")
Back to Journals » Journal of Pain Research » Volume 18
Effect of Physical Activity on Chronic Widespread Pain: Insights From Meta-Analysis and Two-Sample Mendelian Randomization
Authors Yao C , Zhang Y, Zhao SS, Ren J , Sun P, Kong L, Tao J, Li J, Fang M, Zhu Q
Received 25 November 2024
Accepted for publication 6 March 2025
Published 14 March 2025 Volume 2025:18 Pages 1275—1289
DOI https://doi.org/10.2147/JPR.S505397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Chongjie Yao,1– 3,* Yuchen Zhang,2,3,* Sizheng Steven Zhao,4 Jun Ren,3 Pingping Sun,5 Lingjun Kong,3 Jiming Tao,3 Jingxian Li,6 Min Fang,3,7 Qingguang Zhu1,7
1Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 200437, People’s Republic of China; 2School of Acupuncture-Moxibustion and Tuina, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 3Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 4Centre for Musculoskeletal Research, School of Biological Sciences, Faculty of Biological Medicine and Health, the University of Manchester, Manchester, UK; 5School of Rehabilitation Science, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 6School of Human Kinetics, Faculty of Health Sciences, University of Ottawa, Ottawa, K1N 6N5, Canada; 7Research Institute of Tuina, Shanghai Academy of Traditional Chinese Medicine, Shanghai, 200437, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingguang Zhu; Min Fang, Email [email protected]; [email protected]
Background: Chronic widespread pain (CWP) is a core symptom of fibromyalgia that is associated with significant morbidity and mortality. Despite the widespread recommendation for physical activity (PA) in management, the heterogeneity of PA prescriptions limits the in-depth evaluation of its efficacy. By triangulating clinical interventional evidence with human genetic evidence, the aim of this study was to investigate the role of influencing factors such as PA mode, course of treatment, and intensity on PA in the prevention and treatment of CWP.
Methods: Ten international and regional databases were searched for articles published between January 2014 and July 2024. Randomized control trials with CWP or fibromyalgia as an entry criterion and PA as an intervention were included. Meta-analyses were performed using fixed- or random-effects models based on heterogeneity, and subgroup analyses were conducted. Mendelian randomization (MR) was used to estimate the effects of the genetic variants linked to PA intensity on CWP risk.
Results: The analysis included 11 studies with 540 participants. PA effectively improved pain perception (MD: − 1.47; 95% CI: − 2.23, − 0.72), depression (MD: − 4.77; 95% CI: − 7.40, − 2.14), and overall quality of life (SMD: − 1.43; 95% CI: − 2.16, − 0.69). MR analysis revealed that several PA intensities were associated with reduced susceptibility to CWP: walking for pleasure (OR: 0.950; 95% CI: 0.934– 0.966), light do-it-yourself (DIY) (OR: 0.976; 95% CI: 0.961– 0.992), strenuous sports (OR: 0.923; 95% CI: 0.880– 0.967), and other exercises (OR: 0.957; 95% CI: 0.942– 0.973).
Conclusion: PA interventions are beneficial for reducing pain perception and mood disorders and enhancing the quality of life of patients with CWP. A treatment course of approximately three months is preferable, with Ba-Duan-Jin potentially more effective than other PAs, and high-intensity PA offers the most significant protective effect against CWP.
Keywords: chronic widespread pain, fibromyalgia, physical activity, exercise
Introduction
Chronic widespread pain (CWP), defined by the American College of Rheumatology, lasts for at least three months in at least four of five pain regions and affects approximately 10.6% of adults worldwide.1 It is twice as prevalent in females than males, with a higher prevalence in individuals over the age of 40 years.2 When accompanied by symptoms such as fatigue and cognitive impairment, CWP often leads to a diagnosis of fibromyalgia.3 The significant impact of CWP and fibromyalgia on individuals and society, particularly on increased mortality, underscores the need for effective management strategies.4 However, owing to the complex and diverse pathobiology of these conditions, definitive treatments are lacking, resulting in poor medical outcomes and increased mortality.5
Physical activity (PA), which refers to any bodily movement generated by skeletal muscles that leads to energy expenditure, is gaining recognition as a central management strategy for chronic pain.6 International guidelines advocate PA as the cornerstone of treatment regimens for CWP.7 However, the role of PA in CWP relief remains debatable. An earlier study8 reported increased pain after exercise in patients with fibromyalgia, whereas another study9 showed reduced pressure pain thresholds during and after isometric contraction. Conversely, qualitative research10 indicated that PA can alleviate pain-dominated symptoms, and a nine-year prospective cohort study11 demonstrated the lasting benefits of PA on health, pain, disease impact, and quality of life in women with fibromyalgia. Systematic reviews with meta-analyses suggest that aerobic exercise, strength, and resistance training are effective treatments for CWP,12,13 although uncertainties remain regarding specific exercises such as stretching. Notably, even if the interventions studied are limited to one type of exercise, the results can be variable. A recent Spanish pilot study14 found that limiting blood flow speed was an important factor in the effectiveness of aerobic exercise in treating fibromyalgia, emphasizing the high heterogeneity of PA in the treatment of fibromyalgia. Additionally, studies have also revealed that pain may influence or restrict PA participation,15,16 and questions persist regarding exercise intensity, frequency, and progression of PA programs in this population. A latest qualitative evidence synthesis study17 from the United Kingdom raised the importance of overlooked factors such as personalization, group cohesion and emotional experience in maintaining pain management programs for CWP, further highlighting the complexity of PA prescribing. To develop effective, practical, and feasible PA programs for individuals with CWP, it is crucial to investigate the exercise modalities for managing CWP.
Given the importance of developing efficient prevention and treatment strategies, evaluating the efficacy of PA in managing CWP and exploring the impact of PA modalities are critical. Meta-analysis plays a pivotal role in summarizing evidence, but causal inferences may be limited by study design. Therefore, this study evaluated the efficacy of PA in treating CWP by integrating a two-sample Mendelian randomization (MR) with a systematic review and meta-analysis. The study aimed to identify the most effective types of PA, evaluate the efficacy of different PA modes to enhance our understanding of PA’s role in CWP treatment, and provide evidence-based support for developing more effective PA prescriptions.
Methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta‐analyses (PRISMA) 2020 reporting guidelines and adhered to the STROBE-MR guidelines for strengthening reporting in observational epidemiological studies using Mendelian randomization. The systematic review and meta-analysis section was registered in PROSPERO (CRD42023458054).
Search Strategy
From January 2014 to July 2024, we searched Web of Science, the Cochrane Library, PubMed (Medline), EMBASE, Scopus, PEDro (the Physiotherapy Evidence Database), Latin American and Caribbean Health Sciences Literature, China National Knowledge Infrastructure, Wan Fang Digital Journals, and Chinese Science and Technology Periodical Databases. The keywords used were “physical activity”, “exercise”, “muscle strengthening”, and “chronic widespread pain”. There were no language restrictions, and Supplementary file 1 provides a detailed PubMed search strategy. Reviewers reached out to study authors when required.
Study Selection
The inclusion criteria were randomized control trials (RCTs) involving participants with chronic widespread pain or fibromyalgia, without gender or nationality limitations. The interventions included various physical activities, with the control group receiving minimal interventions. The main outcomes measured were pain (visual analog scale [VAS]), quality of life (fibromyalgia impact questionnaire [FIQ]), and psychological issues (Beck Depression Inventory [BDI]). The exclusion criteria were pilot studies, nonrandomized trials, duplicated publications, and studies with incomplete data. The qualified studies were imported into the Endnote 20 application, and duplicate studies were automatically removed. Two authors independently screened the remaining studies based on the inclusion and exclusion criteria. The full texts of potentially eligible articles were obtained and reviewed for a second screening, and the results were cross-checked. Discrepancies were resolved through consensus between the two reviewers. If a decision was not reached, an additional reviewer was added to reach agreement.
Data Extraction and Quality Assessment
A specially designed sheet was used to extract the information from the included studies. The outcomes of interest were the extent of pain, severity of depression, and overall quality of life. The Cochrane revised risk-of-bias tool for randomized trials (RoB 2) was used to evaluate the risk of bias in six domains, classifying studies as “low risk”, “high risk”, or “some concerns”. The certainty of evidence for the efficacy outcomes was evaluated using the Grading of Recommendations Assessment Development and Evaluation (GRADE). The Guideline Development Tool was used to grade the evidence into four levels: high, moderate, low, and very low. Two authors independently used the above tools, and any disagreements were resolved through consultation with a third investigator.
Data Synthesis and Statistical Analysis
The meta-analysis was conducted using RevMan version 5.4 (The Cochrane Collaboration, Software Update, Oxford, United Kingdom). For the efficacy analysis of continuous variables, mean difference (MD), standardized mean difference (SMD), and 95% confidence intervals (CIs) were employed. When the units of effect size data from all the original studies participating in the meta-analysis were consistent, MD was applied in the quantitative analysis; otherwise, SMD was used. Continuous variables initially presented as medians with interquartile ranges are transformed into means and standard deviations using well-established techniques.18,19 In cases where the original articles did not include the mean and standard deviation of changes from baseline, the data were calculated as follows:20


The I2 test was used to assess statistical heterogeneity of the results. An I2 value of ≤ 50% signifies low or moderate heterogeneity, and a fixed-effects model can be used for the analysis. Conversely, I2 > 50% suggested significant heterogeneity, and a random-effects model was used to better deal with clinical heterogeneity. Subgroup analyses were performed by considering various PAs, session durations, and baseline scores. Funnel plots were used to evaluate potential publication bias when more than nine trials were included in the meta-analysis. Sensitivity analyses included sequential exclusion of each individual trial and the use of a fixed-effects model instead of a random-effects model. All P values were two-sided, and the results were considered statistically significant at P < 0.05.
Mendelian Randomization
This MR analysis used publicly available summary data from previous genome-wide association studies (GWAS). All contributing studies sought informed consent from study participants.
Genetic association data for PA were derived from a GWAS involving 460,376 samples from the UK Biobank, as analyzed by the Neale Lab (http://www.nealelab.is/uk-biobank/). PA at different intensities was defined based on self-reported participation within the past four weeks. The questionnaire options included “walking for pleasure”, “other exercises”, “strenuous sports”, “light do-it-yourself (DIY)”, “heavy DIY”, “none of the above”, and “prefer not to answer”. Summary-level data on single nucleotide polymorphisms (SNPs) associated with CWP were obtained from a GWAS consisting of 336,650 samples from the UK Biobank.21 Cases were defined as pain that interfered with daily life, according to the participants’ self-reports. Supplementary file 2 provides an in-depth overview of the GWASs analyzed in this study.
In the present MR section, SNPs that were identified to be associated with exposure factors at the genome-wide significance level (P < 5×10−7) from GWASs and were not in linkage disequilibrium (LD) with other SNPs (r2 < 0.01, within a clumping window of 10000 kb) were utilized as instruments for these PA intensities. Finally, 194 PA-associated SNPs were included in MR analysis. Details regarding the SNPs used as instruments are provided in the Supplementary file 3.
Two-sample inverse-variance weighted (IVW) MR analysis was conducted to estimate the causal relationship between PA and CWP. Cochran’s Q test was used to assess heterogeneity among the genetic instruments. When heterogeneity existed (P < 0.05), a multiplicative random-effect IVW model was applied; otherwise, a fixed-effect IVW model was utilized. MR-Egger regression and causal analysis using summary effect estimates (CAUSE) method were utilized to assess the potential horizontal pleiotropy and correlated pleiotropy, respectively. Additionally, sensitivity analyses were conducted using the MR–Egger regression and weighted median regression. Leave-one-out (LOO) analysis was performed to assess whether the results remained stable after a single removal of each SNP (Figure 1).
 |
Figure 1 The overall framework of the study. Abbreviations: RCT, randomized controlled trial; CAUSE, causal analysis using summary effect estimates; DIY, do it yourself. |
To prevent a potentially weak instrumental bias, the F statistic  was used to assess the robustness of the IVs. If F > 10, the association between IV and exposure is sufficiently strong to protect the results of the MR analysis from a weak instrumental bias. As the SNPs used to derive instruments concerning PAs and CWP were constructed using GWAS from the UK Biobank, bias may have been generated because of participant overlap. An established method was applied to assess the magnitude of the bias and Type 1 error rate inflation in the analysis results.22
was used to assess the robustness of the IVs. If F > 10, the association between IV and exposure is sufficiently strong to protect the results of the MR analysis from a weak instrumental bias. As the SNPs used to derive instruments concerning PAs and CWP were constructed using GWAS from the UK Biobank, bias may have been generated because of participant overlap. An established method was applied to assess the magnitude of the bias and Type 1 error rate inflation in the analysis results.22
The MR analyses utilized the Two-Sample MR and CAUSE R packages in the R software version 4.2.2.23–25 All results are presented as odds ratios (ORs) with 95% CIs of outcomes. Since multiple GWASs were included in this analysis, Bonferroni correction was applied, and results with P-value < 0.008 were considered statistically significant.
