")
Back to Journals » Journal of Pain Research » Volume 18
Enhanced Recovery After Surgery (ERAS) Protocols in Orthopaedic Surgery: Opioids or Not Opioids?
Authors Grossi P
Received 4 October 2024
Accepted for publication 18 March 2025
Published 28 March 2025 Volume 2025:18 Pages 1683—1695
DOI https://doi.org/10.2147/JPR.S496891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Paolo Grossi
Department of Anesthesia, Intensive Care, and Pain Therapy, ASST Orthopaedic Traumatological Specialist Center G. Pini, Milan, Italy
Correspondence: Paolo Grossi, Email [email protected]
Abstract: Enhanced Recovery After Surgery (ERAS) protocols have transformed perioperative care in orthopaedic surgery, emphasising streamlined patient pathways for improved outcomes and treatment of chronic pain. Traditionally, opiates have been pivotal in managing postoperative (PO) pain and their efficacy in providing essential relief during the recovery phase is well-established. However, the evolving landscape of perioperative care, coupled with the opioid crisis and their association with chronic pain, has prompted a re-evaluation of their role. Orthopaedic ERAS protocols emphasise a multimodal approach to pain management, advocating for a reduction in opioid reliance. Alternative analgesic strategies, such as regional nerve blocks and non-opioid medications, are integrated into these protocols. Studies comparing opiates and opioid-free analgesia in orthopaedic ERAS are limited, making it challenging to establish a standardised approach. Some evidence suggests that opioid-free strategies, in some operating settings, may lead to improved recovery outcomes, reduced PO pain, and lower opioid consumption. However, in orthopaedics, evidence is inconclusive, necessitating further exploration. This review provides an overview of the development and multifaceted nature of ERAS protocols, which encompass a holistic approach to perioperative pain management and sustained pain relief, all while aiming to reduce the risks associated with opioid use. Striking the optimal balance between pain control and patient safety remains a priority, with the need for continued exploration and refinement of clinical guidelines in orthopaedics.
Keywords: postoperative pain management, orthopaedic surgery, chronic pain, ERAS protocols, opioids
Introduction
The enhanced recovery or “fast-track” surgical protocol was pioneered by the Danish surgeon Henrik Kehlet in 1997,1 for treating patients following colonic surgery.1,2 However, its scope has widened over time to encompass other surgical specialties, with the core objective of expediting postoperative (PO) recovery, reducing hospital stays, improving patient experiences, and superior clinical outcomes.3–12
In their earlier iterations, enhanced recovery protocols emphasized the pivotal role of nutrition management. This emphasis extended to preoperative preparation and PO period, recognising both phases as integral components of the program.4 Given the comprehensive expertise involved in the process of recovery, the optimization of multiple modalities and fostering relational coordination is crucial. The ERAS Society guidelines, through the collaboration of expert working groups, provide recommendations covering the entire spectrum from surgery planning to recovery.3–12 Seven ERAS Society guidelines exist for several procedures and classes of surgery (eg, colorectal, cystectomy for bladder cancer, pancreaticoduodenectomy, pelvic, gastrectomy, gynaecologic and bariatric surgery),3–12 with more guidelines currently under development. The ERAS Society guidelines provide an evidence-based, multimodal approach to surgical care, with the primary goals of minimizing physical derangement and the stress response following surgery, thereby reducing complication rates and shortening hospital stays (Table 1).13 Notably, in the field of orthopaedic surgery, enhanced recovery programs have been rapidly instituted and developed, particularly in elective hip and knee arthroplasty as well as elective spine surgery,14 to prevent the onset of persistent postsurgical pain.
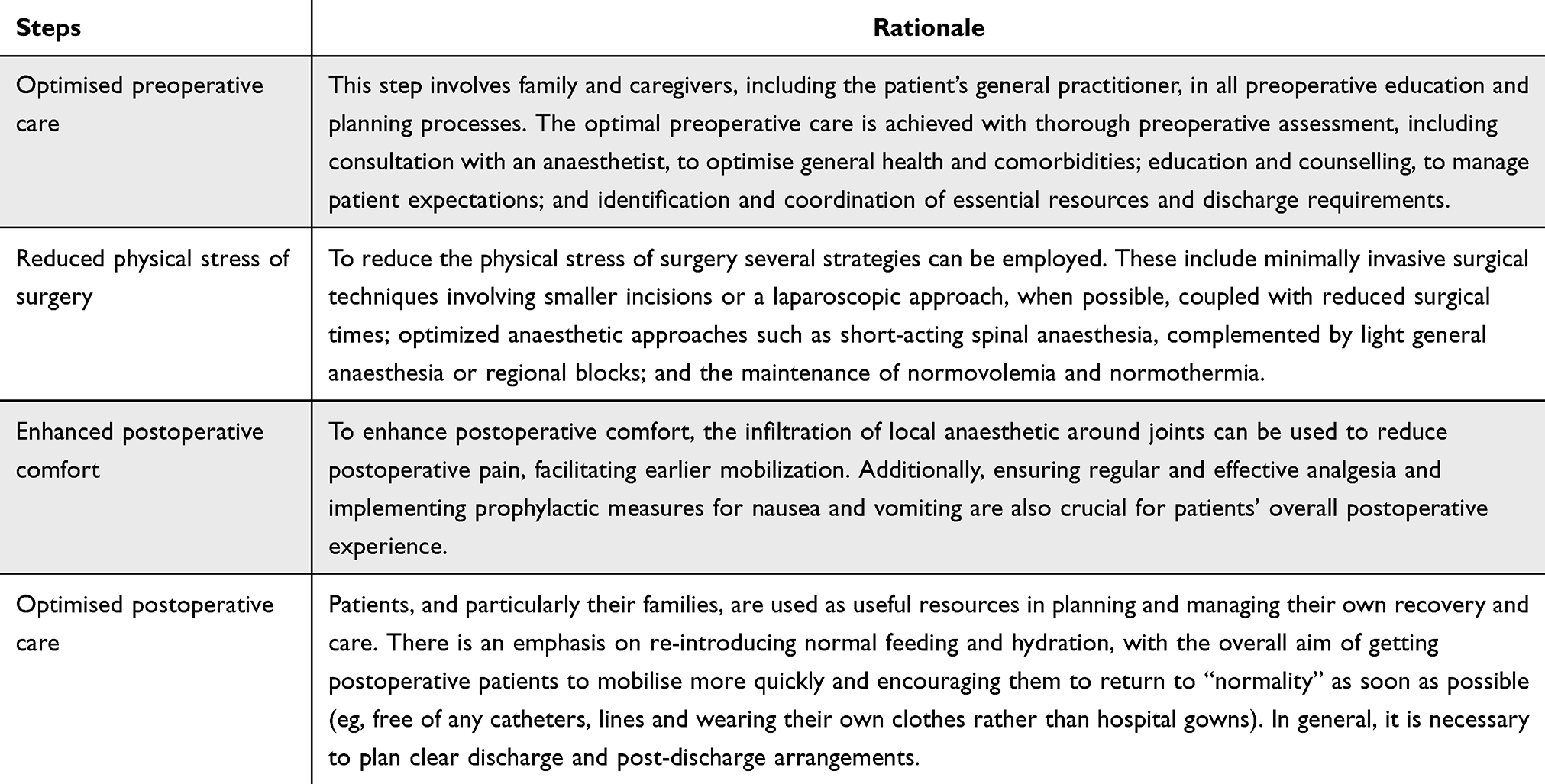 |
Table 1 The Four Key Elements That Characterise an ERAS Programme According to the NHS Institute for Innovation and Improvement (2008).13 |
Clinicians play a pivotal role in spearheading the development of ERAS protocols by collaborating with all other healthcare professionals engaged in the process. The success of ERAS protocols is thus contingent upon effective channels of communication and understanding within these partnerships.
