")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Efficacy and Safety of Colquhounia Root Tablet for Chronic Glomerulopathy: A Real-World Survey With Bioinformatics Insights
Authors Liu H, Yan H, Li Y, Yao Y, Zhang C, Xiong J
Received 24 July 2024
Accepted for publication 19 February 2025
Published 28 February 2025 Volume 2025:19 Pages 1421—1440
DOI https://doi.org/10.2147/DDDT.S488557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mariana Carmen Chifiriuc
Huixia Liu,1,* Hao Yan,2,* Yujuan Li,1 Ye Yao,1 Chun Zhang,1 Jing Xiong1
1Department of Nephrology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China; 2Department of Gynecologic Oncology, Hubei Cancer Hospital, Wuhan, Hubei, 430070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Xiong, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China, Tel +862785726713, Email [email protected]
Background: Colquhounia root tablet (CRT) has been in treatment of autoimmune and inflammatory diseases for decades, but large-scale clinical observations are lacking. The novelty of this study lies in providing the first large-scale real-world clinical data to evaluate the effectiveness and safety of CRT on chronic glomerulopathy and to explore potential molecular mechanisms.
Methods: This is a single-arm retrospective study in the real-world. Data analysis included descriptive statistics, t-tests, non-parametric tests, and analysis of variance, with P < 0.05 considered as the standard for statistical significance. Predicting molecular targets and pathways of CRT through network pharmacology and validating through molecular docking.
Results: (1) Among 317 patients, 74.8% experienced a significant decrease in proteinuria (P < 0.001), particularly in IgA nephropathy (IgAN), type 2 diabetes mellitus-related chronic kidney disease (T2DM related-CKD) and membranous nephropathy (MN). (2) CRT works quickly in reducing proteinuria. 76.7% patients had obvious effect at first visit (P < 0.001). (3) CRT had no obvious effect on creatinine and albumin. (4) Subgroup analysis showed regardless of level of proteinuria and eGFR, CRT had significant efficacy. (5) CRT has good security and low incidence of adverse reactions. (6) Bioinformatics analysis suggested that CRT acts on chronic glomerulopathy by infections, metabolism, Th17 cell differentiation and C-type lectin signaling pathways. The core targets are IL-6, TNF, AKT1, IL-1β and ALB.
Conclusion: CRT treatment for chronic glomerulopathy is safe and effective, which can significantly reduce proteinuria. Network pharmacology results suggest the mechanism of CRT in chronic glomerulopathy may involve Th17 cell differentiation and CLR signaling pathway.
Plain Language Summary: This study evaluated the safety and effectiveness of a medication called Colquhounia root tablet (CRT) for treating chronic glomerulopathy. We discovered that CRT not only significantly reduces proteinuria, but also has a low risk of side effects. Our findings suggest that CRT’s beneficial effects might be due to its impact on Th17 cell differentiation and a specific signaling pathway, C-type lectin signaling pathways, which are involved in the body’s immune response. This insight could pave the way for new treatment strategies for patients suffering from chronic glomerulopathy.
Keywords: chronic glomerulopathy, colquhounia root tablet, network pharmacology, molecular docking
Introduction
Proteinuria is the major clinical manifestation of chronic glomerulopathy and has been identified as the most widely recognized risk factor. Reducing proteinuria can effectively slow the progression to end-stage renal disease. Currently, renin-angiotensin system inhibitor (RASi), glucocorticoid and immunosuppressants are common treatments of treatment for proteinuria. However, long-term glucocorticoids therapy can cause metabolic abnormalities like weight gain and dysglycemia while prolonged immunosuppressants treatment increases the risk of infections and potentially serious side effects such as bone marrow suppression.
There are still no specific therapies for IgA nephropathy (IgAN) and type 2 diabetes mellitus-related CKD (T2DM related-CKD). On the basis of using RASi, T2DM related-CKD patients are treated with glycemic, blood pressure and lipid control while glucocorticoid and mycophenolate mofetil can be considered for IgAN patients with higher risk of CKD progression in Chinese. However, these agents are not effective for some patients. Significant progress has been made in the treatment of membranous nephropathy (MN), including glucocorticoid combined with cyclophosphamide, calcineurin inhibitor and CD20-targeted agents. However, some patients cannot achieve clinical remission even after first-line treatment.
Tripterygium hypoglaucum (H. Lév). Hutch. (THH, SFDA approval number: Z20027411) is a plant of the family Weimao, belonging to the genus Tripterygium. Its active ingredients include triptolide, celastrol and wilforine, which have hormone-like effects such as anti-inflammatory and anti-immune reactions. These components are thought to modulate the immune response and reduce inflammation, which are key pathogenic processes in chronic glomerulopathy. Previous studies have shown that triptolide, in particular, can suppress the proliferation of immune cells and reduce the production of inflammatory cytokines, suggesting a potential therapeutic role in kidney diseases characterized by immune-mediated injury.1–3 Colquhounia root tablet (CRT) is purified and processed from the roots of Kunming shanhaitang. Previously, it was mainly used to therapy immune-related diseases such as rheumatoid arthritis and lupus erythematosus. Currently, there is a significant gap in the literature regarding the efficacy and safety of CRT in chronic glomerulopathy, particularly in real-world. Most studies are case analysis and small-cohort observations, which lack the power to determine the true efficacy and safety of CRT. Additionally, there is a lack of bioinformatics insights into the molecular mechanisms by which CRT may exert its effects in kidney diseases.
Despite its widespread use in autoimmune and inflammatory conditions, CRT’s efficacy in chronic glomerulopathy remains underexplored in large-scale clinical settings. This study aims to fill this gap by assessing CRT’s clinical benefits and elucidating its molecular mechanisms using network pharmacology and molecular docking analyses, providing a novel perspective on its therapeutic potential.
Materials and Methods
Introduction to CRT
Tripterygium hypoglaucum (H. Lév). Hutch. (THH; www.theplantlist.org; February 19, 2022), namely Kunming shanhaitang in Chinese, is a traditional Chinese herb belonging to the genus Tripterygium (Celastraceae). The Tripterygium hypoglaucum specimen used in this study was collected from Xichang District, Sichuan Province, China. The specimen was formally identified by Professor Xie Dengfeng, a certified botanist affiliated with the School of Life Sciences, Sichuan University. A voucher specimen (Accession Number: 02028830) has been deposited in the Plant Specimen Room, Department of Biology, Sichuan University. There was a difference in the contents between THH and Tripterygium wilfordii Hook. f. (TWHF, Leigongteng in China, a morphologically comparable species in the genus Tripterygium) samples.4
CRT was prepared from the water-soluble extract of the THH peeled root, following a rigorous and standardized process to ensure the consistency and potency of the final product. The extraction and purification process is conducted under Good Manufacturing Practice (GMP) conditions, with strict quality control measures at each step to ensure the product’s safety and efficacy. Each batch of CRT is meticulously tested for its active components, including triptolide, triptonide, wilforgine, wilforine, and celastrol, to ensure that the specified amounts are present in each tablet. CRT (lot number: 20191201, each tablet containing 2.951μg triptolide, 0.057μg triptonide, 2.493μg wilforgine, 0.819μg wilforine and 0.594μg celastrol) was obtained from the pharmaceutical factory of the Chongqing Academy of Chinese Mataria Medica (Chongqing, China) and each component quantified using high-performance liquid chromatography (HPLC) to ensure batch uniformity and stability.
