")
Back to Journals » Journal of Pain Research » Volume 18
Efficacy and Safety of Prophylactic Intrathecal or Epidural Normal Saline for Preventing Post-Dural Puncture Headache After Dural Puncture: A Meta-Analysis and Systematic Review
Authors Jing W, Ma Y, Wan Y, Li H
Received 12 September 2024
Accepted for publication 5 February 2025
Published 26 February 2025 Volume 2025:18 Pages 915—927
DOI https://doi.org/10.2147/JPR.S494237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Weiwei Jing, Yushan Ma, Yantong Wan, Hao Li
Department of Anesthesiology, West China Second University Hospital, Sichuan University, Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, Chengdu, Sichuan, People’s Republic of China
Correspondence: Hao Li, Department of Anesthesiology, West China Second University Hospital, Sichuan University, Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, Chengdu, Sichuan, 610041, People’s Republic of China, Tel/Fax +86 028 85503753, Email [email protected]
Background: Post-dural puncture headache (PDPH) is the most common and troublesome complication following iatrogenic puncture of the dura. This study aims to evaluate the efficacy and safety of intrathecal or epidural saline injection to prevent PDPH.
Methods: A systematic literature search was conducted in PubMed, Embase, Web of Science, and the Cochrane Library, supplemented by a manual search of reference lists of related articles. Studies were eligible if they compared intrathecal or epidural injection or continuous saline infusion with no intervention in patients with accidental or intentional dural puncture. Trials reporting PDPH outcomes were considered eligible. The type of surgeries and patient populations were not restricted. Risk ratios (RRs) with 95% confidence intervals (CI) were calculated for the risk estimate of dichotomous outcomes. The funnel plot, Egger, and Begg tests were performed to assess the publication bias.
Results: We identified 13 studies involving 1589 patients, revealing a high publication bias. Normal saline injection reduced the incidence of PDPH (RR=0.57, 95% CI: 0.43 to 0.74, P< 0.0001, I2=66%, P-heterogeneity=0.0004) and the requirement for an epidural blood patch (RR=0.37, 95% CI: 0.25 to 0.54, P< 0.00001, I2=29%, P-heterogeneity=0.23).
Conclusion: Saline administration after dural puncture appears to be a promising option for preventing PDPH. However, heterogeneity among the studies and publication bias with positive results limits the available evidence. Therefore, further large-scale randomized controlled trials are needed to confirm our findings.
Register: CRD42022342509.
Keywords: dural puncture, saline, post-dural puncture headache, meta-analysis
Introduction
Post-dural puncture headache (PDPH) is defined as a headache occurring within five days of a lumbar puncture, which is worsened by standing or sitting and is relieved by lying down.1 The occurrence of PDPH varies widely, with rates ranging from less than 2% to 40%,2 depending on lumbar puncture and population factors. It is the most common and troublesome complication following a dural puncture during neuraxial anesthesia or procedures. PDPH is an annoying condition and has been known to increase the length of hospital stay, and cause dissatisfaction among patients. PDPH is also shown to lead to chronic headaches, backache, neckache, and depression.3–7 In addition, devasting neurological adverse events such as subdural hematoma and intracranial venous thrombosis may occur in patients with PDPH.8–10 Other symptoms associated with PDPH include neck stiffness, photophobia, tinnitus, and hypoacusia.
The mechanism of PDPH is elusive and still needs to be fully understood. It is generally accepted that PDPH is secondary to intracranial hypotension due to cerebrospinal fluid leakage through a dural tear.11 Intracranial hypotension results in traction on the intracranial sinuses, cerebral vessels, and tentorium, causing headaches and neckaches.11,12 This traction effect is more pronounced when the patient is upright or sitting, as gravity facilitates further CSF loss and brain sagging. Moreover, to compensate for the loss of CSF, cerebral blood vessels dilate to increase blood volume and maintain intracranial pressure. This vasodilation can stimulate pain receptors, leading to headaches.13 Furthermore, it has been postulated that reduced cerebrospinal fluid volume and lower intracranial pressure may contribute to the activation of adenosine receptors, leading to PDPH.13 Therefore, reducing the outflow of cerebrospinal fluid is the main strategy for preventing PDPH.
