")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Effects of Intelligence Levels and Autistic Severity on Adaptive Functioning and Cognitive-Adaptive Functioning Gaps in School-Aged Children with Autism Spectrum Disorder
Authors Jin WY, Song C, Wang YY, Liu XL, Li WH, Wu LL, Zhu ZW
Received 6 March 2025
Accepted for publication 23 May 2025
Published 4 June 2025 Volume 2025:21 Pages 1131—1142
DOI https://doi.org/10.2147/NDT.S524042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yu-Ping Ning
Wen-Yuan Jin, Chao Song, Yan-Yan Wang, Xiao-Lin Liu, Wen-Hao Li, Ling-Ling Wu, Zhi-Wei Zhu
Department of Developmental Behavioral Pediatrics, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Zhi-Wei Zhu; Ling-Ling Wu, Department of Developmental Behavioral Pediatrics, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, No. 3333 Binsheng Road, Hangzhou, Zhejiang Province, 310052, People’s Republic of China, Email [email protected]; [email protected]
Purpose: The aim of our study was to explore the underlying influencing factors of adaptive functioning and cognitive-adaptive functioning gaps in school-aged children with autism spectrum disorder (ASD).
Patients and Methods: Adaptive functioning of our subjects (n=107) were evaluated via Adaptive Behavior Assessment System (ABAS). Wechsler Intelligence Scale for Children (WISC) and Autism Diagnostic Observation Schedule (ADOS) were applied to assess the intelligence levels and autistic severity of them, respectively. Spearman correlation analyses were applied to investigate the associations between intelligence levels, autistic symptoms and adaptive functioning and cognitive-adaptive functioning gaps. Hierarchical regressions were performed to examine the effects of demographic data, cognitive levels, autistic severity and behavioral factors on General Adaptive Composite (GAC).
Results: Verbal Comprehension Index (VCI), Perceptual Reasoning Index (PRI), Working Memory Index (WMI) and Processing Speed Index (PSI) of WISC were positively correlated with Conceptual, Social domains and GAC (P< 0.01). There were positive correlations between VCI, PRI and PSI and Practical domain (P< 0.01). Positive associations were discovered between full-scale intelligence quotient (FSIQ) and the three domains and GAC in ABAS (P< 0.01). Social Affect (SA), Restricted and Repetitive Behavior (RRB) and Total scores of ADOS were negatively correlated with the three domains (P< 0.05). Comparison Scores were negatively correlated with Conceptual and Social domains (P< 0.05). Negative correlations were found between SA, RRB, Total scores, Comparison Scores and GAC (P< 0.05). VCI, PRI, WMI, PSI and FSIQ were positively correlated with FSIQ-Conceptual, FSIQ-Social, FSIQ-Practical and FSIQ-GAC gaps (P< 0.01). SA was inversely correlated with FSIQ-Conceptual and FSIQ-Practical gaps (P< 0.05). Total scores were inversely correlated with FSIQ-Conceptual, FSIQ-Practical and FSIQ-GAC gaps (P< 0.05). Hierarchical regressions showed that FSIQ was positively correlated with GAC in the total model (P=0.015); whereas RRB was inversely correlated with GAC (P=0.014).
Conclusion: Intelligence levels and autistic severity were important contributors of adaptive functioning and cognitive-adaptive functioning gaps in children with ASD.
Keywords: autism spectrum disorder, adaptive functioning, cognitive-adaptive functioning gap, intelligence, severity
Introduction
Adaptive functioning describes how well an individual manages the demands of daily life independently, including requirements in socialization, communication, home living, self-care, leisure and community participation.1 Autism spectrum disorder (ASD) is a complex neurodevelopmental disorder characterized by impaired social interaction, restricted and repetitive patterns of behavior beginning early in life.2 The prevalence of ASD in mainland China is estimated to be 0.7% according to a recent literature.3 Children with ASD frequently display weak adaptive behavior functions compared with typically developing children.4–6 Although some ASD individuals have high intelligence quotient (IQ) and are gifted in reasoning and mechanical memory (especially for high-functioning ASD), they still have difficulties in developing their adaptive functioning. Previous research discovered significant discrepancies between IQ scores and adaptive functioning scores in children with ASD, particularly in those autistic individuals without intellectual disabilities.5–8 The gap can be observed both in ASD males and females, starting from toddlerhood and persisting into young adulthood.8–10 This phenomenon suggests that autistic individuals have challenges in translating their intellectual potentials into capabilities for independent living. It is noteworthy that deficits in adaptive functioning of individuals with ASD can impose a heavy burden on both families and society.
Several studies have explored underlying factors influencing adaptive functioning and IQ-adaptive functioning gaps in children with ASD. It has been discovered that adaptive functioning is negatively associated with severity of autistic symptoms. That means more severe social deficits and repetitive stereotyped behaviors predict poorer adaptive functioning of ASD individuals.11 However, a population-based cohort study investigated 421 preschool children with ASD, and revealed the cross-trajectory overlap between autistic symptom severity and adaptive functioning was relatively low.12 Another large cohort study surveyed 2538 school-aged children with ASD and discovered poor associations between adaptive behavior scores and ASD severity.13 Research from Lee et al14 found different temperaments (“even” and “reactive”) might influence the relationship between symptom severity and adaptive behavior functions as a mediator. IQ is another important determinant in the development of adaptive functioning for children with ASD. It has been reported that IQ scores are positively correlated with communication skills, social skills and global adaptive behaviors.4,11 Worse intellectual performance, especially in verbal comprehension and working memory, significantly impacts adaptive functioning.15 Additionally, evidence from previous studies suggested early intensive behavioral intervention (EIBI) effectively improved adaptive behavior skills in young ASD individuals, including daily living skills and motor skills.16–18 If ASD coexisted with attention deficit hyperactivity disorder (ADHD), the symptoms of ADHD exacerbated adaptive functioning impairments.19,20 Furthermore, sex differences of adaptive behaviors were demonstrated in children with ASD. Two studies discovered females with ASD performed worse in social functions, executive functions and daily living skills compared to their male counterparts.21,22 Socioeconomic status was found to be associated with domain-specific communication skills and global adaptive functioning compared to basic demographic factors alone (such as age and gender).23 Additionally, autistic children without intellectual disabilities showed greater IQ-adaptive functioning gaps than those with intellectual disabilities.7 Psychiatric comorbidities (eg, depression and anxiety) were negatively correlated with adaptive functioning in adults with ASD but without intellectual disabilities. There were positive correlations between depression and anxiety symptoms and cognitive-adaptive functioning gaps in autistic adults without intellectual disabilities.10
Adaptive functioning is a critical determinant of outcomes in autistic children (ie, academic performance, employment, self-care, prosocial behaviors and community integration during adolescence and adulthood). It cannot be ignored that there are significant discrepancies between cognitive capabilities and adaptive functioning in children with ASD, particularly among those without intellectual disabilities. Exploring the factors influencing adaptive functioning development and cognitive-adaptive functioning gaps is of great importance. However, relatively few previous studies have addressed this topic in Chinese population. Our study attempts to further investigate the roles of multiple influencing factors in the development of adaptive functioning and cognitive-adaptive functioning gaps among Chinese school-aged children with ASD.
