")
Back to Journals » Nature and Science of Sleep » Volume 16
Effect of General Anesthesia vs Regional Anesthesia on Sleep Disturbance in Elderly Patients After Discharge from the Hospital for 3 Months
Authors Cheng H, Zhou W, Nasuhi VN, Zhu X, Yu C, Zhang H, Wang H
Received 3 July 2024
Accepted for publication 16 October 2024
Published 22 October 2024 Volume 2024:16 Pages 1679—1686
DOI https://doi.org/10.2147/NSS.S483425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Haihong Cheng,1 Wei Zhou,1,* Valeria Nahadi Nasuhi,2,* Xiaoqiang Zhu,1 Chenyuan Yu,1 Hang Zhang,1 Hongwei Wang1
1Department of Anesthesiology, Tongde Hospital Affiliated to Zhejiang Chinese Medical University (Tongde Hospital of Zhejiang Province), Hangzhou, Zhejiang, People’s Republic of China; 2The Second School of Clinical Medicine, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongwei Wang, Department of Anesthesiology, Tongde Hospital Affiliated to Zhejiang Chinese Medical University (Tongde Hospital of Zhejiang Province), Hangzhou, Zhejiang, 310012, People’s Republic of China, Tel +86 13857169356, Email [email protected]
Purpose: This study aims to investigate the impact of anesthetic methods on the occurrence of postoperative sleep disorders in elderly patients following their discharge from the hospital for 3 months.
Patients and Methods: This retrospective observational cohort study included elderly patients aged > 60 years who had undergone general and regional anesthesia from 1 June 2023 to 31 December 2023. These patients were then assessed for sleep by telephone callback using the Athens Insomnia Scale after discharge from the hospital three months later. The duration of pain and sleep disturbance experienced by patients following discharge was also recorded.
Results: Following propensity score matching, 308 individuals were included in the study (154 in the GA group and 154 in the RA group). Compared with general anesthesia (11.7%), regional anesthesia (5.2%) reduced the prevalence of sleep disorders in elderly patients after discharge from the hospital. However, the duration of sleep disturbance and pain exhibited no statistically significant difference between the two groups (p=0.818; p=0.211).
Conclusion: Regional anesthesia was associated with a reduction in the incidence of sleep disorders in elderly patients after discharge from the hospital for 3 months.
Keywords: sleep disturbance, regional anesthesia, general anesthesia, elderly patient
Introduction
Postoperative sleep disturbance refers to the occurrence of insomnia, drowsiness, sleep structure changes, and increased awakening frequency, which is one of the manifestations of postoperative brain dysfunction.1,2 One study reported that about 23% of patients experienced sleep problems after surgery.3 Postoperative sleep disturbances can result in early postoperative fatigue, episodic hypoxemia, hemodynamic instability, and altered mental status. These factors can negatively impact postoperative outcomes.2,4 Elderly patients commonly have a combination of illnesses and frailty.5,6 Anesthesia, surgery, pain, and other multiple impacts make patients vulnerable to developing postoperative sleep disorders.
General anesthesia is a drug-induced state of reduced consciousness that is believed to cause postoperative circadian rhythm disruption. It is regarded as a significant risk factor for the disruption of the patient’s sleep architecture and quality.7 Research has shown that subarachnoid block is more beneficial than general anesthesia in elderly patients following hip fracture surgery, as subarachnoid block reduces the impairment of melatonin rhythm and sleep disturbances and reduces postoperative cognitive dysfunction.8 The study found that patients who underwent abdominal hysterectomy under subarachnoid block experienced significantly better sleep quality than those who underwent the procedure under general anesthesia.9
Postoperative sleep disorders are associated with various postoperative complications, including paroxysmal hypoxemia, pain sensitization, cognitive dysfunction, and fluctuations in blood pressure and heart rhythm due to sympathetic excitation.10–12 The occurrence of sleep disturbance after surgery is prevalent among elderly patients.13 However, few studies have compared the effect of anesthesia methods on post-discharge sleep disorders in surgical patients. We hypothesize that elderly patients undergoing regional anesthesia (RA group) experience fewer post-discharge sleep disorders compared to those who undergo general anesthesia (GA group).
