")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Enhancing Diagnostic and Patient Safety in Healthcare Systems: Key Insights from the World Patient Safety Day 2024 Commemoration in Uganda
Authors Turyasiima M , Niwampeire PM, Ssendyona M, Akot BG, Acheng M, Katongole SP , Okware J, Tumwikirize J, Mutesasira K, Atepo J, Kaitiritimba R, Epuitai J, Tumwesigye BT, Turinawe G , Mutumba R, Ndifuna M, Musinguzi G, Kemigisa DA
Received 5 February 2025
Accepted for publication 8 May 2025
Published 14 May 2025 Volume 2025:17 Pages 135—143
DOI https://doi.org/10.2147/DHPS.S520743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hemalkumar B Mehta
Munanura Turyasiima,1,2 Prima Maria Niwampeire,3 Martin Ssendyona,1 Balbina Gillian Akot,2 Miriam Acheng,4 Simon Peter Katongole,5 Joseph Okware,1 Juliet Tumwikirize,1 Kenneth Mutesasira,6 Joshua Atepo,1 Robinah Kaitiritimba,7 Joshua Epuitai,8 Benson Tuhwezeine Tumwesigye,1 Gaston Turinawe,9 Robert Mutumba,9 Martin Ndifuna,10 Geofrey Musinguzi,11 Denise Asaba Kemigisa1
1Department of Standards Compliance Accreditation and Patient Protection, Ministry of Health, Kampala, Uganda; 2Department of Pediatrics and Child Health, Kampala International University, Kampala, Uganda; 3The Aids Support Organization, Kampala, Uganda; 4Division of Health Information Management, Ministry of Health, Kampala, Uganda; 5Uganda Martyrs University, Kampala, Uganda; 6Quality Improvement Office, World Health Organization, Kampala, Uganda; 7The Uganda National Health Consumers’ Organization, Kampala, Uganda; 8Department of Nursing, Faculty of Health Services, Busitema University, Mbale, Uganda; 9STD/AIDS Control Program, Ministry of Health, Kampala, Uganda; 10Johns Hopkins Program for International Education in Gynecology and Obstetrics (Jhpeigo), Kampala, Uganda; 11Department of Disease Control and Environmental Health, Makerere University School of Public Health, Kampala, Uganda
Correspondence: Munanura Turyasiima, Email [email protected]
Background: The 4th World Patient Safety Day (WPSD) 2024 commemoration in Uganda, themed “Improving Diagnosis for Patient Safety”, highlighted critical challenges and opportunities in reducing diagnostic errors within healthcare systems. This review synthesizes key insights from the event, focusing on factors contributing to diagnostic inaccuracies, systemic gaps, and actionable strategies for improvement.
Methods: Using a qualitative synthesis approach guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ), we analyzed data from a hybrid webinar (210 participants) and a four-day medical camp (600+ patients served). Thematic analysis identified four key areas: (i) factors influencing diagnostic errors, (ii) the role of laboratory and imaging services in diagnosis error prevention, (iii) existing health system interventions, and (iv) patient empowerment in the diagnostic process.
Results: Diagnostic errors in Uganda stem from cognitive biases, systemic inefficiencies (eg, understaffing, inadequate equipment), and financial barriers in private healthcare. Strengthening laboratory capacity, digitizing health records, and enhancing provider-patient communication emerged as pivotal solutions. The Ministry of Health’s initiatives such as laboratory accreditation, the 5S quality improvement framework, and patient feedback mechanisms demonstrate progress but require scaling.
Recommendations: We propose a multi-level approach: (1) national policies for error reporting and patient safety frameworks, (2) expanded supportive supervision and digitization (eg, EHRs with decision support), (3) stricter regulation of private healthcare, and (4) community engagement to improve health literacy and early care-seeking.
Conclusion: Reducing diagnostic errors demands systemic reforms, technological integration, and collaborative stakeholder engagement. Uganda’s WPSD 2024 insights offer a model for similar low-resource settings to enhance diagnostic accuracy and patient safety.
