")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Effect of Thoracic Paravertebral Block on Postoperative Pulmonary Complications After Video-Assisted Thoracoscopic Surgery: A Dual-Center Randomized Clinical Trial
Authors Zhu J , Wei B, Wu L, Li H, Zhang Y , Lu J, Su S, Xi C, Liu W, Wang G
Received 3 January 2025
Accepted for publication 11 May 2025
Published 15 May 2025 Volume 2025:21 Pages 691—703
DOI https://doi.org/10.2147/TCRM.S515093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Jiayu Zhu,1,* Biyu Wei,2,* Lili Wu,1 He Li,1 Yi Zhang,1 Jinfeng Lu,3 Shaofei Su,4 Chunhua Xi,1 Wei Liu,2 Guyan Wang1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Beijing Chest Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Anesthesiology, Beijing Renhe Hospital, Beijing, People’s Republic of China; 4Central Laboratory, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, No. 1 Dongjiaomingxiang, Beijing, 100730, People’s Republic of China, Tel +86-13910985139, Fax +86-10-58268017, Email [email protected] Wei Liu, Department of Anesthesiology, Beijing Chest Hospital, Capital Medical University, No. 9 Beiguan Street, Tongzhou District, Beijing, People’s Republic of China, Tel +86-13621153330, Fax +86-10-89509000, Email [email protected]
Purpose: TPVB can provide effective postoperative analgesia in lung cancer patients undergoing video-assisted thoracoscopic surgery (VATS), which may enhance respiratory mechanics and postoperative expectoration, as well as relieve inflammation and stress. These mechanisms may reduce the incidence of postoperative pulmonary complications (PPCs). This study explored whether TPVB reduces the risk of PPCs in patients undergoing VATS for lung cancer.
Patients and Methods: In this dual-center trial, patients who underwent VATS for lung cancer were randomly divided into the PV group (n = 151, general anesthesia [GA] and TPVB) and the C group (n = 151, GA only). The primary outcome was the incidence of a composite of PPCs within seven days postoperatively.
Results: The incidence of PPCs within seven days postoperatively was lower in the PV group (37.7%, 57/151) compared to the C group (49.0%, 74/151), with a risk ratio of 1.59 (95% CI: 1.00 to 2.50, P=0.048). And within 8– 30 days postoperatively, compared with that in the C group (33.1%, 50/151), the incidence of PPCs was lower in patients in the PV group (22.5%, 34/151), with a risk ratio of 1.70 (95% CI, 1.02 to 2.84, P=0.040). There was a significant difference in the incidence of pneumonia between the PV group (11/151, 7.3%) and the C group (35/151, 23.3%; P < 0.001), and the incidence of pneumothorax between the PV group (27/151, 17.9%) and the C group (45/151, 29.8%; P = 0.015).
Conclusion: Compared to GA alone, TPVB combined with GA reduces the incidence of PPCs within seven days postoperatively in patients undergoing VATS for lung cancer, and this beneficial effect can last up to 30 days after surgery. A possible mechanism is that TPVB reduces acute postoperative pain in patients.
Plain Language Summary: Inadequate analgesia was associated with the incidence of pulmonary complications, and the thoracic paravertebral block provides good postoperative analgesia in patients undergoing thoracic surgery. However, the effect of thoracic paravertebral block on the incidence of postoperative pulmonary complications is unknown. Dr. Wang’s team conducted a randomized controlled study, and the results showed that in patients undergo VATS for lung cancer, thoracic paravertebral block can lower the incidence of postoperative PPCs and encourage quicker recovery.
Keywords: postoperative complications, postoperative pain, nerve block, analgesia, VATS
Introduction
As imaging technology and thoracic surgical methods continue to advance, video-assisted thoracoscopic surgery (VATS) has emerged as a widely used treatment for lung cancer.1 Despite its advantages, VATS is associated with certain risks, particularly postoperative pulmonary complications (PPCs), which remain a significant concern.2 Although VATS is a minimally invasive lung cancer treatment technique, it impacts other tissues such as the pleura, intercostal muscles, and intercostal nerves,3 leading to acute postoperative pain and impaired lung function in the early postoperative phase.4 Furthermore, the use of one-lung ventilation (OLV) during surgery has been associated with increased inflammatory responses, triggering potential risk of lung damage to varying degrees.5,6 All of these factors increase the incidence of PPCs. PPCs increase medical expenses, prolong the length of hospital stay (LOS), and have a mortality incidence of up to 19.5% within 30 days following surgery.2,7,8 Therefore, decreasing the prevalence of PPCs is crucial for enhancing the perioperative recovery and prognosis of patients after VATS.
Studies have demonstrated a correlation between inadequate postoperative analgesia and the development of pulmonary complications following surgery.9,10 Given the role of pain management in lung function recovery, optimizing postoperative analgesia is a key strategy for reducing PPCs. While thoracic epidural analgesia (TEA) is a standard option, existing RCTs supported that TPVB can offer comparable analgesic effects.11,12 Moreover, TPVB has a lower incidence of complications such as hypotension, nausea, and urine retention.4,11,13,14 Compared with serratus anterior plane block and intercostal nerve block, TPVB can effectively block the dorsal branch nerve with a larger block area, which can provide more complete postoperative analgesia for patients with VATS.15
Ultrasound-guided TPVB reduces postoperative pain, preserves respiratory mechanics, and minimizes opioid use.16 Subsequently, by preventing pain-induced splinting and impaired cough reflex, it lowers the risk of atelectasis and pneumonia-two major contributors to PPCs. Furthermore, TPVB can decrease nociceptive stimulation of afferent nerves and block sympathetic nerves on the affected side, thus preventing an increase in stress-related hormones (eg, catecholamines, cortisol) after surgery.17 It can also lower the production of inflammatory factors (eg, TNF-α and IL-6). Eventually, the inhibited stress and inflammation may also lead to a reduced occurrence of complications.14,18 A recent retrospective propensity score matching study revealed that the use of general anesthesia (GA) in conjunction with TPVB was associated with a modest reduction in PPCs (34.2% vs 29.8%),19 but selection bias, inconsistent PPCs definitions, and lack of randomization limit their reliability. In addition, it remains unclear regarding the effect of TPVB on postoperative analgesia and complications in patients with VATS due to limitations such as variability in block success rates and the lack of standardization in dosing and catheter placement. A randomized controlled trial (RCT) is needed to confirm these findings. However, to our knowledge, no randomized controlled trial has specifically examined the impact of TPVB on PPC incidence following VATS.
