")
Back to Journals » Infection and Drug Resistance » Volume 18
Epidemiological Trends and Antimicrobial Resistance of Candida auris: A Focus on 7 Cases in a Single Medical Institution of Southern China
Authors Wang Y, Lin L, Li J, Wang X, Zhang J, Xi L, Cai W, Lu S
Received 6 January 2025
Accepted for publication 8 May 2025
Published 16 May 2025 Volume 2025:18 Pages 2557—2568
DOI https://doi.org/10.2147/IDR.S512301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi Ruan
Yihui Wang,* Li Lin,* Jiahao Li,* Xiaoyue Wang, Junmin Zhang, Liyan Xi, Wenying Cai, Sha Lu
Department of Dermatology and Venereology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Sha Lu, Email [email protected]
Background: Candida auris is an emerging multidrug-resistant yeast associated with high transmission rates in healthcare settings. This study investigates C. auris infections/colonization in a single institution to elucidate their clinical and epidemiological patterns, with the ultimate aim of informing infection control measures.
Objective: To characterize the genetic basis of antifungal resistance in C. auris, specifically through ERG11 gene mutation analysis, and correlate these findings with clinical outcomes and epidemiological data. The results are intended to guide the development of targeted strategies for outbreak prevention and resistance mitigation.
Methods: A case series study of seven C. auris-infected/colonized patients (May–September 2023 and April 2024) was conducted. Epidemiological and clinical data were collected, and ITS and SNP analyses were used to examine genetic relationships and resistance profiles, focusing on fluconazole, amphotericin B, and ERG11 gene mutations.
Results: All seven C. auris isolates were fluconazole resistant, with three also resistant to amphotericin B. ITS and SNP analysis identified two geographic clades (I and III), with clade III strains sharing ERG11 mutations (V125A, F126L) and one clade I strain showing the Y132F mutation. These markers shed light on resistance mechanisms and clade-specific clustering. All patients were elderly individuals (≥ 64 years old) with severe underlying conditions admitted to the ICU. After C. auris was detected, their treatment became delayed or inefficient, resulting in poor clinical outcomes.
Conclusion: This study highlights the value of SNP and ITS analysis in uncovering genetic diversity and adaptation in C. auris. The consistent mutations in Clades I and III enhance our understanding of the genetic mechanisms influencing ERG11 gene variability across clades. Additionally, the challenges in managing multidrug-resistant C. auris infections, especially in elderly patients with severe comorbidities, emphasize the urgent need for effective surveillance, infection control, and new antifungal agents.
Keywords: Candida auris, candidemia, epidemiological trends, clinical characteristics, drug resistance profile, prevention strategy
Introduction
Since the initial reports on Candida auris were published in Japan in 2009,1 this pathogenic fungus has spread to at least 39 countries across all inhabited continents. It tends to cause outbreaks in medical institutions because of its ability to colonize the skin, anterior nares, and other body sites of asymptomatic carriers,2,3 with fluconazole-resistant strains being observed in mostly clinical isolates.4–6
Distinct clades were identified for each geographical region through genotypic analyses, revealing a shared clonal origin within each clade,5,7–9 implying the introduction and local dissemination of C. auris at multiple sites. The rapid acquisition of antifungal resistance is a distinctive characteristic of C. auris. The majority of isolates from clades I and III (over 90%) exhibit acquired resistance to fluconazole,4,5 a crucial component in the treatment of invasive candidiasis. Furthermore, these clades have been reported to exhibit antifungal resistance toward polyenes and echinocandins. Moreover, Clade II isolates are susceptible to azoles and other commonly used antifungal drugs.10,11 Investigations into the mechanisms of resistance in C. auris are currently underway. Mutations causing amino acid substitutions (AASs) in the drug target gene ERG11, which are known to be associated with azole resistance in Candida albicans, have been identified and found to correlate with distinct geographical clades.7 Furthermore, TAC1 orthologues (TAC1a and TAC1b) were annotated, with recent evidence suggesting the involvement of TAC1b in azole resistance.12,13 Recent studies show that the three common C. auris’s ERG11 mutations (VF125AL, Y132F, K143R) significantly increase resistance to fluconazole and voriconazole.14 But no single mutation alone causes clinical drug resistance, which cannot fully explain the significant MIC increase in clinical C. auris isolates. However, TAC1b mutations and its impact on azole resistance are applicable to C. auris remain to be investigated. Thus, more clinical data is needed for detailed verification.
In contrast to the majority of Candida spp. infections originating from commensal flora, C. auris has pronounced potential for interhuman transmission, with isolates obtained from the same healthcare unit exhibiting an identical clonal origin.4,15 The overall mortality rate associated with C. auris infections is notably elevated (40–60%), which is attributed primarily to the severe underlying conditions of patients and the increasing resistance to azoles, amphotericin B, and echinocandins.16,17 The limited therapeutic options combined with the persistent nosocomial presence of this fungus raise concerns regarding large-scale nosocomial outbreaks.
Therefore, it becomes imperative to provide important insights into the epidemiological and resistance characteristics of C. auris infection, offering strategies for clinical prevention and control. In this article, we present a case series of five patients with C. auris infections/colonization concentrated in a single medical institution from May to September 2023, along with two patients colonized with C. auris in April 2024. These patients exhibit certain similar epidemiological and clinical characteristics, and the isolates display consistent drug resistance profiles through single-nucleotide polymorphism (SNP) identification.
Materials and Methods
Patient Information
A retrospective analysis of the medical records of patients diagnosed with C. auris infections/colonization at a single medical institution during the aforementioned period was conducted. Clinical data, including age, sex, underlying diseases, intensive care unit (ICU) admission details, duration of catheterization, previous Candida spp. data concerning infection, antifungal drug use, laboratory results (including G/GM test), treatment regimens, and outcomes were collected and analysed.
Information on the Isolated C. auris Strains
Seven isolates from 7 patients from 2023 to 2024 were collected from a single medical institution (n = 5,2023; n = 2,2024). The isolates were from blood (n = 1), urine (n = 2), sputum (n = 2), or BALF (n = 2).
