")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Effect of Sodium–Glucose Cotransporter 2 Inhibitors on Cardiovascular Outcomes in Patients with Acute Coronary Syndrome and Type 2 Diabetes
Received 20 February 2024
Accepted for publication 25 June 2024
Published 22 November 2024 Volume 2024:17 Pages 4377—4386
DOI https://doi.org/10.2147/DMSO.S459368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Han Xie,1,2 Ming-Jian Jiang3
1Department of Cardiovascular Medicine, The Central Hospital of Wuhan, Wuhan, People’s Republic of China; 2Key Laboratory for Molecular Diagnosis of Hubei Province, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430014, People’s Republic of China; 3Department of Cardiovascular Medicine, Huangshi Aikang Hospital in Hubei Province, Wuhan, People’s Republic of China
Correspondence: Ming-Jian Jiang, Department of Cardiovascular Medicine, Huangshi Aikang Hospital in Hubei Province, No. 563 of Yiyang Road,Xisaishan District, Huangshi, 430051, People’s Republic of China, Tel +86-13677149029, Email [email protected]
Objective: To investigate the effect of sodium–glucose cotransporter 2 inhibitors (SGLT2i) on cardiovascular outcomes in patients with acute coronary syndrome (ACS) and type 2 diabetes (T2D).
Methods: The clinical data of 88 patients with ACS and T2D who were treated with SGLT2i between January 2020 and December 2021 were collected as the case group through convenience sampling. Patients taking other hypoglycaemic drugs were included as the control group in a 1:1 ratio matched with the case group using retrospective propensity score matching. Relevant data were subsequently collected from both groups for comparison.
Results: Statistically significant differences were observed in glycated haemoglobin (HbA1c) between the two groups (8.11[6.93, 9.41] vs 7.51[6.52, 9.14]%; Z=2.109; P=0.035). The SGLT2i group showed a decrease in major adverse cardiovascular events (MACEs) (P< 0.001), secondary composite endpoint events (P=0.024), heart failure readmission (P=0.042) and unplanned revascularisation (P=0.014) compared with the control group. Moreover, the multivariate analysis showed that SGLT2i significantly reduced the risk of MACEs (hazard ratio [HR], 0.472; 95% CI, 0.321– 0.694; P< 0.001) and unplanned revascularisation (HR, 0.422; 95% CI, 0.212– 0.842; P=0.014). In patients with reduced ejection fraction, SGLT2i significantly reduced the risk of MACEs (HR, 0.258; 95% CI, 0.106– 0.626; P=0.003) compared with the control group. By contrast, in patients without reduced ejection fraction, SGLT2i significantly reduced the risk of MACEs (HR, 0.640; 95% CI, 0.412– 0.996; P=0.048) and unplanned revascularisation (HR, 0.464; 95% CI, 0.222– 0.969; P=0.041) compared with the control group.
Conclusion: In addition to significantly reducing the risk of adverse cardiovascular events and unplanned revascularisation in patients with ACS and T2D, the use of SGLT2i can reduce the risk of adverse cardiovascular events regardless of the presence of reduced ejection fraction.
Keywords: sodium–glucose cotransporter 2 inhibitors, acute coronary syndrome, type 2 diabetes, cardiovascular outcomes
Introduction
Atherosclerotic heart disease has always been the leading cause of death among patients with cardiovascular disease (CVD) in China.1 Cardiovascular disease has become one of the major complications of type 2 diabetes (T2D), accounting for at least 50% of the deaths of patients with T2D.2 Acute coronary syndrome (ACS) is the most serious type of CVD, including ST segment elevation myocardial infarction (STEMI), non-ST-segment elevation myocardial infarction (NSTEMI) and unstable angina (UA) pectoris.3 It is reported that people with T2D are three times more likely to experience ACS than healthy people.4 Moreover, CVD is the main cause of death in patients with T2D, which is also a major contributor to unfavourable prognosis in patients with CVD.5,6 The IDF Diabetes Atlas released by the International Diabetes Federation in 2019 shows that there are approximately 128.9 million patients with diabetes in China.7,8 Compared with healthy individuals, patients with diabetes have a 2–4 times higher prevalence of CVD.9 Therefore, the primary goal of treatment is to effectively control the diabetes, improve cardiovascular outcomes in patients with diabetes, mitigate the occurrence of adverse cardiovascular events and reduce the risk of death in these patients.