Results
Search Process
The PRISMA flowchart for the systematic reviews included in Figure 1 presents the search process. This study retrieved 4397 publications from electronic databases. After automatically deleting 977 duplicates, we assessed the remaining 3420 studies by screening titles and abstracts; 2763 studies were excluded. Of the preliminarily excluded articles, 1056 were not randomized controlled trials, and 1707 were excluded because they did not focus on CWP. After examining the full text, 352 articles were excluded because they did not use minimum intervention as the sole intervention for the control group and 290 articles were excluded because they did not use PA therapy as the sole intervention for the experimental group. On the other hand, three articles were removed for not having full text or original data, and one article was removed for duplicated patients with another article.
Ultimately, 11 eligible RCTs that met the inclusion criteria were included in this meta-analysis.
Characteristics of Included Studies
A total of 540 CWP patients from 11 RCTs were included, of which 274 were allocated to the PA group and 266 to the control group. Five trials were performed in Spain,26–30 two in China,31,32 two in Brazil,33,34 one in Italy,35 and one in Iran,36 respectively.
All the included studies used PAs as an experimental intervention for CWP. These exercises included resistance training, aerobic exercise, aquatic physical training, training based on exergames, Qi gong exercises, and Ba-Duan-Jin (a mind-body practice first developed over 5000 years ago, focusing on breathing, increasing flexibility, and strengthening muscles and tendons37). The studies lasted for 6–24 weeks. The duration of each exercise was 40–60 min. The follow-up period ranged from 16 weeks to 24 weeks. The control intervention included waiting lists, education, and treatment as usual. The main outcomes included pain, quality of life, and the severity of depression.
The main characteristics of all included RCTs were shown in Table 1.
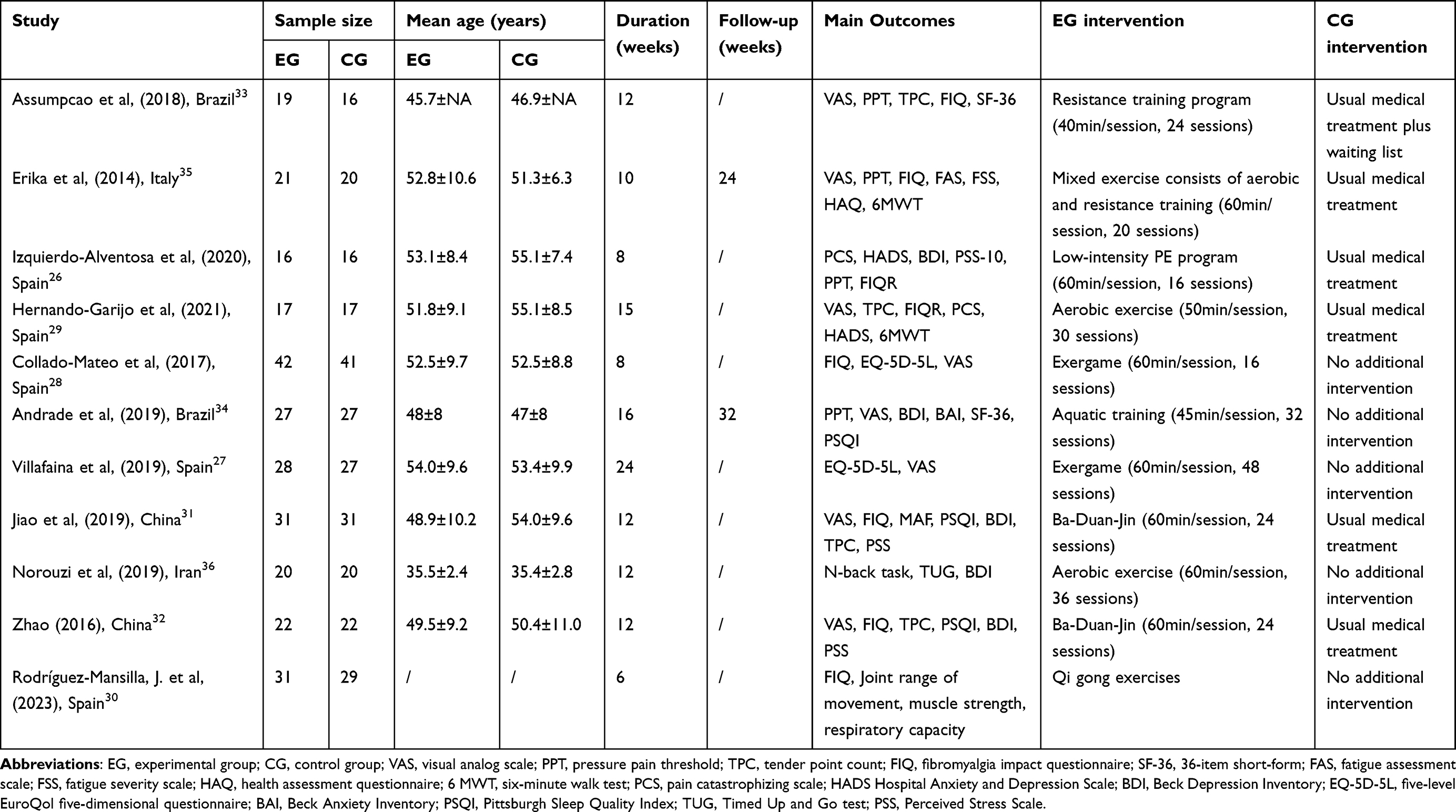 |
Table 1 Characteristic of the Included Randomized Controlled Trials |
Quality Assessment of the Included Studies
Concerning the risk of bias in the randomization process, deviations from intended interventions, and missing outcome data, all the included studies were at low risk. However, two studies28,32 were considered to have some concerns with selective reporting due to the lack of protocol registration, or the actual experiment was different from the registered protocol. For outcome measurement, six studies28,31–33,35,36 were rated as some concerns” for reasons such as not blinding the outcome assessors or obtaining data through participants’ self-reports. Overall, the risk of bias was typically either of concern (18.2%) or low (81.8%). Detailed ratings are provided in Supplementary file 4.
