")
Back to Journals » Infection and Drug Resistance » Volume 18
Epidemiological Trends and Drug Resistance Patterns of Carbapenem-Resistant Gram-Negative Bacteria: A Retrospective Study in a Tertiary Hospital in China (2019-2024)
Authors Hou B, Niu X, Yu Q, Wang W
Received 4 March 2025
Accepted for publication 28 May 2025
Published 5 June 2025 Volume 2025:18 Pages 2867—2880
DOI https://doi.org/10.2147/IDR.S518461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Bailong Hou, Xiaoqin Niu, Qinlong Yu, Wei Wang
Department of Clinical Laboratory, The First Hospital of Jiaxing, The Affiliated Hospital of Jiaxing University, Jiaxing, 314000, People’s Republic of China
Correspondence: Wei Wang, Department of Clinical Laboratory, The First Hospital of Jiaxing, The Affiliated Hospital of Jiaxing University, Jiaxing, 314000, People’s Republic of China, Email [email protected]
Objective: To elucidate the distribution characteristics and drug resistance of carbapenem-resistant gram-negative bacteria (CR-GNB) within a general hospital setting from 2019 to 2024.
Methods: The distribution characteristics of CR-GNB and antimicrobial resistance patterns among inpatients from 2019 to 2024 were investigated. The detection rate, departmental distribution, annual trends, and drug susceptibility profiles of key carbapenem-resistant bacterial species were compared.
Results: A total of 34, 370 patients infected with GNB were investigated, with 2967 cases identified as CR-GNB. Among these, the nosocomial infection rate of carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), and carbapenem-resistant Pseudomonas aeruginosa (CRPA) were 33.11%, 44.02%, and 22.87%, respectively. The positivity rate for CR-GNB among male patients was 72.94%, with the vast majority of these infected patients (71.88%) aged 65 and above. In 2021, notable shifts in hospital infection control concerning CR-GNB were observed, with a reduction of over 40% in CRAB infection rates and a decline of over 35% in CRPA infection rates. The top three clinical departments with CR-GNB detection were the intensive care unit (ICU), intensive rehabilitation ward (HDU), and emergency ward. CR-GNB accounted for the largest proportion of respiratory infections (73.49%). Clinically isolated CR-GNB exhibited pan-resistance to commonly used clinical antimicrobial drugs, with only cefoperazone/sulbactam, amikacin, and tigecycline demonstrating high sensitivity. Analysis of carbapenemase production revealed a significant prevalence of Ambler class A enzymes.
Conclusion: The detection of CR-GNB in this hospital from 2019 to 2024 indicates a widespread distribution across clinical departments and infection sites, coupled with a high rate of resistance to commonly used antimicrobials. Local hospitals should prioritize the distribution patterns of CR-GNB to develop personalized prevention strategies, strengthen hospital public health and infection prevention and control measures, and promote rational use of antibiotics to effectively curb the spread of CR-GNB infections.