Keywords: diagnostic errors, patient safety, healthcare quality, Uganda, world patient safety day
Introduction
Accurate and timely diagnosis is the cornerstone of effective healthcare, yet diagnostic errors remain a leading cause of patient harm globally.1 In low-resource settings like Uganda, where systemic challenges such as workforce shortages, inadequate diagnostic infrastructure, and fragmented health systems persist, diagnostic inaccuracies contribute significantly to preventable morbidity, mortality, and financial burdens.2–4 The 2024 World Patient Safety Day (WPSD) theme, “Improving Diagnosis for Patient Safety”, underscores the urgency of addressing these gaps—a call to action that aligns with Uganda’s commitments to universal health coverage (UHC) and the Sustainable Development Goals (SDGs).1,5
Despite global advancements in diagnostic technologies, Uganda’s healthcare system grapples with persistent challenges. Studies reveal that 52% of healthcare workers in central Uganda have witnessed or committed diagnostic errors, with misdiagnosis rates as high as 9.2% in inpatient settings.4,6 These errors are exacerbated by cognitive biases, limited access to laboratories, and socioeconomic barriers that delay care-seeking.3,7 The consequences are dire: patients endure prolonged suffering, unnecessary costs, and eroded trust in healthcare systems, while providers face moral distress and inefficiencies.8,9
This review synthesizes evidence from Uganda’s WPSD 2024 commemoration to: analyze systemic and cognitive factors driving diagnostic errors in resource-constrained settings, evaluate the role of laboratory/imaging services and existing interventions (for example, accreditation, digital tools) in mitigating errors and propose actionable strategies for policymakers, healthcare providers, and communities to enhance diagnostic safety.
Our findings address a critical gap in literature by integrating frontline provider experiences, patient narratives, and policy insights—a perspective often missing in top-down assessments.10,11 By leveraging Uganda’s WPSD platform, this review captures real-world challenges and solutions, offering a model for similar low- and middle-income countries (LMICs).
The rising burden of non-communicable diseases (NCDs) and post-pandemic health system strains in Uganda amplify the need for accurate diagnostics.5 For healthcare providers, this review highlights training gaps and workflow inefficiencies; for policymakers, it identifies regulatory and infrastructural priorities (eg, electronic health records, equitable resource allocation). Crucially, it empowers patients and communities through strategies to improve health literacy and advocacy (eg, second-opinion campaigns, feedback mechanisms).1,12
By bridging research, policy, and practice, this review contributes to global patient safety agendas while offering locally adaptable solutions. Its urgency is underscored by the preventable human and economic costs of diagnostic errors—a challenge demanding immediate, collaborative action.
Methods and Materials
Study Design
We conducted a systematic qualitative synthesis of evidence from Uganda’s 2024 World Patient Safety Day (WPSD) commemoration activities and peer-reviewed literature on diagnostic errors in low-resource settings. This methodological approach combined: (1) thematic analysis of primary data from WPSD events and (2) a narrative review of existing literature.
Data Sources and Search Strategy
Primary data were collected from: hybrid webinar proceedings (210 participants), field observations from a 4-day medical camp (600+ patients served), policy documents and presentations from Uganda’s Ministry of Health, and media transcripts and stakeholder reports.
For the literature review component, we systematically searched PubMed, Scopus, and African Journals Online using the following key terms: “diagnostic errors”, “patient safety”, “low-resource settings” and “Uganda”. The search was limited to English-language articles published between 2014 and 2024, with priority given to studies from sub-Saharan Africa. See the summary of key literature on diagnostic errors and patient Safety in Table 1.