Antifungal susceptibility tests were performed according to CLSI protocol M38–Ed3. To date, there are no species-specific antifungal susceptibility breakpoints established for C. auris. The antifungal resistance for C. auris was analyzed according to the tentative minimum inhibitory concentrations (MIC) breakpoints published by the CDC (https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html). The strains of C. parapsilosis (ATCC 22019) were used as quality controls.
All the isolates were identified as C. auris via matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) and rDNA ITS sequencing. The genomic DNA of C. auris (SUMS1057; SUMS1056; SUMS1055; SUMS1073; SUMS1075; SUMS1105; SUMS1106) was extracted using the TlANamp Yeast DNA Kit (TIANGEN) following the manufacturer’s instructions. The rDNA internal transcribed spacer (ITS) was amplified using 2 x Tag, Master Mix (Vazyme) and primers ITS-4 (TCCTCCGCTTATTGATATGC) and ITS-5 (GGAAGTAAAAGTCGTAACAAGG). The primers used for amplification of the ERG11 region are listed in Table 1.
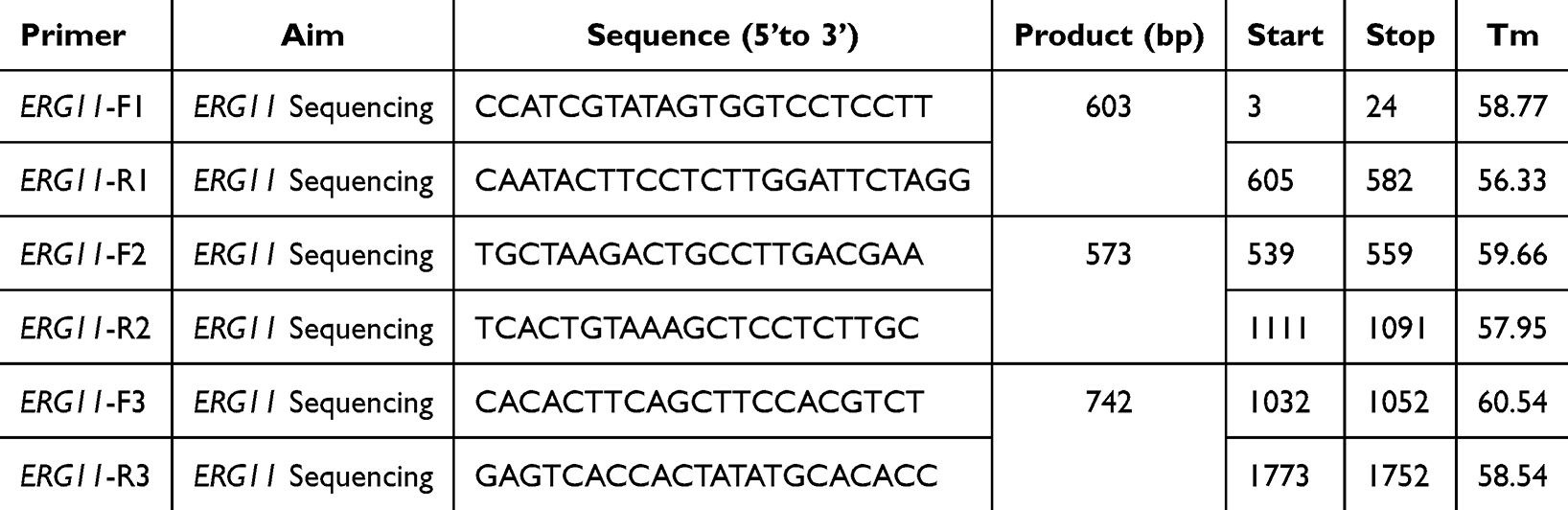 |
Table 1 The Primers Used for Sequencing ERG11 are Listed in the Table |
The PCR products were subjected to Sanger sequencing Biotech), and the resulting sequences were analyzed usingGeneious Prie softwareSangon (https://www.geneious.com) and NCBI BLAST (https://blast.ncbi.nlm.nih.gov). Phylogenetic analysis was accomplished using ega 11 software (https:/www.megasoftware.net) with the Neighbor-joining method based on Maximum Composite Likelihood. Saccharomyces spp and Cryptococcus spp were used as the outgroup. All sequences identified in this study were saved in GenBank. The accession number (ITS:PV093539-PV093545;ERG11: PV114910-PV114916).
Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. Prior to participation, the participants gave their signed, informed consent. The Clinical Research Ethics Committee of Sun Yat-sen Memorial Hospital provided ethical approval.
This study complies with all relevant national and international regulations regarding ethical research involving human subjects. All patient data were anonymized according to HIPAA and GDPR standards. The study followed the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC) guidelines for Candida auris infection control and adhered to all necessary biosafety measures. By following these regulations and guidelines, the study maintains high standards of ethical conduct, data protection, and patient safety, contributing valuable insights into Candida auris infection management.
Results
Antimicrobial Resistance
Internal Transcribed Spacer (ITS) 4/5 sequencing revealed that all the C. auris strains were isolated from the seven patients (hereafter referred to as C1, C2, C3, C4, C5, C6 and C7), belonging to geographic clades I and III, respectively (Figure 1). C2, C3, C4 and C6 were identified as strains of Clade III (South Africa), whereas C1, C5 and C7 belonged to Clade I (South Asia). The antifungal susceptibility results of the C. auris isolates are shown in Table 2 on the basis of tentative MIC breakpoints published by the CDC (https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html). All the isolates exhibited resistance to fluconazole (MIC range: 64–256 μg/mL), whereas all the other isolates were susceptible to echinocandins (MIC range: anidulafungin: 0.12–1 μg/mL, microfergin: 0.03–2 μg/mL, caspofungin: 0.12–0.5 μg/mL). A total of 3/7 of the strains exhibited resistance to amphotericin B, with an MIC of 2 μg/mL.
