")
Back to Journals » Journal of Pain Research » Volume 18
Efficacy and Central Mechanism of Acupuncture Treatment for Subacute Nonspecific Low Back Pain: A Clinical Neuroimaging Protocol
Authors Ren J, Gao Z , Chang BY, Cui MJ , Wang HJ
Received 20 March 2025
Accepted for publication 17 June 2025
Published 30 June 2025 Volume 2025:18 Pages 3299—3308
DOI https://doi.org/10.2147/JPR.S529456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Jia Ren,* Zhen Gao,* Bo-Ya Chang, Meng-Jie Cui, Hai-Jun Wang
Second Clinical Medical College, Shanxi University of Chinese Medicine, Jinzhong, Shanxi, 030619, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hai-Jun Wang, Second Clinical Medical College, Shanxi University of Chinese Medicine, Daxue Street, No. 121, Jinzhong, Shanxi, 030619, People’s Republic of China, Email [email protected]
Purpose: The chronification of pain is a multifaceted process, and low back pain (LBP), being one of the most prevalent health concerns globally, is particularly prone to developing into a chronic condition. Acupuncture is a common method of treating LBP in Chinese medicine, which is safe and effective. However, its mechanism of action is unclear, and more data are needed to support its application in LBP.
Patients and Methods: This study is a randomized controlled neuroimaging trial, involving 120 subacute LBP patients assigned to the true acupuncture group, the sham acupuncture group, or the waiting list control group. The whole study period includes a 4-week treatment period and an 8-week follow-up period. The visual analog scale, Oswestry Disability Index, range of motion, and pressure pain threshold will be used to evaluate clinical efficacy, the short-form 36-item health survey and Pittsburgh Sleep Quality Index will be used to evaluate quality of life, the self-rating anxiety scale and self-rating depression scale will be used for assessing emotional state. The magnetic resonance imaging (MRI) scans will be performed to detect cerebral activity changes between the three groups of patients before and after treatment, as well as during follow-up periods. The clinical data and MRI data will be analyzed, respectively. Correlation analysis will be used to explore the correlation between neuroimaging data and clinical indicators.
Conclusion: This study will provide rigorous evidence for the use of acupuncture to prevent the chronic progression of low back pain.
Trial Registration: International Traditional Medicine Clinical Trial Registry ITMCTR2024000581, Registered on 17 October 2024.
Keywords: acupuncture, neuroimaging, low back pain, randomized control trial
Introduction