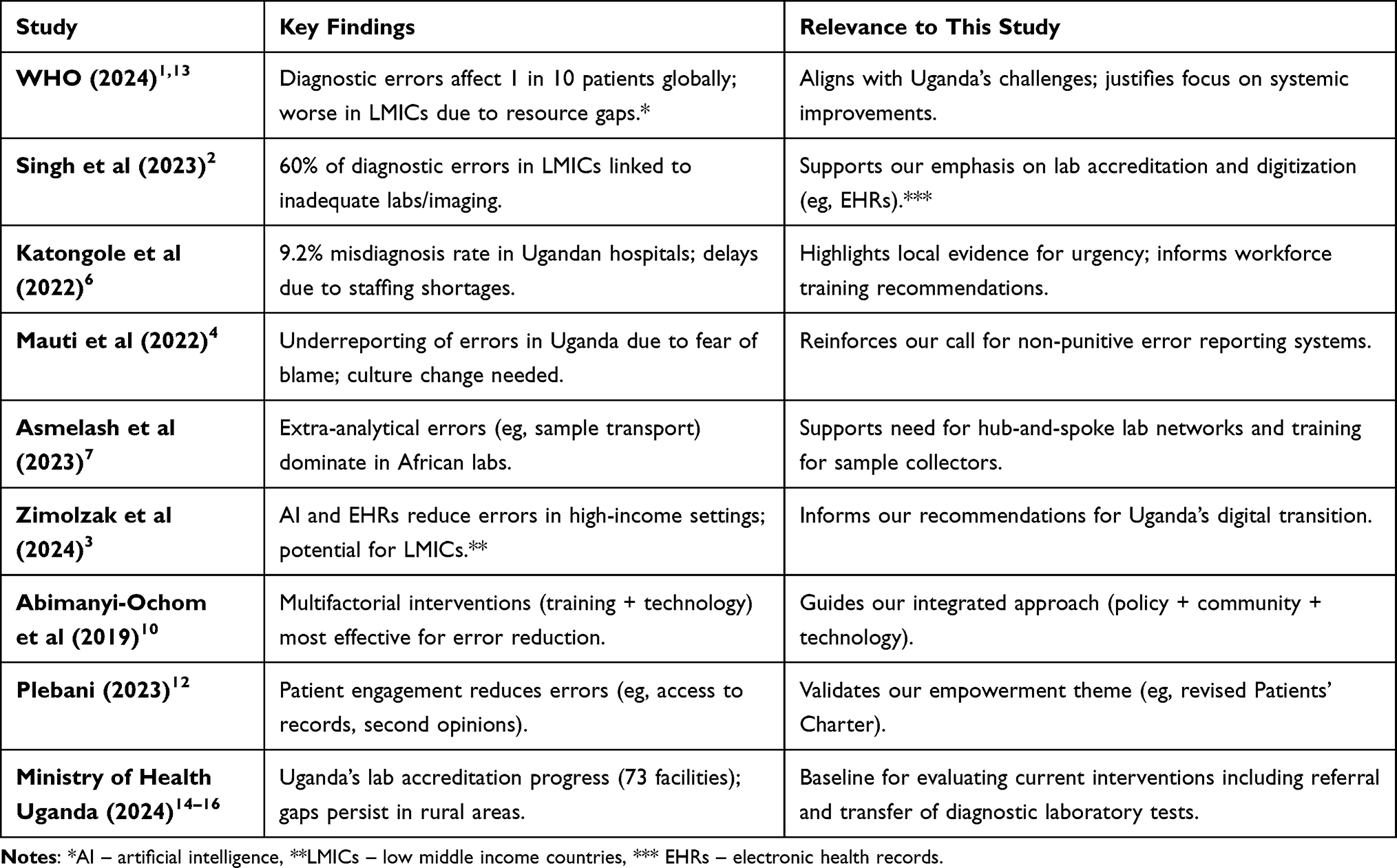 |
Table 1 Summary of Key Literature on Diagnostic Errors and Patient Safety |
Data Extraction and Synthesis
Two independent reviewers extracted data using a standardized form covering: study characteristics (author, year, design), population/setting details, key findings related to diagnostic errors and proposed interventions.
Discrepancies were resolved through consensus with a third reviewer. We employed the Consolidated Criteria for Reporting Qualitative Research (COREQ) framework17 to ensure methodological rigor in analyzing primary qualitative data.
Analytical Framework
Data were analyzed thematically using the Safer Dx framework,2 which examines structural factors (resources, systems), process factors (clinical workflows) and outcome measures (diagnostic accuracy). This was complemented by Donabedian’s structure-process-outcome model18 to evaluate health system performance.
Results
Systematic qualitative synthesis and literature review yielded four main themes: i) factors influencing diagnostic errors, ii) adequate laboratory and imaging services as a means to prevent diagnostic errors, iii) existing health system interventions aimed at reducing diagnostic errors, and iv) empowering patients and families to actively engage with their healthcare providers. Each theme will be elaborated on in the following sections.
Factors That Influence Diagnostic Errors During Clinical Practice
To better understand the influences of diagnostic errors in a healthcare system, we applied the Safer Dx framework2 which is grounded in the Donabedian model18,19 to evaluate the structural, process, and outcome-related factors that affect diagnostic safety.
