")
Back to Journals » Journal of Pain Research » Volume 18
Effectiveness of Jingjin Therapy for Non-Specific Chronic Neck Pain with Extension Dysfunction: A Randomised Controlled Trial
Authors Gong Z , Gao Y, Liu W, Li W , Wu X, Li J
Received 4 February 2025
Accepted for publication 8 May 2025
Published 23 May 2025 Volume 2025:18 Pages 2631—2642
DOI https://doi.org/10.2147/JPR.S515232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Zhichao Gong,1 Yinyan Gao,2 Wenqi Liu,2 Wu Li,3 Xinyin Wu,2 Jiangshan Li3
1Department of Acupuncture and Massage, The Second Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, Hunan, 410005, People’s Republic of China; 2Department of Epidemiology and Biostatistics, Xiangya School of Public Health, Central South University, Changsha, Hunan, 410013, People’s Republic of China; 3College of Acupuncture, Massage and Rehabilitation, Hunan University of Chinese Medicine, Changsha, Hunan, 410208, People’s Republic of China
Correspondence: Xinyin Wu, Department of Epidemiology and Health Statistics, Xiangya School of Public Health, Central South University, No. 168-2, Tongzipo Road, Yuelu District, Changsha, Hunan, 410000, People’s Republic of China, Tel +86-18390825035, Email [email protected] Jiangshan Li, College of Acupuncture, Tuina and Rehabilitation, Hunan University of Chinese Medicine, No. 300, Xueshi Road, Yuelu District, Changsha, Hunan Province, 410208, People’s Republic of China, Tel +86 13707315642, Email [email protected]
Purpose: To evaluate whether Jingjin therapy, a distal manual intervention, could accelerate extension dysfunction for non-specific chronic neck pain (NCNP).
Patients and Methods: In this single-centre, two-arm randomised controlled trial, we enrolled Chinese patients aged 20– 60 years with active neck extension disorder, regardless of prior exposure to manual therapy. We randomly assigned 160 patients to one of the following two arms: Jingjin therapy or general manual therapy. Both groups underwent six treatment sessions: the first three sessions were administered daily, and the last three sessions were administered every other day. The primary outcome was the between-group difference in the angle of active neck extension after the sixth treatment and 1 week after treatment. A repeated-measures linear mixed-effects model was used to assess between-group differences in outcome indices, with group allocation and treatment time points treated as fixed effects and participants as random effects.
Results: The change in the angle of active neck extension from baseline to the sixth treatment session was significant for Jingjin therapy (mean: 29.75° to 51.97°) and general manual therapy (mean: 28.18° to 52.49°). Further, the between-group difference was minimal (mean − 0.26°, 95% confidence interval, − 2.62°, 2.09°) and not statistically significant (P = 0.828).
Conclusion: Jingjin therapy for 9 days significantly improved neck extension function in patients with NCNP, with no significant difference compared to general manual therapy.
Clinical Trial Registry Id: ChiCTR2300068892.
Plain Language Summary: This study evaluated the efficacy of Jingjin therapy, a massage technique employed for the treatment of non-specific chronic neck pain, in comparison with conventional manual therapy in adult populations. The primary objective was to assess whether Jingjin therapy could enhance neck mobility. The findings revealed that both therapeutic modalities were beneficial and exhibited comparable effectiveness. Notably, Jingjin therapy, characterized by its distal intervention site, demonstrated fewer side effects and was more readily accepted by patients. Consequently, Jingjin therapy may represent a viable alternative for the management of chronic neck pain. However, further research is warranted to determine its potential for use in conjunction with other treatment modalities and its efficacy in addressing other types of neck pain.
Keywords: Jingjin, manual therapy, chronic neck pain, neck extension
Introduction
Neck pain is the fourth leading cause of disability-adjusted life years worldwide.1 Non-specific chronic neck pain (NCNP), characterised by persistent neck pain (>3 months) without any evident underlying pathological alterations,2 has emerged as a significant public health issue globally.3 The increasing prevalence of neck pain4 has led to a cascade of health and economic challenges, imposing a heavy familial and societal burden.5
Neck pain is characterised by diverse related symptoms,6 with neck extension dysfunction being the most prevalent. It can be largely due to prolonged periods in which individuals maintain a flexed neck posture while working,7,8 with studies demonstrating a strong relationship between neck pain and decreased strength and stamina in the neck extensor muscles.9,10 Accordingly, targeted neck extension exercises can markedly alleviate neck pain.11
Current guidelines classify neck pain into four categories based on its accompanying symptoms.12 Although manual therapy is the standardised intervention for NCNP treatment, it is mostly operated on the cervical spine to relieve pain13 and has not been investigated in other functional disorders.14 Moreover, as manual therapy involves direct manipulation of the painful area, there is a concomitant decrease in patient compliance.15 Accordingly, tailored treatment strategies have been recommended to address different accompanying symptoms.16
In traditional Chinese medicine (TCM), the Jingjin theory, as detailed in ‘Ling Shu-Jingjin’, is a key therapeutic approach for musculoskeletal pain disorders,17 including neck extension dysfunction. Based on this theory, Jingjin therapy targets distal points to reduce pain and improve function in local areas. Notably, it can avoid irritation to the pain area and improve safety and compliance. However, the effectiveness of Jingjin therapy in treating neck extension dysfunction remains unclear.
