")
Back to Journals » Journal of Pain Research » Volume 18
Efficacy of Selective Nerve Root Block for Different Types of Lumbar Disc Herniation: Study Protocol for a Single-Blind, Prospective Cohort Study
Authors Tan H , Zhou J , Pu Y , He L , Wang L
Received 4 September 2024
Accepted for publication 23 February 2025
Published 28 February 2025 Volume 2025:18 Pages 1035—1043
DOI https://doi.org/10.2147/JPR.S494496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Hongping Tan,1,* Jing Zhou,2,* Yijin Pu,1 Lin He,1 Liu Wang3
1Department of Pain Management, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China; 2Department of Neurology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China; 3Department of Pain Medicine, The Second Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530007, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liu Wang, Email [email protected]
Background: Lumbar disc herniation (LDH) is a common cause of low back pain and radiculopathy. Selective Nerve Root Block (SNRB) has been widely used as a treatment for LDH; however, its efficacy across different types of LDH remains unclear. This study aims to evaluate the clinical efficacy of SNRB in treating various LDH subtypes, classified according to the Michigan State University (MSU) classification system, and to explore its potential as a safe and minimally invasive percutaneous treatment option.
Methods: This is a single-blind, Prospective Cohort Study. A total of 200 patients diagnosed with LDH will be recruited and allocated into 10 groups (20 patients per group) based on their MSU classification (1-A, 1-B, 1-C, 2-AB, 2-A, 2-B, 2-C, 3-AB, 3-A, and 3-B). All patients will receive SNRB treatment under fluoroscopic guidance. Primary outcomes will include the Visual Analogue Scale (VAS) for pain intensity. Secondary outcomes will include the Oswestry Disability Index (ODI), health-related quality of life (Short Form-36, SF-36) and average weekly analgesic consumption. Assessments will be conducted at baseline, 1 day, 1 week, 2 weeks, 1 month, 3 months, 6 months, and 1 year post-treatment.
Discussion: This study will provide high-quality evidence on the efficacy of SNRB in different LDH subtypes, classified according to the MSU system. The findings will guide clinical decision-making and promote the adoption of SNRB as a minimally invasive, safe, and effective treatment option for LDH.
Trial Registration: This clinical trial is registered on the Chinese Clinical Trial Registry platform (ChiCTR) at https://www.chictr.org.cn/index.html, identifier: ChiCTR2200067212.
Keywords: lumbar disc herniation, selective nerve root block, prospective cohort study, pain management, MSU classification
Background
Lumbar disc herniation (LDH) is a prevalent condition characterized by the displacement of the intervertebral disc material beyond the normal confines of the disc space, resulting in compression or irritation of the adjacent neural structures.1 LDH is a major cause of low back pain and radiculopathy, leading to significant disability and reduced quality of life.2 Conservative treatments, such as over-the-counter analgesics, physical therapy, manipulation, and traction interventions, are often the first-line approach for managing LDH.3–5 However, when conservative measures fail, minimally invasive interventional techniques, such as selective nerve root block (SNRB), have been employed to alleviate symptoms and improve function.6,7
SNRB, also known as selective paravertebral nerve block (SPNB), is a targeted procedure in which local anesthetics and corticosteroids are injected around the affected spinal nerve root.6 This technique aims to reduce inflammation, provide analgesia, and promote healing of the affected neural structures.8 Several studies have demonstrated the effectiveness of SNRB in managing LDH-related pain and disability.9–11 However, the efficacy of SNRB in treating different types of LDH, classified based on the Michigan State University (MSU) classification system, remains unclear.
The MSU classification system categorizes LDH into different types based on the morphology, location, and extent of the herniation, and is used to guide surgical strategies for LDH.12,13 The MSU classification system categorizes lumbar disc herniations into three subgroups (1, 2, and 3) based on size/morphology, and three zones (A, B, and C) according to their location on axial T2-weighted MRI. Zone A refers to the central-paracentral region within the spinal canal, Zone B corresponds to the intraforaminal space (within the neural foramen), and Zone C extends beyond the foramen into the extraforaminal region. When the herniation spans both A and B zones, it is designated “-AB”, such as 2 - AB or 3 - AB.12 This classification provides a standardized approach to describe LDH and guides clinical decision-making.14 Evaluating the efficacy of SNRB in treating different MSU types of LDH will provide valuable insights into the role of this intervention in the management of LDH.