Material and Methods
Participants
Between January 2019 and 2022, 107 school-aged outpatients (6–16 years old) who visited the Department of Developmental Behavioral Pediatrics, Children’s Hospital, Zhejiang University School of Medicine and diagnosed with ASD were invited to participate in our study. Children with ASD were diagnosed based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) results and determined by two professionally qualified developmental behavioral pediatricians. The exclusion criteria were consisted of congenital malformations, inherited metabolic diseases and special chromosome abnormalities. Information about age, gender, place of residence, grade, sibling, parental education background, behavioral intervention was collected through questionnaires. Our study was approved by our hospital’s Clinical Research Ethics Committee. Informed consents were acquired from parents or caregivers of every participant.
Adaptive Behavior Assessment System, Second Edition
Adaptive Behavior Assessment System, Second Edition (ABAS-II) was applied to comprehensively and psychometrically evaluate the adaptive behavior functions of children with ASD in our study. The standardized Chinese version of ABAS-II was comparable to the US version in reliability and validity. ABAS-II was comprised of a General Adaptive Composite (GAC) score, three domain scores (Conceptual, Social and Practical) and ten skill area scores (Communication, Functional Academics, Self-Direction, Social, Leisure, Community Use, Home Living, Health and Safety, Self-Care and Work).24 Since our participants were under 17 years old and did not have any work experience, Work skill score was not contained in our ABAS-II scale. The Conceptual domain included Communication, Functional Academics and Self-Direction; the Social domain included Social and Leisure; the Practical domain included Community Use, Home Living, Health and Safety and Self-Care. All the ABAS-II questionnaires were finished by parents or caregivers of the subjects.
Autism Diagnostic Observation Schedule, Second Edition
Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) was a semi-structured, standardized assessment of communication, social interaction, play/imaginative use of materials, and restricted and repetitive behaviors for individuals who were suspected of ASD. It provided examiners with opportunities to observe behaviors which were directly relevant to the diagnosis of ASD at different developmental levels and chronological ages. It had been regarded as a “gold standard” assessment of ASD diagnosis across the world.25 The Overall total score of ADOS-2 was the sum of two algorithm domains: Social Affect (SA) and Restricted and Repetitive Behavior (RRB). The SA domain included items pertaining to “Communication” and “Reciprocal Social Interaction”, and the RRB domain included items pertaining to “Restricted and Repetitive Behaviors”. Comparison Scores in the ADOS-2 (obtained from Overall Total score and age) were applied to indicate the level of autism spectrum-related symptomatology when compared children with ASD of the same chronological age and language level. Comparison Scores ranged from 1 to 10. Comparison Scores in the 8-to-10 range indicated the individual displayed a high level of ASD related symptoms. Comparison Scores in the 5-to-7 range indicated the individual displayed a moderate level of ASD-related symptoms. Comparison Scores in the 3-to-4 range indicated the individual showed a relatively low level of ASD-related symptoms. Comparison Scores in the 1-to-2 range indicated the individual showed minimal-to-no evidence of ASD-related symptoms.
Wechsler Intelligence Scale for Children, Fourth Edition
Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV) was used to evaluate intellectual abilities of our participants. It was a widely applied measurement of IQ with good reliability and validity, which was consisted of four index scores: Verbal Comprehension Index (VCI), Perceptual Reasoning Index (PRI), Working Memory Index (WMI) and Processing Speed Index (PSI). WISC-IV had ten core subtests and five supplemental subtests. The VCI contained Vocabulary, Similarity, Comprehension, Information and Word Reasoning subtests; the PRI contained Block Design, Picture Concept, Matrix Reasoning and Picture Completion subtests; the WMI encompassed Digit Span, Letter-Number Sequencing and Arithmetic subtests; the PSI encompassed Coding, Symbol Search and Cancellation subtests. Full-scale IQ (FSIQ) was calculated on the basis of VCI, PRI, WMI and PSI.26 WISC-IV was conducted for every subject in our study by trained pediatricians.
Statistical Analysis
Characteristics such as age, gender, parental education, place of residence, behavioral factors, WISC-IV scores and ADOS-2 scores in our study were displayed as mean±SD, median (interquartile range, IQR) or N(%). Mann–Whitney U-test was used to explore the differences of adaptive functioning between male and female participants. Spearman correlation analyses were applied to investigate the associations between IQ scores (WISC-IV results), ASD-related symptoms (ADOS-2 results) and adaptive functioning (ABAS-II results). Spearman correlation analyses were also used to investigate the associations between IQ, autistic symptoms and cognitive-adaptive functioning gaps. Hierarchical regressions were performed in sequence to examine the effects of demographic characteristics, intelligence, ASD severity and behavioral factors on GAC (ABAS-II results) in children with ASD. All the analyses were performed through IBM SPSS statistics 25.0 version (SPSS Inc, Chicago, USA). P-values <0.05 were defined as statistically significant.
Results
Demographic Characteristics of Participants
Table 1 presented basic demographic characteristics of our participants. The average age of participants was 7.45±1.28 years. The majority of our subjects were male and resided in cities. About 65.4% of the fathers and 53.3% of the mothers received university or higher education. More than half of our ASD subjects were complicated with ADHD. However, only 31.8% of our participants had a record of EIBI. Subjects with ASD had advantages in PRI and disadvantages in VCI. FSIQ of our subjects ranged from 49 to 146. The median (IQR) of Comparison Score of ADOS-2 was 6 (4–8).