To address this gap, we conducted a RCT to evaluate whether ultrasound-guided TPVB combined with GA reduces PPC incidence within seven days postoperatively compared to GA alone in patients undergoing VATS for lung cancer. This study also evaluates secondary outcomes like postoperative pain, hospital stay, and quality of recovery, giving a more complete assessment of TPVB’s benefits.
Materials and Methods
This was a prospective, dual-center, randomized controlled investigator-initiated trial. The institutional ethics committees of Beijing Tongren Hospital (March 29, 2023, TREC2023-KY020) and Beijing Chest Hospital (June 16, 2023, [2023] LS-KY-N0.18) approved this study, which adhered to the Helsinki Declaration. This study has been registered with Clinicaltrials.gov (NCT05922449; registered date: June 25, 2023). Each participant provided written informed consent before participation; the participants’ private information was not disclosed. This manuscript adheres to the applicable CONSORT guidelines (Figure 1). The details of the experiment can be found in the study protocol (https://doi.org/10.1186/s13063-023-07826-8).20
 |
Figure 1 CONSORT flow diagram. Abbreviations: VATS, video-assisted thoracoscopic surgery; TPVB, thoracic paravertebral nerve block. |
Patients
Patients with lung tumors scheduled for VATS between July 2023 and December 2023 were recruited. The inclusion criteria were an age of 18 years or older, an American Society of Anesthesiologists (ASA) grade I–III, and an expected surgery duration >1 h. Severe respiratory or cardiovascular complications, a history of ipsilateral thoracotomy or mechanical ventilation within four weeks, contraindications to TPVB, and pregnancy or lactation were among the exclusion criteria. Patients with a history of tracheostomy or tracheal abnormalities were also excluded to maintain consistency in intraoperative airway care. The detailed definitions of complications and contraindications are provided in the protocol (see supplementary material “Protocol for this study”).
Randomization and Blinding
This study used stratified blocked randomization with different centers. The patients were divided into two groups at a 1:1 ratio: the paravertebral block group (PV group, n = 151), in which GA was combined with TPVB; and the control group (C group, n = 151), in which GA alone was used. The participants were randomized into groups using a computer-generated allocation sequence in blocks, with random-sized blocking (blocks of sizes 4, 6, and 10). The allocation sequence varied across blocks to maintain randomness. Because the anesthesiologist performing TPVB could not be blinded, the nerve block maneuver was performed by an unblinded anesthesiologist who was not involved in intraoperative patient management. Data collectors, statisticians, follow-up researchers, and the radiology expert panel were blinded to the grouping results on the participants. The surgeon and anesthesiologist for this surgery were also unaware of the participant information. The protocol contains information on the blinding and randomization procedures.
Anesthesia Protocol
Electrocardiography, oxygen saturation measured by pulse oximetry (SpO2), and invasive arterial blood pressure monitoring were performed after the patient entered the operating room. Anesthesia was induced and maintained as per protocol. A chest tube is routinely placed to facilitate postoperative drainage. Before placing a chest tube, intravenous infusions of 5 μg of sufentanil and 8 mg of ondansetron were administered to each patient once more.
Following the procedure, a patient-controlled intravenous analgesia (PCIA) device was used, which contained 1.5 μg/kg sufentanil and 24 mg of ondansetron diluted to 100 mL. The locking time was set to 15 min, and the background dose was 1 mL/h. Unless the patient experienced adverse opioid-related reactions such as nausea and vomiting, the PCIA device was used for at least 48 hours postoperatively.
An individualized fluid management protocol was adopted in this study to prevent the increase in intrapulmonary shunt and pulmonary edema caused by excessive infusion. The nasopharyngeal temperature was monitored during the surgery, and the intraoperative body temperature was maintained using methods such as the control of the ambient temperature of the operating room and the use of warming blankets (see supplementary material “Protocol for this study”).
Interventions
All nerve blocks were performed by an experienced anesthesiologist under ultrasound guidance (Dr. Wu and Dr. Li). When the patients were placed in the lateral decubitus position, patients in the PV group underwent ultrasound-guided TPVB. Using an ultrasound-guided out-of-face technique (using the low-frequency convex array probe), the blocking needle tip was guided to the thoracic paravertebral space of T4 and T7.21 Fifteen milliliters of 0.5% ropivacaine was then injected into each space. Following injection, a successful block was confirmed by observing a downward pleural shift on ultrasound. Patients in the C group did not receive perioperative nerve blocks during the perioperative period.
Lung Protection Ventilation Management Plan
- Two-lung ventilation management: inspiratory: expiratory 1:2, Respiratory rate (RR) 12 breaths/min, tidal volume (VT) 8 mL/kg predicted body weight, positive end-expiratory pressure (PEEP) 5 cmH2O, volume-controlled ventilation mode.
- One-lung ventilation management: starting parameters include VT 6 mL/kg predicted body weight, PEEP 5 cmH2O, RR 14 breaths/min, FIO2 60%, and end inspiratory pause 10% (if oxygenation cannot be maintained, ventilatory parameters are gradually adjusted according to the strategy developed by the protocol).
- Recruitment strategy: In mechanical ventilation mode, the patient was subjected to a recruitment maneuver every 30 minutes or after reconnection to mechanical ventilation. The specific method of recruitment maneuver is detailed in the protocol (see supplementary material “Protocol for this study”).