This single-blind, Prospective Cohort Study aims to evaluate the clinical efficacy of SNRB in treating different types of LDH classified using the MSU system and to explore a safe percutaneous treatment option. The findings of this study will guide clinical practice and potentially promote the use of SNRB as a targeted treatment approach for LDH.
Methods
Study Objectives
The primary objective of this study is to evaluate the clinical efficacy of SNRB in treating different types of LDH classified using the MSU system. The secondary aims are to assess the safety of SNRB and to identify any potential differences in treatment response based on the specific MSU type of LDH.
Study Design
This is a single-blind, Prospective Cohort Study conducted at the Pain Department of the Affiliated Hospital of North Sichuan Medical College. The study protocol has been approved by the Medical Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (Ethics Approval No.: 2022ER492-1) and registered with the China Clinical Trial Registry (Registration No.: ChiCTR2200067212).
Patients will be categorized into 10 cohorts based on their MSU classification (1-A, 1-B, 1-C, 2-AB, 2-A, 2-B, 2-C, 3-AB, 3-A, and 3-B), ensuring adequate representation of all LDH subtypes.12,15 All patients will receive SNRB under fluoroscopic guidance.
Given the morphological heterogeneity of LDH, the MSU classification system provides a structured framework for subgroup analysis. Stratifying patients into 10 distinct MSU-based groups allows for a more precise evaluation of SNRB efficacy across different disc herniation patterns. This natural grouping reflects real-world clinical practice and allows for the comparison of treatment responses across LDH subtypes and ensures sufficient statistical power and clinical relevance.
To assess treatment efficacy, all participants will undergo eight scheduled assessments at the following time points: baseline (pre-treatment), 1 day, 1 week, 2 weeks, 1 month, 3 months, 6 months, and 1 year post-treatment. The study schematic and follow-up schedule are presented in Figure 1 and Table 1.
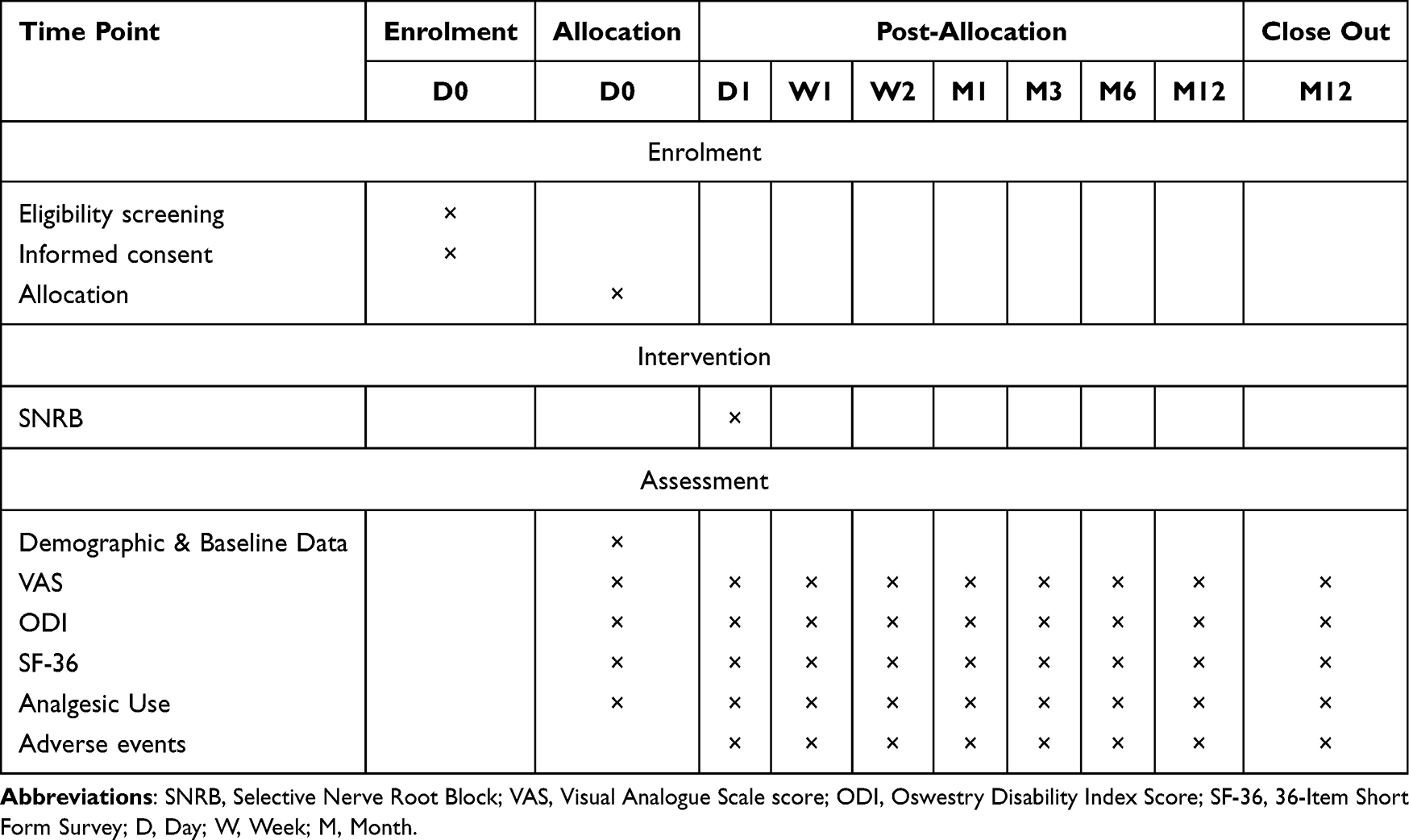 |
Table 1 Time Schedule of Participant Enrolment, Allocation and Assessment |
 |
Figure 1 Trials flow diagram of the trial. |
This study will be conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice (ICH-GCP) guidelines.
Participants
Inclusion Criteria
- Patients diagnosed with LDH based on clinical symptoms, physical examination, and imaging findings (MRI or CT)
- Presence of lumbago or lower extremity radiating pain, with positive signs and imaging data consistent with the clinical presentation
- Age ≥18 years
- Willing to provide written informed consent and agree to the use of their data for analysis in this study
- No contraindications to the drugs used in this study
Exclusion Criteria
- Presence of severe cardiovascular, respiratory, hepatic, or renal diseases
- Clear indications for surgical intervention
- Pregnancy or lactation
- Coagulation disorders or other hematological diseases