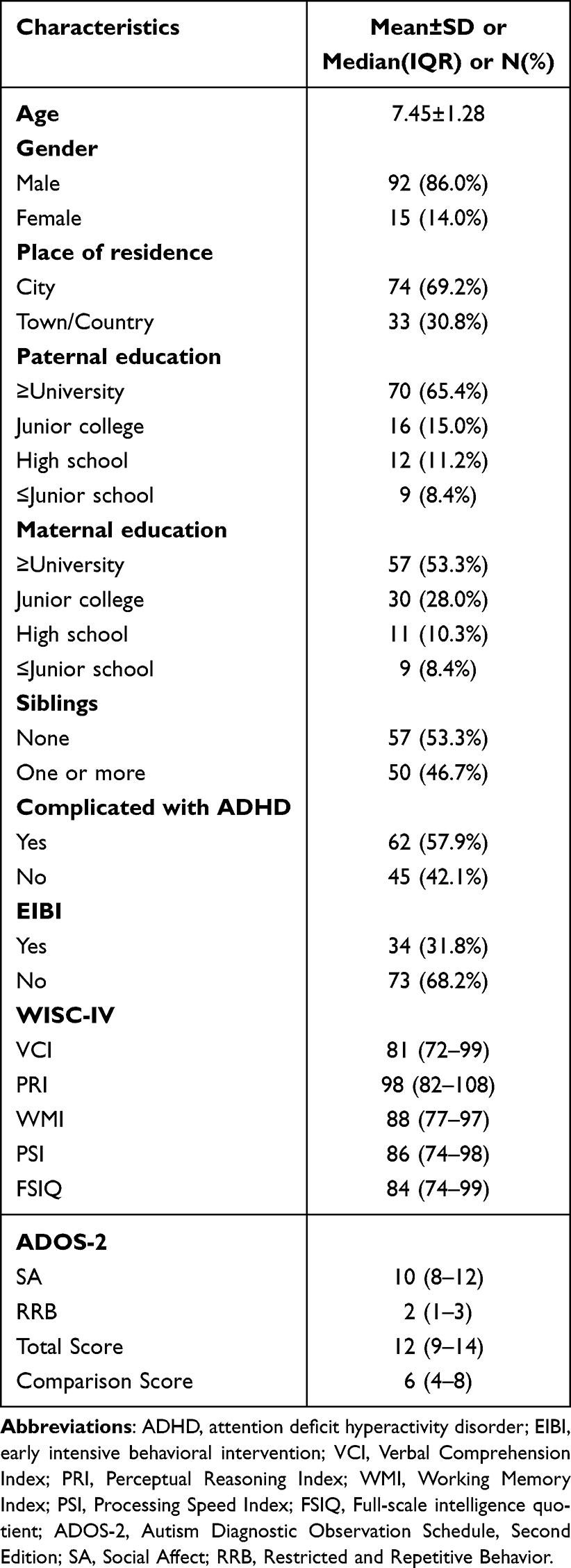 |
Table 1 Demographic Characteristics of Participants |
Adaptive Functioning Profile of Children with ASD
Table 2 demonstrated adaptive functioning profile of children with ASD and compared the differences between male and female subjects. The median (IQR) GAC of our subjects was 82 (74–96). Children with ASD obtained the lowest scores in Social and Self-Direction and the highest score in Community Use. Among the three domains, children with ASD had the lowest score in Social domain and the highest score in Practical domain. Boys were characterized with better performance in Community Use than girls (P=0.021). However, there were no significant differences between male and female ASD individuals in other adaptive behavior skills. There were no remarkable gender differences in the Conceptual, Social and Practical domains, either.
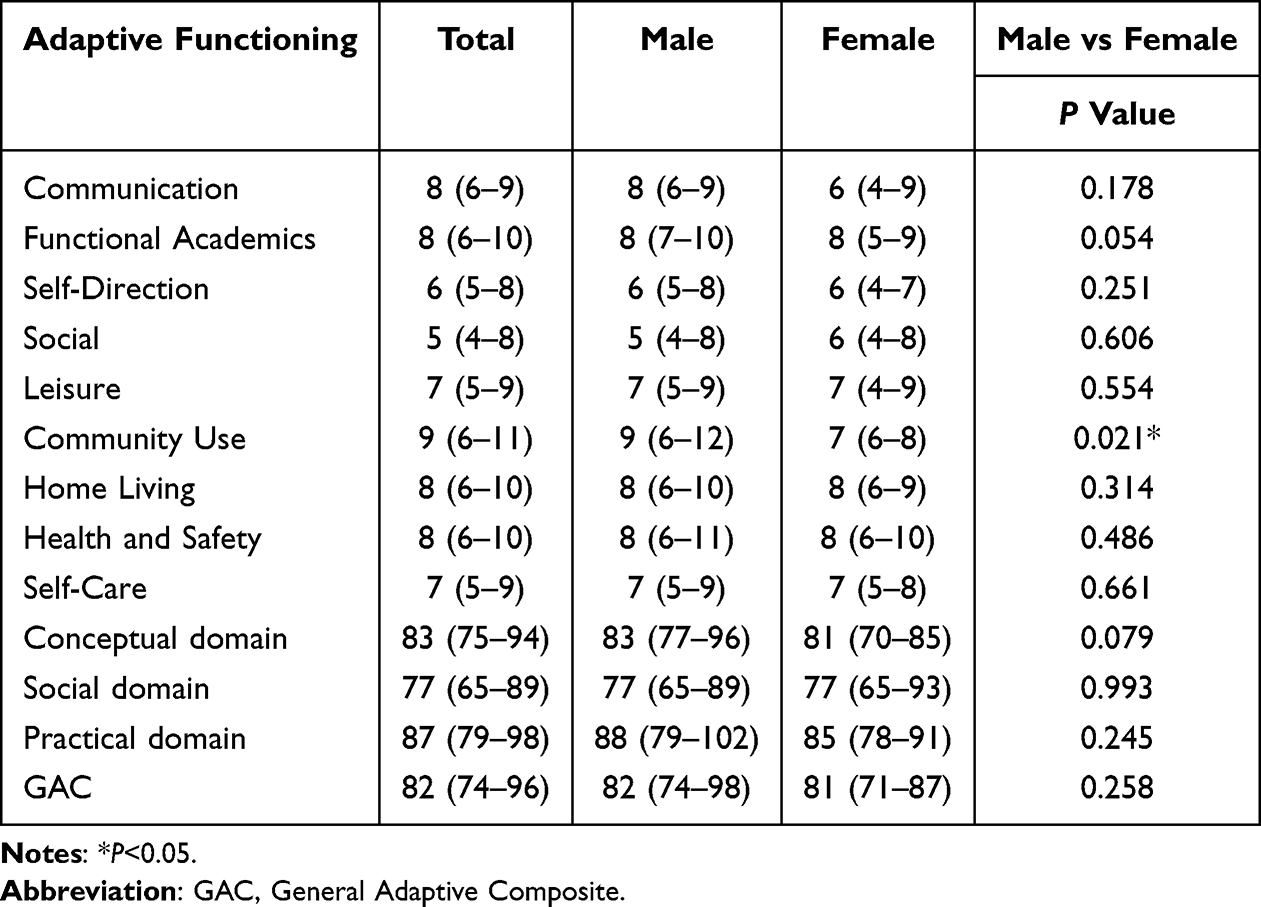 |
Table 2 Adaptive Functioning Profile of Children with Autism Spectrum Disorder |
Associations Between Intelligence, ASD Severity and Adaptive Functioning in Children with ASD
Table 3 showed associations between intelligence levels and adaptive functioning in children with ASD. VCI, PRI, WMI and PSI of WISC-IV were positively correlated with Conceptual domain, Social domain and GAC (P<0.01). There were positive correlations between VCI, PRI and PSI of WISC-IV and Practical domain (P<0.01). WMI had weak association with Practical domain without statistical significance. Furthermore, positive associations were discovered between FSIQ and Conceptual domain, Social domain, Practical domain and GAC (P<0.01).
