")
Back to Journals » Journal of Pain Research » Volume 18
Efficacy and Safety of Non-Pharmacological Therapies for Primary Dysmenorrhea: A Network Meta-Analysis
Authors Liu J , Wang Y, Zhang J, Fan X, Chen H, Zuo G, Wang X , She Y
Received 17 October 2024
Accepted for publication 5 February 2025
Published 27 February 2025 Volume 2025:18 Pages 975—991
DOI https://doi.org/10.2147/JPR.S498184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael A Ueberall
Jun Liu,1,2,* Yu Wang,1,* Juncha Zhang,1,2 Xisheng Fan,1,2 Hao Chen,1 Guang Zuo,1 Xuesong Wang,1 Yanfen She1,2
1College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China; 2Hebei International Joint Research Center for Dominant Diseases in Chinese Medicine and Acupuncture, Hebei University of Chinese Medicine, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuesong Wang; Yanfen She, College of Acupuncture-Moxibustion and Tuina, Hebei University of Chinese Medicine, No. 3 Xingyuan Road, Shijiazhuang, Hebei, 050200, People’s Republic of China, Email [email protected]; [email protected]; [email protected]
Background: This network meta-analysis (NMA) aimed to explore the impact of Non-pharmacological therapies (NPT) on alleviating primary dysmenorrhea (PD) symptoms and assess the effectiveness differences among various NPT.
Methods: We searched seven databases and summarized clinical trials of PD treated with NPT from inception to September 6, 2023. Randomized controlled clinical trials (RCTs) of PD treated with NPT. The outcomes were the Visual Analog Scale (VAS), the Cox menstrual symptom scale (CMSS), and response rate. Quality was assessed using the Cochrane risk of bias assessment tool. Pairwise meta-analysis and network meta-analysis (NMA) was performed by RevMan (5.4), Stata (15.0), and WinBUGS (1.4.3). The ranking probabilities for all treatment interventions were performed using the Surface Under the Cumulative Ranking curve (SUCRA).
Results: A total of 16 RCTs were finally included, involving 8 kinds of NPT. Results of pairwise meta-analyses: For the VAS score results, moxibustion (SMD: − 0.591,95% CI: − 0.916, − 0.266) was more effective than acupuncture, acupuncture (SMD: − 0.948,95% CI: − 1.853, − 0.044) was more effective than placebo, and yoga (SMD: 2.634,95% CI: − 4.28, − 0.988) was more effective than the blank control. NMA results: Compared to the blank control, acupuncture (SMD: − 4.81; 95% CI: − 6.63, − 3.00), auricular point therapy (SMD: − 4.36; 95% CI: − 7.18, − 1.60), yoga (SMD: − 2.12; 95% CI: − 3.13, − 1.09), moxibustion (SMD:5.54; 95% CI: 3.33, 7.68), and placebo (SMD: 3.10; 95% CI: 1.03, 5.27) proved to be a superior reduction in VAS. The use of acupressure (SMD: 2.49; 95% CI: 0.03, 5.03), moxibustion (SMD: − 2.45; 95% CI: − 4.06, − 0.71), and acupuncture (SMD: − 1.72; 95% CI: − 2.75, − 0.56) demonstrated a greater decrease in VAS efficacy than placebo. The consolidated ranking outcomes indicate that moxibustion, acupuncture, and auricular acupoint therapy occupy high SUCRA positions across various outcome metrics.
Conclusion: Acupuncture, moxibustion and auricular point may be the best treatment for PD. In the future, more trials are needed to obtain higher-quality evidence and the best protocols.
Keywords: non-pharmacological therapies, acupuncture, primary dysmenorrhea, network meta-analysis, randomized controlled trials
Background
Primary dysmenorrhea (PD), also referred to as functional dysmenorrhea, is marked by cramping pain in the pelvic area during menstruation, often accompanied by dizziness, fatigue, vomiting, diarrhea, and other symptoms. In severe cases, it can lead to cold extremities and fainting. PD is not associated with any apparent pelvic organic disease.1 The prevalence of PD varies significantly across different regions and age groups, ranging from 31.6% to 89.1%. For instance, the prevalence of PD among female college students in China is 70.3%,2 while it is 45% in India,3 83.7% in Arabia,4 64.7% in Ethiopia,5 64.0% in Mexico,6 89.1% in Iran7 and 91.27% in Indonesian medical students.8 A Japanese study indicated that the prevalence of dysmenorrhea varies with age, being 31.6% at age 12, 39.5% at age 13, and 50.3% at age 14.9 These variations may be attributed to differences in ethnicity, socio-cultural factors, and PD assessment methods. Dysmenorrhea symptoms typically begin in adolescence, potentially leading to school absenteeism and limitations in social, academic, and physical activities.10 Prolonged dysmenorrhea can cause repression, depression, distress, and other negative emotions.11 These symptoms can affect their quality of life, which is why we are concerned about PD.
According to consensus guidelines1,12,13 and evidence reviews,14–17 nonsteroidal anti-inflammatory drugs (NSAIDs) are widely considered the primary treatment, with combined oral contraceptives often used as a secondary option.18–20 However, due to the potential long-term adverse effects on the cardiovascular, hepatic, and renal systems associated with NSAIDs17,19 these treatments are not suitable for prolonged use. Similarly, oral contraceptives can cause vaginal bleeding, weight gain, or venous thrombosis.21,22 All of this suggests that we need to move to Non-pharmacological therapies (NPT) that are safe and easy to use and effective in achieving relief for dysmenorrhea symptoms. NPT include acupuncture, exercise therapy, aromatherapy, acupressure, and so on.23 Recently, NPT yield remarkable efficacy in clinical practice, and are widely proved by previous research.24 Besides, several clinical studies and systematic reviews have also confirmed the efficacy and safety of NPT for PD.25–27 Recent studies suggest that NPT is a viable and effective treatment option for women with PD, particularly for those unsuitable for pharmacologic therapy.28–31
Even though NPT are widely used in PD, there is still a lack of comparison between different NPT. Previous research has mainly focused on single interventions and lacked comprehensive comparisons of multiple non-pharmacological therapeutic interventions.32–34 Given the wide variety of NPT with different efficacy focuses and the lack of studies directly comparing these treatments, this study aims to compare the efficacy of multiple NPT in PD patients using network meta-analysis (NMA) to synthesize evidence from both direct and indirect comparisons.35 This study aims to provide evidence-based medical findings and provide clinicians with a clear understanding of the efficacy of NPT, to help patients with PD choose the best treatment, and to provide researchers with potential avenues for future research design.
Methods
This research was based on the checklist of the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 and extension statement for network meta-analyses (PRISMA-NMA).36 (Appendix 1) Our analysis used an adapted PRISMA checklist, extending the original standard. This study is registered in PROSPERO under the registration number CRD42024493532.37
Search Strategy
To identify randomized controlled clinical trials (RCTs) evaluating NPT for PD, we conducted comprehensive searches in several databases, including China National Knowledge Infrastructure (CNKI), Wanfang Data (WF), China Science and Technology Journal Database (VIP), Chinese Biomedical Literature Database (CBM), Cochrane Library, PubMed, and Embase. The search covered the entire history of these databases, from their inception until September 6, 2023. The search methodology included a combination of Medical Subject Headings (MeSH) terms and free words. The MESH keywords included such as “acupuncture”, “moxibustion”, “non-pharmacological interventions”, “yoga”, “dysmenorrhea”, “acupressure”, “electroacupuncture”, “acupuncture,ear”, “Randomized Controlled Trials” and other related terms. The detailed search strategy is specified in Appendix 2.
Inclusion Criteria
(1) Our inclusion criteria consisted of published RCTs, without restrictions on the age of participants. (2) The 345-Primary Dysmenorrhea Consensus Guideline,12 issued by the Canadian Society of Obstetricians and Gynaecologists (SOGC), outlines the precise criteria for diagnosing PD. The criteria encompass: 1) menstrual pain absent of pelvic pathology, 2) typical onset in adolescence post-ovulation cycles, 3) typical crampy, suprapubic pain starting hours before or after menstruation, 4) peak symptoms characterized by intense flow and persisting for 2 to 3 days, 5) pain often colicky with a focus on the lower abdomen’s midline, though it can be mild and spread to the lumbar area or thighs, and 6) related symptoms like diarrhea, nausea, vomiting, fatigue, lightheadedness, headaches, dizziness, and occasionally syncope and fever. (3) NPT encompass moxibustion (MOX), yoga, acupressure, electroacupuncture (EA), acupuncture (ACU), and auricular point therapy (APT). (4) The control group consisted of either a blank control or rest for the same times at the school health center without treatment. During the study, the control group was advised to abstain from regular exercise, rest for 20 minutes at the school health center without treatment, or receive only a menstrual health education manual without interventions. (5) The placebo group underwent placebo acupuncture using a non-penetrating sham needle. (6) The study outcomes were evaluated using the response rate, the Visual Analog Scale (VAS), and the Cox menstrual symptom scale (CMSS). (7) The eligible publications were restricted to those published in Chinese or English.