Pain is a complex sensation encompassing sensory perception, emotional responses, and cognitive appraisal, typically linked to tissue injury or potential harm, and characterized by an uncomfortable or distressing feeling.1 Acute pain can indicate the presence of a dangerous or life-threatening event, aiding the body in escaping harmful stimuli and serving as a normal protective mechanism in humans. However, pain that persists or recurs for more than three months is classified as chronic pain, which has a profound impact on an individual’s quality of life, socioeconomy, and healthcare systems, necessitating safe and effective pain management. Among these, low back pain, a common musculoskeletal condition in clinical practice, has an average prevalence of about 30%,2 and has become the fifth most common reason for medical consultations.3 According to the latest estimates of healthcare expenditures in the United States, the annual treatment costs for neck and back pain, including low back pain, have been steadily increasing and have reached a staggering 13.45 billion dollars.4 Research shows that a significant 7.6% of adults have suffered from acute low back pain at least once in the past year.5 Although some acute episodes resolve on their own, for many individuals, the discomfort lingers beyond the initial trauma and can stretch over years.6 Additionally, the negative feelings triggered by pain can intensify the sensation of it, leading to a compounded struggle for patients both physically and mentally.7
Acupuncture, a widely practiced complementary and alternative therapy, is commonly used for pain management. Compared to medication, it not only provides faster relief and longer-lasting analgesic effects but also effectively reduces the recurrence rate of diseases and shortens the duration of illness.8–10 The American College of Physicians’ 2017 guidelines on non-invasive treatments for acute, subacute, and chronic low back pain gave a strong recommendation for acupuncture therapy. Furthermore, a study in the BMJ, “Acupuncture Disease Atlas Based on Clinical Evidence”, supported acupuncture for treating eight conditions, including low back pain, reinforcing its clinical benefits.11
The central nervous system’s integration is vital to the effectiveness of acupuncture therapy. Studies indicate that the shift from acute to chronic pain can be tracked through alterations in brain architecture and functional dynamics.12 Individuals suffering from low back pain and similar conditions show disrupted brain structures and functions.13 Acupuncture treatment has the potential to mitigate these disruptions, thereby reducing the severity of low back pain and related symptoms.14 Although some studies have demonstrated the efficacy of acupuncture in treating acute pain disorders,15,16 there is currently a lack of rigorously designed randomized controlled trials on acupuncture for acute pain. Moreover, existing research predominantly focuses on the mechanisms of acupuncture in treating chronic low back pain and acute pain conditions.17,18 In view of this, this study has carefully designed three different groups to explore the therapeutic effect of acupuncture in intervening subacute pain and its underlying central mechanisms in preventing the chronification of pain. Hence, the objective of this study is to utilize functional magnetic resonance imaging (fMRI) to examine the alterations in brain activity following acupuncture treatment, and to analyze the possible associations between clinical symptom alleviation and these brain activity changes. The goal is to delve into the underlying central mechanisms of acupuncture therapy for subacute non-specific low back pain.