Current approaches to preventing PDPH include epidural blood patches, patient positioning, activity modification, pharmacological interventions, and education and training.2 Epidural blood patch is an invasive procedure associated with potential serious complications, such as re-dural puncture and adhesive arachnoiditis,14 and is therefore not routinely employed for the prevention of PDPH.15 However, the effectiveness of alternative measures for PDPH prevention remains limited. Consequently, identifying interventions that effectively reduce the incidence of PDPH in patients experiencing dural puncture is of critical importance. It has been reported that intrathecal or epidural saline injection after dural puncture might effectively decrease the incidence of PDPH and the need for EBP,16,17 which is a simple, inexpensive, and effective method. However, the efficacy of injection of saline as prophylaxis for PDPH is still controversial. Currently, there is a lack of large trials using saline to prevent PDPH. And there is no systematic review and meta-analysis to confirm this issue. Therefore, we performed this review to evaluate the efficacy and safety of administering saline intrathecally or epidurally in decreasing the risk of PDPH after a dural puncture.
Methods
This systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18 The PRISMA statement is available in Appendix 1. This review was registered with PROSPERO (CRD42022342509).
Literature Search
We searched PubMed, Cochrane Library, Embase, and Web of Science for papers published up to June 27, 2024, using MeSH terms “Post-Dural Puncture Headache” and “Saline Solution” along with relevant keywords. Detailed search strategies are shown in Appendix 2. Reference lists of related articles were also screened for additional relevant studies.
Inclusion and Exclusion Criteria
Eligibility criteria included: 1) population: patients who experienced unintentional dural punctures during epidural techniques or intentional dural punctures during neuraxial procedures such as a lumbar puncture or spinal anesthesia; 2) interventions: Intrathecal or epidural injection or continuous saline infusion; 3) Control: no intrathecal or epidural normal saline; 4) outcome: incidence of PDPH; 5) study type: randomized controlled trials, prospective or retrospective cohort studies. Studies on animals were excluded, and only English was considered. Two authors (Weiwei Jing and Hao Li) independently screened the articles for eligibility. Any discrepancies were resolved by discussion until a consensus was achieved.
Data Extraction
Two authors (Weiwei Jing and Yushan Ma) independently extracted study characteristics (eg, first author, year of publication, sample size, study design, study period, country, type of surgery, type of lumbar puncture, mean age in the treatment and control group), treatment parameters (eg, route and method of saline injection, the volume of saline used), the primary outcome (eg, incidence of PDPH), and the secondary outcomes (eg, needs for epidural blood patches, severity of PDPH, incidence of side effect) using a standardized form. Any discrepancies were resolved by discussion until a consensus was reached.
Risk of Bias and Quality Assessment
Two authors (Jing and Li) independently assessed the methodological quality of the included studies according to the Newcastle-Ottawa scale (NOS) for cohort studies (https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) and the Cochrane Handbook for prospective randomized control studies.19 Discrepancies in the assessment were resolved through discussion until a consensus was reached.
Statistical Analysis
Each study’s risk estimates were reported as risk ratios (RRs). We extracted the number of patients with and without PDPH in the treatment and control groups to calculate the RRs that combined the effect size. For the dichotomous outcomes, RRs and 95% confidence intervals (95% CI) were calculated. Statistical heterogeneity among the studies was assessed using Cochran’s Q test and the I2 index. If p-value < 0.05 or I²>50%, indicating significant heterogeneity, a random-effect model was used; otherwise, a fixed-effect model was applied. Four sensitivity analyses were conducted. If the number of included studies exceeds 10, Begg’s test, Egger’s test, and funnel plot were used to assess publication bias. Sensitivity analyses were conducted using the article-by-article culling method. Subgroup analyses were performed based on the volume of saline used, route of saline injection, study design type, method of saline used, type of anesthesia, and date of publication. P-values<0.05 were considered statistically significant. All analyses were performed using Stata/MP 15.0 and Review Manager 5.4.1.