- Recurrent disc prolapse
- Radiculopathy caused by infection or skin infection at the puncture site
Dropout Criteria
Participants may be withdrawn from the study if they meet any of the following criteria:
- Participant requests to withdraw from the study
- Participant experiences a serious adverse event that precludes further participation
- Participant requires surgical intervention for LDH during the study period
- Participant is lost to follow-up, defined as missing two consecutive study visits without prior notification
- Participant becomes pregnant during the study period
- Participant develops a significant medical condition that interferes with the study procedures or outcomes
- Participant is non-compliant with the study protocol, defined as failing to adhere to the study requirements after two verbal reminders
Participants’ data will be strictly protected, using unique participant identification codes to ensure anonymity. All data handling will comply with the General Data Protection Regulation (GDPR) and local data privacy regulations. Participants may withdraw from the study at any time, and this will not affect their routine medical care.
Randomization Method
Randomization
This study is a prospective cohort study; therefore, no randomization procedures will be employed. Participants will be allocated to one of the 10 groups based on their MSU classification of LDH. The allocation will be performed by the research coordinators in a consecutive manner, ensuring an equal number of participants in each group.
Blinding Method
This study employs a single-blind design. The participants, outcome assessors, and data analysts will be blinded to the MSU classification-based group allocation to minimize assessment bias. However, the treating physicians will not be blinded due to the nature of the procedure, as they are responsible for performing the SNRB intervention under fluoroscopic guidance.
Data Handling and Analysis Blinding
Data collection and entry will be handled by an independent data management team. Statisticians performing the data analysis will remain blinded to treatment group allocations until the database is locked.
Interventions
All participants will receive a single SNRB intervention performed by experienced interventional physicians with at least 5 years of expertise in spinal interventions. The decision to perform a single intervention was based on previous studies demonstrating the effectiveness of a single SNRB in treating LDH.16,17 Additionally, this approach was chosen to allow a clear evaluation of treatment effects and to minimize potential complications associated with repeated invasive procedures.18
- Patient Positioning & Injection Site: Patients will be placed in a prone position on a radiolucent table with a pillow under the abdomen to reduce lumbar lordosis. The target nerve root level (L3, L4, L5, or S1) will be determined based on MRI/CT imaging and the patient’s clinical symptoms. Skin preparation will be performed using povidone-iodine and sterile draping.