Quantitative Analysis Considering the Effects on Pain Intensity
In total, eight studies with 408 patients applied the VAS to assess pain intensity. The heterogeneity test showed heterogeneity among the eight studies (I2 = 94%, P < 0.01). Therefore, a random-effects model was used for data analysis. The meta-analysis presented in Figure 2A provides a comparison of VAS scores between the PA and control groups. All PA interventions had a beneficial effect on reducing VAS scores (MD: −1.47; 95% CI: −2.23, −0.72; P < 0.01). As for the subgroup analysis, an 11-to-14-week intervention demonstrated the highest effect size in this analysis (MD: −2.60; 95% CI: −2.83, −2.38; P < 0.01), while an intervention lasting for more than 15 weeks had a moderate effect (MD: −1.31; 95% CI: −1.58, −1.05; P < 0.01). Although intervention within 10 weeks was less effective, the effect size (MD: −0.63; 95% CI: −0.97, −0.29; P < 0.01) also suggested that PA within ten weeks effectively reduced the VAS scores.
 |
Figure 2 Meta-analysis on the effects of physical activity on pain intensity: (A) VAS Pain, (B) tender point count, and (C) pressure pain threshold. |
Five studies involving 216 participants assessed pain intensity using tender point count, of which high scores are thought to correlate with the development of CWP.38 All these studies were included in the meta-analysis. The heterogeneity test showed heterogeneity among the five studies (I2 = 99%, P < 0.01). Therefore, a random-effects model was used for data analysis. As shown in Figure 2B, PA intervention in the analyzed studies effectively reduced TPC scores (MD: −4.11; 95% CI: −6.95, −1.26; P < 0.01). Subgroup analysis based on PA type revealed that the efficacy of Ba-Duan-Jin in reducing the number of tender points (MD: −6.69; 95% CI: −6.97, −6.42; P < 0.01) was better than that of PA intervention based on resistance and aerobic exercise (MD: −2.14; 95% CI: −2.53, −1.76; P < 0.01).
In addition, four studies applying pressure pain threshold as an outcome to assess pain intensity were also included in the meta-analysis (Figure 2C). Random-effect models were used because of the high heterogeneity (I2 = 91%, P < 0.01). However, the results showed no statistically significant difference between the efficacy of PA groups and control groups in this regard (MD: 0.60; 95% CI: −0.09, 1.30; P = 0.09). Further subgroup analyses did not identify sources of heterogeneity.
Quantitative Analysis Considering the Effects on Overall Life Quality
In total, 9 studies with 445 patients who underwent FIQ to assess the patients’ overall quality of life were included (Figure 3A). The heterogeneity test showed high heterogeneity among the 9 studies (I2 = 91%, P < 0.01). Therefore, a random-effects model was used for data analysis. The aggregated results showed the beneficial effects of PAs in improving the overall quality of life of patients with CWP (SMD: −1.43; 95% CI: −2.16, −0.69; P < 0.01). As for the analysis of the subgroups, the efficacy of the short-term intervention with a duration less than 10 weeks was relatively weak in this regard, but still demonstrated a statistically significant advantage over the control group (SMD: −0.64; 95% CI: −0.94, −0.35; P < 0.01). Interventions lasting for 15 weeks showed a moderate effect in reducing FIQ scores (SMD: −1.89; 95% CI: −2.71, −1.06; P < 0.01). Despite the high heterogeneity (I2 = 93%, P < 0.05) within the group of 11-to-14-week duration, the effect size (SMD: −3.75; 95% CI: −6.18, −1.33; P < 0.01) suggested that this intervention duration may be the most effective in improving overall quality of life.
 |
Figure 3 Meta-analysis on the effects of physical activity on overall quality of life (A) and depression (B). Subgroup analyses for quality of life were based on the length of treatment, while that for depression were based on baseline scores. |
Quantitative Analysis Considering the Effects on the Depression Severity
Five trials were included in the meta-analysis of depression because they reported BDI as an outcome (Figure 3B). Random-effect models were used because of the high heterogeneity (I2 = 83%, P < 0.01). Compared to the control group, the PA group showed a more significant decrease in BDI scores after the intervention (MD: −4.77; 95% CI: −7.40, −2.14; P<0.01). Based on different baseline scores, subgroup analyses categorized studies into mild to moderate depression (mean ranged, 8.3 to 20.6) and severe depression (mean ranged from 29.31 to 30.98). The efficacy of studies with lower baseline scores was slightly weaker in alleviating depression (MD: −3.23; 95% CI: −3.69, −2.76; P < 0.01) than those with high baseline scores (MD: −7.91; 95% CI: −9.79, −6.03; P < 0.01).
Sensitivity Analyses and the GRADE Level of Evidence
Regarding the sensitivity analyses, the change from a random-effects model to a fixed-effects model and the sequential omission of each study had no substantial effect on the outcomes, except pressure pain threshold. The main reason may be the small number of included articles and high heterogeneity among the studies.
The certainty of the evidence was rated for meta-analytic outcomes as moderate and moderate-to-very low for individual study outcomes (Supplementary file 5). The main reasons for downgrading the evidence were RoB, inconsistency, and imprecision. We did not grade down due to publication bias, because the number of analyzed studies was less than ten. Indirectness was not downgraded as this review followed strict population, intervention, comparator, and outcome eligibility criteria.