Therefore, this study aimed to determine whether Jingjin therapy could improve extension dysfunction in patients with NCNP compared to general manual therapy. It also aimed to provide evidence-based support for the effectiveness of Jingjin therapy in addressing the specific needs of patients with NCNP, potentially offering a more targeted and effective treatment approach.
Materials and Methods
Study Design and Setting
We conducted a single-centre, randomised, analyst- and assessor-blinded controlled trial in accordance with the CONSORT Guidelines.18,19 This parallel-design study used a 1:1 allocation ratio and was approved by the Ethics Committee of the Second Affiliated Hospital of Hunan University of Chinese Medicine (ID: 2023-KY-021). Further, it was registered in the Chinese Clinical Trial Registry (ID: ChiCTR2300068892). This study was conducted in accordance with the Declaration of Helsinki.
The study was conducted at the Second Affiliated Hospital of Hunan University of Chinese Medicine, a tertiary hospital in Changsha, China. A team of three certified physical therapists administered the treatment. Participant eligibility was independently assessed by a master’s degree candidate blinded to group allocation. Outcome assessments were performed at baseline, after each treatment session (on days 1, 2, 3, 5, 7, and 9), and 1-week post-treatment. No methodological changes were made after trial commencement.
Participants
Participants who presented to a general practitioner or acupuncture and tuina clinic with a primary complaint of neck extension pain or dysfunction were assessed for eligibility and recruited. Moreover, recruitment information was available through advertisements on WeChat and hospital bulletin boards. NCNP was defined as cervical pain (with or without radiation) lasting ≥3 months without a known pathological cause (eg, neurological or trauma-induced). The inclusion criteria included moderate pain severity (visual analogue scale [VAS] score >3), pain or an angle <30° during active neck extension, and having not received neck pain treatment within the past week.
The exclusion criteria were as follows: severe mental disorders or cognitive impairment; other serious chronic conditions, including cardiovascular, hepatic, renal, gastrointestinal, haematologic, infectious diseases, or malignant tumours; contraindications to manual therapy, including bleeding tendency or local infection at acupuncture points; pregnancy; refusal to follow the treatment course; or participation in another clinical study. Eligible participants provided informed consent before enrolment.
Randomisation and Masking
A researcher not involved in any other trial process handled the randomisation process, including sequence generation, envelope preparation, and group allocation concealment. The random sequence was generated using SPSS software (IBM SPSS Statistics Version 26; Armonk, NY, USA). Participants were randomly assigned to receive Jingjin or general manual therapy, following a 1:1 allocation ratio. A sealed opaque envelope concealing the group allocation was placed within the folder of each patient. Given the nature of the intervention, patients and therapists were not blinded to the group allocations. However, researchers responsible for data collection and analysis were blinded.
Interventions
All participants underwent six manual therapy sessions: three during the first 3 days and three within the subsequent 6 days. The treatments were administered by a team of three therapists, each with over 5 years of TCM education and over 2 years of clinical experience.
Jingjin Therapy
Jingjin theory suggests that the Shaoyin meridian of the foot has specific therapeutic properties for treating posterior extension dysfunction. We targeted the segment of the Shaoyin meridian that traverses from the ankle to the knee joint.
The intervention group received acupressure applied to the Taixi (KI3), Zhubin (KI9), and Yingu (KI10) points on the affected side, with pressure intensity standardised to elicit the sensation of deqi.20 Additionally, the therapists applied kneading techniques along the Shaoyin meridian tendon from the ankle to the knee, with the strength of manipulation guided by the sensation of qi. Each session lasted 25 min, with 15 min dedicated to acupoint pressing and 10 min to the meridian tendon kneading technique (specific procedural details are illustrated in Supplementary Figures 1–5).
General Manual Therapy
The general manual therapy protocol was based on clinical guidelines and previous research.21,22
Patients in this group received a 9-min massage to relax stiff soft tissues in the neck, shoulders, and upper back. This was followed by a 5-min acupressure session targeting the Fengchi (GB20), Jianjing (GB21), and Jianzhongshu (SI15) points on the painful side. The acupressure intensity was modulated based on the patient’s sensation of ‘deqi’, often characterised by dull pain, numbness, heaviness, or soreness. Subsequently, a 1-min passive stretch was applied to the upper trapezius muscle on the affected side. Each patient underwent six 25-min sessions, with 15 min dedicated to acupoint stimulation and 10 min to soft tissue relaxation (specific procedural details are illustrated in Supplementary Figures 6–10).
As aforementioned, the initial treatment phase comprised three daily sessions, followed by three other sessions over the subsequent 6 days, with an optimal 2-day interval between sessions. A follow-up was conducted 1 week after treatment completion. Consistency of care was maintained by assigning the same therapist to each participant throughout the trial, whenever possible. Additionally, therapists were instructed not to disclose the group assignments of participants and to answer questions without offering confident or overly positive reassurances regarding outcomes.
All participants were advised not to use any other NCNP-related pain control interventions, including medications and acupuncture, which could have affected the study results. The utilisation of other therapeutic modalities was meticulously recorded in the Case Report Form to ensure transparency and control for potential confounding factors.
All therapists completed a standardised 40-h training program on Jingjin therapy protocols, which included practical demonstrations of key techniques (eg, muscle tension release and meridian alignment) and competency assessments to ensure protocol adherence. Senior TCM practitioners with over 10 years of clinical experience supervised the training sessions.