- Needle Placement & Approach: A 22-gauge spinal needle will be inserted using a transforaminal approach, targeting the ventral aspect of the nerve root sleeve in the paravertebral space at the affected level. Under fluoroscopic guidance, the needle will be advanced towards the posterior aspect of the intervertebral foramen, ensuring accurate placement. The positioning will be confirmed using anteroposterior (AP) and lateral views.
- Contrast Injection & Confirmation: After appropriate needle positioning, 1 mL of non-ionic contrast agent will be injected under real-time fluoroscopy to confirm proper spread around the target nerve root and to rule out intravascular or epidural injection.
- Injection Protocol: The injectate consists of 2 mL of 0.5% bupivacaine combined with 80 mg triamcinolone.7 Before administration, negative aspiration for blood or cerebrospinal fluid will be performed to rule out intravascular uptake, and the solution will then be slowly injected over 30–60 seconds.
- Post-procedure Monitoring & Follow-up: Patients are monitored for 30 minutes for adverse effects (eg, hypotension, transient weakness). (VAS, ODI, SF-36) are assessed at baseline and scheduled intervals up to 1 year.
- Rationale for Fluoroscopic Guidance: Fluoroscopic guidance was preferred over ultrasound or surface landmarks due to its superior needle placement accuracy and ability to visualize injectate spread.19 This approach minimizes the risk of complications, such as intravascular injection or inadvertent spinal cord injury, and ensures that the therapeutic solution reaches the intended site of action.
Outcomes
The baseline data of all participants will be collected either by searching the institution’s electronic medical records or by directly interviewing the participants prior to the SNRB intervention. Data retrieved from the electronic medical records will consist of demographic characteristics such as age, gender, and body mass index (BMI), medical history including the duration of LDH symptoms, previous treatments, and comorbidities, as well as imaging findings like MRI or CT results and the MSU classification of LDH. Data obtained directly from the patients will include pain intensity measured by the Visual Analogue Scale (VAS) score, functional disability evaluated by the Oswestry Disability Index (ODI) score, quality of life reflected by the SF - 36 questionnaire scores, physical examination findings such as the straight leg raise test results and the presence of sensory and motor deficits, and information about concomitant medications like analgesics, anti - inflammatory drugs, and muscle relaxants. All these data will be used for comparison with the post - intervention outcomes. The follow-up assessments include the following:
Primary Outcomes
Visual Analogue Scale (VAS): Patients will mark their current pain intensity on a 10-cm line anchored by “no pain” (0) and “worst imaginable pain” (10).20,21 A reduction of ≥2 points is considered clinically significant.
Secondary Outcomes
- Oswestry Disability Index (ODI): A validated Chinese version of the ODI questionnaire evaluates 10 domains of daily living (eg, pain impact on walking, sitting, sleeping). Each item is scored 0 (no disability) to 5 (maximal disability), with total scores converted to a percentage (0–100%).22,23
- SF-36 health Survey: Assesses eight health domains (Physical Functioning, Role-Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional, Mental Health). Scores are standardized to 0–100, with higher scores indicating better quality of life.24
Analgesic Use: Record specific medication names, and the mean quantity of each pain-relieving medication consumed on a weekly basis.
All outcome measures will be assessed at baseline, 1 day post-treatment, 1 week post-treatment, 2 weeks post-treatment, 1 month post-treatment, 3 months post-treatment, 6 months post-treatment, and 1 year post-treatment.
Adverse Events
Adverse events will be actively monitored and recorded throughout the study period. Participants will be instructed to report any adverse events to the study team, and these events will be assessed at each follow-up visit. The severity, duration, and potential relationship of the adverse event to the SNRB procedure will be documented. Common adverse events associated with SNRB may include injection site pain or tenderness, transient numbness or weakness in the lower extremity, vasovagal reactions (eg, dizziness, lightheadedness, or fainting), allergic reactions to the injectable medications, and infection at the injection site. Although serious adverse events such as nerve injury, spinal cord injury, or epidural hematoma are rare, they will be closely monitored. A detailed protocol has been established for the management of serious adverse events, including immediate medical intervention, reporting to the study’s Data and Safety Monitoring Board (DSMB) and the Institutional Review Board (IRB), and comprehensive documentation. All serious adverse events will be followed up until resolution or stabilization to ensure patient safety.