Materials and Methods
Ethical Approval and Patients
This single-center retrospective observational cohort study was approved by the Ethics Committee of Tongde Hospital of Zhejiang Province (2023–092(K)) and complied with the Declaration of Helsinki. As all patients in the study had been discharged from the hospital, they were subsequently contacted by telephone. Following the obtaining of verbal consent from the patients at the time of the telephone callback, the next stage of the scale assessment was initiated. We got permission from the Ethics Committee of Tongde Hospital of Zhejiang Province to do the study without written consent and kept it in the form of telephone recordings. The study was also registered on the Chinese Clinical Trial Registry (ChiCTR2300076157). This study is reported in line with the STROBE statement.
We accessed the hospital database, and recruitment for this study began on 1 June 2023 and ended on 31 December 2023. Inclusion Criteria: (1) patients older than 60 years of age, of either sex; (2) American Society of Anesthesiologists (ASA) physical status grade I–III; (3) telephone follow-up with verbal consent to participate in this study; (4) non-neurosurgical, non-cardiac surgery with general anesthesia (lasting more than 2 hours) or regional anesthesia (spinal anesthesia, epidural anesthesia, and brachial plexus block). Exclusion criteria: (1) patients with a history of sleep apnea syndrome and/or preoperative sleep disorders; (2) patients requiring long-term use of hypnotics and sedatives; (3) patients with a history of mental and psychological disorders and recent use of antipsychotic drugs and antidepressant drugs; (4) patients who are unwilling to participate or unable to communicate; (5) patients with severe cardiopulmonary disorders.
Study Protocol
Demographic information, ASA physical status, type of anesthesia, and co-morbidities were recorded for each enrolled patient. To assess sleep disorders, we used the Athens Insomnia Scale (AIS),14 which was designed by the Ohio State University College of Medicine in 1985. Because of the accuracy of its self-rating results and its ease of use, it has been widely used in clinical practice and has become a standard scale recognized by the international medical community for the assessment of insomnia. The AIS is a self-rating psychometric instrument designed to quantify sleep difficulties based on ICD-10 criteria. It consists of eight items: the first five relate to sleep onset, awakenings during the night, final awakening, total sleep time and sleep quality, and the last three refer to well-being, functional capacity, and daytime drowsiness. Insomnia can be diagnosed if the AIS score is 6 points or higher. The AIS score ranges from 0 to 24 points.
The researchers collected data from patients who were discharged for three months after surgery. We followed up on the patients’ sleep status by telephone after discharge. Prior to the telephone callback, we screened the patients’ medical and medication histories. Prepared the discourse (without implying the patient, but a callback on the entire postoperative recovery) and performed an AIS score if the patient mentioned poor sleep and more than 3 times per week. We tried to be as objective as possible in our assessment. Sleep disorders are diagnosed when the AIS score exceeds 6. The primary outcome was the incidence of post-discharge sleep disorders, and the secondary outcomes were the duration of sleep disturbance and pain.
Sample Size
A previous study found that the incidence of sleep deprivation during hospitalization was 22.95% for patients who received general anesthesia and 8.6% for those who received subarachnoid block.8 We applied the PASS 15 Power Analysis and Sample Size Software (NCSS, LLC. Kaysville, Utah, USA, ncss.com/software/pass) to determine our sample size. We selected the “proportions-two independent proportions-test (inequality)-test for two proportions” to count the number of patients required per group for 90% power to distinguish the variance, with a two-tailed significance level of 0.05. As a result, we computed a sample size of 132 patients per group. Considering the missing sample size after propensity score matching, we decided to recruit 172 patients in each group.
Statistical Analysis
Continuous variables with normal distribution were presented as mean ± standard deviation (SD). Non-normal variables were presented as median (interquartile range). The distribution of continuous variables was analyzed using the Kolmogorov–Smirnov normality test. Categorical data were expressed as percentages (%). Independent-sample t-test or Mann–Whitney U-test was used to analyze continuous variables. The χ2 test was used to analyze categorical variables.