Results
Search Process and Characteristics of the Included Studies
The flow chart concerning the selection of references is shown in Figure 1. A total of 1154 records were identified, and 469 duplicates were excluded. Among the remaining 685 records, 655 were excluded due to non-eligible study types, studies on animals, irrelevant topics, or non-English language. Thirty full-text papers were assessed for eligibility, and 17 were excluded (outcome and participant, criteria, n=1; no available data, n=4; no control group, n=6; intervention criteria, n=3; letter or case report, n=3). Finally, 13 studies, including 1589 patients, were included in the meta-analysis.13,16,17,20–29 Studies included in this review were published between 1952 and 2023. The characteristics of the enrolled studies are summarized in Table 1. There were five RCTs, five prospective cohort studies, and three retrospective cohort studies. Assessment of the methodological study quality is provided in Figure 2a and b (for RCTs) and Table 2 (for cohort studies).
 |
Figure 1 Flow diagram of the study selection process. |
 |
Figure 2 Cochrane collaboration risk of bias evaluation graph (a) and summary (b) for each included randomized controlled study. |
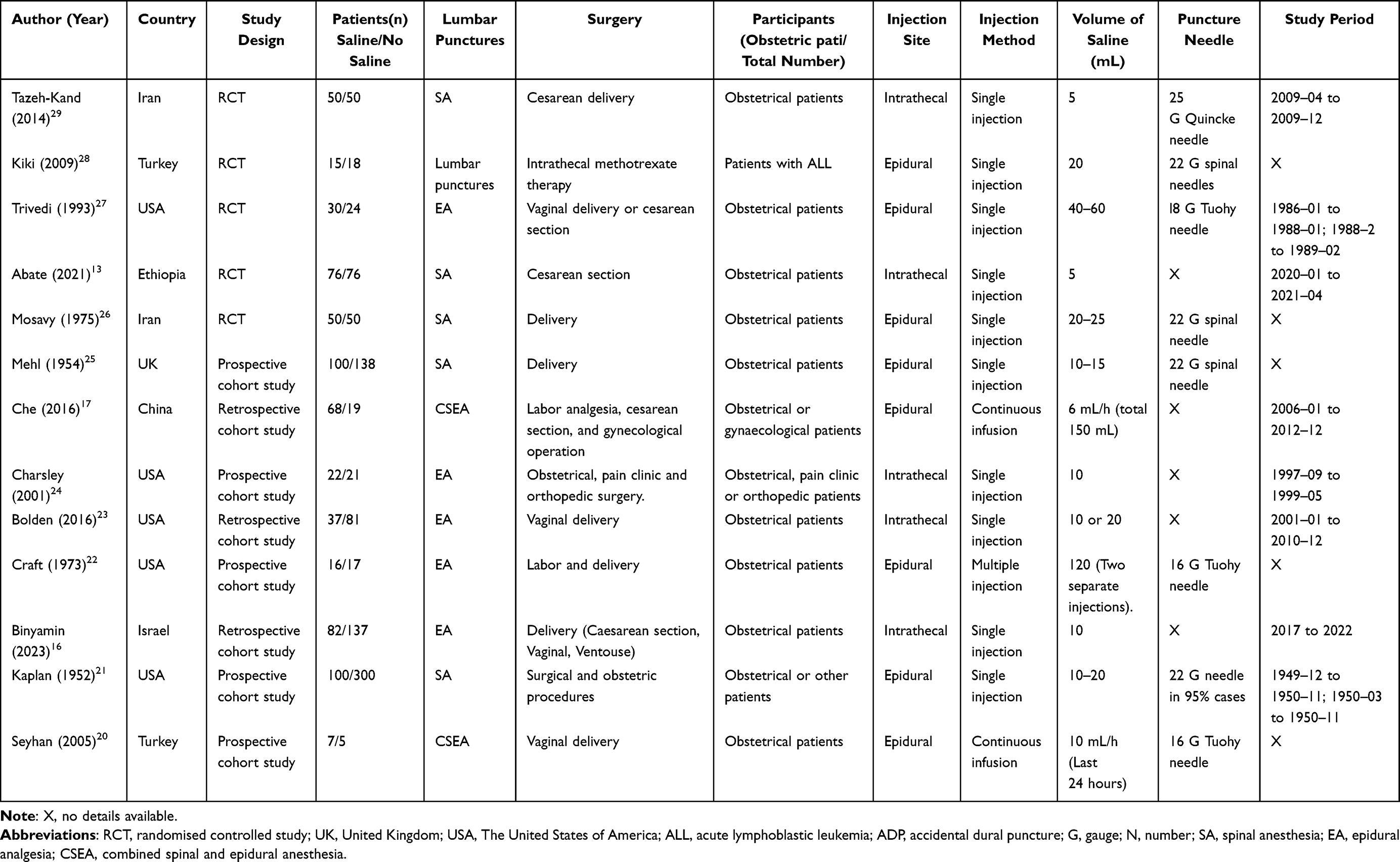 |
Table 1 Characteristics of 13 Enrolled Studies in the Meta-Analysis |
 |
Table 2 Quality Evaluation of the Eligible Cohort Studies With the Newcastle-Ottawa Scale |
Incidence of PDPH
13 studies involving 1589 patients reported the incidence of PDPH.13,16,17,20–29 The results revealed a significant decrease in the incidence of PDPH in the saline group compared to the no-saline group (P<0.0001, RR 0.57, 95% CI 0.43 to 0.74; I2=66%) (Figure 3a). Due to the significant heterogeneity, we performed a sensitivity analysis (Figure 3b). The pooled RRs showed no significant difference in the incidence of PDPH when any of the included trials were excluded, indicating that the results are robust. However, the funnel plot (Figure 3c and d) showed significant asymmetry in the analysis of PDPH, as confirmed by Egger’s (P<0.001) and Begg’s tests (F) (P<0.001).