Sodium–glucose cotransporter 2 inhibitors (SGLT2i) are a novel type of hypoglycaemic drug. Recent clinical studies have shown that SGLT2i significantly improve the risk of cardiovascular events in patients with T2D compared with traditional hypoglycaemic drugs10,11 and have cardiovascular protective effects.12 Additionally, several large-scale clinical randomised controlled trials on SGLT2i have demonstrated their potential cardiovascular benefits. In addition, the EMPA-REG study demonstrated that empagliflozin reduced the risk of major adverse cardiovascular events (MACEs), which include acute myocardial infarction, cardiac death and ischemic stroke, and all-cause mortality in patients with T2D at high risk of CVD.13 The CANVAS study suggested that canagliflozin reduces the risk of MACEs in patients with T2D at high risk of CVD.14 Moreover, the DECLARE-TIMI58 study showed that dapagliflozin exhibited no significant effect on the occurrence of MACEs but effectively reduced the occurrence of cardiac death and heart failure readmission in patients with atherosclerotic heart disease or at high-risk of T2D, whereas the DECLARE-HF study involving patients with heart failure with reduced ejection fraction demonstrated that dapagliflozin significantly improved the outcome of heart failure readmission.15,16 Based on the cardiovascular benefits demonstrated by SGLT2i in these studies, these inhibitors have been recommended as a first-line treatment for patients with T2D combined with atherosclerotic heart disease to reduce the risk of developing cardiovascular complications. They have also been recommended by the European Society of Cardiology for improving cardiovascular outcomes and preventing adverse cardiovascular events in patients with heart failure with reduced ejection fraction.17–19
Studies have indicated that SGLT2i can significantly improve the prognosis of patients with heart failure with reduced ejection fraction. Based on these findings, SGLT2i are recommended for the treatment of patients with T2D with concomitant atherosclerotic heart disease along with the recommendation of dapagliflozin for treating patients with heart failure with reduced ejection fraction. Moreover, randomised controlled studies involving patients with T2D and a history of myocardial infarction have revealed that SGLT2i can significantly reduce the risk of MACEs, cardiac death or heart failure readmission in these patients.
However, there remains a lack of real-world research evidence regarding the effect of SGLT2i on cardiovascular outcomes in patients with ACS and T2D. Therefore, this study explores the effect of SGLT2i on cardiovascular outcomes in this patient population while further investigating whether the presence or absence of reduced ejection fraction (ie left ventricular ejection fraction ≤40%) has different effects on cardiovascular outcomes.
Study Participants and Methods
Study Participants
The clinical data of 88 patients with ACS complicated with T2D following percutaneous coronary intervention who were treated with SGLT2i between January 2020 and December 2021 in our hospital were collected as the case group using the convenience sampling method. The patients in the case group had taken SGLT2i regularly for at least 3 months prior to admission. Patients who took other hypoglycaemic drugs were selected and included as the control group in a 1:1 ratio matched with the case group using retrospective propensity score matching. Matching factors included gender, age, smoking history, duration of diabetes, history of hypertension, history of abnormal lipid metabolism, type of coronary heart disease, presence of heart failure upon admission and medication treatment (including antiplatelet drugs, lipid-lowering drugs, antihypertensive drugs and hypoglycaemic drugs).
The inclusion criteria were as follows: (1) age ≥18 years; (2) patients hospitalised with a confirmed diagnosis of ACS (including UA, acute NSTEMI and acute STEMI), with the criteria for diagnosis being patients with at least one coronary artery stenosis ≥50% identified through computed tomography coronary angiography or coronary angiography; (3) patients hospitalised with a confirmed diagnosis of T2D, with the criteria for diagnosis being diabetic symptoms (including polyuria, polydipsia, polyphagia and unexplained weight loss), and either random plasma glucose levels >11.1 mmol/l (200 mg/dl) or fasting blood glucose levels >7.0 mmol/l (126 mg/dl) or 2-hour plasma glucose levels >11.1 mmol/l (200 mg/dl) during oral glucose tolerance testing (with 75 g of anhydrous glucose load) and regular use of hypoglycaemic drugs for hypoglycaemic treatment.
The exclusion criteria were as follows: (1) patients with type 1 diabetes; (2) patients with other severe heart diseases, such as severe valvular heart disease or severe dilated cardiomyopathy; (3) patients with more than one episode of hypoglycaemia following the use of other hypoglycaemic drugs or insulin in the past 6 months; (4) patients with more than one instance of estimated glomerular filtration rate (eGFR) <30 mL/min/1.73m2 during hospitalisation (calculated using the MDRD formula); (5) patients with hemodynamic instability (ie more than one instance of systolic blood pressure <100 mmHg monitored during hospitalisation); (6) patients with other malignant underlying diseases (eg malignant tumours, immune system diseases) and with an expected survival time of less than 1 year; and (7) patients who died during hospitalisation.