Assessments and Outcomes
Primary Outcome
The primary outcome was the change in the angle of active neck extension measured using the CROM3 device after the sixth treatment and one week after treatment. The CROM3 device is widely recognised for its excellent reliability and validity in assessing cervical spine angles.23
Each angle was evaluated twice, with the average value being recorded. Active range of motion (AROM) was assessed when the patient experienced neck pain or reached the limiting position accompanied by a pulling sensation.
Secondary Outcomes
Secondary outcomes included the following: (1) neck pain intensity; (2) neck functionality; and (3) properties of relevant muscle groups, including tension, firmness, and elasticity.
A 10-cm horizontal VAS was used to assess pain during active neck extension. The VAS is a universally accepted, reliable, and valid tool for assessing pain intensity.24 The scale ranges from 0 (‘no pain’) to 10 cm (‘the most severe pain’). VAS is more patient-friendly than other pain assessment scales.25
The neck disability index (NDI) was used to assess neck functionality during daily activities. It comprises 10 questions, each with 6 response options ranging from 0 (no disability) to 5 (total disability), with a total possible score of 0–50. A total NDI score <5, 5–14, 15–24, 25–34, and >35 indicates no, mild, moderate, severe, and total disability, respectively. The NDI has good reliability and validity.26
The MyotonPRO device was used to measure muscle properties such as tension, elasticity, and stiffness in the upper trapezius and semispinalis capitis muscles, which are crucial for neck extension. After 1 week of training, an evaluator placed the device on the targeted muscle of the seated participant and took readings when a green light appeared, following a beep. The MyotonPRO is a reliable tool, as demonstrated by its consistent performance across different patient populations.27
Outcome assessments were conducted at baseline, after each treatment session (on days 1, 2, 3, 5, 7, and 9), and at 1-week post-treatment.
Adverse Event Monitoring
After the intervention, adverse events were documented and categorised as minor or major. Minor events included transient discomfort, including pain during the session, soreness for up to 48 h, or stiffness not requiring further intervention. Major events included prolonged pain lasting ≥72 h, serious complications, or symptom exacerbation requiring additional assessment and medical attention. Patients were instructed to report any adverse events at the beginning and end of each session. All reported events were meticulously recorded in the data files of patients for monitoring and review.
Statistical Analyses
The sample size was calculated using PASS 15 software, based on the primary outcome of active neck extension angle. Assuming a two-sided significance level of α = 0.05, a statistical power of 80% (1–β = 0.80), and a medium effect size of Cohen’s d = 0.5 for the between-group comparison, the required total sample size was 128. Allowing for a 20% attrition rate, the final required sample size was 160 participants (n = 80 per group).
This study adhered to the intention-to-treat principles. Categorical variables are presented as frequencies and proportions. Normally and non-normally distributed continuous variables are reported as mean ± standard deviation and median with interquartile range, respectively. Missing data were addressed through multiple imputations (five imputations).
A repeated-measures linear mixed-effects model was employed to assess between-group differences in outcomes, with group allocation and treatment time points treated as fixed effects and participants as random effects. An autoregressive correlation structure (AR(1) model) was selected for the covariance pattern owing to decreased correlation between repeated measures over time. Mean differences and 95% confidence intervals (CIs) were calculated for each outcome measure.
A per-protocol analysis was performed as per the intention-to-treat (ITT) analysis, with restriction to participants who underwent Jingjin therapy within 16 days after randomisation and primary outcome assessment within the specified window, compared to those randomised to the control group and remained within that group.
Per-treatment analysis was performed as per the ITT analysis, with a comparison of all participants who underwent Jingjin and general manual therapy at any time during follow-up, regardless of initial randomisation group, and completed the primary outcome assessment within the specified window.
Subgroup analyses were conducted based on sex, age, body mass index (BMI), disease duration, and pain location. Sensitivity analyses were performed for the primary outcome and pain intensity across various datasets, including the per-protocol, safety analysis, and the set with missing data excluded.
Statistical significance was set at P < 0.05 for two-tailed tests. Statistical analyses were conducted using SPSS software version 26 (SPSS Inc).
Patient and Public Involvement in Research
Participants were not involved in the study’s design, conduct, interpretation, or translation.
Results
Baseline Characteristics
Between May 2023 and February 2024, 1752 patients were screened for the study. Among them, 163 declined to participate for personal reasons, and 1429 did not meet the eligibility criteria. Finally, 160 patients (mean age, 34.49±11.24 years) were recruited, with 80 randomly assigned to each group. During the 16-day trial, 17 participants (10.6%) withdrew from the trial (10 and 7 in the intervention and control groups, respectively). No major between-group differences were observed in baseline characteristics, including age, BMI, year of education, duration of symptoms, and employment status. Both groups had a higher number of female patients than male patients (Table 1). The trial flow chart is illustrated in Figure 1.