Materials and Methods
Design and Setting
This randomized controlled neuroimaging trial adheres to the Standard Protocol Items: Recommendations for Intervention Trials (SPIRIT) guidelines (Supplementary File 1). Additionally, it follows the principles outlined in the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).19,20
A total of 120 patients with subacute nonspecific low back pain will be randomly assigned in a 1:1:1 ratio to the true acupuncture, sham acupuncture, or waiting list control group. The study protocol is detailed in Figure 1 and Table 1.
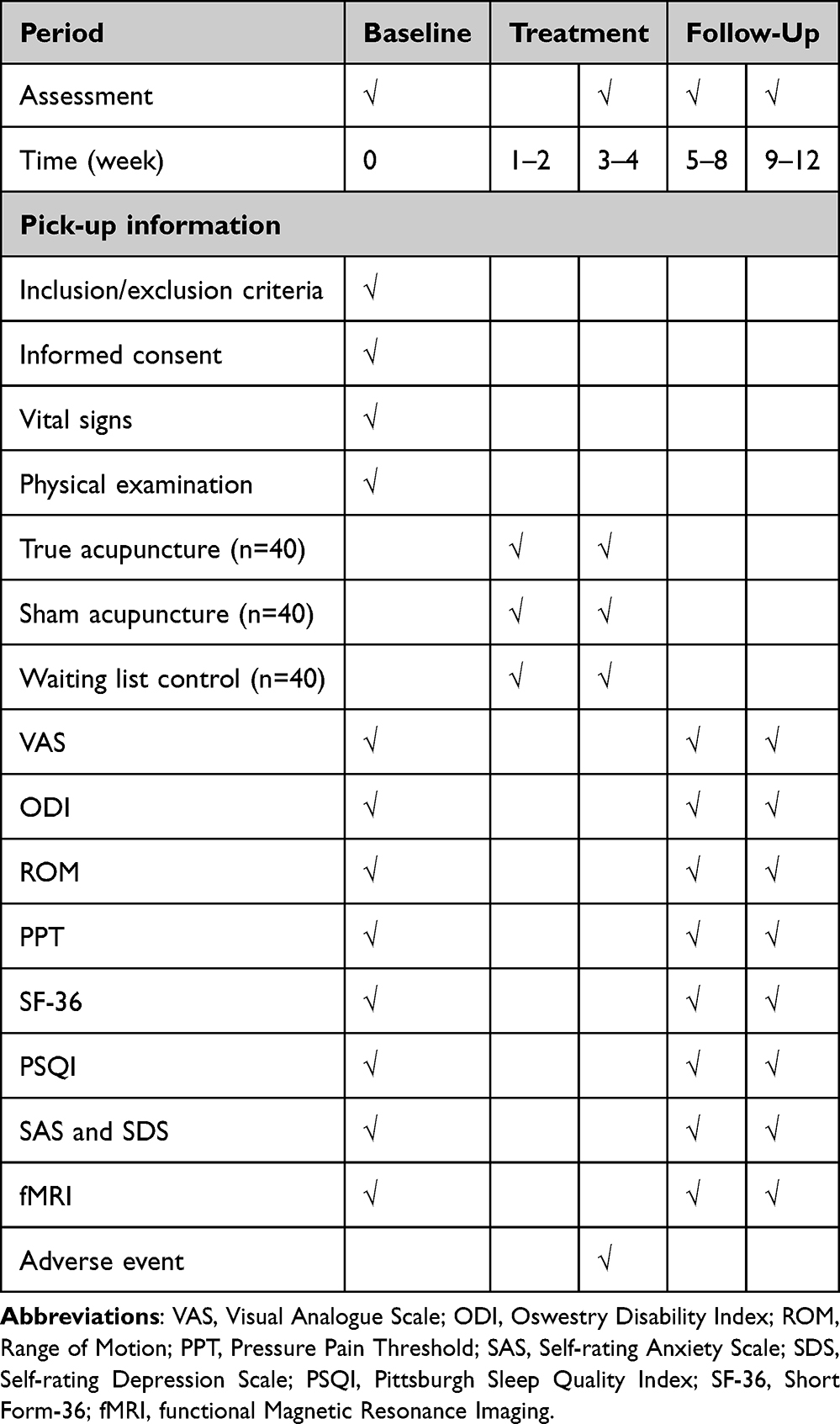 |
Table 1 Study Schedule for Data Collection |
 |
Figure 1 Flowchart of the procedure through the trial. |
Sample Size
Since neuroimaging mechanism studies involving humans differ from clinical trials, traditional clinical trial sample size calculations are not applicable.21–25 Some researchers suggest that 20 participants per group can achieve 80% statistical power.22 To account for potential data unavailability due to various factors, this trial will include 40 patients per group for MRI scans.
Participants
Recruitment Strategy
Patients will be recruited from the outpatient clinic of Shanxi Acupuncture Hospital, as well as from the community and Shanxi University of Traditional Chinese Medicine campus. Eligible participants will be required to provide informed consent.
Inclusion Criteria
Participants meeting all of the following criteria will be included: 1) Diagnosis of nonspecific low back pain based on the 2022 Chinese Clinical Practice Guidelines for Nonspecific Low Back Pain; 2) Illness duration between 4 and 12 weeks; 3) Visual analogue scale (VAS) score above 4 out of 10; 4) Age between 18 and 55 years with right-hand dominance; 5) Willingness to provide informed consent.
Exclusion Criteria
Participants will be excluded if they meet any of the following criteria: 1) Pregnancy or lactation; 2) Presence of severe primary illness or psychiatric/neurological disorders; 3) Contraindications to MRI, including pacemakers or claustrophobia; 4) Participation in other clinical trials.
Randomization
Randomization will be conducted in two steps: 1) An independent, blinded statistician will generate a random allocation sequence using SPSS 26.0 (IBM, Chicago, IL, USA), assigning 120 patients equally to the true acupuncture, sham acupuncture, and waiting list control groups (1:1:1 ratio); 2) Allocation concealment will be ensured through sequentially numbered, opaque, sealed envelopes.
Blinding
Due to the inherent nature of acupuncture, operator blinding is not feasible. However, patients, outcome assessors, and statistical analysts will remain blinded to group assignments and treatments.
Interventions
Acupuncturists who have held a practicing qualification for at least two years and have successfully passed our clinical training assessment will provide the interventions.
