")
Back to Journals » Journal of Pain Research » Volume 18
Efficacy of Acupuncture and Pharmacotherapy for Migraine Prophylaxis: A Systematic Review and Meta-Analysis
Authors Liu AR, Zhu Q , Li J, Cao Y, Pei T, Shi L
Received 1 February 2025
Accepted for publication 7 May 2025
Published 17 May 2025 Volume 2025:18 Pages 2521—2540
DOI https://doi.org/10.2147/JPR.S519846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
An Rong Liu1 *, Qian Zhu1 *, Jingyi Li,1 Yufei Cao,1 Tian Pei,1 Lei Shi2
1First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, People’s Republic of China; 2Center for Acupuncture in Brain Disease Treatment, Jinjiang Hospital of Traditional Chinese Medicine, Jinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Shi, Center for Acupuncture in Brain Disease Treatment, Jinjiang Hospital of Traditional Chinese Medicine, 1105 Quanan Middle Road, Jinjiang, Quanzhou, Fujian, 362200, People’s Republic of China, Email [email protected]
Purpose: This meta-analysis aimed to systematically evaluate the efficacy and safety of acupuncture compared to conventional oral medications for the prophylactic treatment of migraine, following the PRISMA guidelines.
Methods: Comprehensive searches of international and Chinese databases were conducted up to January 2024 using terms such as “migraine” and “acupuncture”. Two researchers independently screened studies and extracted data. Following the refinement of the inclusion criteria during the revision process, only studies focusing on the prophylactic treatment of migraine were included in the final analysis. The primary outcomes included migraine intensity, frequency of migraine attacks, number of migraine days, and the proportion of patients achieving at least a 50% reduction in migraine days. The secondary outcomes included migraine duration, the overall effective rate, and the overall effective rate at 6 months follow-up. Meta-analyses were conducted using RevMan 5.3.
Results: Nineteen randomized controlled trials (2296 patients) were included. Compared to conventional medication, acupuncture was associated with greater reductions in frequency of migraine attacks (SMD = – 0.17, 95% CI [– 1.05, – 0.37]; P < 0.0001), migraine intensity (MD = – 1.48, 95% CI [– 2.51, – 0.46]; P = 0.005), number of migraine days (MD = – 1.50, 95% CI [– 2.52, – 0.48]; P = 0.004), and migraine duration (SMD = – 0.60, 95% CI [– 0.81, – 0.40]; P < 0.00001). A higher proportion of patients achieved at least a 50% reduction in migraine days (RR = 2.08, 95% CI [1.22, 3.55]; P = 0.007). Acupuncture also showed a higher overall effective rate (RR = 1.25, 95% CI [1.16, 1.35]; P < 0.00001) and overall effective rate at 6 months follow-up (RR = 1.34, 95% CI [1.19, 1.50]; P < 0.00001), with fewer adverse events reported. However, the overall quality of evidence was moderate to low.
Conclusion: Acupuncture may offer potential benefits in the prophylactic treatment of migraine; however, substantial heterogeneity across studies, methodological limitations, and the moderate to low quality of evidence limit the certainty of these findings. Further high-quality randomized controlled trials are needed to confirm these results.
Keywords: acupuncture, pharmacotherapy, migraine, meta-analysis, systematic review
Introduction
Migraine is a prevalent neurological disorder typically characterized by moderate to severe, often but not always unilateral, pulsating headache. Without treatment or with ineffective treatment, attacks typically last 4 to 72 hours and are often accompanied by nausea, vomiting, photophobia, and phonophobia.1 As per the 2016 Global Burden of Diseases (GBD) study,2 Migraine is the second most common neurological disabling disease. More recent data from the 2021 GBD study further highlight its substantial health burden, particularly among women of reproductive age (15–49 years). In 2021, the global prevalence of migraine in this population was approximately 493.94 million, with 33.33 million new cases and 18.25 million disability-adjusted life years (DALYs).3 However, historical data reveals a concerning trend: In China, merely 52.9% of migraine sufferers seek medical consultation, with a mere 13.8% receiving accurate diagnoses from physicians.4 Presently, oral pharmacotherapy approaches to migraine management primarily comprise two facets: preventive measures during remission periods and analgesic interventions during attacks. While the efficacy of pharmaceuticals is established, the potential side effects accompanying their administration warrant careful consideration;5 As pointed out in the 2022 edition of the Chinese Guidelines for the Diagnosis and Treatment of Migraine,5 nonsteroidal anti-inflammatory drugs (NSAIDs), as one of the pharmacological options for acute migraine management, are commonly associated with gastrointestinal adverse effects, and in some cases, gastrointestinal bleeding. Triptans, another class of medications for acute relief, may induce adverse effects such as fatigue, weakness, and delayed responsiveness. In the prophylactic setting, β-blockers (eg, propranolol, metoprolol), widely recommended for migraine prevention, are associated with adverse effects including fatigue, hypotension, bradycardia, and depressive symptoms. Flunarizine, a calcium channel antagonist, commonly triggers lethargy and weight gain. The antiepileptic medication topiramate may cause drowsiness, cognitive and language impairments, and paresthesia. Amitriptyline, a tricyclic antidepressant frequently used for migraine prophylaxis, is associated with drowsiness, weight gain, dry mouth, and constipation. Beyond medication-induced complications, instances of migraine compounded by medication overuse headaches can arise from the excessive consumption of analgesic drugs. Beyond medication-related adverse effects, long-term and frequent reliance on acute-phase analgesic medications for treatment may trigger medication overuse headache (MOH).6 Acupuncture, a key component of traditional Chinese medicine, has been proven to have definitive efficacy in pain alleviation.7,8 In the management of migraine, acupuncture can be utilized in two distinct therapeutic strategies: acute treatment, which focuses on alleviating pain during migraine attacks, and prophylactic treatment, which aims to prevent recurrent episodes and reduce the frequency and severity of migraine.5,9,10 Thus, the number of clinical trials of acupuncture therapy for migraine has increased in recent years. Considering the differences between these two therapeutic approaches, this study focuses exclusively on evaluating the efficacy of acupuncture in the prophylactic treatment of migraine. To further validate the efficacy of acupuncture compared with conventional medicine, we conducted a meta-analysis of randomized controlled trials using pharmacotherapy as a control, aiming to provide more evidence-based medical support for acupuncture in the prophylactic treatment of migraine.