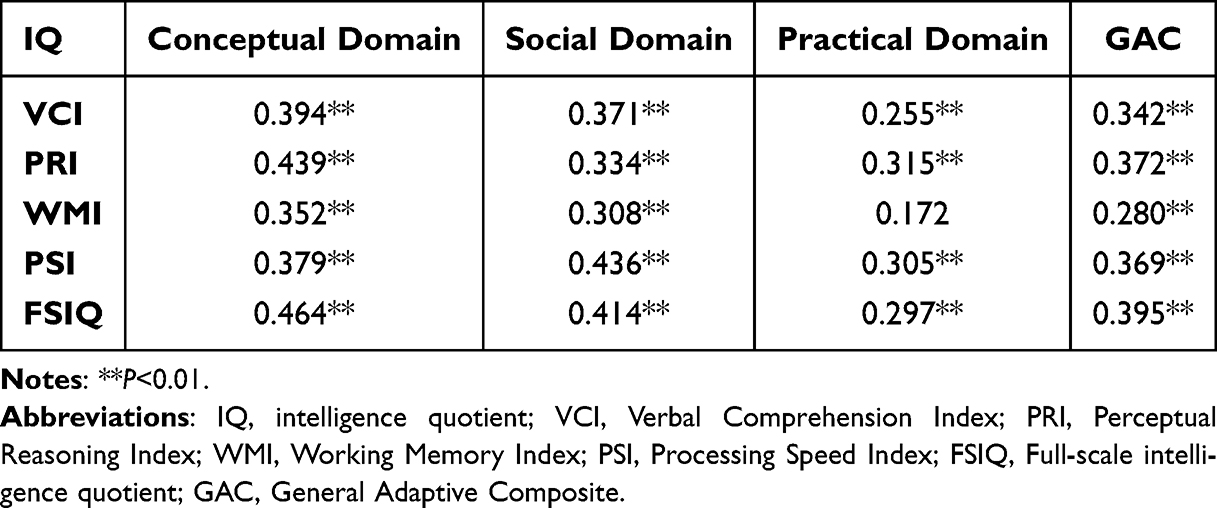 |
Table 3 Associations Between Intelligence Levels and Adaptive Functioning in Children with Autism Spectrum Disorder |
Table 4 displayed associations between ADOS-2 scores and adaptive functioning in children with ASD. SA scores, RRB scores and Total scores of ADOS-2 were negatively correlated with Conceptual, Social and Practical domains (P<0.05). Comparison Scores of ADOS-2 were negatively correlated with Conceptual domain and Social domain except for Practical domain (P<0.05). In addition, negative correlations were found between SA, RRB, Total scores and Comparison Scores of ADOS-2 and GAC (P<0.05).
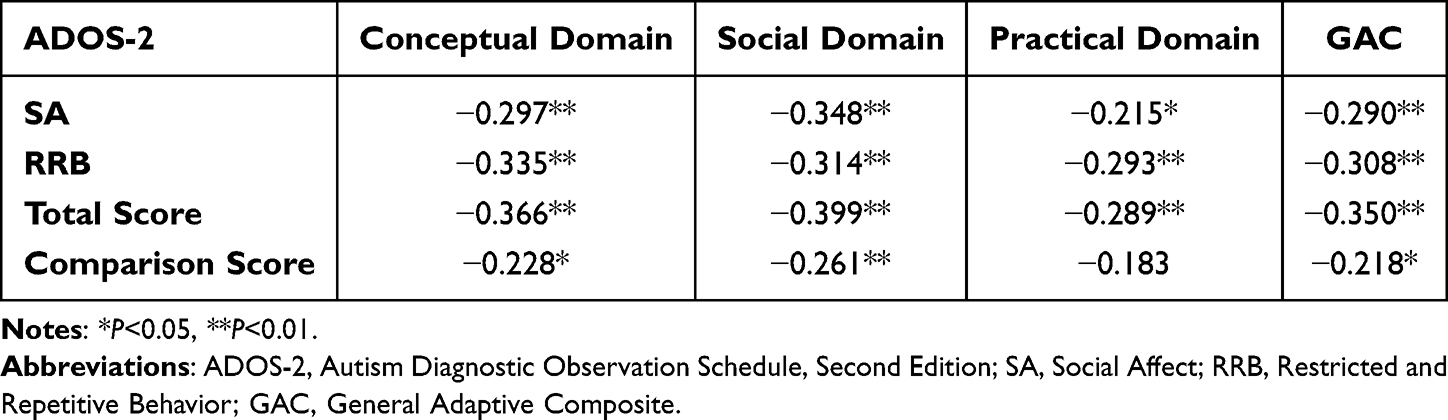 |
Table 4 Associations Between Autistic Severity and Adaptive Functioning in Children with Autism Spectrum Disorder |
Associations Between Intelligence, ASD Severity and Cognitive-Adaptive Functioning Gaps in Children with ASD
Table 5 demonstrated associations between IQ and cognitive-adaptive functioning gaps in children with ASD. VCI, PRI, WMI and PSI of WISC-IV were positively correlated with FSIQ-Conceptual skills, FSIQ-Social skills, FSIQ-Practical skills and FSIQ-GAC gaps (P<0.01). Besides, FSIQ itself was positively associated with FSIQ-GAC gaps (P<0.01). These outcomes reflected that cognitive-adaptive functioning gaps gradually increased with the elevation of IQ.