True Acupuncture Group
Patients in the true acupuncture group will receive needle insertion at both sides of Weizhong (BL 40), Dachangshu (BL 25), Shenshu (BL 23), and Yaoyangguan (GV3) points.
Sham Acupuncture Group
To enhance the rigor of our study, we opted to use a previously well-validated placebo that does not produce specific physiological effects.26,27 Patients in the sham acupuncture group will receive needle insertion at pre-verified non-acupoint locations (Figure 2). The sham acupuncture locations will be as follows:
 |
Figure 2 Locations of acupoint. |
Sham Point 1: Midpoint between the armpit and the elbow.
Sham Point 2: Midpoint between the brachioradialis and the shoulder peak.
Sham Point 3: 1 cun beside the radial side of Neiguan (PC6).
Sham Point 4: 1 cun beside the radial side of Shenmen (HT7).
Waiting List Control Group
Throughout the observation period, no acupuncture treatment will be provided. Afterward, participants will receive 12 treatments identical to those in the true acupuncture group.
The acupuncture procedure will use disposable sterile needles (0.30 × 75 mm, Huatuo Medical Instrument Co., Ltd., China). In the true acupuncture group, needle depth and direction will be adjusted based on the treatment site, with Deqi sensation required. In contrast, the sham acupuncture group will undergo shallow insertion without requiring Deqi. Needles will be retained for 30 minutes in both groups.
Patients will receive acupuncture three times per week, totaling 12 sessions over four weeks.
Concomitant Medications
Patients will be instructed to avoid analgesic medication during the study. If symptoms worsen, ibuprofen (300 mg/capsule) may be used as an adjunct treatment and must be recorded in the case report form.
Outcomes
Primary Outcome
The change in VAS score before and after treatment will be used as the primary outcome.
Secondary Outcome
All patients will undergo a total of 4 clinical efficacy evaluations during the baseline period, after treatment completion, and during the follow-up period.
- The Oswestry Disability Index (ODI) will be utilized to assess the level of low back disability related to activities of daily living.
- The range of motion (ROM) will be measured using a digital protractor (Aicai Instruments Co., Ltd., China, Specification: 0–200 mm, Measurement Range: 0–360°) to assess the movement of the lower back.
- Short-form 36-item health survey (SF-36) will be used to measure quality of life in 8 dimensions, including physical health and mental health.
- The pain pressure threshold (PPT) will be used to measure deep muscle tissue sensitivity.
- The self-rating anxiety scale (SAS) and self-rating depression scale (SDS) will be used to measure the severity of anxiety and depression.
- The Pittsburgh Sleep Quality Index (PSQI) will be used to assess sleep status.
MRI Data Acquisition
Patients will undergo resting-state fMRI using a 3.0T MR scanner (Siemens 3T Tim Trio, Erlangen, Germany) at Shanxi Provincial People’s Hospital. The scanning protocol includes a localizer, three-dimensional T1-weighted imaging (3D-T1WI), and blood oxygenation level-dependent (BOLD) fMRI.28,29 The 3D-T1WI parameters are: repetition time (TR) = 1900 ms, echo time (TE) = 2.26 ms, data matrix = 128 × 128, and field of view (FOV) = 256×256 mm². BOLD-fMRI parameters include 31 contiguous slices (5 mm thickness), TR = 2000 ms, TE = 30 ms, FOV = 240×240 mm², matrix = 128 × 128, flip angle = 90°, and a total of 240 volumes.
Data Analysis
Clinical Data Analysis
Statistical analysis will be performed using SPSS 26.0 (IBM, Chicago, IL, USA) software. Quantitative data will be described by mean ± standard deviation, and qualitative data will be presented by frequency and percentage. Generalized Estimating Equations (GEE) will be applied to analyze the data from the three groups at four time points: baseline, post-treatment, and follow-up. A model will be constructed with time points and group as independent variables, including their interaction terms, to investigate the impact of time points and group on the outcome variable. Additionally, Bonferroni correction will be applied for multiple comparisons to identify which specific time points exhibit statistically significant differences between groups. All statistical analyses will be conducted at a significance level of P<0.05.