Method
Study Design and PRISMA Compliance
This systematic review and meta-analysis were conducted in accordance with PRISMA guidelines to ensure comprehensive and transparent reporting. The study protocol was registered in PROSPERO (CRD42024521428). The PRISMA 2020 checklist was followed, and the study selection process is illustrated using a PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA flow diagram showing the study selection process. Abbreviations: CNKI, China National Knowledge Infrastructure; CQVIP, Chongqing VIP; CBM, China Biology Medicine. |
Inclusion Criteria
Type of Study
Randomized controlled trials (RCTs) conducted in Chinese or English were eligible for inclusion in this study. Only studies evaluating the prophylactic treatment of migraine were included. The trials were clinical, with the exclusion criterion being a sample size of fewer than 20 participants. No constraints were imposed regarding the implementation of blinding techniques.
Treatment Targets
Patients who met the migraine diagnostic criteria established by the International Headache Society were enrolled.1,5 The study population included individuals diagnosed with migraine, migraine without aura, migraine with or without aura, and chronic migraine. No restrictions were placed based on age, gender, race, or disease duration.
Intervention Measure
In the treatment arm, participants received either manual acupuncture or electroacupuncture alone, or acupuncture combined with a placebo intervention. In contrast, the control cohort underwent either sole pharmacotherapy or a combination of pharmacotherapy with sham acupuncture, the latter targeting non-head and non-meridian acupoints to ensure the integrity of blinding. Only studies using comparable acupuncture techniques (manual acupuncture or electroacupuncture) were included to ensure the consistency of interventions.
Result Type
In consideration of the clinical relevance of outcome measures, endpoints were categorized into primary and secondary outcomes. Primary outcomes focused on migraine intensity, frequency of migraine attacks, number of migraine days and the proportion of patients achieving at least a 50% reduction in migraine days. Migraine intensity was measured using a 10-cm Visual Analogue Scale (VAS), where 0 indicated “no pain” and 10 indicated “worst pain”. Participants indicated the severity of their headache attacks by marking the scale, and the scores were quantified accordingly. Migraine frequency was defined as the number of migraine attacks occurring within a specified time period (eg, per month), whereas migraine days were defined as the number of days during which migraine symptoms were experienced, regardless of the number of attacks per day. The frequency of migraine attacks was calculated on a monthly or 4-week basis, the number of migraine days was determined based on the number of days with migraine attacks in the month preceding each assessment time point. Frequency of migraine attacks and number of migraine days were primarily assessed through patient-reported outcomes, typically recorded in headache diaries where available; in studies where the use of headache diaries was not explicitly stated, data were extracted based on reported methods and were assumed to reflect retrospective recall unless otherwise specified. Secondary outcomes included migraine duration, the overall effective rate, and overall effective rate at 6 months follow-up. Migraine duration was defined as the average duration of each migraine episode, recorded in hours. The effective rate was defined as the proportion of patients categorized as cured, markedly effective, or effective. Studies were eligible if they reported an effective rate based on explicit clinical efficacy criteria, with preference given to those following the Guiding Principles of Clinical Research on New Drugs of Traditional Chinese Medicine,11 although alternative but comparable definitions were also accepted. Long-term efficacy was assessed based on patient outcomes six months after the end of treatment.
Exclusion Criteria
(1) Participants excluded from the study encompassed those failing to meet migraine diagnostic criteria, individuals with undetermined diagnoses, or those experiencing other forms of headaches.
(2) Both the experimental and control groups underwent a combination of interventions, including massage, bloodletting, cupping, acupoint injection, Chinese herbal medicine, and additional therapies.
(3) Exclusions comprised duplicate publications or literature containing overlapping content.
(4) Literature exhibiting conspicuous data inaccuracies was omitted from the analysis.
Literature Retrieval
From the inception of the database until January 2024, a comprehensive search strategy was implemented, encompassing eight prominent databases: Cochrane, PubMed, Embase, Web of Science, China Biomedical Literature Database (CBM), China Journal Full Text Database (CNKI), Chinese Science and Technology Journal Database (VIP), and Wanfang Database. Systematic searches were conducted employing the MeSH thesaurus, amalgamating subject terms with free terms such as “migraine”, “chronic migraine”, “migraine with aura”, “migraine without aura”, “acupuncture”, “body acupuncture”, and “electroacupuncture”. Furthermore, English search terms like “Migraine”, “Migraine Disorder”, “Migraine Headache”, “Acupuncture Therapy”, and “Acupuncture Treatment” were utilized to broaden the search scope, taking PubMed as an example, its detailed search formula is as follows “(((((((((((((((((((((((((((((((((((Disorder, Migraine[Title/Abstract]) OR (Disorders, Migraine[Title/Abstract])) OR (Migraine Disorder[Title/Abstract])) OR (Migraine[Title/Abstract])) OR (Migraines[Title/Abstract])) OR (Migraine Headache[Title/Abstract])) OR (Headache, Migraine[Title/Abstract])) OR (Headaches, Migraine[Title/Abstract])) OR (Migraine Headaches[Title/Abstract])) OR (Acute Confusional Migraine[Title/Abstract])) OR (Acute Confusional Migraines[Title/Abstract])) OR (Migraine, Acute Confusional[Title/Abstract])) OR (Migraines, Acute Confusional[Title/Abstract])) OR (Status Migrainosus[Title/Abstract])) OR (Hemicrania Migraine[Title/Abstract])) OR (Hemicrania Migraines[Title/Abstract])) OR (Migraine, Hemicrania[Title/Abstract])) OR (Migraines, Hemicrania[Title/Abstract])) OR (Migraine Variant[Title/Abstract])) OR (Migraine Variants[Title/Abstract])) OR (Variant, Migraine[Title/Abstract])) OR (Variants, Migraine[Title/Abstract])) OR (Sick Headache[Title/Abstract])) OR (Headache, Sick[Title/Abstract])) OR (Headaches, Sick[Title/Abstract])) OR (Sick Headaches[Title/Abstract])) OR (Abdominal Migraine[Title/Abstract])) OR (Abdominal Migraines[Title/Abstract])) OR (Migraine, Abdominal[Title/Abstract])) OR (Migraines, Abdominal[Title/Abstract])) OR (Cervical Migraine Syndrome[Title/Abstract])) OR (Cervical Migraine Syndromes[Title/Abstract])) OR (Migraine Syndrome, Cervical[Title/Abstract])) OR (Migraine Syndromes, Cervical[Title/Abstract])) OR (“‘Migraine Disorders’”[Mesh])) AND (((((((((((Acupuncture Treatment[Title/Abstract]) OR (Acupuncture Treatments[Title/Abstract])) OR (Treatment, Acupuncture[Title/Abstract])) OR (Therapy, Acupuncture[Title/Abstract])) OR (Pharmacoacupuncture Treatment[Title/Abstract])) OR (Treatment, Pharmacoacupuncture[Title/Abstract])) OR (Pharmacoacupuncture Therapy[Title/Abstract])) OR (Therapy, Pharmacoacupuncture[Title/Abstract])) OR (Acupotomy[Title/Abstract])) OR (Acupotomies[Title/Abstract])) OR (“‘Acupuncture Therapy’”[Mesh]))”