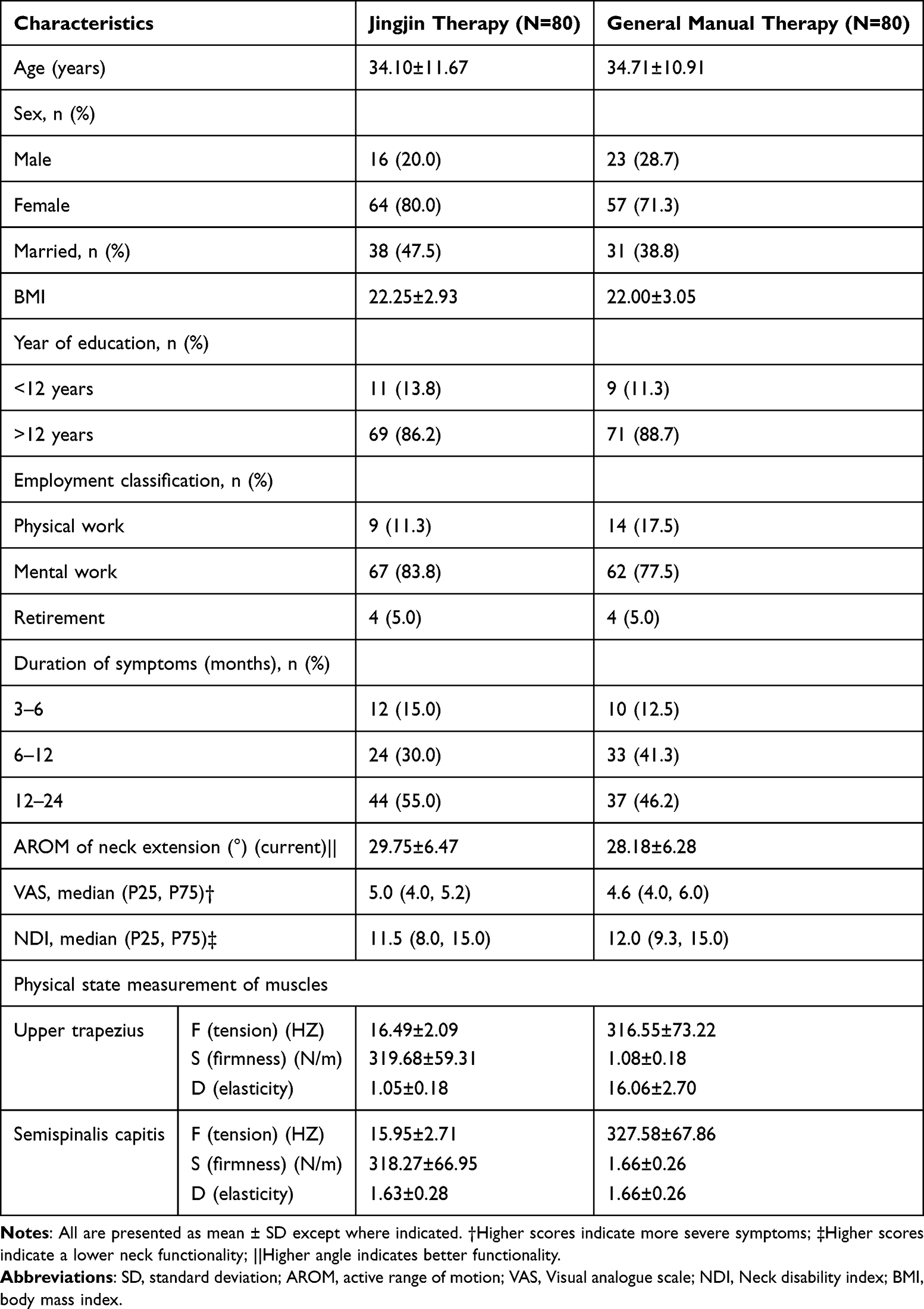 |
Table 1 Baseline Characteristics of Participants |
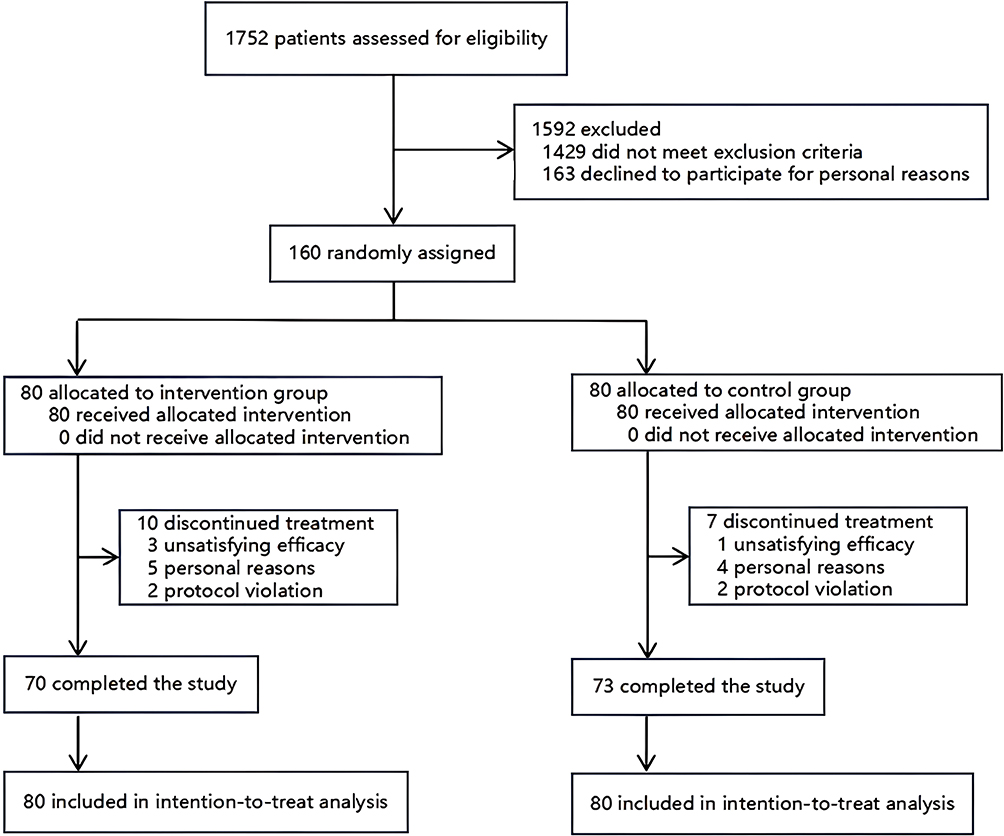 |
Figure 1 CONSORT participants flow diagram. CONSORT, Consolidated Standards of Reporting Trials. |
Primary Outcome
By the sixth treatment session, the mean AROM improved from 29.75° (95% CI: 27.61°, 31.89°) to 51.97° (95% CI: 49.75°, 54.20°) and from 28.18° (95% CI: 26.03°, 30.32°) to 52.49° (95% CI: 50.26°, 54.72°) in the intervention and control groups, respectively. The mean between-group difference of the main group effect was −0.26° (95% CI: −2.62°, 2.09°) (Table 2).