Study Methods
The follow-up began from the date of patient discharge and continued for 1 year of regular medication. Patient endpoint events were recorded through outpatient follow-up medical records or contact via telephone, with the occurrence time of the endpoint events also documented.
Endpoint events during follow-up were divided into MACEs and three secondary endpoint events. Specifically, MACEs included acute myocardial infarction, cardiac death, ischemic stroke, heart failure readmission and unplanned revascularisation. The three secondary endpoint events were (1) a secondary composite endpoint (SCE) consisting of acute myocardial infarction, cardiac death and ischemic stroke; (2) heart failure readmission; and (3) unplanned revascularisation.
Cardiac death refers to death caused by cardiac problems where other non-cardiac causes can clearly be excluded.13 Acute myocardial infarction is defined as recurrent symptoms, with dynamic changes in the electrocardiogram of new-onset symptoms and changes in the markers of myocardial infarction consistent with the condition diagnosis.15 Ischemic stroke refers to symptoms or signs of neurological damage, supported by imaging examination findings indicating the diagnosis of new stroke lesions.15 Heart failure readmission refers to the reappearance of heart failure symptoms, with heart failure markers and cardiac ultrasound results supporting the diagnosis of heart failure upon readmission.16 Unplanned revascularisation refers to percutaneous coronary intervention due to frequent episodes of UA pectoris.
Data Collection
General data and clinical data of the patients were collected. The general data included gender, age, smoking history, history of hypertension, history of cerebrovascular disease, history of lipid metabolism disorders and type of coronary heart disease. The clinical data included left ventricular ejection fraction, B-type natriuretic peptide, glycated haemoglobin (HbA1c), body mass index (BMI), eGFR, history of percutaneous coronary intervention, use of antiplatelet drugs, use of statin lipid-lowering drugs, use of angiotensin receptor-neprilysin inhibitor drugs, use of antihypertensive drugs, use of metformin, use of acarbose, use of insulin, use of dipeptidyl peptidase-4 inhibitors and use of glucagon-like peptide-1 receptor agonists.
Statistical Analysis
The statistical analysis was performed using SPSS 26.0 software ((IBM Corp., Armonk, N.Y., USA). Normality was tested using the Kolmogorov–Smirnov method, with normally distributed measurement data expressed as mean ± standard deviation and intergroup mean comparisons conducted using the t-test. Count data were expressed as frequency (n) or rate (%) and analysed using the chi-square (χ2) test. The skewed distribution data were compared through the Kruskal–Wallis H rank sum test. Logistic multivariate regression was utilised for propensity score matching of the SGLT2i group and the control group in a 1:1 ratio. Kaplan–Meier curves were used to plot the survival curves of various endpoint events at 1-year follow-up, whereas the log rank test was applied for the intergroup comparison of survival functions. Additionally, Cox risk regression analysis was utilised to explore the relevant risk factors of patients. The significance level was set at α=0.05.
Results
General Data
The findings showed that the SGLT2i group consisted of 56 men and 32 women, with an average age of 65.94±12.61 years and an average BMI of 24.57±3.47 kg/m2. By comparison, the control group included 45 men and 43 women, with an average age of 64.37±11.47 years and an average BMI of 23.87±3.12 kg/m2. Statistically significant differences were observed in HbA1c (8.11 [6.93, 9.41] vs 7.51 [6.52, 9.14]%, Z=2.109, P=0.035) between the two groups. However, there were no statistically significant differences in gender, BMI, age, smoking history, duration of diabetes, history of hypertension, history of cerebrovascular disease, history of lipid metabolism disorders or type of ACS between the two groups (P>0.05), as shown in Table 1.