Keywords: carbapenem-resistant gram-negative bacteria, epidemiology, drug resistance
Introduction
The escalating global prevalence of carbapenem-resistant Gram-negative bacteria (CR-GNB), attributed to the widespread use of carbapenem antibiotics, has resulted in a critical public health concern. The World Health Organization ranks CR-GNB as a primary risk among antibiotic-resistant bacteria.1 CR-GNB mainly includes carbapenem-resistant Enterobacteriaceae bacteria (CRE), carbapenem-resistant Acinetobacter baumannii (CRAB), and carbapenem-resistant Pseudomonas aeruginosa (CRPA). The extensive spread of CR-GNBs has become a major public health challenge worldwide. In China, the detection rate of CR-GNBs has generally exhibited an upward trend, with exceptionally high rates in northeast China, South China and North China. Infections caused by these organisms have been shown to significantly increase hospital mortality, hospitalization duration and healthcare costs. Data from the China Bacterial Resistance Monitoring Network (CHINET) from 2005 to 2024 indicated a consistent increase in resistance rates of imipenem and meropenem in Klebsiella pneumoniae from 3.0% and 2.9% in 2005 to 25.0% and 26.3% in 2018, respectively. Next, a continuous downward trend was observed, with a subsequent recovery to 15.3% and 15.4% in 2024 (https://www.chinets.com). Similarly, resistance rates to imipenem and meropenem in Acinetobacter baumannii steadily rose from 32.9% and 41.3% in 2005 to 77.7% and 79% in 2019, followed by a continuous decline starting in 2020 and a subsequent increase to 61.0% and 62.0% in 2024. In Pseudomonas aeruginosa, resistance rates to imipenem and meropenem fluctuated between 36.8% and 35.3% in 2005, ultimately reaching 26.0% and 14.4% by 2024.2,3
The economic cost burden of bacterial resistance is substantial, extending beyond death and disability. Prolonged illness leads to prolonged hospital stay and use of more, more expensive drugs, thereby increasing the economic burden on patients.4 Due to the high pathogenicity, pan-drug resistance,5 and propensity for nosocomial transmission,6 CR-GNB pose significant pressure and challenges to hospital infection prevention and control.7 Moreover, there have been limited reports on the latest five years of international drug resistance monitoring data.
It is now understood that CR-GNB arises through multifactorial mechanisms, which can be categorized into three primary pathways: (i) enzymatic inactivation mediated by diverse carbapenemases (eg, KPC and NDM variants), often facilitated by the co-occurrence of multiple β-lactamase genes; (ii) hyperexpression of efflux pumps enabling broad-spectrum antibiotic extrusion; and (iii) structural alterations in outer membrane porins that restrict drug permeation.8 The convergence of these mechanisms frequently drives pan-drug resistance phenotypes. While KPC carbapenemases remain the predominant resistance mediators, New Delhi metallo-β-lactamase (NDM) variants demonstrate significant prevalence, particularly concerning their capacity to confer resistance to ceftazidime-avibactam. Notably, emerging evidence reveals that certain KPC-producing strains have developed reduced susceptibility to ceftazidime-avibactam through novel resistance pathways (eg, structural mutations in KPC enzymes or porin modifications), thereby exacerbating therapeutic challenges in managing CR-GNB infections.
Therefore, this study sought to investigate the distribution and antibiotic susceptibility characteristics of CR-GNB in a general hospital in northern Zhejiang from 2019 to 2024. Based on these data, we sought to provide a reference protocol for prevention, treatment, rational use of antibiotics, and guidance of empirical medication.
Materials and Methods
The interviewees were hospitalized patients with Gram-negative bacterial infections between 2019 and 2024. The study protocol was reviewed and approved by the Ethics Committee of the hospital (No.2024-LY-823). Gram-negative bacteria that met any of the following conditions were defined as CR-GNB: (1) Resistance to one or more carbapenems (imipenem, meropenem, ertapenem or doripenem); for bacterial species with intrinsic reduced susceptibility to imipenem (Morganella, Proteobacteria, Provydon, etc.), resistance was determined based on susceptibility results to other carbapenem agents; (2) Production of carbapenemases.9
Sample Collection
Epidemiological data on GNB nosocomial infections were collected by nosocomial infection management professionals. Relevant data were investigated and recorded by reviewing electronic health records, clinical laboratory information systems, and real-time nosocomial infection surveillance systems. The collected data included name, gender, age, department, hospitalization number, site of hospital infection, specimens submitted for examination, and drug sensitivity results. Data discrepancies were resolved by referring to the original investigation records.
Pathogen Identification and Drug Sensitivity Test
The infection types of interest included GNB strains associated with nosocomial infections. Cases of contamination, community-acquired infection, colonization, and repeatedly detected strains were excluded. Only the first isolate per patient was included in the analysis; colonizing and repeat isolates from the same specimen were excluded.