Moreover, effective pain management is a cornerstone of these plans, and traditionally, opioids have been a primary component in addressing PO pain in orthopaedic patients. However, poorly managed pain protocols have prompted their excessive use with the induction of pathophysiologic changes such as tolerance, physical dependence, addiction, and the harmful effects of opioid-induced hyperalgesia (OIH) (ie, respiratory depression, nausea, emesis, itching, gastrointestinal dysfunction, and chronic pain), which have been associated with a considerable burden on patients’ quality of life.15–21 These adverse events also have an economic impact, as they are associated with increased hospital costs and longer lengths of stay.22 The acknowledgment that pain is a dynamic experience with diverse underlying causes and manifestations paves the way for simultaneous interventions that act through different pathways. The optimal role of opioids in perioperative pain management remains a subject of ongoing debate. To improve PO pain control, a multimodal analgesic approach is crucial, incorporating strategies such as regional anesthesia, nonsteroidal anti-inflammatory drugs (NSAIDs), and acetaminophen alongside opioids. This approach also aligns with the broader goals of ERAS protocols, focusing on minimising stress responses, optimising organ function, and expediting the return to normal activities.13 A comprehensive perioperative plan also encompasses strategies to reduce inflammation, accelerate wound healing and promote early mobilisation, as physical therapy and rehabilitation programmes, in conjunction with chronic pain management strategies, tailored to the specific needs of orthopaedic patients, are integral components. The benefits of this approach for orthopaedic patients include a decline in PO morbidity, rehabilitation time, and hospitalisation costs.23,24
Indicators and Strategies for Chronic Pain Prevention and Control
Acute pain has been frequently reported across a wide range of surgical procedures, even with the use of analgesic medications.25–31 PO pain is usually evaluated through questionnaires and surveys. A prospective German cohort study involving 50,523 patients across 179 surgical groups found that pain scores on the first PO day were highest following obstetric and orthopaedic/trauma surgeries. However, elevated pain levels were also noted after routine minor procedures, including appendectomy, cholecystectomy, hemorrhoidectomy, tonsillectomy, and certain laparoscopic surgeries.31 Apfelbaum et al, instead, conducted a national study in the United States by using telephone surveys conducted on a random sample of 250 adults who had previously undergone surgical procedures (either as an inpatient or as an outpatient);28 patients were asked about the severity of PO pain, analgesic medications, patient education and their satisfaction with the treatment. From the survey, it has emerged that morphine and meperidine were the most administered medications for inpatients (33% and 27% respectively), while acetaminophen with codeine or ibuprofen were the most administered for outpatients (23% and 15% respectively). Around 80% of patients reported experiencing acute pain following surgery.28 Of these, 86% described their pain as moderate, severe, or extreme, with a higher number of patients experiencing pain after discharge than before. PO pain emerged as the most frequent concern, with 59% of survey participants identifying it as their primary issue.28 The most frequently prescribed medications after surgery were acetaminophen with or without codeine (17%) for inpatients and acetaminophen with codeine (21%) or oxycodone with acetaminophen (20%) for outpatients. Of the patients who received pain medications, 23% experienced adverse effects (eg, drowsiness, nausea, and constipation); however, nearly 90% of them were satisfied with their analgesic medications.28 A more recent US national survey by Gan et al evaluated similar aspects on a random sample of 300 adults who had undergone surgery within the past five years.25 The findings revealed that approximately 86% of patients reported experiencing pain following surgery. Of these, 75% endured moderate to extreme pain during the immediate PO phase, and 74% continued to experience similar pain levels after being discharged.25 PO pain emerged as the most significant pre-surgical concern, with nearly half of the patients indicating high or very high levels of anxiety about pain before surgery. Additionally, approximately 88% of patients were prescribed analgesic medications for pain management. Opioids (hydrocodone, oxycodone, and morphine) were the most prescribed analgesics for managing PO pain. Of the patients receiving analgesic medications, 80% experienced adverse effects—such as drowsiness, nausea, and constipation—and 39% reported experiencing moderate-to-severe pain even after receiving their initial dose.25 Nonetheless, these studies had limitations, including a relatively small sample size, potential recall bias due to the time elapsed between the date of surgery and the date of the survey, and the inability to consider how the type of surgery and the use of intraoperative anaesthetics or analgesics might have affected the survey outcomes.
A relevant factor affecting the frequency and intensity of pain is the time elapsed after surgery. A Dutch study involving 1,490 surgical inpatients from various departments who were receiving PO pain management under an acute pain protocol, found that 41% of patients experienced moderate to severe pain on the day of surgery. This percentage gradually decreased to 30%, 19%, 16%, and 14% on PO days 1, 2, 3, and 4, respectively.29 In a study conducted by Chan et al, a questionnaire was administered to 174 patients who underwent total knee arthroplasty across 10 hospitals in Australia, two weeks post-discharge. The results revealed that 54% of these patients experienced severe pain at least occasionally during the first two weeks after returning home, while 23% experienced “severe/extreme” pain.30 Close to 70% of patients consumed opioids alone or in combination with non-opioid analgesics. However, 73% of patients reported receiving sufficient information about analgesics, while only 47% were informed about non-pharmacological pain relief methods. Furthermore, around 20% had negative perceptions about analgesic use, associated with the severity of the analgesic-related side effects like constipation and drowsiness.30 Increased pain intensity resulted in reduced patient satisfaction and a decrease in the amount of time spent walking daily. Many participants sought additional medical assistance to address their pain. In a systematic literature review that pooled data from 165 studies on acute pain following major surgeries (abdominal, thoracic, orthopaedic, and gynaecological), it was found that within the first 24 hours post-surgery, the mean incidence of moderate-to-severe pain was 30%, while severe pain occurred in 11% of cases.32 The frequency of these pain levels differed based on the analgesic technique used, with lower incidence reported for patient-controlled and epidural analgesia compared to intramuscular analgesia.32 Beyond the type of surgery and analgesic/anaesthetic approach, other factors predicting acute PO pain severity included younger age, female gender, preoperative pain, anxiety or mood disorders, and the size of the incision.33–40 In orthopaedics, worse pain at the surgical site on the day of surgery has been identified as a significant predictor of persistent opioid use over six months in patients undergoing total knee or hip arthroplasty.41 Additionally, data from a large national registry analysed by Franklin et al revealed that greater pain at the operated joint, reported one year after total knee arthroplasty, was associated with continued opioid use 12 months after the surgery.42
Despite an increased focus and the establishment of new standards for perioperative pain management, numerous patients still endure significant pain following surgical procedures. PO pain is frequently underestimated and undertreated, with short- and long-term sequelae.43,44 A survey from 2006 on PO pain therapy in 34 Italian hospitals gave a quite disturbing picture, confirming not only the low use of opioids, but also the wide use of NSAIDs drugs without gastroprotective agents, and the absence of a real multimodal therapy.45 It is noteworthy that 20% of patients did not receive any pain medication during the entire PO period and patient-controlled analgesia and regional anaesthesia were used less frequently than in another national study (the RICALOR study).46 Thus, additional efforts are necessary to enhance patients’ PO pain experiences. Poorly managed acute pain following surgery is known to potentially lead to the development of chronic pain. The consequences of inadequate pain control during or after surgery may include adverse effects, such as toxicity from prolonged or high-dose anaesthetic medications. As a result, effective pain management is a key quality improvement objective on individual, institutional, and societal levels.47 According to a substantial body of research, persistent pain affects between 10% and 60% of patients after common surgeries.48–53 Chronic pain is defined as lasting at least two months post-surgery, extending beyond the normal healing period, without an identifiable cause.48,49,54 Therefore, reducing perioperative pain frequency and severity, and preventing its progression to chronic pain, is crucial and may require a comprehensive, multifaceted approach. One of the factors implicated in the onset of persistent post-surgical pain may be linked to either acute or chronic exposure to opioids. These analgesics work by binding to opioid receptors—specifically μ, Κ, δ, and opioid-like receptor type 1 (ORL1)—which are found in peripheral tissues, the spinal cord, and various regions of the brain, affecting multiple organ systems.55 Opioid-induced analgesia requires inhibition at both the dorsal horn of the spinal cord and supraspinal circuits for effective systemic relief. However, neurons in the rostral ventral medulla, sensitive to opioids, also facilitate hyperalgesia.55 As opposed to opioid tolerance, where increased doses are necessary to achieve the same effect, OIH refers to an increase in widespread pain, without another explanation, that can worsen or improve with changes in opioid dosage.55 Given the high rates of opioid use in the perioperative period, strategies to mitigate the risk of developing chronic PO pain should be employed throughout this timeframe. These strategies include opting for surgical techniques that minimize the risk of tissue or nerve injury and inflammation when possible.56 Additionally, during the preoperative assessment, identifying patients who may be at higher risk of developing pain during or after surgery is crucial. Implementing an ERAS protocol, which starts with a comprehensive physical, emotional, and psychological evaluation, can help alleviate surgical stress.57–59 Furthermore, selecting appropriate perioperative analgesic or anaesthetic approaches is essential to reducing pain and limiting noxious stimuli that can lead to peripheral and central sensitization.38,48,60–65
Local anaesthetics are commonly used during surgical procedures as supplementary measures to control acute pain and decrease the need for analgesics. However, there is a limited amount of research evaluating their impact on subsequent PO outcomes, such as the development of chronic postsurgical pain and overall quality of life.66–70 One study investigated the efficacy of a tumor necrosis factor-alpha inhibitor for inguinal hernia repair compared to a placebo,67 while another trial assessed the effects of pregabalin versus placebo in a cardiac surgery model.68 Additionally, a third study explored the use of minocycline, a broad-spectrum tetracycline antibiotic known to inhibit microglial activation, in comparison to a placebo following lumbar discectomy.69 None of these trials demonstrated a significant preventative analgesic effect; however, one study did find that propofol-based anaesthesia was associated with a reduced incidence of chronic PO pain in patients undergoing open abdominal hysterectomy.70 Achieving effective PO pain management in individuals with chronic pain presents even greater difficulties due to the biological and psychological changes related to the condition. In this context, the modulation of opiate doses is of utmost importance to ensure an appropriate level of analgesia while simultaneously preventing opioid-related adverse events. Despite these challenges, ensuring effective PO pain management is not just an ethical obligation for perioperative healthcare providers; it is also a fundamental right for patients. Consequently, adopting a comprehensive, patient-centred approach is crucial for achieving optimal PO pain management.