Primary Outcome
The primary outcome was the incidence of a composite of PPCs within seven days postoperatively. Each complication was weighted equally for the composite outcome of the PPCs. Patients with at least one complication were considered eligible for the primary endpoint analysis. Imaging data were interpreted by a member of the radiology expert panel, and other outcomes were determined by the clinician. For patients discharged within seven days, we would follow up daily by phone to obtain their clinical symptoms. PPCs included pneumonia, aspiration pneumonia, atelectasis, respiratory failure, bronchospasm, pulmonary congestion, pleural effusion, and pneumothorax. Definitions of PPCs are based on guidelines from the European Perioperative Clinical Outcome (EPCO).22 (Details can be found in Table S1). Seven days was chosen because most PPCs, especially pneumonia, atelectasis, and pneumothorax, occur within the first postoperative week. Later complications (8–30 days) are included as secondary outcomes.
Secondary Outcomes
At the perioperative T1-T4 time points (T1: preoperation; T2: 30 min after the initiation of OLV; T3: after the cessation of OLV; T4: 10 min after admission to the PACU), we measured perioperative blood gas analysis indicators, including pH, arterial partial pressure of oxygen (PaO2), arterial partial carbon dioxide pressure (PaCO2), arterial blood lactate concentration, and the oxygen index. The lung ultrasound score (LUS), the numeric rating scale (NRS), score and the 15-item quality of recovery scale (QoR-15) score were recorded 1–2 days after surgery. The unplanned ICU hospitalization rate, the postoperative hospitalization duration, hospitalization costs, and the incidences of various postoperative pulmonary and extrapulmonary complications within seven days after surgery were also recorded. Long-term outcomes were assessed via clinic visits and telephone follow-ups at 1 and 3 months, including the incidence of pulmonary, extrapulmonary complications and mortality within 8–30 and 31–90 days after surgery, Numeric Rating Scale scores, and QoR-15 scores at postoperative day 30 and day 90. The participant timeline is presented in Table S2. Members of the follow-up team (Drs. Zhu, Wei, Zhang, and Lu) blinded to the patient grouping were responsible for collecting all in-hospital and long-term follow-up data.
Statistical Analysis
PASS 15.0 was used to determine the sample size. In our pre-experiment with 50 patients, the postoperative incidence of PPCs was 32% in the PV group and 48% in the C group. A power analysis (80%, α = 0.05) determined 144 patients per group, increased to 151 to allow for 5% loss to follow-up.