Study Design and Population
This study retrospectively collected 375 patients treated with CRT in Wuhan Union Hospital from January 1, 2020, to December 31, 2023, and 317 patients with complete follow-up data were included in the final analysis. To minimize selection bias, patients were selected using a systematic sampling method, ensuring a representative and random selection from the patient pool. Inclusion criteria: (1) age 18–80 years old with unlimited gender and ethnicity; (2) 24-h proteinuria ≥ 150 mg or urinary protein creatinine ratio ≥ 150 mg/g; (3) regular CRT treatment for 3 months. Exclusion criteria: (1) presence of life-threatening complications; (2) pregnant, lactating and pregnancy preparation patients. Withdrawal criteria: (1) serious adverse reactions and poor compliance; (2) incomplete follow-up data and irregular follow-up.
Patients who met the inclusion criteria and did not meet the exclusion criteria received oral CRT treatment. Baseline data were collected from patients at the beginning of CRT treatment and patients were closely monitored. The interval between each visit and the results of hematological and urinalysis tests were recorded to further evaluate the efficacy and safety of CRT in the treatment of chronic glomerulonephritis.
Medication Regimen
A total of 317 patients received CRT treatment (three times a day, three to five tablets each time). Some patients used CRT monotherapy, while others used CRT in combination when treatment with RASI, SGLT-2 inhibitors, glucocorticoids, or immunosuppressants was not effective.
Observation Indicators
Follow-up indicators were obtained through the inpatient and outpatient medical record systems, including gender, age, complications (hypertension and diabetes mellitus history), drug history, white blood cell (WBC), platelets (PLT), glutaminase, alanine aminotransferase (ALT), aspartate transaminase (AST), total protein (TP), albumin (ALB), 24-h proteinuria or urinary protein creatinine ratio, blood urea nitrogen (BUN), serum creatinine (Scr), estimated glomerular filtration rate (eGFR), fasting blood glucose, total cholesterol (TC), and total triglycerides(TG). Adverse reactions were recorded such as gastrointestinal reactions, rashes, and female menstruation through the method of outpatient follow-ups and questionnaires.
Subgroup Analysis
According to different etiology or pathology, patients were divided into IgA nephropathy group, T2DM-related CKD group, MN group and other pathological types or unspecified pathological types groups. According to 24-h proteinuria or urinary protein creatinine ratio is divided into 3 groups: (1) heavy proteinuria group: 24-h proteinuria or urinary protein creatinine ratio > 3500 mg; (2) moderate proteinuria group: 1000mg < 24-h proteinuria or urinary protein creatinine ratio ≤ 3500 mg; (3) mild proteinuria group: 24-h proteinuria or urinary protein creatinine ratio ≤ 1000 mg. According to the estimated glomerular filtration rate (eGFR), eGFR > 60 mL/min/1.73 m2 and eGFR ≤ 60 mL/min/1.73m2 were divided. The above groups were self-controlled before and after medication. To control for the increased risk of Type I error due to multiple comparisons, we applied the Bonferroni correction to our statistical analyses.
Statistical Analyses
In this study, SPSS 20.0 was applied to statistically analyze the collected data. Statistical description: categorical variables were described in the form of number of cases (percentage). For continuous variables, those that met the normal distribution were described in the form of mean ± standard deviation; continuous variables that did not follow a normal distribution and were described in terms of medians (upper quartile, lower quartile). This study used the method of analyzing patients who completed each follow-up. For data conforming to normal distribution, and the comparison between groups was performed using paired-samples T-test, with P < 0.05 considered statistically significant. Continuous variables that did not follow a normal distribution were compared between groups using nonparametric tests, and differences were considered statistically significant at P < 0.05. Analysis of variance was used for comparison among the three groups.
CRT Components and Related Target Prediction
CRT components were collected by literature search, and the structural formula of the compounds were downloaded using the PubChem database and saved in sdf format. Drug type screening using SwissADME platform (http://www.swissadme.ch): (1) Gastrointestinal absorption was “High” and (2) two or more results of five class drug activity prediction (Lipinski, Ghose, Veber, Egan, Muegge) were “Yes”. For compounds that did not meet the screening criteria, they were included as appropriate.
Through swisstargetprediction (http://www.swisstargetprediction.ch/) and Traditional Chinese Medicine Systems Pharmacology Database and Analysis Platform(TCMSP) database (https://old.tcmsp-e.com/tcmsp.php) to predict CRT molecular targets. The UniProt database (https://www.uniprot.org/) was used to further standardize the molecular targets.
Disease Target Prediction and Venn Diagram of Common Targets
Using the GeneCards database (https://www.genecards. org/), OMIM database (https://www.omim.org/) and TTD database (http://bidd./group/cjttd/)) collected IGAN, T2DM related-CKD and MN disease targets. Disease targets acquired in the three databases were summarized and duplicate values were removed. CRT targets and disease targets were interposed to obtain the common target and Venn diagram.
Construct CRT-Component-Target Network and PPI Network and Screening of Core Targets
CRT-component-target network was constructed using cytoscape3.7.2. The common targets of CRT and the three diseases were uploaded to STRING11.5 database (https://string-db.org/), the “Homo sapiens” species was selected, and the confidence score of the protein interaction relationship was set to medium confidence (score ≥ 0.4) to obtain the PPI network. The PPI network was analyzed using cytoscape3.7.2, network topology parameters were calculated using Analyze Network tool, core targets were adjusted and screened according to Degree, Closeness and Betweenness, and finally visualized using cytoscape3.7.2.
GO and KEGG Biological Enrichment Analysis
The GO (Gene Ontology) and KEGG (Kyoto Encyclopedia of Gene and Genomes) biological enrichment analysis and functional annotation of the intersection targets were performed using the R4.2.0 clusterProfiler package. GO annotation includes biological program (BP), cell components (CC), and molecular function (MF). According to the corrected P-value, the top 20 enrichment results were finally selected.
Molecular Docking Technology
Molecular docking of the obtained core targets (top six according to Degree value). Using PubChem and Chem3D 20.0 optimization (binding energy minimization) and preserving the 3D structure of core components (mol2 format), the crystal structure of core receptor protein (pdb format) was downloaded using the RCSB PDB database (https://www.rcsb.org/). The AutoDockTools 1.5.7 is used to hydrogenation the receptor protein, process the small-molecule ligand, calculate the local charge (Partial charges), and set rotatable ligand bonds. Finally, the processed ligand and receptor structure were saved in pdbqt lattice type. Molecular docking predictions were performed using AutoDock Vina 1.1.2.
