")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Efficacy and Safety of Adding Empagliflozin to Liraglutide on Renal Function in Patients with Advanced-Stage Type 2 Diabetic Kidney Disease: A Randomized Controlled Trial
Authors Sunagawa K, Hirai K , Sunagawa S, Kamiya N, Komesu I, Sunagawa Y, Sunagawa H, Nakachi K, Hirai A, Ookawara S, Morishita Y
Received 30 March 2024
Accepted for publication 4 October 2024
Published 14 October 2024 Volume 2024:17 Pages 3767—3781
DOI https://doi.org/10.2147/DMSO.S471535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Kae Sunagawa,1,2 Keiji Hirai,3 Sumito Sunagawa,1,2 Norifumi Kamiya,1 Isao Komesu,1 Yusako Sunagawa,1 Hiroshi Sunagawa,1 Ken Nakachi,4 Aizan Hirai,5 Susumu Ookawara,3 Yoshiyuki Morishita3
1Sunagawa Medical Clinic, Okinawa, Japan; 2Division of Endocrinology, Diabetes and Metabolism, Hematology, and Rheumatology, University of the Ryukyus, Okinawa, Japan; 3Division of Nephrology, Saitama Medical Center, Jichi Medical University, Saitama, Japan; 4Department of Internal Medicine, Shonan Hospital, Okinawa, Japan; 5Department of Internal Medicine, Chiba Cerebral and Cardiovascular Center, Chiba, Japan
Correspondence: Keiji Hirai, Division of Nephrology, First Department of Integrated Medicine, Saitama Medical Center, Jichi Medical University, 1-847 Amanuma-cho, Saitama-shi, Saitama-ken, 330-8503, Japan, Tel +81 48 647 2111, Fax +81 48 647 6831, Email [email protected]
Purpose: The aim of this study was to investigate the additional effects of empagliflozin on liraglutide in patients with advanced-stage type 2 diabetic kidney disease.
Patients and Methods: Forty-one patients were randomly assigned (1:1) to treatment with liraglutide alone during the first 6 months and subsequent treatment with liraglutide plus empagliflozin during the next 6 months (liraglutide plus empagliflozin group) (n = 20) or treatment with liraglutide alone for 12 months (liraglutide group) (n = 21). Liraglutide was administered subcutaneously once daily at a starting dose of 0.3 mg/day and up-titrated weekly by 0.3 mg to a maximum dose of 0.9 mg/day. Empagliflozin was administered orally at a dose of 10 mg once daily. The primary outcome was the change in renal function (estimated glomerular filtration rate) during the latter 6 months. Secondary outcomes were changes in body weight, systolic blood pressure, hemoglobin, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglyceride, uric acid, blood glucose, hemoglobin A1c, and urine protein creatinine ratio during the latter 6 months.
Results: Empagliflozin significantly increased the hemoglobin concentration (from 12.9 ± 1.9 to 13.7 ± 1.9 g/dL; p< 0.05) and decreased body weight (from 66.1 ± 12.9 to 64.5 ± 12.6 kg; p< 0.05). No significant differences were observed between the groups for estimated glomerular filtration rate, systolic blood pressure, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglyceride, uric acid, blood glucose, hemoglobin A1c, and urine protein creatinine ratio.
Conclusion: Empagliflozin increased hemoglobin concentration and decreased body weight in patients with advanced-stage type 2 diabetic kidney disease who received liraglutide. However, empagliflozin did not provide short-term benefits with regard to renal function decline, urinary protein excretion, or glycemic control in these patients.