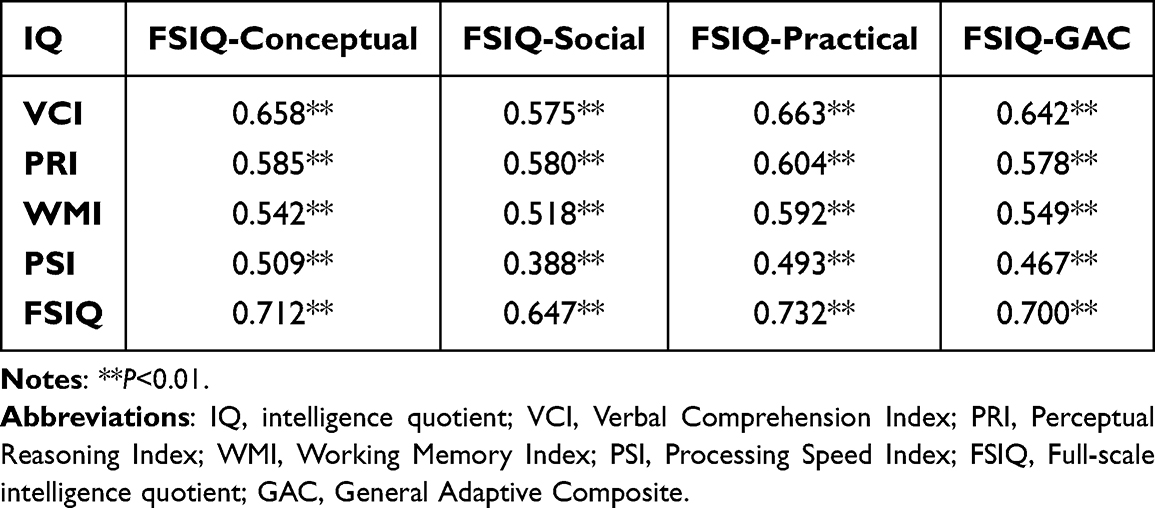 |
Table 5 Associations Between IQ and Cognitive-Adaptive Functioning Gaps in Children with Autism Spectrum Disorder |
Table 6 showed associations between ADOS-2 scores and cognitive-adaptive functioning gaps in children with ASD. SA of ADOS-2 was inversely correlated with FSIQ-Conceptual skills and FSIQ-Practical skills gaps (P<0.05). Total scores of ADOS-2 were inversely correlated with FSIQ-Conceptual skills, FSIQ-Practical skills and FSIQ-GAC gaps (P<0.05). These results indicated that cognitive-adaptive functioning gaps gradually narrowed with the exacerbation of autistic severity.
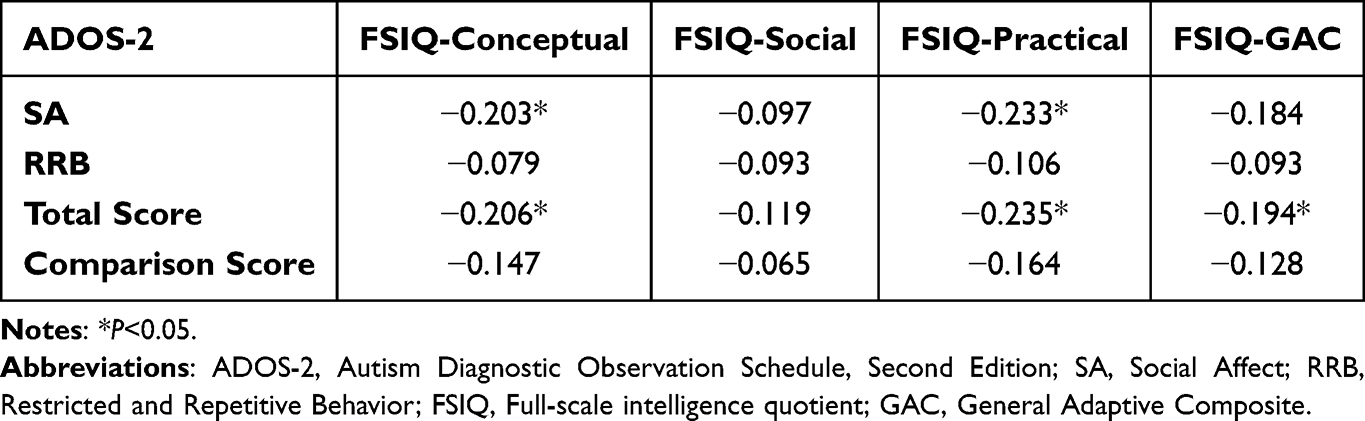 |
Table 6 Associations Between ADOS-2 Scores and Cognitive-Adaptive Functioning Gaps in Children with Autism Spectrum Disorder |
Effects of Demographic Characteristics, Intelligence, ASD Severity and Behavioral Factors on Adaptive Functioning in Children with ASD
Table 7 presented effects of gender, parental education, intelligence, ASD severity and behavioral factors on overall adaptive functioning (GAC) in children with ASD. Demographic characteristics including gender, age, paternal education and maternal education did not have significant associations with GAC in step 1, step 2, step 3 and the total model (all P>0.05). FSIQ was an important contributor to overall adaptive functioning in step 2 (β= 0.38, P<0.001), step 3 (β= 0.25, P=0.014) and the total model (β= 0.25, P=0.015), which indicated that FSIQ was positively correlated with GAC. There were significant inverse associations between RRB and GAC in step 3 (β= −0.27, P=0.017) and the total model (β= −0.28, P=0.014). However, behavioral factors including ADHD complication and EIBI did not have significant correlations with GAC in the total model (all P>0.05).