To reduce the likelihood of selection bias and baseline disparities between the RA and GA groups, propensity score matching (PSM) was conducted initially. The groups were matched in a 1:1 ratio using a caliper value of 0.02. The propensity score was calculated by using the following covariates: age, sex, smoking status, drinking status, and comorbid conditions. A binary logistic regression was conducted to examine the correlation between the anesthesia method and sleep disturbance after discharge. The level of statistical significance was set at a two-sided P value of <0.05. Statistical analyses were performed using IBM SPSS Statistics 25.
Results
Between 1 June and 31 December 2023, a total of 561 participants aged over 60 years were enrolled in this trial. During follow-up phone calls, 103 individuals declined participation or were unreachable, 59 were excluded due to depression, insomnia, or related conditions, and 53 were unable to participate due to communication difficulties or an invalid phone number. Ultimately, 346 individuals were successfully followed up and included in the study (Figure 1).
 |
Figure 1 Flow diagram of included patient numbers. |
There were no significant differences between the two groups at baseline before and after PSM, except for BMI and length of stay. (Table 1).
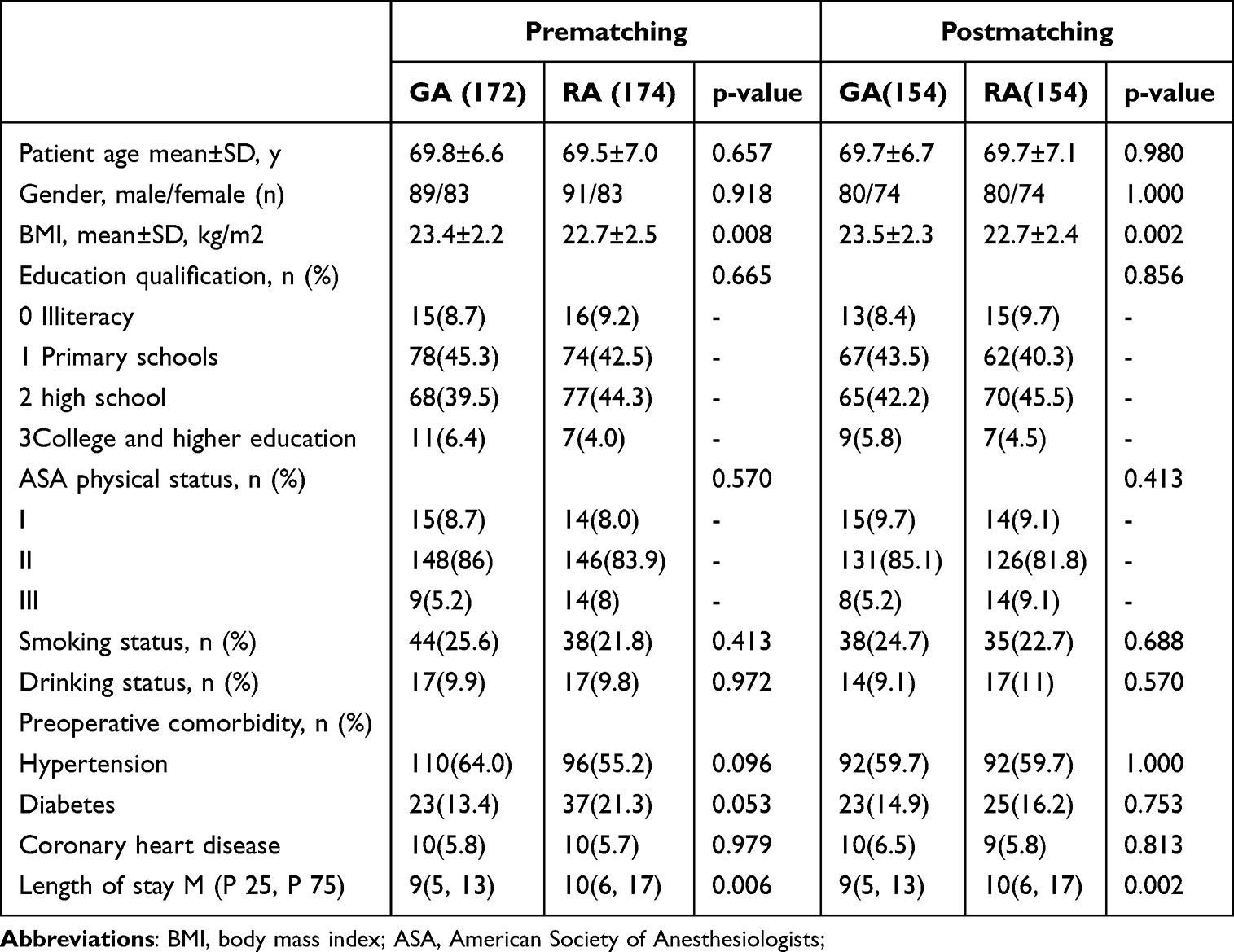 |
Table 1 Patient Demographics and Perioperative Characteristics |
The frequency of sleep disorders after discharge was higher in the GA (13.4%, 11.7%) compared to the RA group (6.3%, 5.2%) before and after matching (Table 2). Meanwhile, sleep disorders during hospitalization also showed a significant difference between the two groups before (p = 0.025) and after matching (p = 0.033) (Table 2). However, both the duration of post-discharge sleep disturbance and pain showed no difference between the GA group and the RA group whether in prematching (p = 0.574, 0.772) or postmatching (p = 0.818, 0.211). There was also no difference in the sleep scores (AIS) on the GA and the RA groups before PSM (p =0.504) and after PSM (p = 0.578) (Table 3).
 |
Table 2 The Comparison of Sleep Disorders Between the Group GA and the Group RA |
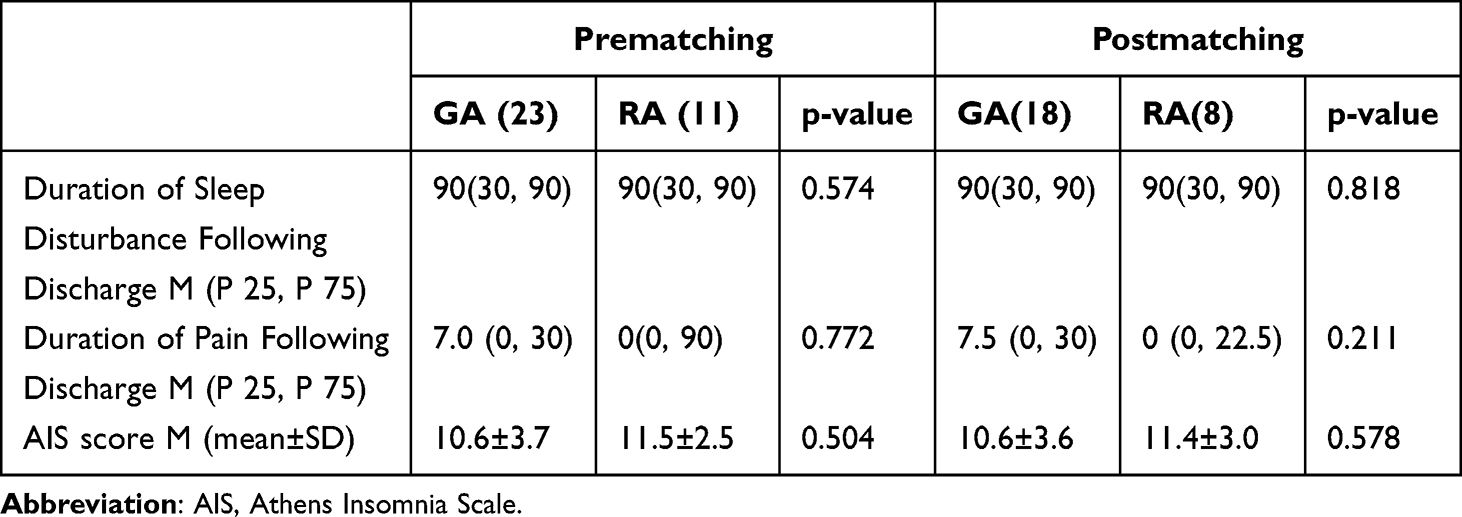 |
Table 3 Secondary Outcomes |
Binary logistic regression was employed to investigate the risk factors linked to sleep disorders following discharge. Postdischarge sleep disorders are more likely to occur after general anesthesia than after regional anesthesia (p = 0.021; OR, 2.93; 95% CI, 1.18–7.28) (Figure 2).