Pathogen identification and drug susceptibility tests were conducted by the VITEK mass spectrometer (BioMérieux), the VITEK 2 Compact automatic microbial identification and drug susceptibility analyzer (BioMérieux), and the BD PhoenixTM M50 automatic microbial susceptibility analyzer (BD). Antimicrobial susceptibility was further assessed using the Kirby-Bauer (K-B) method and E-test strips as supplementary methods. All operations adhered strictly to the National Clinical Inspection Operation Procedures (4th edition). The drug susceptibility test results were interpreted according to the American Association for Standardization of Clinical Laboratory (Clinical and Laboratory Standards Institute, CLSI) standard M100 interpretation.10,11 Quality control was maintained using Escherichia coli (ATCC 25922) and Pseudomonas aeruginosa (ATCC 27853) strains.
Carbapenemase detection in Gram-negative bacteria utilizes complementary phenotypic and genotypic approaches. The phenotypic inhibitor-based assay distinguishes serine carbapenemases (KPC, OXA-48) from metallo-β-lactamases (NDM, VIM) by comparing carbapenem disk inhibition zones with/without 3-aminophenylboronic acid (APB) or EDTA, adhering to CLSI interpretive criteria (a ≥5 mm increase in zone diameter indicates the likely enzyme class). Enzyme-linked immunochromatographic assays enable rapid (<15 min) detection of specific carbapenemase genotypes (KPC, NDM, IMP, etc). via monoclonal antibodies, achieving >95% accuracy versus PCR.
Quality Control in Microbiological Testing
Comprehensive quality control protocols were rigorously implemented throughout the microbiological workflow to ensure result reliability. Pre-analytical quality assurance measures included specimen integrity verification and media validation using ATCC reference strains. Analytical standardization encompassed daily calibration of automated identification systems (VITEK®2/MS) with E. coli ATCC 25922, while antimicrobial susceptibility testing adhered to CLSI M100 guidelines and routine disk diffusion QC with E. coli ATCC 25922 and P. aeruginosa (ATCC 27853). Post-analytical quality assurance measures featured algorithmic validation of discordant results and 5-year retention of raw instrument data per ISO 15189. Through these multilayered controls, laboratory performance metrics achieved <1.5% identification errors and >97% categorical agreement in susceptibility results compared to reference broth microdilution.
Statistical Analysis
Antimicrobial susceptibility testing results were analyzed using WHONET 5.6 software (http://www.whonet.org/software.html). Data were summarized using Microsoft Excel software, and statistical analysis was performed using IBM SPSS Statistics 22.0 (IBM Corp., Chicago, Illinois, USA). Clinical data had been downloaded from the Haiti Electronic Medical Record System, from which potential risk factor data were subsequently identified and compiled. Categorical data were expressed as the number of cases and proportions, and χ²-tests were used for comparisons, with p<0.05 considered statistically significant.
Results
Distribution of CR-GNB and Patient Characteristics in Hospital Infections
This study analyzed a total of 34370 GNB strains between January 2019 and December 2024, comprising 20863 isolates from males and 13507 isolates from females. CR-GNB was detected in 2987 of the GNB isolates. The positivity rate of CR-GNB in male patients was 72.94%. Most culture-positive samples (49.54%) in the GNB isolates were from patients over the age of 65 years, but 71.88% in CR-GNB isolates. Analysis of specimen source data indicated that respiratory specimens constituted the largest proportion (50%) in GNB and CR-GNB, followed by sterile body fluid specimens, urine specimens, and blood specimens (Table 1).