Keywords: empagliflozin, sodium-glucose co-transporter 2 inhibitor, liraglutide, glucagon-like peptide-1 receptor agonist, diabetic kidney disease, diabetic nephropathy
Introduction
Diabetic kidney disease is a common complication of diabetes mellitus and is the most prevalent cause of end-stage kidney disease worldwide.1 Glucagon-like peptide (GLP)-1 analogs improve insulin resistance, promote insulin secretion, and suppress glucagon secretion, leading to improved glycemic control.2 GLP-1 analogs also mitigate oxidative stress, suppress mesangial proliferation, and inhibit the renin-angiotensin system, which attenuates renal function decline.3 Sodium-glucose co-transporter (SGLT)2 inhibitors promote urinary glucose excretion, leading to improved glycemic control.4 SGLT2 inhibitors also reduce intra-glomerular pressure, mitigate tubulointerstitial hypoxia, and modulate sympathetic activity, which attenuates renal function decline.5 Thus, GLP-1 analogs and SGLT2 inhibitors are recommended as first-line medications for the treatment of type 2 diabetes mellitus patients with chronic kidney disease.6
Recently, combination therapy comprising SGLT2 inhibitors and GLP-1 analogs has been reported to have additive effects on glucose metabolism and body weight in type 2 diabetes mellitus patients.7 However, the additional effects of SGLT2 inhibitors on GLP-1 analogs have not been fully investigated in type 2 diabetes mellitus patients with chronic kidney disease. Therefore, we performed a randomized controlled trial to investigate the additional effects of SGLT2 inhibitor on GLP-1 analog in patients with advanced-stage type 2 diabetic kidney disease. Empagliflozin was the only SGLT2 inhibitor that was shown to attenuate the progression of diabetic nephropathy at the time when we designed this study.8 Also, liraglutide was the only GLP-1 analog that was reported to reduce the development of renal events at that time.9 Therefore, we selected empagliflozin and liraglutide as study drugs.
Materials and Methods
Ethical Approval
This study was approved by the Ethics Committee of the University of Ryukyus (approval number: 2018–49), Japan, and performed in accordance with the principles of the Helsinki Declaration. Written informed consent was obtained from all participants before inclusion in the study. This study was registered in the University Hospital Medical Information Network clinical trial registry in Japan (UMIN 000031651).
Participants
The inclusion criteria in this study were: (1) age ≥ 20 years; (2) advanced-stage diabetic kidney disease defined as urine protein creatinine ratio (UPCR) ≥ 0.5 g/gCr and/or estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2.10 The exclusion criteria were: (1) type 1 diabetes mellitus; (2) secondary diabetes mellitus; (3) undergoing renal replacement therapy; (4) previous SGLT2 inhibitor or GLP-1 analog therapy; (5) hypersensitivity to SGLT2 inhibitors or GLP-1 analogs; and6 pregnant or intending to become pregnant.
Study Design
This was a multicenter, open-label, randomized, parallel design study performed between 1 April 2018 and 31 March 2021 at Sunagawa Medical Clinic and Shonan Hospital. The study design diagram is shown in Figure 1. The patient enrollment period was between 1 April 2018 and 31 March 2020. Patient randomization was performed at the registration center of Saitama Medical Center using a computer-based allocation program with a minimization method.
 |
Figure 1 Study design diagram. Abbreviations: eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; UPCR, urine protein creatinine ratio. |
Eligible patients were randomly assigned in a 1:1 ratio to receive liraglutide plus empagliflozin (liraglutide plus empagliflozin group) or liraglutide (liraglutide group). Patients in the liraglutide plus empagliflozin group received liraglutide, only, during the first 6 months (run-in period), and were then treated with liraglutide plus empagliflozin during the next 6 months (study period). Patients in the liraglutide group were treated with liraglutide alone during the run-in and study periods (12 months). Liraglutide was administered subcutaneously once daily at the same time each day. The starting dose was 0.3 mg/day, and the dose was up-titrated weekly by 0.3 mg to a maximum dose of 0.9 mg/day, because liraglutide was approved by national medical insurance for the treatment of type 2 diabetes mellitus at a maximum dose of 0.9 mg/day. Empagliflozin was administered orally at a dose of 10 mg once daily in the morning. All participants were examined every 3 months during the run-in and study periods. Body weight, systolic blood pressure, hemoglobin, eGFR, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride, uric acid, blood glucose, hemoglobin A1c (HbA1c), and UPCR were evaluated at each medical examination.
The primary outcome was the change in eGFR during the 6 months of the study period (second 6-month period). The secondary outcomes were changes in body weight, systolic blood pressure, hemoglobin, HDL-C, LDL-C, triglyceride, uric acid, blood glucose, HbA1c, and UPCR. Changes in body components, namely body fat mass, skeletal muscle mass, and total body water, were also evaluated.