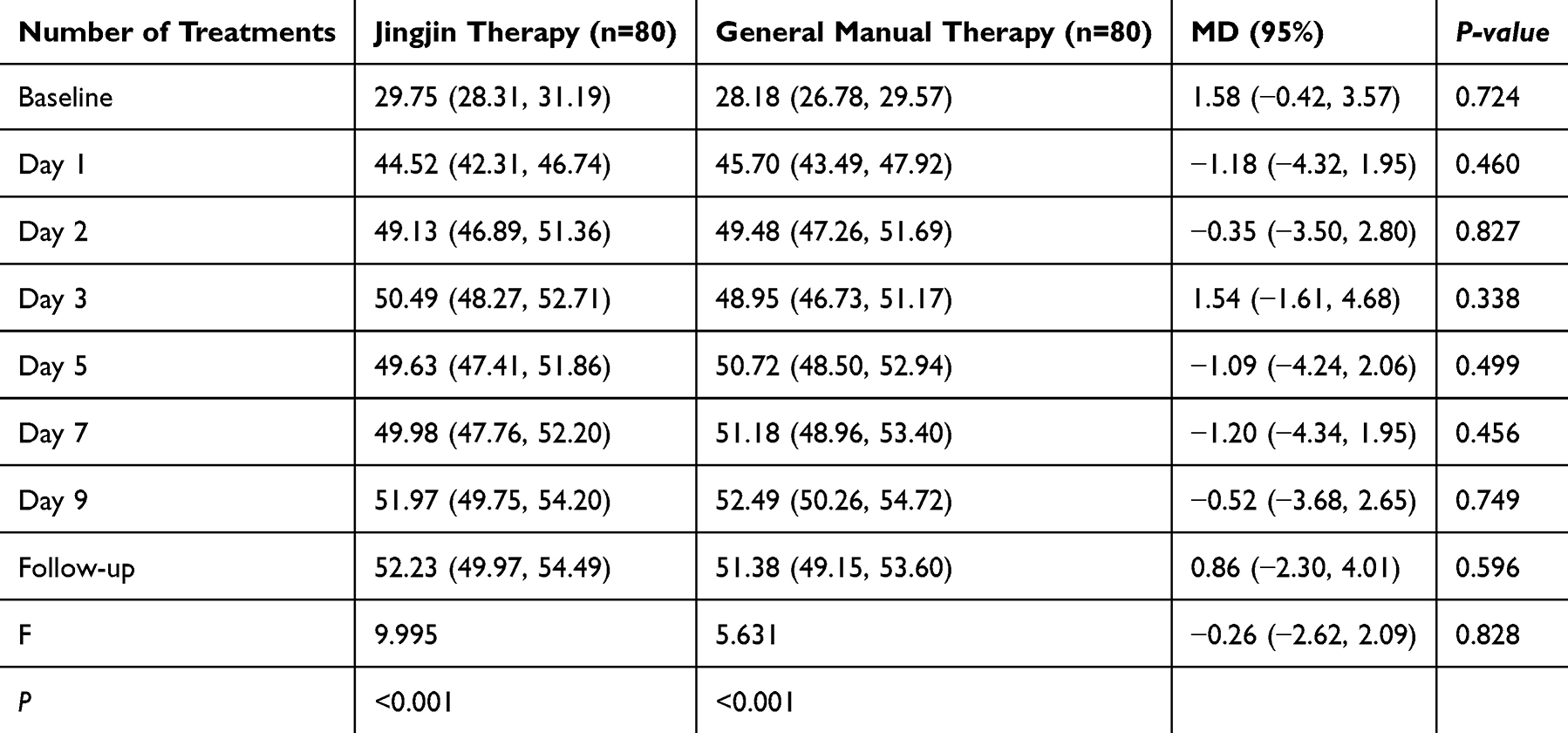 |
Table 2 Angle of Active Neck Extension in Both Groups |
No significant between-group difference was observed in AROM improvement (P = 0.828). The results were consistent across multiple imputations, including the per-protocol, safety analysis, and missing data excluded sets (Figure 2).
 |
Figure 2 Primary outcomes for both groups. Abbreviation: AROM, active range of motion. Notes: ** denotes statistically significant within-group differences (p < 0.01) in the Jingjin therapy group; ## indicates statistically significant within-group differences (p < 0.01) in the general manual therapy group. |
Secondary Outcome
No significant difference was observed in physical functioning, measured using the VAS, for pain intensity between the two groups (P = 0.116). The mean difference of the main group effect between the two groups was −0.26 (95% CI: −0.58, 0.06) (Figure 3). Similarly, no significant between-group difference was observed in the NDI for neck functionality (P = 0.113). The mean between-group difference of the main group effect was −0.62 (95% CI: −1.38, 0.15) (Figure 4).