The intention-to-treat (ITT) principle was followed, and all randomized patients were included in the analysis. According to the study protocol, since less than 5% of each secondary outcome set had missing values, the missing data were not imputed. Furthermore, as a sensitivity analysis, we carried out a per-protocol (PP) analysis of the incidence of PPCs. The data were processed via SPSS 25.0. A statistically significant result was defined as a P-value < 0.05 in a 2-tailed test. Categorical variables were reported as the percentage of cases (n%). Continuous variables were expressed as mean (standard deviation, SD) or median (first quartile [Q1]-third quartile [Q3]). The normal distribution of data was evaluated with the Kolmogorov–Smirnov test. The incidence of PPCs was evaluated with the χ2 test, and the incidence risk ratio and 95% Wald confidence intervals were used for each point estimate. For the secondary outcomes, categorical and continuous variables were respectively analyzed using the χ2 test and the independent samples t-test or Mann–Whitney U-test. To calibrate confounding factors and better determine the independent effect of groups, multivariate logistic regression analyse was used to perform sensitivity analyses for primary outcomes.
Results
Participant Characteristics
From July 2023 to December 2023, a total of 365 patients were screened, of whom 302 patients who met the inclusion criteria were included in the ITT population and were randomized with 151 in the PV group and 151 in the C group (Figure 1). A total of 22 patients who underwent randomization were excluded from the PP set, resulting in the inclusion of 280 patients in the PP set, with 139 in the PV group and 141 in the C group. There was no significant difference between groups in baseline indicators (eg, ARISCAT risk score and FEV1), and intraoperative characteristics (eg, surgical type and OLV duration). (Table 1 and Table S3).
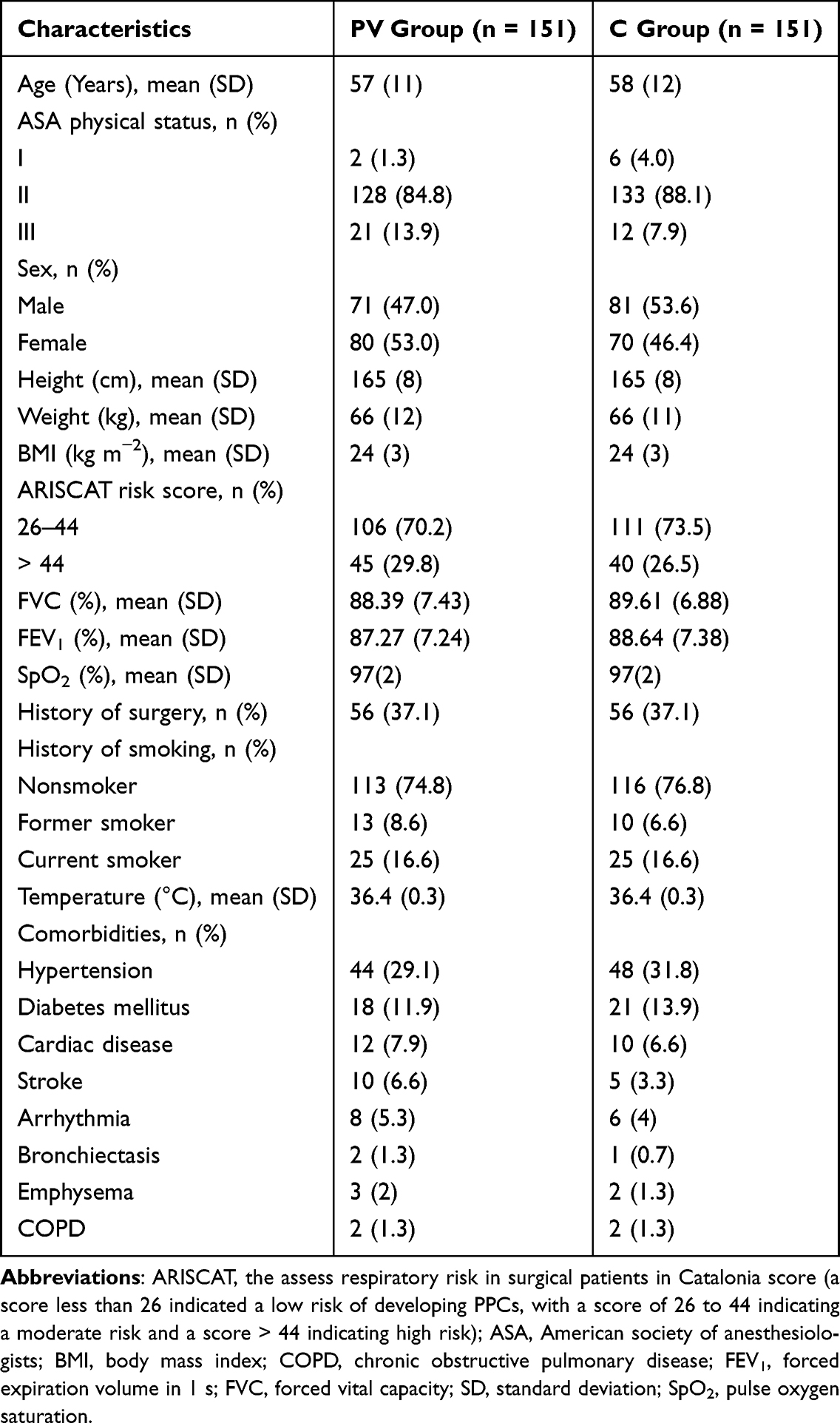 |
Table 1 Participant Baseline Characteristics |
Primary Outcomes
We obtained primary outcome data for all participants (Table 2 and Figure 2). Within seven days following surgery, 57 patients in the PV group (37.7%) and 74 patients in the C group (49.0%) respectively had postoperative pulmonary complications (risk ratio, 1.585; 95% CI, 1.002 to 2.506; P = 0.048). The overall incidence of PPCs was 43.4%. The absolute reduction in PPCs was 11.3%, corresponding to a number needed to treat (NNT) of 9, suggesting that TPVB is a clinically effective intervention for reducing PPCs in VATS patients.
 |
Table 2 Incidence of Postoperative Pulmonary Complications |
 |
Figure 2 Incidence of postoperative pulmonary complications postoperatively in the two groups. PPCs, postoperative pulmonary complications. (A) incidence of PPCs within 7 days postoperatively; (B) incidence of PPCs within 8–30 days postoperatively; (C) incidence of PPCs within 31–90 days postoperatively. *P <0.05. |
According to the analysis of the incidence of each component of the PPC, 11 patients in the PV group and 35 patients in the C group experienced pneumonia (7.3% vs 23.3%; risk ratio, 3.84; 95% CI, 1.868 to 7.895; P < 0.001). 27 patients in the PV group and 45 patients in the C group developed pneumothorax (17.9% vs 29.8%; risk ratio, 1.950; 95% CI, 1.133 to 3.356; P = 0.015). However, there was no statistically significant difference in the incidence of atelectasis, pleural effusion, respiratory failure, or bronchospasm. Pulmonary congestion did not occur in either group. PP analysis results (P=0.039) were consistent with ITT findings. (Table S4).