Exclusion Criteria
(1) Repeatedly published literature; (2) Systematic Reviews, letters, Meta-Analysis, non-randomized controlled trials, self-controlled trials, and experimental studies; (3) Literature in which the diagnosis was made of polycystic ovary syndrome, endometriosis, uterine fibroids, or other gynecological problems confirmed by ultrasound and gynecological examination; (4) Literature in which the study subject suffers from psychiatric system disorders such as severe depression or anxiety disorders; (5) Literature in which the study subject suffers from concomitant life-threatening diseases such as neurological, cardiovascular, cerebrovascular, hepatic, renal, and hematopoietic disorders; (6) Literature in which the study subject is pregnant or lactating or preparing to become pregnant; (7) Literature that includes spaced out MOX, herbal, and western medicine interventions; (8) Studies that incorporated multiple interventions within the same cohort of subjects; (9) Research lacking definitive primary data, where the authors’ accessibility for data verification was unattainable.
Literature Screening and Data Extraction
To ensure the accuracy and consistency of literature screening and data extraction, we have two independent researchers (JL and YW) to conduct literature screening and data extraction, respectively, and cross-check them. In case of disagreement, we will reach a consensus through in-depth discussion, and if we still need clarification, a third researcher (XW) will be introduced to adjudicate. In the data extraction process, we used a unified data extraction form. The extracted content mainly included: (1) The compilation of the review involved collecting core information about the studies included, covering the research’s title, the name of the lead writer, and its publication year; (2) the fundamental traits of the participants in the study, encompassing comprehensive details like the number of samples and the ages of those in the intervention groups; (3) the specific content of the interventions, such as the intervention method, the frequency of implementation, and the duration of the course of treatment; (4) the factors related to the risk of bias evaluation, involving randomization method, allocation concealment, blinding, and the risk of bias; (5) Factors related to risk of bias evaluation, including randomization method, allocation concealment, blinding; (6) Conclusion indicators: VAS, CMSS, response rate.
Assessing the Likelihood of Bias in Studies on Inclusion
We followed the guidelines indicated in the Cochrane Handbook 6.438,39 to analyze the potential bias risks in the studied research by using the recommended bias risk assessment tool to evaluate the studies separately.
Use of Statistical Analysis
For our statistical analysis, we selected Review Manager (5.4), Stata (15.0), and WinBUGS (1.4.3). For data processing, we employed the Standardized Mean Difference (SMD) as a metric for numerical variables like VAS and CMSS scores. On the other hand, we employed the relative risk (RR) to analyze categorical variables, such as the response rate. We computed the disparity between the post-treatment and pre-treatment values for the numerical variable SMD. Regarding statistical processing, we initially conducted a traditional pairwise meta-analysis utilizing the RevMan software. To assess the level of variation among several RCTs, we employed the I-square (I²) test.40 If the I² value exceeded 50%, it suggested substantial heterogeneity, prompting us to use the random effects model. Conversely, if the I² value did not reach the significance level,41 we utilized the fixed effects model.