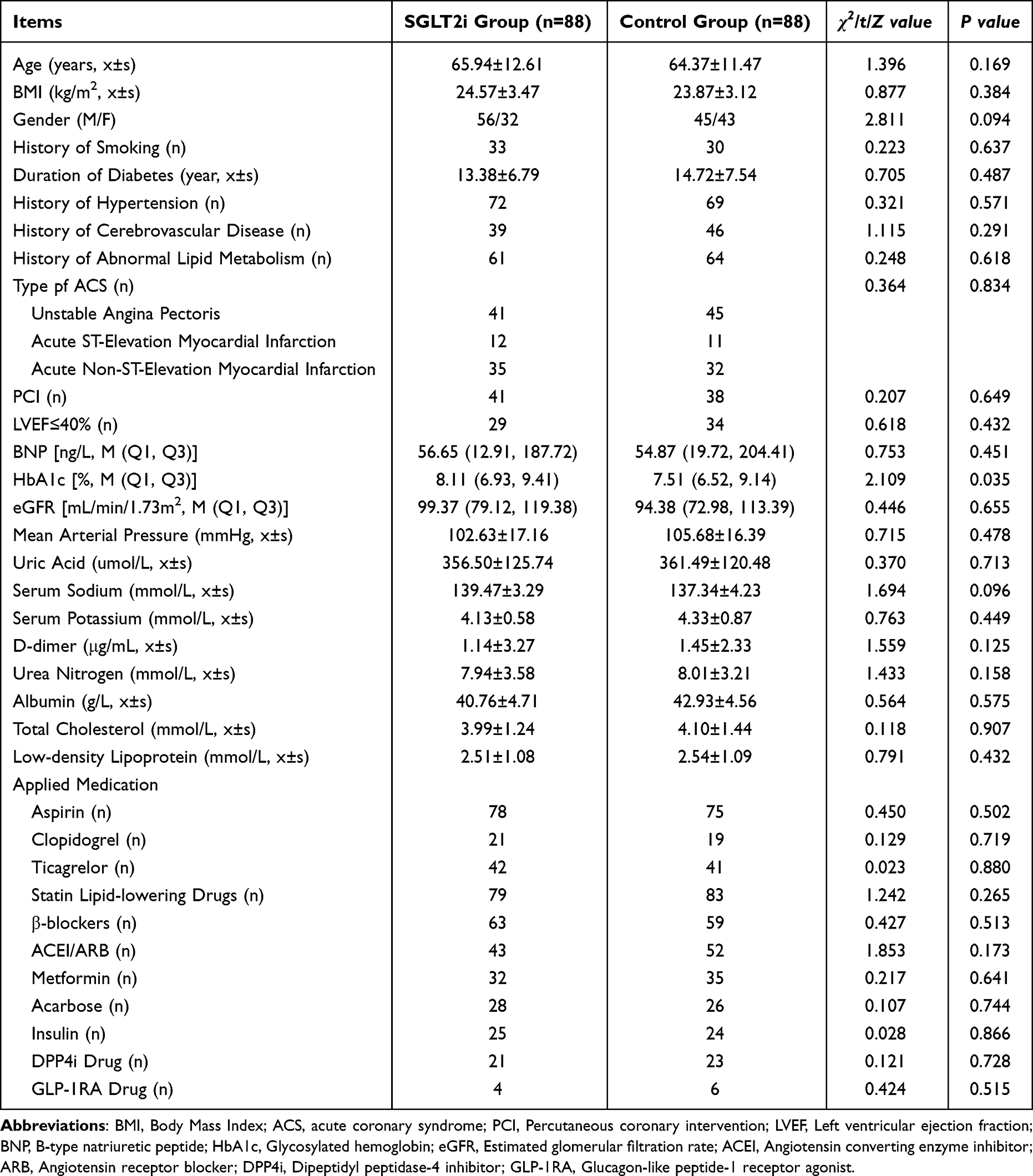 |
Table 1 General Data |
Outcome Events in the Two Groups
Follow-up of the occurrence of outcome events in the two groups after 1 year of drug treatment and survival analysis revealed that the SGLT2i group had a lower incidence of MACEs (12.5% vs 25.0%, P<0.001), and unplanned revascularisation (3.4% vs 9.1%, P=0.014) compared with the control group, and the differences in the incidence between the two groups were statistically significant (Figures 1 and 2). However, no statistically significant differences were found in the comparison of the incidence of acute myocardial infarction, heart failure readmission, all-cause death, ischemic stroke, or SCES between the two groups (P>0.05) (Figure 2).