 |
Figure 2 Forest Plot of Factors Analyzed for Association with Incidence of Sleep Disturbance after Discharge from the Hospital in Binary Logistic Regression. |
Discussion
The important findings of this study were the presence of sleep disturbance in older patients who had no preoperative sleep disturbance after discharge, and the persistence of sleep disturbance for up to 3 months. Our study showed that in the older population, postdischarge sleep disturbance occurred after both general anesthesia and regional anesthesia. However, there was a higher incidence of sleep disorders in elderly patients who underwent general anesthesia than in this who underwent regional anesthesia, both during hospitalization (11%) and after discharge (13.4%), which is consistent with the previous literature.8,9,15 Gibian et al found that patients were still suffering from sleep disturbances an average of 90 days after surgery.16,17 This finding is also in line with our research. Our results indicate that older individuals experience sleep disturbances for up to three months after discharge, which seriously impacts the postoperative recovery of elderly patients.
The results of this study show that general anesthesia is significantly associated with the incidence of postdischarge sleep disorders in elderly patients. General anesthesia is a drug-induced hyporesponsive state of consciousness.18 Brain blood flow imaging studies have shown that anesthetic-induced loss of consciousness is similar to non-rapid eye movement,19,20 and anesthesia leads to a decrease in both rapid eye movement sleep and slow wave sleep, a reduction in total sleep time, and an increase in sleep fragmentation. Similar to previous studies, when we administered the AIS scale questionnaire to patients who continued to have sleep disturbances after discharge, they reported not getting enough sleep overall, waking up easily during the night, and having difficulty falling asleep. Van Zuylen et al have also demonstrated that surgical procedures requiring general anesthesia result in a significant phase shift of diurnal sleep-wake rhythms and a deterioration of sleep quality.21 Furthermore, general anesthetics such as propofol and thiopental sodium increase the activity of GABA neurons in the ventrolateral preoptic nucleus (VLPO) of the hypothalamus and induce sleep, and the hypothalamus, which is involved in sleep regulation, may be the target of general anesthetics for sedation and hypnosis.22,23 GABA also plays a significant role in resetting the circadian clock in response to changes in the light/dark cycle.24,25 This is crucial for gaining an understanding of the effects of general anesthesia on circadian rhythms, as most anesthetics are GABA agonists. In the meantime, some studies have demonstrated that GA has the capacity to modify the internal clock and disrupt circadian rhythms.26,27
In contrast, regional anesthesia has less impact on postoperative sleep disturbances in older patients (5.2%). Factors affecting postoperative sleep disorders are complex, such as the severity of surgical trauma, age, anesthetic mode, postoperative pain, postoperative complications, anesthetics and analgesics, environmental and psychological factors.10,13,28 The lower incidence of postdischarge sleep disorders in elderly patients under regional anesthesia compared to general anesthesia may be attributed to several factors: (1) Regional anesthesia is a local anesthetic that does not suppress the central nervous system and has less impact on brain function. (2) Regional anesthesia can effectively block the stress response triggered by incoming injurious stimuli, such as surgical operations, by inhibiting the upward transmission pathway of the reflex arc of the corresponding injurious stimuli. Song et al found that regional anesthesia reduces the impairment of melatonin rhythm and sleep. In their study, surgical trauma and inflammatory cytokine levels were similar between the GA and RA groups, except for pain scores. Therefore, it is thought that the differences in melatonin secretion between the two groups may be related to the anesthetic method and associated pain management.8 However, a randomized, controlled, open multicenter trial (82 patients who received spinal anesthesia and 80 patients who received general anesthesia) demonstrated that the sleep quality was better in the SA group than in the GA group, but they attributed this to lower opioid consumption in the SA group.9 In our study, there was no statistically significant difference in the duration of pain and disturbance between the two groups (Table 3), but the median duration of pain was shorter than the duration of sleep disorders. This means that patients may continue to experience sleep disturbance even when their pain was no longer present after they have been discharged from the hospital, which requires further study.