Furthermore, 95% confidence intervals (95% CI) of SMD and relative risk (RR) were used as effect sizes. Subsequently, we plotted the NMA evidence relationships using Stata 15.0 software to demonstrate the associations and strength of evidence between different studies. Afterward, we analyzed the necessary data for the NMA using the WinBugs 1.4.3 software. The Markov Chain Monte Carlo (MCMC) Bayesian inference technique was utilized in this procedure to derive posterior probability from prior probabilities and to estimate and justify hypotheses. In order to maintain the stability of the MCMC algorithm, we specified a total of 50,000 iterations when executing the WinBUGS program. The first 20,000 iterations were specifically designated for annealing, which helped eliminate any potential biases that may have been introduced by the initial values. When there is a closed loop, if the 95% CI of the inconsistency factor (if) is 0, then the direct and indirect evidence is consistent; otherwise, there is a possibility of inconsistent operation.42 Following the completion of data processing, we utilized Stata 15.0 once more to generate funnel plots. These plots were employed to evaluate the existence of small-sample effects in the studies that were included43 thus guaranteeing the dependability and consistency of the results. Finally, the cumulative area under the ranking curve (SUCRA) graphs were generated using Stata 15.0, allowing for the presentation of SUCRA ratings for each intervention. The SUCRA assessments precisely reflect the advantages and disadvantages of the treatment categories, providing a strong basis for our decision-making.
Results
Study Search and Description
The literature search identified a total of 7608 relevant studies. After deleting duplicate documents, the selected articles are 5737 remaining. After reading the title and abstract, there are 930 remaining. After reading the full text, the selected articles are 488 remaining. Further detailed full-text screening was conducted, with 472 studies excluded because they did not meet the established criteria. Therefore, the final screening included 16 RCTs.The final screening included 16 RCTs with a total of 1033 PD patients, of which 573 were Chinese patients. In Figure 1, this paper presents the findings of the literature screening process. Eight interventions, including MOX, yoga, acupressure, EA, ACU and APT, placebo, and control. All were two-arm trials. Baseline characteristics and details of NPT methods included in the study are shown in Table 1.
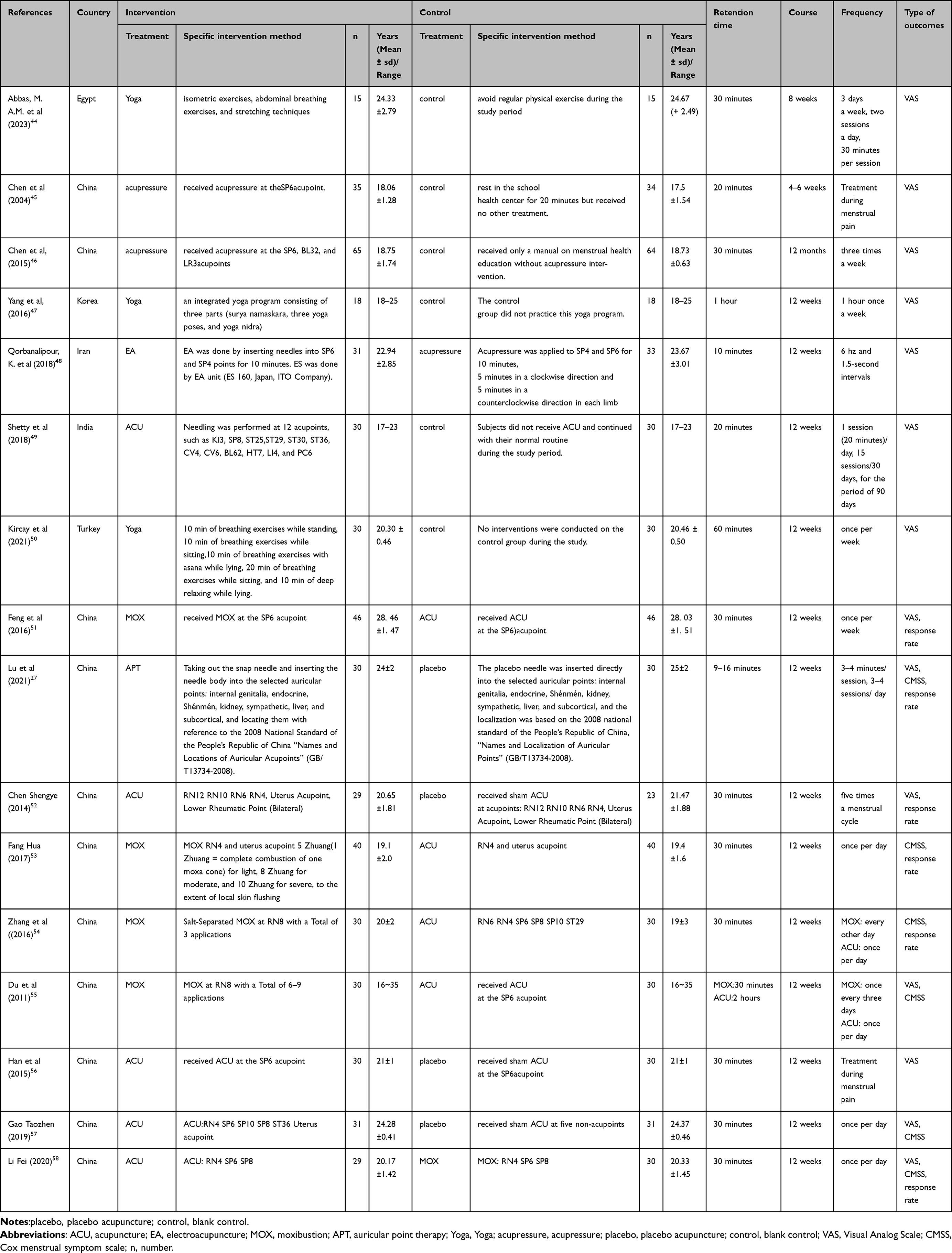 |
Table 1 Baseline Characteristics of the Included Studies and Descriptions of the Included Non-Pharmaceutical Therapy |
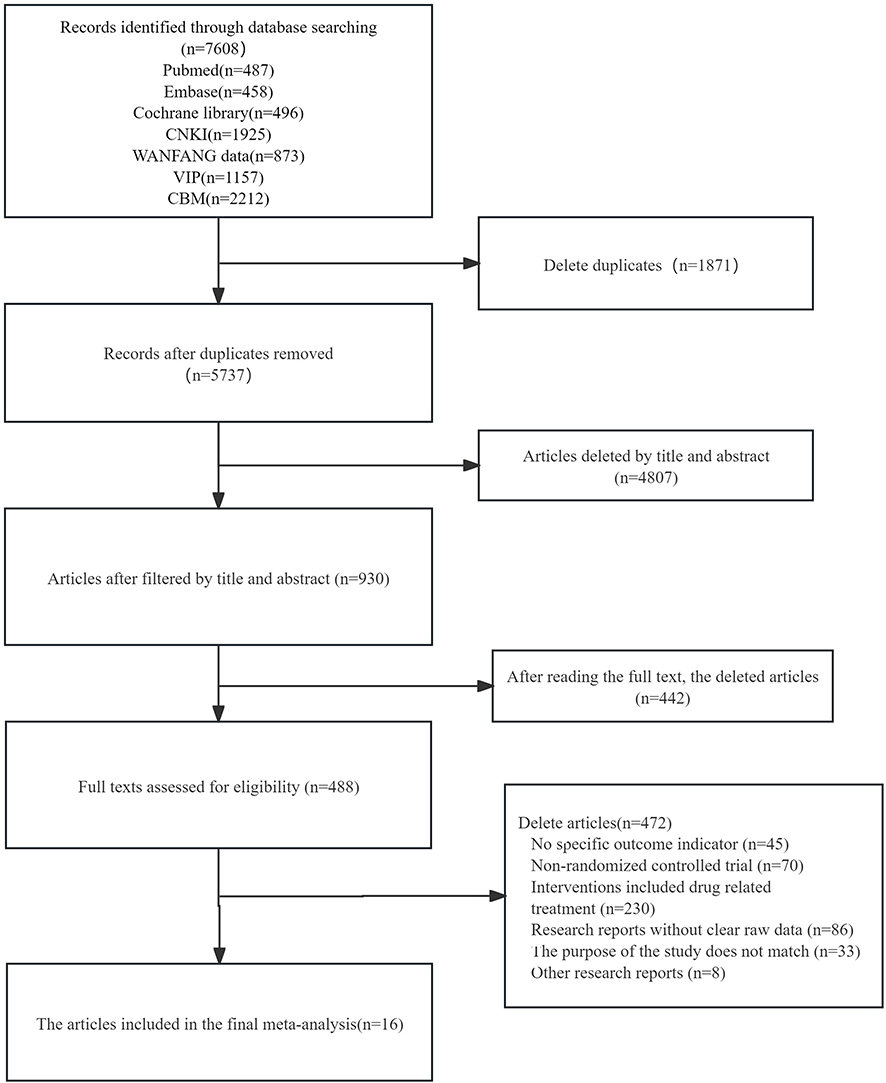 |
Figure 1 Study flow diagram. |
Quality Assessment of Included Studies
Two of our investigators (HC and GZ) independently assessed the risk of bias in the included studies, including seven items such as randomization method, allocation concealment method, and blinding method. Among the 16 RCTs included, 5 adopted the random number table method, 5 employed the computer-generated random number method, 3 utilized the central stratified block randomization method, and 1 employed the envelope random allocation method, all of which were rated as low risk. Two merely mentioned randomization without specifying the detailed scheme and were rated as unknown risk. Two mentioned double-blinding and both were rated as low risk; 3 mentioned single-blinding and all were rated as high risk. All the included literature had complete data and were rated as low risk. Selective outcome reporting and other bias risks were not mentioned and were all rated as unknown risk. The results of the risk assessment are shown in Figure 2.
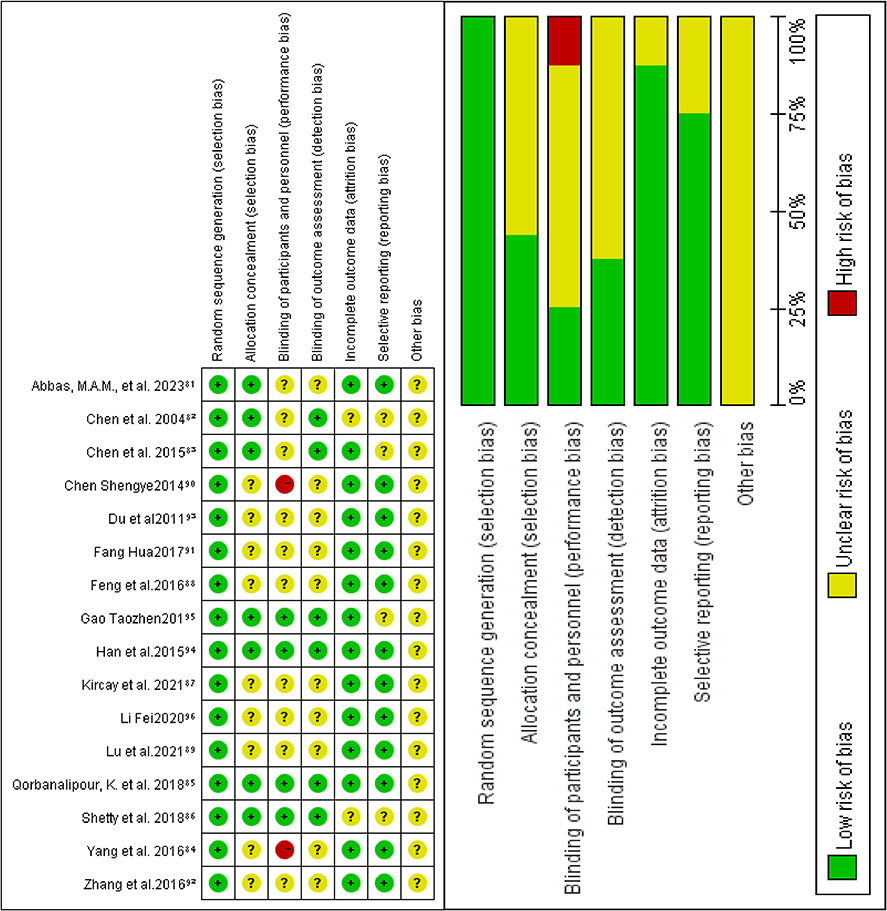 |
Figure 2 Quality assessment of included studies. |
Results of Pairwise Meta-Analyses
For the VAS score results, MOX (SMD: −0.591,95% CI: −0.916, −0.266) was more effective than ACU, ACU (SMD: −0.948,95% CI: −1.853, −0.044) was more effective than placebo, and yoga (SMD: 2.634,95% CI: −4.28, −0.988) was more effective than the blank control. For CMSS score results, MOX (SMD: −0.061,95% CI: −0.495,0.374) p=0.784 was not statistically different from ACU, and for response rate, MOX (RR: 0.871,95% CI: 0.311,2.239) p = 0.793 was not statistically different as compared to ACU (Table 2).