Mendelian Randomization Estimates of the Association Between Different Physical Activity Intensities and CWP
As shown in Figure 4, PA intensity was significantly negatively associated with CWP risk. Specifically, walking for pleasure (odds ratio [OR] = 0.950; 95% confidence interval [CI]: 0.934–0.966; P < 0.001), light DIY (OR = 0.976; 95% CI: 0.961–0.992; P = 0.003), strenuous sports (OR = 0.923; 95% CI: 0.880–0.967; P = 0.001), and other exercises (OR = 0.957; 95% CI: 0.942–0.973; P < 0.001) are protective factors for CWP. However, not all PA intensities were associated with CWP. From the perspective of genetic susceptibility, there is no significant causal relationship between heavy DIY and CWP (OR = 0.971; 95% CI: 0.948–0.994; P = 0.014). At the same time, not surprisingly, not doing any PA was identified as a predisposing contributor for the risk of CWP (OR = 1.100; 95% CI: 1.036–1.168; P = 0.002). Detailed MR results of PAs on the risk of CWP with scatter plots and heterogeneity and horizontal pleiotropy among genetic instruments can be found in Supplementary file 6. Notably, the CAUSE method revealed limited evidence that the causal model fit the data better than the sharing model in the present study, indicating that correlated pleiotropy could not be discounted (Supplementary file 7 and Supplementary Figures 1-6).
 |
Figure 4 The putative causal effect of physical activity on chronic widespread pain. Abbreviations: OR, odd ratio; CI, confidence interval; FEM, fixed-effect model; REM, random-effect model; MR, Mendelian randomization; DIY, do it yourself. |
LOO analyses suggested that the causal estimates were not driven by any single SNP (Supplementary file 8). Additionally, the F statistics for the IVs ranged from 25.25 to 84.95, suggesting that this MR study did not have weak instrument bias. Because the maximum sample overlap determined by the sample size was 73.13%, the corresponding maximum type-1 error rate was 0.06 among all outcomes, suggesting that the estimated biases due to the sample overlap were small to moderate.
Discussion
Physical activity (PA) has become an integral part of treating patients with chronic widespread pain (CWP). However, the high variability in PA prescriptions hampers in-depth analysis of its efficacy. By combining meta-analysis and Mendelian randomization (MR), two complementary methods, we assessed the effects of different PA modes, durations, and intensities on CWP. The meta-analysis revealed that interventions with a moderate duration (approximately three months), incorporating simple or progressive exercise sequences, yielded superior outcomes compared to other therapeutic options. The MR analysis further suggested that intense PA (exceeding six metabolic equivalents) may exhibit the strongest protective effect. These findings provide a foundation for clinicians to devise detailed exercise prescriptions.
Our findings align with previous reports,4,12 indicating that PA is an effective intervention for patients with CWP and fibromyalgia. Exercise-induced hypoalgesia is the most frequently cited pain-relieving effect. Muscle contraction is thought to stimulate central downstream pain pathways and increase the release of endogenous opioids, resulting in an analgesic effect.39 Additionally, PA is known to alleviate CWP symptoms by improving psychological disorders and overall well-being,40 consistent with our findings, highlighting PA’s effectiveness of PA through multiple pathways. The limited follow-up data in the included studies may be attributed to PA’s self-sustaining nature of PA. As individuals experience benefits from PA, they tend to adhere to it, potentially leading to spontaneous exercise habits post-intervention, which can interfere with follow-up accuracy. While this limits our analysis of the long-term efficacy of PA, it underscores the self-sustaining advantages of exercise therapy.
Regarding different PA types, our meta-analysis revealed Ba-Duan-Jin to be more effective than aerobic and resistance training, particularly in reducing tender point count. Ba-Duan-Jin, a multicomponent therapy integrating physical, psychosocial, cognitive, and spiritual elements,41 may exert analgesic effects by altering blood flow in the prefrontal cortex, which is implicated in pain processing. Patients with chronic pain often exhibit reduced blood flow in the prefrontal cortex, potentially indicating endothelial dysfunction or arterial stiffness.42 Furthermore, the simplicity of Ba-Duan-Jin movements may boost participants’ confidence and effort, leading to improved outcomes and suggesting that progressive difficulty or a lower entry threshold may benefit inexperienced exercisers.
Subgroup analysis contributed to the further determination of the optimal PA prescription course for the treatment of CWP. It is widely recognized that the therapeutic window for CWP and fibromyalgia is narrow, with insufficient exercise failing to provide benefits and excessive exercise exacerbating the symptoms.43 A previous meta-analysis44 indicated that a moderate-duration programof 13-24 weeks demonstrated the best efficacy. Extending this, our results further screened for an optimal intervention regimen, revealing that a 60-minute session duration, with interventions lasting 10–15 weeks, is more effective than longer durations in relieving pain and improving overall quality of life. Alongside existing evidence, it appears that three months may be the critical period for peak efficacy for most PAs. The nonlinear relationship between efficacy and session length may arise from the balance between the PA-related and induced fatigue relief. Patients with fibromyalgia exhibit dysregulated purine, pyrimidine, and glutaminergic metabolism with elevated systemic glutamate and glutamine levels, indicative of a fatigued state.45 Plasma glutamine levels increased during exercise followed by a significant decrease during post-exercise recovery. If recovery between PAs is inadequate, the acute effects of PA on plasma glutamine levels may accumulate, manifesting as exacerbation of clinical symptoms due to overtraining. Our findings suggest that, for patients with CWP and fibromyalgia, prolonged PA at low exercise volumes or PA prescriptions interspersed at appropriate intervals may be promising.