 |
Figure 1 K-M Curves of Outcome Events with Statistically Significant Differences between the 2 Groups. Note: MACE: Major adverse cardiovascular event (including acute myocardial infarction, all-cause mortality, ischemic stroke, heart failure readmission, and unplanned revascularization); SCE: Secondary composite endpoint. |
 |
Figure 2 Forest Plot of Patient Outcome Events in the 2 Groups. Note: MACE: Major adverse cardiovascular event (including acute myocardial infarction, all-cause mortality, ischemic stroke, heart failure readmission, and unplanned revascularization); SCE: Secondary composite endpoint; HR: Hazard ratio; 95% CI: 95% confidence interval. |
Cox risk regression analysis was performed on outcome events with statistically significant differences between the two groups (including variables such as grouping, gender, age, smoking history, diagnosis, presence of heart failure, HbA1c, BMI, eGFR and use of metformin and statin lipid-lowering drugs). The analysis revealed that patients in the SGLT2i group had a significantly lower risk of MACEs (hazard ratio [HR]=0.472; 95% CI, 0.321–0.694; P<0.001) and unplanned revascularisation (HR=0.422; 95% CI, 0.212–0.842; P=0.014) compared with the control group, with statistical significance. Despite no statistically significant differences in the occurrence risk of SCEs (HR=0.563; 95% CI, 0.315–1.006; P=0.053) and readmission for heart failure (HR=0.419; 95% CI, 0.173–1.018; P=0.055) between the SGLT2i group and the control group, the use of SGLT2i reduced the risk of SCEs and readmission for heart failure by 44% and 49%, respectively (Figure 2).
Ejection Fraction Subgroup Analysis
Following propensity score matching, all patients were divided into two subgroups (one with reduced ejection fraction and one without reduced ejection fraction) based on whether the left ventricular ejection fraction was <40%. The subgroup with reduced ejection fraction included a total of 63 patients (SGLT2i group: n=29; control group: n=34), whereas that without reduced ejection fraction included a total of 113 patients (SGLT2i group: n=59; control group: n=54).
The survival analysis of outcome events in the subgroup with reduced ejection fraction revealed no statistically significant difference (P>0.05) in the occurrence of SCEs and unplanned revascularisation compared with the control group. In addition, Cox risk regression analysis was performed on outcome events with statistically significant differences between the two groups, indicating a significantly reduced risk of MACEs in patients of the SGLT2i group (HR=0.258; 95% CI, 0.106–0.626; P=0.003) compared with the control group, with statistically significant differences. Despite no statistically significant differences in the risk of heart failure readmission between the SGLT2i group and the control group (HR=0.133; 95% CI, 0.017–1.017; P=0.052), the use of SGLT2i reduced the risk by 84% (Figure 3).
 |
Figure 3 Forest Plot of Patient Outcome Events in Subgroups. Note: MACE: Major adverse cardiovascular event (including acute myocardial infarction, all-cause mortality, ischemic stroke, heart failure readmission, and unplanned revascularization); LVEF: left ventricular ejection fraction; SCE: Secondary composite endpoint; HR: hazard ratio; 95% CI: 95% confidence interval. |
By contrast, the survival analysis of outcome events in the subgroup without reduced ejection fraction showed no statistically significant differences (P>0.05) in reduced occurrence of SCEs and heart failure readmission between the SGLT2i and control groups. Cox risk regression analysis was performed on outcome events with statistically significant differences between the two groups, revealing that the SGLT2i group had a significantly lower risk of MACEs (HR=0.640; 95% CI, 0.412–0.996; P=0.048) and unplanned revascularisation (HR=0.464; 95% CI, 0.222–0.969; P=0.041) than the control group, and the differences were statistically significant (Figure 3).