Sample Size Calculation
The sample size calculation for this study was based on detecting differences in pain scores between the MSU type groups after the SNRB intervention. Assuming a clinically meaningful difference of 2 points in the pain score, with a standard deviation of 3 points, a power of 80%, a significance level of 5%, and an allocation ratio of 1:1:1:1:1:1:1:1:1:1 for the 10 MSU type groups, and accounts for a potential dropout rate of 10%, a total sample size of 200 participants (20 per group) was calculated using PASS 15.0 (NCSS, LLC, Kaysville, UT, USA). This sample size also accounts for a potential dropout rate of 10%.
Data Collection and Management
Data will be collected using standardized electronic case report forms (eCRFs) and managed using a secure, web-based electronic data capture (EDC) system. The EDC system will have built-in data validation checks to ensure data accuracy and completeness. Access to the EDC system will be restricted to authorized study personnel, and all user activities will be logged for audit purposes.
The data management team, consisting of the study coordinator, data manager, and statistician, will be responsible for regular data monitoring and validation. They will review the eCRFs for missing data, inconsistencies, and outliers, and they will query the study sites for clarification or resolution of any data discrepancies.
All data will be stored on secure, password-protected servers with regular backup procedures in place. Confidentiality of participant data will be maintained through the use of unique participant identification numbers, and no personally identifiable information will be included in the study database. Data will be stored and handled in compliance with local regulations, the General Data Protection Regulation (GDPR), and the study’s data management plan.
At the conclusion of the study, the final dataset will be locked and securely archived. The locked dataset will be used for statistical analysis and will be accessible only to the study statistician and authorized investigators.
Statistical Analysis
Descriptive statistics will be used to summarize the baseline characteristics of the participants. Continuous variables will be presented as means with standard deviations (SDs) for normally distributed data or medians with interquartile ranges (IQRs) for non-normally distributed data. Categorical variables will be summarized using frequencies and percentages.
To evaluate the effectiveness of SNRB across different MSU classification groups, a mixed-effects model for repeated measures (MEM) will be used, with time as the within-subject factor and MSU type as the between-subject factor.
Post hoc pairwise comparisons between MSU subgroups at each follow-up time point will be performed using Bonferroni correction to adjust for multiple comparisons, reducing the risk of Type I errors.
An intention-to-treat (ITT) approach will be used for all analyses, ensuring that all enrolled participants are included. Missing data will be handled using multiple imputation (MI) with chained equations (MICE), assuming a Missing at Random (MAR) mechanism. Sensitivity analyses will be conducted to assess the robustness of the results under different missing data assumptions, including complete case analysis and best/worst-case scenario imputation.
All statistical analyses will be performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA). A two-sided p-value < 0.05 will be considered statistically significant. The results will be reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines for non-pharmacological interventions.
Discussion
This single-blind, Prospective Cohort Study aims to evaluate the clinical efficacy of SNRB in treating different types of LDH classified using the MSU system. The MSU classification provides a standardized approach to categorize LDH based on morphology, location, and extent, guiding clinical decision-making.12 By evaluating the efficacy of SNRB in treating different MSU types of LDH, this study will provide valuable insights into the role of this intervention in the management of LDH.
Although SNRB has been widely used for pain management in LDH, there is limited evidence comparing its efficacy across different MSU-classified LDH subtypes.19 Few studies have specifically analyzed the outcomes of SNRB based on MSU-classified disc herniation morphology and location.13 This study is unique in that it systematically evaluates the therapeutic response of SNRB in 10 distinct MSU subgroups, allowing for a more tailored approach to LDH treatment. Understanding the differential responses among MSU types will provide valuable insights into personalized treatment selection and optimization.
Additionally, prior research on interventional pain management techniques, such as ozone chemonucleolysis, has demonstrated variable success rates depending on the herniation subtype.25,26 However, whether these trends hold true for SNRB remains unexplored. By incorporating an MSU-based subgroup analysis, this study aims to clarify these distinctions and refine clinical decision-making regarding minimally invasive pain management strategies.This minimally invasive approach may help patients avoid or delay the need for surgical intervention, which is associated with higher costs and potential complications.27,28
While randomized controlled trials (RCTs) are considered the gold standard for comparing interventions, this cohort study design was chosen to evaluate the natural variation in SNRB efficacy across MSU subtypes; The cohort design allows for subgroup comparisons within a real-world clinical setting, avoiding ethical concerns related to withholding treatment for several practical and ethical reasons. First, strict randomization would require withholding treatment from certain MSU subtypes or administering alternative interventions, which may not be ethically justifiable given the known benefits of SNRB. Second, an MSU-based stratification ensures an adequate number of patients in each subgroup, facilitating more robust statistical analysis. Random allocation could lead to an uneven distribution of patients across MSU subtypes, which would weaken the power of subgroup comparisons. To minimize potential selection bias, consecutive allocation was employed, ensuring balanced group sizes while maintaining real-world applicability.