 |
Figure 3 Forest plot for PDPH (a), Sensitive analysis of the effect of each study on the overall meta-analysis of PDPH (b), Begg’s (c) and Egger’s (d) funnel plots test of studies that examined PDPH as a test for publication bias. |
Incidence of Mild and Moderate or Severe PDPH
Five studies17,22,26,27,29 involving 374 patients reported the severity of PDPH. The study by Tazeh-kand et al29 only compared the incidence of no and mild headaches between groups. Data on mild PDPH alone were not available. Therefore, only four studies were included for the incidence of mild PDPH. The results showed that saline does not decrease the incidence of mild PDPH (RR 0.72, 95% CI 0.17 to 3.05, p=0.65; I2 =73%) (Figure 4a). There was a statistically significant reduction in the incidence of moderate or severe PDPH in the saline group when compared to the no-saline group. (RR 0.29, 95% CI 0.11 to 0.80, p=0.02; I2 =80%) (Figure 4b).
 |
Figure 4 Forest plot for mild PDPH (a), moderate or severe PDPH (b), Sensitive analysis of the effect of each study on the overall meta-analysis of mild PDPH (c), and moderate or severe PDPH (d). |
However, the heterogeneity in our analyses was high, as reflected by the significantly elevated I2 value. We performed a sensitivity analysis and found no significant change in pooled RRs when any of the enrolled studies were excluded (Figure 4c and d). The various definitions of PDPH severity among the included studies may account for this heterogeneity. For instance, Che et al17 graded the severity of PDPH using a visual analog score. Trivedi et al27 did not provide a specific definition for PDPH classification, so this review defined mild PDPH as headaches that could be improved with conservative treatment (oral fluid therapy and analgesic medications). Otherwise, it was described as moderate or severe. In the trial by Mosavy et al,26 headaches were classified as “severe” if they were not relieved by non-narcotic analgesics and were accompanied by nausea, vomiting, and dizziness. Otherwise, they were defined as mild. Craft et al22 classified PDPH as mild, moderate, or severe based on symptoms associated with PDPH according to their own criteria. Tazeh-Kand et al29 provided data on mild, moderate, and severe PDPH but did not describe a specific grading scheme.
The Need for EBP
Five studies16,23,24,27,28 involving 466 patients reported data on the need for EBP and were included in the meta-analysis. The results showed that saline significantly reduces the need for EBP in patients with dural puncture (RR 0.37, 95% CI 0.25 to 0.54, p<0.00001; I2 =29%) (Figure 5).
 |
Figure 5 Forest plot for the need for epidural blood patch. |
Complications of Saline Injection
None of the 13 trials in this systematic review reported complications directly related to using saline. Three studies compared the incidence of nausea and vomiting in saline and non-saline patients. The meta-analysis results showed no significant difference in the incidence of nausea and vomiting between the saline and non-saline groups (RR 0.74, 95% CI 0.50 to 1.09, p=0.13; I2 =32%) (Figure 6). Kiki et al28 reported two patients in the non-saline group who developed generalized convulsion attacks, with one patient experiencing apnea necessitating respiratory support.