Study Selection and Data Extraction
The study selection followed PRISMA guidelines, with a PRISMA-compliant flowchart illustrating the inclusion and exclusion process. Data extraction was performed independently by two researchers, following the PRISMA checklist to ensure transparency and reproducibility. Initially, titles and abstracts were perused for preliminary assessment, followed by a comprehensive examination of the full-text articles for confirmation. Subsequently, the researchers exchanged their screening findings, resolving discrepancies through deliberation or recourse to a third-party arbiter when necessary. Two individuals independently extracted data, encompassing a comprehensive array of parameters, including study particulars, intervention modalities, diagnostic criteria, efficacy evaluation standards, outcome measures, and follow-up data. A third party meticulously scrutinized the data extraction process to ensure consistency and accuracy.
Assessment of Risk Bias
Two researchers independently evaluated the risk of bias using the “Risk of Bias” tool as outlined in the Cochrane Handbook 5.2. The assessment encompassed eight dimensions: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other sources of bias. Study bias was categorized as unclear, low, or high. Any assessment disparities were resolved through discourse or adjudication by a third party.
GRADE Quality of Evidence Evaluation
The quality of outcome indicators was assessed utilizing the GRADE methodology, restricting inclusion to randomized controlled trials. Consequently, evidence quality was categorized into four grades: high, moderate, low, or very low, adhering to the GRADE framework criteria. This comprehensive evaluation considered five key factors: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Two researchers independently appraised the evidence quality for each outcome using GRADEpro software, facilitating the generation of systematic tables.
Data Synthesis and Statistical Analysis
Meta-analysis was conducted utilizing RevMan 5.3 software provided by the Cochrane Collaboration. For dichotomous data, relative risk (RR) with corresponding 95% confidence intervals (CI) was employed, while mean difference (MD) was utilized for continuous data when measurements were in the same unit, and standardized mean difference (SMD) when measurements varied in units. Heterogeneity among included results was assessed using the χ2 test (significance threshold set to 0.1), complemented by I2 statistics for further evaluation. A P-value > 0.1 and I2 < 50% indicated minimal heterogeneity, warranting the adoption of the fixed-effect model; conversely, the random-effects model was applied. The outcomes included in the meta-analysis were migraine intensity (measured by a 10-cm Visual Analogue Scale [VAS]), frequency of migraine attacks (number of attacks per month or 4-week period), number of migraine days (number of days with migraine symptoms per month), migraine duration (average hours per episode), overall effective rate, and overall effective rate at 6 months follow-up. For continuous outcomes measured on the same scale (eg, VAS scores, migraine duration in hours), mean difference (MD) was used; for continuous outcomes measured on different scales across studies, standardized mean difference (SMD) was used. For dichotomous outcomes (eg, overall effective rate, ≥50% reduction in migraine days), relative risk (RR) with 95% confidence intervals was calculated. When pooling data, outcome measurements were extracted at the primary endpoint after treatment completion. If multiple time points were reported, the latest available time point after treatment was used for analysis. A random-effects model was applied when significant heterogeneity was detected (P ≤ 0.1 or I² ≥ 50%), while a fixed-effect model was used when heterogeneity was minimal.
Result
Research Selection
A systematic search of eight electronic databases yielded 7744 records. After removing duplicates and screening titles, abstracts, and full-text articles according to the eligibility criteria,19 studies were included in the final analysis, of which 14 were published in Chinese and 5 in English, as shown in the PRISMA flow diagram (Figure 1).
Research Characteristics
Basic Characteristics of the Included Literature
A total of 19 clinical randomized controlled trials were included in the analysis, all featuring a dual-arm design. All included studies investigated the prophylactic treatment of migraine, and no studies focusing on the acute treatment of migraine attacks were retained after applying the refined inclusion criteria. Four10,12–14 were multicenter randomized controlled trials. Additionally, one trial14 employed a single-blind, double-simulated, randomized controlled methodology. Notably, in this trial, the location of the “placebo acupuncture point” is 3 mm further to the side of the point in the TCM reference book which is unrelated to headache and is located near the elbow and knee joints. The trial originated from Germany,12 while another hailed from Italy,10 with the remainder conducted in China.13–29 The total sample size across all trials amounted to 2296 cases, with the largest trial comprising 207 cases and the smallest containing 28 cases. Within the treatment group, 1212 cases received filiform needle acupuncture, of which 229 underwent electroacupuncture. In the control group, 1065 patients were treated with pharmacotherapy, including nimodipine (n = 372), flunarizine hydrochloride (n = 483), metoprolol (n = 55), and topiramate (n = 33). One study employed a combination therapy of nimodipine and flunarizine hydrochloride (n = 61). Among the migraine subtypes investigated in the studies, six10,12,15,16,24,28 specifically targeted migraine with or without aura, while seven13,14,18,19,25,29 focused solely on migraine without aura. One27 addressed chronic migraines, and the remaining seven17,20–23,26 did not distinctly specify migraine type. Notably, four studies10,12,14,27 mandated participants to maintain a headache diary, documenting particulars such as headache duration, intensity, and utilization of emergency medication. Furthermore, eight studies10,12–14,26–28 meticulously recorded participant dropout rates. The characteristics of trials included are shown in Table 1.