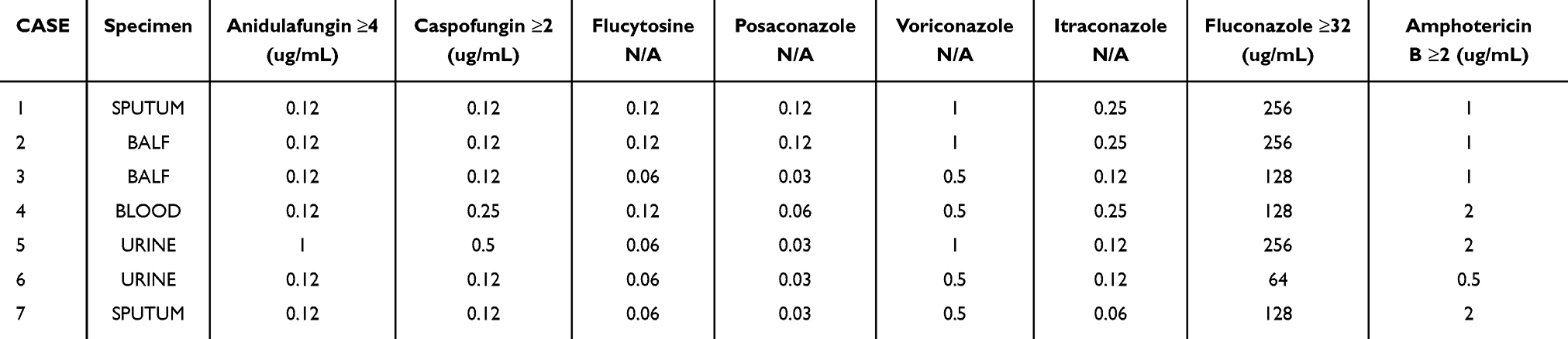 |
Table 2 The Antifungal Susceptibility Profile of the Seven C. auris Isolates |
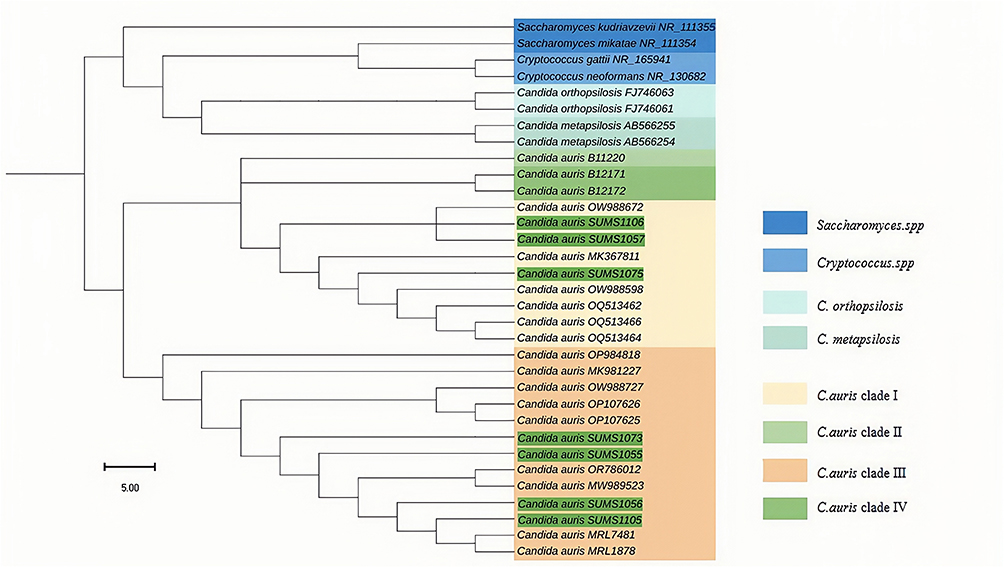 |
Figure 1 Maximum-likelihood phylogenetic tree of the 7 isolated C. auris strains. The tree was generated by using the ITS region of Candida auris strains with closely related Candida species. The scale bar indicates the branch length. Different colored branches denote different lineages. The seven isolates in the present study are covered with green bars. The corresponding strain numbers are as follows: C1, Candida auris SUMS1057; C2, Candida auris SUMS1056; C3, Candida auris SUMS1055; C4, Candida auris SUMS1073; C5, Candida auris SUMS1075; C6, Candida auris SUMS1105; and C7, Candida auris SUMS1106. |
ERG11 Mutation Analysis
In this study, we investigated the SNP mutations in the ERG11 gene (primers listed in Table 1) among two clades: Clade I and Clade III. The strains analysed were C1, C5, and C7 for Clade I and C2, C3, C4, and C6 for Clade III (Figure 2). The specific loci examined were positions 50, 125, 126, 132, 187, 243, 288, and 476 (Figure 3). In Clade III, samples C2, C3, C4, and C6 all presented missense mutations at position 125 (GTT > GCT), resulting in a valine to alanine substitution (V125A), and at position 126 (TTC > CTC), resulting in a phenylalanine to leucine substitution (F126L). In Clade I, strains C1 and C7 lacked missense mutations at positions 125 and 126, as well as synonymous mutations at position 243. In contrast, strain C5 shared the same missense mutations at positions 125 and 126 with Clade III. Notably, only strain C7 carried a missense mutation at position 132 (TAC > TTC), resulting in a tyrosine-to-phenylalanine substitution (Y132F). Additionally, all the samples in Clades I and III had identical synonymous mutation sites at positions 50, 187, and 476.