Results
Patient Characteristics
By December 31, 2023, 375 patients received CRT treatment in Wuhan Union Hospital. Among them, 58 patients were excluded from the analysis: 13 patients had incomplete baseline data and 45 patients had incomplete follow-up data. Finally, a total of 317 patients were eligible for statistical analysis. Baseline data were shown in Table 1. The patients were followed up 1–6 times, with a single follow-up interval of approximately 5 weeks. The objective of this study was to assess the relatively short-term efficacy (follow-up ≤3 visits) and relatively long-term efficacy (follow-up > 3 visits) of CRT treatment, with 113 patients were followed up more than 3 times.
 |
Table 1 General Characteristics of 317 Patients |
Efficacy of CRT in Chronic Glomerulopathy
CRT is highly effective in reducing proteinuria in IgAN, T2DM related-CKD, MN and other chronic glomerulopathy patients and works quickly. Although there are fluctuations, the overall trend was downward. Proteinuria decreased in 74.8% patients. At a median follow-up of 18.9 weeks, proteinuria was significantly reduced to 1459 mg/d compared with 2204 mg/d before treatment (P < 0.001) (Figure 1A). The results revealed an overall fluctuating downward trend (Figure 1B).
 |
Figure 1 Efficacy of CRT. (A) Comparison of 24-h urine protein before and after CRT treatment. (B) Changes of 24-h urine protein at each follow-up. (C) Changes of serum creatinine before and after CRT treatment. (D) Changes of serum albumin before and after CRT treatment. (**P < 0.01, ***P < 0.001, ns = not significant). |
CRT had no significant influence on serum creatinine and albumin levels. As shown in Figure 1, the overall average creatinine level before and after treatment were 107.1μ mol/L and 106.9 μmol/L, respectively (n = 291, P = 0.239); the average serum albumin levels before and after treatment were 37.2 g/L and 37.3 g/L, respectively (n = 278, P = 0.14), with no statistically significant difference.
The Efficacy of CRT in IgAN
Proteinuria declined from 1568 mg/d to 788 mg/d in IgAN patients at a median follow-up time of 29.7 weeks (P < 0.001). Proteinuria decreased by 50%. Proteinuria levels showed a continuous decline at the first three visits, and increased slightly at the fourth, fifth and sixth visits.
Fifty-one cases completed the first follow-up. There was a significant reduction in proteinuria from 1568 mg/d to 831.9 mg/d (P < 0.001) (Figure 2A). Forty-one patients finished the second visit. Compared to a mean proteinuria of 1660 mg/d at baseline, proteinuria decreased to 865.75 mg/d and 726 mg/d at the first two visits (P < 0.001) (Figure 2B). Thirty-two patients completed three visits. Proteinuria decreased from a baseline value of 1614 mg/d to 853.45 mg/d, 753 mg/d and 642.5 mg/d (P < 0.001) (Figure 2C). Twenty-four patients finished four follow-ups, with the first three follow-ups showing a consistent downward trend (P<0.01). The fourth follow-up visit showed a slight increase to 808 mg/d (P < 0.01) (Figure 2D). Among the patients 19 and 16 finished five and six visits, the first three visits showed a gradual decline, and the fifth to sixth follow-ups showed fluctuations, but all were below baseline value (Figure 2E and F).
 |
Figure 2 Changes of 24-h urine protein in IgAN patients. (A) Changes of 24-h urine protein in IgAN patients who completed one follow-up. (B) Changes of 24-h urine protein in IgAN patients who completed two follow-ups. (C) Changes of 24-h urine protein in IgAN patients who completed three follow-ups. (D) Changes of 24-h urine protein in IgAN patients who completed four follow-ups. (E) Changes of 24-h urine protein in IgAN patients who completed five follow-ups. (F) Changes of 24-h urine protein in IgAN patients who completed six follow-ups. (**P < 0.01, ***P < 0.001). |
The Efficacy of CRT in T2DM-Related CKD
T2DM-related CKD patients decreased from 3233.5 mg/d to 2726.14 mg/d at a median follow-up time of 13.8 weeks (P < 0.01). Proteinuria decreased by 16%. Forty patients finished the first visit. There was a significant reduction in proteinuria from 3233.5 mg/d to 2704.77 mg/d (P < 0.05) (Figure 3A). Twenty patients completed two visits. Compared with an average proteinuria of 4820.67 mg/d at baseline, proteinuria decreased to 3162.27 mg/d in patients at the first follow-up (P=0.04). The value decreased to 3078.9 mg/d at the second visit (P=0.002) (Figure 3B). Thirteen patients finished three visits. Proteinuria levels decreased from 5020.93 mg/d to 2167.83 mg/d at the first two follow-ups (P=0.011), but increased in third follow-ups (P < 0.05) (Figure 3C). 6 patients completed four follow-ups and the proteinuria decrease from 2300.17 mg/d to 1889.67 mg/d (P=0.064) at the first two follow-ups, but increased above the baseline in third and fourth follow-ups (P>0.05) (Figure 3D). Five patients finished five follow-ups (Figure 3E).
 |
Figure 3 Change of 24-h urine protein in T2DM-related CKD patients. (A) Changes of 24-h urine protein in T2DM-related CKD patients who completed one follow-up. (B) Changes of 24-h urine protein in T2DM-related CKD patients who completed two follow-ups. (C) Changes of 24-h urine protein in T2DM-related CKD patients who completed three follow-ups. (D) Changes of 24-h urine protein in T2DM-related CKD patients who completed four follow-ups. (E) Changes of 24-h urine protein in T2DM-related CKD patients who completed five follow-ups. (*P < 0.05, **P < 0.01, ns = not significant). |
The Efficacy of CRT in MN
MN patients decreased from 2808 mg/d to 1395 mg/d at a median follow-up time of 22.4 weeks (P < 0.05). Proteinuria decreased by 50%. Eighty-one cases completed the first follow-up, who had a significant reduction in proteinuria from 2808 mg/d to 1390.18 mg/d (Figure 4A). Sixty-seven patients completed two visits and proteinuria decreased to 1390.18 mg/d compared to 2937 mg/d at baseline (P = 0.005). The value in the second follow-up increased to 1895 mg/d (Figure 4B). Fifty-two patients completed three visits. At the first follow-up, proteinuria decreased from 2685 mg/d to 1336.5 mg/d (P = 0.041), and at the second visit, it decreased to 1775.5 mg/d (P = 0.002). At the third follow-up, proteinuria decreased to 1499.5 mg/d (P < 0.001) (Figure 4C).
 |
Figure 4 Changes of 24-h urine protein in MN patients. (A) Changes of 24-h urine protein in MN patients who completed one follow-up. (B) Changes of 24-h urine protein in MN patients who completed two follow-ups. (C) Changes of 24-h urine protein in MN patients who completed three follow-ups. (D) Changes of 24-h urine protein in MN patients who completed four follow-ups. (E) Changes of 24-h urine protein in MN patients who completed five follow-ups. (F) Changes of 24-h urine protein in MN patients who completed six follow-ups. (*P < 0.05, **P < 0.01, ***P < 0.001, ns = not significant). |
Forty-two patients completed four visits with a fluctuating downward trend. The first follow-up was a decrease from 2962 mg/d at baseline to 1270.19 mg/d (P=0.006). At the second and third visits, it changed to 1620.18 mg/d and 1438.5 mg/d (P < 0.001). There was a mild increase to 1649.21mg/d at the fourth follow-up (P < 0.001) (Figure 4D). Among the patients 29 and 20 finished five and six follow-ups, proteinuria levels showed a fluctuating downward trend (Figure 4E and F).