 |
Figure 3 Changes in VAS. VAS, visual analogue scale. Notes: ** denotes statistically significant within-group differences (p < 0.01) in the Jingjin therapy group; ## indicates statistically significant within-group differences (p < 0.01) in the general manual therapy group. |
 |
Figure 4 Changes in NDI. NDI, neck disability index. Notes: ** denotes statistically significant within-group differences (p < 0.01) in the Jingjin therapy group; ## indicates statistically significant within-group differences (p < 0.01) in the general manual therapy group. |
In terms of muscle physical state, the general manual therapy group exhibited significantly greater reductions in muscle firmness and tension than the Jingjin therapy group (P < 0.001). Specifically, the mean differences in muscle tension and firmness were 0.47 (95% CI: 0.19, 0.74) and 13.81 (95% CI: 5.46, 22.16), respectively. The most pronounced differences in muscle tension and stiffness of the upper trapezius muscle occurred following the fourth treatment session.
No significant between-group difference was noted in muscle tension (P = 0.106) or firmness (P = 0.367) of the semispinalis capitis. The mean between-group differences in muscle tension and firmness were 0.28 (95% CI: −0.06, 0.62) and 4.15 (95% CI: −4.86, 13.16), respectively.
No major adverse events were observed in either group. A few minor adverse events (Table 3) were noted in both groups.
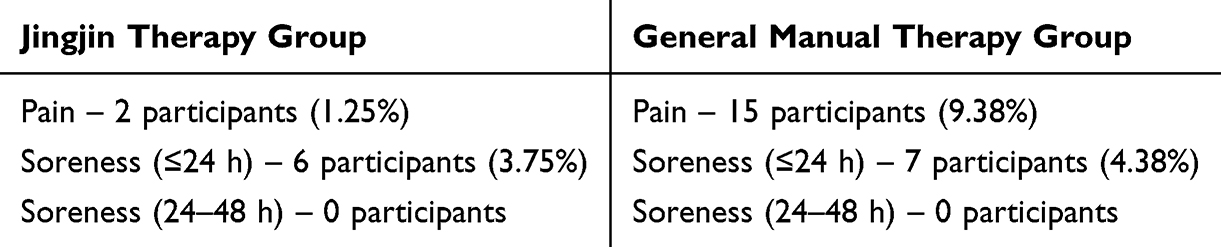 |
Table 3 Adverse Events |
Since all non-compliers in this study were directly lost to follow-up and no one from the other group received treatment, the per-protocol set, safety analysis set, and data set with missing data deleted in this study were identical. Therefore, the sensitivity analysis was conducted only on the original unimputed data. In the unimputed data, the improvement effects of the intervention group and the control group on the active posterior extension range of motion of the cervical spine (°), pain intensity (VAS), and cervical disability index (NDI) were consistent and statistically significant after imputation.
Discussion
Our findings demonstrated that Jingjin and general manual therapy significantly improved neck extension function, reduced pain, and enhanced neck functionality. Although Jingjin therapy resulted in greater improvements in pain and neck functionality than general manual therapy, these differences were smaller than the minimal clinically significant differences and were not statistically significant.
Regarding adverse reactions, the incidence of neck pain and soreness in the Jingjin therapy group was only 50% of that in the general manual therapy group. This may be because general manual therapy directly targets the pain area; this finding is consistent with previous studies.28,29 Jingjin therapy likely reduces adverse reactions by avoiding local stimulation that could irritate nerves and blood vessels. Moreover, the two manual therapies exhibited different effects on firmness and tension of muscles related to neck extension function. General manual therapy, which directly stimulates the muscles involved in extension, significantly reduced muscle tension and firmness. Conversely, Jingjin therapy, which does not directly contact the target muscles, achieved similar effects on the tension and firmness of the deep semispinalis capitis muscle.
Although the precise mechanisms underlying the effectiveness of distal acupoints remain unclear, current hypotheses suggest that they exert their analgesic effects by modulating the sympathetic nervous system and hypothalamic-pituitary-adrenocortical axis30 or through endogenous opioid release.31 TCM posits that distal acupoint stimulation can regulate qi in deeper tissues through the Jingjin system, contributing to disease recovery. This is consistent with our findings and may provide new insights into effective distal interventions.
A previous study32 reported that distal acupressure, which utilises fewer acupoints than local acupressure, yielded better overall effectiveness in pain management; however, there are no standardised protocols for selecting distal acupoints. In our study, although we observed no significant between-intervention difference in clinical efficacy, their clinical implications differ significantly from a socioeconomic perspective. Jingjin therapy is a treatment approach that combines distant acupoints with manual therapy, providing a safer and more acceptable approach than local treatment of the cervical spine and other intervention types such as acupuncture. Further, it is suitable for implementation in the initial stage of NCNP treatment. Additionally, prior to treatment for neck pain, high-level imaging tests are often required, which increases the treatment time for patients and may lead to overtreatment.33 In the United States, neck pain accounts for tens of billions of dollars in healthcare costs annually.34 Therefore Jingjin therapy may offer an approach for addressing this waste of medical resources.