MR results further revealed that high-intensity PA had the greatest protective effect against CWP. Moderate to vigorous PA has been reported to have a more pronounced anti-inflammatory effect, consistent with MR results.46 Neutrophils are critical for the development of CWP through infiltration of the peripheral sensory ganglia, and relieving neuroinflammation is an effective way to treat fibromyalgia.47 It has already been observed that high-intensity exercise reduces both neutrophil migration and adhesion molecule expression,48 which may be an important factor impeding the initiation and progression of CWP, but the specific associations need to be further investigated. In LOO analysis, the direction of all results was consistent, and the confidence interval for all the results was not cross the invalid line which represents the OR value of 1, indicating the high robustness of the present MR result. However, the findings from CAUSE method indicated that only the associations between “walking for pleasure”, “other exercises” and the risk of CWP remained unaffected by horizontal pleiotropy. Therefore, the risk of false positives due to horizontal pleiotropy must be vigilant when interpreting the other MR results.25 Based on the MR results and previous studies,49–51 representative exercises corresponding to different PA intensities were listed (evaluated by metabolic equivalents) (Figure 5). Notably, although intense PA had the strongest protective effect, it should not be the only factor promoted. As mentioned earlier, ease of acquisition and gradual difficulty of the PA modality are important factors for training participants. High-intensity PA also tends to have higher dropout rates than low-intensity PA. In general, individualized PA prescriptions that incorporate multiple factors, such as patient willingness, clinical outcomes, along with the basic and progression of physical capacity, are recommended. Additionally, as successful initiatives such as “Fibro Friends” have demonstrated the efficacy of multidisciplinary educational health promotion programs in treating fibromyalgia,52 integrating PA prescription with patient education or incorporating it into multidisciplinary intervention plans is of significance.
 |
Figure 5 Representative physical activities in different intensities and their effect on the risk of chronic widespread pain. Abbreviations: DIY, do it yourself; MET, metabolic equivalent. |
This study had several limitations. The lack of follow-up data in the included studies limited our ability to assess long-term effectiveness. Additionally, the small sample sizes in most of the analyzed studies may have weakened the statistical power of the meta-analysis; however, we mitigated the potential sources of heterogeneity through subgroup analyses. Despite the introduction of a third-party discussion to balance the inconsistency of evaluations using the RoB 2 tool, the assessment of the quality of literature may still be somewhat biased. Furthermore, because of the limited selection of GWASs related to similar topics, non-overlapping samples for MR analyses could not be used. Coupled with the presence of correlational pleiotropy in the MR Analysis, estimates of causal effects can be biased toward the observational correlation.53 Finally, all participants from the analyzed GWASs were UK residents, which could limit the generalizability of the MR results across populations with different ethnic backgrounds or from other regions. Since routine adjustments may not fully account for sample structures influenced by socioeconomic status or geographical factors,54 GWASs based solely on the UK population could also be a significant confounding factor in this study.
Conclusions
PA has been shown to be effective in reducing pain and depression, as well as in enhancing the overall quality of life of people with CWP and fibromyalgia, even without specific medications. A three-month PA intervention program should be developed and recommended for these individuals, focusing on incorporating simple and practical movements, such as Ba-Duan-Jin, to ensure feasibility and proactivity. Integrating a high-intensity exercise component, which is feasible for patients, could further enhance the intervention efficacy in managing CWP. Further research is necessary to elucidate the mechanism of action of exercise in CWP, which could lead to more targeted and effective treatment programs, ultimately improving the quality of life of patients suffering from fibromyalgia.
Abbreviations
CWP, Chronic widespread pain; PA, Physical activity; MR, Mendelian randomization; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta‐analyses; PEDro, The Physiotherapy Evidence Database; RCT, Randomized control trial; VAS, Visual analogue scale; FIQ, Fibromyalgia impact questionnaire; BDI, Beck depression inventory; RoB 2, Revised risk-of-bias tool for randomized trials; GRADE, Grading of Recommendations Assessment Development and Evaluation; MD, Mean difference; SMD, Standardized mean difference; CIs, Confidence intervals; GWAS, Genome-wide association studies; DIY, do-it-yourself; SNP, Single nucleotide polymorphism; LD, Linkage disequilibrium; IVW, Inverse-variance weighted; CAUSE, Causal analysis using summary effect estimates; LOO, Leave-one-out; OR, Odds ratio.
Data Sharing Statement
The GWAS summary statistics can be obtained from http://www.nealelab.is/uk-biobank/ and https://doi.org/10.5523/bris.2fahpksont1zi26xosyamqo8rr.
Ethics Approval and Consent to Participate
In accordance with item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China, the current study, which utilizes publicly available and legally obtained anonymized data, is exempt from ethical review.
Acknowledgments
We would like to thank all participants and investigators of the included GWAS studies for their contributions to the GWAS data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82305423, 82030121, 82274670), China Postdoctoral Science Foundation (2023M732338), Shanghai Post-doctoral Excellence Program (2022515), Yangfan Special Project of Shanghai Science and Technology Innovation Action Plan (23YF1447600), Shanghai Health System Key Supported Discipline (2023ZDFC0301), Shanghai University of TCM Science and Technology Development Project (23KFL009), Shanghai Innovative Medical Device Application Demonstration Project (23SHS05400), the Pain Relief Foundation, the National Institute for Health Research (NIHR) Clinical Lectureship (21173, 21754, and 21755), and the NIHR Manchester Biomedical Research Centre. The views expressed are those of the authors and do not necessarily represent the views of any organization or institution.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Wolfe F, Clauw DJ, Fitzcharles MA. et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheumatism. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
2. Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain. 2016;157(1):55–64. doi:10.1097/j.pain.0000000000000314
3. Staud R. Peripheral pain mechanisms in chronic widespread pain. Best Pract Res Clin Rheumatol. 2011;25(2):155–164. doi:10.1016/j.berh.2010.01.010
4. Treister-Goltzman Y, Peleg R. Fibromyalgia and mortality: a systematic review and meta-analysis. RMD Open. 2023;9(3):e003005. doi:10.1136/rmdopen-2023-003005
5. Bruce BK, Allman ME, Rivera FA, et al. Opioid use in fibromyalgia continues despite guidelines that do not support its efficacy or risk. J Clin Rheumatol. 2021;27(5):187–193. doi:10.1097/RHU.0000000000001273
6. Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29(1):120–130. doi:10.1016/j.berh.2015.04.022
7. Thieme K, Mathys M, Turk DC. Evidenced-based guidelines on the treatment of fibromyalgia patients: are they consistent and if not, why not? Have effective psychological treatments been overlooked? J Pain. 2017;18(7):747–756. doi:10.1016/j.jpain.2016.12.006
8. Vierck CJ, Staud R, Price DD, Cannon RL, Mauderli AP, Martin AD. The effect of maximal exercise on temporal summation of second pain (Windup) in patients with fibromyalgia syndrome. J Pain. 2001;2(6):334–344. doi:10.1054/jpai.2001.25533
9. Kosek E, Ekholm J, Hansson P. Modulation of pressure pain thresholds during and following isometric contraction in patients with fibromyalgia and in healthy controls. Pain. 1996;64(3):415–423. doi:10.1016/0304-3959(95)00112-3
10. Juhlin S, Mannerkorpi K, Bergenheim A. Factors promoting improvements in symptoms and health in women with fibromyalgia and chronic widespread pain: a qualitative interview study. Disability Rehabil. 2023;46(11):2234–2239. [(ahead of print)]. doi:10.1080/09638288.2023.2218655
11. Campos M, Parraga-Montilla JA, Aragon-Vela J, Latorre-Roman PA. Effects of a functional training program in patients with fibromyalgia: a 9-year prospective longitudinal cohort study. Scand J Med Sci Sports. 2020;30(5):904–913. doi:10.1111/sms.13640
12. Couto N, Monteiro D, Cid L, Bento T. Effect of diff erent types of exercise in adult subjects with fibromyalgia: a systematic review and meta-analysis of randomised clinical trials. Sci Rep. 2022;12(1):10391. doi:10.1038/s41598-022-14213-x
13. Andrade A, Dominski FH, Sieczkowska SM. What we already know about the effects of exercise in patients with fibromyalgia: an umbrella review. Semin Arthritis Rheumatism. 2020;50(6):1465–1480. doi:10.1016/j.semarthrit.2020.02.003
14. Rodríguez-Bautista JC, López-Lluch G, Rodríguez-Torres P, et al. Feasibility, safety, and effects of an aerobic training program with blood flow restriction on functional capacity, and symptomatology in women with fibromyalgia: a pilot study. Biomedicines. 2024;12(8):1895. doi:10.3390/biomedicines12081895
15. Vancampfort D, McGrath RL, Hemmings L, Gillis V, Bernar K, Van Damme T. Physical activity correlates in people with fibromyalgia: a systematic review. Disability Rehabil. 2023;45(25):4165–4174. doi:10.1080/09638288.2022.2146911
16. Lazaridou A, Paschali M, Schreiber K, et al. The association between daily physical exercise and pain among women with fibromyalgia: the moderating role of pain catastrophizing. Pain Rep. 2020;5(4):e832. doi:10.1097/PR9.0000000000000832
17. Hu X-Y, Young B, Santer M, et al. Self-management interventions for chronic widespread pain including fibromyalgia: a systematic review and qualitative evidence synthesis. Pain. 2024;166(3):e36–e50. doi:10.1097/j.pain.0000000000003379
18. Luo DH, Wan X, Liu JM, Tong TJ. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Statistical Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
19. Wan X, Wang WQ, Liu JM, Tong TJ. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Method. 2014;14(1):135. doi:10.1186/1471-2288-14-135
20. Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. (editors): Cochrane handbook for systematic reviews of interventions version 6.4 (updated August 2023). 2023.
21. Elsworth B, Mitchell R, Raistrick CA, Paternoster L, Hemani G, Gaunt TR. MRC IEU UK Biobank GWAS pipeline version 1. In. 2017.
22. Burgess S, Davies NM, Thompson SG. Bias due to participant overlap in two-sample Mendelian randomization. Genetic Epidemiol. 2016;40(7):597–608. doi:10.1002/gepi.21998
23. Hemani G, Zhengn J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408. doi:10.7554/eLife.34408
24. Codd V, Nelson CP, Albrecht E, et al. Identification of seven loci affecting mean telomere length and their association with disease. Nature Genet. 2013;45(4):422–427. doi:10.1038/ng.2528
25. Morrison J, Knoblauch N, Marcus JH, Stephens M, He X. Mendelian randomization accounting for correlated and uncorrelated pleiotropic effects using genome-wide summary statistics. Nature Genet. 2020;52(7):740–747. doi:10.1038/s41588-020-0631-4
26. Izquierdo-Alventosa R, Inglés M, Cortés-Amador S, et al. Low-intensity physical exercise improves pain catastrophizing and other psychological and physical aspects in women with fibromyalgia: a randomized controlled trial. Int J Environ Res Public Health. 2020;17(10):3634. doi:10.3390/ijerph17103634
27. Villafaina S, Collado-Mateo D, Dominguez-Munoz FJ, Fuentes-Garcia JP, Gusi N. Benefits of 24-week exergame intervention on health-related quality of life and pain in women with fibromyalgia: a single-blind, randomized controlled trial. Games Health J. 2019;8(6):380–386. doi:10.1089/g4h.2019.0023
28. Collado-Mateo D, Dominguez-Muñoz FJ, Adsuar JC, Garcia-Gordillo MA, Gusi N. Effects of exergames on quality of life, pain, and disease effect in women with fibromyalgia: a randomized controlled trial. Arch Phys Med Rehabil. 2017;98(9):1725–1731. doi:10.1016/j.apmr.2017.02.011
29. Hernando-Garijo I, Ceballos-Laita L, Mingo-Gómez MT, et al. Immediate effects of a telerehabilitation program based on aerobic exercise in women with fibromyalgia. Int J Environ Res Public Health. 2021;18(4):2075. doi:10.3390/ijerph18042075
30. Rodríguez-Mansilla J, Mejías-Gil A, Garrido-Ardila EM, Jiménez-Palomares M, Montanero-Fernández J, González-López-Arza MV. Effects of an exercise for well-being and physical training programme on muscle strength, range of movement, respiratory capacity and quality of life in women with fibromyalgia: a randomized controlled trial. J Clin Med. 2023;12(3):774. doi:10.3390/jcm12030774
31. Jiao J, Russell IJ, Wang W, Wang J, Zhao YY, Jiang Q. Ba-Duan-Jin alleviates pain and fibromyalgia-related symptoms in patients with fibromyalgia: results of a randomised controlled trial. Clin Exp Rheumatol. 2019;37(6):953–962.