The Efficacy of CRT in Other Chronic Glomerulopathy
In other patients, proteinuria decreased from 2022 mg/d to 1459.7 mg/d at a median follow-up time of 17.4 weeks (P < 0.001). One hundred and forty-five patients completed first follow-up, who had a significant reduction in proteinuria from 2022 mg/d to 1275 mg/d (P < 0.001) (Figure 5A). Ninety-one patients finished two visits, and proteinuria decreased from 1787.8 mg/d to 1166 mg/d (P<0.001). The patient had an increase in proteinuria to 1375.7 mg/d (P = 0.001) (Figure 5B). Sixty-seven patients completed three visits. Proteinuria decreased from 2022 mg/d to 1174 mg/d at the first follow-up (P < 0.001). Proteinuria increased to 1488 mg/d (P=0.008) and 1652 mg/d (P =0.034) at the second and third visits (Figure 5C).
 |
Figure 5 Changes of 24-h urine protein in other CGN patients. (A) Changes of 24-h urine protein in other CGN patients who completed one follow-up. (B) Changes of 24-h urine protein in other CGN patients who completed two follow-ups. (C) Changes of 24-h urine protein in other CGN patients who completed three follow-ups. (D) Changes of 24-h urine protein in other CGN patients who completed four follow-ups. (E) Changes of 24-h urine protein in other CGN patients who completed five follow-ups. (F) Changes of 24-h urine protein in other CGN patients who completed six follow-ups. (*P < 0.05, **P < 0.01, ***P < 0.001, ns = not significant). |
Over the course of four follow-up visits, proteinuria levels of 42 cases decreased from a baseline value of 2011.69 mg/d to 1170 mg/d (P<0.001), 1307.36 mg/d (P<0.001), 1502.5 mg/d (P=0.01), and 993.16 mg/d (P<0.001) in order (Figure 5D). Among the patients 30 and 20finished five and six follow-ups, the level of proteinuria showed a fluctuating downward trend (Figure 5E and F).
Subgroup Analysis
Subgroup analysis revealed CRT reduced proteinuria remarkably regardless of proteinuria and eGFR levels, and there was no statistical difference between subgroups.
Different Proteinuria Levels Subgroups
Based on the baseline proteinuria levels, patients were divided into heavy (>3500 mg/d), moderate (1500 to 3500 mg/d) and mild (≤1500 mg/d) proteinuria subgroups. Proteinuria significantly reduced from 6175.78 mg/d to 3515.74 mg/d in the heavy subgroup (P < 0.001). The moderate subgroup significantly declined from 2245.95 mg/d to 1577 mg/d (P < 0.01). The mild subgroup significantly descended from 1027 mg/d to 590 mg/d. There was no statistically significant difference in the rate of decrease in urine protein among the three groups (Figure 6A and B).
 |
Figure 6 Changes of 24-h urine protein in subgroups. (A) Changes of 24-h urine protein in heavy, moderate and mild proteinuria patients. (B) Comparison of the rate of decline with 24-h urine protein in heavy, moderate, and mild proteinuria patients. (C) Changes of 24-h urine protein in eGFR>60 mL/min/1.73m² and ≤ 60 mL/min/1.73m² patients. (D) Comparison of the rate of decline with 24-h urine protein in eGFR>60 mL/min/1.73m² and ≤ 60 mL/min/1.73m² patients. (**P < 0.01, ***P < 0.001, ns = not significant). |
Different eGFR Levels Subgroups
Patients were divided into high eGFR (>60mL/min/1.73m2) and low eGFR (≤60mL/min/1.73m2) subgroups. Proteinuria in the high eGFR subgroup significantly reduced from 1816 mg/d to 1058 mg/d (P < 0.001). The low eGFR group decreased from 2547.2 mg/d to 1763 mg/d (P < 0.001). There was no statistically significant difference in the rate of decrease in proteinuria between two subgroups (P > 0.05) (Figure 6C and D).
Adverse Effects
Figure 7 revealed the incidence of adverse reactions including leukopenia, thrombocytopenia, hepatic insufficiency, menstrual disorders, skin rash, and gastrointestinal reactions in 317 patients (Figure 7).
 |
Figure 7 Adverse reactions of CRT. |
CRT had no obvious myelosuppression effect. There was no significant reduction in leukocytes and platelets after CRT treatment. One hundred and sixty-three patients underwent analysis of myelosuppression. After treatment, 50.3% (82 patients) had leukopenia, 5 of which were below normal leukocyte values, while 52.8% (36 patients) had thrombocytopenia, 7 of which were below normal platelet values.
CRT did not cause significant liver injury. A total of 278 patients were included in the analysis. Transaminase elevation exceeded the normal value in 6.8% patients, and only 0.36% (1 case) of patients with elevated transaminase persistently increased more than 3 times the upper limit of normal (ULN).
In addition, there were 2.21% patients (7 cases) with menstrual disorders. Due to missing data, we did not perform statistical analysis. However, clinical experience suggested that CRT had obvious gonadal suppression, including menstrual disorders in women and decreased sperm motility in men. It is related to the duration of CRT use and dose. 0.95% patients (3 cases) with skin rash after CRT treatment. There were 1.26% patients (4 cases) with gastrointestinal reactions.
These indicated that CRT had minimal adverse reactions and was relatively safe in the treatment of chronic glomerulopathy.