There are several limitations in our study. First, this retrospective study was unable to use objective indicators to record changes in patients’ sleep rhythms, such as polysomnography and sleep logs, to track patients’ sleep-wake patterns. Second, since the consultation was conducted via telephone, it was difficult to accurately assess the patient’s level of pain using visual analogue scale or numerical rating scale. Third, although we tried to identify and exclude patients with unclear recall of their post-discharge sleep disorders as objectively as possible, recall bias may still exist. Forth, this cohort study was observational and exploratory. Consequently, we are unable to rule out the chance of unmeasured group confounding. Prospective, randomized, controlled, multicentre studies are needed to further clarify the long-term effects of methods of anesthesia on sleep disturbance in older patients.
Conclusion
In summary, regional anesthesia was associated with a reduction in the incidence of sleep disorders in elderly patients after discharge from the hospital for 3 months. Our findings suggest that the choice of anesthetic method may influence the incidence of sleep disturbances in elderly patients. Further research is needed.
Acknowledgments
We are grateful to those who have given us guidance on the statistical methods and the linguistic nuances of this experiment.
Disclosure
All authors have no conflicts of interest, financial or otherwise to disclose for this work.
References
1. Rosenberg J. Sleep disturbances after non-cardiac surgery. Sleep Med Rev. 2001;5(2):129–137. doi:10.1053/smrv.2000.0121
2. Rosenberg-Adamsen S, Kehlet H, Dodds C, Rosenberg J. Postoperative sleep disturbances: mechanisms and clinical implications. Br J Anaesth. 1996;76(4):552–559. doi:10.1093/bja/76.4.552
3. Kain ZN, Caldwell-Andrews AA. Sleeping characteristics of adults undergoing outpatient elective surgery: a cohort study. J Clin Anesthesia. 2003;15(7):505–509. doi:10.1016/j.jclinane.2003.02.002
4. Krenk L, Jennum P, Kehlet H. Sleep disturbances after fast-track Hip and knee arthroplasty. Br J Anaesth. 2012;109(5):769–775. doi:10.1093/bja/aes252
5. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
6. Dent E, Martin FC, Bergman H, Woo J, Romero-Ortuno R, Walston JD. Management of frailty: opportunities, challenges, and future directions. Lancet. 2019;394(10206):1376–1386. doi:10.1016/S0140-6736(19)31785-4
7. Luo M, Song B, Zhu J. Sleep disturbances after general anesthesia: current perspectives. Front Neurol. 2020;11. doi:10.3389/fneur.2020.00629
8. Song Y, Liu Y, Yuan Y, et al. Effects of general versus subarachnoid anaesthesia on circadian melatonin rhythm and postoperative delirium in elderly patients undergoing Hip fracture surgery: a prospective cohort clinical trial. EBioMedicine. 2021;70:103490. doi:10.1016/j.ebiom.2021.103490
9. Kjølhede P, Langström P, Nilsson P, Wodlin NB, Nilsson L. The impact of quality of sleep on recovery from fast-track abdominal hysterectomy. J Clin Sleep Med. 2012;08(04):395–402. doi:10.5664/jcsm.2032
10. Rampes S, Ma K, Divecha YA, Alam A, Ma D. Postoperative sleep disorders and their potential impacts on surgical outcomes. J Biomed Res. 2020;34(4):271. doi:10.7555/JBR.33.20190054
11. Chouchou F, Khoury S, Chauny JM, Denis R, Lavigne GJ. Postoperative sleep disruptions: a potential catalyst of acute pain? Sleep Med Rev. 2014;18(3):273–282. doi:10.1016/j.smrv.2013.07.002