The Pain Management Plan Within ERAS Pathways
ERAS aims to enhance patient outcomes and accelerate recovery following surgery. The protocol concentrates on optimizing each stage of the surgical journey, encouraging patients to take an active role in their recovery. The underlying philosophy is that providing comprehensive education before surgery, coupled with an effective anaesthetic and analgesic strategy, enables patients—particularly those undergoing orthopaedic procedures—to mobilize sooner.13 As a result, these patients can meet physiotherapy objectives more quickly and advance at a faster pace compared to conventional timelines, thereby shortening their hospital stay and minimizing the likelihood of typical hospital-associated complications (ie, acquired infections). The overarching goal is to ensure that all patients, including those with chronic conditions, can achieve a safe and timely discharge without compromising the quality of their outcomes. Thus, it is crucial to understand the role of multimodal analgesia within the ERAS settings. This approach utilizes various pain management strategies that work together to enhance analgesic effects while simultaneously reducing the required doses of individual agents, thereby minimizing the risk of side effects.71–74 The extensive range of adverse effects linked to opioid analgesics—such as nausea, respiratory depression, hyperalgesia, delirium, and tolerance—highlights the need for an opioid-sparing strategy whenever feasible.75,76 Given that multiple pathways and mediators are involved in nociception, it is important to target various areas within the central and peripheral nervous systems using different mechanisms of action (ie, blocking receptors or using alternative medications), in addition to traditional therapies, which can improve analgesic efficacy and pain control.77,78 The timing and dosage of opioids administered to the patients are essential to produce the desired analgesic effect. A recent multimodal pain management protocol scheduled pre-emptive medications before surgery. This approach, together with preoperative classes, reduced the anxiety of the patients regarding the potential delays between the onset of pain and the administration of medication. Additionally, implementing a comprehensive pre-medication protocol is essential to prevent extreme pain at any stage, which can help avoid central sensitization—a phenomenon known to heighten pain perception.79,80 Oral opioids, which act on the μ-receptor to reduce the release of excitatory neurotransmitters, may serve as effective preemptive analgesics. The most frequently used is Oxycontin, for example, the oral administration of OxyContin 10mg has been successfully used as a pre-emptive narcotic in orthopaedics.81 This is especially crucial within the first 48 hours post-surgery to prevent the development of pain imprinting and sensitization with consequent opioid-induced hyperalgesia. Preoperative opioid abusers, for example, require more PO intravenous rescue narcotics compared to matched controls and are at increased risk for morbidity and mortality after orthopaedic surgery.82,83 Conversely, a well-administered protocol for multimodal analgesia aims to prevent pain transduction (local tissue), transmission (peripheral nerves and spinal cord), and perception (central nervous system), nearly eliminating or at least reducing the need for parenteral narcotics (especially opioids) in post-op patients.81 Already in 2009 there have been reports on the use of pre-emptive analgesia combined with PO pain management to shorten the overall length of stay (LOS) following total knee arthroplasty.84 More recently, Trasolini et al described how the implementation of preoperative education, medications, and the administration of spinal anaesthesia, and intraoperative wound injections of morphine, ketorolac (Toradol), and ropivacaine have eliminated the necessity for stronger oral pain medications beyond Norco (at a dose of 10mg every 3–4 hours prn).81 For both hip and knee patients, the same pain medications used in the hospital (eg, Norco, acetaminophen, tramadol) were prescribed for home use. Additionally, each patient was instructed to take 200 mg of celecoxib twice daily for three weeks.81 Another anaesthetic technique used for hip and knee replacement surgery consisted of morphine 100µg or sufentanil 2.5–5µg in addition to local anaesthetics for patients younger than 80 years;85 analgesia was started intraoperatively with intravenous paracetamol and ketoprofen, and following the insertion of the implant, tranexamic acid was administered at a dosage of 20mg/kg.85 After surgery, patients were first taken to the recovery room. Once their pain and PO nausea and vomiting were effectively managed, and in the absence of any active bleeding, they were then transferred to the ward. The PO analgesia protocol consisted of oral administration of paracetamol 1g 3x per day, celecoxib 200mg/die, oxycodone 5–10mg 2x per day (depending on numerical rating scale NRS pain assessment) and 20 oral drops of tramadol 100mg/mL drops as “rescue” medication.85 This prescription was advised for use not only during hospitalization but also following discharge, ensuring sufficient comfort during rest and physical therapy.85 This clinical evidence shows that an optimal opioid-induced anaesthesia protocol requires a peak of narcotic as pre-emptive medication or prior to surgery when the receptors are still available and the sensitization to pain did not occur, while postoperatively only milder opiates in combination with different analgesic techniques are required to maintain an adequate level of analgesia during recovery (Table 2).86 While preventing the occurrence of chronic pain, this model of pain management aims to decrease opiate doses altogether, thereby reducing the potential for side effects from opioid use, which can hinder recovery. Additionally, proactive plans are made with patients and their families for a smooth transition to home care following surgery. The discharge process is closely monitored, particularly during the first week, to significantly minimize the likelihood of emergency room visits.
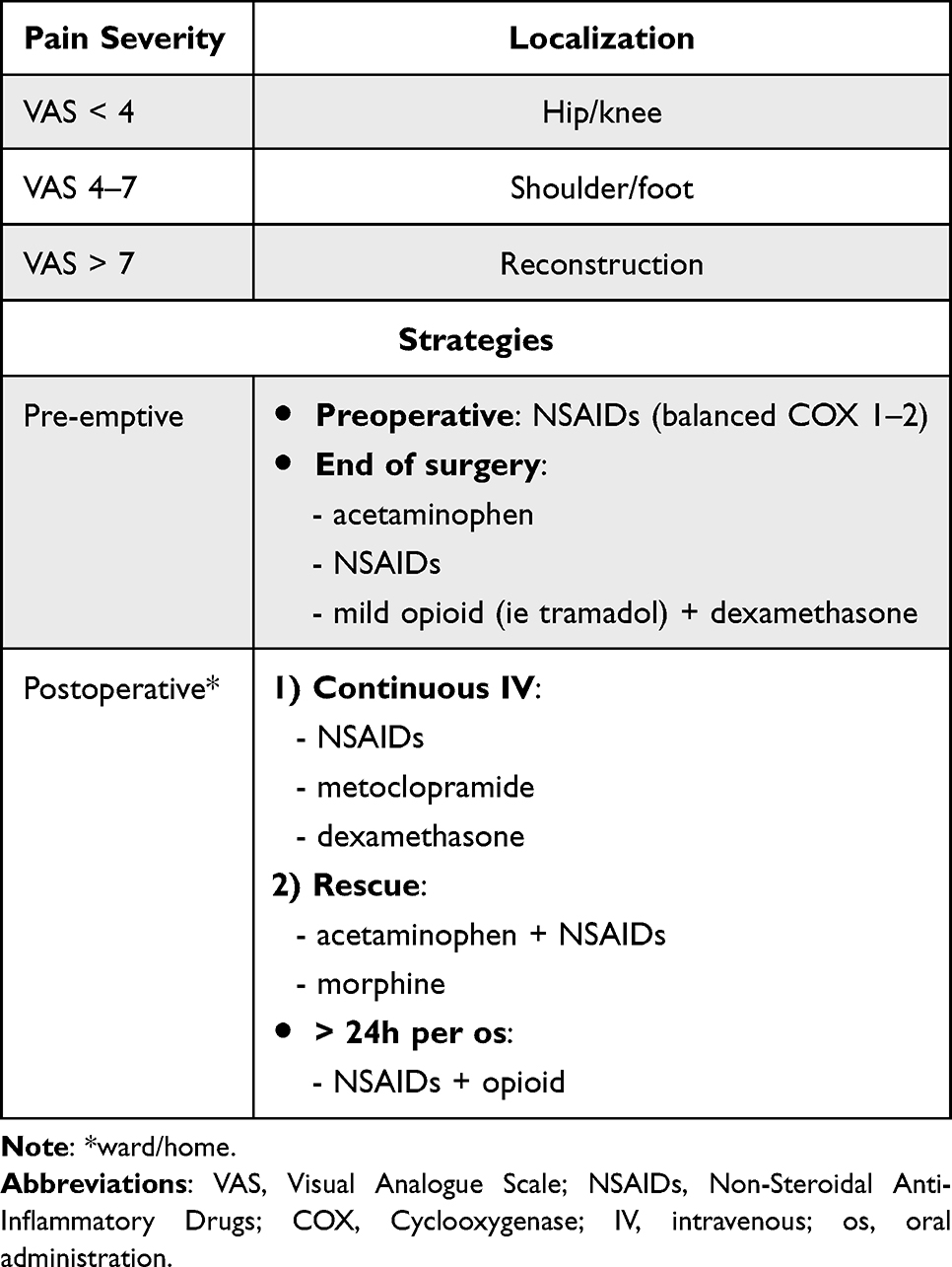 |
Table 2 Perioperative Multimodal Pain Management Plan for Orthopaedic Surgery |
While the theoretical framework of multimodal analgesia is compelling, its widespread adoption necessitates a solid empirical foundation, encompassing controlled trials, observational studies, and systematic reviews. This becomes imperative to substantiate the purported benefits and elucidate the specific contexts where multimodal approaches excel. Thus, further research should explore not only the efficacy of pain relief but also the long-term outcomes, patient satisfaction, and potential economic implications.