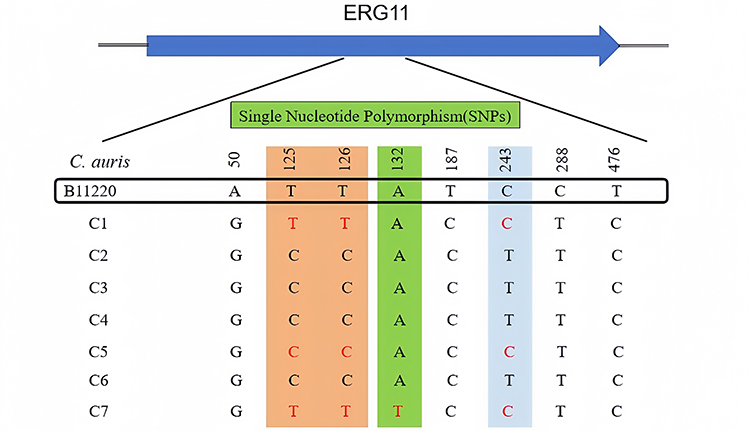 |
Figure 2 Distribution of single-nucleotide polymorphisms (SNPs) in the ERG11 gene among the 7 isolated C. auris strains. The bars in Orange refer to the 2 missense mutations found in C2, C3, C4, and C6, which were identified as clade III; The bars in green refer to the 1 missense mutation found in C1, C5, and C7, which was identified as clade I; And the bars in blue refer to C1, C5, and C7, which were identified as clade I and did not exhibit any mutation at position 243 of the ERG11 gene locus.The red letters in the orange bars represent bases at positions 125 and 126 of C1, C5, and C7 for comparison with other clade of C. auris; The red letters in the green bar represent bases at positions 132 of C7 for comparison with other strains of C. auris; The red letters in the blue bars represent bases at positions 243 of C1, C5, and C7 for comparison with other clade of C. auris; Inside the black rectangle is the fluconazole-susceptible strain B11220 used as a control. |
 |
Figure 3 Amino acid sequence variations (AASs) in the ERG11 gene among the 7 isolated C. auris strains. A total of 8 AASs corresponding to ERG11 were identified for 7 C. auris isolates (the strains isolated from the seven patients). The bars in green refer to the 3 missense mutations, V125A, F126L, and Y132F. The text in red represents the base of the mutation site corresponding to each amino acid mutation. |
Epidemiological and Clinical Features
As shown in Table 3, all patients were elderly individuals (≥64 years old) with severe underlying diseases admitted to the intensive care unit (ICU). The mean time from admission to C. auris detection was 39.4 days (range: 1–56 days) (Figure 4A), with an average duration of catheterization of 30.6 days (range: 3–49 days) (Figure 4B). Four of the seven patients had a history of previous Candida spp. infection/colonization involving Candida albicans (C2, C4, C5) or Candida tropicalis (C3). Six patients had documented prior use of antifungal medication, predominantly caspofungin (C2, C3, C4, C5, C6, and C7), while amphotericin B (C5), fluconazole (C3) and voriconazole (C5) were also used. In terms of fungal culture, three individuals presented positive single-sample results: C1 and C7 presented positive sputum cultures, whereas C2 presented positive bronchoalveolar lavage fluid cultures. Among the four individuals with positive results in multiple samples or more, C3, C5, and C6 had positive cultures in both the sputum and urine samples, whereas C4 had positive cultures not only in the sputum and urine but also in the blood. In addition, 85% of the 1,3-β-d-glucan (G)/galactomannan (GM) experiments yielded negative results. Following the detection of C. auris, all patients experienced delays or inefficiencies in their treatment, leading to unfavourable clinical outcomes. These included two fatalities, two cases with a Glasgow Coma Scale (GCS) score of E1VTM2, and one case with a modified Rankin scale (mRS) score of 5. The two patients discovered in April 2024 had GCS scores of E2VTM3 and E3VTM3. And C. auris was detected in multiple body sites (oral cavity, axilla, groin) and environmental samples (nasogastric tube, tracheostomy site, bed rail, air) from two patients (C6 and C7), with additional colonization in C7’s urethra and C6’s tracheostomy tube site, reflecting widespread fungal colonization.
 |
Figure 4 The mean time from admission to C. auris detection (A) and the duration of catheterization (B). |
Discussion
Internal Transcribed Spacer (ITS) 4/5 sequencing revealed that all C. auris strains isolated from the seven patients belonged to geographic clades I and III, indicating distinct origins or transmission routes within the studied patient cohort. By December 2023, a total of 312 cases of C. auris infection or colonization had been reported in China.18 Molecular epidemiological analysis revealed the presence of three genetic clades (II, III, and I) among the C. auris isolates in China, with clades I and III being predominant, mirroring our own findings. However, it is important to note that our phylogenetic analysis was based solely on ITS sequences, which, while useful for initial clade classification, may not provide the same resolution as WGS data. This limitation should be considered when interpreting the results, and future studies incorporating WGS are warranted to further elucidate the genetic relationships and potential hospital transmission routes among these isolates.
Consistent with previous studies reporting a high prevalence of acquired fluconazole resistance in clades I and III (>90%),4,18,19 our data consistently revealed that all the isolates exhibited fluconazole resistance while remaining susceptible to echinocandins. Notably, one of the strains exhibited resistance to amphotericin B. However, due to the limited number of cases and the fact that the MIC values for AMB were near the susceptibility breakpoint, the observed resistance may be subject to variability in antifungal susceptibility testing (AFST). Retesting could potentially yield sensitive results, highlighting the need for cautious interpretation of these findings. Further studies are needed to determine whether resistance to amphotericin B is characteristic of a particular C. auris clade. These strains presented significant resistance to fluconazole, a commonly employed antifungal agent, while maintaining sensitivity to echinocandins, which aligns with global trends in C. auris resistance patterns.4 Moreover, the emergence of multidrug-resistant strains was evident through their resistance to amphotericin B, and further complicating treatment strategies are needed. The most common mechanism of azole resistance in C. auris involves mutations in the drug target lanosterol 14-α-demethylase (encoded by the ERG11 gene), such as Y132F, K143R and F126L.20 These substitutions were strongly associated with geographic clades: F126L, Y132F and K143R with (India and Pakistan) clade III and Y132F with Venezuela clade IV. In our study, by comparing ERG11 amino acid sequences between all the isolates and the C. auris strain B11220, 3 amino acid substitutions, including V125A, F126L, and Y132F, were identified in C. auris isolates. The Y132F missense mutation was common in clade IV and clade I. This is consistent with the Y132F mutation found in Clade I. However, the K143R mutation was not detected in any isolates classified within this clade. This finding may suggest that, contrary to previous studies,14 the K143R site may not be critical and requires further investigation to verify. It is worth noting that our study did not include analysis of the FKS1 gene, which is associated with echinocandin resistance. While our focus was primarily on azole resistance mediated by ERG11 and TAC1 mutations, the absence of FKS1 analysis represents a limitation. Future studies should incorporate FKS1 gene analysis to provide a more comprehensive understanding of C. auris resistance mechanisms. The presence of identical silent mutation sites in both Clades I and III suggests a certain degree of genetic similarity, whereas the distinct missense mutations observed in each clade underscore significant genetic differentiation. Given that the majority of C. auris belong to Clades III and the low prevalence of Clades I and IV, further data and studies are needed to investigate whether some genetic correlation also exists between Clades I and IV. Clade III’s conserved mutations at loci 125 and 126, in contrast with Clade I’s unique mutation at locus 132, suggest different evolutionary pressures or functional requirements between the clades. Recent studies have demonstrated that the mutations (VF125AL, Y132F, K143R) mentioned above significantly increase resistance to fluconazole and voriconazole.14 However, no single mutation alone causes the antifungal resistance, which cannot fully explain the significant MIC increase in clinical C. auris isolates. Therefore, additional clinical data are required for further validation.