 |
Table 1 Demographic and Clinical Profile of Patients with Infections Caused by Gram-Negative Bacteria (GNB) and Carbapenem-Resistant Gram-Negative Bacteria (CR-GNB) |
Hospital-Acquired Infection of CR-GNB
A total of 34370 patients infected with GNB were investigated, including 2987 cases infected in CR-GNB, and the hospital infection rate of CR-GNB was 8.70%. Among the hospital-infected patients in CR-GNB, the prevalence of carbapenem-resistant Enterobacteriaceae was 33.08%, carbapenem-resistant Acinetobacter baumannii was 44.06%, and carbapenem-resistant Pseudomonas aeruginosa was 22.87%. Detailed statistical values are presented in Supplement Table 1, while Figure 1 highlights the species composition of the CR-GNB distribution. From 2019 to 2024, the number of CR-GNB infections was 508 (11.75%), 442 (10.13%), 328 (6.36%), 363 (6.91%), 507 (8.43%), and 839 (9.06%), with the lowest hospital infection rate in 2021. Supplement Table 2 contrasts detailed statistical values, enabling comparative analysis across various groups, and Figure 2 depicts the temporal trends in the CR-GNB detection rate.
 |
Figure 1 Species composition of CR-GNB in clinical isolates from 2019 to 2024. |
 |
Figure 2 Changes in the CR-GNB detection rate from 2019 to 2024. |
Quarterly Trends in Nosocomial CR-GNB Infection Rates
No significant variation was observed in the detection rates of CRE and CRPA nosocomial infections (p > 0.05). However, a significant seasonal disparity was noted for CRAB (p < 0.05), with the highest incidence occurring in the first quarter (69.73%), followed by the fourth quarter (42.30%). Supplement Table 3 provides comprehensive statistical data, and Figure 3 illustrates the seasonal fluctuations in CR-GNB detection rates.
 |
Figure 3 Changes in the CR-GNB detection rate across different quarters from 2019 to 2024. Abbreviations: Q1, first quarter; Q2, second quarter; Q3, third quarter; Q4, fourth quarter. |
Nosocomial CR-GNB Infection Rates Across Hospital Departments
The incidence of CR-GNB infections in critical care departments was higher than in general wards. Between 2019 and 2024, the CR-GNB detection rate was the highest in ICUs, followed by the intensive care rehabilitation department, the emergency ward, neurosurgery, hepatobiliary and pancreatic surgery, and respiratory medicine. During this period, temporal trends in CRAB detection exhibited distinct patterns: a decline followed by an increase in ICUs, an initial rise followed by a decrease in the emergency ward, and fluctuating trends in hepatobiliary-pancreatic surgery for CRE. The difference in detection rates of resistant bacteria in these three departments was statistically significant (p <0.05) (Table 2).
 |
Table 2 Detection of Resistant Bacteria in the Top Five Hospital CR-GNB Departments From 2019 to 2024 |
Distribution of Nosocomial Infection Sites in CR-GNB
Among the CR-GNB infections, respiratory system infections accounted for the largest proportion (74.05%), followed by sterile body fluid (7.30%), urinary system (7.26%), and blood system (5.72%). Among the specimens infected with CRAB and CRPA, respiratory specimens accounted for 86.32% and 83.02%, respectively, representing a notably high proportion and highlighting their significance as major pathogens causing hospital-acquired infections. Among the specimens infected with CRE, the sources of specimens were relatively diverse, with respiratory specimens accounting for 51.52%, while sterile body fluid, urine, and blood specimens accounted for 12.96%, 18.83%, and 12.55%, respectively (Table 3).