Opioid-Free or Opioid-Balanced Strategies for Multimodal Analgesia in Orthopedics
The concept of synergy, by combining medications with complementary mechanisms of action, is pivotal in the development of multimodal analgesia strategies; in fact, the goal is not just additive relief, but an amplified effect that surpasses the sum of the individual components. For instance, the judicious combination of opioids, NSAIDs, and local anaesthetics can create a balance that optimises pain relief while minimising the risks associated with higher doses of any single agent. Concerning this approach to perioperative pain management, orthopaedic and spinal surgery literature highlights successful outcomes with various techniques, including epidurals, spinal and paravertebral blocks, pectorals I and II blocks, and field blocks, providing procedure-specific evidence for the implementation of already existing ERAS Society guidelines.87–96 Multimodal analgesia is an essential component of the ERAS protocols97 and opioid-sparing or opioid-balanced anaesthesia.98 Recently, an alternative approach has been introduced: opioid-free anaesthesia, which is a multimodal anaesthesia protocol combining different drugs and/or techniques to address perioperative pain without the use of opioids.
Opioid-free anaesthesia has been used in several surgical procedures, and the benefits of this approach were evaluated in different meta-analyses.99–101 Nevertheless, the heterogeneity of the studies included was high and some studies administered dexmedetomidine at the same time as opioids. A cohort study that evaluated an opioid-free anaesthesia regimen for lumbar decompressive surgery, comparing it with traditional opioid-balanced anaesthesia, showed a significant decrease in total perioperative opioid consumption in patients who received opioid-free anaesthesia (2.43 ± 0.86 oral morphine equivalents [OMEs]; mean ± SEM), compared to patients who received opioid-balanced anaesthesia (38.125 ± 6.11 OMEs). However, there were no statistically significant differences observed between the two groups regarding the worst PO pain scores (NRS scores 2.55 ± 0.70 vs 2.58 ± 0.73), opioid consumption in the post anaesthesia care unit (5.28 ± 1.7 vs 4.86 ± 1.5 OMEs for opioid-free anaesthesia and opioid-balanced anaesthesia, respectively), and time to readiness for discharge.102 Despite the implementation of new pain management protocols, post-spinal surgery chronic pain is still a significant issue, affecting 10–40% of patients.103 Misdiagnosis and flawed surgical planning are key contributing factors.103,104 In this regard, the canonical approach recommended by international guidelines imposes a choice of drugs according to pain intensity, in a “chronological” order, which starts with paracetamol, NSAIDs, or cyclooxygenase (COX)-2 inhibitors and then moves to opioids, if the first ones are ineffective.105 It must be noted however that opioids are often considered to have more haemodynamic stability compared to non-opioid medications; they generally do not interfere with coagulation factors or the modulation of haemostasis. Adverse cardiovascular events associated with non-opioid analgesics, such as NSAIDs, are often attributed to the inhibition of COX enzymes. COX enzymes play a role in the synthesis of prostaglandins, which are involved in various physiological processes, including inflammation and regulation of blood flow.106 Non-opioid analgesics, particularly NSAIDs, may pose risks in certain patient populations. Hence, caution is advised in patients with pre-existing conditions such as renal, pulmonary, dermatological, and haematological issues.107 While NSAIDs have the potential for adverse effects, they are generally considered safe when used for short periods at the lowest effective dose, but the duration and dosage should be carefully monitored, especially in patients with risk factors for complications.106 Already in 2012, Allegri et al proposed to include the global vision of the patients and their pathology, encompassing every pain type when choosing an analgesic approach. This paradigmatic vision puts the three categories of analgesics at the same level because the choice will be driven by the specific conditions of the patient.105 It is important to direct every effort not only towards improvement in pain management but also towards the personalization of therapy based on the patient, type of surgery (including the type of pathophysiology of pain), and identification of therapies/techniques that can improve the long-term outcome (reduction of side effects and reduction of chronic pain).108 In 2020, in a pilot study the feasibility and potential efficacy of a motivational interviewing and guided opioid tapering support (MI-Opioid Taper) compared to usual care was investigated in patients undergoing total hip or knee arthroplasty. This approach, while feasible, necessitates validation on a larger scale to establish its efficacy in promoting complete PO opioid cessation.109 Hence, the problem is not related to whether drugs/techniques are effective and/or safe, but to which approach will be optimal for meeting the patient’s needs in specific contexts. To mitigate long-term opioid therapy risks in chronic pain, several strategies are recommended: prioritizing non-pharmacological and non-opioid pharmacological approaches; prescribing the lowest effective dose of immediate-release opioids to minimize misuse/addiction risk; avoiding long-term opioid use for acute pain; limiting opioid duration (preferably <7 days), with risk-benefit reassessment within 1–4 weeks; avoiding concurrent opioid and benzodiazepine use to prevent overdose; and regularly reassessing narcotic effects.110 Thus, although opioid-free anaesthesia represents an opportunity to minimise perioperative opioid exposure in some surgical settings, it is still not ready for standardised use in orthopaedics, especially considering its target population (often composed of elderly people or individuals with pre-existing conditions) and the recurrence of pain in the postsurgical period.
Despite the availability of various analgesic strategies for improving perioperative pain management, there is not a gold standard protocol for orthopaedic patients.111 Interestingly, a retrospective analysis examined the impact of three analgesic techniques—morphine, epidural anaesthesia, and continuous nerve block—on PO rehabilitation in 90 total hip arthroplasty patients, with an average age of 55 years. In the epidural group, anaesthesia was administered at the L2–3 or L3–4 level before general anaesthesia, using a dose of 0.2% ropivacaine (2 mg/mL) combined with 0.5 mg of fentanyl (4.5 × 10⁻³ mg/mL) at a rate of 2–4 mL/hr postoperatively. Epidural fentanyl was continued for 48 hours, with catheter removal on PO day 2. Patients in the morphine group were instructed on the use of patient-controlled anaesthesia (PCA) devices,112 which delivered 1.0 mg/hr of morphine with a demand dose of 1.0 mg and a lockout interval of 20 minutes, allowing for additional bolus doses prn. In the continuous nerve block group, a continuous 3-in-1 nerve block was performed after the induction of general anaesthesia. Fondaparinux (2.5mg/day) was initiated on PO day 1 for patients receiving PCA and continuous nerve block and on PO day 2 for those in the epidural group. Movement and strengthening exercises commenced on PO day 1, with full weight-bearing exercises encouraged starting on PO day 2.112 Pain intensity was assessed using a Visual Analog Scale 24 hours after surgery. For patients experiencing intolerable pain, loxoprofen sodium (60 mg) was administered orally every 6 hours prn and, if the pain persisted after 30 minutes, diclofenac sodium suppository (25mg) was administered. Patients using PCA with morphine required supplemental analgesia less frequently compared to the other groups, but the continuous nerve block was associated with fewer side effects, including nausea and/or emesis, and lower D-dimer levels (a marker for thrombotic events after surgery) while providing the same level of pain relief when compared to the other analgesics.112