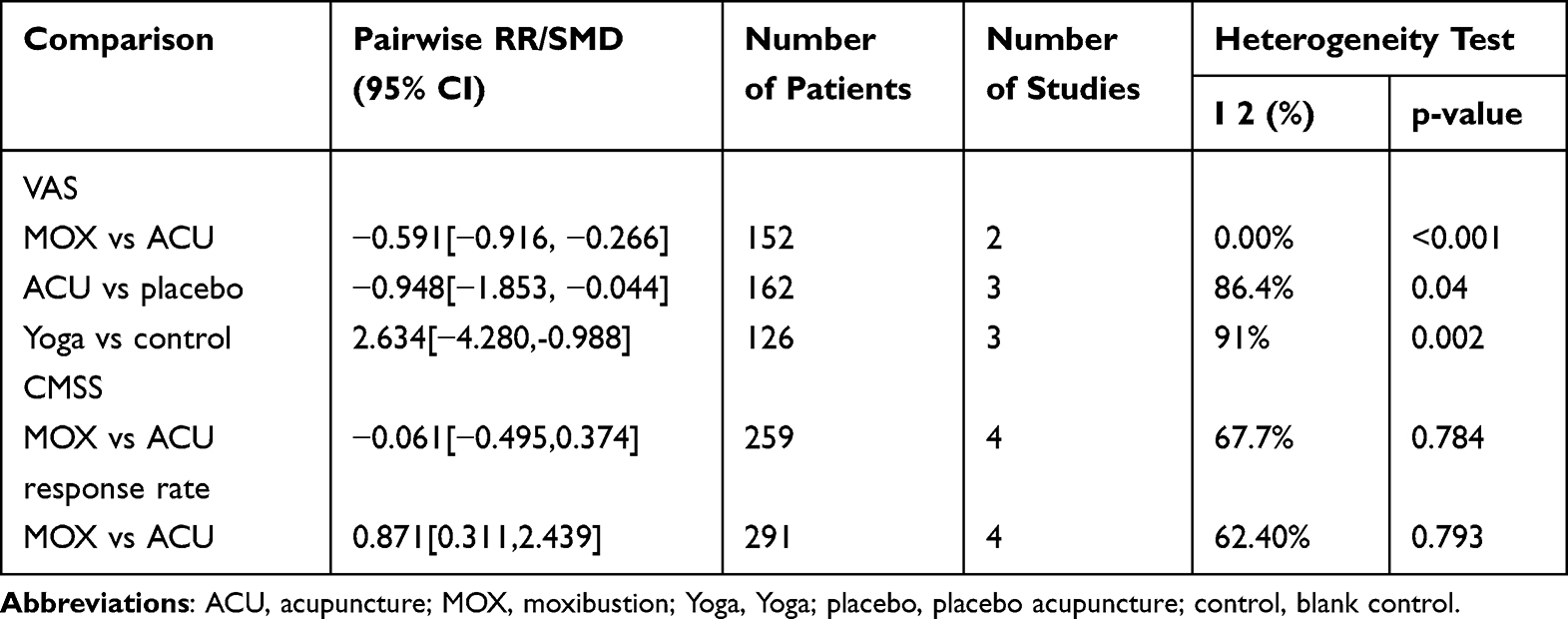 |
Table 2 Pairwise Meta-Analyses |
Network Meta-Analysis Results
Utilizing Stata 15.0 created three distinct network diagrams. The thickness of the connections between two points might indicate the strength or consistency of the connections. Thicker connecting lines may indicate more direct comparisons or connections between these two nodes. Circle size is positively correlated with the sample size of patients for the corresponding intervention. The size of the dots was positively correlated with the treatment sample size (Figure 3).
 |
Figure 3 The network structure for treatment comparisons. (A) VAS scores; (B) CMSS scores; (C) response rate. (ACU, acupuncture; EA, electroacupuncture; MOX, moxibustion; APT, auricular point therapy; Yoga, Yoga; acupressure, acupressure; placebo, placebo acupuncture; control, blank control). |
Primary Outcomes: VAS Scores and CMSS Scores
A total of 13 studies were identified that reported on VAS scores, involving eight distinct interventions and 834 patients. There were no closed loops or no inconsistency analyses. Compared to these methods: yoga (SMD: 3.42; 95% CI: 1.04, 5.79), acupressure (SMD: 4.94; 95% CI: 2.40, 7.50), and EA (SMD: 4.78; 95% CI 1.72, 7.90), MOX proved more beneficial. The NMA findings indicated acupuncture’s superior efficacy over these interventions in VAS: yoga (SMD: −2.69; 95% CI: −4.76, −0.62), acupressure (SMD: −4.20; 95% CI: −6.38, −1.94), EA (SMD: −4.06; 95% CI: −6.86, −1.24), placebo (SMD: −1.72; 95% CI: −2.75, −0.56), and blank control (SMD: -4.81; 95% CI: -6.63, −3.00). They all showed that ACU provided better relief of dysmenorrhea in PD patients (Table 3). The efficacy of APT surpasses these methods: acupressure (SMD: −3.76; 95% CI: −6.84, −0.77), EA (SMD: −3.59; 95% CI: −7.23, −0.18; Table 3), and blank control (SMD: −4.36; 95% CI −7.18, −1.60). The use of acupressure (SMD: 2.49; 95% CI: 0.03, 5.03), MOX (SMD: −2.45; 95% CI: −4.06, −0.71), and ACU (SMD: −1.72; 95% CI: −2.75, −0.56) demonstrated greater efficacy compared to placebo. Compared to the blank control, ACU (SMD: −4.81; 95% CI: −6.63, −3.00), APT (SMD: −4.36; 95% CI: −7.18, −1.60), yoga (SMD: −2.12; 95% CI: −3.13, −1.09), MOX (SMD: 5.54; 95% CI: 3.33, 7.68), and placebo (SMD: 3.10; 95% CI: 1.03, 5.27) proved to be superior in efficacy.
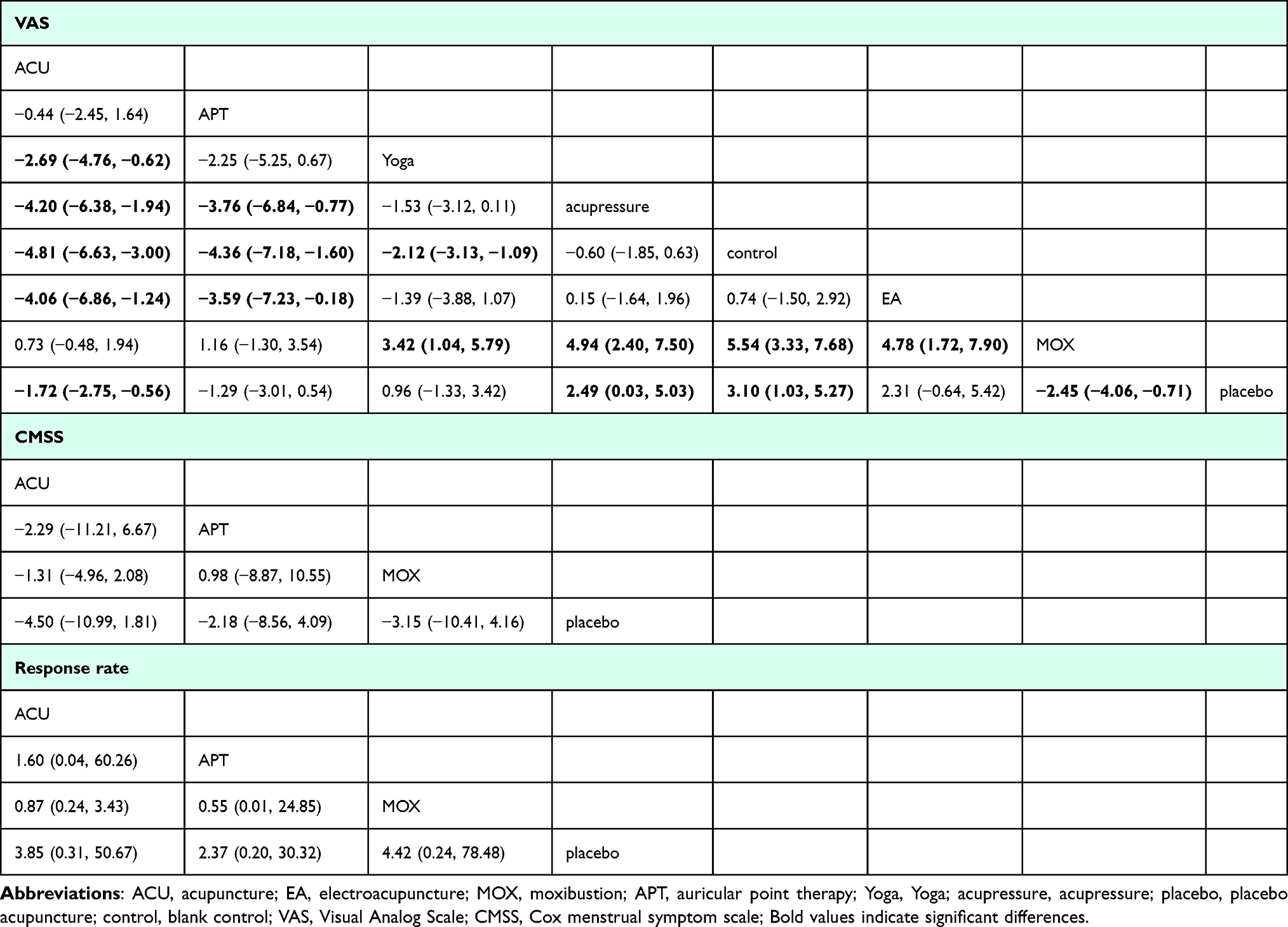 |
Table 3 Network Meta-Analysis Results |
Results ranked from the study revealed MOX (88%), ACU (75.5%), and APT (74.6%) as the top three methods to reduce VAS, with the control group having the most detrimental effects (12.1%; Figure 4A).
 |
Figure 4 Surface under the cumulative ranking curves. (A) VAS scores; (B) CMSS scores; (C) response rate; (ACU, acupuncture; EA, electroacupuncture; MOX, moxibustion; APT, auricular point therapy; Yoga, Yoga; acupressure, acupressure; placebo, placebo acupuncture; control, blank control). |
Six research papers presented CMSS scores over four different treatments involving 369 patients. There were no closed loops and no inconsistency analyses. The ranked data revealed that the leading trio of treatments lowering CMSS scores consisted of ACU (94.6%), MOX (71.5%), and APT (32.6%), as depicted in Figure 4B.