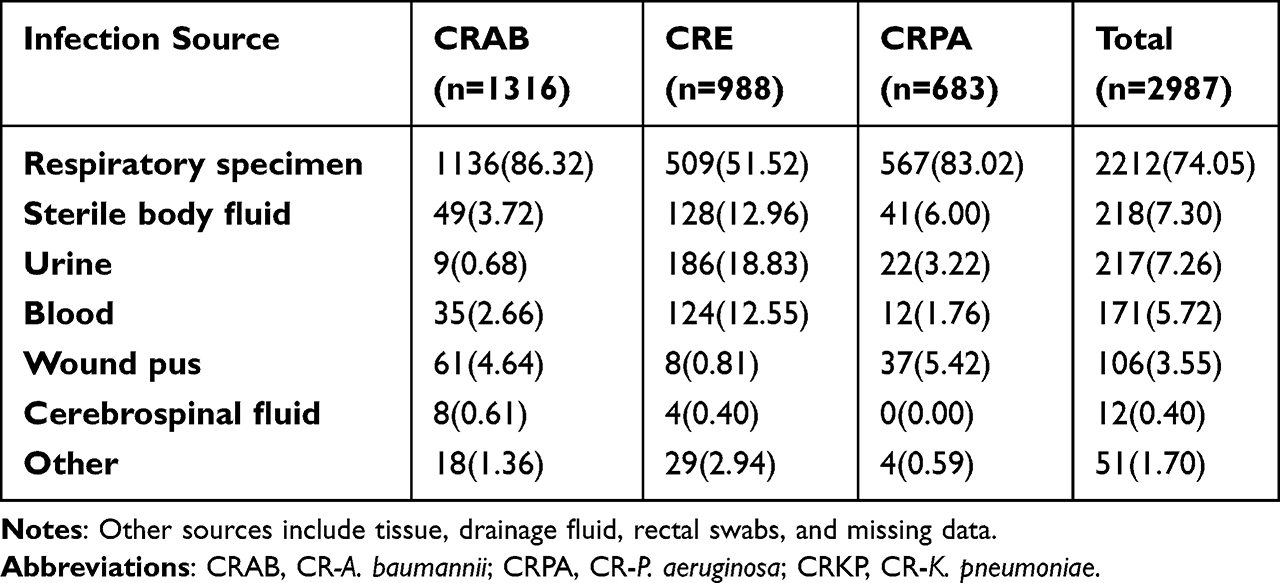 |
Table 3 The Distribution of CR-GNB Detected in Different Infection Sites From 2019 to 2024 [Strain (%)] |
Stratification according to specimen sources revealed that CRAB was the predominant strain in respiratory tract, pus, and cerebrospinal fluid specimens, accounting for 51.35%, 57.55%, and 66.67%, respectively. CRE was predominant in sterile body fluids, urine, and blood samples, accounting for 58.72%, 85.71%, and 72.51%, respectively (Figure 4).
 |
Figure 4 Distribution of CR-GNB detected across different infection sites from 2019 to 2024. |
Distribution of the Strains Detected in CR-GNB
From 2019 to 2024, the predominant CR-GNB strains were Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, E. coli, Enterobacter cloacae, Proteus mirabilis, Klebsiella aerogenes, Serratia marcescens, Citrobacter freundii and Morganella. From 2019 to 2024, the total CR-GNB detection rate was high, with the CRAB detection rate reaching 66.10% in 2024 (Table 4).
 |
Table 4 CR-GNB with the Top 10 Strains Detected From 2019 to 2024 [Strain (%)] |
Analysis of Drug Resistance in CR-GNB Hospital Infection
Among the CR-GNB clinical isolates from 2019 to 2024, CRAB exhibited the highest overall resistance. With the exception of cefoperazone/sulbactam (1.62%), amikacin (35.63%), minocycline (3.13%), and tigecycline (9.55%), the resistance rates to commonly used clinical antibiotics exceeded 50%. CRE demonstrated a broad drug resistance spectrum; resistance rates to cefoperazone/sulbactam, amikacin, and tigecycline were 1.60%, 31.53%, and 6.00%, respectively, while resistance to other commonly used clinical antibiotics also surpassed 50%. In contrast, CRPA showed notable susceptibility to cefoperazone/sulbactam and aminoglycosides, with resistance rates for most other antimicrobial drugs exceeding 40% (Table 5).