Laboratory Methods
Blood and urine parameters were measured in the laboratory of each hospital. Blood parameters, including blood glucose, were evaluated either in the fasting state or randomly (non-fasting state) depending on the patients’ visiting time. Spot urine samples were used for urinalysis. Body components were assessed using a bioelectrical impedance device (InBody 770; Biospace, Tokyo, Japan). HbA1c concentrations were presented as National Glycohemoglobin Standardization Program values. eGFR was calculated using the following formula proposed by the Japanese Society of Nephrology: eGFR (mL/min/1.73 m2) = 194 × age−0.287 × serum creatinine−1.094 (multiplied by 0.739 for women). Hypertension was defined as blood pressure ≥ 140/90 mm Hg or the use of antihypertensive agents. Diabetes mellitus was defined as HbA1c ≥ 6.5% or the use of oral hypoglycemic agents and/or insulin therapy.
Statistical Analyses
Statistical analysis was performed using JMP® 11 (SAS Institute Inc., Cary, NC, USA). Data were expressed as means ± standard deviations for continuous variables and as counts and percentages for categorical variables. Comparisons of clinical parameters between the two groups were performed using Student’s t-test. Comparisons of component ratios between the two groups were performed using Fisher’s exact test. Comparisons of serial measurements within each group were performed using repeated measures of analysis of variance with Tukey’s test. p-values <0.05 were considered statistically significant. On the basis of a previous report,11 we assumed that the difference in mean eGFR between the two groups would be 1.0 mL/min/1.73 m2 with a standard deviation of 1.5 mL/min/1.73 m2 at 52 weeks. Thirty-six patients in each group were needed to establish the superiority of the test treatment for the primary endpoint with 80% power at a two-sided significance level of 5%. Therefore, we planned to enroll 40 patients per group in consideration of potential dropouts.
Results
Patient Characteristics
Forty-seven patients were enrolled in the study. During the run-in period, four patients withdrew consent, one patient changed to another hospital, and one patient developed bladder cancer; therefore, these patients were excluded from the study. The remaining 41 patients (22 men and 19 women, mean age 66.3 ± 10.1 years, body mass index 27.0 ± 5.0 kg/m2) were randomized to the liraglutide plus empagliflozin group (n = 20) and liraglutide group (n = 21) (Figure 2). All 41 patients completed the study period. Their mean eGFR, UPCR, and HbA1c at baseline were 41.0 ± 18.9 mL/min/1.73 m2, 1.5 ± 1.4 g/gCr, and 6.9 ± 1.1%, respectively. The proportion of the participants with hypertension was 97.6%. The percentages of the participants with diabetic neuropathy and retinopathy were 51.2% and 58.5%, respectively. Five (12.2%) patients had a history of ischemic heart disease and 7 (17.1%) had a history of stroke. The proportions of participants taking each of the following medications were: statin, 68.3%; renin-angiotensin system inhibitor, 80.5%; calcium channel blocker, 73.2%; diuretic, 22.0%; antihyperuricemic agent, 48.8%; glinide, 2.4%; α-glucosidase inhibitor, 43.9%; insulin, 19.5%; iron supplement, 7.3%; and erythropoiesis-stimulating agent, 9.8%. The baseline patients’ characteristics, laboratory values, and medications in each group are summarized in Table 1. There were no significant differences in any clinical parameter between the groups. The administered dose of liraglutide was 0.9 mg/day in all patients except two (0.6 mg/day, 1; 1.8 mg/day, 1).
 |
Table 1 Baseline Patients’ Characteristics, Laboratory Values, and Medications in the Liraglutide Plus Empagliflozin Group and Liraglutide Group |
 |
Figure 2 Patient flow diagram. |
Primary and Secondary Outcomes
The changes in eGFR in each group are shown in Figure 3. There was no significant difference in eGFR between the groups during the study period. The hemoglobin concentration of the liraglutide plus empagliflozin group increased significantly from 12.9 ± 1.9 g/dL at baseline to 13.5 ± 1.9 g/dL at 3 months (p<0.05) and 13.7 ± 1.9 g/dL at 6 months (p<0.05). The hemoglobin concentrations at 3 months and 6 months were significantly higher in the liraglutide plus empagliflozin group than in the liraglutide group (each, p<0.05) (Figure 4). The body weight of the patients in the liraglutide plus empagliflozin group decreased significantly from 66.1 ± 12.9 kg at baseline to 65.0 ± 13.1 kg at 3 months (p<0.05) and 64.5 ± 12.6 kg at 6 months (p<0.05). Body weight at 3 months and 6 months was significantly lower in the liraglutide plus empagliflozin group compared with the liraglutide group (each, p<0.05) (Figure 5). Other clinical parameters, namely systolic blood pressure (Figure 6), HDL-C (Figure 7), LDL-C (Figure 8), triglyceride (Figure 9), uric acid (Figure 10), blood glucose (Figure 11), HbA1c (Figure 12), and UPCR (Figure 13) did not differ significantly between the groups during the study period.