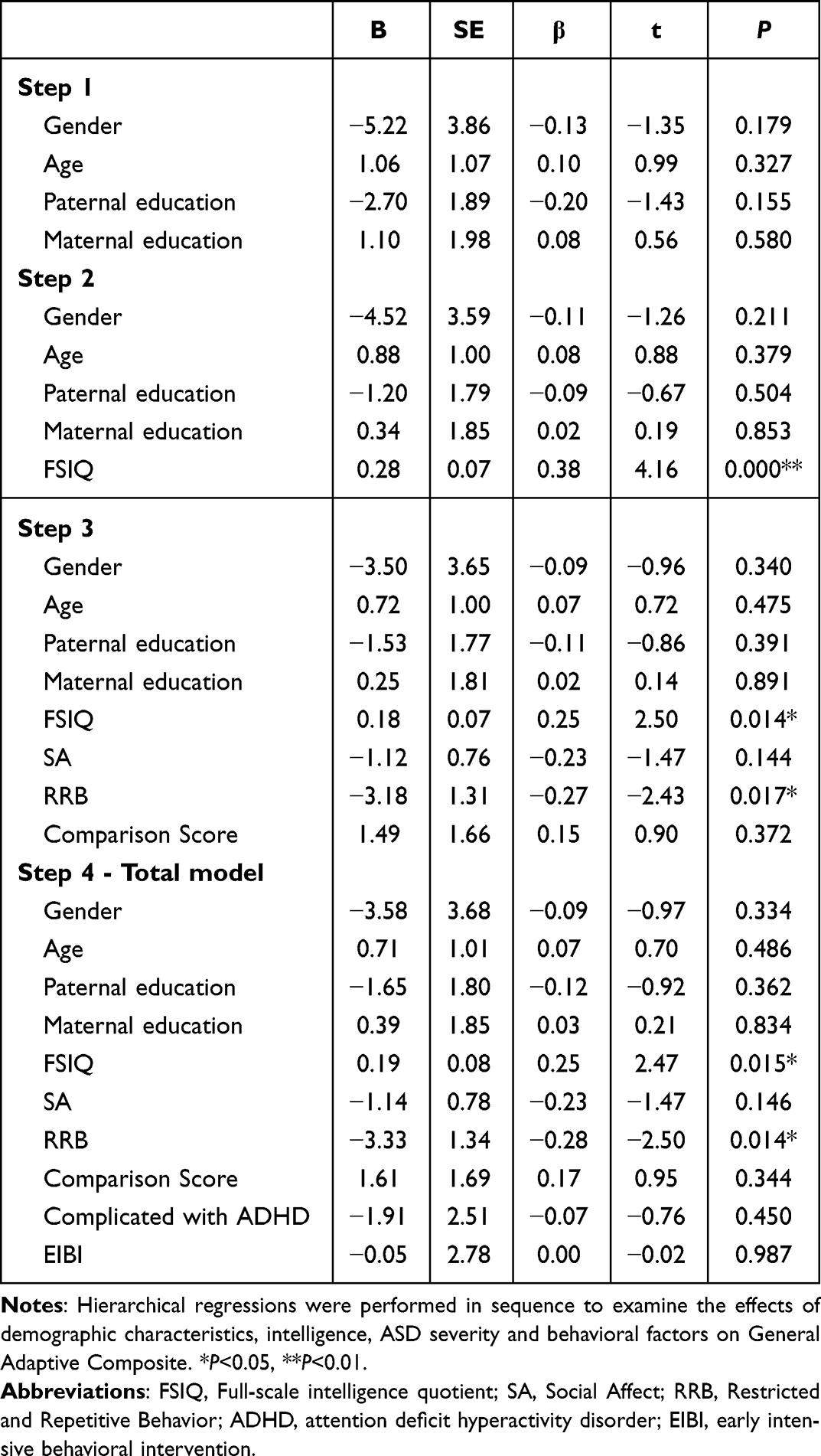 |
Table 7 Effects of Demographic Characteristics, Intelligence, Autistic Severity and Behavioral Factors on Overall Adaptive Functioning in Children with Autism Spectrum Disorder |
Additionally, we explored the effects of demographic characteristics, intelligence, ASD severity and behavioral factors on Conceptual, Social and Practical domains. In the total model, FSIQ had a positive correlation with Conceptual domain (β= 0.34, P=0.001), whereas RRB had a negative correlation with Conceptual domain (β= −0.26, P=0.016). There was a positive correlation between FSIQ and Social domain (β= 0.23, P=0.024), but a negative correlation between RRB and Social domain (β= −0.23, P=0.047). Moreover, there was an inverse correlation between RRB and Practical domain (β= −0.35, P=0.004).
Discussion
Adaptive functioning of ASD subjects was affected by multiple factors in previous studies. Our study discovered that intelligence levels and severity of autistic symptoms were important contributors to adaptive functioning of children with ASD, whether ASD subjects had comorbid intellectual disabilities or not. There existed significant positive correlations between intelligence levels (including verbal comprehension, perceptual reasoning, working memory, processing speed and FSIQ) and adaptive functioning (including Conceptual domain, Social domain, Practical domain and GAC). Whereas remarkable negative correlations were found between autistic symptoms (including social deficits and repetitive stereotyped behaviors) and adaptive functioning. These discoveries were consistent with the findings of previous studies and provided convincing evidence supporting them.4,11–15 It was worth noting that past studies mostly applied Vineland Adaptive Behavior Scales (VABS) as the assessment tool of adaptive functioning.12–15 We drew the same conclusions using ABAS as the assessment measure. As we all know, both VABS and ABAS were extensively used scales for evaluating adaptive behaviors of children with ASD. They had different emphases and presented strengths and weaknesses of children with ASD in different domains.6 Our study further confirmed the strong relationships between intelligence, autistic symptoms and adaptive functioning of school-aged individuals with ASD.
Additionally, we found cognitive-adaptive functioning gaps were influenced by intelligence levels and autistic severity. In our study, greater discrepancies between IQ and adaptive behaviors were positively correlated with cognitive abilities, but inversely correlated with ASD severity, especially social interaction impairments. Previous research found the discrepancies existed both in ASD males and females, starting from toddlerhood and persisting into young adulthood.8–10 Our results revealed the gaps between IQ and adaptive functioning in children with ASD, which were in accord with previous studies. We further explored the underlying influencing factors of cognitive-adaptive functioning gaps, which was a noteworthy highlight of our study. Few previous studies have explored this issue in Chinese population. Our study found the discrepancies between cognitive abilities and adaptive functioning gradually enlarged with the increase of IQ, implying children with ASD had difficulties in transforming their intelligence into adaptive functioning. Social deficits and repetitive stereotyped behaviors hindered the development of daily living skills, both in autistic children with or without intellectual disabilities. For those high-functioning autistic individuals, the development of adaptive functioning was seriously affected by emotions. It has been revealed that greater gaps between intelligence and adaptive behaviors in autism without intellectual disabilities persisted to young adulthood was linked to psychiatric comorbidities, including anxiety and depression.10 In a recent study, reduced executive functions were discovered to be consistently correlated with greater cognitive-adaptive functioning gaps in socialization domains for both preschool and school-aged autistic children without cognitive delay.27 Moreover, cognitive-adaptive functioning gaps gradually narrowed with the exacerbation of social-communication symptoms in our study, suggesting children with severe autistic symptoms always demonstrated weak cognitive abilities and adaptive functioning. Severe social deficits and repetitive stereotyped behaviors also hampered the development of intellectual abilities to some extent. In the research of Tillmann J et al28 higher IQ scores and more severe social-communication symptoms were associated with greater IQ-adaptive functioning gaps. By contrast, sensory ASD symptoms, ADHD symptoms and psychiatric comorbidities including anxiety and depression were not associated with IQ-adaptive functioning discrepancies. These findings suggested further studies concerning the underlying influencing factors of cognitive-adaptive functioning gaps were warranted to better elucidate this issue in the future.