Secondary Outcomes
With respect to postoperative pain, the NRS score at 24 h after surgery was lower in the PV group than in the C group (2 [2–3]) vs 3 [2–3]; P < 0.001). Nevertheless, there was no significant difference in the NRS score at 48 h after surgery between the two groups (Table 3). The sufentanil dosage of the PV group was lower than that of the C group within 48 h after surgery (50.06 [10.47] vs 53.30 [12.62] μg; P = 0.016).
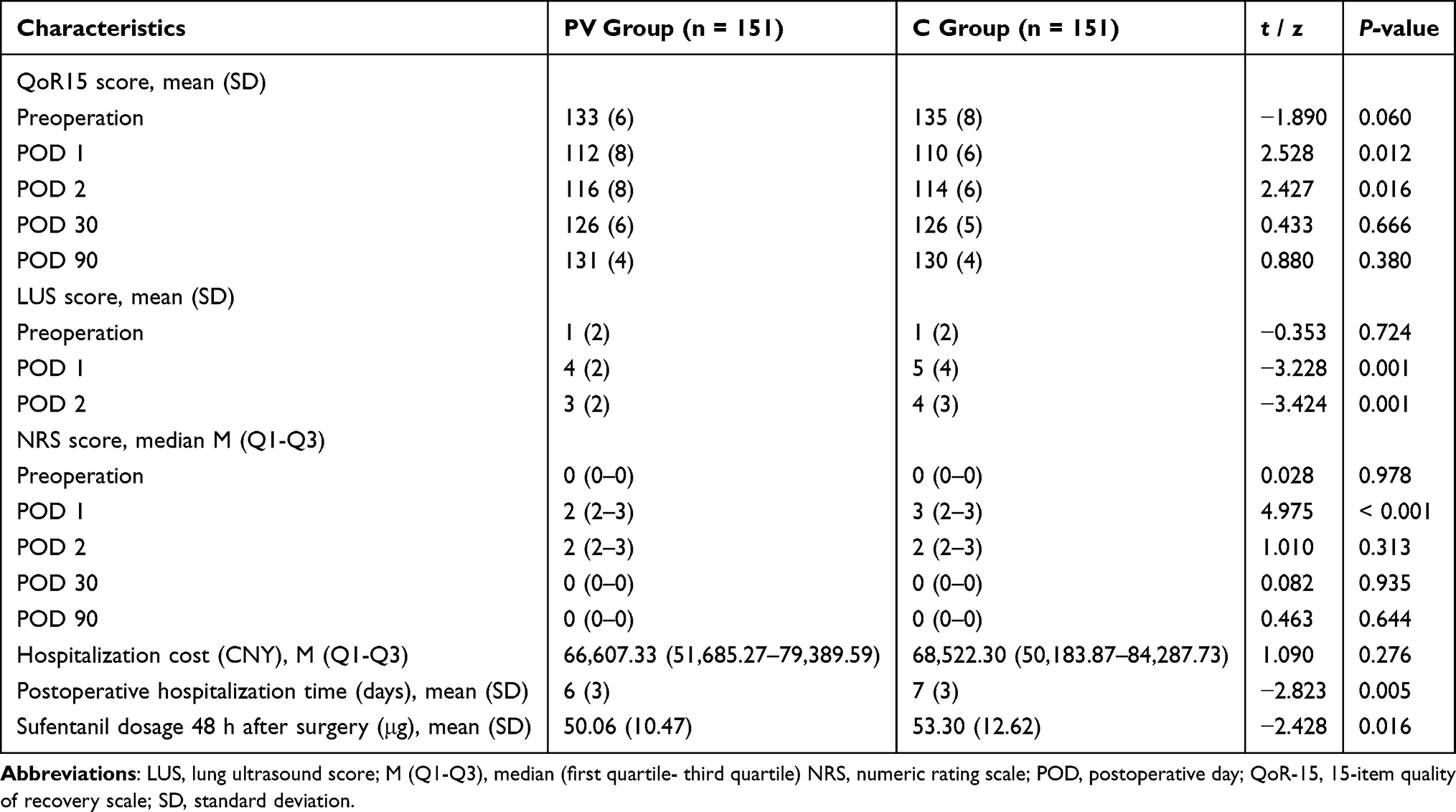 |
Table 3 Postoperative Characteristics |
The PV group had lower LUSs and greater QoR-15 scores at 24 h and 48 h postoperatively (Table 3). PV group had a shorter hospital stay (median 6 vs 7 days, P = 0.005). Other postoperative clinical outcomes, including the incidence of nausea and vomiting, total hospitalization cost, rate of unplanned ICU hospitalization, and incidence of extrapulmonary complications within seven days after surgery, were not different between the two groups. (Table 3)
PPCs incidence was lower in the PV group at 8–30 days (P = 0.040), but not at 31–90 days (P = 0.497). Additionally, the PV group experienced fewer cases of pneumonia and pneumothorax between 8 and 30 days. (Table 2 and Figure 2). There was no difference in the extrapulmonary complication rate, numeric rating scale score, or QoR-15 score at long-term follow-up. No fatalities occurred throughout the follow-up period.
Safety Outcomes
The serum lactate concentration in the PV group was lower than that in the C group at 30 min after the initiation of OLV (0.95 [0.38] vs 1.04 [0.39] mmol/L; P = 0.040), 5 min after the cessation of OLV (0.95 [0.35] vs 1.07 [0.39] mmol/L; P = 0.006) and 10 min after admission to the postanesthesia care unit (PACU) (1.10 [0.42] vs 1.25 [0.56] mmol/L; P = 0.006) (Figure S1 and Table S5). The other blood gas analyzer indicators showed no differences.
Except for the PV group having a lower PACU heart rate (72 vs 74 bpm, P = 0.045), there was no significant difference in hemodynamic indicators or SpO2 between the perioperative time points (Figure S1 and Table S5). According to the analysis of the incidence of intraoperative adverse events, the incidence of hypoxemia was 5.3% in both the PV group and the C group, and one patient in both groups developed emergence agitation after anesthesia. There were no significant differences in hypotension, hypertension, or arrhythmia rates. No statistically significant difference was detected in the occurrence of extrapulmonary problems (Table S6).
Sensitivity Analyses
The results of multivariate regression analyses showed that TPVB was still associated with lower incidence of PPCs after adjusting for confounding factors (OR = 1.67, 95% CI 1.05–2.68, P = 0.032). (Table S7)
Discussion
In this randomized controlled trial of patients undergoing VATS for lung cancer, compared with GA alone, GA combined with TPVB reduced the incidence of PPCs within seven days and 8–30 days after surgery, shortened the hospital LOS, and improved the QoR-15 score in the early postoperative period. There was a decrease in the postoperative LUS, postoperative pain score, and perioperative lactate concentration.