Among the seven patients who presented with nonspecific clinical manifestations, including chemosis, oral cleft (cheilitis), long-term fever, coma, shock, oliguria, etc., and considering the results of fungal culture for each patient, in accordance with the latest international consensus21 on the diagnosis of invasive candidiasis, one patient (C4) could be proven to have candidemia with probable deep-seated candidiasis, and the remaining six patients could be diagnosed with probable deep-seated candidiasis. This indicates the severity of C. auris infection, which can cause health care-associated outbreaks of lethal candidiasis. These patients had similar characteristics (Table 3), primarily being elderly individuals (≥64 years old) with severe underlying diseases admitted to the ICU. The median duration from admission to C. auris detection was 39.4 days (excluding C4, the average duration was 45.8 days) (Figure 4A). Additionally, the average duration of catheterization was 34.7 days (excluding C4, the average duration was 40 days) (Figure 4B), indicating a potential risk factor for infection development, especially in critically ill patients requiring prolonged catheter use. This resembles the situation observed in China,12 as well as other regions with high incidence rates of C. auris infection, such as Colombia,22 Türkiye23 and India,24 over the past five years. These areas commonly reported a prevalence of elderly patients with multiple comorbidities and critical vital signs, alongside prolonged hospitalization periods and catheterization durations, among other associated risk factors. The abbreviated duration of detection in Patient 4 (C4) could be attributed to the patient’s antecedent history of hospitalization, distinguishing it from other cases. Therefore, beyond C4, we hypothesize that C. auris can typically be identified and diagnosed as “probable deep candidiasis” in high-risk patients more than one month after admission. However, additional data are needed to substantiate this conjecture. Importantly, this raises the question of whether ICU patients presenting severe symptoms could undergo comprehensive screening for C. auris colonization. Aldejohann et al suggested that25 ideally, screening should commence as soon as the first infected patient is admitted to a healthcare facility. If this is not feasible, they recommend setting the start of the screening period at least seven days prior to the date when the second case is identified. However, considering the characteristics of skin colonization prior to C. auris infection, we believe that this method is not timely available at most medical institutions. Therefore, we propose that comprehensive colonization screening should be regularly performed on eligible patients once a week or twice a week, encompassing the entire integumentary system, various types of indwelling catheter surfaces, and the patient’s immediate living environment.
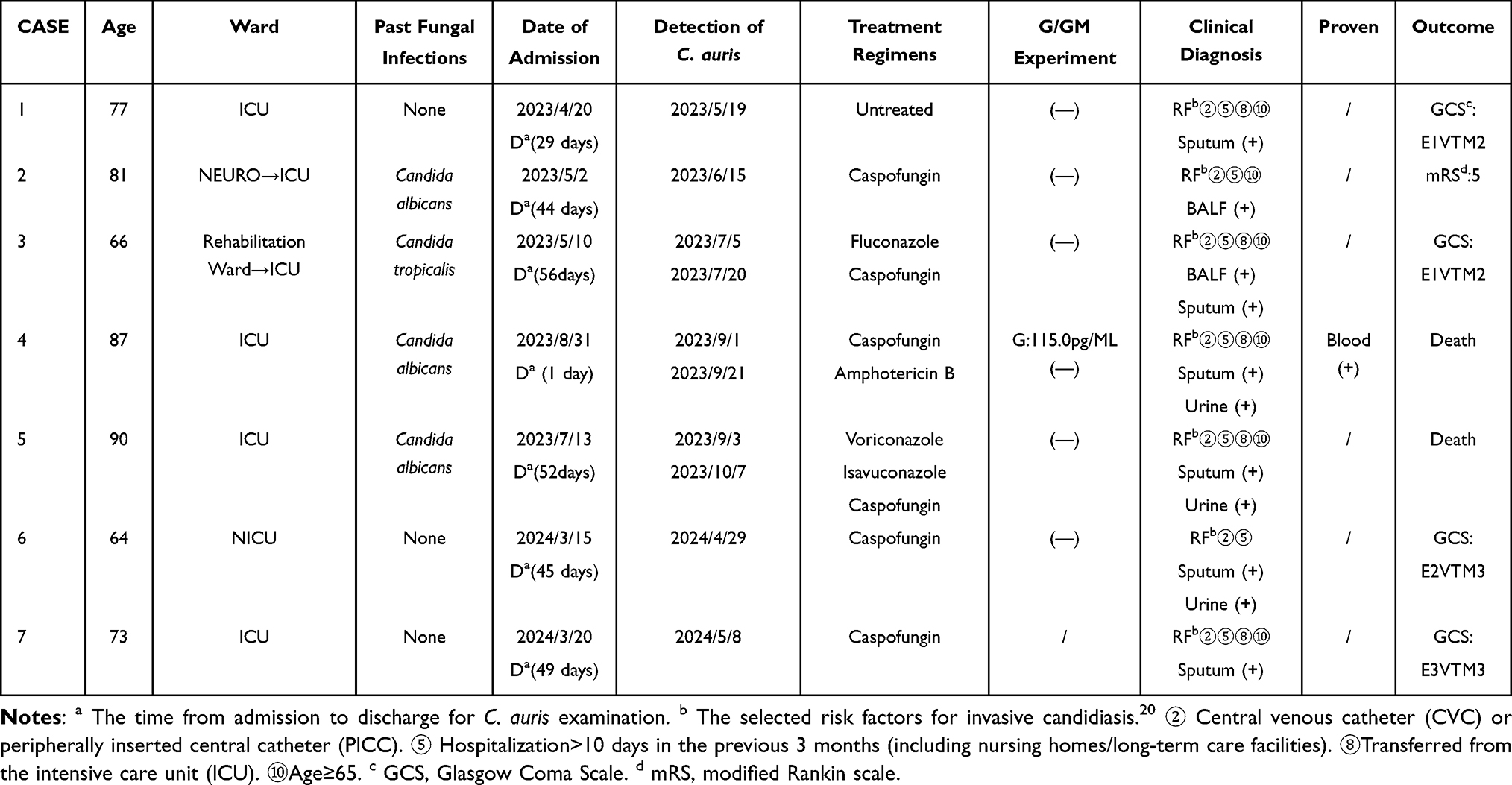 |
Table 3 Epidemiological and Clinical Characteristics of Seven Patients |
In this study, 85% of the GM test results were negative. It is important to note that this outcome may be attributed to the majority of isolates being derived from non-sterile sites. The G/GM test is widely employed as a screening tool for diagnosing fungal infections in clinical settings especially in bloodstream infections, but its specificity and sensitivity in detecting C. auris infections require further validation. Based on our findings, there appear to be limitations associated with traditional diagnostic methods when applied to C. auris infections, underscoring the need for the development of more sensitive and specific diagnostic techniques to enhance early detection and improve treatment outcomes. To date, the MALDI-TOF MS database has been expanded to encompass C. auris. Additionally, a variety of PCR-based assays have been developed for the identification of C. auris in healthcare settings,26,27 including real-time PCR and loop-mediated isothermal amplification assays designed to screen for C. auris on patient skin.28,29 However, not all laboratories can implement laboratory-developed tests, and many do not have access to MALDI-TOF MS or a Vitek 2 system. The number of alternative commercially available tests is still quite limited, which leaves definitive identification of C. auris as a send-out test in many facilities. An especially glaring deficiency is the lack of a point-of-care test for the detection of C. auris colonization. This would be an important tool for the identification of colonized patients, which plays an important role in the implementation of infection control practices, especially in cities where C. auris has become endemic.30