BOLD-fMRI Data Analysis
The fMRI data preprocessing (format conversion, slice timing correction, head motion correction, etc.) will be performed using the DPARSF software (http://www.fil.ion.ucl.ac.uk/spm/) based on MATLAB 2022b.28 During the preprocessing of fMRI data, the following steps are carried out: First, the original DICOM format files are converted into NIFITI format files that can be used for analysis using the MRICroGL software. Considering that the magnetic field may be unstable and the subjects may be affected by their own mood at the beginning of the MRI scan, which can lead to unstable signal acquisition, the first 10 time points of the scan are removed. Given that the data is acquired through interleaved scanning, resulting in time differences between the acquisition of different slices, time-layer correction is performed. It assumes that the data is collected at the same time point and uses the image of the middle time point as the reference layer. Since head motion can cause voxel misalignment, in order to align the images at different time points and reduce the impact of head motion on the data, head motion correction is applied. Data with translations greater than 2.0 mm in the X, Y, and Z axes and rotations greater than 2° around these three axes are excluded. Additionally, considering the differences in head size and shape among subjects, in order to align the subjects’ images and ensure that the anatomical structures corresponding to the same voxel are consistent across different subjects, T1 registration (a two-step registration method) is employed. First, the high-resolution T1 structural images are registered with the standard template, and then these registration parameters are applied to the functional images. The main analysis methods include 1) the amplitude of low-frequency fluctuation (ALFF) and regional homogeneity (ReHo), reflecting local brain functional activity, and 2) seed-based functional connectivity analysis, using local differential brain regions as seed points to reflect integration of brain functions. In statistical analysis, to control the false-positive issues arising from multiple comparisons, a significance threshold of p-value less than 0.05 after Family-Wise Error Rate (FWE) correction will be adopted. Additionally, the False Discovery Rate (FDR) correction method may also be considered for auxiliary analysis according to the research requirements.
Furthermore, Pearson correlation analysis will be employed to examine linear relationships between neuroimaging metrics including ALFF, ReHo, and functional connectivity strength with clinical indicators.
Discussion
To our knowledge, this study represents the first randomized controlled trial aimed at exploring the clinical effectiveness of acupuncture for the treatment of subacute low back pain, as well as the underlying central mechanisms. The findings of this research are poised to shed light on how acupuncture inhibits the progression to chronic pain.
Reasonable Grouping is a Crucial Step in Validating the Therapeutic Effectiveness of Acupuncture
This study was structured around three distinct groups: the true acupuncture group, the sham acupuncture group, and the waiting list control group. The primary objective of contrasting the true acupuncture group with the sham acupuncture group was to eliminate the placebo effect that can be associated with acupuncture treatment. In the true acupuncture group, the selection of acupoints for needle insertion was based on their established efficacy through clinical practice. Moreover, the procedure emphasized the importance of achieving “De Qi”, a pivotal therapeutic response. Operators were required to manipulate the needles to a precise depth and angle to induce “De Qi”, thereby optimizing the therapeutic potential of acupuncture.30 On the other hand, the sham acupuncture group involved superficial needle insertion at locations known to be non-acupoints and devoid of therapeutic effects, with no attempt to trigger “De Qi”. This approach helps to delineate the actual therapeutic impact of acupuncture from the participants’ perceived effects, effectively mitigating the placebo influence of the treatment process. Furthermore, since acute low back pain has the potential to resolve spontaneously, the waiting list control group serves as a critical comparator. It aids in understanding the natural course of acute low back pain when left untreated, enabling a clearer comparison between the outcomes of acupuncture intervention and the likelihood of spontaneous recovery. This enhances our ability to discern acupuncture’s role in preventing the progression to chronic low back pain.
