque envelopes. Patients, attending surgeons, data collectors, and individuals performing final statistical analyses were unaware of group assignments.
Anesthetic and Analgesic Techniques
Electrocardiogram (ECG), heart rate (HR), peripheral vascular oxygen saturation (SpO2), blood pressure (BP), and Bispectral index (BIS) were routinely detected on admission, and oxygen denitrification was administered for 3 min (oxygen flow rate of 6 L/min). The peripheral venous access was opened, and 8 mL·kg−1·h−1 of crystalloid or colloid fluid was infused intravenously, and under local anesthesia, the patients’ intraoperative invasive arterial pressure was monitored by radial artery puncture catheterization. Anesthesia was induced in the GA group by the intravenous injection of midazolam 0.03 mg/kg, propofol 1.5–2.5 mg/kg, sufentanil 0.3–0.5 μg/kg, and rocuronium bromide 0.6–1.2 mg/kg, and after successful tracheal intubation, mechanical ventilation was implemented with an oxygen concentration of 60%, a tidal volume of 6–8 mL/kg, and a ventilation rate of 12–16 times/min. The partial pressure of end-expiratory carbon dioxide (PETCO2) was maintained at 35–45 mmHg (1 mmHg = 0.133 kPa). For anesthesia maintenance, propofol and remifentanil were infused by inhalation of sevoflurane and target-controlled infusion, with initial effector compartment concentrations of 3 μg/mL and 4 ng/mL, respectively (adjusted intraoperatively according to the BIS value and hemodynamic dynamics), and myorelaxation was maintained with an intravenous infusion of cisatracurium 0.1 mg·kg−1·h−1. If the patient’s blood pressure dropped more than 20% of the basal value or the systolic blood pressure <90mmHg during the operation, ephedrine 6mg was injected to elevate the blood pressure; if the heart rate was ≤50 beats/min, atropine 0.5mg was injected to increase the heart rate.
Postoperatively, both groups received patient-controlled intravenous analgesia (PCIA), in which we used a mixture of oxycodone (0.8 mg/kg) and tropisetron (6 mg) diluted to 100 mL with saline. PCIA settings included a background dose of 2 mL/h, a single dose of 2 mL, and a lockout duration of 15 minutes. If remedial analgesia was required, 75 mg of diclofenac sodium lidocaine was injected intramuscularly.
Intervening Measure
After anesthesia induction was completed in patients of group GT, they were placed in supine position, and the probe was placed transversely under the raphe to find the paired rectus abdominis muscle images and white lines, followed by panning the probe along the edge of the ribs to the midclavicular line, which clearly showed the triple structure of the external abdominal obliquity, internal abdominal obliquity, and transversus abdominis muscle. Using the in-plane approach, the puncture needle was inserted into the superficial surface of the transversus abdominis muscle below the tendinous membrane of the internal oblique muscle, and after retracting without blood and gas, 30 mL of 0.25% ropivacaine was injected, and the contralateral TAPB was performed in the same way (Figure 1). Group GA was injected bilaterally with equal amounts of saline in the same way.
 |
Figure 1 TAPB ultrasound schematic. The plane of local anesthetic injection is indicated by the arrow in the figure. Abbreviations: OEA, obliquus externus abdominis; OIA, obliquus internus abdominis; TA, Transversus abdominis. |
Clinical Data Collection
Intraoperatively, detailed records of fluid intake, bleeding, urine output, anesthesia time, operation time, anesthesia medication dosage, as well as remedial analgesia and the total number of analgesic pump compressions were recorded for 48 hours after the operation. Sleep parameters, including the percentage of deep sleep, percentage of light sleep, percentage of REM, number of wakefulness, sleep continuity score, and sleep respiratory quality score, were monitored on P1 and D1, D3 nights (8:00 pm to 8:00 am the next day) using a wearable device (wireless smart band Honor 7, Honor Terminal Company Limited). At P1, D1 and D3 follow-up, subjective sleep quality was assessed using the PSQI9 scale, which consists of 7 parts and 18 entries, with a total score ranging from 0 to 21, and the higher the score, the poorer the sleep quality. To screen for nonanxious and depressed patients, 1 day before surgery we assessed using the Hamilton Anxiety Scale (HAMA)10 and the Depression Screening Scale (PHQ-9).11 The same anesthesiologist responsible for PSQI scoring would record the patient’s VAS12 scores at 0.5h after extubation, and at 6h, 12h, and 24h postoperatively in the activity and rest states.