The history of previous Candida spp. Infections/colonization underscores the recurrent nature of fungal infections in this vulnerable patient population. Moreover, all patients had documented prior antifungal drug use, underscoring the importance of preventing, monitoring, and managing drug resistance in clinical practice for individuals with a history of fungal infection who are at increased risk for C. auris infection. In terms of treatment effect, all patients had delayed treatment or ineffective treatment, which we believe partly contributed to the poor clinical outcome of patients based on their poor physical condition. This included two fatalities, two cases with a GCS score of E1VTM2 indicating severe neurological impairment, and one case with a mRS score of 5 indicating severe disability. The subsequent findings of two patients in April 2024 demonstrated marginally improved outcomes compared with those of the initial five patients, as indicated by the GCS scores of E2VTM3 (C6) and E3VTM3 (C7). Notably, comprehensive fungal cultures (Figure 5) were promptly conducted on the entire integumentary system, encompassing the external auditory canal, oral cavity, nasal cavity, axilla, groin, and urethra of two patients identified in April 2024. Additionally, various types of catheter surfaces, including PICCs, CVCs, tracheostomy tube sites, nasogastric tubes and samples from the patient’s immediate living environment, were subjected to analysis. Positive results for C. auris cultures were obtained from samples derived from patient C7’s oral cavity, urethra, axilla, groin and nasogastric tube, whereas positive cultures were observed in samples collected from patient C6’s oral cavity, axilla, tracheostomy tube site, bed rail and air sample (2m2), which is consistent with the previously reported high colonization rate of C. auris documented in the literature.2,3 Therefore, we hypothesize that the inferior prognosis of C6 compared with that of C7 may be attributed to the extensive fungal colonization observed in both in vivo and in vitro settings, particularly the positive detection at sites such as the tracheotomy tube site, bed rail, and air samples. The seven isolates were obtained from distinct patients at different time points, yet they exhibit similar mutations at the ERG11 locus. In conjunction with the environmental investigation results from two patients in 2024, our findings indicate that C. auris infection or colonization can spread within the immediate environment of affected individuals. These observations suggest a potential risk of contact transmission within healthcare settings. However, determining the likelihood of cross-infection among these cases remains challenging and would require additional clinical data for a comprehensive analysis.
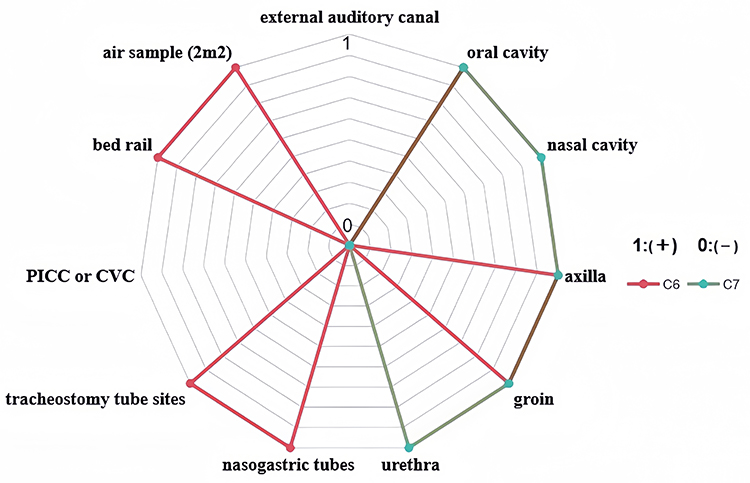 |
Figure 5 Results of comprehensive fungal cultures for C. auris conducted in April 2024 on patients C6 and C7. In April 2024, comprehensive fungal cultures of C. auris were conducted on two patients (C6 and C7), covering the entire integumentary system, various catheter surfaces, and the patients’ immediate living environments. Positive results for C. auirs were found in both patients. 1 indicates fungal cultures (+), 0 indicates fungal cultures (-). The red line represents the results of various source samples for C6, and the green line represents the results of various source samples for C7. |
These outcomes underscore the critical need for swift and effective therapeutic interventions for managing C. auris infections, especially in critically ill patients. Conversely, regarding the necessity of treatment for colonization, prior reports have indicated that C. auris colonization may not warrant treatment,31,32 and we contend that timely intervention is essential. We believe that the tailored use of topical agents is based on the propensity of C. auris for skin colonization when its colonization status is determined, as opposed to the use of systemic medications during the infection stage. Specific topical drugs and their efficacy need to be further explored and verified experimentally. The in vitro efficacy of chlorhexidine-containing preparations for skin colonization has been confirmed in several studies.33 However, despite repeated disinfection and washing with chlorhexidine, some patients still exhibit persistent pathogens. In vitro studies have demonstrated the activity of nitroquinoline against C. auris, suggesting its potential use for urinary tract purification; however, clinical data supporting this claim are currently lacking.34 Simultaneously, meticulous adherence to sterile protocols during invasive procedures such as catheterization is imperative. With respect to systemic medication, two new antifungals in development, ibrexafungerp and manogepix, have shown good in vitro activity against multidrug-resistant isolates of C. auris and Candida spp.35,36 However, prior to the implementation of these novel drugs in clinical practice, many clinical trials must be conducted, and a substantial amount of time is needed.