Integrated Bioinformatics Analysis
CRT and Diseases Target Predictions
A total of 46 CRT components were identified, of which 26 potential active ingredients were selected by SwissADME. Ultimately, 523 targets were obtained finally. The CRT-component-target network was established by cytoscape3.7.2 (Figure 8–10A).
 |
Figure 8 Bioinformatics analysis of IgAN. (A) CRT-components-target network diagram. (B) Venn diagram of CRT targets and IgAN. (C) Visual analysis of CRT-IGAN (Betweenness: 66.61; Closeness: 0.0062; Degree: 39.31). (D) GO enrichment analysis of potential targets of CRT intervention in IgAN (BP, CC and MF analysis/Triad diagram of BP, CC and MF). (E) KEGG enrichment analysis of potential targets of CRT intervention in IgAN. |
 |
Figure 9 Bioinformatics analysis of T2DM related-CKD. (A) CRT-components-target network diagram. (B) Venn diagram of CRT targets and T2DM related-CKD. (C) Visual analysis of T2DM related-CKD. (Betweenness: 66.61; Closeness: 0.0062; Degree: 39.31). (D) GO enrichment analysis of potential targets of CRT intervention in T2DM related-CKD (BP, CC and MF analysis/Triad diagram of BP, CC and MF). (E) KEGG enrichment analysis of potential targets of CRT intervention in T2DM related-CKD. |
 |
Figure 10 Bioinformatics analysis of MN. (A) CRT-components-target network diagram. (B) Venn diagram of CRT targets and MN. (C) Visual analysis of CRT-MN. (Betweenness: 137.03; Closeness: 0.0033; Degree: 47.7). (D) GO enrichment analysis of potential targets of CRT intervention in MN (BP, CC and MF analysis/Triad diagram of BP, CC and MF). (E) KEGG enrichment analysis of potential targets of CRT intervention in MN. |
Disease targets were collected in GeneCards, OMIM and TTD databases. Disease targets were crossed with CRT targets, and Venn diagram was drawn. Ultimately, 101 common targets of CRT-IGAN were identified (Figure 8B), while 175 CRT-MN common targets and 183 CRT-T2DM related-CKD common targets were obtained (Figure 9–10B).
Core Target Screening
According to Degree, Closeness and Betweenness, a total of 27 IGAN, 34 MN and 38 T2DM related-CKD core targets were obtained and visually analyzed (Figure 8–10C). Ranked by Degree, top core targets of chronic glomerulopathy were interleukin 6 (IL-6), tumor necrosis factor (TNF), interleukin 1β (IL-1β), serine/threonine kinase 1 (AKT1), albumin (ALB) andγ-interferon (IFNG).
GO and KEGG Analysis
GO analysis revealed that core CRT-Chronic glomerulopathy targets were mainly involved in biological processes (BP) such as cell proliferation and migration, positive regulation of MAP kinase activity, and inflammatory response. It is mainly localized on the cellular component (CC) such as the extracellular matrix, membrane raft, plasma membrane, cell surface and exosome. The main molecular functions (MF) involve protein/phosphatase/enzyme/ATP-binding and serine/threonine/tyrosine kinase activity (Figure 8–10D).
KEGG results suggested that CRT acts on similar signaling pathways in these three diseases, which mainly included tumor (prostate and pancreatic cancer), infection (parasite, virus and tuberculosis), metabolism (blood glucose and lipid), Th17 cell differentiation and C-type lectin signaling pathway (Figure 8–10E).
Molecular Docking
Molecular docking of the core components of CRT, triptolide, celastrol, L-Epicatechin, triptonide and wilforlide A were used with the top five core targets of the three diseases. We further validate the molecular targets selected by network pharmacology (Figure 11).
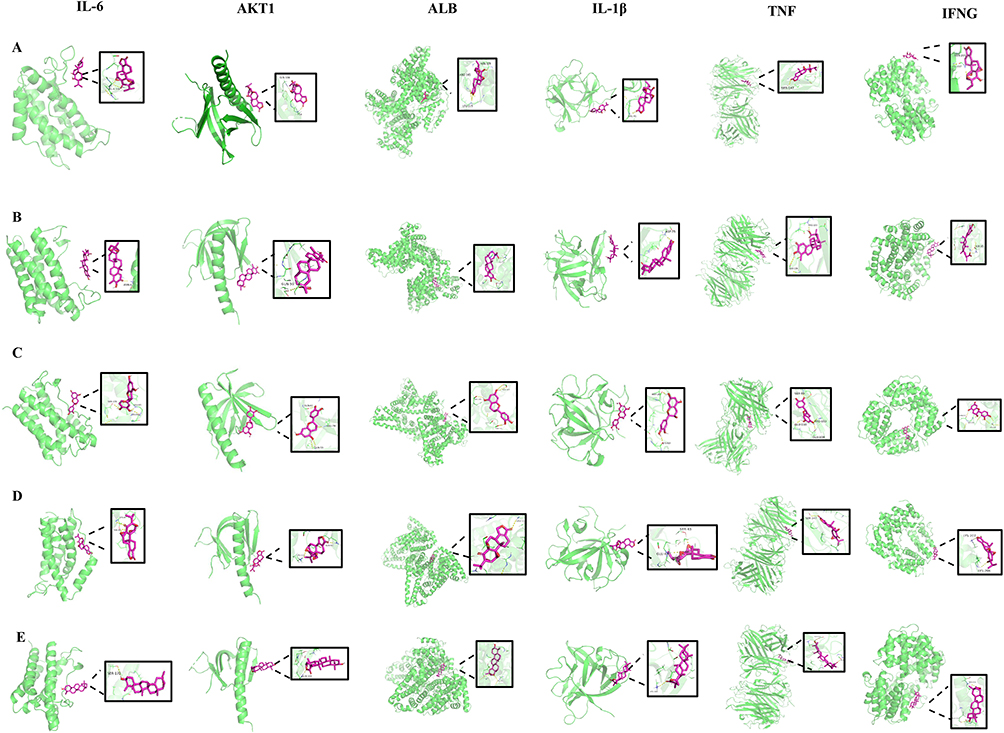 |
Figure 11 The molecular docking of CRT. (A) Molecular docking diagram of triptolide with the top five core targets of three diseases. (B) Molecular docking diagram of celastrol with the top five core targets of three diseases. (C) Molecular docking diagram of L-Epicatechin with the top five core targets of three diseases. (D) Molecular docking diagram of triptonide with the top five core targets of three diseases. (E) Molecular docking diagram of wilforlide A with the top five core targets of three diseases. |
Discussion
Presently, the researches on CRT for kidney disease are dominated by case reports and small sample studies. This real-world study collected 375 patients and analyzed 317 patients and is the largest sample size in China. This is a single-arm retrospective real-world study designed to investigate the efficacy and safety of CRT in the treatment of chronic glomerulopathy and to provide evidence for rational clinical use.