 |
Table 1 Characteristics of the Included Studies in the Meta-Analysis |
Evaluation of Therapeutic Efficacy Criteria
Among the included studies, 1313,15–20,22–26,29 incorporated the overall effective rate as a key efficacy evaluation metric. Calculation of the overall effective rate was standardized across eight studies,15,18,19,22,25–27,29 adhering to the guidelines outlined in the Clinical Guidelines for New Chinese Medicines. Specifically, these studies employed the Nimodipine scoring method: (pre-treatment migraine score - post-treatment migraine score) divided by pre-treatment migraine score, multiplied by 100%. Clinical cure denotes the absence of migraine attacks throughout the treatment duration. A significant effect is indicated by a reduction of more than 50% in the migraine score post-treatment. Effectiveness is recognized when the migraine score decreases by 21% to 50% following treatment. Conversely, an outcome is deemed invalid if the migraine score decreases by less than 20% after treatment. Three studies16,17,24 adhered to the diagnosis and efficacy evaluation criteria for headaches established by the National Collaborative Group of Brain Diseases and Emergencies under the State Administration of Traditional Chinese Medicine in 1992. These studies calculated efficacy as follows: percentage of efficacy = [(pre-treatment headache index - post-treatment headache index) / pre-treatment headache index] multiplied by 100%. Basic recovery signifies an efficacy percentage ranging from 90% to 100% two months post-treatment. An obvious effect is characterized by an efficacy percentage falling between 55% and less than 90%. Effectiveness is recognized when the efficacy percentage ranges from 20% to less than 55%. Conversely, ineffectiveness is indicated when the efficacy percentage is less than 20%. Conversely, ineffectiveness is indicated when the efficacy percentage is less than 20%. One study20 referenced the diagnostic and therapeutic evaluation criteria for migraines proposed by Sun Zenghua, Yang Yujin, and others. In this study, cure was defined as the absence of episodic migraine symptoms at the conclusion of the treatment regimen, with no recurrence observed for one month thereafter. A significant effect was identified when symptom severity decreased by more than 50% post-treatment. Effectiveness was recognized when symptom severity decreased by 20% to 50% post-treatment. Conversely, an outcome was deemed invalid if the reduction in symptom severity was less than 20% post-treatment. One study13 employed the nimodipine method for scoring points, calculated as follows: points scoring method = [(pre-treatment points value - post-treatment points value) divided by treatment period points value] multiplied by 100%. Clinical control was defined as the absence of migraine attack symptoms at the conclusion of the treatment regimen, with no recurrence observed for one month after treatment cessation. A significant effect was noted when there was a reduction of more than 50% in points after treatment. Effectiveness was recognized when there was a reduction of 20% to 50% in points after treatment. Conversely, ineffectiveness was indicated by a reduction of less than 20% in points after treatment. Furthermore, it should be noted that the overall effective rate and the overall effective rate at 6 months follow-up were primarily derived from studies conducted in China. Most of these studies followed the Guiding Principles of Clinical Research on New Drugs of Traditional Chinese Medicine or comparable national standards, where an improvement of 20% to 50% is classified as “effective”, and an improvement of less than 20% is considered “ineffective”. This differs from internationally recognized standards, where a 30% improvement is typically regarded as the threshold for effectiveness. This methodological difference should be carefully considered when interpreting the results.
Risk of Bias in the Included Study
Judged through the lens of the Cochrane “risk of bias” tool, the methodology of random assignment varied across the studies under scrutiny. Five studies18,21,22,25,28 employed random number tables, while four10,13,14,27 opted for computer-generated randomized lists. Additionally, two studies12,16 employed stratified randomization. In contrast, eight studies15,17,19,20,23,24,26,29 merely made passing reference to randomization without specifying the methodology employed. This diversity underscores the need for clarity and transparency in reporting the specifics of random assignment methodologies. In the realm of concealed allocation strategies, four studies13,14,18,28 employed sequentially numbered, sealed, and opaque envelopes. Meanwhile, two studies12,27 implemented randomization centrally. However, details regarding allocation concealment were absent in the remaining 13 studies.10,15–17,19–26,29 Regarding blinding procedures, one study14 ensured patient blinding, while six studies10,12–14,25,27,28 secured blinding for outcome assessors. Concerning the comprehensiveness of study data, six pilot studies12–14,26–28 exhibited data incompleteness. Among these, two studies14,27 addressed missing values by substituting data from previous instances, while the remaining four12,13,26,28 restricted analysis to patients with complete datasets. Notably, one study14 displayed variance in result indicators compared to the prior protocol, whereas clarity on this aspect was lacking in the remaining studies. Moreover, sources of potential bias across all studies remained ambiguous. The risk of bias evaluation for the included studies is delineated in Figures 2 and 3.
 |
Figure 2 Risk of bias summary: review authors’ judgments about each risk of bias item for each included study. |
 |
Figure 3 Risk of bias graph: review authors’ judgments about each risk of bias item across all included studies. |
Results of the Study
To ensure consistent interpretation across different outcome measures, reductions in migraine intensity, frequency of attacks, number of migraine days, and migraine duration were considered beneficial, while increases in the proportion of patients achieving a ≥50% reduction in migraine days, in the overall effective rate, and in the overall effective rate at 6-month follow-up were also regarded as beneficial. Forest plots were constructed accordingly: for outcomes where reductions were beneficial, results favoring acupuncture were located on the left side of the plot; for outcomes where increases were beneficial, results favoring acupuncture are located on the right side. This approach ensures a consistent interpretation of beneficial effects across different outcome types.