Finally, it is important to acknowledge the limitations of our study. The small sample size of only seven C. auris isolates restricts the generalizability of our findings. But, we have supplemented the data of clinical isolates of C. auris from Guangdong Province, especially including two amphotericin B-resistant isolates. At the same time, we have also supplemented the information on the colonization environment of C. auris. This can provide more references for clinical treatment in this region.
Conclusion
Overall, in this study, we present a case series of five patients with C. auris infections/colonization concentrated in a single medical institution from May to September 2023, along with two patients colonized with C. auris in April 2024. By investigating these patients and the C. auris strains isolated from them, we identified certain similar epidemiological and clinical characteristics and resistance characteristics of C. auris infection/colonization, suggesting strategies for clinical prevention and control. This study underscores the importance of SNP analysis in understanding genetic diversity and adaptation. The unique and consistent mutations observed in Clades I and III provide a foundation for further research into their functional implications and evolutionary significance. These findings increase our understanding of the genetic mechanisms driving the diversity of the ERG11 gene across different clades. Moreover, this study highlights the challenges in preventing, diagnosing, and treating C. auris infections/colonization, particularly in elderly patients with severe comorbidities, in which comprehensive colonization screening should be regularly performed on eligible patients once a week or twice a week, encompassing the entire integumentary system, various types of indwelling catheter surfaces, and the patient’s immediate living environment. The emergence of multidrug resistance underscores the urgent need for effective surveillance, infection control measures, and the development of novel antifungal agents to combat this global public health threat.
Abbreviations
C. auris, Candida auris; SNPs, single-nucleotide polymorphism identification; AASs, amino acid sequence variations; ICU, intensive care unit; MALDI-TOF MS, matrix-assisted laser desorption ionization time of flight mass spectrometry; ITS, internal transcribed spacer; MIC, minimum inhibitory concentration; V125A, valine to alanine; F126L, phenylalanine to leucine; Y132F, tyrosine to phenylalanine; K143R, lysine to arginine; GM, galactomannan; GCS, Glasgow Coma Scale score; mRS, modified Rankin scale score; PICCs, peripherally inserted central catheters; CVCs, central venous catheter.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The participants provided written informed consent before participation. Ethical approval was provided by the Clinical Research Ethics Committee of Sun Yat-sen Memorial Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82172289).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Satoh K, Makimura K, Hasumi Y, et al. Candida auris sp. nov. a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53:41–44. doi:10.1111/j.1348-0421.2008.00083.x
2. Eyre David W, Sheppard Anna E, Hilary M, et al. A Candida auris outbreak and its control in an intensive care setting. N Engl J Med. 2018;379:1322–1331. doi:10.1056/NEJMoa1714373
3. Ruiz-Gaitán A, Moret AM, Tasias-Pitarch M, et al. An outbreak due to Candida auris with prolonged colonization and candidaemia in a tertiary care European hospital. Mycoses. 2018;61:498–505. doi:10.1111/myc.12781
4. Lockhart SR, Etienne KA, Vallabhaneni S, et al. Simultaneous emergence of multidrug-resistant candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. CLINID. 2017;64:134–140. doi:10.1093/cid/ciw691
5. Chowdhary A, Prakash A, Sharma C, et al. A multicentre study of antifungal susceptibility patterns among 350 Candida auris isolates (2009–17) in India: role of the ERG11 and FKS1 genes in azole and echinocandin resistance. J Antimicrob Chemother. 2018;73:891–899. doi:10.1093/jac/dkx480
6. Arendrup MC, Prakash A, Meletiadis J, et al. Comparison of EUCAST and CLSI reference microdilution MICs of eight antifungal compounds for candida auris and associated tentative epidemiological cut-off values. Antimicrob Agents Chemother. 2017;61:
7. Fisher MC, Garner TWJ. Chytrid fungi and global amphibian declines. Nat Rev Microbiol. 2020;18:332–343. doi:10.1038/s41579-020-0335-x
8. Schorling SR, Kortinga HC, Froschb M, et al. The role of Candida dubliniensis in oral candidiasis in human immunodeficiency virus-infected individuals. Crit Rev Microbiol. 2000;26:59–68. doi:10.1080/10408410091154183
9. Dellière S, Gits-Muselli M, Bretagne S, et al. Outbreak-Causing Fungi: pneumocystis jirovecii. Mycopathologia. 2020;185:783–800. doi:10.1007/s11046-019-00408-w
10. Sharma C, Kumar N, Pandey R, et al. Whole genome sequencing of emerging multidrug resistant Candida auris isolates in India demonstrates low genetic variation. New Microbes New Infections. 2016;13:77–82. doi:10.1016/j.nmni.2016.07.003
11. Centers for Disease Control and Prevention. Tracking Candida auris. Available from: http://www.cdc.gov/fungal/diseases/candidiasis/tracking-c-auris.html.