12. Gögenur I, Middleton B, Burgdorf S, Rasmussen LS, Skene DJ, Rosenberg J. Impact of sleep and circadian disturbances in urinary 6-sulphatoxymelatonin levels, on cognitive function after major surgery. J Pineal Res. 2007;43(2):179–184. doi:10.1111/j.1600-079X.2007.00460.x
13. Su X, Wang D-X. Improve postoperative sleep. Curr Opin Anaesthesiol. 2018;31(1):83–88. doi:10.1097/ACO.0000000000000538
14. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosomatic Res. 2000;48(6):555–560. doi:10.1016/S0022-3999(00)00095-7
15. Lei M, Zhang P, Liu Y, Fu F, Ye L, Zhu T. Propofol and sufentanil may affect the patients’ sleep quality independently of the surgical stress response: a prospective nonrandomized controlled trial in 1033 patients’ undergone diagnostic upper gastrointestinal endoscopy. BMC Anesthesiol. 2017;17(1):53. doi:10.1186/s12871-017-0341-3
16. Gibian JT, Bartosiak KA, Lucey BP, Riegler V, King J, Barrack RL. Sleep disturbances following total knee arthroplasty. J Arthroplasty. 2023;38(6):S120–S124. doi:10.1016/j.arth.2023.01.066
17. Pitaro NL, Herrera MM, Alasadi H, et al. Sleep disturbance trends in the short-term postoperative period for patients undergoing total joint arthroplasty. J Am Acad Orthopaedic Surg. 2023;31(19):e859–e867.
18. Kushikata T, Yosmda H, Yasuda T, Tose R, Hirota K, Matsuki A. Sleep and anesthesia--part 2, on the relationship between sleep and general anesthesia. Masui Japanese J Anesthesiol. 2007;56(10):1148–1154.
19. Nelson LE, Franks NP, Maze M. Rested and refreshed after anesthesia? Overlapping neurobiologic mechanisms of sleep and anesthesia. Anesthesiology. 2004;100(6):1341–1342. doi:10.1097/00000542-200406000-00003
20. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthesia. Science. 2008;322(5903):876–880. doi:10.1126/science.1149213
21. van Zuylen ML, Meewisse AJG, Ten Hoope W, et al. Effects of surgery and general anaesthesia on sleep–wake timing: CLOCKS observational study. Anaesthesia. 2021;77(1):73–81. doi:10.1111/anae.15564
22. Mashour GA, Hudetz AG. Bottom-up and top-down mechanisms of general anesthetics modulate different dimensions of consciousness. Front Neural Circuits. 2017;11:44. doi:10.3389/fncir.2017.00044
23. Fukuda S, Yasuda A, Lu Z, et al. Effect sites of anesthetics in the central nervous system network--looking into the mechanisms for natural sleep and anesthesia. Masui Japanese J Anesthesiol. 2011;60(5):544–558.
24. Myung J, Hong S, DeWoskin D, De Schutter E, Forger DB, Takumi T. GABA-mediated repulsive coupling between circadian clock neurons in the SCN encodes seasonal time. Proc Natl Acad Sci. 2015;112(29):E3920–3929.
25. Ralph MR, Menaker M. GABA regulation of circadian responses to light. I. Involvement of GABAA-benzodiazepine and GABAB receptors. J Neurosci: Off J Soc Neurosci. 1989;9(8):2858–2865. doi:10.1523/JNEUROSCI.09-08-02858.1989
26. Coppola S, Caccioppola A, Chiumello D. Internal clock and the surgical ICU patient. Curr Opin Anaesthesiol. 2020;33(2):177–184. doi:10.1097/ACO.0000000000000816
27. Poulsen RC, Warman GR, Sleigh J, Ludin NM, Cheeseman JF. How does general anaesthesia affect the circadian clock? Sleep Med Rev. 2018;37:35–44. doi:10.1016/j.smrv.2016.12.002
28. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2019;45(1):205–216. doi:10.1038/s41386-019-0439-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.