Exploring Central Mechanisms Offers a New Approach to Studying Acupuncture’s Prevention of Low Back Pain Chronicity
The brain is instrumental in the process of pain chronification, where abnormal neural activity and changes in neural plasticity contribute to the enhancement of abnormal pain perception, emotional disturbances, and cognitive impairments, ultimately leading to the perpetuation and exacerbation of pain. Prior neuroimaging studies have uncovered discrepancies in both the functional and structural aspects of the brain in individuals suffering from chronic pain. For instance, research has indicated that an increased functional connectivity between the nucleus accumbens and the prefrontal cortex is indicative of ongoing pain and serves as a precise predictor of the shift from subacute to chronic pain.31 Moreover, studies have proposed that structural anomalies within the corticolimbic system may pose a risk factor for the development of chronic pain.32 With the advancement of neuroimaging techniques, a non-invasive and visual approach to studying the human brain has emerged, making it a pivotal tool in investigating the effects of pain chronification on brain function—a topic that has garnered significant interest in the field of pain research.
Since the 20th century, researchers have increasingly focused on how the central nervous system responds to acupuncture. The mechanisms by which acupuncture, as a form of information regulation, alters neural circuits within the brain and triggers neural information responses to exert its therapeutic effects are still not fully understood. Building on this foundation, studies have revealed that following acupuncture treatment, the connectivity between the medial prefrontal cortex, insula, putamen, and caudate nucleus in individuals with low back pain is markedly correlated with their therapeutic outcomes.33 The brain regions implicated in the analgesic effects of acupuncture for low back pain are primarily situated within the pain matrix, default mode network, salience network, and the descending pain modulation system.14 Consequently, our hypothesis is that acupuncture can effectively mitigate subacute low back pain and intercept the progression to chronic pain through the modulation of brain activity.
Quality Control is the Guarantee of the Reliability and Repeatability of Study Results
Quality control is the key to influencing research results, and strict quality control plays an essential role in the guarantee of a high repeatability.34 Accordingly, we will conduct quality control from the following aspects: 1) participants inclusion: all participants included in this study will be diagnosed by an orthopedic specialist, and inclusion and exclusion criteria will be formulated to strictly limit the participants to a specific range and reduce the differences between them, so as to make objective conclusions about the observed factors; 2) trial design: randomized control design is adopted in this study, which can effectively avoid the generation of selective bias. Due to the particularity of acupuncture in this study, the efficacy evaluation and blind statistical analysis were carried out by a third party who did not know the grouping, so as to ensure the authenticity and reliability of the research results; 3) acupuncture treatment: Acupuncturists who have held a practicing qualification for at least two years and have successfully passed our clinical training assessment will provide the intervention. In addition, the operation of acupuncture is carried out in strict accordance with the standard operation specification of acupuncture; 4) neuroimage data collection: strictly limit the factors that affect the data collection results, minimize the influence of environment, equipment, operator and other factors, and use standard operating guidelines to regulate researchers’ operations to minimize individual differences. At the same time, participants will be required to maintain a normal lifestyle before data collection to ensure the stability of their physical and psychological state.
Limitations
The limitations of this trial include the short follow-up period and the inability to blind the acupuncturists due to the nature of acupuncture intervention. This study focuses on the transition from acute to chronic pain. However, since pain persisting beyond 12 weeks is clinically classified as chronic pain, we established an 8-week follow-up period for this investigation. The lack of practitioner blinding may potentially enhance placebo effects. To address this, we implemented enhanced standardized training for acupuncturists while maintaining blinding of patients, outcome assessors, and statisticians regarding group allocation and treatment details. These measures help mitigate potential biases to some extent and improve the reliability and scientific validity of our findings.
Abbreviations
fMRI, functional Magnetic Resonance Imaging; VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; SF-36, Short-Form 36-Item Health Survey; PPT, Pain pressure threshold; SAS, Self-rating Anxiety Scale; SDS, Self-rating Depression Scale; PSQI, Pittsburgh Sleep Quality Index; 3D-T1WI, three-dimensional T1-weighted imaging; TR, Repetition Time; TE, Echo Time; FOV, Field of View; GEE, Generalized Estimating Equations; ALFF, Amplitude of Low Frequency Fluctuation; ReHo, Regional Homogeneity.