 |
Figure 6 Forest plot for nausea and vomiting. |
Subgroup Analysis
We performed a subgroup analysis based on publication dates (Figure 7a), study design (Figure 7b), different saline injection sites (Figure 7c), the volume of saline (Figure 7d), type of saline use (Figure 7e), and type of lumbar puncture (Figure 7f). Except for patients receiving continuous saline infusion (n=2) and those receiving combined spinal-epidural anesthesia (n=2), the incidence of PDPH was not significantly different between groups; similar results were observed in other subgroups.
 |
Figure 7 Forest plot of subgroup analysis of publication dates (a), study design (b), different saline injection sites (c), the volume of saline (d), type of saline use (e), and type of lumbar puncture (f) for PDPH. |
Discussion
In this systematic review and meta-analysis, we found that epidural or intrathecal injection of normal saline following dural puncture significantly decreases the incidence of post-dural puncture headache (PDPH). The results indicate that while saline does not reduce the incidence of mild PDPH, it significantly reduces the incidence of moderate or severe PDPH. Additionally, saline significantly decreases the need for an epidural blood patch (EBP) in patients with dural puncture.
Lumbar puncture is widely used, including various spinal anesthesia and surgery types. PDPH is the most common and bothersome complication of dural puncture. PDPH not only severely impairs early patient recovery but is also strongly associated with chronic headaches, back pain, depression, and traumatic stress syndrome.3,6,7 Various approaches are suggested to prevent and treat PDPH, including bed rest, fluid therapy, acetaminophen, NSAIDs, and caffeine.2 However, a body of evidence2,12,30,31 revealed those conservative measurements failed to show significant benefit in most cases. An epidural blood patch is the definitive treatment for PDPH but is not considered a preventive measure because it is invasive and not always successful.32 There are very few effective measures to prevent PDPH.31
Our systematic review showed that saline could be injected intrathecally or epidurally in patients with dural puncture for PDPH prevention, providing a straightforward, cost-effective preventive approach. None of the studies in this review reported adverse effects directly related to injecting normal saline. One possible explanation for the beneficial effect of the saline injection is that the increased CSF pressure may cause the dura and arachnoid to come together at the puncture site, sealing the defect.16,29 Reducing the leak would allow the dura to be repaired.28 Another possible explanation is that injection of intrathecal or epidural normal saline may prevent activation of the adenosine receptors, thereby decreasing the incidence and severity of PDPH.24 Both intrathecal and epidural saline injections can directly or indirectly increase cerebrospinal fluid (CSF) volume and pressure, suggesting a shared mechanism in reducing the incidence of PDPH. Given the limited number of studies addressing this issue, we combined intrathecal and epidural saline studies in our analysis. This meta-analysis aims to guide further exploration of prophylactic measures for post-dural puncture headache. Future large-scale randomized controlled trials are needed to validate our findings, investigate the underlying mechanisms of saline, and determine the optimal injection site.
However, there are several doubts regarding the mechanism underlying the effect of saline injection. Firstly, it remains uncertain whether saline persists at the site of the defect long enough to reduce leakage, allowing a fibrin clot to form or the pia mater to repair the defect. Secondly, continuous confusion saline may have a more significant effect on increasing the pressure in the epidural space than single saline injections. However, we did not find significance in the subgroup of continuous confusion with saline, possibly because only two trials were included. Large randomized controlled trials are needed to compare the efficacy of single and constant saline injections on PDPH. Our results indicated the prophylaxis value of saline was consistent with findings from some studies,16,17,20–22,24–29 while other studies disputed this.13,23 Reasons for discrepancy include the study population, type of study design, variation in the definition of PDPH, number of days followed up, and volume of normal saline.
Our review has several strengths. Firstly, it is the first meta-analysis to systematically evaluate the prophylactic value and safety of saline for preventing post-dural puncture headache (PDPH) in patients with dural puncture, encompassing 13 reports with 1589 patients. This large sample size significantly enhances the statistical power and credibility of our results. Secondly, the comprehensive inclusion of multiple studies enabled us to perform subgroup and sensitivity analyses, which helped assess the consistency and reliability of the findings. Sensitivity analyses showed that the occurrence of PDPH remained stable regardless of which studies were excluded. Subgroup analyses based on different injection sites, saline volumes, type of injection, date of publication, and study designs also revealed no significant differences. Furthermore, using funnel plots and Egger’s test to assess publication bias ensured that the selective publication of positive findings did not significantly skew the results.