Diagnostic errors during clinical practice are influenced by a variety of cognitive and systemic factors. Cognitive errors, such as the failure to synthesize available evidence or utilize physical examination and test data effectively contribute significantly to misdiagnoses.7,20 Additionally, systemic flaws including communication breakdowns, inadequate access to medical records, and limited availability of specialists compound these issues.13,21 Many errors occur before laboratory tests in a phase where systemic failures are particularly evident.7,22,23
In Uganda, key structural issues that contribute to diagnostic errors exist including the inability to track patients and abnormal findings over time, insufficient recognition of critical symptoms (or “red flags”), and the lack of reliable quality measurement and feedback systems to assess diagnostic performance. Additional structural concerns stem from pressures related to clinical productivity, legal considerations, reimbursement challenges, and the burden of mandatory quality measurements.6
Healthcare safety teams are encouraged to focus not only on structural factors but also on process factors involved in the patient-provider encounter, including the history-taking, physical exams, ordering necessary tests or referrals, interpreting diagnostic tests, and tracking diagnostic information over time.2,13,20 The identification of intermediate outcomes, such as safe diagnosis—ensuring diagnoses are accurate and timely is essential, alongside accounting for patient and healthcare delivery outcomes.
Further discussions revealed specific structural factors such as gender stereotypes in healthcare-seeking behavior, lower health literacy, cultural norms, delayed health-seeking behaviors, and the temporal context of hospitalization (eg, night versus day, weekends versus weekdays).20 Notably, male patients frequently face misdiagnosis due to lower health literacy levels and a healthcare system that often prioritizes women’s and children’s health. Nighttime admissions particularly increase the risk of misdiagnosis as care is typically focused on stabilizing patients rather than thorough investigation, compounded by clinician fatigue and limited access to diagnostic tools during these hours.
Additional structural contributors to diagnostic errors encompass issues related to human resources, such as understaffing, inadequate training, and insufficient mentoring, which hinder diagnosticians in effectively managing various medical conditions, especially in resource-limited settings.11,20 Leadership and governance challenges, including poor oversight and a lack of a patient safety culture, further exacerbate diagnostic errors. The financing structure of Uganda’s healthcare system plays a critical role. Out-of-pocket payments, particularly in private-for-profit facilities, may lead to diagnostic malpractice, where financial incentives override the commitment to accurate diagnoses.
Conversely, public health facilities may focus less on diagnostic precision due to accessibility challenges such as limitations in medical technology and equipment, access to laboratory, imaging, and radiological resources which hamper timely and precise diagnostic capabilities.20,24
Overall, a multifaceted approach that addresses cognitive errors, systemic flaws, human resource challenges, financial incentives, and technological deficiencies is crucial for reducing diagnostic errors in any healthcare setting.
Adequate Laboratory and Imaging Services as a Means to Prevent Diagnostic Errors
The second major theme focused on the importance of adequate laboratory and imaging services in preventing diagnostic errors.
High quality, timely laboratory tests and imaging are crucial for accurate diagnosis and treatment decisions.12,25 Access to accurate test results and appropriate imaging allows healthcare professionals to make informed decisions, reduce misdiagnoses, and improve patient outcomes.
The MOH Uganda emphasizes the importance of well-equipped medical laboratories through its national health laboratory services policy and strategic plan.14,15,26 Despite this, many of its public health facilities face diagnostic challenges due to inadequate funding, which undermines the quality of healthcare services. A survey revealed that many lower-level health centers (levels III–IV) in Uganda lacked essential resources such as equipment, reagents, and rapid test kits for critical diagnostic tests, resulting in delays and diagnostic errors.24
To enhance access to laboratory services in Uganda healthcare, strategies like mobile labs and a hub system for transferring tests to higher-level facilities have been initiated. When laboratories are unable to perform necessary tests, patients are referred to higher-level or private facilities for those services.15,27
It is also crucial to understand that errors can occur even with correctly performed tests. A significant number of laboratory errors arise from improperly completed request forms, often due to a lack of compliance with standard operating procedures and inadequate cooperation from lab staff.12,21,25,28
Ministries of Health should always advocate for better diagnostic stewardship, urging healthcare providers to assess pre-test probabilities. Additionally, experts stressed the importance of laboratory accreditation, standardization in testing procedures, proper documentation and interpretation of results, and effective communication between laboratory professionals, radiologists, and clinicians to prevent errors that could lead to patient harm.
Training for sample collectors could also minimize diagnostic errors caused by delays in reporting, as many test results remain pending for days. Overall, addressing these challenges is essential for improving laboratory services and ensuring better health outcomes.
Existing Health System Interventions to Reduce Diagnostic Errors in Uganda Healthcare
During the commemoration events, health officials underscored the importance of collective efforts to improve healthcare quality. They emphasized active stakeholder engagement, including healthcare providers and patients, in refining the diagnostic process. Patients were encouraged to advocate for their safety, playing a vital role in reducing diagnostic errors.