Ethics Approval and Consent to Participate
This trial has been approved by the Institutional Review Board of Shanxi Acupuncture Hospital (approved number: 2024-013) and registered at International Traditional Medicine Clinical Trial Registry (registration number: ITMCTR2024000581, protocol version number: V1.0). This trial will be conducted in accordance with the Declaration of Helsinki. Only patients who have signed the informed consent form will be included. All methods were carried out in accordance with relevant guidelines and regulations.
Trial Status
The trial is currently in the recruitment phase, and the study is expected to end in December 2026.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by the Shanxi Province Basic Research Program (Grant No. 2024000581), and Scientific Research Fund for the Doctoral Scholars of Shanxi University of Chinese Medicine (Grant No. 2023BK17, 2023BKS12). Funders and sponsors have no role in the design of this study.
Disclosure
The authors declare that there are no competing interests.
References
1. Özüdoğru A, Canlı M, Ceylan İ, et al. Five times sit-to-stand test in people with non-specific chronic low back pain-a cross-sectional test-retest reliability study. Ir J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
2. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi:10.1002/art.34347
3. Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine. 1995;20(1):11–19. doi:10.1097/00007632-199501000-00003
4. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996-2016. JAMA. 2020;323(9):863–884. doi:10.1001/jama.2020.0734
5. Carey TS, Evans AT, Hadler NM, et al. Acute severe low back pain. A population-based study of prevalence and care-seeking. Spine. 1996;21(3):339–344. doi:10.1097/00007632-199602010-00018
6. Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89(2–3):127–134. doi:10.1016/S0304-3959(00)00355-9
7. He C, Chen H, Guo L, et al. Prevalence and factors associated with comorbid depressive symptoms among people with low back pain in China: a cross-sectional study. Front Psychiatry. 2022;13:922733. doi:10.3389/fpsyt.2022.922733
8. Grissa MH, Baccouche H, Boubaker H, et al. Acupuncture vs intravenous morphine in the management of acute pain in the ED. Am J Emergency Med. 2016;34(11):2112–2116. doi:10.1016/j.ajem.2016.07.028
9. Liu L, Zhang CS, Liu HL, et al. Acupuncture for menstruation-related migraine prophylaxis: a multicenter randomized controlled trial. Front Neurosci. 2022;16:992577. doi:10.3389/fnins.2022.992577
10. Wu LM, Liu Q, Yin XH, et al. Wrist-ankle acupuncture combined with pain nursing for the treatment of urinary calculi with acute pain. World J Clin Cases. 2023;11(18):4287–4294. doi:10.12998/wjcc.v11.i18.4287