 |
Figure 3 Changes in eGFR in the liraglutide plus empagliflozin group and liraglutide group. Abbreviations: eGFR, estimated glomerular filtration rate. |
 |
Figure 4 Changes in hemoglobin concentrations in the liraglutide plus empagliflozin group and liraglutide group. Note: *p<0.05 vs baseline; † p<0.05 vs liraglutide group. |
 |
Figure 5 Changes in body weight in the liraglutide plus empagliflozin group and liraglutide group. Note: *p<0.05 vs baseline; †p<0.05 vs liraglutide group. |
 |
Figure 6 Changes in systolic blood pressure in the liraglutide plus empagliflozin group and liraglutide group. |
 |
Figure 7 Changes in HDL-C in the liraglutide plus empagliflozin group and liraglutide group. Abbreviations: HDL-C, high-density lipoprotein cholesterol. |
 |
Figure 8 Changes in LDL-C in the liraglutide plus empagliflozin group and liraglutide group. Abbreviations: LDL-C, low-density lipoprotein cholesterol. |
 |
Figure 9 Changes in triglyceride in the liraglutide plus empagliflozin group and liraglutide group. |
 |
Figure 10 Changes in uric acid in the liraglutide plus empagliflozin group and liraglutide group. |
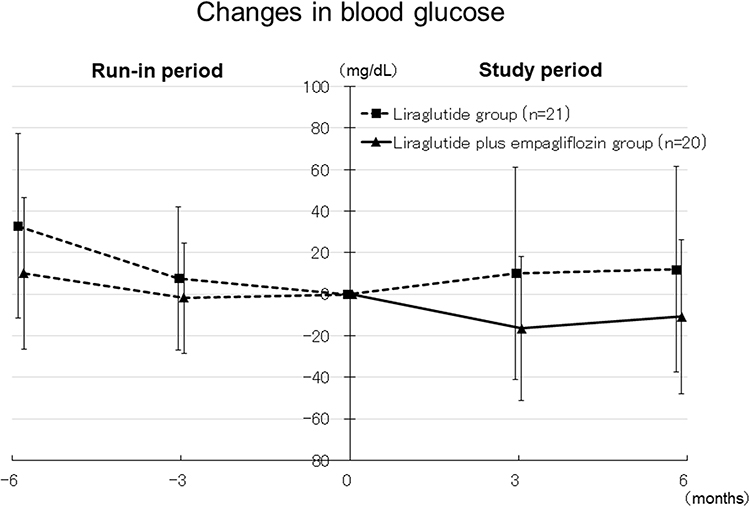 |
Figure 11 Changes in blood glucose in the liraglutide plus empagliflozin group and liraglutide group. |
 |
Figure 12 Changes in HbA1c in the liraglutide plus empagliflozin group and liraglutide group. Abbreviations: HbA1c, hemoglobin A1c. |
 |
Figure 13 Changes in UPCR in the liraglutide plus empagliflozin group and liraglutide group. Abbreviations: UPCR, urine protein creatinine ratio. |
Changes in body components are shown in Table 2. In the liraglutide plus empagliflozin group, body weight, skeletal muscle mass, and total body water decreased significantly at 6 months compared with baseline. However, body fat mass was unchanged at 6 months compared with baseline. In the liraglutide group, body weight, body fat mass, skeletal muscle mass, and total body water were unchanged at 6 months compared with baseline.
 |
Table 2 Changes in Body Components in the Liraglutide Plus Empagliflozin Group and Liraglutide Group |
Adverse Events
Adverse events were observed in 5 patients (pneumonia, 2; sepsis, 1; cerebral infarction, 1; fracture, 1) in the liraglutide group. However, liraglutide was tolerated by these patients and its administration was continued. No adverse event including euglycemic diabetic ketoacidosis was observed in the liraglutide plus empagliflozin group.
Discussion
In the present study, we found that empagliflozin increased the hemoglobin concentration in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide. We also found that empagliflozin decreased body weight in these patients. However, empagliflozin did not attenuate renal function decline, reduce urinary protein excretion, or improve glycemic control.