CRT can rapidly and effectively reduce proteinuria in patients of chronic glomerulopathy, especially in IgAN. Compared with baseline values, proteinuria decreased by up to 50% in IgAN and MN patients. Some patients showed a slight rebound of proteinuria in the second or third month, especially in T2DM-related CKD group while fewer fluctuations in IgAN. However, if CRT continues to be used, proteinuria still shows a downward trend. The mechanism of CRT reducing proteinuria has not been fully defined. Some studies have suggested the active components of CRT, such as triptolide and celastrol, help to protect and repair glomerular charge and mechanical barrier,5,6 inhibit T cell immunity,7 induce apoptosis of peripheral blood monocytes and influence Th17 cell differentiation,8 reduce podocytes injury. In addition, the anti-inflammatory effect of CRT does not depend on the pituitary-adrenal-axis, and will not cause obvious rebound phenomenon compared with other anti-inflammatory agents. Long-term use has little damage to the immune system.9
CRT had little effect on serum creatinine. A small number of patients had a slight and transient increase in creatinine levels, particularly in some T2DM-related CKD patients, but they were not statistically significant (data not presented). Elevated creatinine levels were related to the dose and duration of CRT. The increase in creatinine may be affected by alkaloid components of CRT, which can induce renal tubular hypoxic damage and renal interstitial injury.10 Compared with TWHFs, CRT uses aqueous decoction, which has a lower content of alkaloids inducing less nephrotoxicity.11
TWHFs and other THHs (such as Kunxian capsules), have been reported to cause a decrease of serum albumin in patients with kidney diseases. The exact mechanism is still unclear and may be correlated with the inhibition of liver albumin synthesis.12,13 Figure 1C suggested that there was no significant reduction in albumin levels after CRT treatment, which may be related to the reduction of proteinuria and lower hepatotoxicity of CRT.
Subgroup analysis explored the efficacy of CRT in different proteinuria and eGFR levels.14–16 Figure 6A indicated that regardless of heavy (>3500 mg/d), moderate (1500 to 3500 mg/d), and mild (≤1500 mg/d) proteinuria, CRT treatment demonstrated a favorable effect with no statistically significant among three subgroups (Figure 6B). This means that CRT is effective regardless proteinuria levels, which differs from the other two novel proteinuria-lowering drugs, finerenone and dapagliflozin. Finerenone (a novel, selective, nonsteroidal mineralocorticoid receptor antagonist) had a more pronounced effect on heavy proteinuria compared with moderate proteinuria.17 Dapagliflozin, a sodium glucose cotransporter 2 inhibitors (SGLT2i), had a better therapeutic influence on patients with moderate to heavy proteinuria.18 The mechanics are also unknown. The insufficient sample sizes in subgroup analyses may limit the statistical power. To mitigate this, we have conducted a post-hoc power analysis for these subgroups and found that while the relatively small sample sizes affect the power, the observed effects are still directionally consistent with our hypotheses.
Non-dialysis patients with CKD stage 1–5 were included in this research. Regardless of eGFR levels (>or≤60 mL/min/1.73m2), CRT showed great treatment effects without statistically significant between subgroups (Figure 6C and D). It is similar to the research results of empagliflozin (another SGLT2i).18 To date, there is no subgroup analysis of eGFR for finerenone.19
CRT had little myelosuppressive effect without significant decrease in WBC and PLT. Triptolide is an important active ingredient of CRT for its proteinuria-lowering effect, but it also has side effects, such as obvious cytotoxic effect on hematopoietic stem cells.20 The effect of CRT on transaminase was also minimal. After CRT treatment, 6.8% patients showed transaminase levels higher than ULN, but only 1.1% more than 1 time of ULN required close monitoring, and 1 case more than 3 times of ULN needed drug withdrawal. Mildly elevated transaminase can be alleviated by combining liver-protective drugs or reducing the dose of CRT. The hepatotoxicity of CRT was significantly lower than TWHFs, which may be related to less alkaloid content. And the metabolism of CRT in the liver can lead to direct damage to hepatocytes.21
In addition, the inhibitory effect of CRT on gonads should also be vigilant. Although statistical analysis was not performed due to the large number of missing data, the incidence of gonadal suppression was obvious in reproductive patients through clinical observation. The main manifestations of gonadal suppression in women were reduced menstruation, menstrual cycle prolongation and amenorrhea with increased menstrual volume and shortened menstrual interval in very few patients. For men, gonadal suppression was manifested as reduced sperm quantity and quality, causing infertility. However, there are individual differences in gonadal suppression. In most patients, gonadal suppression was reversible after discontinuation of CRT, and the recovery time was positively correlated with the duration and dose of CRT. Therefore, CRT is not recommended as the first choice for patients with reproductive needs.22 Gonadal suppression may be related to triptolide, which has reproductive toxicity and can reduce the synthesis of estrogen and progesterone and reproductive function.20,23
CRT has been treated skin diseases such as psoriasis, neurodermatitis, hormone-dependent dermatitis, and vasculitis due to its anti-immune effect.24 However, it can also cause skin allergic reactions, manifested as skin erosions, ulcers, and nodular erythema.13 But the incidence is low and mild cases are followed up for observation, and severe rashes need to be discontinued. Rashes only occurring in 0.95% patients in this study, which may be related to the mechanism of immune response, drug toxicity and accumulation in the body.25 The most common adverse reactions of TWHFs are gastrointestinal reactions, such as nausea, vomiting, abdominal pain and diarrhea. This is mainly due to the irritation of triptolide on the gastrointestinal tract, causing smooth muscle spasticity. CRT contains lower levels of triptolide, the symptoms are mild and resolve spontaneously. Therefore, CRT is relatively safe, and its overall toxicity is lower than TWHFs.26
Real-world studies have confirmed the effectiveness and safety of CRT treatment for chronic glomerulopathy, especially in IgAN, T2DM-related CKD and MN, with significant therapeutic effects. However, the mechanism of action and therapeutic targets of CRT remain unclear. This study further explored the possible molecular mechanisms of CRT intervention in IgAN, T2DM-related CKD and MN based on network pharmacology and molecular docking techniques. Firstly, the core targets were obtained by intersection of CRT targets and disease targets, followed by bioinformatics analysis and finally validated by molecular docking technology. Integrated bioinformatics analysis suggested that CRT treated three diseases through similar core targets and signaling pathways. Core targets were centered on IL-6, TNF, and IL-1 β, AKT1, ALB and IFNG. Signaling pathways mainly enriched in tumor (prostate cancer and pancreatic cancer), infection (parasites, viruses and tuberculosis), metabolism (blood glucose and lipids), Th17 cell differentiation and C-type lectin signaling pathway. Active components of CRT had good combination with core targets.
T cell dysregulation has been reported to contribute to the pathogenesis of IgAN, MN and T2DM-related CKD, of which Th17/regulatory T (Treg) imbalance has emerged as a prominent factor.27–29 Th17 cells are pro-inflammatory immune cells while Treg cells and Th17 cells are two subsets with opposite actions.30,31 Decreased number of Treg cells and increased Th17 cells were observed in IgAN, T2DM-related CKD, and MN, and were positively correlated with disease severity.27,29,32 However, how CRT affects Th17/Treg balance and related signaling pathways in these three diseases remains unclear.