Main Results
Frequency of Migraine Attacks
Six studies10,12,13,17,20,21 encompassing 697 participants compared the frequency of migraine attacks between the acupuncture group and the medication group. Due to significant heterogeneity among the studies (P=0.0004; I² =78%), a random-effects model was applied. The overall effect is depicted on the left side of the forest plot. The summary analysis indicates that the acupuncture group outperforms the medicine group in reducing the frequency of migraine attacks (SMD=−0.17, 95% CI [−1.05, −0.37]; P<0.0001), as illustrated in Figure 4.
 |
Figure 4 Forest plot comparing acupuncture with pharmacotherapy in reducing the frequency of migraine attacks. |
Migraine Intensity
Three studies14,21,28 presented findings on migraine intensity among migraine sufferers treated with acupuncture compared to those receiving medicine. Involving 314 participants, the studies utilized the Visual Analog Scale (VAS) to measure migraine intensity. Statistical analysis revealed a significant reduction in VAS scores within the acupuncture group post-treatment (MD = –1.48, 95% CI [–2.51, –0.46]; P = 0.005). However, notable heterogeneity was observed (P = 0.001; I2 = 85%), as depicted in Figure 5.
 |
Figure 5 Forest plot comparing acupuncture with pharmacotherapy in reducing migraine intensity. |
Given the significant heterogeneity observed in the outcome indicator of migraine intensity, a subgroup analysis was conducted to explore potential sources of variability. All three included studies focused on migraine prophylaxis. However, in the study by Zeng et al,21 although flunarizine 5 mg daily was used as a preventive treatment, patients were required to be enrolled during an acute migraine attack. In contrast, the other two studies did not specifically require patients to be enrolled during an acute migraine attack. Considering this difference in patient enrollment criteria, subgroup analyses were performed. Notably, the heterogeneity within the subgroup without acute enrollment requirements was negligible (P = 0.62; I² = 0%), suggesting that the different enrollment conditions, specifically the inclusion of patients during an acute migraine attack in Zeng et al, may have been the primary source of the observed heterogeneity, as illustrated in Figure 6.
 |
Figure 6 Forest plot of subgroup analysis based on enrollment criteria for migraine intensity. |
Number of Migraine Days
Four studies,12,14,27,28 comprising 425 participants, examined the efficacy of acupuncture versus medicine in reducing the number of migraine days. Significant heterogeneity among the studies was observed (P = 0.009; I2 = 74%), leading to the adoption of a random-effects model. The collective effect is illustrated on the left side of the forest plot, demonstrating that the acupuncture group exhibited greater efficacy in reducing the number of migraine days compared to the medicine group (MD = –1.50, 95% CI [–2.52, –0.48]; P = 0.004). These findings are detailed in Figure 7.
 |
Figure 7 Forest plot comparing acupuncture with pharmacotherapy in reducing the number of migraine days. |
Proportion of Patients Achieving at Least a 50% Reduction in Migraine days
A comparison of the proportion of patients achieving at least a 50% reduction in migraine days between those treated with acupuncture therapy and medication was conducted across three trials,12,14,27 involving a total of 319 participants. Noteworthy heterogeneity between studies was detected (P = 0.06; I2 = 65%), necessitating the utilization of a random-effects model. The aggregate effect is depicted on the right side of the forest plot, revealing that the acupuncture group outperformed the medicine group in improving the proportion of patients achieving at least a 50% reduction in migraine days (RR = 2.08, 95% CI [1.22, 3.55]; P = 0.007), as illustrated in Figure 8.
 |
Figure 8 Forest plot comparing acupuncture with pharmacotherapy in the proportion of patients achieving at least a 50% reduction in migraine days. |
Secondary Outcome
Migraine Duration
An assessment of the migraine duration was undertaken across three trials,13,20,21 encompassing a total of 372 participants, comparing acupuncture therapy to medication. Notable heterogeneity among the studies was observed (P = 0.95; I2 = 0%), prompting the adoption of a random-effects model. The collective impact is portrayed on the right side of the forest plot, indicating that the acupuncture group surpassed the medicine group in reducing the migraine duration (SMD = −0.60, 95% CI [−0.81, −0.40]; P <0.00001), as delineated in Figure 9.
 |
Figure 9 Forest plot comparing acupuncture with pharmacotherapy in reducing migraine duration. |
The Overall Effective Rate
Thirteen studies,13,15–20,22–26,29 encompassing a total of 1670 participants, evaluated the total effective rate as an outcome measure. Data synthesis involved amalgamating instances of cure, significant improvement, and effectiveness as documented in the literature and subsequently computing the total effective rate based on the aggregated data. Substantial heterogeneity across studies was observed (P = 0.004; I² = 59%), prompting the adoption of a random-effects model. The collective impact is depicted on the right side of the forest plot. The Summary analysis indicates that the acupuncture group demonstrates a superior overall effective rate in migraine treatment compared to the medication group (RR = 1.25, 95% CI [1.16, 1.35]; P < 0.00001), as illustrated in Figure 10.
 |
Figure 10 Forest plot comparing acupuncture with pharmacotherapy in improving the overall effective rate. |
To explore potential sources of heterogeneity, subgroup analyses were conducted based on (1) the type of acupuncture intervention (manual acupuncture vs electroacupuncture) and (2) whether the control group medication complied with guideline recommendations. Subgroup analysis based on intervention type (Figure 11) showed that both manual acupuncture and electroacupuncture were associated with a higher overall effective rate compared to medication, with similar effect sizes. Subgroup analysis based on pharmacotherapy guideline compliance (Figure 12) revealed that acupuncture remained superior in both subgroups; however, studies using non-pharmacotherapy -recommended medications exhibited slightly higher effect sizes than those using guideline-recommended medications. These findings suggest that differences in acupuncture techniques and control group medication selection may have contributed to the observed heterogeneity, but did not substantially alter the overall conclusion that acupuncture is more effective than pharmacotherapy in improving the total effective rate for migraine prophylaxis.