Observation Outcomes
Primary outcome: the incidence of postoperative sleep disorders in the two groups. Secondary outcomes: PSQI scores of P1, D1 and D3; sleep parameters monitored by P1, D1 and D3 using wearable smart bracelets; the situation of VAS scores in the 24h postoperative period; the number of effective presses of analgesic pumps in the 48h postoperative period, and the situation of remedial analgesia in the ward.
Sample Size
In this study, PASS 17.0 software was used to estimate the sample size, and the main outcome was the incidence of POSD in D1. Based on the pre-test, the incidence of POSD in D1 was 64% and 30% in the GA and GT groups, respectively. A two-sided test was set with α=0.05 and 1-β=0.9, and a minimum of 43 patients were required in each group. Considering a 10% dropout rate, the plan was to recruit at least 47 subjects in each group.
Statistical Analysis
SPSS software version 26.0 was used for analysis in this study, and P<0.05 was considered statistically significant. The measurement variables are represented as mean±standard deviation (SD), and countable data are represented by case number or percentage. The t-test of independent samples was used for pairwise comparisons between groups, and the analysis of variance of repeated measurement data was used for intra- and inter-group comparisons at different time points. During data processing, we will eliminate data that are too biased and lack practical significance.
Results
We initially evaluated 102 patients for eligibility to participate in this study, of which 6 patients did not meet the inclusion criteria and 2 patients declined to participate. The remaining 94 patients were enrolled in the study. Subsequently, 1 patient changed the surgical procedure, 1 withdrew midway, 3 were lost to postoperative visits, and 2 were transferred to the ICU; a total of 7 cases were excluded. Finally 87 cases were included in the statistical analysis, 44 cases in the group GA and 43 cases in the group GT (Figure 2).
 |
Figure 2 Flow chart of included population. |
There were no significant differences between the two groups in terms of gender, age, BMI, preoperative anxiety and depression assessment, and type of surgery (P>0.05), as shown in Table 1. In the group GT, we did not observe any record of adverse reactions, including but not limited to infection, hematoma formation, nerve damage, and local anesthetic toxicity, which ensured the safety of the operation.
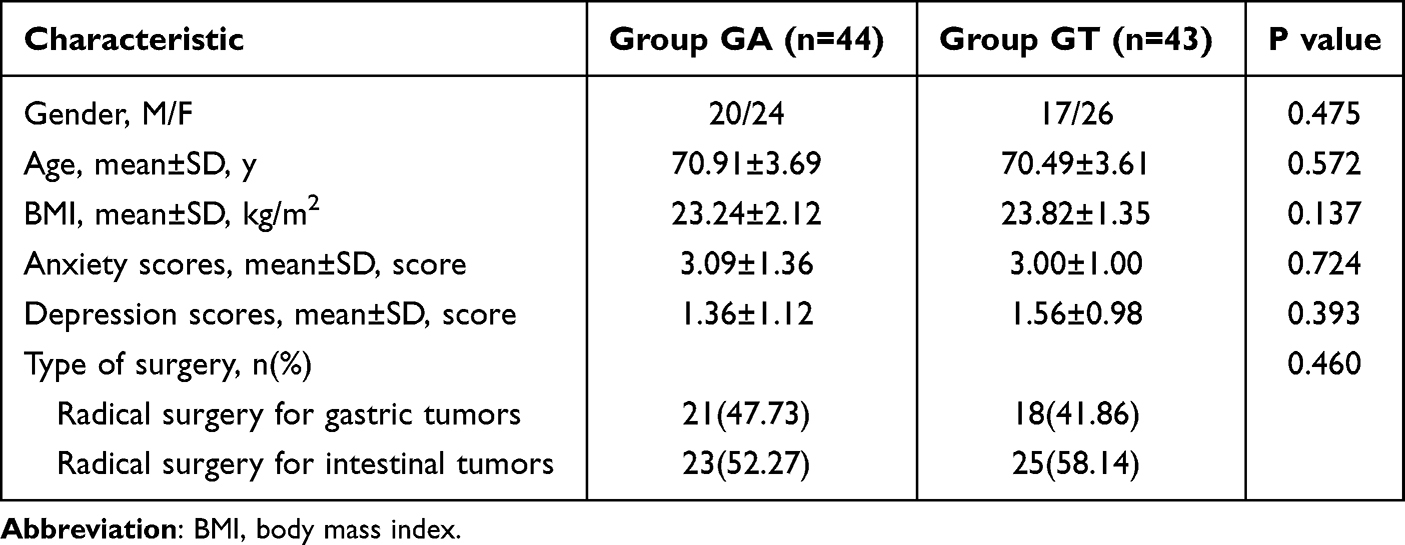 |
Table 1 Patient Baseline Profile Characteristics |
Compared with the group GA, the use of remifentanil during the operation was significantly lower in the group GT (P<0.05). However, there was no significant difference between the two groups in terms of operation time, anesthesia time, propofol, sufentanil and ephedrine dosage, as well as fluid intake, bleeding, urine output, number of analgesic pump presses and remedial analgesic needs (P>0.05) (Table 2).