The Ministry of Health in Uganda has made significant investments in diagnostic equipment and infrastructure, including advanced technologies such as CT (computed tomography) scanners at Regional Referral Hospitals. Additionally, over 73 laboratories in government hospitals have achieved international accreditation standards,5,15,16 underscoring significant advancements in the quality of laboratory services.
Uganda’s patient referral systems facilitate the transfer of patients to higher-level care, ensuring access to qualified personnel and advanced diagnostic services at national referral hospitals, including specialized centers for cancer and heart diseases.14,15
The implementation of the 5S (sort, set, shine, standardize and sustain) at Uganda health facilities since 2010,29 with regular assessments for both public and private facilities have improved management practices at workplace as well as continuous quality improvement. Additionally, the Ministry’s Client Satisfaction Feedback Initiative30 has allowed patients to report gaps in healthcare services directly, promoting patient-centered care and community engagement.
In Uganda, medical training includes an intensive five-year program followed by a one-year supervised internship, preparing doctors to make accurate diagnoses using the International Statistical Classification of Diseases (ICD).31 To uphold high standards of care, healthcare professionals must annually earn continuous professional development (CPD) points for license renewal. This requirement is crucial for ensuring ongoing skill enhancement and effectiveness in patient care.
All in all, diagnostic errors are complex to understand, requiring detailed chart reviews by trained professionals or peer reviews by subsequent physicians.10,25 Each instance of diagnostic error—whether found through chart reviews or peer reports—should be treated as an opportunity for analyzing the diagnostic process and implementing quality improvement measures.
Blaming individuals for diagnostic errors is counterproductive, as errors are inevitable for all clinicians. Instead, fostering open discussions and focusing on systemic improvements alongside individual skill development is essential for continuous improvement in diagnostics.9
Ministries of Health should prioritize minimizing diagnostic errors through effective interventions, collaboration with patients, healthcare workers, and leaders, and adherence to the principle of “First, do no harm”. This approach promotes patient safety and cultivates accountability and excellence in healthcare.
Empowering Patients and Families to Actively Engage with Their Health Care Providers
Patient empowerment emerged as the central theme of the WPSD 2024 commemoration in Uganda, as empowered patients play a crucial role in improving healthcare quality and reducing diagnostic errors. Experts emphasized the importance of seeking second opinions and ensuring patient access to medical records, among other strategies, to prevent misdiagnoses and promote greater patient engagement in healthcare.
The MOH Uganda has enhanced the human rights-based approach to provide health services. In collaboration with partners, there is a revised Patients’ Charter,32 outlining the rights and responsibilities of patients. Mechanisms for feedback and redress at health facilities are assessed through the Client Satisfaction Feedback Initiative.30 Healthcare workers have been empowered through capacity-building initiatives to educate both patients and colleagues about the Right to Health, as outlined in the Patients’ Charter. These efforts promote access to medical information and encourage improved communication regarding treatment options.
Conflicts between patients and healthcare workers have been effectively addressed through targeted training and community dialogue. These efforts have strengthened feedback mechanisms at health facilities by fostering communication through community meetings and supporting the Health Unit Management Committees (HUMCs).
There are also ongoing campaigns focusing on promoting health-seeking behavior, emphasizing early diagnosis and improving the interaction time between healthcare providers and patients (Figure 1). The belief is that a knowledgeable patient is an empowered patient, capable of making informed decisions about their care.
 |
Figure 1 Demonstration of Community Health Initiatives for Improving Patient Safety at the World Patient Safety Day 2024 Commemoration in Uganda. |
Despite these initiatives, challenges still exist particularly in ensuring diagnostic equipment availability, promoting patient responsibility for their health, maintaining confidentiality of patient information, and establishing a centralized information system for patient records to minimize diagnostic errors.
Multi-Level Approaches for Improving Diagnostic Safety
During the World Patient Safety Day 2024 commemoration in Uganda, discussions led to key recommendations for improving diagnostic safety in similar healthcare settings. Leveraging the Safer Dx framework,2 which underscores the complexity of diagnostic errors, a series of interventions were proposed at the national, health facility, and community levels to address sociotechnical gaps in diagnostic safety.
National Level Interventions
The Ministries of Health must take the lead role by developing a comprehensive national patient safety framework and implementation plan that prioritizes diagnostic safety within the broader scope of patient safety and quality improvement initiatives. Diagnostic errors should be seen as opportunities for learning, ultimately leading to enhancements in healthcare quality. A significant step forward would be the establishment of standardized mechanisms and incentives for healthcare providers to voluntarily report diagnostic errors.