Therefore, opioid-balanced, multidisciplinary pain management strategies have gained significant traction over the last decade with superior clinical outcomes in terms of early ambulation, LOS, opioid consumption, and PO complications (Table 3).102,113–119
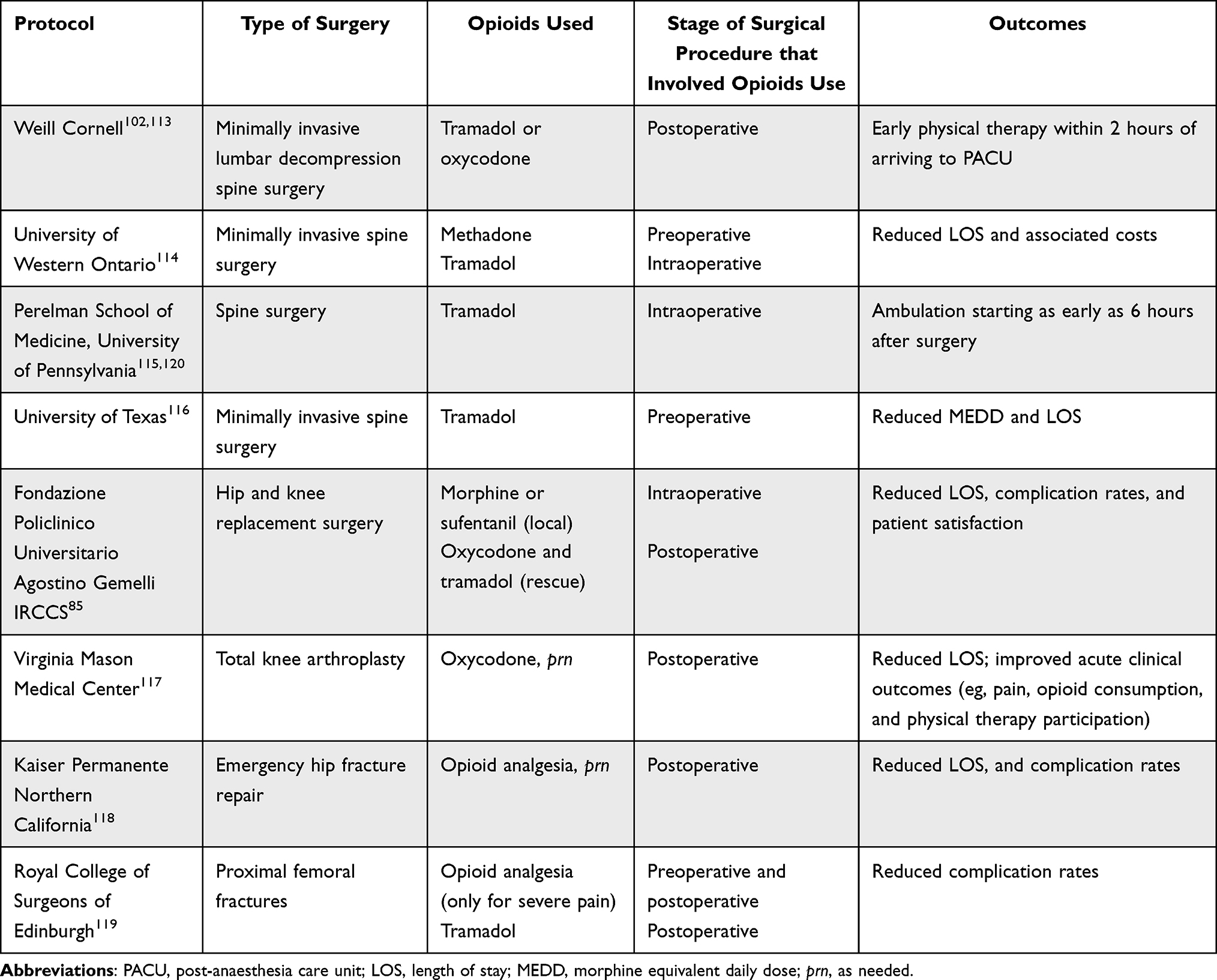 |
Table 3 The Use of Opioids Within Different Multimodal Analgesia Protocols in Orthopaedics |
A multimodal analgesia protocol was implemented in 126 total knee arthroplasty patients (average age 66). Key updates from the previous protocol included pre-operative education and caregiver assignment. The analgesic plan consisted of pre-and intra-operative tranexamic acid, a transdermal scopolamine patch (for patients <70), IV dexamethasone, spinal anesthesia, and a 48-hour (or until discharge) continuous adductor canal nerve block. Postoperatively, physical therapy began on the day of surgery (post-anesthesia resolution), and all patients received a standard oral analgesic regimen (acetaminophen, NSAIDs, gabapentin). Oral oxycodone (prn) was the primary opioid, used only when needed and not contraindicated.117 This survey revealed that the incorporation of perioperative care based on multimodal pain management and early rehabilitation decreased PO LOS (IQR: 53.3, 76.5, P < 0.001) without increasing readmission rates, and improved acute clinical outcomes such as pain, opioid consumption, and physical therapy participation. In 2017 the outcomes of an ERAS pathway were evaluated in a target population of 5,002 elderly patients who underwent emergency hip fracture repair across 20 hospitals in Northern California.118 The pain management protocol for these patients focused on opioid-balanced approaches using multimodal analgesia, which included preoperative and PO intravenous acetaminophen, NSAIDs, and peripheral nerve blocks.118 Patients were encouraged to begin ambulating within 12 hours post-surgery, aiming for a daily walking goal of at least 6.4 meters during the first three PO days.118 To enhance patient engagement, an infographic-based calendar outlining the expected care processes from the night before surgery to discharge was distributed, along with an informational video series aimed at improving patient education.118 The results of this study showed that ERAS implementation significantly increased the relative rate of early ambulation (4.44; 95% CI, 3.19–6.21; P < 0.001) and led to a decrease in opioid use (0.73; 95% CI, 0.63–0.85; P < 0.001).118 There were no significant changes in benzodiazepine usage, but the ERAS protocol was associated with a reduction in hospital LOS and PO complications.118 Notably, the rate of discharge to home improved (1.24; 95% CI, 1.06–1.44; P = 0.007), with no difference in the 30-day readmission rate compared to the orthopedics-comparable cohort prior to ERAS implementation.118 To corroborate these findings, a meta-analysis encompassing 38 trials and 5,099 patients demonstrated significant reductions in LOS and 30-day complication rates following ERAS implementation, without notable differences in mortality or readmission rates.121 Among these trials, only three focused on patients undergoing lower extremity joint replacement. In a study by Macfie et al involving 232 patients with femoral neck fractures, the ERAS protocol was found to reduce PO complications; however, it did not affect the length of hospital stay or 30-day mortality.119
Thus, opioid-balanced multimodal analgesia is important to address acute PO pain and prevent chronic pain after surgery. The adoption of enhanced clinical programmes in orthopaedics has shown an important improvement in PO outcomes with a reduction in the need for opioid use over longer periods and increased patient satisfaction; however, practical considerations, such as optimal drug combinations, dosing regimens, and patient-specific factors, require meticulous exploration. Further research is thus encouraged to navigate these complexities, offering insights that can refine clinical guidelines and practice.
Conclusion
The evolution of perioperative management, exemplified by ERAS programmes, signifies a paradigm shift towards comprehensive and patient-centred care. The journey from traditional approaches to the embrace of multimodal strategies, especially in orthopaedic surgery, has demonstrated significant strides in improving PO outcomes. The emphasis on multimodal analgesia, characterised by an opioid-balanced approach, has emerged as a pivotal component of these protocols. By integrating the proper use of opiates (in time and dosage) with various pain management strategies, such as regional nerve blocks, NSAIDs, and acetaminophen, orthopaedic ERAS programmes aim to enhance patient recovery, minimise PO morbidity and prevent the development of chronic pain, while reducing the long-term reliance on opioids. The multifaceted nature of ERAS, encompassing preoperative education, optimised anaesthesia, and early mobilisation, contributes to shorter hospital stays, decreased complication rates, and improved patient satisfaction. Opioid-free anaesthesia has also been explored in some specialities, for example, bariatric surgery; however, its use requires further optimisation and improvement. Current clinical evidence suggests that an opioid-balanced strategy within a multimodal framework yields superior outcomes in terms of pain control, recovery, and patient experience. As the field advances, continued research and collaboration among healthcare professionals are crucial to refine protocols, tailor approaches to specific patient needs, and further optimise the long-term outcomes of orthopaedic surgeries. Moreover, practical considerations, such as optimal drug combinations, dosing regimens, and patient-specific factors, require meticulous exploration to avoid unwanted side effects. The quest for an optimal balance between pain control and patient safety continues, reflecting a commitment to enhance not only the immediate PO period but also the overall well-being and recovery trajectory of patients undergoing orthopaedic procedures. Thus, a final plea is directed to all national societies and institutions to endorse the implementation of these principles, with validation aimed at achieving the strategic objectives of individual hospitals in terms of efficiency, patient safety, prompt recovery, and reintegration into the community.