This review has several limitations that should be considered when interpreting the results. Firstly, only five randomized controlled trials were included, and some studies were either outdated or insufficient. Nevertheless, a subgroup analysis showed that the application of saline effectively prevent PDPH. Secondly, Some studies involved patients with accidental dural punctures, which have a low incidence (0.5–1%) and pose challenges for randomization and blinding. Finally, the high heterogeneity among the included study in this meta-analysis may have influenced the results. Heterogeneity likely stems from variations in study design, publication periods, anesthetic techniques, and needle sizes, all of which significantly impact PDPH incidence. However, subgroup analyses showed consistency across anesthesia types and timeframes, supporting the robustness of the findings despite the inclusion of both accidental and intentional dural punctures. Therefore, Further studies are required to confirm the details of the normal saline administration, such as the optimal injection site, volume of saline and population.
In conclusion, this systematic review and meta-analysis demonstrated that intrathecal or epidural injection of normal saline after dural puncture can reduce the incidence of PDPH and the requirement for EBP. These findings support the potential integration of saline injection into routine clinical practice as a simple, cost-effective measure to improve patient outcomes and reduce the healthcare burden. However, most of the studies are retrospective, and the studies included in our meta-analysis exhibit high heterogeneity. Therefore, large, prospective, randomized studies are needed to confirm these findings and to clarify key aspects such as the optimal saline volume, timing of injection, target patient populations, and the mechanism underlying the effect of saline.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Nature Science Foundation of China (grant number: 82101313).
Disclosure
All authors have nothing to disclose for this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
2. Uppal V, Russell R, Sondekoppam RV, et al. Evidence-based clinical practice guidelines on postdural puncture headache: a consensus report from a multisociety international working group. Reg Anesth Pain Med. 2023:104817. doi:10.1136/rapm-2023-104817
3. Mims SC, Tan HS, Sun K, et al. Long-term morbidities following unintentional dural puncture in obstetric patients: a systematic review and meta-analysis. J Clin Anesth. 2022;79:110787. doi:10.1016/j.jclinane.2022.110787
4. Lacombe A, Downey K, Ye XY, et al. Long-term complications of unintentional dural puncture during labor epidural analgesia: a case-control study. Reg Anesth Pain Med. 2022:103266. doi:10.1136/rapm-2021-103266
5. Liu CW, Loh LW. Chronic disabling postpartum headache after unintentional dural puncture during epidural anaesthesia: a prospective cohort study. Comment on Br J Anaesth 2021; 127: 600-7. Br J Anaesth. 2021;127(6):e204–e205. doi:10.1016/j.bja.2021.09.015
6. Kapan A, Waldhör T, Schiffler T, et al. Health-related quality of life, work ability and disability among individuals with persistent post-dural puncture headache. J Headache Pain. 2024;25(1):64. doi:10.1186/s10194-024-01765-8
7. Orbach-Zinger S, Eidelman LA, Livne MY, et al. Long-term psychological and physical outcomes of women after postdural puncture headache: a retrospective, cohort study. Eur J Anaesthesiol. 2021;38(2):130–137. doi:10.1097/eja.0000000000001297
8. Pontes R, Junqueira F, Paiva M, et al. Intracranial subdural haematoma following dural puncture accidental: clinical case. Revista espanola de anestesiologia y reanimacion. 2021;68(2):103–106. doi:10.1016/j.redar.2020.05.023
9. Niazi AK, Minko P, Elliott KK, et al. Cerebral venous thrombosis after a possible inadvertent dural puncture for labor epidural analgesia. Cureus. 2019;11(6):e4822. doi:10.7759/cureus.4822
10. Chambers DJ, Bhatia K, Columb M. Postpartum cerebral venous sinus thrombosis following obstetric neuraxial blockade: a literature review with analysis of 58 case reports. Int J Obstet Anesth. 2022;49:103218. doi:10.1016/j.ijoa.2021.103218