C-type lectins are a superfamily of proteins that recognize ligands and regulate various physiological functions, playing an important role in autoimmune diseases.33,34 For instance, mannose-binding lectin (MBL) protein belonging to C-type lectin receptors, and is the main protein in the lectin pathway, which is one of the important pathways for activating the complement system. Studies have showed that the MBL pathway leading to excessive complement activation can be involved in the pathogenesis of three diseases.35–37 Autoantibodies reactive to kidney-expressed self-antigens and/or antibody/antigen complexes deposited in the kidney can activate plasma complement through the MBL pathway, which triggers a cascade of inflammation. Mincle, another C-type lectin receptor, is expressed mainly on membrane of macrophage and plays a key role in inflammatory response of macrophage. Suppression of Mincle and Mincle-maintained M1 macrophage polarization is a potential target for DKD.38 However, the role of Mincle in IgAN and MN remains unclear. The network pharmacology results of this study also suggest that the therapeutic effect of CRT may involve regulating Th17 cell differentiation and the C-type lectin signaling pathway, but the specific mechanism is still unclear and requires further basic research to clarify, including cell experiments and animal experiments.
While this study provides significant evidence for the efficacy and safety of CRT in chronic glomerulopathy, there are areas where further research is essential. The lack of a control group in this study suggests a need for future trials to include a control arm to more definitively attribute treatment effects to CRT. Additionally, larger sample sizes in subgroup analyses will be crucial to increase the statistical power and confirm the broad applicability of CRT across different patient populations. The retrospective nature of this study also points to the need for prospective studies to validate our findings and to minimize potential biases. Future research should also focus on longer-term follow-ups to assess the durability of CRT’s effects and to monitor for any late-onset adverse effects. Moreover, the potential mechanisms of CRT’s action, as suggested by our molecular docking and network pharmacology analysis, warrant further exploration. Basic research, including cell and animal studies, will be instrumental in elucidating the precise pathways through which CRT reduces proteinuria and its impact on kidney disease progression.
Conclusion
CRT treatment for chronic glomerulopathy is safe and effective, especially in IgAN, MN and T2DM-related CKD patients, which can significantly reduce proteinuria and without obvious effect on blood creatinine and albumin. The side effects incidence of liver injury and gastrointestinal reactions is low. However, it is important to be vigilant of its suppression on the gonads and use with caution for childbearing age patients. The network pharmacology results suggest that the mechanism of action of CRT in treating chronic glomerulopathy may involve Th17 cell differentiation and the CLR signaling pathway, which requires further research to verify.
Data Sharing Statement
Data provided upon request.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Ethics Committee of Wuhan Union Hospital and complied with the Declaration of Helsinki. All patients were informed that consent to participate in the study and publish their data would be assumed on completion and submission of the study survey.
Acknowledgment
This work was supported by grants from the National Natural Science Foundation of China (No.81770736).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No.81770736).
Disclosure
The authors declare that they have no competing interests.
References
1. Sun Y, Wang J, Hu P, et al. Molecular mechanism through which Tripterygium hypoglaucum (Lévl.) Hutch alleviates psoriasis. Biomed Pharmacothe. 2024;181:117647. doi:10.1016/j.biopha.2024.117647
2. He H, Takahashi A, Mukai T, et al. the immunomodulatory effect of triptolide on mesenchymal stromal cells. Front Immunol. 2021;12:686356. doi:10.3389/fimmu.2021.686356
3. Zhu KJ, Shen QY, Cheng H, Mao XH, Lao LM, Hao GL. Triptolide affects the differentiation, maturation and function of human dendritic cells. Int Immunopharmacol. 2005;5(9):1415–1426. doi:10.1016/j.intimp.2005.03.020
4. Jiang X, Huang XC, Ao L, et al. Total alkaloids of Tripterygium hypoglaucum (levl.) Hutch inhibits tumor growth both in vitro and in vivo. J Ethnopharmacol. 2014;151(1):292–298. doi:10.1016/j.jep.2013.10.045
5. Wang Y, Zhou M, Yu R. Reevaluation of systematic evaluation of Tripterygium glycosides in the treatment of diabetic kidney disease. China Pharm. 2023;34(23):2915–2921.
6. Gu Z. Mechanism and case analysis of multi-glycosides of Tripterygium wilfordii hook. in the treatment of renal proteinuria. Chinese J Integr Traditional and Western Nephrol. 2008;(08):744–745.
7. Zhou R, Li X, Yang Y. Effect of tripterygium glycosides on vascular endothelial function and T lymphocyte subsets in patients with early diabetic nephropathy. World Chin Med. 2017;12(08):1840–1843.
8. He M, Zhang X, Peng A, et al. Triptolide inhibits the differentiation of Th17 cells induced by inflammatory monocytes. J Pra Med. 2015;31(11):1763–1766.
9. Zhong J, Xian D, Xu Y, Liu J. Efficacy of Tripterygium hypoglaucum Hutch in adults with chronic urticaria. J Altern Complement Med. 2011;17(5):459–464. doi:10.1089/acm.2009.0648
10. Wu F, Wei L. Inhibition of renal interstitial fibrosis by mulberry leaf alkaloids in rats with diabetic nephropathy. J Clin Nephrol. 2022;22(08):666–673.
11. Wang K, Mao X, Zhang Y, et al. In vitro ”benefit-risk” evaluation and network regulation mechanism of colquhounia root tablets and its key material basis. China J Chinese Materia Medica. 2022;47(23):6438–6449. doi:10.19540/j.cnki.cjcmm.20221010.401
12. Xing H, Li X, Ren Y, Zhang M, Yan M, Yang Z. Reflection and experience on the treatment of idiopathic membranous nephropathy with Kunxian capsules. Chinese J Integr Traditional and Western Nephrol. 2020;21(05):436–437.
13. Li L, Xu X. Literature investigation and analysis of 294 adverse reactions of Tripterygium. Shanxi Med J. 2011;40(01):88–90.
14. Xu C. Colquhounia root tablet in the treatment of idiopathic membranous nephropathy with sub-nephrotic proteinuria. Inter Urol Nephrol 2023;56(2):699–706. https://link.cnki.net/doi/10.27652/d.cnki.gzyku.2023.001185.