Currently, very few hospitals in Uganda have a medical error reporting system in place,4 which hampers transparency and accountability regarding adverse events during medical practice. For facilities already engaged in reporting adverse events, it is essential to integrate diagnostic error reporting into existing systems to create a holistic approach to patient safety.
Supportive Supervision and Healthcare System Reorientation
Enhancing technical supportive supervision specifically targeting diagnostic safety is crucial. In Uganda, previous efforts have primarily focused on enhancing patient safety culture in regional referral hospitals (RRHs). To build on this progress, technical teams at RRHs should expand their oversight to district general hospitals and lower-level health facilities through a structured regional supportive supervision system.
Health facility managers should focus on internal supportive supervision and optimize care, particularly during nights and weekends when staffing shortages impact quality. Health systems must adapt to changing demographics, including multimorbidity and emerging diseases,33 while healthcare services and health management information systems (HMIS) should support an aging population. Additionally, targeted interventions are needed to address men’s health-seeking behaviors, as many experience delays or inaccuracies in diagnosis.
Digitization and EHR Implementation
Fast-tracking the institutionalization of Electronic Health Records (EHRs) integrated with decision support systems can further improve diagnostic accuracy. Evidence from developed nations shows that EHRs have significantly reduced diagnostic errors.8,28 Following the Ministry of Health’s digitization efforts initiated in 2023, it is imperative to implement these systems comprehensively across all health facilities. Additionally, enhancing utilization of technology, such as precision medicine and artificial intelligence (AI), can alleviate healthcare workers’ burdens and enhance care,34,35 particularly in rural areas with limited resources.
Regulation of Private Healthcare Practices
To bolster patient safety within the broader healthcare ecosystem, improving regulation of private healthcare practices is necessary. There has been increasing concern regarding unethical practices by some private clinicians who may intentionally misdiagnose or recommend unnecessary investigations for profit.4,36 The MOH must ensure adherence to patient safety standards in private facilities, preventing profit-driven motives from overshadowing patient care.
Continuous Education and Team Communication
Mandatory continuous professional development and medical education programs are essential for healthcare professionals, especially in emergency and outpatient departments, to ensure accurate diagnostics. Restructuring services and implementing diagnostic protocols will further enhance accuracy. Cultivating a patient safety culture that prioritizes diagnostic accuracy, supported by tools like autopsies and clinical discrepancy reviews, is key. Treating diagnostic errors as learning opportunities helps improve patient care and reduce future errors.
Teamwork and Communication Enhancement
Maximizing teamwork and communication among healthcare teams is key to improving diagnostic outcomes. Online peer-to-peer consultations provide real-time second opinions, enhancing diagnostic safety and fostering trust. Collaboration across specialties helps reduce diagnostic errors and improves patient outcomes.
Limitations and Future Research Recommendations
This review provided a comprehensive qualitative synthesis of Uganda’s diagnostic safety challenges by integrating insights from World Patient Safety Day 2024 with existing literature, offering context-specific analysis and policy-relevant recommendations grounded in established frameworks. While its multi-stakeholder approach and localized focus represent key strengths, limitations include reliance on self-reported data, limited generalizability, and lack of quantitative metrics. Future research should prioritize quantitative error tracking systems, expanded private sector inclusion, longitudinal studies, and pilot testing of proposed interventions like AI decision-support tools to strengthen evidence and validate findings in comparable LMIC settings, ultimately advancing diagnostic safety improvements.
Conclusions
The 2024 World Patient Safety Day commemoration in Uganda has illuminated critical gaps and opportunities in diagnostic safety within resource-constrained settings. This review underscores that diagnostic errors driven by systemic inefficiencies, cognitive biases, and technological limitations are not inevitable but require deliberate, multi-level interventions. Uganda’s progress in laboratory accreditation, digital health adoption, and community engagement offers a foundation for scalable solutions, yet challenges persist, particularly in private-sector regulation, workforce training, and equitable access to diagnostics.
The proposed strategies ranging from national policy reforms (eg, mandatory error reporting systems) to localized actions (for example, patient empowerment campaigns) provide a roadmap for reducing diagnostic errors. Crucially, these recommendations align with global patient safety agendas while remaining adaptable to Uganda’s unique context. For policymakers, this study highlights the urgency of investing in diagnostic infrastructure and governance; for healthcare workers, it stresses the need for continuous learning and teamwork; and for patients, it reaffirms their role as active partners in the diagnostic process.