 |
Table 5 Drug Resistance of CR-GNB Strains Clinically Isolated in a Hospital From 2019 to 2024 [Strain (%)] |
Distribution of CRE Among the Total Isolates in Hospital Infections
Among 928 carbapenem-resistant isolates, carbapenem-resistant genes were detected in 600 (64.55%) isolates encoding Ambler class A, 302 (32.54%) encoding Ambler class B, and 26 (2.8%) encoding Ambler class D. Supplement Table 4 documents the statistical values (p <0.05), while Figure 5 illustrates the distribution trends of bacterial/specimen/department according to carbapenemase type.
 |
Figure 5 Distribution of carbapenemase types among 928 CRE strains isolated from 2019–2024 in a hospital. Abbreviations: CR, carbapenem-resistant; ICU, Intensive care unit; Class A, serine enzymes; Class B, metallo-ß-lactamases; Class D, oxacillinase-48. Notes: (A), Bacterial distribution of carbapenemase types among 928 CRE strains isolated; (B), Specimen-type distribution of carbapenemase types among 928 CRE strains isolated; (C), Department-wise distribution of carbapenemase types among 928 CRE strains isolated. |
Figure 5A illustrates the distribution of carbapenemase among various CRE isolates. Serine carbapenemases were the most frequently detected, with Klebsiella pneumoniae accounting for 541 isolates (90.10%) and Klebsiella aerogenes contributing 21 isolates (3.5%), followed by Serratia marcescens and Escherichia coli. Metallo-ß-lactamases were predominantly observed in Escherichia coli, with 125 isolates (41.3%) and Enterobacter cloacae with 68 isolates (22.5%), while Klebsiella pneumoniae had 55 isolates (18.2%). Oxacillinase-48 was equally distributed between Klebsiella pneumoniae and Klebsiella aerogenes, each contributing 23 isolates (88.40%).
Figure 5B illustrates the distribution of carbapenemase types across specimen types. Serine carbapenemases were the most frequently detected, with respiratory specimens accounting for 377 isolates (62.8%) and whole blood contributing 116 isolates (19.3%). The metallo-ß-lactamase was predominantly observed in respiratory specimens with 94 isolates (31.1%) and urine with 75 isolates (24.8%). The oxacillinase-48 was distributed across respiratory specimens (53.8%) and whole blood (23%).
Figure 5C illustrates the distribution of carbapenemases across departments. The intensive care unit (ICU) was the department with the highest number of isolates harboring Ambler class A carbapenemases (n=236, 29.3%) and Ambler class B carbapenemases (n=64, 21.1%). The neurosurgery department had the highest proportion of Ambler class D carbapenemase-producing isolates, accounting for 6 isolates (23%).
Discussion
The emergence of nosocomial infections caused by multidrug-resistant Gram-negative bacteria poses a significant challenge to global health systems. In this respect, infections caused by organisms such as Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa are of particular concern due to their association with increased morbidity, mortality, and healthcare costs. In 2019, the US Antimicrobial Resistance Threat Report first listed antimicrobial resistance (Antimicrobial resistance, AMR) as one of the top 10 threats to global health, CRAB and CRE as emergency threats, and multiple resistant Multiple-drug resistant Pseudomonas aeruginosa (MDR-PA) as a serious threat.4,12 In 2024, the World Health Organization (WHO) Bacterial Priority Pathogens List (BPPL) categorizes 15 families of antibiotic-resistant (ABR) pathogens based on their public health impact. Notably, CRAB and CRE were classified as critical-priority pathogens due to three key factors: their demonstrated capacity for horizontal gene transfer of resistance determinants, the life-threatening nature of associated infections, and their substantial global disease burden. In the same classification framework, CRPA was designated as a high-priority pathogen in the 2024 BPPL evaluation.13 These pathogens have exhibited alarming trends in antibiotic resistance, especially to carbapenems, which are often considered the last line of defense against severe bacterial infections. The rise in resistance not only complicates treatment regimens but also necessitates the urgent implementation of effective infection control measures and antibiotic stewardship programs to mitigate the economic burden on healthcare systems and improve patient outcomes.14,15