Our results showed that GA combined with TPVB can reduce the incidence of composite PPCs (37.7% vs 49.0%; P = 0.048) within seven days following surgery. These findings imply that TPVB can protect the lungs of patients undergoing VATS during the perioperative period. Although the primary outcome P-value is close to 0.05, all analyses were pre-specified, and the sample size was powered for this effect size. Additionally, baseline characteristics were balanced, minimizing potential confounders. In sensitivity analysis, there was a significant difference in the incidence of PPCs between the two groups after adjusting for confounders (OR = 1.67, 95% CI 1.05 to 2.68, P = 0.032). According to a recent retrospective cohort study, in the early postoperative phase following thoracoscopic lung cancer surgery, TPVB was observed to lower the incidence of PPCs.19 Our findings also support this view. The significant PPCs reduction observed in the TPVB group is likely due to improved postoperative analgesia, favoring early rehabilitation exercises and thus enhancing oxygenation in patients. Furthermore, the decrease in postoperative pain promotes efficient coughing and better sputum retention, which further contributes to improved pulmonary outcomes.9
TPVB primarily decreases the incidence of pneumonia (7.3% vs 23.3%; P < 0.001) and pneumothorax (17.9% vs 29.8%; P = 0.015), according to our study of the incidence of PPC subtypes. Prolonged lung air leaks have been reported as the most frequent single PPCs in patients undergoing thoracic surgery.23 One possible explanation for how TPVB lowers the risk of pneumothorax is that it lessens the release of inflammatory factors such as bradykinin and PGE2, resulting in decreased sensitivity of the cough reflex, thereby reducing postoperative incidence of severe cough.24 Severe cough after surgery is a significant risk factor for postoperative pneumothorax. The reason is that cough-induced intratracheal positive pressure may tear the dissected lung parenchyma and reopen the alveolar fistula, resulting in postoperative pneumothorax.25 However, it still necessitates further in-depth investigation owing to inadequate data currently. Pneumonia also occurs frequently and is linked to longer ICU stays and a higher mortality.2 Regional nerve blocks, including TPVB, have been documented to exert beneficial anti-inflammatory effects and stress-modulating effects, thereby reducing perioperative inflammation and stress responses.17 However, this study did not focus on the assessment of perioperative inflammatory factors, generating no direct evidence to uncover the mechanism by which TPVB reduces lung inflammation. According to research, the inflammatory response in the lungs causes cytokines to be produced, which may raise vascular permeability and, in turn, extravascular lung water levels.26 To measure the amount of extravascular lung water, we used LUS. At 24 h and 48 h following surgery, we observed that the TPVB group had decreased LUSs, indicating that TPVB can reduce fluid in the lung tissue space, decrease the loss of ventilation in the lung tissue, and protect oxygenation function. Eventually, it may lower the risk of PPCs. An observational study revealed a correlation between TPVB and a decreased incidence of postoperative atelectasis.27 However, because lung protection strategies were used in our study, the incidence of atelectasis and respiratory failure among research participants was too low to allow for significant comparisons. Our analyses revealed no statistically significant difference in the incidence of pleural effusion between groups. In general, pleural effusion formation is a complicated and multifactorial process, which may be affected by surgical procedures, postoperative inflammatory status, and fluid management.28 Our results suggest that TPVB has less effect on postoperative pleural effusions. Studies have shown that after general anesthesia for major surgery, it takes up to 6 weeks for respiratory function to return to its preoperative state.9,29 The incidence of pulmonary complications in patients who received a TPVB was also lower at 8–30 days following surgery (P = 0.040). The outcome of our study showed that these potential benefits may persist for more than a week.
Poor pain control after thoracoscopic lung surgery is strongly associated with the development of PPCs.9,30,31 A meta-analysis of regional block techniques for postoperative pain control in VATS patients revealed that TPVB provides greater analgesia without increasing adverse effects.15 In our study, TPVB reduced the NRS score at 24 h after surgery (P < 0.001). TPVB can relieve postoperative pain and may improve patients’ ability to perform deep breathing exercises and produce sputum.19 It enhances lung expansion and secretion clearance to maintain respiratory tract patency. Patients can turn, get out of bed, and walk more easily in the early postoperative phase because of the decrease in postoperative pain, which also helps to prevent the buildup of respiratory secretions in the lungs, thus avoiding the occurrence of PPCs.16
In postoperative analgesia, opioids alone can have adverse effects such as nausea, vomiting, and respiratory depression. These side effects may impede patients’ early ambulation and delay the recovery of lung function.9,15 The use of regional block techniques can reduce the need for opioids after surgery and provide better analgesia.32 According to our research, the sufentanil dose in the PV group decreased within 48 hours following surgery; however, the frequency of sufentanil side effects did not decrease. The reason for the lack of significant effect in reducing side effects may be firstly explained by the use of 5-HT3-receptor antagonists in patients postoperatively, and secondly, our study did not use a continuous thoracic paravertebral technique, resulting in no entirely evident benefit of lowering the incidence of adverse events.33,34
Despite no discernible change in pH, the blood lactate level in the C group was greater than that in the PV group during surgery and in the PACU. The probable reason is that TPVB reduces the metabolic rate and lowers the risk of stress hyperlactic acidemia by inhibiting the sympathetic nerve chain and intercostal nerve.35 A study by Richardson et al14 revealed that TPVB reduced the neuroendocrine stress response, resulting in lower plasma cortisol and glucose concentrations in patients. However, there is no further research to support this view. In our study, except patients’ heart rates, which were lower in the PV group when they entered the PACU than in the C group, there was no discernible difference in the other hemodynamic indices because TPVB only inhibited the unilateral sympathetic nervous system. In the PV group of patients in our research, the TPVB failure rate was 2.6%, which was significantly lower than the reported TEA failure rate of 14%–30%.4 Therefore, we believe that TPVB is safe and reliable.
This study has several limitations. First, this study had no comprehensive exploration of the relationship between TPVB and inflammatory or perioperative stress response, necessitating future studies to examine the role of TPVB in inflammatory response. Second, it is unclear whether the findings apply to other kinds of one-lung ventilation surgery because the study included only patients who underwent video-assisted thoracoscopic surgery for lung cancer. Third, because of worries about its high failure and complication rates, the study’s control group did not get a TEA or continuous TPVB. Consequently, it is currently unknown if the effects of PPCs differ between TPVB and thoracic epidural block, further comparison studies are needed. Fourth, our study did not notice a significant decrease in the incidence of pulmonary complications such as atelectasis and pleural effusion, despite a reduction in the overall incidence of PPCs. Fifth, the study was limited to two centers, necessitating future multicenter studies to validate these findings across diverse populations. Sixth, the primary measure used in this review was defined as a composite outcome of PPCs. However, this study lacked further distinctions between PPCs based on the severity and mechanism of occurrence, which may compromise the clinical impact of some complications.
Conclusion
The combination of TPVB and GA significantly reduced perioperative pain, thereby decreasing the incidence of overall PPCs within seven days after surgery, with an absolute risk reduction of 11.3%; this translates to an NNT of ~9. These potential benefits last up to 30 days. However, its effect varied by complication type, with the most pronounced reductions seen in pneumonia and pneumothorax. The use of this approach not only promotes faster postoperative recovery but also shortens the length of hospital stay, making it an effective strategy for improving patient outcomes following surgery. While the study demonstrates a clear benefit of TPVB, it is limited to two centers and does not assess long-term PPCs recurrence. Further studies are needed to determine the optimal TPVB protocol, its role in different patient populations, and its cost-effectiveness in routine VATS care.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request (Guyan Wang: [email protected]).