 |
Table 2 Patient Perioperative Data Characteristics |
In terms of sleep parameters captured by the smart band, compared to the group GA, the proportion of both deep sleep and REM increased in the group GT in D1 (P<0.05), and the number of wakefulness decreased (P<0.05). In D3, the proportion of REM was still higher in the group GT (P<0.05). There was no significant difference between the two groups in each sleep parameter of P1 and the number of wakefulness, sleep continuity and sleep breathing quality scores (P>0.05) (Figure 3).
 |
Figure 3 Sleep parameters captured by the wearable smart band ((a):percentage of deep sleep; (b):percentage of light sleep; (c):percentage of REM; (d):number of wakefulness; (e):sleep continuity score; (f):sleep respiratory quality score). *P<0.05 versus the Group GA. Abbreviations: REM, rapid eye movement; P1, first day before surgery; D1, first day after surgery; D3, third day after surgery. |
The patient’s perioperative PSQI score and incidence of POSD were assessed by a specialized anesthesiologist. Compared with the group GA, the group GT showed a significant decrease in D1 and D3 PSQI scores (P<0.05) and a decrease in the incidence of D1 POSD (P<0.05). There was no significant difference between the two groups in P1 PSQI scores and the incidence of D3 POSD (P>0.05) (Table 3).
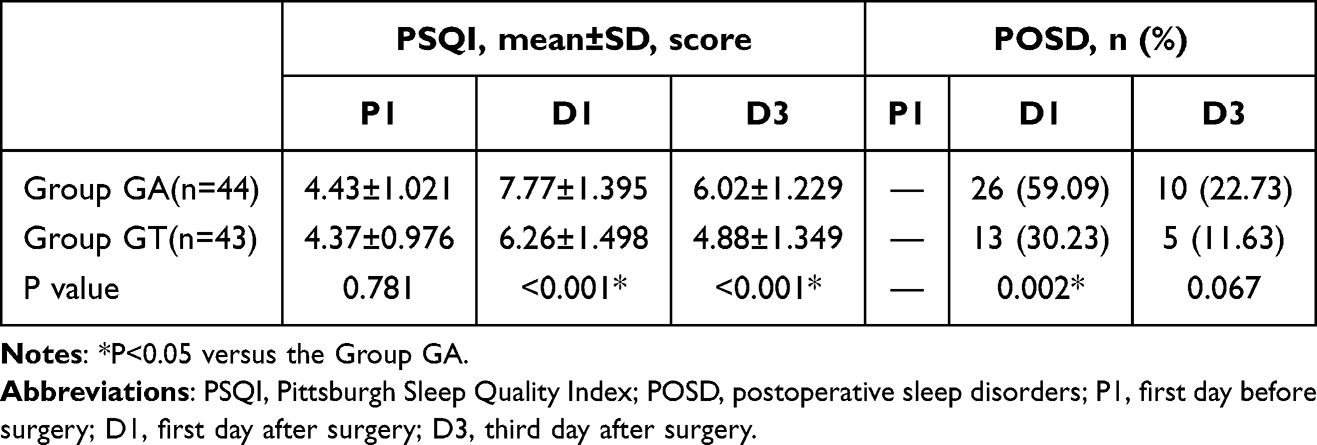 |
Table 3 Patient PSQI Scores and Incidence of POSD |
Comparing the VAS scores of the two groups of patients at each time point during the 24h postoperative period, the VAS scores at 0.5h and 6h postoperative activity were decreased in the group GT (P<0.05), and no significant difference was observed in the VAS scores at 6h and 12h postoperative activity and at rest at all postoperative time points (P>0.05)(Figure 4).