Limitations
This study has several limitations. First, the single-center design may limit the generalizability of findings, and future multi-center studies are needed to validate our results across diverse populations. Second, the 1-year follow-up period may be insufficient to assess long-term outcomes; extended follow-up could clarify whether treatment effects persist beyond this timeframe. Third, as a cohort study grouping patients by baseline MSU classification, residual confounding may persist despite adjustments for known factors (eg, age, symptom duration). While consecutive enrollment and outcome assessor blinding reduced selection and detection biases, unmeasured confounders (eg, psychosocial factors, subtle anatomical variations) could still influence outcomes. Finally, although this design aligns with real-world decision-making, randomized trials remain essential to isolate the specific effects of SNRB across MSU subtypes and establish causal relationships.
Conclusion
In conclusion, this study protocol describes a well-designed prospective cohort study that aims to evaluate the clinical efficacy of SNRB in treating different types of LDH classified using the MSU system. This study will provide valuable insights into the role of SNRB in managing LDH. Future studies are needed to validate its effectiveness and further refine minimally invasive treatment options.
Data Sharing Statement
The datasets generated and analyzed during the study will be available from the corresponding author upon reasonable request after the completion of the study. The data will be made available in accordance with the principles of data sharing and open access, while ensuring participant confidentiality.
Ethics Approval and Consent to Participate
The study protocol has been approved by the Medical Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (2022ER492-1). Written informed consent will be obtained from all participants prior to their enrollment in the study.
Trial Status
The trial is currently in the recruitment phase. Recruitment commenced in January 2023 and is expected to be completed by May 2025.
Consent for Publication
Not applicable, as no individual participant data will be published.
Acknowledgments
The authors would like to thank the study participants for their involvement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is funded by a grant from Affiliated Hospital of North Sichuan Medical College (2022LC017). The funding body had no role in the design of the study, collection, analysis, and interpretation of data, or in writing the manuscript.
Disclosure
The authors declare that they have no competing interests.
References
1. Kögl N, Petr O, Löscher W. et al. Lumbar Disc Herniation. Dtsch Arztebl Int. 2024;121(13):440–448. doi:10.3238/arztebl.m2024.0074
2. Zhang AS, Xu A, Ansari K, et al. Lumbar Disc Herniation: diagnosis and Management. Am J Med. 2023;136(7):645–651. doi:10.1016/j.amjmed.2023.03.024
3. Peck J, Urits I, Peoples S, et al. A Comprehensive Review of Over the Counter Treatment for Chronic Low Back Pain. Pain Ther. 2021;10(1):69–80. doi:10.1007/s40122-020-00209-w
4. Kim CH, Choi Y, Chung CK, et al. Nonsurgical treatment outcomes for surgical candidates with lumbar disc herniation: a comprehensive cohort study. Sci Rep. 2021;11(1):3931. doi:10.1038/s41598-021-83471-y
5. Yoon WW, Koch J. Herniated discs: when is surgery necessary? EFORT Open Rev. 2021;6(6):526–530. doi:10.1302/2058-5241.6.210020
6. Kanaan T, Abusaleh R, Abuasbeh J, et al. The Efficacy of Therapeutic Selective Nerve Block in Treating Lumbar Radiculopathy and Avoiding Surgery. J Pain Res. 2020;13:2971–2978. doi:10.2147/jpr.S276331
7. Kanna RM, Shetty AP, Rajasekaran S. Predictors of Successful Outcomes of Selective Nerve Root Blocks for Acute Lumbar Disc Herniation. Global Spine J. 2019;9(5):473–479. doi:10.1177/2192568218800050
8. Ii S H, Harmon PC, Noe C, et al. Transforaminal Epidural Steroid Injections: a Systematic Review and Meta-Analysis of Efficacy and Safety. Pain Physician. 2021;24(S1):S209–s232.