SGLT2 inhibitors reduce body fluid levels and concentrate blood by increasing urine volume.12 A randomized controlled trial showed that empagliflozin reduced total body water and increased hemoglobin concentration compared with placebo in patients with type 2 diabetes.13 In contrast, SGLT2 inhibitors promote sirtuin 1 activity by their off-target effects, thereby activating hypoxia-inducible factor 2α, which then increases the release of erythropoietin.14 A randomized controlled trial reported that empagliflozin increased erythropoietin concentration and hemoglobin concentration compared with placebo in patients with type 2 diabetes.15 In the present study, empagliflozin reduced total body water and increased hemoglobin concentration in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide; however, erythropoietin concentration was not assessed in this study. Further studies are needed to elucidate the mechanism underlying the improvement effect of empagliflozin on anemia in patients with type 2 diabetic kidney disease.
SGLT2 inhibitors promote sodium and water excretion in urine by inhibiting reabsorption of sodium and water in the proximal renal tubule, thereby reducing body fluid volume.16 SGLT2 inhibitors also promote glucose excretion in urine by inhibiting reabsorption of glucose in the proximal renal tubule, thereby increasing glucagon concentrations, which results in proteolysis in muscle.17 Several randomized controlled studies reported that empagliflozin reduced body weight, total body water, and skeletal muscle mass in patients with type 2 diabetes.13,18 In the present study, 6 months of empagliflozin therapy reduced body weight, total body water, and skeletal muscle mass in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide. These results suggest that empagliflozin reduced body weight by decreasing total body water and skeletal muscle mass in patients with type 2 diabetic kidney disease. The combined use of GLP-1 analogs and SGLT2 inhibitors has been shown to reduce body weight synergistically by their different mechanism of action.7 It has been reported that CKD patients and diabetic patients are prone to develop sarcopenia,19 which contributes to frailty and increased risk of mortality.20,21 Therefore, reduced muscle mass is a major problem in patients with diabetic kidney disease. Addition of SGLT2 inhibitors to GLP-1 analogs might be harmful with respect to development of sarcopenia in patients with diabetic kidney disease. Large-scale, long-term studies are necessary to clarify the influence of SGLT2 inhibitors on muscle mass in patients with advanced-stage type 2 diabetic kidney disease who are treated with GLP-1 analogs.
Numerous studies reported that SGLT2 inhibitors improved glycemic control in patients with type 2 diabetes.22 However, the blood glucose-lowering effect of SGLT2 inhibitors is attenuated as renal function declines.23 In the present study, empagliflozin did not decrease blood glucose concentration in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide. These results suggest that SGLT2 inhibitors might not improve glycemic control in patients with advanced-stage type 2 diabetic kidney disease.
Several GLP-1 analogs, namely liraglutide, dulaglutide, and semaglutide, have been shown to have renoprotective effect on type 2 diabetic kidney disease in large-scale clinical trials.9,24–26 These trials demonstrated that GLP-1 analogs reduced composite renal events including ≥ 30–50% reduction in eGFR and initiation of renal replacement therapy by 15–35%. Several SGLT2 inhibitors, namely empagliflozin, canagliflozin, and dapagliflozin, have been shown to have renoprotective on type 2 diabetic kidney disease in large-scale clinical trials.8,27–29 These trials demonstrated that SGLT2 inhibitors reduced composite renal events including ≥ 40% reduction in eGFR and end-stage kidney disease by 30–50%. Among all SGLT2 inhibitors, empagliflozin was the first SGLT2 inhibitor that was shown to have renoprotective effect on type 2 diabetic kidney disease in a large-scale clinical trial.8 In this trial, the effect of empagliflozin on renal outcomes was comparable between 10 mg/day and 25 mg/day.8 Therefore, in the present study, empagliflozin was administered at a dose of 10 mg/day. However, in the present study, empagliflozin did not attenuate renal function decline or reduce proteinuria in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide. Several reasons are considered for the discrepancy between results in previous studies and those in the present study. First, the number of patients in our study was small (n = 41), which might have reduced the power to detect a statistically significant difference between the two groups. Second, the study period was short (6 months). In a previous study of patients with advanced-stage type 2 diabetic kidney disease, an effect of SGLT2 inhibitors on renal function decline was observed 12 months after the initiation of therapy.28 Therefore, the study period in our study might have been too short to detect the renoprotective effect of empagliflozin. Large-scale, long-term, randomized controlled studies are needed to clarify the renoprotective effect of SGLT2 inhibitors in patients with advanced-stage type 2 diabetic kidney disease who are treated with GLP-1 analogs.