 |
Figure 4 Patients’ activity VAS and rest VAS scores at different postoperative time points. ((a):Score of activity VAS; (b):Score of activity VAS). *P<0.05 versus the Group GA. |
Discussion
Normal human physiological sleep is divided into non-rapid eye movement (NREM) and REM, and the NREM and REM cycles are repeated 4–6 times per night, each lasting 90–100 minutes. NREM is divided into three stages, N1, N2, and N3, which account for 2%-5%, 45%-55%, and 15–20% of the total sleep time, respectively, while REM accounts for 20–25% of the entire total duration of sleep.13,14 High-quality sleep is essential for maintaining normal physical and mental health, and the prevalence of POSD is high in patients undergoing major surgery and in elderly patients.15 POSD can weaken the immune system, increase the risk of cardiovascular disease, and interfere with postoperative recovery, leading to anxiety, depression, postoperative delirium, or prolonged cognitive decompensation.5,15 Studies have found that intraoperative opioids, as well as postoperative pain, can lead to decreased sleep quality after falling asleep, such as shorter sleep duration, reduced sleep efficiency, and reduced sleep depth.16 In addition, it has also been shown that POSD may enhance patients’ pain perception by affecting pain modulation pathways, and that lack of sleep can lower pain thresholds and make patients more sensitive to the perception of pain.17,18 Our study was conducted on patients who underwent laparoscopic radical surgery for gastrointestinal malignant tumors with intraoperative Bilateral TAPB was performed before surgery, and patients’ preoperative and postoperative sleep was carefully evaluated using the PSQI scale and the smart band honor 7. We found that TAPB can improve POSD, reduce the use of opioids, improve patients’ comfort, and has important clinical value in pain management in gastrointestinal oncologic surgery.
Polysomnography is the gold standard for the diagnosis of sleep-related diseases and a commonly used means of sleep monitoring, but its complexity, accessibility, and impact on subject comfort are all shackles to its further development and application. Studies have confirmed that wearable devices can objectively monitor the body’s activity level and sleep, that they are easy to operate, and that they can monitor postoperative sleep in real time and objectively, which can meet the needs of clinical sleep monitoring.19 The smart bracelet Honor 7 used in this study is based on the TruSleepTM sleep monitoring algorithm (TruSeenTM 2.0) with heart rate and motion sensors, which is validated by the University of Bern in Switzerland. With high-precision monitoring capability, it can accurately differentiate between deep sleep, light sleep, REM and awakening states, and its accuracy is as high as 96.3% when benchmarked against professional polysomnography monitors. With a PSQI score of 7, the sensitivity and specificity of assessing sleep disorders were 98.3% and 90.2%, respectively (Kappa=0.89, P<0.01)20, which justifies the subjective assessment of sleep with the PSQI scale. Therefore, in this study, we used the PSQI scale and wearable smart band honor 7 to comprehensively assess the sleep of elderly patients undergoing surgery for gastrointestinal tumors from both subjective and objective aspects.
The results of this study showed that the group GT had a higher proportion of deep sleep and REM and a lower number of wakefulness at D1, a higher proportion of REM at D3, and lower PSQI scores at D1 and D3, in addition to a significantly lower incidence of POSD at D1, which suggests that general anesthesia in combination with a TAPB can effectively improve POSD in elderly patients undergoing surgery for gastrointestinal tumors. In the present study, we demonstrated that intraoperative remifentanil use in the GT group was significantly lower than that in the GA group, probably because TAPB provided additional intraoperative analgesia, patients’ intraoperative pain perception was reduced, and opioid requirements were reduced accordingly. One previous study demonstrated that21 normally, adenosine levels peak during sleep and promote sleep, and that opioids may reduce the pontine reticular formation of the basal forebrain and the anaphase region of the anterior cerebral plexus by either blocking the release of adenosine or by promoting the degradation of adenosine and anaphase regions of the basal forebrain, thereby interfering with sleep. Previous reports have shown that one way in which opioids affect sleep is through μ-opioid receptors on GABAergic neurons located in the ventrolateral prefrontal cortex (VLPO), and that, in isolated brain slices, opioids hyperpolarize the membrane potential in the VLPO and inhibited the firing of these sleep-promoting neurons.22,23 One researcher demonstrated that patients with intraoperative remifentanil had significantly lower quality of sleep, with a 72.3% reduction in REM sleep period, which is consistent with the findings of the present study.24 Therefore, it can be hypothesized in this study that the effect of general anesthesia combined with TAPB to improve POSD in elderly patients undergoing gastrointestinal oncologic surgery may stem from the reduction in intraoperative remifentanil use.