Ethics Approval and Informed Consent
The institutional ethics committees of Beijing Tongren Hospital (March 29, 2023, TREC2023-KY020) and Beijing Chest Hospital (June 16, 2023, [2023] LS-KY-N0.18) approved this study, which adhered to the Helsinki Declaration. This study was registered with Clinicaltrials.gov (study identifier: NCT05922449). Each participant provided written informed consent before participation; the participants’ private information was not disclosed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by Beijing Hospitals Authority’s Ascent Plan (Code: DFL20220203) and Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (Code: ZYLX202103). The funding institution does not play any role in research design, data collection, statistical analysis, data interpretation, report writing, or article publication.
Disclosure
The authors declare no competing interests in this work.
References
1. Yang HX, Woo KM, Sima CS, et al. Long-term survival based on the surgical approach to lobectomy for clinical stage i nonsmall cell lung cancer: comparison of robotic, video-assisted thoracic surgery, and thoracotomy lobectomy. Ann Surg. 2017;265(2):431–437. doi:10.1097/SLA.0000000000001708
2. Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the perioperative research network investigators. JAMA Surg. 2017;152(2):157. doi:10.1001/jamasurg.2016.4065
3. Colquhoun DA, Leis AM, Shanks AM, et al. A lower tidal volume regimen during one-lung ventilation for lung resection surgery is not associated with reduced postoperative pulmonary complications. Anesthesiology. 2021;134(4):562–576. doi:10.1097/ALN.0000000000003729
4. Yeung JHY, Gates S, Naidu BV, Wilson MJA, Gao Smith F. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016;2(2):CD009121. doi:10.1002/14651858.CD009121.pub2
5. Lohser J, Slinger P. Lung injury after one-lung ventilation: a review of the pathophysiologic mechanisms affecting the ventilated and collapsed lung. Surv Anesthesiol. 2016;60(3):98–99. doi:10.1097/01.sa.0000482339.06198.0d
6. Li XF, Hu JR, Wu Y, Chen Y, Zhang MQ, Yu H. Comparative effect of propofol and volatile anesthetics on postoperative pulmonary complications after lung resection surgery: a randomized clinical trial. Anesth Analg. 2021;133(4):949–957. doi:10.1213/ANE.0000000000005334
7. Paul S, Sedrakyan A, Chiu YL, et al. Outcomes after lobectomy using thoracoscopy vs thoracotomy: a comparative effectiveness analysis utilizing the nationwide inpatient sample database. Eur J Cardiothorac Surg. 2013;43(4):813–817. doi:10.1093/ejcts/ezs428
8. Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369(5):428–437. doi:10.1056/NEJMoa1301082
9. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
10. Hausman MS, Jewell ES, Engoren M. Regional versus general anesthesia in surgical patients with chronic obstructive pulmonary disease: does avoiding general anesthesia reduce the risk of postoperative complications? Anesth Analg. 2015;120(6):1405–1412. doi:10.1213/ANE.0000000000000574
11. Pintaric TS, Potocnik I, Hadzic A, Stupnik T, Pintaric M, Jankovic VN. Comparison of continuous thoracic epidural with paravertebral block on perioperative analgesia and hemodynamic stability in patients having open lung surgery. Reg Anesth Pain Med. 2011;36(3):256–260. doi:10.1097/AAP.0b013e3182176f42
12. Thanh Trung T, Van Khoa D, Van Dong T. The comparison of analgesic efficacy between ultrasound-guided continuous thoracic paravertebral block and continuous thoracic epidural block using bupivacaine - fentanyl in patients undergoing lung surgery: a prospective, randomized, controlled trial. Turk J Surg. 2021;37(3):232–241. doi:10.47717/turkjsurg.2021.5053
13. Ozturk T. Comparison of thoracic epidural and paravertebral analgesia for postoperative pain control after thoracotomy. Ağrı - J Turk Soc Algol. 2015. doi:10.5505/agri.2015.22043
14. Richardson J, Sabanathan S, Jones J, Shah RD, Cheema S, Mearns AJ. A prospective, randomized comparison of preoperative and continuous balanced epidural or paravertebral bupivacaine on post-thoracotomy pain, pulmonary function and stress responses. Br J Anaesth. 1999;83(3):387–392. doi:10.1093/bja/83.3.387
15. Sandeep B, Huang X, Li Y, Xiong D, Zhu B, Xiao Z. A comparison of regional anesthesia techniques in patients undergoing video-assisted thoracic surgery: a network meta-analysis. Int J Surg. 2022;105:106840. doi:10.1016/j.ijsu.2022.106840
16. Kang K, Meng X, Li B, et al. Effect of thoracic paravertebral nerve block on the early postoperative rehabilitation in patients undergoing thoracoscopic radical lung cancer surgery. World J Surg Oncol. 2020;18(1):298. doi:10.1186/s12957-020-02071-8
17. De Liyis BG, Hartawan IGAGU, Widyadharma IPE, Senapathi TGA, Mahadewa TGB. Cervical-level regional paraspinal nerve block in cervical spine surgery: a systematic review and meta-analysis of randomized controlled trials. World Neurosurg. 2024;190:470–480.e2. doi:10.1016/j.wneu.2024.08.021
18. Zhen SQ, Jin M, Chen YX, Li JH, Wang H, Chen HX. Ultrasound-guided paravertebral nerve block anesthesia on the stress response and hemodynamics among lung cancer patients. World J Clin Cases. 2022;10(7):2174–2183. doi:10.12998/wjcc.v10.i7.2174