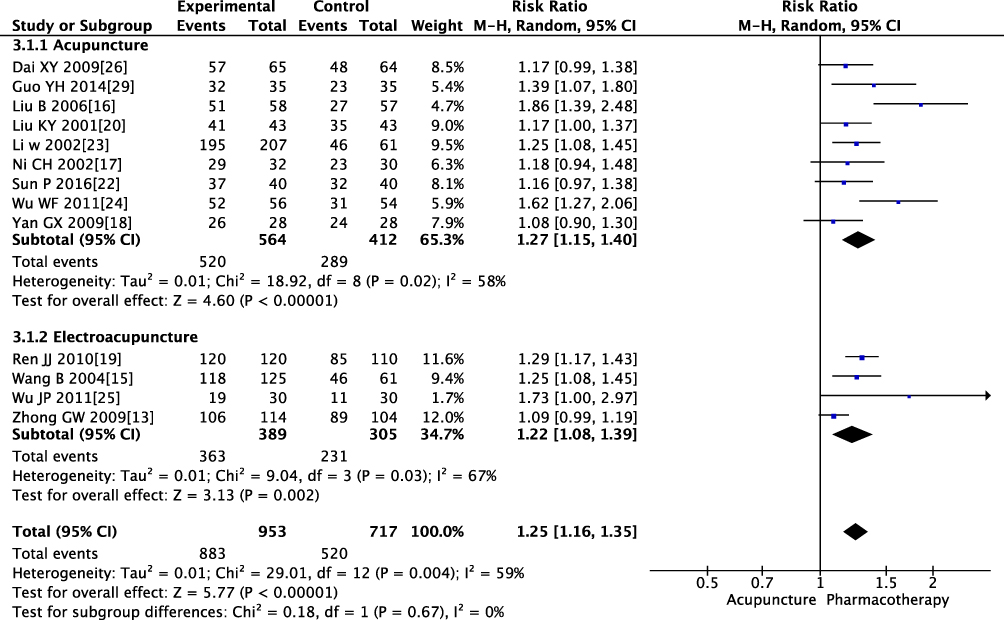 |
Figure 11 Subgroup analysis of overall effective rate based on acupuncture intervention type (manual acupuncture vs electroacupuncture). |
 |
Figure 12 Subgroup analysis of overall effective rate based on pharmacotherapy guideline compliance. |
Overall Effective Rate at 6 months Follow-up
Three studies,13,16,22 encompassing 413 participants, compared the clinical efficacy of acupuncture with that of medication over a 6-month treatment period. The data processing method involved combining the cases of cured, markedly effective, and effective treatments recorded at 6 months post-treatment into a total effective treatment count, as documented in the literature. The overall efficacy rate was then calculated based on the recorded data. The studies demonstrated homogeneity (P=0.19; I²=39%), justifying the use of a fixed-effects model. The pooled analysis, depicted in Figure 8, revealed a significant advantage of the acupuncture group over the medication group in terms of overall effective rate at 6-month follow-up (RR = 1.34, 95% CI [1.19, 1.50]; P < 0.00001), as illustrated in Figure 13.
 |
Figure 13 Forest plot comparing acupuncture with pharmacotherapy for overall effective rate at 6-month follow-up. |
Publication Bias
In this study, the number of included trials for the outcome measure of overall effective rate exceeded 10, allowing for the construction of a funnel plot to assess publication bias. The resulting plot exhibited an asymmetrical distribution, as illustrated in Figure 14, indicating the presence of publication bias. This asymmetry suggests the potential existence of unpublished trials with negative results.
 |
Figure 14 Funnel plot assessing publication bias for the outcome of overall effective rate. |
GRADE Evaluation of Outcome Indicators
The quality of evidence for the outcome indices was assessed using GRADEpro filer 3.6 software, comparing acupuncture with pharmacotherapy. Due to various biases, inconsistencies, and inaccuracies, the quality of evidence for migraine duration, number of migraine days, and overall effective rate at 6 months follow-up was classified as moderate. The evidence level for the overall effective rate, the proportion of patients achieving at least a 50% reduction in migraine attack days, and the outcome index of frequency of migraine attacks were deemed low. Additionally, the evidence level for the migraine intensity outcome index was very low. Refer to Figure 15 for detailed information.
 |
Figure 15 Summary of GRADE quality assessment for primary and secondary outcomes. |
Discussion
Summary of Main Results
Based on an analysis of the results from the 19 included studies, acupuncture was more effective than pharmacotherapy in reducing the frequency of migraine attacks, migraine intensity, the number of migraine days, and migraine duration. Additionally, acupuncture demonstrated a higher overall effective rate as well as a superior overall effective rate at 6 months follow-up compared to pharmacotherapy. However, the substantial heterogeneity among the included studies, along with imprecision and various biases, downgraded the level of evidence for outcomes such as the frequency of migraine attacks, migraine intensity, number of migraine days, proportion of patients achieving at least a 50% reduction in migraine days, and the overall effective rate. Therefore, more standardized studies are required to validate these findings further. It should be emphasized that all included studies focused on migraine prophylaxis, and no studies on acute treatment were retained after applying the refined inclusion criteria.
Possible Interpretations of the Results
The interventions across the included studies encompassed both manual acupuncture and electroacupuncture, while therapies such as bloodletting, moxibustion, and acupoint injection were excluded. The control groups utilized various pharmacotherapies, including calcium channel blockers, β-blockers, and antiepileptic drugs, with differences in dosages across trials. Variations in intervention types, migraine subtypes, and outcome evaluation criteria likely contributed to the observed heterogeneity. In addition, although two studies permitted the use of acute-phase pharmacotherapies such as ergots (eg, ergotamine-caffeine) during migraine attacks to provide acute symptom relief. These treatments were administered only for acute symptom relief and were not part of the prophylactic interventions. Moreover, it is noteworthy that some control group interventions, such as the use of nimodipine or ergotamine-caffeine, are not aligned with current international or Chinese migraine management guidelines, which may further impact the comparability and generalizability of the results. Although the included studies utilized comparable acupuncture techniques (manual acupuncture or electroacupuncture), minor variations in stimulation parameters, such as frequency, intensity, treatment duration, and acupoint selection protocols, may have contributed to clinical heterogeneity. This heterogeneity may have affected the robustness and interpretability of the pooled results.