Discussion
Based on the overall findings, the multivariate risk regression analysis demonstrated that SGLT2i can significantly reduce the risk of MACEs and unplanned revascularisation in patients with ACS and T2D, with statistically significant differences. It also reduces the occurrence risk of SCEs and heart failure readmission. Moreover, the use of statin lipid-lowering drugs, an age less than 65 years and no history of acute myocardial infarction are also influencing factors in reducing the risk of SCEs. Reduced ejection fraction also increases the risk of heart failure readmission in patients. Several large-scale randomised controlled trials on the cardiovascular outcomes of SGLT2i have also demonstrated their cardiovascular protective effects in patients with T2D.13–15 Studies on dapagliflozin in patients with chronic heart failure with reduced ejection fraction alone have shown its cardiovascular protective effects independent of its glycaemic control.16 However, a subgroup analysis of the DECLARE-TIMI58 study showed that dapagliflozin reduced the relative risk of MACEs (including acute myocardial infarction, cardiac death, ischemic stroke) in patients with a history of myocardial infarction and T2D by 16%, with an absolute risk reduction of 2.6% (15.2% vs 17.8%, HR=0.84; 95% CI, 0.72–0.99; P=0.039), thereby reducing the absolute risk of cardiac death or heart failure readmission by 1.9% (8.6% vs 10.5%; HR=0.81; 95% CI, 0.65–1.00; P=0.046).20
A large number of studies have demonstrated the protective effect of strict control of blood glucose on the heart. Strict glycaemic control can play a cardioprotective role through anti-inflammatory and anti-apoptotic mechanisms, anti-oxidative stress, endothelial protection, free fatty acid reduction, anti-glucotoxicity, IR and cardiac fuel metabolism improvement, cardiac stem cell protection and activation of adrenergic system reduction.21–23 As a new hypoglycaemic drug, SGLT2i can significantly reduce the occurrence risk of ischemic heart disease in patients with T2D.24 Moreover, research involving ischemia-reperfusion animal models and cellular-level experiments has confirmed that SGLT2i can alleviate cardiac remodelling and the occurrence of heart failure following myocardial infarction.25,26 Furthermore, research by Lahnwong et al involving rats with acute myocardial ischemia-reperfusion injury confirmed that dapagliflozin may exhibit cardiovascular protective effects by improving myocardial infarct size, increasing left ventricular function and reducing arrhythmias.26 Potential mechanisms may include the delayed progression of diabetes, improved myocardial energy metabolism, activated cardiac protection mechanisms to counteract the remodelling process, myocardial anti-fibrotic and anti-apoptotic effects, potential anti-inflammatory mechanisms and direct interactions with cardiomyocytes.27 These studies have demonstrated the SGLT2i-induced improvement in myocardial ischemic symptoms from multiple perspectives, consistent with the findings of the present study.
In the analysis of the subgroup with reduced ejection fraction, SGLT2i significantly reduced the occurrence risk of MACEs. It is speculated that the underlying molecular mechanism is that the significant decrease in intracellular sodium levels induced by SGLT2i improves cardiac contractility and dysfunction. This is considered to be the key molecular mechanism for SGLT2i’s role in cardio protection, especially in reducing the risk of heart failure and protecting the cardiac function of patients with heart failure from further deterioration.28 Moreover, in patients with T2D, SGLT2i prevents the upregulation of SGLT2 expression in endothelial cells and reduces oxidative stress, pro-inflammatory cytokines and the content of myocardial interstitial collagen.29,30 It effectively prevents the risk of acute ischemic events caused by inflammation-dependent atherosclerotic plaque rupture.31
However, the present study found no statistically significant reduction in the occurrence risk of heart failure readmission compared with the control group. This differs from the findings of the DAPA-HF study, which showed a reduced risk of heart failure readmission in patients with New York Heart Association cardiac function ≥class II or left ventricular ejection fraction ≤40%. It is hypothesised that this may be due to the relatively fewer recorded occurrences of outcome events.
By comparison, the analysis of the subgroup without reduced ejection fraction showed that SGLT2i significantly reduced the occurrence risk of MACEs and unplanned revascularisation compared with the control group, without affecting the occurrence of SCEs and heart failure readmission. The multivariate risk regression analysis also suggested that a history of acute myocardial infarction is an independent influencing factor for the occurrence of SCEs. A clinical cohort study on the effect of SGLT2i on ischemic cardiomyopathy found that SGLT2i reduced the incidence risk of ischemic cardiomyopathy in patients with T2D, which was significant at 6 months of follow-up.32 Additionally, the effect of SGLT2i on reducing the risk of unplanned revascularisation in patients with coronary artery disease and T2D was also observed in this study, further confirming the ameliorative effect of SGLT2i on ischemic symptoms. The increased excretion of urinary glucose and sodium by SGLT2i, as well as its reduction in blood volume and alleviation of volume load, may be associated with the reduction in the occurrence risk of ischemic events.22 Moreover, relevant animal experiments have also confirmed that SGLT2i can improve vascular endothelial and smooth muscle cell function while alleviating oxidative stress and inflammatory responses.23 These effects all contribute positively to improving adverse cardiovascular outcomes in patients using SGLT2i.