12. Rybak JM, Muñoz JF, Barker KS, et al. Mutations in TAC1B: a novel genetic determinant of clinical fluconazole resistance in Candida auris. mBio. 2020;11:
13. Mayr E-M, Ramírez-Zavala B, Krüger I, et al. A zinc cluster transcription factor contributes to the intrinsic fluconazole resistance of Candida auris. mSphere. 2020;5:
14. Rybak JM, Sharma C, Doorley LA, Barker KS, Palmer GE, Rogers PD. Delineation of the direct contribution of Candida auris ERG11 mutations to clinical triazole resistance. Microbiol Spectr. 2021;9(3):e0158521. doi:10.1128/Spectrum.01585-21
15. Schelenz S, Hagen F, Rhodes JL, et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control. 2016;5:1–7. doi:10.1186/s13756-016-0132-5
16. Chowdhary A, Anil Kumar V, Sharma C, et al. Multidrug-resistant endemic clonal strain of Candida auris in India. Eur J Clin Microbiol Infect Dis. 2014;33:919–926. doi:10.1007/s10096-013-2027-1
17. Chowdhary A, Sharma C, Duggal S, et al. New clonal strain of Candida auris, Delhi, India: new clonal strain of Candida auris, Delhi, India. Emerg Infect Dis. 2013;19:1670–1673. doi:10.3201/eid1910.130393
18. Bing J, Du H, Guo P, et al. Candida auris -associated hospitalizations and outbreaks, China, 2018–2023. Emerging Microbes Infect. 2024;13:2302843. doi:10.1080/22221751.2024.2302843
19. Lockhart SR, Chowdhary A, Gold JAW. The rapid emergence of antifungal-resistant human-pathogenic fungi. Nat Rev Microbiol. 2023;21:818–832. doi:10.1038/s41579-023-00960-9
20. Scudeller L, Bassetti M, Concia E, et al. MEDical wards invasive Candidiasis ALgorithms (MEDICAL): Consensus proposal for management. Eur J Internal Med. 2016;34:45–53. doi:10.1016/j.ejim.2016.07.007
21. Bassetti M, Giacobbe DR, Agvald-Ohman C, et al. Invasive fungal diseases in adult patients in intensive care unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM. Intensive Care Med. 2024;50:502–515. doi:10.1007/s00134-024-07341-7
22. Li J, Coste AT, Liechti M, et al. Novel ERG11 and TAC1b mutations associated with azole resistance in Candida auris. Antimicrob Agents Chemother. 2021;65:e02663–20. doi:10.1128/AAC.02663-20
23. Erturk Sengel B, Ekren BY, Sayin E, et al. Identification of molecular and genetic resistance mechanisms in a candida auris isolate in a tertiary care center in Türkiye. Mycopathologia. 2023;188(6):929–936. doi:10.1007/s11046-023-00787-1
24. Rudramurthy SM, Chakrabarti A, Paul RA, et al. Candida auris candidaemia in Indian ICUs: analysis of risk factors. J Antimicrob Chemother. 2017;72:1794–1801. doi:10.1093/jac/dkx034
25. Aldejohann AM, Wiese-Posselt M, Gastmeier P, et al. Expert recommendations for prevention and management of Candida auris transmission. Mycoses. 2022;65:590–598. doi:10.1111/myc.13445
26. De Jong AW, Dieleman C, Carbia M, et al. Performance of two novel chromogenic media for the identification of multidrug-resistant candida auris compared with other commercially available formulations. J Clin Microbiol. Hanson KE, editor. 2021;59(4):e03220. doi:10.1128/JCM.03220-20.
27. Das S, Singh S, Tawde Y, et al. A selective medium for isolation and detection of Candida auris, an emerging pathogen. J Clin Microbiol. 2021; 59:e00326–20
28. Borman AM, Fraser M, Johnson EM. CHROMagarTM Candida Plus: a novel chromogenic agar that permits the rapid identification of Candida auris. Med Mycol. 2021;59:253–258. doi:10.1093/mmy/myaa049
29. Mulet Bayona JV, Salvador García C, Tormo Palop N, et al. Evaluation of a novel chromogenic medium for Candida spp. identification and comparison with CHROMagarTM Candida for the detection of Candida auris in surveillance samples. Diagn Microbiol Infect Dis. 2020;98:115168. doi:10.1016/j.diagmicrobio.2020.115168
30. Adams E, Quinn M, Tsay S, et al. Candida auris in healthcare facilities, New York, USA, 2013–2017. Emerging Infecti Dis. 2018;24:1816. doi:10.3201/eid2410.180649
31. Kean R, McKloud E, Townsend EM, et al. The comparative efficacy of antiseptics against Candida auris biofilms. Int J Antimicrob Agents. 2018;52:673–677. doi:10.1016/j.ijantimicag.2018.05.007
32. Moore G, Schelenz S, Borman AM, et al. Yeasticidal activity of chemical disinfectants and antiseptics against Candida auris. J Hosp Infect. 2017;97(4):371–375. doi:10.1016/j.jhin.2017.08.019
33. Ku TSN, Walraven CJ, Lee SA. Candida auris: disinfectants and implications for infection control. Front Microbiol. 2018;9:726. doi:10.3389/fmicb.2018.00726
34. Fuchs F, Hof H, Hofmann S, et al. Antifungal activity of nitroxoline against Candida auris isolates. Clin Microbiol Infect. 2021;27:
35. Berkow EL, Lockhart SR. Activity of novel antifungal compound APX001A against a large collection of Candida auris. J Antimicrob Chemother. 2018;73:3060–3062. doi:10.1093/jac/dky302
36. Berkow EL, Angulo D, Lockhart SR. In vitro activity of a novel glucan synthase inhibitor, SCY-078, against clinical isolates of Candida auris. Antimicrob Agents Chemother. 2017;61:e00435–17. doi:10.1128/AAC.00435-17
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Candidemia Case Caused by a Novel Drug-Resistant Candida auris with the Y132F Mutation in Erg11 in Mainland China
Xu Z, Zhang L, Han R, Ding C, Shou H, Duan X, Zhang S
Infection and Drug Resistance 2023, 16:3065-3072
Published Date: 18 May 2023