Secondary Outcomes: Response Rate
A total of 6 studies were identified that reported response rates involving four distinct interventions and 403 patients. Importantly, the study did not include any closed-loop or inconsistent evaluations. The ranking of interventions based on their ability to enhance the response rate revealed MOX (69.7%), ACU (61.3%), and APT (50.3%) as the top three, while placebo (18.8%) emerged as the least effective (as illustrated in Figure 4C). Examining the funnel plot uncovers an even spread of research across the vertical line X = 0, suggesting a low likelihood of bias in small sample sizes. Furthermore, Figure 5 illustrates a balanced distribution across the studies, thereby confirming the dependability of the findings and reducing the influence of effects from small samples.
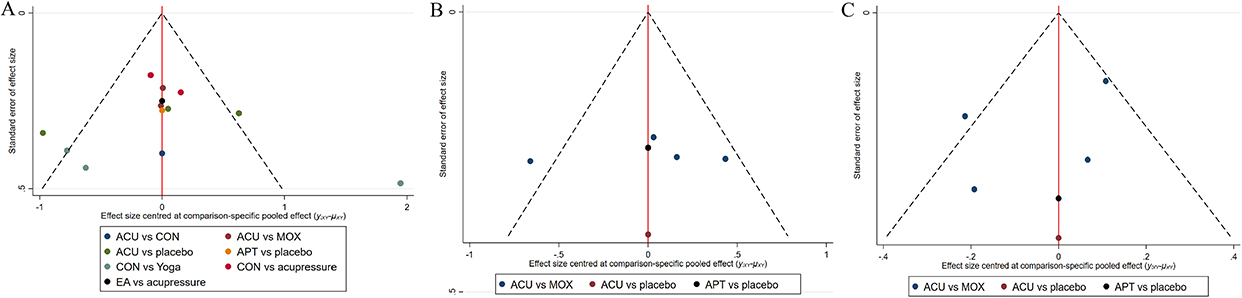 |
Figure 5 Funnel diagram. (A) VAS scores; (B) CMSS scores; (C) response rate; (ACU, acupuncture; EA, electroacupuncture; MOX, moxibustion; APT, auricular point therapy; Yoga, Yoga; acupressure, acupressure;placebo, placebo acupuncture; control, blank control). |
Adverse Events
Of the 16 RCTs included, 0 cases of adverse events were reported. Overall, studies on non-pharmacological interventions have indicated a low likelihood of adverse events, suggesting the safety of treatments related to NPT.
Discussion
In our network meta-analysis, a total of 16 RCTs involving 1033 patients with PD were included, evaluating eight different non-pharmacological interventions, with overall clinical effectiveness, VAS pain scores, and dysmenorrhea symptom scores as outcome indicators. The results of our study showed that: 1. the most commonly used intervention, except for control, was ACU, followed by MOX, and the least was APT; 2. the results of two-by-two meta-analysis showed that MOX was superior to ACU, ACU was superior to placebo, and Yoga was superior to control in improving VAS scores in patients with PD; however, the results of the NMA showed that MOX, ACU, and APT were all were superior to the blank control. Typically, MOX, APT, and ACU showed greater efficacy; 3. The ranking results revealed that MOX, ACU, and APT achieved higher SUCRA scores in different outcome metrics, suggesting their effectiveness in reducing dysmenorrheal pain in PD patients; 4. The findings on adverse events revealed no adverse events linked to NPT in the study’s literature, thereby further undermining the safety of such treatments.
PD is recognized as one of the most common functional disorders for gynecological counseling and one of the most common reasons for short-term absenteeism from school or work in both young and adult women.21 Despite extensive research, the pathological mechanisms of dysmenorrhea are not fully understood. Previous studies have shown that PD is a complex process that may depend on many factors14,59,60 Among them, the level of prostaglandin and uterine contractile activity are one of the factors leading to dysmenorrhea. PD is primarily treated to relieve pain and other related symptoms (such as back and leg pain, anxiety, stress, and other symptoms that affect quality of life).61,62 At present, pain VAS as a subjective way of assessing pain has been widely used to evaluate various pain disorders. Woodforde and Merskey first reported use of the VAS pain scale in patients presenting with a range of pain conditions.63 Therefore, we use the VAS as the primary outcome measure of NPT for PD. CMSS is developed by Daniel J. Cox in 1978, including 18 items, a more comprehensive summary of dysmenorrhea-related symptoms. For patients with PD, in addition to improving uterine pain, other clinically relevant symptoms are also more important. In the treatment of PD, CMSS can monitor the treatment effect very well.64 As the treatment progresses, the symptoms of dysmenorrhea in patients will change, and CMSS can capture these changes in a timely and sensitive manner. By the decrease of the total score of CMSS, it can be inferred that the treatment may be effective, and by analyzing the changes in the subitems, further understanding can be gained as to whether the degree of pain has decreased or whether accompanying symptoms have improved.65 A number of studies have shown66 that NPT are effective in improving related symptoms caused by PD.
MOX is an external therapeutic method originating from traditional Chinese medicine (TCM), which is based on TCM theories and usually uses burning moxa to stimulate acupuncture points. MOX has a history of more than 2,500 years with the advantages of simple operation and high cost-effectiveness.67 Studies have shown that qi stagnation, cold condensation, and blood stasis are prevalent in PD.68 The warm stimulation of moxibustion warms the meridians, activates the collateral branches, maintains the smooth flow of qi and blood, and relieves pain symptoms.69 MOX can regulate immune functions, endocrine hormones, and neural factors, and enhance uterine microcirculation to alleviate the symptoms of dysmenorrhea.70 MOX also alleviates menstrual pain in patients with PD in various ways,71–76 and a large number of studies confirm its efficacy and effectiveness. The results of this study show that MOX is superior to other NPTs in improving VAS scores in patients with PD, which further confirms the clinical guideline of “moxibustion in case of cold” in Chinese medicine theory.
ACU, a fundamental component of Chinese medicinal practices, boasts an extensive background in addressing gynecological issues. ACU, in contrast to medication, presents fewer adverse effects. ACU works by stimulating acupuncture points in specific parts of the body to unblock meridians and promote circulation of qi and blood.77,78 The Food and Drug Act has approved it. Modern studies have shown that acupuncture treatment for PD may be associated with improving uterine circulation disorders,79,80 regulating endocrine function,81 and affecting neurotransmitters.82–84 PD, as a common visceral pain condition, is also closely related to inflammatory factors. ACU could reduce the release of PGs and downstream inflammatory cytokines by regulating nuclear factor-κB (NF-κB) signaling pathway, further relieving the inflammatory environment of uterus and uterine ischemia and hypoxia to alleviate menstrual pain.85 Clinical studies have shown that ACU is more effective than NSAIDs in reducing the pain of PD.86 ACU is widely recognized as one of the best NPT for the treatment of PD. The results of this study showed that ACU was the most commonly used therapy among the eight NPT and was also more advantageous in improving VAS, CMSS, and overall clinical effectiveness of PD.
APT is a Chinese medicine method that regulates the body’s physiological and pathological states by stimulating specific acupoints on the auricle to treat disease or promote health.87–89 These auricular points are believed to be connected to various organs and parts of the body and can influence the function of the entire body through the reflex zones of the ear. APT originated in ancient Chinese medicine and has been documented in ancient texts such as the Yellow Emperor’s Classic of Internal Medicine. Over time, APT has evolved into an independent treatment system widely used and recognized. Modern medical research has also confirmed that APT can alleviate PD pain symptoms by activating and regulating the flow of qi and blood and reducing uterine tension and contraction.90 As reported previously, it can relieve pain and neuronal excitability through regulating proinflammatory cytokines, such as IL-1b, IL-6, and TNF.91 The results of the present study showed that APT ranked first in improving CMSS scores in treating PD.