However, this study has some limitations. First, this was a single-centre observational study and no intervention was performed throughout the study, meaning it may not be strong enough to define a cause–effect relationship. Second, detailed information on glycaemic control of the patients was not obtained during the 1-year clinical follow-up, resulting in a lack of comparison between the efficacy of glycaemic control between SGLT2i and other hypoglycaemic drugs. Third, it was difficult for the outcome events to develop due to the insufficient sample size of the SGLT2i group in the subgroup with reduced ejection fraction, thereby affecting the stability of the study results. It is suggested that the sample size be expanded in future studies and more prospective intervention studies be conducted to further demonstrate the conclusions of this study.
Conclusion
In conclusion, the application of SGLT2i can significantly reduce the occurrence risk of MACEs, SCEs, heart failure readmission and unplanned revascularisation compared with other hypoglycaemic drugs. Specifically, SGLT2i can reduce the occurrence risk of MACEs and heart failure readmission in patients with reduced ejection fraction while also significantly reducing the occurrence risk of MACE and unplanned revascularisation in those without reduced ejection fraction.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of Huangshi Aikang Hospital in Hubei Province.Written informed consent was obtained from all participants.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any funding support.
Disclosure
The authors declare that they have no competing interests.
References
1. Eder S, Leierer J, Kerschbaum J, et al. Guidelines and clinical practice at the primary level of healthcare in patients with type 2 diabetes mellitus with and without kidney disease in five European countries. Diab Vasc Dis Res. 2019;16(1):47–56. doi:10.1177/1479164118795559
2. Ma CX, Ma XN, Guan CH, Li YD, Mauricio D, Fu SB. Cardiovascular disease in type 2 diabetes mellitus: progress toward personalized management. Cardiovasc Diabetol. 2022;21(1):74. doi:10.1186/s12933-022-01516-6
3. Liu T, Fan Z, Xiao B, He C, Wang S. Association of sodium-glucose cotransporter 2 inhibitors with risk of major adverse cardiovascular events in type 2 diabetes patients with acute coronary syndrome: a propensity score‑matched analysis. Cardiovasc Diabetol. 2024;23(1):106. doi:10.1186/s12933-024-02200-7
4. Babes EE, Bustea C, Behl T, et al. Acute coronary syndromes in diabetic patients, outcome, revascularization, and antithrombotic therapy. Biomed Pharmacother. 2022;148:112772. doi:10.1016/j.biopha.2022.112772
5. Tesfaye A, Josef H, Wube TB, et al. Magnitude of, and factors associated with cardiovascular disease among type two diabetes mellitus patients. Diabetes Metab Syndr Obes. 2020;13:4123–4129. doi:10.2147/DMSO.S254883
6. Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339(4):229–234. doi:10.1056/NEJM199807233390404
7. Chinese Diabetes Society, Chinese Medical Association. Chinese guidelines for the prevention and treatment of type 2 Diabetes (2017 Edition). Chin J Pract Internal Med. 2018;38(4):292–344. doi:10.3760/cma.j.issn.1674-5809.2018.01.003
8. Guo L. The epidemic situation and intervention strategies of diabetes mellitus. Chin J Clin Healthcare. 2020;23(4):433–436. doi:10.3969/J.issn.1672-6790.2020.04.001
9. Fox CS, Coady S, Sorlie PD, et al. Increasing cardiovascular disease burden due to diabetes mellitus: the Framingham heart study. Circulation. 2007;115(12):1544–1550. doi:10.1161/CIRCULATIONAHA.106.658948
10. Cosmi F, Shen L, Magnoli M, et al. Treatment with insulin is associated with worse outcome in patients with chronic heart failure and diabetes. Eur J Heart Fail. 2018;20(5):888–895. doi:10.1002/ejhf.1146
11. Roumie CL, Min JY, D’Agostino McGowan L, et al. Comparative safety of sulfonylurea and metformin monotherapy on the risk of heart failure: a cohort study. J Am Heart Assoc. 2017;6(4):e005379. doi:10.1161/JAHA.116.005379
12. Sarafidis PA, Tsapas A. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2016;374(11):1092. doi:10.1056/NEJMc1600827
13. Zinman B, Wanner C, Lachin JM, EMPA-REG OUTCOME Investigators, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi:10.1056/NEJMoa1504720