11. Reis AE, Spano M, Davis-Hayes C, et al. Lumbar puncture complications: a review of current literature. Curr Pain Headache Rep. 2024:01262. doi:10.1007/s11916-024-01262-2
12. Schyns-van den Berg A, Gupta A. Postdural puncture headache: revisited. Best Pract Res Clin Anaesth. 2023;37(2):171–187. doi:10.1016/j.bpa.2023.02.006
13. Abate SM, Ahmed S, Anbese GM, et al. Efficacy and safety of prophylactic intrathecal normal saline for prevention of post dural puncture headache among women undergoing cesarean section under spinal anesthesia: a randomized controlled trial. Int J Surg Open. 2021;35:100396. doi:10.1016/j.ijso.2021.100396
14. Carlswärd C, Darvish B, Tunelli J, et al. Chronic adhesive arachnoiditis after repeat epidural blood patch. Int J Obstet Anesth. 2015;24(3):280–283. doi:10.1016/j.ijoa.2015.04.005
15. Li H, Wang Y, Oprea AD, et al. Postdural puncture headache-risks and current treatment. Curr Pain Headache Rep. 2022;26:441–452. doi:10.1007/s11916-022-01041-x
16. Binyamin Y, Azem K, Heesen M, et al. The effect of placement and management of intrathecal catheters following accidental dural puncture on the incidence of postdural puncture headache and severity: a retrospective real-world study. Anaesthesia. 2023;78(10):1256–1261. doi:10.1111/anae.16088
17. Che XM, Zhang WY, Xu MJ. Continuous epidural pumping of saline contributes to prevent and treat postdural puncture headache. J Clin Anesth. 2016;34:154–158. doi:10.1016/j.jclinane.2016.03.066
18. Page MJ, j E M, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
19. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:Ed000142. doi:10.1002/14651858.Ed000142
20. Seyhan TO, Baskan I, Karadeniz M, et al. Epidural saline infusion for prophylaxis of postdural puncture headache a preliminary report. Reg Anesth Pain Med. 2005;30(5 Suppl 1):75. doi:10.1016/j.rapm.2005.07.126
21. Kaplan MS, Arrowood JG. Prevention of headache following spinal anesthesia; the use of epidural saline; a preliminary report. Anesthesiology. 1952;13(1):103–107. doi:10.1097/00000542-195201000-00015
22. Craft JB, Epstein BS, Coakley CS. Prophylaxis of dural puncture headache with epidural saline. Anesth Analg Curr Res. 1973;52(2):228–231. doi:10.1213/00000539-197303000-00021
23. Bolden N, Gebre E. Accidental dural puncture management: 10-Year Experience at an Academic Tertiary Care Center. Reg Anesth Pain Med. 2016;41(2):169–174. doi:10.1097/aap.0000000000000339
24. Charsley MM, E AS. The injection of intrathecal normal saline reduces the severity of postdural puncture headache. Reg Anesth Pain Med. 2001;26(4):301–305. doi:10.1053/rapm.2001.22584
25. Mehl LB. Epidural injection of normal saline as a means of prevention of spinal headache. Am J Obstet Gynecol. 1954;68(4):1105–1108. doi:10.1016/s0002-9378(16)38406-x
26. Mosavy SH, Shafei M. Prevention of headache consequent upon dural puncture in obstetric patient. Anaesthesia. 1975;30(6):807–809. doi:10.1111/j.1365-2044.1975.tb00961.x
27. Trivedi NS, Eddi D, Shevde K. Headache prevention following accidental dural puncture in obstetric patients. J Clin Anesth. 1993;5(1):42–45. doi:10.1016/0952-8180(93)90086-t
28. Kiki I, Gundogdu M, Alici HA, et al. A simple, safe and effective approach to prevent postdural puncture headache: epidural saline injection. Eurasian J Med. 2009;41(3):175–179.
29. n f T-K, Eslami B, Marzony SG, et al. Injection of intrathecal normal saline in decreasing postdural puncture headache. J Anesth. 2014;28(2):206–209. doi:10.1007/s00540-013-1683-8
30. Patel R, Urits I, Orhurhu V, et al. A comprehensive update on the treatment and management of postdural puncture headache. Curr Pain Headache Rep. 2020;24(6):24. doi:10.1007/s11916-020-00860-0
31. Cognat E, Koehl B, Lilamand M, et al. Preventing post-lumbar puncture headache. Ann Emergency Med. 2021;78(3):443–450. doi:10.1016/j.annemergmed.2021.02.019
32. Thon JN, Weigand MA, Kranke P, et al. Efficacy of therapies for post dural puncture headache. Curr Opin Anaesthesiol. 2024;37(3):219–226. doi:10.1097/aco.0000000000001361
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.