9. Riew KD, Yin Y, Gilula L, et al. The effect of nerve-root injections on the need for operative treatment of lumbar radicular pain. A prospective, randomized, controlled, double-blind study. J Bone Joint Surg Am. 2000;82(11):1589–1593. doi:10.2106/00004623-200011000-00012
10. Riew KD, Park JB, Cho YS, et al. Nerve root blocks in the treatment of lumbar radicular pain. A minimum five-year follow-up. J Bone Joint Surg Am. 2006;88(8):1722–1725. doi:10.2106/jbjs.E.00278
11. Karppinen J, Ohinmaa A, Malmivaara A, et al. Cost effectiveness of periradicular infiltration for sciatica: subgroup analysis of a randomized controlled trial. Spine. 2001;26(23):2587–2595. doi:10.1097/00007632-200112010-00013
12. Mysliwiec LW, Cholewicki J, Winkelpleck MD, et al. MSU classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection. Eur Spine J. 2010;19(7):1087–1093. doi:10.1007/s00586-009-1274-4
13. Li H, Xiao C, Pan H, et al. Surgical Strategy for Lumbar Disc Herniation based on the MSU Classification: percutaneous Endoscopic Lumbar Discectomy versus Transforaminal Lumbar Interbody Fusion: a 5-year Retrospective Study. Orthop Surg. 2024;16(8):1963–1973. doi:10.1111/os.14145
14. d’Ercole M, Innocenzi G, Ricciardi F, et al. Prognostic Value of Michigan State University (MSU) Classification for Lumbar Disc Herniation: is It Suitable for Surgical Selection? Int J Spine Surg. 2021;15(3):466–470. doi:10.14444/8068
15. Çelen ZE, Hanege F, Sarı S, et al. Medium- to long-term functional outcomes of artcure diffusional patch therapy for lumbar disc herniation: which herniation is more likely to require surgery? BMC Musculoskelet Disord. 2025;26(1):49. doi:10.1186/s12891-025-08314-7
16. Manchikanti L, Benyamin RM, Falco FJ, et al. Do Epidural Injections Provide Short- and Long-term Relief for Lumbar Disc Herniation? A Systematic Review. Clin Orthop Relat Res. 2015;473(6):1940–1956. doi:10.1007/s11999-014-3490-4
17. Ackerman III WE, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg. 2007;104(5):1217–1222. doi:10.1213/01.ane.0000260307.16555.7f
18. Benyamin RM, Manchikanti L, Parr AT, et al. The effectiveness of lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain. Pain Physician. 2012;15(4):E363–404. doi:10.36076/ppj.2012/15/E363
19. Viswanathan VK, Kanna RM, Farhadi HF. Role of transforaminal epidural injections or selective nerve root blocks in the management of lumbar radicular syndrome - A narrative, evidence-based review. J Clin Orthop Trauma. 2020;11(5):802–809. doi:10.1016/j.jcot.2020.06.004
20. Younger J, McCue R, Mackey S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep. 2009;13(1):39–43. doi:10.1007/s11916-009-0009-x
21. Chiarotto A, Maxwell LJ, Ostelo RW, et al. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients With Low Back Pain: a Systematic Review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
22. Smeets R, Köke A, Lin CW, et al. Measures of function in low back pain/disorders: low Back Pain Rating Scale (LBPRS), Oswestry Disability Index (ODI), Progressive Isoinertial Lifting Evaluation (PILE), Quebec Back Pain Disability Scale (QBPDS), and Roland-Morris Disability Questionnaire (RDQ). Arthritis Care Res. 2011;63(11):S158–173. doi:10.1002/acr.20542
23. Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940–2952. doi:10.1097/00007632-200011150-00017
24. Brazier JE, Harper R, Jones NM, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305(6846):160–164. doi:10.1136/bmj.305.6846.160
25. Leoni MLG, Caruso A, Micheli F. Factors Predicting Successful Outcome for Ozone Chemonucleolysis in Lumbar Disk Herniation. Pain Pract. 2021;21(6):653–661. doi:10.1111/papr.13006
26. Hosseini B, Taheri M, Sheibani K. Comparing the results of intradiscal ozone injection to treat different types of intervertebral disc herniation based on MSU classification. Interv Neuroradiol. 2019;25(1):111–116. doi:10.1177/1591019918800458
27. Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA. 2006;296(20):2451–2459. doi:10.1001/jama.296.20.2451
28. Rogerson A, Aidlen J, Jenis LG. Persistent radiculopathy after surgical treatment for lumbar disc herniation: causes and treatment options. Int Orthop. 2019;43(4):969–973. doi:10.1007/s00264-018-4246-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.