Jingjin therapy and modern medical techniques including physiotherapy show distinctive features in the treatment of neck pain. Rooted in traditional Jingjin theory, Jingjin therapy systematically stimulates acupuncture points and myofascial knots to regulate the flow of qi and blood and loosen fascial adhesions. Its advantages lie in holistic treatment, non-invasiveness and immediate pain relief, but its efficacy still needs to be further verified by clinical research. Modern medical techniques are based on biomechanics and neurophysiology using structured rehabilitation programmes including joint release, neuromuscular training, physical modalities (eg ultrasound, interventional current therapy) and progressive exercise prescription. These approaches are supported by reliable evidence-based research and allow for quantitative outcome assessment.
The two therapeutic modalities complement each other in terms of therapeutic dimensions: Jingjin therapy emphasises whole-body meridian regulation, and modern medicine focuses on restoring local biomechanical balance. Although this study primarily examined the clinical efficacy of jingjin therapy, future research could explore its synergistic mechanisms with modern rehabilitation techniques (eg, Maitland joint release, McKenzie mechanotherapy). By designing a multi-centre controlled trial to compare the differences in effects of different intervention modalities, it will help to construct a precise diagnostic model for the integration of Chinese and Western medicine, and provide a theoretical basis for the development of an individualised integrated treatment plan for neck pain. The organic connection between traditional therapy and modern medicine is realised.
This study has several limitations. First, given the nature of the interventions, we could not blind the therapists and participants, which could introduce potential bias. However, to mitigate this, the investigators responsible for data collection, outcome measurement, and statistical analyses were blinded. Second, an intensive manual therapy programme was adopted, which may have improved the treatment effects but could hinder the widespread adoption. Finally, the study period was relatively short compared to that of other pharmacological trials, which usually extend beyond 12 weeks.
In summary, the Jingjin theory, a cornerstone of TCM for treating musculoskeletal pain, enables targeted treatment of specific distal acupoints based on accompanying symptoms. Jingjin therapy plays an important role in the early clinical diagnosis and treatment of neck pain given its high safety and patient acceptability. Therefore, Jingjin therapy is recommended to be used in early-stage neck pain interventions.
Conclusion
After 9 days of Jingjin therapy, patients with NCNP experienced a significant increase in the angle of active neck extension, with no significant differences compared to general manual therapy. Future studies should explore the efficacy of Jingjin therapy in combination with other interventions in patients with different types of neck pain.
Abbreviations
AROM, active range of motion; ITT, Intention-to-treat; NCNP, Non-specific chronic neck pain; NDI, Neck disability index; TCM, Traditional Chinese Medicine; VAS, Visual analogue scale.
Data Sharing Statement
De-identified sections of the dataset are available from the corresponding author upon reasonable request at the time of publication.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the Second Affiliated Hospital of Hunan University of Chinese Medicine (ID: 2023-KY-021) and registered in the Chinese Clinical Trial Registry (ID: ChiCTR2300068892). Eligible participants provided informed consent before enrolment.
Author Contributions
All authors made a significant contribution to the work, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. They participated in drafting, revising or critically reviewing the article, gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and accepted accountability for all aspects of the work.
Funding
This work was supported by the Hunan Provincial Young Science and Technology Talents (Hejian) Project (2022RC1221). The study design, execution, analysis, interpretation of data, and reporting of results were conducted independently of the funding sources.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD. Diseases and injuries collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
2. Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. 2017;358:j3221. doi:10.1136/bmj.j3221
3. Esakki S, MacDermid JC. Appraisal of: management of neck pain and associated disorders: a clinical practice guideline from the Ontario Protocol for Traffic Injury Management (Optima) collaboration. J Physiother. 2018;64(1):62. doi:10.1016/j.jphys.2017.07.011
4. Safiri S, A–A K, Hoy D, et al. Global, regional, and national burden of neck pain in the general population, 1990–2017: systematic analysis of the global burden of disease study 2017. BMJ. 2020;368:m791. doi:10.1136/bmj.m791
5. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–147. doi:10.1016/j.mayocp.2014.09.010
6. Cohen SP. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clin Proc. 2015;90(2):284–299. doi:10.1016/j.mayocp.2014.09.008
7. Aegerter AM, Deforth M, Volken T, et al. A multi–component intervention (NEXpro) reduces neck pain–related work productivity loss: a randomized controlled trial among Swiss office workers. J Occup Rehabil. 2023;33(2):288–300.
8. Pieper C, Schröer S, Eilerts AL. Evidence of workplace interventions–A systematic review of systematic reviews. Int J Environ Res Public Health. 2019;16(19):3553. doi:10.3390/ijerph16193553
9. Giménez–Costa M, Schomacher J, Murillo C, Blanco–Hernández T, Falla D, Lluch E. Specific versus non–specific exercises for the neck extensor muscles in women with chronic idiopathic neck pain: a randomized controlled trial. Musculoskelet Sci Pract. 2022;60:102561. doi:10.1016/j.msksp.2022.102561
10. Yajima H, Nobe R, Takayama M, Takakura N. The mode of activity of cervical extensors and flexors in healthy adults: a cross–sectional study. Medicina. 2022;58(6):728. doi:10.3390/medicina58060728
11. Tsiringakis G, Dimitriadis Z, Triantafylloy E, McLean S. Motor control training of deep neck flexors with pressure biofeedback improves pain and disability in patients with neck pain: a systematic review and meta–analysis. Musculoskelet Sci Pract. 2020;50:102220. doi:10.1016/j.msksp.2020.102220
12. Blanpied PR, Gross AR, Elliott JM, et al. Neck pain: revision 2017. J Orthop Sports Phys Ther. 2017;47(7):A1–A83. doi:10.2519/jospt.2017.0302
13. Li Y, Hou Y, Sun J, et al. Therapeutic effect of acupotomy at Sanheyang for cartilage collagen damage in moderate knee osteoarthritis: a rabbit model. J Inflamm Res. 2023;16:2241–2254. doi:10.2147/JIR.S400956
14. Ishaq I, Mehta P, Skinner IW, Bagg MK, Bier J, Verhagen AP. Treatment classifications and interventions for neck pain: a scoping review. J Clin Epidemiol. 2023;159:1–9. doi:10.1016/j.jclinepi.2023.04.010