The Quality of Evidence
Overall, the quality of evidence in the included studies was influenced by the consistency of outcome measures, heterogeneity in interventions, and methodological limitations. The primary outcome measures, including migraine intensity assessed by a 10-cm Visual Analog Scale, frequency of migraine attacks, number of migraine days, and duration of migraine episodes, were generally standardized across studies. Data were primarily collected through headache diaries or retrospective patient recall when diaries were not available. However, while most studies adopted the same clinical efficacy evaluation criteria for secondary outcomes such as the overall effective rate, a few studies used alternative definitions, which may have contributed to some inconsistency. Notably, all studies employed Chinese evaluation systems rather than international diagnostic criteria. In addition, differences in acupuncture modalities, treatment frequencies, and course durations across studies may have contributed to clinical heterogeneity. The methodological quality of the included trials was generally low. Many studies lacked clear reporting of randomization methods, allocation concealment, and blinding, thereby increasing the risk of bias. Only one study14 achieved patient blinding through a double-dummy design. Most included trials focused on short-term efficacy, and only a few studies reported long-term outcomes assessed six months after treatment cessation, limiting the ability to evaluate the sustained benefits of acupuncture. In addition, deviations in control group interventions from guideline-recommended therapies may have further compromised the overall quality of evidence.
Potential Bias
In this study, a systematic search was conducted across eight Chinese and international databases, employing subject terms in conjunction with free terms, supplemented by manual searches. However, it is important to acknowledge the possibility that additional trials, either unpublished or missed in the search, might exist, potentially introducing publication bias. Moreover, in the assessment of the total effective rate and long-term effects, all included literature was sourced from Chinese publications, adhering solely to the relevant evaluation criteria in China. Some studies did not specify whether headache diaries were used; and if outcomes were based on retrospective recall, recall bias may have affected the reliability of the results. Additionally, the number of studies included in the analysis of certain outcome indicators was relatively limited. These factors may potentially influence the reliability and generalizability of the results. Although two of the included studies were conducted in Europe (Germany and Italy), most studies were conducted in China. This geographical concentration may limit the generalizability of the findings. Future multicenter randomized controlled trials across diverse populations are necessary to validate these results. Furthermore, although information on treatment frequency, duration, and run-in phases was extracted and summarized, most included studies did not explicitly report a run-in or baseline observation period. The lack of detailed run-in phase reporting may have limited the comparability of baseline conditions across studies and introduced potential bias into the pooled results.
Safety
Five studies12–14,27,28 documented adverse reactions and side effects. Common adverse reactions in the acupuncture group included localized pain, sensory abnormalities, and post-needle removal bleeding at the acupuncture site. Conversely, common side effects in the pharmacotherapy group encompassed drowsiness, weight gain, and fatigue. Notably, no participants in the acupuncture group withdrew from the study due to adverse reactions. However, in the pharmacotherapy group, some patients had to reduce the dosage or discontinue participation due to medication-related adverse events.
Inspiration for Clinical Practice
In this review, acupuncture demonstrated a lower incidence of adverse events compared to conventional pharmacotherapy, suggesting that it may be a safer treatment option for specific populations, such as pregnant or lactating women and individuals preferring non-pharmacological interventions. Moreover, some patients withdrew immediately after randomization upon learning that they had been assigned to the pharmacotherapy group, indicating a strong baseline preference for acupuncture treatment. Strong pre-existing preferences might enhance treatment outcomes, as positive patient expectations have been reported to exert a favorable influence on pain relief,30 which may represent an additional advantage of acupuncture therapy for migraine management. However, current migraine management guidelines still predominantly recommend pharmacotherapy, possibly due to the limited quantity and moderate to low quality of supporting evidence for acupuncture.
Inspiration for Clinical Research
Although this review comprehensively evaluated the efficacy and safety of acupuncture compared to conventional pharmacotherapy in migraine patients, certain limitations in existing clinical studies should be noted. Most included trials had relatively short treatment and follow-up durations, with limited reporting on Overall effective rate at 6 months follow-up after treatment cessation. Future randomized controlled trials (RCTs) should extend follow-up periods, adopt standardized diagnostic criteria for migraine, and apply consistent outcome measures to better assess the long-term preventive effects of acupuncture. Additionally, the design of placebo acupuncture remains a methodological challenge in migraine research. In the included studies, one trial14 used superficial needling or skin penetration at head acupoints or non-acupoints as a placebo. However, both methods may have inadvertently produced therapeutic effects. Validated sham acupuncture devices, such as the Streitberger needle,31 offer established strategies to optimize blinding in acupuncture trials, and future studies should consider adopting these or similar methods to enhance the methodological rigor and credibility of acupuncture research for migraine management.
Conclusion
Although the findings of this meta-analysis suggest that acupuncture may have potential advantages over conventional pharmacotherapy in migraine prophylaxis, the interpretation of these results should be approached with caution. The included studies exhibited considerable heterogeneity in acupuncture techniques and control interventions, and the overall quality of evidence was moderate to low due to methodological limitations, inconsistency, and potential publication bias. Therefore, while acupuncture appears to be a promising option for the preventive treatment of migraine, further rigorously designed, large-scale, and high-quality randomized controlled trials are necessary to validate these conclusions and better define its role in clinical practice.
Data Sharing Statement
In accordance with PRISMA guidelines, the availability of study materials is reported as follows: The template data collection forms and data extracted from included studies are not publicly available but can be provided upon reasonable request. The summary data used for all analyses are included in the manuscript and Supplementary Materials, while raw data may be shared upon request. The analytic code is not publicly available; however, all statistical analyses were conducted using RevMan 5.3, with methodological details outlined in the manuscript. Additionally, the PRISMA checklist is available in the Supplementary Materials. For further inquiries or access to specific materials, please contact the corresponding author.
Acknowledgments
An Rong Liu and Qian Zhu are co-first authors for this study. Thanks to all the participants and clinical researchers involved in the publications cited in this review.