In addition, VAS scores at 0.5h and 6h of postoperative activity were significantly lower in the group GT than in the group GA in this study. Numerous studies found that pain patients experienced longer delays in falling asleep, woke up more often during the night, and had a shorter duration of sleep, lower sleep efficiency, and less deep sleep;25,26 Kapustin and others confirmed that pain patients spent more time and experience more sleep fragmentation, altered NREM sleep, REM sleep and wakefulness periods, and altered delta power during NREM sleep.27,28 Therefore, it can be speculated in this study that the ameliorative effect of TAPB on POSD may also be related to postoperative pain relief in patients.
This study has some limitations because its sample only included patients aged between 65 and 80 years, and further stratification is needed in the future to explore the effects of TAPB on POSD in patients of different ages; secondly, the postoperative follow-up time in this study was only 3 days, which may not fully reflect the long-term effects and complication rates, and prolonging the follow-up time may be more helpful in assessing the effects of general anesthesia combined with transversus abdominis plane block on the patients with sleep disorders and its long-lasting effects; furthermore, this study did not adequately control for other factors that may affect sleep quality, such as postoperative medication use, postoperative complications, noise, light, and turnover in the ward at night, which are potential factors that may affect the accuracy and reliability of the results.
Conclusion
In conclusion, general anesthesia combined with transversus abdominis plane block can reduce the dosage of opioids in abdominal surgery, especially gastrointestinal surgery, alleviate postoperative pain in elderly gastrointestinal tumor patients, improve the quality of sleep, and reduce the incidence of sleep disorders.
Data Sharing Statement
Data supporting the results of this study are available from the corresponding author (Yimin Hu) upon request.
Statement of Ethics
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Medical Ethics Committee of the Second People’s Hospital of Changzhou Affiliated to Nanjing Medical University (No. 2023YLJSA030). All patients and their families have signed an informed consent form.
Acknowledgments
The authors would like to thank the Second People’s Hospital of Changzhou City affiliated with Nanjing Medical University for supporting this study. We would also like to thank the gastrointestinal surgeons for their support of this study. This paper has been uploaded to Research Square as a preprint:https://www.researchsquare.com/article/rs-4806447/v1.
Funding
This study was supported by the Changzhou Municipal Health Commission Science and Technology Project Establishment Project (Major Project) (ZD202315).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown RE, Spratt TJ, Kaplan GB, et al. Translational approaches to influence sleep and arousal. Brain Res Bull. 2022;185:140–161. doi:10.1016/j.brainresbull.2022.05.002
2. Romigi A, Brown RE. Editorial: consequences of sleep deprivation. Front Neurosci. 2023;17:1254248. doi:10.3389/fnins.2023.1254248
3. Mueller C, Nenert R, Catiul C, et al. Relationship between sleep, physical fitness, brain microstructure, and cognition in healthy older adults: a pilot study. Brain Res. 2024;1839:149016. doi:10.1016/j.brainres.2024.149016
4. Gao Y, Zhou Q, Li H, et al. Melanin-concentrating hormone is associated with delayed neurocognitive recovery in older adult patients with preoperative sleep disorders undergoing spinal anesthesia. Anesth Analg. 2024;138(3):579–588. doi:10.1213/ANE.0000000000006768
5. Rampes S, Ma K, Divecha YA, et al. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2019;34(4):271–280. doi:10.7555/JBR.33.20190054
6. Yoshikawa F, Nozaki-Taguchi N, Yamamoto A, et al. Preoperative sleep-disordered breathing and craniofacial abnormalities are risk factors for postoperative sleep-disordered breathing in patients undergoing skin-flap oropharyngeal reconstruction surgery for oral cavity cancer: a prospective case-control study. Sleep Breath. 2024;28(2):797–806. doi:10.1007/s11325-023-02962-6
7. Iaquinandi F, Mongelli F, Christoforidis D, et al. Laparoscopic vs. ultrasound-guided transversus abdominis plane (TAP) block in colorectal surgery: a systematic review and meta-analysis of randomized trials. Surg Endosc. 2024;38(3):1119–1130. doi:10.1007/s00464-023-10658-x