15. Smith MS, Olivas J, Smith K. Manipulative therapies: what works. Am Fam Phys. 2019;99(4):248–252.
16. Gong Z, Guo Y, Liu X, Ai K, Li W, Li J. Bibliometric analysis of research trends on tuina manipulation for neck pain treatment over the past 10 years. J Pain Res. 2023;16:2063–2077. doi:10.2147/JPR.S410603
17. Kang X, Huang Y, Zheng Y, et al. Meta–analysis of the efficacy of Jingjin acupuncture therapy in the treatment of spastic cerebral palsy. Front Neurol. 2024;15:1358732. doi:10.3389/fneur.2024.1358732
18. Pandis N, Turpin DL. Enhancing CONSORT compliance for improved reporting of randomized controlled trials. Am J Orthod Dentofacial Orthop. 2014;145(1):1. doi:10.1016/j.ajodo.2013.11.005
19. Falci SGM, Marques LS. CONSORT: when and how to use it. Dent Press J Orthod. 2015;20(3):13–15.
20. Zhou K, Fang J, Wang X, et al. Characterization of de qi with electroacupuncture at acupoints with different properties. J Altern Complement Med. 2011;17(11):1007–1013. doi:10.1089/acm.2010.0652
21. Llamas–Ramos R, Pecos–Martín D, Gallego–Izquierdo T, et al. Comparison of the short–term outcomes between trigger point dry needling and trigger point manual therapy for the management of chronic mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. 2014;44(11):852–861. doi:10.2519/jospt.2014.5229
22. Zhang W, Li J, Lou B, et al. Clinical practice guidelines for rehabilitation in traditional Chinese medicine – xiang paralysis (cervical spondylosis). RM. 2020;30:337–342. doi:10.3724/sp.j.1329.2020.05002
23. Audette I, J–P D, Côté JN, De Serres SJ. Validity and between–day reliability of the cervical range of motion (CROM) device. J Orthop Sports Phys Ther. 2010;40(5):318–323. doi:10.2519/jospt.2010.3180
24. Modarresi S, Lukacs MJ, Ghodrati M, et al. A systematic review and synthesis of psychometric properties of the numeric pain rating scale and the visual analog scale for use in people with neck pain. Clin J Pain. 2021;38(2):132–148. doi:10.1097/AJP.0000000000000999
25. He S, Renne A, Argandykov D, Convissar D, Lee J. Comparison of an emoji–based visual analog scale with a numeric rating scale for pain assessment. JAMA. 2022;328(2):208–209. doi:10.1001/jama.2022.7489
26. Young IA, Dunning J, Butts R, Mourad F, Cleland JA. Reliability, construct validity, and responsiveness of the neck disability index and numeric pain rating scale in patients with mechanical neck pain without upper extremity symptoms. Physiother Theor Pract. 2019;35(12):1328–1335. doi:10.1080/09593985.2018.1471763
27. Lettner J, Królikowska A, Ramadanov N, et al. Evaluating the reliability of myotonpro in assessing muscle properties: a systematic review of diagnostic test accuracy. Medicina. 2024;60(6):851. doi:10.3390/medicina60060851
28. Paanalahti K, Holm LW, Nordin M, Asker M, Lyander J, Skillgate E. Adverse events after manual therapy among patients seeking care for neck and/or back pain: a randomized controlled trial. BMC Musculoskelet Disord. 2014;15(1):77.
29. Smith WS, Johnston SC, Skalabrin EJ, et al. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology. 2003;60(9):1424–1428. doi:10.1212/01.wnl.0000063305.61050.e6
30. McFadden KL, Hernández TD. Cardiovascular benefits of acupressure (Jin Shin) following stroke. Complement Ther Med. 2010;18(1):42–48. doi:10.1016/j.ctim.2010.01.001
31. Trentini JF, Thompson B, Erlichman JS. The antinociceptive effect of acupressure in rats. Am J Chin Med. 2005;33(1):143–150. doi:10.1142/S0192415X05002746
32. C–Y K, Lee B. Clinical effects of acupressure on neck pain syndrome (nakchim): a systematic review. Integr Med Res. 2018;7(3):219–230. doi:10.1016/j.imr.2018.01.002
33. Mokdad AH, Ballestros K, Echko M, et al. US Burden of Disease Collaborators. The state of US health, 1990–2016: burden of diseases, injuries, and risk factors among US States. JAMA. 2018;319(14):1444–1472. doi:10.1001/jama.2018.0158.
34. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996–2016. JAMA. 2020;323(9):863–884. doi:10.1001/jama.2020.0734
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Thoracic Spine Manipulation on the Management of Neck Pain: A Systematic Review and Meta-Analysis of Randomized Control Trials
Tsegay GS, Gebregergs GB, Weleslassie GG, Hailemariam TT
Journal of Pain Research 2023, 16:597-609
Published Date: 27 February 2023