Compared with previous studies,90,92–95 our study reaffirmed the advantages of ACU in improving the symptoms of primary dysmenorrheal pain, and that NPT, such as ACU, have a better safety profile compared with pharmacological therapies. However, we also found some discrepancies. For example, studies by Ukachukwu Okoroafor et al,96 Mike Armour et al,97 and Remedios López-Liria et al,34 found advantages of acupressure, self-care, and physical therapy (yoga) in relieving the symptoms of PD through meta-analysis, which may be at variance with the results of our study. In addition, a meta-analysis has shown that physical therapy and warm bath therapy are more effective at alleviating gynecological problems.98 These differences may be because all of these studies used the traditional two-by-two controlled meta-analysis method, which only allowed comparison of the two interventions included. In contrast, our study used a reticulated meta-analysis approach that allowed for simultaneous comparison of multiple treatments and allowed for indirect comparisons. Such an analytic approach made it possible to estimate the relative effect between treatments without direct comparison data. Additionally, NMA can provide an ordering of the best probabilities for the included interventions, thus providing a prioritization for medical decision-making. In summary, the use of NMA in this study to assess the effectiveness and ranking of all known NPT for treating PD may be more clinically recommendable than the conclusions drawn from previous studies.
However, this study still has some limitations: (1) the quality of the included studies was low, which may pose a risk of bias; the sample sizes of some of the interventions were small, and the statistical efficacy may be insufficient; (2) the methodological quality of all the RCTs was moderate, which may have stemmed from the difficulties of randomization and blinding. Due to the unique nature of NPT, it is difficult to practice double blindness in clinic; (3) the total clinical effectiveness was not used as the primary outcome indicator, which may have led to a biased result; (4) the majority of the included RCTs were conducted in China, which may reduce the generalizability of the findings; (5) In this study, the results did not form a closed loop, and the effect estimation was mainly based on indirect comparison, which may affect the robustness of the results to some extent.
Conclusion
In summary, this study’s evidence suggests that compared to placebo and no treatment, non-pharmacological therapy can reduce the severity of primary dysmenorrhea in patients. Among them, acupuncture, moxibustion, and auricular point therapy may be the best treatments for improving symptoms associated with primary dysmenorrhea. Indeed, future large, well-designed randomized controlled trials, extensive follow-up and better methodological quality are needed in the future to summarize and update the results of this analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Hebei Administration of Traditional Chinese Medicine (NO.2022091), the National Natural Science Foundation of China (Nos. 81973755, 82474395) and the Hebei Province Yan Zhao Golden Talent Platform Key Talent Program (HJZD202505).
Disclosure
The authors state that they have no known competing financial interests or personal relationships that could influence the work reported in this article.
References
1. ACOG Committee Opinion No. 760: dysmenorrhea and endometriosis in the adolescent. Obstet Gynecol. 2018;132(6):e249–e258. doi:10.1097/AOG.0000000000002978
2. Liu J, Wang Y, Wu L, Wang L, Fang H. Study on the influencing factors of primary dysmenorrhea in female college students: systematic review and meta-analysis. Medicine (Baltimore). 2024;103(49):e40906. doi:10.1097/MD.0000000000040906
3. Maitri S, Anuradha M, Sangita P, Malay S, Harsh B. A study of prevalence of primary dysmenorrhea in young students-A cross-sectional study. Healthline, J Ind Assoc Prevent Soc Med. 2013;4(2):30–34.
4. Katib Y, Almehmadi M, Alhajaji F, et al. Prevalence of primary dysmenorrhea and its effect on the quality of life among female students at umm Al-Qura University. Cureus. 2024;16(10):e72136. doi:10.7759/cureus.72136
5. Azagew AW, Kassie DG, Walle TA. Prevalence of primary dysmenorrhea, its intensity, impact and associated factors among female students’ at Gondar town preparatory school, Northwest Ethiopia. BMC Women's Health. 2020;20(1):5. doi:10.1186/s12905-019-0873-4
6. Ortiz MI. Primary dysmenorrhea among Mexican university students: prevalence, impact and treatment. Eur J Obstet Gynecol Reprod Biol. 2010;152(1):73–77. doi:10.1016/j.ejogrb.2010.04.015
7. Habibi N, Huang MSL, Gan WY, Zulida R, Safavi SM. Prevalence of primary dysmenorrhea and factors associated with its intensity among undergraduate students: a cross-sectional study. Pain Manag Nurs. 2015;16(6):855–861. doi:10.1016/j.pmn.2015.07.001
8. Situmorang H, Sutanto RL, Tjoa K, Rivaldo R, Adrian M. Prevalence and risk factors of primary dysmenorrhoea among medical students: a cross-sectional survey in Indonesia. BMJ Open. 2024;14(10):e086052. doi:10.1136/bmjopen-2024-086052
9. Kazama M, Maruyama K, Nakamura K. Prevalence of dysmenorrhea and its correlating lifestyle factors in Japanese female junior high school students. Tohoku J Exp Med. 2015;236(2):107–113. doi:10.1620/tjem.236.107
10. Banikarim C, Chacko MR, Kelder SH. Prevalence and impact of dysmenorrhea on Hispanic female adolescents. Arch Pediatr Adolesc Med. 2000;154(12):1226–1229. doi:10.1001/archpedi.154.12.1226
11. Zou L, Li L, Yan H, Cai Q. Symptom relief for patients with primary dysmenorrhea. Asian J Surg. 2024;47(3):1439–1440. doi:10.1016/j.asjsur.2023.11.119
12. Burnett M, Lemyre M. No. 345-primary dysmenorrhea consensus guideline. J Obstet Gynaecol Can. 2017;39(7):585–595. doi:10.1016/j.jogc.2016.12.023
13. Kirsch E, Rahman S, Kerolus K, et al. Dysmenorrhea, a narrative review of therapeutic options. J Pain Res. 2024;17:2657–2666. doi:10.2147/JPR.S459584
14. Dawood MY. Primary dysmenorrhea: advances in pathogenesis and management. Obstet Gynecol. 2006;108(2):428–441. doi:10.1097/01.AOG.0000230214.26638.0c
15. Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. 2020;323(3):268–269. doi:10.1001/jama.2019.16921
16. Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015;2015(7):CD001751. doi:10.1002/14651858.CD001751.pub3
17. Harel Z. Dysmenorrhea in adolescents and young adults: from pathophysiology to pharmacological treatments and management strategies. Expert Opin Pharmacother. 2008;9(15):2661–2672. doi:10.1517/14656566.9.15.2661
18. Proctor M, Farquhar C. Diagnosis and management of dysmenorrhoea. BMJ. 2006;332(7550):1134–1138. doi:10.1136/bmj.332.7550.1134
19. Zahradnik H-P, Hanjalic-Beck A, Groth K. Nonsteroidal anti-inflammatory drugs and hormonal contraceptives for pain relief from dysmenorrhea: a review. Contraception. 2010;81(3):185–196. doi:10.1016/j.contraception.2009.09.014
20. Nie W, Xu P, Hao C, Chen Y, Yin Y, Wang L. Efficacy and safety of over-the-counter analgesics for primary dysmenorrhea: a network meta-analysis. Medicine (Baltimore). 2020;99(19):e19881. doi:10.1097/MD.0000000000019881
21. Bernardi M, Lazzeri L, Perelli F, Reis FM, Petraglia F. Dysmenorrhea and related disorders. F1000Res. 2017;6:1645. doi:10.12688/f1000research.11682.1