8. Jung J, Jung W, Ko EY, et al. Impact of bilateral subcostal plus lateral transversus abdominis plane block on quality of recovery after laparoscopic cholecystectomy: a randomized placebo-controlled trial. Anesth Analg. 2021;133(6):1624–1632. doi:10.1213/ANE.0000000000005762
9. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
10. Dos Santos ERP, Coelho JCF, Ribeiro I, et al. Translation, cultural adaptation and evaluation of the psychometric properties of the Hamilton Anxiety Scale among a sample of Portuguese adult patients with mental health disorders. BMC Psychiatry. 2023;23(1):520. doi:10.1186/s12888-023-05010-5
11. Kendrick T, Dowrick C, Lewis G, et al. Depression follow-up monitoring with the PHQ-9: an open cluster-randomised controlled trial. Br J Gen Pract. 2024;74(744):e456–e465. doi:10.3399/BJGP.2023.0539
12. Redford E, Heuer S. A visual analog scale for self-reported quality of life: a comparison of VAS and QoL-AD in older adults. Alzheimer Dis Assoc Disord. 2023;37(4):343–348. doi:10.1097/WAD.0000000000000581
13. Leu-Semenescu S, Maranci J-B, Lopez R, et al. Comorbid parasomnias in narcolepsy and idiopathic hypersomnia: more REM than NREM parasomnias. J Clin Sleep Med. 2022;18(5):1355–1364. doi:10.5664/jcsm.9862
14. Mehta R, Bhattacharya R, Mallick BN, et al. Sleep and neuroimmunomodulation for maintenance of optimum brain function: role of noradrenaline. Brain Sci. 2022;12(12):1725. doi:10.3390/brainsci12121725
15. Su X, Wang DX. Improve postoperative sleep: what can we do? Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
16. Gupta CC, Sprajcer M, Johnston-Devin C, et al. Sleep hygiene strategies for individuals with chronic pain: a scoping review. BMJ open. 2023;13(2):e060401. doi:10.1136/bmjopen-2021-060401
17. Stroemel-Scheder C, Kundermann B, Lautenbacher S, et al. The effects of recovery sleep on pain perception: a systematic review. Neurosci Biobehav Rev. 2020;113:408–425. doi:10.1016/j.neubiorev.2020.03.028
18. Stroemel-Scheder C, Lautenbacher S. The effects of recovery sleep on experimental pain. J Pain. 2023;24(3):490–501. doi:10.1016/j.jpain.2022.10.009
19. Burkart S, Beets MW, Armstrong B, et al. Comparison of multichannel and single-channel wrist-based devices with polysomnography to measure sleep in children and adolescents. J Clin Sleep Med. 2021;17(4):645–652. doi:10.5664/jcsm.8980
20. Mollayeva T, Thurairajah P, Burton K, et al. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
21. Eacret D, Veasey SC, Blendy JA, et al. Bidirectional relationship between opioids and disrupted sleep: putative mechanisms. Mol Pharmacol. 2020;98(4):445–453. doi:10.1124/mol.119.119107
22. Zhao Y-N, Yan Y-D, Wang C-Y, et al. The rostromedial tegmental nucleus: anatomical studies and roles in sleep and substance addictions in rats and mice. Nat Sci Sleep. 2020;12:1215–1223. doi:10.2147/NSS.S278026
23. Oishi Y, Lazarus M. The control of sleep and wakefulness by mesolimbic dopamine systems. Neurosci Res. 2017;118:66–73. doi:10.1016/j.neures.2017.04.008
24. Wenk M, Pöpping DM, Chapman G, et al. Long-term quality of sleep after remifentanil-based anaesthesia: a randomized controlled trial. Br J Anaesth. 2013;110(2):250–257. doi:10.1093/bja/aes384
25. Duo L, Yu X, Hu R, et al. Sleep disorders in chronic pain and its neurochemical mechanisms: a narrative review. Front Psychiatry. 2023;14:1157790. doi:10.3389/fpsyt.2023.1157790
26. Miettinen T, Sverloff J, Lappalainen O-P, et al. Sleep problems in pain patients entering tertiary pain care: the role of pain-related anxiety, medication use, self-reported diseases, and sleep disorders. Pain. 2022;163(7):e812–e820. doi:10.1097/j.pain.0000000000002497
27. Kapustin D, Bhatia A, McParland A, et al. Evaluating the impact of gabapentinoids on sleep health in patients with chronic neuropathic pain: a systematic review and meta-analysis. Pain. 2020;161(3):476–490. doi:10.1097/j.pain.00000000000001743
28. Nordstoga AL, Mork PJ, Meisingset I, et al. The joint effect of sleep duration and insomnia symptoms on the risk of recurrent spinal pain: the HUNT study. Sleep Med. 2022;99:11–17. doi:10.1016/j.sleep.2022.07.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Investigation of Sleep Disorders and Related Influencing Factors Among the Elderly in Southeast Coastal Regions of China: A Cross-Sectional Survey Analysis
Chen Y, Su F, Xiang H, Xia J
Clinical Interventions in Aging 2025, 20:171-181
Published Date: 19 February 2025