There were still some controversial results in our research. Evidence from previous studies revealed that EIBI could effectively promote the development of adaptive behavior skills for ASD individuals.16–18 However, our results did not provide sufficient evidence supporting the viewpoint. Lack of long-term, sustained and effective interventions was hypothesized to be the predominant reason leading to the inconsistent conclusion. Unfortunately, most of our subjects received intermittent professional interventions for less than two years, which was frequently restricted to limited parental awareness of ASD and heavy financial burdens of ASD families.29,30 Furthermore, it has been reported that ADHD comorbidity aggravated the impairments in adaptive functioning of ASD individuals.1,19,20 Our study tested the executive function deficits of subjects with ASD combined with ADHD, discovering these subjects presented weaker performance in working memory and processing speed than those without ADHD. However, the differences did not reach statistical significance. As well, we did not find significant differences of adaptive functioning in ASD accompanied by ADHD or not. It has been debated in literature that the attentional impairment reported among autistic children might be a distinct characteristic of ASD—joint attention deficit, rather than an ADHD attention deficit.31,32 Attention deficits in ASD were prone to be the “not listening” and “difficulty shifting focus” type than the “short attention span” and “excessive distractibility” type.31 There was a possibility that some children diagnosed with ASD and ADHD did not really have ADHD. Whether ADHD coexistence aggravated the impairments of adaptive functioning in ASD still deserves further study and discussion. Additionally, gender differences of adaptive functioning were investigated in our study. There were no significant differences in adaptive functioning except for community use between male and female ASD subjects in the present study. Results of hierarchical regressions showed gender was not a predominant contributor to overall adaptive functioning in ASD. Whereas White EI et al22 reported that females with ASD performed relatively worse executive functions and daily living skills than their male counterparts. Mahendiran T et al21 found female ASD individuals obtained lower scores compared to males in communication, leisure and social skill areas at older ages, despite females performing better at younger ages. It was speculated that gender differences of adaptive functioning in ASD individuals might be affected by complicated confounding factors, such as age and early developmental trajectories.
There existed some limitations that could not be ignored in our study. Firstly, our sample size was insufficient. Given the huge population of China, a multicenter study with larger sample size could be more representative. Secondly, the amount of female ASD subjects was limited in our study. Although the prevalence of ASD was significantly higher in boys than in girls, we still need a sex-matched study to better analyse other potential affecting factors. Thirdly, ABAS-II questionnaire was self-reported in our study. We could not rule out the possibility of reporting bias. Our findings were vulnerable to over-evaluation of adaptive behavior scores, as the caregivers of ASD subjects were more likely to report what they could perform, rather than what they did perform independently without support. Fourthly, emotion regulation was a crucial mediating factor which always affected adaptive functioning of children with ASD. It has been discovered that psychiatric complications such as depression and anxiety were negatively correlated with adaptive behavior skills in young adulthood with ASD.10 Adding emotion-related scales into our study would be helpful for further investigating multiple influencing factors of adaptive functioning and cognitive-adaptive functioning gaps. Finally, considering the potential interactions among influencing factors of adaptive functioning, Structural Equation Modeling would be a better model for statistical analysis for it could more effectively illustrate mediating and moderating effects.
Conclusion
Intelligence levels and autistic severity were important contributors to adaptive functioning of school-aged children with ASD. IQ and ASD symptoms were also crucial factors affecting the cognitive-adaptive functioning gaps in ASD. Adaptive functioning was a determinant of long-term outcomes for autistic children. Exploring the influencing factors of adaptive functioning and cognitive-adaptive functioning gaps was of great importance to improve quality of life for individuals with ASD.
Data Sharing Statement
The raw data generated and analyzed in this study are not publicly available due to the appropriate protection of the personal protection of children and adolescents but are available from the corresponding authors on a reasonable request.
Ethics Approval and Informed Consent
Our research was conducted in accordance with the Declaration of Helsinki. Our study was approved by Clinical Research Ethics Committee of Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health (No. 2022-IRB-099). Informed consents were acquired from parents or caregivers of every participant.
Acknowledgments
We are grateful for all the researchers from Department of Developmental Behavioral Pediatrics, Children’s Hospital, Zhejiang University School of Medicine in the data acquisition. We also thankful to all the subjects for their participation in our study. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-5771996/v1.