Acknowledgments
Realised with the unconditional support of L. Molteni & C. dei F.lli Alitti Società di Esercizio S.p.A. In accordance with the Good Publication Practice 2022 guidelines, the author(s) wish to acknowledge Dr. Maria Donatella Semeraro (MediAbout s.r.l., Milan) for medical writing support.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78(5):606–617. doi:10.1093/bja/78.5.606
2. Basse L, Hjort Jakobsen D, Billesbølle P, Werner M, Kehlet H. A clinical pathway to accelerate recovery after colonic resection. Ann Surg. 2000;232(1):51–57. doi:10.1097/00000658-200007000-00008
3. Fearon KCH, Ljungqvist O, Von Meyenfeldt M, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24(3):466–477. doi:10.1016/j.clnu.2005.02.002
4. Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: enhanced recovery after surgery (ERAS) group recommendations. Arch Surg. 2009;144(10):961–969. doi:10.1001/archsurg.2009.170
5. Gustafsson UO, Scott MJ, Schwenk W, et al. Guidelines for perioperative care in elective colonic surgery: enhanced recovery after surgery (ERAS(®)) Society recommendations. World J Surg. 2013;37(2):259–284. doi:10.1007/s00268-012-1772-0
6. Cerantola Y, Valerio M, Persson B, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: enhanced recovery after surgery (ERAS(®)) society recommendations. Clin Nutr. 2013;32(6):879–887. doi:10.1016/j.clnu.2013.09.014
7. Lassen K, Coolsen MME, Slim K, et al. Guidelines for perioperative care for pancreaticoduodenectomy: enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg. 2013;37(2):240–258. doi:10.1007/s00268-012-1771-1
8. Nygren J, Thacker J, Carli F, et al. Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced recovery after surgery (ERAS(®)) Society recommendations. World J Surg. 2013;37(2):285–305. doi:10.1007/s00268-012-1787-6
9. Mortensen K, Nilsson M, Slim K, et al. Consensus guidelines for enhanced recovery after gastrectomy: enhanced recovery after surgery (ERAS®) Society recommendations. Br J Surg. 2014;101(10):1209–1229. doi:10.1002/bjs.9582
10. Nelson G, Altman AD, Nick A, et al. Guidelines for postoperative care in gynecologic/oncology surgery: enhanced recovery after surgery (ERAS®) Society recommendations--Part II. Gynecol Oncol. 2016;140(2):323–332. doi:10.1016/j.ygyno.2015.12.019
11. Nelson G, Altman AD, Nick A, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: enhanced recovery after surgery (ERAS®) society recommendations--Part I. Gynecol Oncol. 2016;140(2):313–322. doi:10.1016/j.ygyno.2015.11.015
12. Thorell A, MacCormick AD, Awad S, et al. Guidelines for perioperative care in bariatric surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. 2016;40(9):2065–2083. doi:10.1007/s00268-016-3492-3
13. White JJE, Houghton-Clemmey R, Marval P. Enhanced recovery after surgery (ERAS): an orthopaedic perspective. J Perioper Pract. 2013;23(10):228–232. doi:10.1177/175045891302301004
14. Stanton E, Buser Z, Mesregah MK, et al. The impact of enhanced recovery after surgery (ERAS) on opioid consumption and postoperative pain levels in elective spine surgery. Clin Neurol Neurosurg. 2024;242:108350. doi:10.1016/j.clineuro.2024.108350
15. Dahan A, Aarts L, Smith TW. Incidence, reversal, and prevention of opioid-induced respiratory depression. Anesthesiology. 2010;112(1):226–238. doi:10.1097/ALN.0b013e3181c38c25
16. Barletta JF, Asgeirsson T, Senagore AJ. Influence of intravenous opioid dose on postoperative ileus. Ann Pharmacother. 2011;45(7–8):916–923. doi:10.1345/aph.1Q041
17. Goettsch WG, Sukel MPP, van der Peet DL, van Riemsdijk MM, Herings RMC. In-hospital use of opioids increases rate of coded postoperative paralytic ileus. Pharmacoepidemiol Drug Saf. 2007;16(6):668–674. doi:10.1002/pds.1338
18. Smith HS, Laufer A. Opioid induced nausea and vomiting. Eur J Pharmacol. 2014;722:67–78. doi:10.1016/j.ejphar.2013.09.074
19. Bell TJ, Panchal SJ, Miaskowski C, Bolge SC, Milanova T, Williamson R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European patient survey (PROBE 1). Pain Med. 2009;10(1):35–42. doi:10.1111/j.1526-4637.2008.00495.x
20. Dorn S, Lembo A, Cremonini F. Opioid-induced bowel dysfunction: epidemiology, pathophysiology, diagnosis, and initial therapeutic approach. Am J Gastroenterol Suppl. 2014;2(1):31–37. doi:10.1038/ajgsup.2014.7
21. Benson JL, Campbell HE, Phillips CN. Opioid-induced pruritus. Consult Pharm. 2015;30(4):221–227. doi:10.4140/TCP.n.2015.221
22. Oderda GM, Said Q, Evans RS, et al. Opioid-related adverse drug events in surgical hospitalizations: impact on costs and length of stay. Ann Pharmacother. 2007;41(3):400–406. doi:10.1345/aph.1H386
23. Brunenberg DE, van Steyn MJ, Sluimer JC, Bekebrede LL, Bulstra SK, Joore MA. Joint recovery programme versus usual care: an economic evaluation of a clinical pathway for joint replacement surgery. Med Care. 2005;43(10):1018–1026. doi:10.1097/01.mlr.0000178266.75744.35
24. Walter FL, Bass N, Bock G, Markel DC. Success of clinical pathways for total joint arthroplasty in a community hospital. Clin Orthop Relat Res. 2007;457:133–137. doi:10.1097/01.blo.0000246567.88585.0a
25. Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014;30(1):149–160. doi:10.1185/03007995.2013.860019
26. Theunissen M, Peters ML, Schepers J, et al. Recovery 3 and 12 months after hysterectomy: epidemiology and predictors of chronic pain, physical functioning, and global surgical recovery. Medicine. 2016;95(26):e3980. doi:10.1097/MD.0000000000003980
27. Setälä P, Kalliomäki ML, Järvelä K, Huhtala H, Sisto T, Puolakka P. Postoperative hyperalgesia does not predict persistent post-sternotomy pain; observational study based on clinical examination. Acta Anaesthesiol Scand. 2016;60(4):520–528. doi:10.1111/aas.12659
28. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–540. doi:10.1213/01.ANE.0000068822.10113.9E
29. Sommer M, de Rijke JM, van Kleef M, et al. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol. 2008;25(4):267–274. doi:10.1017/S0265021507003031
30. Chan EY, Blyth FM, Nairn L, Fransen M. Acute postoperative pain following hospital discharge after total knee arthroplasty. Osteoarthritis Cartilage. 2013;21(9):1257–1263. doi:10.1016/j.joca.2013.06.011
31. Gerbershagen HJ, Aduckathil S, van Wijck AJM, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
32. Dolin SJ, Cashman JN, Bland JM. Effectiveness of acute postoperative pain management: i. Evidence from published data. Br J Anaesth. 2002;89(3):409–423.
33. Munafò MR, Stevenson J. Anxiety and surgical recovery. Reinterpreting the literature. J Psychosom Res. 2001;51(4):589–596. doi:10.1016/s0022-3999(01)00258-6
34. Caumo W, Schmidt AP, Schneider CN, et al. Preoperative predictors of moderate to intense acute postoperative pain in patients undergoing abdominal surgery. Acta Anaesthesiol Scand. 2002;46(10):1265–1271. doi:10.1034/j.1399-6576.2002.461015.x
35. Kalkman JC, Visser K, Moen J, Bonsel JG, Grobbee ED, Moons MKG. Preoperative prediction of severe postoperative pain. Pain. 2003;105(3):415–423. doi:10.1016/S0304-3959(03)00252-5
36. Pavlin DJ, Sullivan MJL, Freund PR, Roesen K. Catastrophizing: a risk factor for postsurgical pain. Clin J Pain. 2005;21(1):83–90. doi:10.1097/00002508-200501000-00010
37. Granot M, Ferber SG. The roles of pain catastrophizing and anxiety in the prediction of postoperative pain intensity: a prospective study. Clin J Pain. 2005;21(5):439–445. doi:10.1097/01.ajp.0000135236.12705.2d
38. Grosu I, de Kock M. New concepts in acute pain management: strategies to prevent chronic postsurgical pain, opioid-induced hyperalgesia, and outcome measures. Anesthesiol Clin. 2011;29(2):311–327. doi:10.1016/j.anclin.2011.04.001
39. Aubrun F, Valade N, Coriat P, Riou B. Predictive factors of severe postoperative pain in the postanesthesia care unit. Anesth Analg. 2008;106(5):1535–1541,tableofcontents. doi:10.1213/ane.0b013e318168b2ce
40. Ip HY, Abrishami A, Peng PWH, Wong J, Chung F. Predictors of postoperative pain and analgesic consumption: a qualitative systematic review. Anesthesiology. 2009;111(3):657–677. doi:10.1097/ALN.0b013e3181aae87a
41. Goesling J, Moser SE, Zaidi B, et al. Trends and predictors of opioid use after total knee and total Hip arthroplasty. Pain. 2016;157(6):1259–1265. doi:10.1097/j.pain.0000000000000516
42. Franklin PD, Karbassi JA, Li W, Yang W, Ayers DC. Reduction in narcotic use after primary total knee arthroplasty and association with patient pain relief and satisfaction. J Arthroplasty. 2010;25(6 Suppl):12–16. doi:10.1016/j.arth.2010.05.003
43. Breivik H, Stubhaug A. Management of acute postoperative pain: still a long way to go! Pain. 2008;137(2):233–234. doi:10.1016/j.pain.2008.04.014
44. Chang SH, Maney KM, Mehta V, Langford RM. Pain assessment and management in medical wards: an area of unmet need. Postgrad Med J. 2010;86(1015):279–284. doi:10.1136/pgmj.2008.076497
45. Tufano R, Puntillo F, Draisci G, et al. Italian observational study of the management of mild-to-moderate post-operative pain (ITOSPOP). Minerva Anestesiol. 2012;78(1):15–25.