32. Yayun Z. The effect of Lu Eight Brocades in the treament of fibromyalgia syndrome: a clinical trial. 2016.
33. Assumpçao A, Matsutani LA, Yuan SL, et al. Muscle stretching exercises and resistance training in fibromyalgia: which is better? A three-arm randomized controlled trial. Eur J Phys Rehabil Med. 2018;54(5):663–670. doi:10.23736/S1973-9087.17.04876-6
34. Andrade CP, Zamunér AR, Forti M, Tamburús NY, Silva E. Effects of aquatic training and detraining on women with fibromyalgia: controlled randomized clinical trial. Eur J Phys Rehabil Med. 2019;55(1):79–88. doi:10.23736/S1973-9087.18.05041-4
35. Giannotti E, Koutsikos K, Pigatto M, Rampudda ME, Doria A, Masiero S. Medium-/long-term effects of a specific exercise protocol combined with patient education on spine mobility, chronic fatigue, pain, aerobic fitness and level of disability in fibromyalgia. Biomed Res. Int. 2014;2014:474029. doi:10.1155/2014/474029
36. Norouzi E, Hosseini F, Vaezmosavi M, Gerber M, Pühse U, Brand S. Zumba dancing and aerobic exercise can improve working memory, motor function, and depressive symptoms in female patients with Fibromyalgia. Eur J Sport Sci. 2020;20(7):981–991. doi:10.1080/17461391.2019.1683610
37. Xiao CM, Zhuang YC. Effect of health Baduanjin Qigong for mild to moderate Parkinson’s disease. Geriatrics Gerontol Int. 2016;16(8):911–919. doi:10.1111/ggi.12571
38. Gupta A, McBeth J, Macfarlane GJ, et al. Pressure pain thresholds and tender point counts as predictors of new chronic widespread pain in somatising subjects. Ann Rheumatic Dis. 2007;66(4):517–521. doi:10.1136/ard.2006.054650
39. Neelapala YVR, Mercuri D, Macedo L, Hanna S, Kobsar D, Carlesso L. Mechanisms hypothesized for pain-relieving effects of exercise in fibromyalgia: a scoping review. Therapeutic Adv Musculoskeletal Dis. 2023;15: 1759720X231182894. doi:10.1177/1759720X231182894
40. Bernik M, Sampaio TPA, Gandarela L. Fibromyalgia comorbid with anxiety disorders and depression. Combined Med Psycholl Treatment Curr Pain and Headache Rep. 2013;17(9):358. doi:10.1007/s11916-013-0358-3
41. Zeng ZP, Liu YB, Fang JJ, Liu Y, Luo J, Yang M. Effects of Baduanjin exercise for knee osteoarthritis: a systematic review and meta-analysis. Complementary Ther Med. 2020;48:102279. doi:10.1016/j.ctim.2019.102279
42. Ong WY, Stohler CS, Herr DR. Role of the prefrontal cortex in pain processing. mol Neurobiol. 2019;56(2):1137–1166. doi:10.1007/s12035-018-1130-9
43. Busch AJ, Webber SC, Brachaniec M, et al. Exercise therapy for fibromyalgia. Curr Pain Headache Rep. 2011;15(5):358–367. doi:10.1007/s11916-011-0214-2
44. Albuquerque MLL, Monteiro D, Marinho DA, Vilarino GT, Andrade A, Neiva HP. Effects of different protocols of physical exercise on fibromyalgia syndrome treatment: systematic review and meta-analysis of randomized controlled trials. Rheumatology International. 2022;42(11):1893–1908. doi:10.1007/s00296-022-05140-1
45. Zetterman T, Nieminen AI, Markkula R, Kalso E, Lotsch J. Machine learning identifies fatigue as a key symptom of fibromyalgia reflected in tyrosine, purine, pyrimidine, and glutaminergic metabolism. Clin. Transl. Sci. 2024;17(3):e13740. doi:10.1111/cts.13740
46. Kingsbury C, Karelis AD, Hains-Monfette G, Bernard P. Association between daily level of objective physical activity and C-Reactive protein in a representative national sample of adults with self-reported diagnosed arthritis or fibromyalgia. Rheumatology International. 2020;40(9):1463–1471. doi:10.1007/s00296-020-04571-y
47. Pang L, Chen X, Lan Y, et al. Research progress of acupuncture analgesia based on autonomic nerve regulation pathway. Acupuncture and Herbal Med. 2023;3(4):285–295. doi:10.1097/HM9.0000000000000087
48. Borges L, Dermargos A, Gray S, et al. Neutrophil migration and adhesion molecule expression after acute high-intensity street dance exercise. J Immunol Res. 2018;2018:1684013. doi:10.1155/2018/1684013
49. Park SA, Lee AY, Lee HS, Lee KS, Son KC. A comparison of exercise intensity between two horticultural and four common physical activities among male adults in their 20s. Korean J Horticultural Sci Technol. 2015;33(1):133–142. doi:10.7235/hort.2015.14084
50. Mendes MD, da Silva I, Ramires V, et al. Metabolic equivalent of task (METs) thresholds as an indicator of physical activity intensity. PLoS One. 2018;13(7):e0200701. doi:10.1371/journal.pone.0200701
51. Herrmann SD, Willis EA, Ainsworth BE, et al. 2024 adult compendium of physical activities: a third update of the energy costs of human activities. J Sport Health Sci. 2024;13(1):6–12. doi:10.1016/j.jshs.2023.10.010
52. Antunes MD, Schmitt ACB, Marques AP. Amigos de fibro (fibro friends): validation of an educational program to promote health in fibromyalgia. Int J Environ Res Public Health. 2022;19(9):5297. doi:10.3390/ijerph19095297
53. Mounier N, Kutalik Z. Bias correction for inverse variance weighting Mendelian randomization. Genetic Epidemiol. 2023;47(4):314–331. doi:10.1002/gepi.22522
54. Hu XH, Zhao J, Lin ZX, et al. Mendelian randomization for causal inference accounting for pleiotropy and sample structure using genome-wide summary statistics. Proc Natl Acad Sci USA. 2022;119(28). doi:10.1073/pnas.2106858119
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.