It has been reported that SGLT2 inhibitors have favorable effects on blood pressure, uric acid metabolism, and lipid profile.30 In the present study, empagliflozin tended to decrease systolic blood pressure, uric acid, and LDL-C and tended to increase HDL-C. However, these changes were not significant. These results might be due to small sample size and short-term study duration. Large-scale, long-term studies are necessary to clarify the effects of SGLT2 inhibitors on blood pressure, lipid profile, and uric acid metabolism in patients with advanced-stage type 2 diabetic kidney disease who are treated with GLP-1 analogs.
This study had two main advantages. First, we assessed the changes in clinical parameters including hemoglobin, HDL-C, LDL-C, triglyceride, uric acid, blood glucose, HbA1c, eGFR, and UPCR in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide plus empagliflozin. Second, we also assessed the changes in body components in these patients. This study might provide the foundation for further research to investigate the additional effects of SGLT2 inhibitors on GLP-1 analogs in patients with type 2 diabetic kidney disease.
There were several limitations in our study. First, we used an open-label design, which may have led to bias with regard to the study outcomes. Second, the study sample size was small, which might have reduced the statistical power to detect between-group differences. Third, this was a short-term study. Fourth, this study did not include type 2 diabetes mellitus patients with UPCR < 0.5 g/gCr and eGFR ≥ 30 mL/min/1.73 m2. Double-blind, large-scale, long-term, randomized controlled studies including type 2 diabetes mellitus patients with UPCR < 0.5 g/gCr and eGFR ≥ 30 mL/min/1.73 m2 are needed to elucidate the additional effects of SGLT2 inhibitors on GLP-1 analogs in patients with type 2 diabetic kidney disease.
Conclusion
Empagliflozin increased hemoglobin concentration and decreased body weight in patients with advanced-stage type 2 diabetic kidney disease who were treated with liraglutide. However, empagliflozin did not provide short-term benefits with regard to renal function decline, urinary protein excretion, or glycemic control in these patients.
Abbreviations
eGFR, estimated glomerular filtration rate; GLP-1, glucagon-like peptide-1; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SGLT2, sodium-glucose co-transporter; UPCR, urine protein creatinine ratio.
Data Sharing Statement
The data analyzed in this study are available from the corresponding author on reasonable request.
Consent for Publication
All patients provided consent for the publication of their data and were shown the article contents to be published.
Acknowledgments
The authors thank all patients and clinicians who participated in the study. We also thank Jane Charbonneau, DVM, from Edanz for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ghaderian SB, Hayati F, Shayanpour S, Beladi Mousavi SS. Diabetes and end-stage renal disease; a review article on new concepts. J Renal Injury Prev. 2015;4(2):28–33. doi:10.12861/jrip.2015.07
2. Sharma D, Verma S, Vaidya S, Kalia K, Tiwari V. Recent updates on GLP-1 agonists: current advancements & challenges. Biomed Pharmacother. 2018;108:952–962. doi:10.1016/j.biopha.2018.08.088
3. Vitale M, Haxhi J, Cirrito T, Pugliese G. Renal protection with glucagon-like peptide-1 receptor agonists. Curr Opin Pharmacol. 2020;54:91–101. doi:10.1016/j.coph.2020.08.018
4. Chao EC. SGLT-2 inhibitors: a new mechanism for glycemic control. Clin Diabetes. 2014;32(1):4–11. doi:10.2337/diaclin.32.1.4
5. Leoncini G, Russo E, Bussalino E, Barnini C, Viazzi F, Pontremoli R. SGLT2is and renal protection: from biological mechanisms to real-world clinical benefits. Int J Mol Sci. 2021;22(9):4441. doi:10.3390/ijms22094441
6. American Diabetes. A. 9. pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S111–S24. doi:10.2337/dc21-S009
7. DeFronzo RA. Combination therapy with GLP-1 receptor agonist and SGLT2 inhibitor. Diabetes Obes Metab. 2017;19(10):1353–1362. doi:10.1111/dom.12982
8. Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–334. doi:10.1056/NEJMoa1515920