19. Tong C, Zheng J, Wu J. The effects of paravertebral blockade usage on pulmonary complications, atrial fibrillation and length of hospital stay following thoracoscopic lung cancer surgery. J Clin Anesth. 2022;79:110770. doi:10.1016/j.jclinane.2022.110770
20. Zhu J, Wei B, Wu L, et al. Thoracic paravertebral block for perioperative lung preservation during VATS pulmonary surgery: study protocol of a randomized clinical trial. Trials. 2024;25(1):74. doi:10.1186/s13063-023-07826-8
21. Marhofer P, Kettner SC, Hajbok L, Dubsky P, Fleischmann E. Lateral ultrasound-guided paravertebral blockade: an anatomical-based description of a new technique. Br J Anaesth. 2010;105(4):526–532. doi:10.1093/bja/aeq206
22. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
23. Dugan KC, Laxmanan B, Murgu S, Hogarth DK. Management of Persistent Air Leaks. Chest. 2017;152(2):417–423. doi:10.1016/j.chest.2017.02.020
24. Al-Shamlan F, El-Hashim AZ. Bradykinin sensitizes the cough reflex via a B2 receptor dependent activation of TRPV1 and TRPA1 channels through metabolites of cyclooxygenase and 12-lipoxygenase. Respir Res. 2019;20(1):110. doi:10.1186/s12931-019-1060-8
25. Ishibashi H, Wakejima R, Kurihara Y, et al. Extubation by supraglottic airway after lobectomy prevents cough-associated air leaks and prolonged coughing or sore throat. Eur J Cardiothorac Surg. 2023;63(5):ezad158. doi:10.1093/ejcts/ezad158
26. Lindow T, Quadrelli S, Ugander M. Noninvasive imaging methods for quantification of pulmonary edema and congestion. JACC Cardiovasc Imaging. 2023;16(11):1469–1484. doi:10.1016/j.jcmg.2023.06.023
27. Tong C, Zhu H, Li B, Wu J, Xu M. Impact of paravertebral blockade use in geriatric patients undergoing thoracic surgery on postoperative adverse outcomes. J Thorac Dis. 2019;11(12):5169–5176. doi:10.21037/jtd.2019.12.13
28. Hao X, Guo Y, Xu Z, et al. Effect of perioperative methylprednisolone administration on postoperative pleural effusion in older patients with non-small cell lung cancer. BMC Anesthesiol. 2025;25(1):20. doi:10.1186/s12871-025-02891-9
29. Nieuwenhuijs D, Bruce J, Drummond GB, Warren PM, Wraith PK, Dahan A. Ventilatory responses after major surgery and high dependency care. Br J Anaesth. 2012;108(5):864–871. doi:10.1093/bja/aes017
30. Odor PM, Bampoe S, Gilhooly D, Creagh-Brown B, Moonesinghe SR. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ. 2020;m540. doi:10.1136/bmj.m540
31. Pirie K, Traer E, Finniss D, Myles PS, Riedel B. Current approaches to acute postoperative pain management after major abdominal surgery: a narrative review and future directions. Br J Anaesth. 2022;129(3):378–393. doi:10.1016/j.bja.2022.05.029
32. Kumar K, Kirksey MA, Duong S, Wu CL. A review of opioid-sparing modalities in perioperative pain management: methods to decrease opioid use postoperatively. Anesth Analg. 2017;125(5):1749–1760. doi:10.1213/ANE.0000000000002497
33. Cowie B, McGlade D, Ivanusic J, Barrington MJ. Ultrasound-guided thoracic paravertebral blockade: a cadaveric study. Anesth Analg. 2010;110(6):1735–1739. doi:10.1213/ANE.0b013e3181dd58b0
34. Termpornlert S, Sakura S, Aoyama Y, Wittayapairoj A, Kishimoto K, Saito Y. Distribution of injectate administered through a catheter inserted by three different approaches to ultrasound-guided thoracic paravertebral block: a prospective observational study. Reg Anesth Pain Med. 2020;45(11):866–871. doi:10.1136/rapm-2020-101545
35. Garcia-Alvarez M, Marik P, Bellomo R. Stress hyperlactataemia: present understanding and controversy. Lancet Diabetes Endocrinol. 2014;2(4):339–347. doi:10.1016/S2213-8587(13)70154-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The ARISCAT Risk Index as a Predictor of Pulmonary Complications After Thoracic Surgeries, Almoosa Specialist Hospital, Saudi Arabia
Eldaabossi S, Al-Ghoneimy Y, Ghoneim A, Awad A, Mahdi W, Farouk A, Soliman H, Kanany H, Antar A, Gaber Y, Shaarawy A, Nabawy O, Atef M, Nour SO, Kabil A
Journal of Multidisciplinary Healthcare 2023, 16:625-634
Published Date: 6 March 2023
Analgesic Efficacy of an Ultrasound-Guided Transversus Thoracis Plane Block Combined with an Intermediate Cervical Plexus Block on Postoperative Pain Relief After Trans-Areolar Endoscopic Thyroidectomy: A Single Center Prospective Randomized Controlled Study
Zhong R, Zou Y, Bao S, Chen Y, Huang G, Wang L, Chen L, Zhong M, Liang W
Journal of Pain Research 2023, 16:1059-1067
Published Date: 24 March 2023
Pharmacological Methods of Pain Management: Narrative Review of Medication Used
Alorfi NM
International Journal of General Medicine 2023, 16:3247-3256
Published Date: 31 July 2023
Correlation Between Pain Intensity and Quality of Recovery After Video-Assisted Thoracic Surgery for Lung Cancer Resection
Yoon SH, Bae J, Yoon S, Na KJ, Lee HJ
Journal of Pain Research 2023, 16:3343-3352
Published Date: 2 October 2023
Analgesic Effects of Different Local Infiltration Anesthesia Techniques Combined with Femoral Nerve Block in Patients Undergoing Total Knee Arthroplasty: A Randomized Controlled Clinical Trial
Gui YK, Xiao R, Luo YR, Liu Y, Da X, Zhu SH, Shi DW, Hu XD, Xu GH
Local and Regional Anesthesia 2023, 16:183-192
Published Date: 22 December 2023