46. Allegri M, Niebel T, Bugada D, et al. Regional analgesia in Italy: a survey of current practice. Eur J Pain Suppl. 2010;4(S4):219–225. doi:10.1016/j.eujps.2010.09.007
47. Gordon DB, Pellino TA, Miaskowski C, et al. A 10-year review of quality improvement monitoring in pain management: recommendations for standardized outcome measures. Pain Manag Nurs. 2002;3(4):116–130. doi:10.1053/jpmn.2002.127570
48. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
49. Macrae WA. Chronic pain after surgery. Br J Anaesth. 2001;87(1):88–98. doi:10.1093/bja/87.1.88
50. Poobalan AS, Bruce J, Smith WCS, King PM, Krukowski ZH, Chambers WA. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain. 2003;19(1):48–54. doi:10.1097/00002508-200301000-00006
51. Johansen A, Romundstad L, Nielsen CS, Schirmer H, Stubhaug A. Persistent postsurgical pain in a general population: prevalence and predictors in the Tromsø study. Pain. 2012;153(7):1390–1396. doi:10.1016/j.pain.2012.02.018
52. Wildgaard K, Ravn J, Kehlet H. Chronic post-thoracotomy pain: a critical review of pathogenic mechanisms and strategies for prevention. Eur J Cardiothorac Surg. 2009;36(1):170–180. doi:10.1016/j.ejcts.2009.02.005
53. Wang L, Guyatt GH, Kennedy SA, et al. Predictors of persistent pain after breast cancer surgery: a systematic review and meta-analysis of observational studies. CMAJ. 2016;188(14):E352–E361. doi:10.1503/cmaj.151276
54. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77–86. doi:10.1093/bja/aen099
55. Wilson SH, Hellman KM, James D, Adler AC, Chandrakantan A. Mechanisms, diagnosis, prevention and management of perioperative opioid-induced hyperalgesia. Pain Manag. 2021;11(4):405–417. doi:10.2217/pmt-2020-0105
56. Aasvang E, Kehlet H. Chronic postoperative pain: the case of inguinal herniorrhaphy. Br J Anaesth. 2005;95(1):69–76. doi:10.1093/bja/aei019
57. Yarnitsky D, Crispel Y, Eisenberg E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. 2008;138(1):22–28. doi:10.1016/j.pain.2007.10.033
58. Minnella EM, Bousquet-Dion G, Awasthi R, Scheede-Bergdahl C, Carli F. Multimodal prehabilitation improves functional capacity before and after colorectal surgery for cancer: a five-year research experience. Acta Oncol. 2017;56(2):295–300. doi:10.1080/0284186X.2016.1268268
59. Joshi GP, Schug SA, Kehlet H. Procedure-specific pain management and outcome strategies. Best Pract Res Clin Anaesthesiol. 2014;28(2):191–201. doi:10.1016/j.bpa.2014.03.005
60. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North Am. 2005;23(1):21–36. doi:10.1016/j.atc.2004.11.013
61. Badiola IJ. Can chronic pain be prevented? Anesthesiol Clin. 2016;34(2):303–315. doi:10.1016/j.anclin.2016.01.008
62. Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377(9784):2215–2225. doi:10.1016/S0140-6736(11)60245-6
63. Dahl JB, Kehlet H. Preventive analgesia. Curr Opin Anaesthesiol. 2011;24(3):331–338. doi:10.1097/ACO.0b013e328345afd9
64. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–S15. doi:10.1016/j.pain.2010.09.030
65. Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother. 2009;9(5):723–744. doi:10.1586/ern.09.20
66. Clarke H, Poon M, Weinrib A, Katznelson R, Wentlandt K, Katz J. Preventive analgesia and novel strategies for the prevention of chronic post-surgical pain. Drugs. 2015;75(4):339–351. doi:10.1007/s40265-015-0365-2
67. Cohen SP, Galvagno SM, Plunkett A, et al. A multicenter, randomized, controlled study evaluating preventive etanercept on postoperative pain after inguinal hernia repair. Anesth Analg. 2013;116(2):455–462. doi:10.1213/ANE.0b013e318273f71c
68. Joshi SS, Jagadeesh AM. Efficacy of perioperative pregabalin in acute and chronic post-operative pain after off-pump coronary artery bypass surgery: a randomized, double-blind placebo controlled trial. Ann Card Anaesth. 2013;16(3):180–185. doi:10.4103/0971-9784.114239
69. Martinez V, Szekely B, Lemarié J, et al. The efficacy of a glial inhibitor, minocycline, for preventing persistent pain after lumbar discectomy: a randomized, double-blind, controlled study. Pain. 2013;154(8):1197–1203. doi:10.1016/j.pain.2013.03.028
70. Ogurlu M, Sari S, Küçük M, et al. Comparison of the effect of propofol and sevoflurane anaesthesia on acute and chronic postoperative pain after hysterectomy. Anaesth Intensive Care. 2014;42(3):365–370. doi:10.1177/0310057X1404200314
71. Gritsenko K, Khelemsky Y, Kaye AD, Vadivelu N, Urman RD. Multimodal therapy in perioperative analgesia. Best Pract Res Clin Anaesthesiol. 2014;28(1):59–79. doi:10.1016/j.bpa.2014.03.001
72. Prabhakar A, Mancuso KF, Owen CP, et al. Perioperative analgesia outcomes and strategies. Best Pract Res Clin Anaesthesiol. 2014;28(2):105–115. doi:10.1016/j.bpa.2014.04.005
73. Beverly A, Kaye AD, Urman RD. SCAMPs for multimodal post-operative analgesia: a concept to standardize and individualize care. Curr Pain Headache Rep. 2017;21(1):5. doi:10.1007/s11916-017-0603-2
74. Wachholtz A, Ziedonis D, Gonzalez G. Comorbid pain and opioid addiction: psychosocial and pharmacological treatments. Subst Use Misuse. 2011;46(12):1536–1552. doi:10.3109/10826084.2011.559606
75. Oderda GM, Evans RS, Lloyd J, et al. Cost of opioid-related adverse drug events in surgical patients. J Pain Symptom Manage. 2003;25(3):276–283. doi:10.1016/s0885-3924(02)00691-7
76. Koppert W, Schmelz M. The impact of opioid-induced hyperalgesia for postoperative pain. Best Pract Res Clin Anaesthesiol. 2007;21(1):65–83. doi:10.1016/j.bpa.2006.12.004
77. Prabhakar A, Cefalu JN, Rowe JS, Kaye AD, Urman RD. Techniques to optimize multimodal analgesia in ambulatory surgery. Curr Pain Headache Rep. 2017;21(5):24. doi:10.1007/s11916-017-0622-z
78. Baribeault T. Opioid-free anesthesia for an emergency laparoscopic cholecystectomy in a patient taking buprenorphine-naloxone for opioid addiction: a case report. Anesthesia eJournal. 2018;6:37–40.
79. Wall PD. The prevention of postoperative pain. Pain. 1988;33(3):289–290. doi:10.1016/0304-3959(88)90286-2
80. Reuben SS, Sklar J. Pain management in patients who undergo outpatient arthroscopic surgery of the knee. J Bone Joint Surg Am. 2000;82(12):1754–1766. doi:10.2106/00004623-200012000-00010
81. Trasolini NA, McKnight BM, Dorr LD. The opioid crisis and the orthopedic surgeon. J Arthroplasty. 2018;33(11):3379–3382.e1. doi:10.1016/j.arth.2018.07.002
82. Menendez ME, Ring D, Bateman BT. Preoperative opioid misuse is associated with increased morbidity and mortality after elective orthopaedic surgery. Clin Orthop Relat Res. 2015;473(7):2402–2412. doi:10.1007/s11999-015-4173-5
83. Rozell JC, Courtney PM, Dattilo JR, Wu CH, Lee GC. Preoperative opiate use independently predicts narcotic consumption and complications after total joint arthroplasty. J Arthroplasty. 2017;32(9):2658–2662. doi:10.1016/j.arth.2017.04.002
84. Duellman TJ, Gaffigan C, Milbrandt JC, Allan DG. Multi-modal, pre-emptive analgesia decreases the length of hospital stay following total joint arthroplasty. Orthopedics. 2009;32:1–5.