15. Li M. Analysis of 70 clinical cases of massive proteinuria of diabetic nephropathy under the treatment of Huoba Huagen tablets. Chin J Hospital Pharm. 2014;34(20):1762–1764. doi:10.13286/j.cnki.chinhosppharmacyj.2014.20.17
16. Xu C, Xu T, Liu N, et al. Colquhounia root tablet in the treatment of idiopathic membranous nephropathy with subnephrotic proteinuria. Inter Urol Nephrol. 2024;56(2):699–706. doi:10.1007/s11255-023-03682-2
17. Ruilope LM, Pitt B, Anker SD, et al. Kidney outcomes with finerenone: an analysis from the FIGARO-DKD study. Nephrol Dial Transplant. 2023;38(2):372–383. doi:10.1093/ndt/gfac157
18. Mosenzon O, Wiviott SD, Heerspink HJL, et al. The effect of dapagliflozin on albuminuria in DECLARE-TIMI 58. Diabetes Care. 2021;44(8):1805–1815. doi:10.2337/dc21-0076
19. Bramlage P, Lanzinger S, Mühldorfer S, et al. An analysis of DPV and DIVE registry patients with chronic kidney disease according to the finerenone Phase III clinical trial selection criteria. Cardiovasc Diabetol. 2023;22(1):108. doi:10.1186/s12933-023-01840-5
20. Song X, Gao C. Progress on pharmacology, toxicity and attenuated strategies of Tripterygium wilfordii. J Gannan Medl Univ. 2023;43(10):
21. Ding Y. Overview of side reactions to Tripterygium wilfordii poison. Res Tradit Chin Med. 1994;(03):
22. Du W, Zhang L, Song X, Chen H, Mei X, Wang T. Preliminary study on testicular toxicity of huobahuagen hablets by network pharmacology and animal experiment. J Toxicol. 2022;36(05):408–413. doi:10.16421/j.cnki.1002-3127.2022.05.014
23. Tang Y, Wang J, Cheng J, Wang L. Antiestrogenic activity of triptolide in human breast cancer cells MCF-7 and immature female mouse. Drug Dev. Res. 2017;78(3–4):164–169. doi:10.1002/ddr.21387
24. Han X, Li T, Wang Q. The clinical application of colquhounia root tablet in dermatology. Chin J Integr Med Tradit Western Med. 2022;21(04):357–360.
25. Dou Z, Liu Y. Mucocutaneous adverse reaction of tripterygium wilfordii and its prevention and treatment. Lishizhen Medicine and Materia Medica Res. 1998;(4):8.
26. Fan X, Chen Y, Li X. Investigation of adverse reactions caused by Tripterygium wilfordii Hook. f in patients with immune diseases. Chinese J Integr Traditional and Western Nephrol. 2001;02:83–85.
27. Du W, Gao CY, You X, et al. Increased proportion of follicular helper T cells is associated with B cell activation and disease severity in IgA nephropathy. Front Immunol. 2022;13:901465. doi:10.3389/fimmu.2022.901465
28. Cremoni M, Brglez V, Perez S, et al. Th17-immune response in patients with membranous nephropathy is associated with thrombosis and relapses. Front Immunol. 2020;11:574997. doi:10.3389/fimmu.2020.574997
29. Wang D, Zhang Q, Dong W, et al. SGLT2 knockdown restores the Th17/Treg balance and suppresses diabetic nephropathy in db/db mice by regulating SGK1 via Na(). mol Cell Endocrinol. 2024;584:112156. doi:10.1016/j.mce.2024.112156
30. Liu C, Yang H, Shi W, Wang T, Ruan Q. MicroRNA-mediated regulation of T helper type 17/regulatory T-cell balance in autoimmune disease. Immunology. 2018;155(4):427–434. doi:10.1111/imm.12994
31. Chen Q, Kim YC, Laurence A, Punkosdy GA, Shevach EM. IL-2 controls the stability of Foxp3 expression in TGF-beta-induced Foxp3+ T cells in vivo. J Immunol. 2011;186(11):6329–6337. doi:10.4049/jimmunol.1100061
32. Motavalli R, Etemadi J, Soltani-Zangbar MS, et al. Altered Th17/Treg ratio as a possible mechanism in pathogenesis of idiopathic membranous nephropathy. Cytokine. 2021;141:155452. doi:10.1016/j.cyto.2021.155452
33. Brown GD, Willment JA, Whitehead L. C-type lectins in immunity and homeostasis. Nat Rev Immunol. 2018;18(6):374–389. doi:10.1038/s41577-018-0004-8
34. Drouin M, Saenz J, Chiffoleau E. C-type lectin-like receptors: head or tail in cell death immunity. Front Immunol. 2020;11:251. doi:10.3389/fimmu.2020.00251
35. Wang Z, Xie X, Li J, et al. Complement activation is associated with crescents in IgA nephropathy. Front Immunol. 2021;12:676919. doi:10.3389/fimmu.2021.676919
36. Byf S, Chan GCW, Yap DYH, Chan TM. The role of the complement system in primary membranous nephropathy: a narrative review in the era of new therapeutic targets. Front Immunol. 2022;13:1009864. doi:10.3389/fimmu.2022.1009864
37. Li XQ, Chang DY, Chen M, Zhao MH. Complement activation in patients with diabetic nephropathy. Diabetes Metab. 2019;45(3):248–253. doi:10.1016/j.diabet.2018.04.001
38. Lin X, Lei XQ, Yang JK, et al. Astragalus mongholicus Bunge and Panax notoginseng formula (A&P) improves renal mesangial cell damage in diabetic nephropathy by inhibiting the inflammatory response of infiltrated macrophages. BMC Complement Med Therap. 2022;22(1):17. doi:10.1186/s12906-021-03477-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anti-Inflammatory Effects and Molecular Mechanisms of Shenmai Injection in Treating Acute Pancreatitis: Network Pharmacology Analysis and Experimental Verification
He Y, Hu C, Liu S, Xu M, Liang G, Du D, Liu T, Cai F, Chen Z, Tan Q, Deng L, Xia Q
Drug Design, Development and Therapy 2022, 16:2479-2495
Published Date: 2 August 2022
A Novel Approach Based on Gut Microbiota Analysis and Network Pharmacology to Explain the Mechanisms of Action of Cichorium intybus L. Formula in the Improvement of Hyperuricemic Nephropathy in Rats

Amatjan M, Li N, He P, Zhang B, Mai X, Jiang Q, Xie H, Shao X
Drug Design, Development and Therapy 2023, 17:107-128
Published Date: 20 January 2023
Network Pharmacology and Experimental Validation to Explore That Celastrol Targeting PTEN is the Potential Mechanism of Tripterygium wilfordii (Lév.) Hutch Against IgA Nephropathy

Zhao J, Liu H, Xia M, Chen Q, Wan L, Leng B, Tang C, Chen G, Liu Y, Zhang L, Liu H
Drug Design, Development and Therapy 2023, 17:887-900
Published Date: 23 March 2023
Investigating the Mechanism of Action of Schisandra chinensis Combined with Coenzyme Q10 in the Treatment of Heart Failure Based on PI3K-AKT Pathway

Wen S, Yang K, Bai Y, Wu Y, Liu D, Wu X, Zhang X, Sun J
Drug Design, Development and Therapy 2023, 17:939-957
Published Date: 27 March 2023
Network Pharmacology Analysis of the Mechanisms Underlying the Therapeutic Effects of Yangjing Zhongyu Tang on Thin Endometrium
Zhang L, Li H, Zhang L, Zu Z, Xu D, Zhang J
Drug Design, Development and Therapy 2023, 17:1805-1818
Published Date: 17 June 2023