22. Group ECW. Noncontraceptive health benefits of combined oral contraception. Hum Reprod Update. 2005;11(5):513–525.
23. Yu A. Complementary and alternative treatments for primary dysmenorrhea in adolescents. Nurse Pract. 2014;39(11):1–12. doi:10.1097/01.NPR.0000454984.19413.28
24. Smith CA, Armour M, Zhu X, Li X, Lu ZY, Song J. Acupuncture for dysmenorrhoea. Cochrane Database Syst Rev. 2016;4(4):CD007854. doi:10.1002/14651858.CD007854.pub3
25. Yang J, Xiong J, Yuan T, et al. Effectiveness and safety of acupuncture and moxibustion for primary dysmenorrhea: an overview of systematic reviews and meta-analyses. Evid Based Complement Alternat Med. 2020;2020(1):8306165. doi:10.1155/2020/8306165
26. Xu N, Huang Y, Huang H, et al. Curative effect of heat-sensitive moxibustion on primary dysmenorrhea: a meta-analysis. Evid Based Complement Alternat Med. 2022;2022:1281336. doi:10.1155/2022/1281336
27. Lu C-X, Deng X-J, Chen M, Xiao C-H, Cui J. Different stimulation methods on auricular points for primary dysmenorrhea: a r andomized controlled trial. Zhongguo Zhen Jiu. 2021;41(7):737–741. doi:10.13703/j.0255-2930.20200531-k0002
28. Zhang H-R, Tu H-Y, Wang Y, et al. Effectiveness and safety of moxibustion robots on primary dysmenorrhea: a randomized controlled pilot trial. Chin J Integr Med. 2021;27(8):578–584. doi:10.1007/s11655-021-3287-8
29. Ma Y-X, Ye X-N, Liu C-Z, et al. A clinical trial of acupuncture about time-varying treatment and points selection in primary dysmenorrhea. J Ethnopharmacol. 2013;148(2):498–504. doi:10.1016/j.jep.2013.04.045
30. Xue X, Liu X, Pan S, et al. Electroacupuncture treatment of primary dysmenorrhea: a randomized, participant-blinded, sham-controlled clinical trial protocol. PLoS One. 2023;18(5):e0282541. doi:10.1371/journal.pone.0282541
31. Cha NH, Sok SR. Effects of auricular acupressure therapy on primary dysmenorrhea for female high school students in south Korea. J Nurs Scholarsh. 2016;48(5):508–516. doi:10.1111/jnu.12238
32. Wu Z, Yang Y, Xiong J, Yu X, Zuo Z, Xie Q. Which acupuncture and moxibustion technique is more effective for primary dysmenorrhea: a protocol for a network meta-analysis of randomized controlled trials. Medicine (Baltimore). 2020;99(35):e21713. doi:10.1097/MD.0000000000021713
33. Lv Y, Feng H, Jing F, et al. A systematic review of Tuina for women with primary dysmenorrhea: a protocol for systematic review and meta-analysis. Medicine (Baltimore). 2021;100(47):e27935. doi:10.1097/MD.0000000000027935
34. López-Liria R, Torres-álamo L, Vega-Ramírez FA, et al. Efficacy of physiotherapy treatment in primary dysmenorrhea: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(15):7832. doi:10.3390/ijerph18157832
35. Uthman OA, van der Windt DA, Jordan JL, et al. Exercise for lower limb osteoarthritis: systematic review incorporating trial sequential analysis and network meta-analysis. Br J Sports Med. 2014;48(21):1579. doi:10.1136/bjsports-2014-5555rep
36. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
37. Comparative Effectiveness of Non-Pharmacological Therapies for Primary Dysmenorrhea: A network meta-analysis of randomized controlled trials Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024493532.
38. Cochrane. Handbook for systematic reviews of interventions version 6.4.
39. Higgins JPTTJ, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. 2nd Edition. In. Edn. Chichester (UK): John Wiley & Sons; 2019.
40. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560.
41. Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One. 2013;8(10):e76654. doi:10.1371/journal.pone.0076654
42. Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making. 2013;33(5):641–656. doi:10.1177/0272989X12455847
43. Salanti G, Ades AE, Ioannidis JPA. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. 2011;64(2):163–171. doi:10.1016/j.jclinepi.2010.03.016
44. Abbas MAM, Afify AM, Sayed AM. Impact of different exercise techniques on menstrual pain severity in postacute covid-19 Women. J Popul Ther Clin Pharmacol. 2023;30(7):177–183.
45. Chen H-M, Chen C-H. Effects of acupressure at the Sanyinjiao point on primary dysmenorrhoea. J Adv Nurs. 2004;48(4):380–387. doi:10.1111/j.1365-2648.2004.03236.x
46. Chen H-M, Wang -H-H, Chiu M-H, Hu H-M. Effects of acupressure on menstrual distress and low back pain in dysmenorrheic young adult women: an experimental study. Pain Manag Nurs. 2015;16(3):188–197. doi:10.1016/j.pmn.2014.06.002
47. Yang N-Y, Kim S-D. Effects of a yoga program on menstrual cramps and menstrual distress in undergraduate students with primary dysmenorrhea: a single-blind, randomized controlled trial. J Altern Complement Med. 2016;22(9):732–738. doi:10.1089/acm.2016.0058
48. Qorbanalipour K, Ghaderi F, Jafarabadi MA. Comparison of the effects of acupressure and electroacupuncture in primary dysmenorrhea: a randomized controlled trial. Int J Women Health Reprod Sci. 2018;6(4):471–476. doi:10.15296/ijwhr.2018.78
49. Shetty GB, Shetty B, Mooventhan A. Efficacy of acupuncture in the management of primary dysmenorrhea: a randomized controlled trial. J Acupunct Meridian Stud. 2018;11(4):153–158. doi:10.1016/j.jams.2018.04.001
50. Kirca N, Celik AS. The effect of yoga on pain level in primary dysmenorrhea. Health Care Women Int. 2023;44(5):601–620. doi:10.1080/07399332.2021.1958818
51. Feng Yanna XY. Analysis of the analgesic effects of moxibustion and acupuncture on primary dysmenorrhea. J Sichuan of Traditional Chin Med. 2016;34(10):166–168.
52. Chen S: Controlled Clinical Trial of Treating Primary Dysmenorrhealwith Abdominal Acupuncture and Placebo Acupuncture. academic dissertation. Guangzhou University of Chinese Medicine; 2014.
53. Hua F. Clinical observation on the treatment of primary dysmenorrhea with cold-congealed blood stasis by spaced ginger moxibustion. J PRACT TRADITION CHIN MED. 2017;33(12):1438–1439.
54. Zhang X, Wang Q. Clinical observation of salt-partitioned moxibustion at Shenque (CV 8) for primary dysmenorrhea due to cold coagulation and blood stagnation. Shanghai Zhenjiu Zazhi. 2016;35(2):175–177.
55. Dong-qing DU, Cui-ju YIN, Yu-xia MA, Xiao-lan LIU, Shu-zhong GAO. Xiu-ying W: clinical Study on Herb-partitioned Moxibustion on Shenque (CV 8) for Treating Primary Dysmenorrhea. Shanghai J Acu-Mox. 2011;30(8):514–516.
56. Hang Y, Zhou Y, Guo X, Liu Y, Li H, Chen X. Analgesic effect on primary dysmenorrheal treated with conventional and sham acupuncture at San-yinjiao (SP 6). Zhongguo Zhen Jiu. 2015;35(4):318–322.
57. Gao T: Clinical Observation of Acupuncture in Prevention and Treatment of Primary Dysmenorrhea. MASTER DISSERTATION. Hubei University of Chinese Medicine; 2019.
58. Fei L, Peng Z, Lu C. Immediate pain relief effect and clinical efficacy of acupuncture and moxibustion in the treatment of primary dysmenorrhea. HUNAN UNIV CHIN MED. 2020;15. doi:10.1186/s13020-020-00325-x
59. Ryan SA. The Treatment of Dysmenorrhea. Pediatr Clin North Am. 2017;64(2):331–342. doi:10.1016/j.pcl.2016.11.004
60. Hailemeskel S, Demissie A, Assefa N. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: evidence from female university students in Ethiopia. Int J Women's Health. 2016;8:489–496. doi:10.2147/IJWH.S112768
61. Yonglitthipagon P, Muansiangsai S, Wongkhumngern W, et al. Effect of yoga on the menstrual pain, physical fitness, and quality of life of young women with primary dysmenorrhea. J Bodyw Mov Ther. 2017;21(4):840–846. doi:10.1016/j.jbmt.2017.01.014
62. Özgül S, Üzelpasaci E, Orhan C, Baran E, Beksaç MS, Akbayrak T. Short-term effects of connective tissue manipulation in women with primary dysmenorrhea: a randomized controlled trial. Complement Ther Clin Pract. 2018;33:1–6. doi:10.1016/j.ctcp.2018.07.007
63. Woodforde JM, Merskey H. Some relationships between subjective measures of pain. J Psychosom Res. 1972;16(3):173–178. doi:10.1016/0022-3999(72)90041-4
64. Liu J, Liu J, Wang X-S, et al. Comparative study of different dosages of grain-sized moxibustion on uterine artery blood flow in patients with cold and dampness primary dysmenorrhea. Zhen Ci Yan Jiu. 2024;49(7):760–766. doi:10.13702/j.1000-0607.20230026
65. Shi J, Chen Z. Fu’s subcutaneous needling combined with monkshood cake-separated moxibustion for primary dysmenorrhea with cold congealing and blood stasis: a randomized controlled trial. Zhongguo Zhen Jiu. 2024;44(8):905–909. doi:10.13703/j.0255-2930.20230919-k0002
66. Ozturk N, Gerçek Öter E, Kürek Eken M. The effect of abdominal massage and stretching exercise on pain and dysmenorrhea symptoms in female university students: a single-blind randomized-controlled clinical trial. Health Care Women Int. 2023;44(5):621–638. doi:10.1080/07399332.2022.2061973
67. Deng H, Shen X. The mechanism of moxibustion: ancient theory and modern research. Evid Based Complement Alternat Med. 2013;2013:379291. doi:10.1155/2013/379291
68. Yang Y, Wang F, Zhao H. Research progress of diagnostic criteria of TCM syndrome type and its common syndrome differentiation in primary dysmenorrhea. Global Traditional Chin Med. 2020;13:1454–1456.