14. Neal B, Perkovic V, Mahaffey KW, CANVAS Program Collaborative Group, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
15. Wiviott SD, Raz I, Bonaca MP, DECLARE–TIMI 58 Investigators, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/NEJMoa1812389
16. McMurray JJV, Solomon SD, Inzucchi SE, DAPA-HF Trial Committees and Investigators, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995–2008. doi:10.1056/NEJMoa1911303
17. McGuire DK, Shih WJ, Cosentino F, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol. 2021;6(2):148–158. doi:10.1001/jamacardio.2020.4511
18. Patorno E, Pawar A, Franklin JM, et al. Empagliflozin and the risk of heart failure hospitalization in routine clinical care. Circulation. 2019;139(25):2822–2830. doi:10.1161/CIRCULATIONAHA.118.039177
19. Seino Y, Kim DJ, Yabe D, EMPRISE East Asia study group, et al. Cardiovascular and renal effectiveness of empagliflozin in routine care in East Asia: results from the EMPRISE East Asia study. Endocrinol Diabetes Metab. 2020;4(1):e00183. doi:10.1002/edm2.183
20. Furtado RHM, Bonaca MP, Raz I, et al. Dapagliflozin and cardiovascular outcomes in patients with type 2 diabetes mellitus and previous myocardial infarction. Circulation. 2019;139(22):2516–2527. doi:10.1161/CIRCULATIONAHA.119.039996
21. Caturano A, Galiero R, Pafundi PC, et al. Does a strict glycemic control during acute coronary syndrome play a cardioprotective effect? Pathophysiology and clinical evidence. Diabet Res Clin Pract. 2021;178:108959. doi:10.1016/j.diabres.2021.108959
22. Packer M. Cardioprotective effects of Sirtuin-1 and its downstream effectors: potential role in mediating the heart failure benefits of SGLT2 (sodium-glucose cotransporter 2) inhibitors. Circ Heart Fail. 2020;13(9):e007197. doi:10.1161/CIRCHEARTFAILURE.120.007197
23. Neuen BL, Arnott C, Perkovic V, et al. Sodium-glucose co-transporter-2 inhibitors with and without metformin: a meta-analysis of cardiovascular, kidney and mortality outcomes. Diabetes Obes Metab. 2021;23(2):382–390. doi:10.1111/dom.14226
24. Shen Y, Zhou J, Shi L, et al. Effectiveness of sodium-glucose co-transporter-2 inhibitors on ischaemic heart disease. Diabetes Obes Metab. 2020;22(7):1197–1206. doi:10.1111/dom.14025
25. Oshima H, Miki T, Kuno A, et al. Empagliflozin, an SGLT2 inhibitor, reduced the mortality rate after acute myocardial infarction with modification of cardiac metabolomes and antioxidants in diabetic rats. J Pharmacol Exp Ther. 2019;368(3):524–534. doi:10.1124/jpet.118.253666
26. Lahnwong S, Palee S, Apaijai N, et al. Acute dapagliflozin administration exerts cardioprotective effects in rats with cardiac ischemia/reperfusion injury. Cardiovasc Diabetol. 2020;19(1):91. doi:10.1186/s12933-020-01066-9
27. Cowie MR, Fisher M. SGLT2 inhibitors: mechanisms of cardiovascular benefit beyond glycaemic control. Nat Rev Cardiol. 2020;17(12):761–772. doi:10.1038/s41569-020-0406-8
28. Palmiero G, Cesaro A, Vetrano E, et al. Impact of SGLT2 inhibitors on heart failure: from pathophysiology to clinical effects. Int J Mol Sci. 2021;22(11):5863. doi:10.3390/ijms22115863
29. Ganbaatar B, Fukuda D, Shinohara M, Yagi S, Kusunose K, Yamada H. Empagliflozin ameliorates endothelial dysfunction and suppresses atherogenesis in diabetic apolipoprotein E-deficient mice. Eur J Pharmacol. 2020;15:875. doi:10.1016/j.ejphar.173040
30. Salvatore T, Caturano A, Galiero R, et al. Cardiovascular benefits from gliflozins: effects on endothelial function. Biomedicines. 2021;9(10):1356. doi:10.3390/biomedicines9101356
31. D’Onofrio N, Sardu C, Trotta MC, et al. Sodium-glucose co-transporter2 expression and inflammatory activity in diabetic atherosclerotic plaques: effects of sodium-glucose co-transporter2 inhibitor treatment. Mol Metab. 2021;54:101337. doi:10.1016/j.molmet.2021.101337
32. Oelze M, Kröller-Schön S, Welschof P, et al. The sodium-glucose co-transporter 2 inhibitor empagliflozin improves diabetes-induced vascular dysfunction in the streptozotocin diabetes rat model by interfering with oxidative stress and glucotoxicity. PLoS One. 2014;9(11):e112394. doi:10.1371/journal.pone.0112394
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.