85. Frassanito L, Vergari A, Nestorini R, et al. Enhanced recovery after surgery (ERAS) in hip and knee replacement surgery: description of a multidisciplinary program to improve management of the patients undergoing major orthopedic surgery. Musculoskelet Surg. 2020;104(1):87–92. doi:10.1007/s12306-019-00603-4
86. Aroke EN, McMullan SP, Woodfin KO, Richey R, Doss J, Wilbanks BA. A practical approach to acute postoperative pain management in chronic pain patients. Journal of PeriAnesthesia Nursing. 2020;35(6):564–573. doi:10.1016/j.jopan.2020.03.002
87. Dizdarevic A, Fernandes A. Thoracic paravertebral block, multimodal analgesia, and monitored anesthesia care for breast cancer surgery in primary lateral sclerosis. Case Rep Anesthesiol. 2016;2016:6301358. doi:10.1155/2016/6301358
88. Zhang X, Shu L, Lin C, et al. Comparison between intraoperative two-space injection thoracic paravertebral block and wound infiltration as a component of multimodal analgesia for postoperative pain management after video-assisted thoracoscopic lobectomy: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2015;29(6):1550–1556. doi:10.1053/j.jvca.2015.06.013
89. Bashandy GMN, Abbas DN. Pectoral nerves I and II blocks in multimodal analgesia for breast cancer surgery: a randomized clinical trial. Reg Anesth Pain Med. 2015;40(1):68–74. doi:10.1097/AAP.0000000000000163
90. Thomazeau J, Rouquette A, Martinez V, et al. Acute pain factors predictive of post-operative pain and opioid requirement in multimodal analgesia following knee replacement. Eur J Pain. 2016;20(5):822–832. doi:10.1002/ejp.808
91. Kim SI, Ha KY, Oh IS. Preemptive multimodal analgesia for postoperative pain management after lumbar fusion surgery: a randomized controlled trial. Eur Spine J. 2016;25(5):1614–1619. doi:10.1007/s00586-015-4216-3
92. Greze J, Vighetti A, Incagnoli P, et al. Does continuous wound infiltration enhance baseline intravenous multimodal analgesia after posterior spinal fusion surgery? A randomized, double-blinded, placebo-controlled study. Eur Spine J. 2017;26(3):832–839. doi:10.1007/s00586-016-4428-1
93. Fabi DW. Multimodal analgesia in the hip fracture patient. J Orthop Trauma. 2016;30 Suppl 1:S6–S11. doi:10.1097/BOT.0000000000000561
94. Milani P, Castelli P, Sola M, Invernizzi M, Massazza G, Cisari C. Multimodal analgesia in total knee arthroplasty: a randomized, double-blind, controlled trial on additional efficacy of periarticular anesthesia. J Arthroplasty. 2015;30(11):2038–2042. doi:10.1016/j.arth.2015.05.035
95. Halawi MJ, Grant SA, Bolognesi MP. Multimodal analgesia for total joint arthroplasty. Orthopedics. 2015;38(7):e616–25. doi:10.3928/01477447-20150701-61
96. Cho CH, Song KS, Min BW, Jung GH, Lee YK, Shin HK. Efficacy of interscalene block combined with multimodal pain control for postoperative analgesia after rotator cuff repair. Knee Surg Sports Traumatol Arthrosc. 2015;23(2):542–547. doi:10.1007/s00167-012-2272-3
97. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
98. Kumar K, Kirksey MA, Duong S, Wu CL. A review of opioid-sparing modalities in perioperative pain management: methods to decrease opioid use postoperatively. Anesth Analg. 2017;125(5):1749–1760. doi:10.1213/ANE.0000000000002497
99. Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;74(5):651–662. doi:10.1111/anae.14582
100. Singh PM, Panwar R, Borle A, Mulier JP, Sinha A, Goudra B. Perioperative analgesic profile of dexmedetomidine infusions in morbidly obese undergoing bariatric surgery: a meta-analysis and trial sequential analysis. Surg Obes Relat Dis. 2017;13(8):1434–1446. doi:10.1016/j.soard.2017.02.025
101. Tsaousi GG, Pourzitaki C, Aloisio S, Bilotta F. Dexmedetomidine as a sedative and analgesic adjuvant in spine surgery: a systematic review and meta-analysis of randomized controlled trials. Eur J Clin Pharmacol. 2018;74(11):1377–1389. doi:10.1007/s00228-018-2520-7
102. Soffin EM, Wetmore DS, Beckman JD, et al. Opioid-free anesthesia within an enhanced recovery after surgery pathway for minimally invasive lumbar spine surgery: a retrospective matched cohort study. Neurosurg Focus. 2019;46(4):E8. doi:10.3171/2019.1.FOCUS18645
103. Chen YC, Lee CY, Chen SJ. Narcotic addiction in failed back surgery syndrome. Cell Transplant. 2019;28(3):239–247. doi:10.1177/0963689718796072
104. Daniell JR, Osti OL. Failed back surgery syndrome: a review article. Asian Spine J. 2018;12(2):372–379. doi:10.4184/asj.2018.12.2.372
105. Molfetta L, Saviola G, Fornasari D, Grossi PA, Corcione A, Frediani B. Osteoarticular pain: therapeutic approach by paradigms. Eur Rev Med Pharmacol Sci. 2022;26(11):4054–4068. doi:10.26355/eurrev_202206_28975
106. van Rensburg R, Reuter H. An overview of analgesics: nSAIDs, paracetamol, and topical analgesics Part 1. South African Family Practice. 2019;61(sup1):S4–S10. doi:10.1080/20786190.2019.1610228
107. Tarr GS, Reuter H. Review of the safety of nonsteroidal anti-inflammatory drugs and selective cyclo-oxygenase-2 inhibitors. South African Family Practice. 2015;57(3):18–21.
108. Allegri M, Grossi P. Management of postoperative pain: how accurate and successful is our acute pain management? Minerva Anestesiol. 2012;78(1):1–3.
109. Hah JM, Trafton JA, Narasimhan B, et al. Efficacy of motivational-interviewing and guided opioid tapering support for patients undergoing orthopedic surgery (MI-Opioid Taper): a prospective, assessor-blind, randomized controlled pilot trial. EClinicalMedicine. 2020;28:100596. doi:10.1016/j.eclinm.2020.100596
110. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. JAMA. 2016;315(15):1624. doi:10.1001/jama.2016.1464
111. Correll DJ, Vlassakov KV, Kissin I. No evidence of real progress in treatment of acute pain, 1993-2012: scientometric analysis. J Pain Res. 2014;7:199–210. doi:10.2147/JPR.S60842
112. Tetsunaga T, Sato T, Shiota N, et al. Comparison of continuous epidural analgesia, patient-controlled analgesia with morphine, and continuous three-in-one femoral nerve block on postoperative outcomes after total hip arthroplasty. Clin Orthop Surg. 2015;7(2):164–170. doi:10.4055/cios.2015.7.2.164
113. Ali ZS, Flanders TM, Ozturk AK, et al. Enhanced recovery after elective spinal and peripheral nerve surgery: pilot study from a single institution. J Neurosurg Spine. 2019;30(4):532–540. doi:10.3171/2018.9.SPINE18681
114. Corniola MV, Debono B, Joswig H, Lemée JM, Tessitore E. Enhanced recovery after spine surgery: review of the literature. Neurosurg Focus. 2019;46(4):E2. doi:10.3171/2019.1.FOCUS18657
115. Wang MY, Grossman J. Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: initial clinical experience with 1-year follow-up. Neurosurg Focus. 2016;40(2):E13. doi:10.3171/2015.11.FOCUS15435
116. Grasu RM, Cata JP, Dang AQ, et al. Implementation of an enhanced recovery after spine surgery program at a large cancer center: a preliminary analysis. J Neurosurg Spine. 2018;29(5):588–598. doi:10.3171/2018.4.SPINE171317
117. Auyong DB, Allen CJ, Pahang JA, Clabeaux JJ, MacDonald KM, Hanson NA. Reduced length of hospitalization in primary total knee arthroplasty patients using an updated enhanced recovery after orthopedic surgery (ERAS) pathway. J Arthroplasty. 2015;30(10):1705–1709. doi:10.1016/j.arth.2015.05.007
118. Liu VX, Rosas E, Hwang J, et al. Enhanced recovery after surgery program implementation in 2 surgical populations in an integrated health care delivery system. JAMA Surg. 2017;152(7):e171032. doi:10.1001/jamasurg.2017.1032
119. Macfie D, Zadeh RA, Andrews M, Crowson J, Macfie J. Perioperative multimodal optimisation in patients undergoing surgery for fractured neck of femur. Surgeon. 2012;10(2):90–94. doi:10.1016/j.surge.2011.01.006
120. Soffin EM, Vaishnav AS, Wetmore DS, et al. Design and implementation of an enhanced recovery after surgery (ERAS) program for minimally invasive lumbar decompression spine surgery. Spine (Phila Pa 1976). 2019;44(9):E561–E570. doi:10.1097/BRS.0000000000002905
121. Nicholson A, Lowe MC, Parker J, Lewis SR, Alderson P, Smith AF. Systematic review and meta-analysis of enhanced recovery programmes in surgical patients. Br J Surg. 2014;101(3):172–188. doi:10.1002/bjs.9394
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cohort Description: Preventing an Opioid Epidemic in Norway – Focusing on Treatment of Chronic Pain (POINT) – A National Registry-Based Study
Hamina A, Odsbu I, Borchgrevink PC, Chen LC, Clausen T, Espnes KA, Gjesdal K, Handal M, Hartikainen S, Hjellvik V, Holter MTS, Høibø T, Kurita GP, Langaas HC, Lid TG, Nøst TH, Sjøgren P, Skurtveit S
Clinical Epidemiology 2022, 14:1477-1486
Published Date: 8 December 2022
Tapentadol: A Review of Experimental Pharmacology Studies, Clinical Trials, and Recent Findings
Alshehri FS
Drug Design, Development and Therapy 2023, 17:851-861
Published Date: 21 March 2023
Association Between Pharmacotherapy and Sleep Quality in Patients with Chronic Orofacial and Chronic Body Pain: A Cross-Sectional Study
Bavia PF, Khawaja S, Hernández-Nuño de la Rosa MF, Tseng LA, Keith DA
Journal of Pain Research 2023, 16:3433-3440
Published Date: 10 October 2023
Engagement in Integrative and Nonpharmacologic Pain Management Modalities Among Adults with Chronic Pain: Analysis of the 2019 National Health Interview Survey
Rodgers-Melnick SN, Trager RJ, Love TE, Dusek JA
Journal of Pain Research 2024, 17:253-264
Published Date: 16 January 2024
Pharmacological Prescribing and Satisfaction with Pain Treatment Among Non-Hispanic Black Men with Chronic Pain
Oloruntoba O, Bergeron CD, Zhong L, Merianos AL, Sherman LD, Kew CL, Goidel RK, Smith ML
Patient Preference and Adherence 2024, 18:187-195
Published Date: 19 January 2024