9. Mann JFE, Orsted DD, Brown-Frandsen K, et al. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med. 2017;377(9):839–848. doi:10.1056/NEJMoa1616011
10. Haneda M, Utsunomiya K, Koya D, et al. A new classification of diabetic nephropathy 2014: a report from joint committee on diabetic nephropathy. J Diabetes Investig. 2015;6(2):242–246. doi:10.1111/jdi.12319
11. Cherney DZI, Zinman B, Inzucchi SE, et al. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: an exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5(8):610–621. doi:10.1016/S2213-8587(17)30182-1
12. Tang J, Ye L, Yan Q, Zhang X, Wang L. Effects of sodium-glucose cotransporter 2 inhibitors on water and sodium metabolism. Front Pharmacol. 2022;13:800490. doi:10.3389/fphar.2022.800490
13. Hoshika Y, Kubota Y, Mozawa K, et al. Effect of empagliflozin versus placebo on body fluid balance in patients with acute myocardial infarction and type 2 diabetes mellitus: subgroup analysis of the EMBODY trial. J Card Fail. 2022;28(1):56–64. doi:10.1016/j.cardfail.2021.07.022
14. Iacobini C, Vitale M, Haxhi J, Pesce C, Pugliese G, Menini S. Mutual regulation between redox and hypoxia-inducible factors in cardiovascular and renal complications of diabetes. Antioxidants. 2022;11(11). doi:10.3390/antiox11112183
15. Mazer CD, Hare GMT, Connelly PW, et al. Effect of empagliflozin on erythropoietin levels, iron stores, and red blood cell morphology in patients with type 2 diabetes mellitus and coronary artery disease. Circulation. 2020;141(8):704–707. doi:10.1161/CIRCULATIONAHA.119.044235
16. Wilcox CS. Antihypertensive and renal mechanisms of SGLT2 (Sodium-Glucose Linked Transporter 2) inhibitors. Hypertension. 2020;75(4):894–901. doi:10.1161/HYPERTENSIONAHA.119.11684
17. Yabe D, Nishikino R, Kaneko M, Iwasaki M, Seino Y. Short-term impacts of sodium/glucose co-transporter 2 inhibitors in Japanese clinical practice: considerations for their appropriate use to avoid serious adverse events. Expert Opin Drug Saf. 2015;14(6):795–800. doi:10.1517/14740338.2015.1034105
18. Zeng YH, Liu SC, Lee CC, Sun FJ, Liu JJ. Effect of empagliflozin versus linagliptin on body composition in Asian patients with type 2 diabetes treated with premixed insulin. Sci Rep. 2022;12(1):17065. doi:10.1038/s41598-022-21486-9
19. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
20. Ribeiro HS, Neri SGR, Oliveira JS, Bennett PN, Viana JL, Lima RM. Association between sarcopenia and clinical outcomes in chronic kidney disease patients: a systematic review and meta-analysis. Clin Nutr. 2022;41(5):1131–1140. doi:10.1016/j.clnu.2022.03.025
21. Lin JA, Hou JD, Wu SY. Effect of sarcopenia on mortality in type 2 diabetes: a long-term follow-up propensity score-matched diabetes cohort study. J Clin Med. 2022;11(15):4424. doi:10.3390/jcm11154424
22. Fujita Y, Inagaki N. Renal sodium glucose cotransporter 2 inhibitors as a novel therapeutic approach to treatment of type 2 diabetes: clinical data and mechanism of action. J Diabetes Investig. 2014;5(3):265–275. doi:10.1111/jdi.12214
23. Cherney DZI, Cooper ME, Tikkanen I, et al. Pooled analysis of Phase III trials indicate contrasting influences of renal function on blood pressure, body weight, and HbA1c reductions with empagliflozin. Kidney Int. 2018;93(1):231–244. doi:10.1016/j.kint.2017.06.017
24. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and renal outcomes in type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet. 2019;394(10193):131–138. doi:10.1016/S0140-6736(19)31150-X
25. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
26. Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109–121. doi:10.1056/NEJMoa2403347
27. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
28. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi:10.1056/NEJMoa1811744
29. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/NEJMoa1812389
30. Xu J, Hirai T, Koya D, Kitada M. Effects of SGLT2 inhibitors on atherosclerosis: lessons from cardiovascular clinical outcomes in type 2 diabetic patients and basic researches. J Clin Med. 2021;11(1):137. doi:10.3390/jcm11010137
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.