Funding
This article was supported by grants from the Chinese State Administration of TCM (2019XZZX-ZJ013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
2. Feigin VL, Nichols E, Alam T, Global. regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
3. Cen J, Wang Q, Cheng L, Gao Q, Wang H, Sun F. Global, regional, and national burden and trends of migraine among women of childbearing age from 1990 to 2021: insights from the Global Burden of Disease Study 2021. J Headache Pain. 2024;25(1):96. doi:10.1186/s10194-024-01798-z
4. Liu R, Yu S, He M, et al. Health-care utilization for primary headache disorders in China: a population-based door-to-door survey. J Headache Pain. 2013;14(1):47. doi:10.1186/1129-2377-14-47
5. Association NBot CM; Association HaSDPCoCRH. Chinese guidelines for the diagnosis and treatment of migraine (2022 Edition). Chin J Pain Med. 2022;28(12):881–898.
6. Ailani J, Burch RC, Robbins MS. The American Headache Society Consensus Statement: update on integrating new migraine treatments into clinical practice. Headache. 2021;61(7):1021–1039. doi:10.1111/head.14153
7. Patil S, Sen S, Bral M, et al. The role of acupuncture in pain management. Curr Pain Headache Rep. 2016;20(4):22. doi:10.1007/s11916-016-0552-1
8. Shen FJ, Xu J, Zhan YJ, Fu QH, Pei J. Acupuncture for migraine: a systematic review and meta-analysis review. World Journal of Acupuncture - Moxibustion. 2019;29(1):7–14. doi:10.1016/j.wjam.2019.03.004
9. Li Y, Liang F, Yang X, et al. Acupuncture for treating acute attacks of migraine: a randomized controlled trial. Headache. 2009;49(6):805–816. doi:10.1111/j.1526-4610.2009.01424.x
10. Allais G, De Lorenzo C, Quirico PE, et al. Acupuncture in the prophylactic treatment of migraine without aura: a comparison with flunarizine. Headache. 2002;42(9):855–861. doi:10.1046/j.1526-4610.2002.02203.x
11. Zheng X. Guidelines for Clinical Research of New Traditional Chinese Medicines (Trial). Vols. 105-109. China Medical Science and Technology Press; 2002.
12. S A, L K, H A, et al. Effectiveness and tolerability of acupuncture compared with metoprolol in migraine prophylaxis. Headache. 2006;46(10):1492–1502. doi:10.1111/j.1526-4610.2006.00598.x
13. Zhong GW, Li W, Luo YH, et al. Acupuncture at points of the liver and gallbladder meridians for treatment of migraine: a multi-center randomized and controlled study journal article. Zhongguo Zhen Jiu. 2009;29(4):
14. Wang LP, Zhang XZ, Guo J, et al. Efficacy of acupuncture for migraine prophylaxis: a single-blinded, double-dummy, randomized controlled trial Journal article. Pain. 2011;152(8):
15. Wang B. Nape multiple acupuncture plus surrounding acupuncture for migraine. Shanghai J Acu-Mox. 2004;23(4):14–5.
16. Bo L, Limin Q. Clinical studies on treatment of migraine by acupuncture TaiYang(EX-HN5) And FengChi(GB20). Clinical studies on treatment of migraine by puncturing Taiyang(EX-HN5) and Fengchi(GB20). Liaoning Zhongyi Zazhi. 2006;33(11):2006360832.
17. Chenghao N. 32 cases of migraine without aura treated by opening the “Si-Guan Points”. Shanghai Zhongyiyao Daxue Xuebao. 2002;16(4):24–25
18. Ga-xi Y, Jing M. Acupuncture at points of lesser yang meridians for treatment of migraine. Liaoning Zhongyiyao Daxue Xuebao. 2009;11(12):134–135.
19. Jianjun R. Acupuncture treatment for 120 cases of migraine. Shanghai J Acu-Mox. 2010;29(11):731
20. Keying L, Liu X, Chengfu M, Peisen Q, Ping Z. Comparative study on clinical therapeutic effects of acupuncture and medicine on migraine. Zhongguo Zhen Jiu. 2001;21(9):515–517
21. Linghong Z, Gang L. Effect of acupuncture in migraine patients and its influence on serum MMP – 2 activity. Liaoning Zhongyi Zazhi. 2015;42(10):1971–1974.
22. Pei S, Yue L. Effect of acupuncture therapy based on multiple – needle shallow needling at ashi pointon cephalagra with syndrome of qi and blood deficiency. JCAM. 2016;(6):49–51.
23. Wei L, Ganchu D, Yuanzhen L, et al. Clinical study on acupuncture of liver and gallbladder meridian points for the treatment of 207 cases of migraine. JTCM. 2002;43(11):824–825
24. Wenfeng W, Fan H. 56 cases of migraine treatment with balance acupuncture. JETCM. 2011;20(6):2011683343.
25. Wu JP, Gu SZ. Randomized controlled clinical trials for acupuncture treatment of aura-absence migraine patients journal article. Zhen CI yan jiu. 2011;36(2):
26. Xiaoyu D, Yuanhao D. Acupuncture treatment of 65 cases of migraine using the method of regulating the mind and relieving stress. Shaanxi Zhongyi. 2009;30(9):1220–1221
27. Yang CP, Chang MH, Liu PE, et al. Acupuncture versus topiramate in chronic migraine prophylaxis: a randomized clinical trial Journal article. Cephalalgia. 2011;31(15):
28. Yiwen C, Jian P, Qinhui F, et al. Electroacupuncture at Siguan points for migraine of liver yang hyperactivity: a randomized controlled trial. Zhongguo Zhen Jiu. 2022;42(05):498–502. doi:10.13703/j.0255-2930.20210403-0001
29. Yuhong G, Xiaohong D, Xiuying T, Weiwei Y, Zhongqiu L. Clinical study on the treatment of migraine without aura with head and body acupuncture therapy. JCAM. 2014;30(8):18–20
30. Bausell RB, Lao L, Bergman S, Lee WL, Berman BM. Is acupuncture analgesia an expectancy effect? Preliminary evidence based on participants’ perceived assignments in two placebo-controlled trials. Eval Health Prof. 2005;28(1):9–26. doi:10.1177/0163278704273081
31. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998;352(9125):364–365. doi:10.1016/S0140-6736(97)10471-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bibliometric of Trends on Acupuncture Research About Migraine: Quantitative and Qualitative Analyses
He K, Zhan M, Li X, Wu L, Liang K, Ma R
Journal of Pain Research 2022, 15:1257-1269
Published Date: 28 April 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024