11. Lu L, Zhang Y, Tang X, et al. Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ. 2022;376:e067475.
12. Apkarian VA, Hashmi JA, Baliki MN. Pain and the brain: specificity and plasticity of the brain in clinical chronic pain. Pain. 2011;152(3 Suppl):S49–s64. doi:10.1016/j.pain.2010.11.010
13. Lamichhane B, Jayasekera D, Jakes R, et al. Functional disruptions of the brain in low back pain: a potential imaging biomarker of functional disability. Front Neurol. 2021;12:669076. doi:10.3389/fneur.2021.669076
14. Wen Q, Ma P, Dong X, et al. Neuroimaging studies of acupuncture on low back pain: a systematic review. Front Neurosci. 2021;15:730322. doi:10.3389/fnins.2021.730322
15. Nielsen A, Olson J, Quesada M, et al. Acupuncture intervention for acute pain in the emergency department trial: a consensus process. Acupuncture Med. 2022;40(4):339–346. doi:10.1177/09645284221076507
16. Choi KH, Cho SJ, Kim M, et al. What is the analgesic range of acupuncture stimulus for treating acute pain? Front Human Neurosci. 2023;17:1281832. doi:10.3389/fnhum.2023.1281832
17. Mao X, He H, Ding J. Efficacy of laser acupuncture for treatment of chronic low back pain: a systematic review and meta-analysis. Pain Manage Nurs. 2024;25(5):529–537. doi:10.1016/j.pmn.2024.05.001
18. Lin Y, Li X, Huang L, et al. Acupuncture combined with Chinese herbal medicine for discogenic low back pain: protocol for a multicentre, randomised controlled trial. BMJ Open. 2024;14(11):e088898. doi:10.1136/bmjopen-2024-088898
19. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
20. MacPherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of Acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–155. doi:10.1111/j.1756-5391.2010.01086.x
21. Hayasaka S, Peiffer AM, Hugenschmidt CE, et al. Power and sample size calculation for neuroimaging studies by non-central random field theory. Neuroimage. 2007;37(3):721–730. doi:10.1016/j.neuroimage.2007.06.009
22. Desmond JE, Glover GH. Estimating sample size in functional MRI (fMRI) neuroimaging studies: statistical power analyses. J Neurosci Methods. 2002;118(2):115–128. doi:10.1016/S0165-0270(02)00121-8
23. Poldrack RA. The future of fMRI in cognitive neuroscience. Neuroimage. 2012;62(2):1216–1220. doi:10.1016/j.neuroimage.2011.08.007
24. Lu W, Dong K, Cui D, et al. Quality assurance of human functional magnetic resonance imaging: a literature review. Quant Imaging Med Surg. 2019;9(6):1147–1162. doi:10.21037/qims.2019.04.18
25. Chen X, Lu B, Yan CG. Reproducibility of R-fMRI metrics on the impact of different strategies for multiple comparison correction and sample sizes. Human Brain Mapp. 2018;39(1):300–318. doi:10.1002/hbm.23843
26. Melchart D, Streng A, Hoppe A, et al. Acupuncture in patients with tension-type headache: randomised controlled trial. BMJ. 2005;331(7513):376–382. doi:10.1136/bmj.38512.405440.8F
27. Sun M, Geng G, Chen J, et al. Acupuncture for chronic neck pain with sensitive points: study protocol for a multicentre randomised controlled trial. BMJ Open. 2019;9(7):e026904. doi:10.1136/bmjopen-2018-026904
28. Gao Z, Yin T, Lan L, et al. Efficacy and central mechanism of acupuncture treatment in patients with neck pain: study protocol for a randomized controlled trial. Trials. 2021;22(1):536. doi:10.1186/s13063-021-05507-y
29. Gao Z, Cui MJ, Wang HJ, et al. Investigating brain structure and functional alterations in the transition from acute to chronic neck pain: a resting-state fMRI study. J Pain Res. 2025;18:579–587. doi:10.2147/JPR.S500924
30. Zhong Z, Yao L, Liu YZ, et al. Objectivization study of acupuncture Deqi and brain modulation mechanisms: a review. Front Neurosci. 2024;18:1386108. doi:10.3389/fnins.2024.1386108
31. Baliki MN, Petre B, Torbey S, et al. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012;15(8):1117–1119. doi:10.1038/nn.3153
32. Vachon-Presseau E, Tétreault P, Petre B, et al. Corticolimbic anatomical characteristics predetermine risk for chronic pain. Brain. 2016;139(Pt 7):1958–1970. doi:10.1093/brain/aww100
33. Tu Y, Ortiz A, Gollub RL, et al. Multivariate resting-state functional connectivity predicts responses to real and sham acupuncture treatment in chronic low back pain. NeuroImage Clin. 2019;23:101885. doi:10.1016/j.nicl.2019.101885
34. Gao Z, Liu G, Zhang J, et al. The status of the quality control in neuroimaging studies of acupuncture analgesia. Evid Based Complement Alternat Med. 2020;2020(1):8502530. doi:10.1155/2020/8502530
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.