Author Contributions
All the authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Natural Science Foundation of Zhejiang Province (LGF20H090015).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chandler S, Carter Leno V, White P. et al. Pathways to adaptive functioning in autism from early childhood to adolescence. Autism Res. 2022;15(10):1883–1893. doi:10.1002/aur.2785
2. Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. 2020;9(Suppl 1):S55–S65. doi:10.21037/tp.2019.09.09
3. Jiang X, Chen X, Su J, et al. Prevalence of autism spectrum disorder in mainland China over the past 6 years: a systematic review and meta-analysis. BMC Psychiatry. 2024;24(1):404. doi:10.1186/s12888-024-05729-9
4. Jin WY, Wu LL, Hu LF, et al. Intelligence profiles and adaptive behaviors of high-functioning autism spectrum disorder and developmental speech and language disorders. Front Pediatr. 2023;10:972643. doi:10.3389/fped.2022.972643
5. Lopata C, Smith RA, Volker MA, Thomeer ML, Lee GK, McDonald CA. Comparison of Adaptive Behavior Measures for Children with HFASDs. Autism Res Treat. 2013;2013:415989. doi:10.1155/2013/415989
6. Tamm L, Day HA, Duncan A. Comparison of Adaptive Functioning Measures in Adolescents with Autism Spectrum Disorder Without Intellectual Disability. J Autism Dev Disord. 2022;52(3):1247–1256. doi:10.1007/s10803-021-05013-9
7. Wang SH, Zhou Q, Chen KY, et al. Cognitive-adaptive Functioning Gap and Mediating Factors that Impact Adaptive Functioning in Chinese Preschool-aged Children with Autism Spectrum Disorder. J Autism Dev Disord. 2024;54(8):3107–3121. doi:10.1007/s10803-023-06029-z
8. McQuaid GA, Pelphrey KA, Bookheimer SY, et al. The gap between IQ and adaptive functioning in autism spectrum disorder: disentangling diagnostic and sex differences. Autism. 2021;25(6):1565–1579. doi:10.1177/1362361321995620
9. Bradshaw J, Gillespie S, Klaiman C, Klin A, Saulnier C. Early emergence of discrepancy in adaptive behavior and cognitive skills in toddlers with autism spectrum disorder. Autism. 2019;23(6):1485–1496. doi:10.1177/1362361318815662
10. Kraper CK, Kenworthy L, Popal H, Martin A, Wallace GL. The Gap Between Adaptive Behavior and Intelligence in Autism Persists into Young Adulthood and is Linked to Psychiatric Co-morbidities. J Autism Dev Disord. 2017;47(10):3007–3017. doi:10.1007/s10803-017-3213-2
11. Kenworthy L, Case L, Harms MB, Martin A, Wallace GL. Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. J Autism Dev Disord. 2010;40(4):416–423. doi:10.1007/s10803-009-0911-4
12. Szatmari P, Georgiades S, Duku E, et al. Developmental trajectories of symptom severity and adaptive functioning in an inception cohort of preschool children with autism spectrum disorder. JAMA Psychiatry. 2015;72(3):276–283. doi:10.1001/jamapsychiatry.2014.2463
13. Pathak M, Bennett A, Shui AM. Correlates of adaptive behavior profiles in a large cohort of children with autism: the autism speaks Autism Treatment Network registry data. Autism. 2019;23(1):87–99. doi:10.1177/1362361317733113
14. Lee V, Duku E, Zwaigenbaum L, et al. Temperament influences the relationship between symptom severity and adaptive functioning in children with autism spectrum disorder. Autism. 2020;24(8):2057–2070. doi:10.1177/1362361320933048
15. Rosa M, Puig O, Lázaro L, et al. Broad Cognitive Profile in Children and Adolescents with HF-ASD and in Their Siblings: widespread Underperformance and its Clinical and Adaptive Correlates. J Autism Dev Disord. 2017;47(7):2153–2162. doi:10.1007/s10803-017-3137-x
16. Reichow B, Hume K, Barton EE, Boyd BA. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Cochrane Database Syst Rev. 2018;5(5):CD009260. doi:10.1002/14651858.CD009260.pub3
17. Daniolou S, Pandis N, Znoj H. The Efficacy of Early Interventions for Children with Autism Spectrum Disorders: a Systematic Review and Meta-Analysis. J Clin Med. 2022;11(17):5100. doi:10.3390/jcm11175100
18. MacDonald R, Parry-Cruwys D, Dupere S, Ahearn W. Assessing progress and outcome of early intensive behavioral intervention for toddlers with autism. Res Dev Disabil. 2014;35(12):3632–3644. doi:10.1016/j.ridd.2014.08.036
19. Liu Y, Wang L, Xie S, et al. Attention Deficit/Hyperactivity Disorder Symptoms Impair Adaptive and Social Function in Children With Autism Spectrum Disorder. Front Psychiatry. 2021;12:654485. doi:10.3389/fpsyt.2021.654485
20. Yerys BE, Bertollo JR, Pandey J, Guy L, Schultz RT. Attention-Deficit/Hyperactivity Disorder Symptoms Are Associated With Lower Adaptive Behavior Skills in Children With Autism. J Am Acad Child Adolesc Psychiatry. 2019;58(5):525–533.e3. doi:10.1016/j.jaac.2018.08.017
21. Mahendiran T, Dupuis A, Crosbie J, et al. Sex Differences in Social Adaptive Function in Autism Spectrum Disorder and Attention-Deficit Hyperactivity Disorder. Front Psychiatry. 2019;10:607. doi:10.3389/fpsyt.2019.00607
22. White EI, Wallace GL, Bascom J, et al. Sex differences in parent-reported executive functioning and adaptive behavior in children and young adults with autism spectrum disorder. Autism Res. 2017;10(10):1653–1662. doi:10.1002/aur.1811
23. Hodge MA, Boulton KA, Sutherland R, et al. Predictors of adaptive functioning in preschool aged children with autism spectrum disorder. Autism Res. 2021;14(7):1444–1455. doi:10.1002/aur.2501
24. Harrison PL, Oakland T. Adaptive Behavior Assessment System.
25. Lord C, Rutter M, DiLavore PC, et al. Autism Diagnostic Observation Schedule Manual-2. Los Angeles, CA: Western Psychological Services; 2012.
26. Wechsler D. The Wechsler Intelligence Scale for Children-Fourth Edition. San Antonio, TX: The Psychological Corporation; 2003.
27. Braverman Y, Edmunds SR, Hastedt I, Faja S. Mind the Gap: executive Function Is Associated with the Discrepancy Between Cognitive and Adaptive Functioning in Autistic Children Without Cognitive Delay. J Autism Dev Disord. 2024. doi:10.1007/s10803-024-06354-x
28. Tillmann J, San José Cáceres A, Chatham CH, et al. Investigating the factors underlying adaptive functioning in autism in the EU-AIMS Longitudinal European Autism Project. Autism Res. 2019;12(4):645–657. doi:10.1002/aur.2081
29. Zhao Y, Lu F, Wang X, et al. The economic burden of autism spectrum disorder with and without intellectual disability in China: a nationwide cost-of-illness study. Asian J Psychiatr. 2024;92:103877. doi:10.1016/j.ajp.2023.103877
30. Singh JKA, Ling WH, Sivanesom RS, Huay CCS, Lan ACS. Age at autism spectrum disorder diagnosis and its association with child and family characteristics in a tertiary care hospital in Malaysia. Autism Res. 2024;17(3):637–649. doi:10.1002/aur.3106
31. hours C, Recasens C, Baleyte JM. ASD and ADHD Comorbidity: what Are We Talking About? Front Psychiatry. 2022;13(13):837424. doi:10.3389/fpsyt.2022.837424
32. Gargaro BA, Rinehart NJ, Bradshaw JL, Tonge BJ, Sheppard DM. Autism and ADHD: how far have we come in the comorbidity debate? Neurosci Biobehav Rev. 2011;35(5):1081–1088. doi:10.1016/j.neubiorev.2010.11.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.