Moving forward, implementation research must test these interventions, particularly the integration of artificial intelligence and electronic health records in low-resource settings. By fostering collaboration among stakeholders and centering patient safety as a shared priority, Uganda can model transformative change for similar health systems worldwide. The lessons from WPSD 2024 are clear: accurate diagnosis is both a moral imperative and achievable target, one that demands commitment, innovation, and collective action.
Acknowledgments
The organization of the World Patient Safety Day (WPSD) 2024 Commemoration in Uganda received valuable support from Uganda COVID-19 Response and Emergency Preparedness Project (UCREPP), Japan International Cooperation Agency (JICA), World Health Organization (WHO) Uganda, National Drug Authority (NDA), Johns Hopkins Program for International Education in Gynecology and Obstetrics (JhPeigo) Uganda, and Uganda National Health Consumers’ Organization (UNHCO). Special thanks to Prof. Adam J Rose of Hebrew University of Jerusalem for his technical input and to Ministry of Health officials for their contributions regarding WPSD 2024 Commemoration in Uganda.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization. World patient safety day, 17 September 2024: “improving diagnosis for patient safety”. 2024.
2. Singh H, Sittig DF. Advancing the science of measurement of diagnostic errors in healthcare: the safer dx framework. BMJ Qual Saf. 2015;24(2):103–110. doi:10.1136/bmjqs-2014-003675
3. Zimolzak AJ, Wei L, Mir U, et al. Machine learning to enhance electronic detection of diagnostic errors. JAMA Network Open. 2024;7(9):e2431982. doi:10.1001/jamanetworkopen.2024.31982
4. Mauti G, Githae M. Medical error reporting among physicians and nurses in Uganda. Afr Health Sci. 1970;19(4):3107–3117. doi:10.4314/ahs.v19i4.33
5. Ministry of Health. Annual health sector performance report 2023/24. 2024. Available from: https://library.health.go.ug/monitoring-and-evaluation/annual-quarterly-performance-reports/annual-health-sector-performance-8.
6. Katongole SP, Akweongo P, Anguyo R, Kasozi DE, Adomah-Afari A. Prevalence and classification of misdiagnosis among hospitalised patients in five general hospitals of central Uganda. Clinical Audit. 2022;14:65–77. doi:10.2147/CA.S370393
7. Asmelash D, Worede A, Teshome M. Extra-analytical clinical laboratory errors in Africa: a systematic review and meta-analysis. EJIFCC. 2020;31(3):208–224.
8. Dixit RA, Boxley CL, Samuel S, Mohan V, Ratwani RM, Gold JA. Electronic health record use issues and diagnostic error: a scoping review and framework. J Patient Saf. 2023;19(1):e25–30. doi:10.1097/PTS.0000000000001081
9. Balogh EP, Miller BT, Ball JR. Improving Diagnosis in Health Care. Washington, D.C: National Academies Press; 2015.
10. Abimanyi-Ochom J, Bohingamu Mudiyanselage S, Catchpool M, Firipis M, Wanni Arachchige Dona S, Watts JJ. Strategies to reduce diagnostic errors: a systematic review. BMC Med Inform Decis Mak. 2019;19(1):174. doi:10.1186/s12911-019-0901-1
11. Manyazewal T. Using the world health organization health system building blocks through survey of healthcare professionals to determine the performance of public healthcare facilities. Arch Public Health. 2017;75(1):50. doi:10.1186/s13690-017-0221-9
12. Plebani M. Diagnostic errors and laboratory medicine - causes and strategies. EJIFCC. 2015;26(1):7–14.
13. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO. diagnostic errors: technical series on safer primary care. 2016.
14. Ministry of Health Uganda. Ministry of health launches $5 million laboratory systems strengthening (ILSS) project. Available from: https://cphl.go.ug/ministry-health-launches-5-million-laboratory-systems-strengthening-ilss-project.
15. Ministry of Health. Uganda national health laboratory services strategic plan 2021-25. 2021. Available from: https://guluhospital.net/wp-content/uploads/2023/01/NATIONAL-HEALT-LAB-SERVICES-STRATEGIC-PLAN.pdf.
16. SLMTA. SLMTA laboratories that have achieved accreditation. 2024. Available from: https://slmta.org/accredited-labs/.
17. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
18. Moore L, Lavoie A, Bourgeois G, Lapointe J. Donabedian’s structure-process-outcome quality of care model. J Trauma Acute Care Surg. 2015;78(6):1168–1175. doi:10.1097/TA.0000000000000663
19. Berwick D, Fox DM. “evaluating the quality of medical care”: donabedian’s classic article 50 years later. Milbank Q. 2016;94(2):237–241. doi:10.1111/1468-0009.12189
20. Dorothy A, Yadesa TM, Atukunda E. Prevalence of medication errors and the associated factors: a prospective observational study among cancer patients at Mbarara regional referral hospital. Cancer Manag Res. 2021;13:3739–3748. doi:10.2147/CMAR.S307001
21. Clark BW, Derakhshan A, Desai SV. Diagnostic errors and the bedside clinical examination. Med Clin North Am. 2018;102(3):453–464. doi:10.1016/j.mcna.2017.12.007
22. Alrashidi MMO, Alharbi ASW, Alharbi ASW, Alharbi MSA, Alharbi NMA. Analyzing errors in laboratory testing: causes and prevention strategies. N Am J Med Sci. 2022;19(S8):1152–1562.
23. Plebani M. Quality indicators to detect pre-analytical errors in laboratory testing. Clin Biochem Rev. 2012;33(3):85–88.
24. Namuhani N, Namusoke Kiwanuka S, Akulume M, Kalyesubula S, Bazeyo W, Nakanwagi Kisakye A. Laboratory diagnostics performance in Uganda: a survey of test availability and constraints. J Interventional Epidemiol Public Health. 2024;7(10). doi:10.37432/jieph.2024.7.1.101
25. van Moll C, Egberts T, Wagner C, Zwaan L, ten Berg M. The nature, causes, and clinical impact of errors in the clinical laboratory testing process leading to diagnostic error: a voluntary incident report analysis. J Patient Saf. 2023;19(8):573–579. doi:10.1097/PTS.0000000000001166
26. Ministry of Health U. Uganda national health laboratory services policy. Available from: https://ahpc.ug/sites/default/files/2024-06/UGANDA%20NATIONAL%20HEALTH%20LABORATORY%20SERVICES%20POLICY.pdf.
27. Health Journalist Network in Uganda. Uganda launches $5 million strategic plan to enhance children surgery. Available from: https://hejnu.ug/moh-launches-first-ever-5-million-strategic-plan-to-enhance-children-surgery/.
28. Improved diagnostics & patient outcomes. Available from: https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/improved-diagnostics-patient-outcomes.
29. Ministry of Health U. 5S-continuous quality improvement (Kaizen)-total quality management implementation guidelines in Uganda. 2019. Available from: https://library.health.go.ug/sites/default/files/resources/5S-CQI-TQM%20Guidelines%20signed%20copy%202.pdf.
30. Ministry of Health. Routine client satisfaction feedback implementation guidelines. 2024. Available from: https://library.health.go.ug/clinical-services/routine-client-satisfaction-feedback-implementation-guidelines.
31. WHO. ICD-11 for mortality and morbidity statistics (Version: 01/2023). Available from: https://icd.who.int/browse11/l-m/en.
32. Ministry of Health U. Ministry of health clients charter 2021. 2021. Available from: https://library.health.go.ug/sites/default/files/resources/MoH%20Client%20Chater%20July%202021.pdf.
33. Mbonye MK, Burnett SM, Colebunders R, et al. Disease diagnosis in primary care in Uganda. BMC Fam Pract. 2014;15(1):165. doi:10.1186/1471-2296-15-165
34. Johnson KB, Wei W, Weeraratne D, et al. Precision medicine, AI, and the future of personalized health care. Clin Transl Sci. 2021;14(1):86–93. doi:10.1111/cts.12884
35. Zlobina K, Jafari M, Rolandi M, Gomez M. The role of machine learning in advancing precision medicine with feedback control. Cell Rep Phys Sci. 2022;3(11):101149. doi:10.1016/j.xcrp.2022.101149
36. Simon Peter K, Robert Anguyo DDMO, Nanyingi M, Stella Regina N. Common medical errors and error reporting systems in selected hospitals of central Uganda. Int J Public Health Res. 2015;3(5):292–299.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnostic Challenges and Patient Safety: The Critical Role of Accuracy – A Systematic Review
Alharbi TAF, Rababa M, Alsuwayl H, Alsubail A, Alenizi WS
Journal of Multidisciplinary Healthcare 2025, 18:3051-3064
Published Date: 30 May 2025