69. Nie R, Huang S, Liao W, Mao Z, Li X, Xiong J. Moxibustion for primary dysmenorrhea: a protocol for evidence-based clinical practice guideline. Medicine. 2021;100(7):e24466. doi:10.1097/MD.0000000000024466
70. Pan S, Wang S, Li J, et al. Moxibustion for primary dysmenorrhea: an adjuvant therapy for pain relief. Evid Based Complement Alternat Med. 2022;2022:6864195. doi:10.1155/2022/6864195
71. Ma Y-X, Yang X-Y, Guo G, Du D-Q, Yu Y-P, Gao S-Z. Research of herb-partitioned moxibustion for primary dysmenorrhea patients based on the LC-MS metabonomics. Evid Based Complement Alternat Med. 2015;2015:621490. doi:10.1155/2015/621490
72. Fan Y-S, Miao F-R, Liao A-N, Xu F. Effect of drug-paste separated moxibustion on expression of estrogen, progestogen and their endometrial receptor mRNA in rats with primary dysmenorrhea. Zhen Ci Yan Jiu. 2013;38(5):352–357.
73. J-n H, Luo M-F. Luo M-f: [Progress in the study on the relationship between effects of acu-moxibustion and mast cells in acupoints]. Zhen Ci Yan Jiu. 2007;32(3):214–216.
74. Li X, Ma M, Gao Y. Effect of umbilical cord therapy on mast cells in shenque acupoint area of cold coagulation and blood stasis dysmenorrhea rats. Lishizhen Medicine and Materia Medica Res. 2017;28(9):2288–2290.
75. Shuangshuang Q, Panbi C, Jingming H. Effect of moxibustion at different acupoints on NK cell activity of primary dysmenorrhea rat model. Asia Pac Trad Med. 2017;13:4–7.
76. Chen PB, Qi SS, Cui J, et al. Herbal-cake-partitioned moxibustion of “Shenque” (CV8) has a relative specific effect in relieving abdominal pain and in regulating neuroendocrine-immune network in primary dysmenorrhea rats. Zhen Ci Yan Jiu. 2019;44(2):120–124. doi:10.13702/j.1000-0607.170811
77. Zhang Z, Li R, Chen Y, Yang H, Fitzgerald M, Wang Q, Xu Z, Huang N, Lu D and Luo L. (2024). Integration of traditional, complementary, and alternative medicine with modern biomedicine: the scientization, evidence, and challenges for integration of traditional Chinese medicine. Acupuncture and Herbal Medicine, 4(1), 68–78. 10.1097/HM9.0000000000000089
78. Liu B, Chen B, Guo Y and Tian L. (2021). Acupuncture – a national heritage of China to the world: international clinical research advances from the past decade. Acupuncture and Herbal Medicine, 1(2), 65–73. 10.1097/HM9.0000000000000017
79. Stener-Victorin E, Waldenström U, Andersson SA, Wikland M. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Hum Reprod. 1996;11(6):1314–1317. doi:10.1093/oxfordjournals.humrep.a019378
80. McDonald JL, Cripps AW, Smith PK. Mediators, receptors, and signalling pathways in the anti-inflammatory and antihyperalgesic effects of acupuncture. Evid Based Complement Alternat Med. 2015;2015:975632. doi:10.1155/2015/975632
81. Wang S-F, Lee J-P, Hwa H-L. Effect of transcutaneous electrical nerve stimulation on primary dysmenorrhea. Neuromodulation: Technol Neural Interface. 2009;12(4):302–309. doi:10.1111/j.1525-1403.2009.00226.x
82. Zhao Z-Q. Neural mechanism underlying acupuncture analgesia. Progress in Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
83. Liu F, Xiong J, Huang G-Y, Wang W. Study on the underlying mechanism of acupuncture in regulating neuroendocrine activity in dysmenorrhea rats. Zhen Ci Yan Jiu. 2009;34(1):3–8.
84. Papka RE, Traurig HH, Schemann M, Collins J, Copelin T, Wilson K. Cholinergic neurons of the pelvic autonomic ganglia and uterus of the female rat: distribution of axons and presence of muscarinic receptors. Cell Tissue Res. 1999;296(2):293–305. doi:10.1007/s004410051290
85. Yu W-Y, Ma L-X, Zhang Z, et al. Acupuncture for primary dysmenorrhea: a potential mechanism from an anti-inflammatory perspective. Evid Based Complement Alternat Med. 2021;2021:1907009. doi:10.1155/2021/1907009
86. Lin J-G, Kotha P, Chen Y-H. Understandings of acupuncture application and mechanisms. Am J Transl Res. 2022;14(3):1469–1481.
87. Wang Y, Li S-Y, Wang D, et al. Transcutaneous auricular vagus nerve stimulation: from concept to application. Neurosci Bull. 2021;37(6):853–862. doi:10.1007/s12264-020-00619-y
88. Hou P-W, Hsu H-C, Lin Y-W, Tang N-Y, Cheng C-Y, Hsieh C-L. The history, mechanism, and clinical application of auricular therapy in traditional Chinese medicine. Evid Based Complement Alternat Med. 2015;2015:495684. doi:10.1155/2015/495684
89. Gori L, Firenzuoli F. Ear acupuncture in European traditional medicine. Evid Based Complement Alternat Med. 2007;4(Suppl 1):13–16. doi:10.1093/ecam/nem106
90. Kong X, Fang H, Li X, Zhang Y, Guo Y. Effects of auricular acupressure on dysmenorrhea: a systematic review and meta-analysis of randomized controlled trials. Front Endocrinol (Lausanne). 2022;13:1016222. doi:10.3389/fendo.2022.1016222
91. Liu M, Tong Y, Chai L, et al. Effects of auricular point acupressure on pain relief: a systematic review. Pain Manag Nurs. 2021;22(3):268–280. doi:10.1016/j.pmn.2020.07.007
92. Ge SJ LI. ZHAO Chen,GE Long,TIAN Jinhui,SHANG Hongcai,WANG Zixin,XU Xiangling, WANG Shuhe: network meta-analysis on clinical effects of acupuncture in treatment of primary dysmenorrhea. Chinese J of Evidence-Based Med. 2017;17:10.
93. Woo HL, Ji HR, Pak YK, et al. The efficacy and safety of acupuncture in women with primary dysmenorrhea: a systematic review and meta-analysis. Medicine (Baltimore). 2018;97(23):e11007. doi:10.1097/MD.0000000000011007
94. Ying X, MY WH. ZB: [Meta-analysis of Therapeutic Effect of Moxibustion on Primary Dysmenorrhea]. WORID CHIN MED. 2023;18(15):2178–2184.
95. Li X, Hao X, Liu J and Huang J. (2024). Efficacy of non-pharmacological interventions for primary dysmenorrhoea: a systematic review and Bayesian network meta-analysis. BMJ EBM, 29(3), 162–170. 10.1136/bmjebm-2023-112434
96. Abaraogu UO, Tabansi-Ochuogu CS. As acupressure decreases pain, acupuncture may improve some aspects of quality of life for women with primary dysmenorrhea: a systematic review with meta-analysis. J Acupunct Meridian Stud. 2015;8(5):220–228. doi:10.1016/j.jams.2015.06.010
97. Armour M, Smith CA, Steel KA, Macmillan F. The effectiveness of self-care and lifestyle interventions in primary dysmenorrhea: a systematic review and meta-analysis. BMC Complement Altern Med. 2019;19(1):22. doi:10.1186/s12906-019-2433-8
98. Wójcik M, Placek K. APPLICATION PHYSIOTHERAPY AND BALNEOCLIMATOLOGY IN GYNAECOLOGY. Acta Balneologica. 2023;174(4):253–262. doi:10.36740/ABal202304110
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture and Related Therapies for Endometriosis: A Network Meta-Analysis of Randomized Controlled Trials
Li H, Wang X, Wang Y, Gao Y, Zheng X, Zhang X, Li X, Zheng X, Fan X, Zuo G, She Y
Journal of Pain Research 2024, 17:3197-3216
Published Date: 2 October 2024