This study aimed to elucidate the epidemiological and phenotypic characteristics of CR-GNB infections in hospitalized patients from 2019 to 2024. Through a retrospective observational study design, we analyzed demographic data, treatment protocols, and clinical outcomes associated with CR-GNB infections. We analyzed data from 34,370 patients, identifying 2987 cases (8.70%) of CR-GNB. Our findings highlighted a patient demographic predominantly over 65 years, with a higher prevalence in ICUs. Resistance testing revealed alarming rates, with 85% of isolates resistant to multiple drug classes, underscoring the urgent need for novel treatment strategies. Notably, we observed a seasonal variation in CRAB infections, peaking in the first quarter, and a predominance of respiratory infections among CR-GNB cases. The elevated CRAB detection rates observed in this study may be associated with seasonal antibiotic prescribing patterns, enhanced bacterial transmission under low-temperature conditions, and periodic lapses in infection control compliance during holiday periods. Similar seasonal trends have been documented in epidemiological studies of carbapenem-resistant Enterobacterales.16 Our analysis of carbapenemase production revealed a significant prevalence of Ambler class A enzymes.17,18
Notably, our findings indicated an increasing prevalence of CR-GNB infections over the study period, with Acinetobacter baumannii and Klebsiella pneumoniae being the predominant pathogens. Compared to previous studies, which highlighted the rising incidence of multidrug-resistant organisms, our research provides the first comprehensive analysis of CR-GNB in hospitalized patients within this timeframe. In our study, we observed decline in antimicrobial resistance rates during 2021 (CR-GNB incidence decreased by 45% compared to 2019) likely reflects multifaceted impacts of COVID-19 containment measures. Enhanced infection control protocols (universal masking, contact restrictions, and 75% alcohol-based disinfectant consumption doubling) reduced nosocomial transmission.19 Post-COVID-19 microbiological surveillance conducted by Professor Zhang’s team revealed notable shifts in nosocomial pathogen distribution: The isolation rate of Acinetobacter baumannii demonstrated a statistically significant decline (p=0.0059), whereas a marked elevation in detection frequencies was observed in Klebsiella pneumoniae (K. pneumoniae), Pseudomonas aeruginosa, Enterobacter cloacae, and Enterococcus faecalis, all showing statistically robust associations (p<0.05 for each species).20 Studies have suggested that stay-at-home orders may be associated with a reduction in the incidence of COVID-19 in some countries. Mask wearing decreases the risk of COVID-19 in the community, especially when the surgical masks are used for vulnerable people. N-95 respirators protect health workers from COVID-19 in Bestetti RB et al.21 The unique resistance mechanisms identified, particularly the emergence of new carbapenemases, underscore the urgent need for ongoing surveillance and innovative therapeutic strategies, as well as the importance of developing new antimicrobial agents to combat this alarming trend.12,14
In this study, the incidence of CR-GNB hospital infection rate was higher in ICU wards was higher than in general wards, consistent with studies conducted abroad.22,23 While some studies in China have found the internal medicine system as a high-incidence area for CR-GNB,24 other studies25 suggest variations may arise due to differences in the patient populations and the types of diseases treated within the hospital, consistent with the present study. Indeed, the ICU and HDU primarily treat patients following craniocerebral trauma and tumor surgery, with long hospitalization times, extensive intubations, and extended indwelling medical devices. These factors also contribute to these departments having the highest detection rates of drug-resistant bacteria. There are reports indicating that invasive CRAB infection rate was significantly higher among CRAB carriers (OR 11.14, 95% CI 4.95–25.05, with substantial heterogeneity stemming from size rather than direction of the effect). Negative predictive value of noncarriage for invasive infection was 97%. CRAB bloodstream infection rate was significantly higher among carriers (odds ratio 16.23, 95% confidence interval 2.9–110.08).26 Therefore, it is recommended to conduct routine CR-GNB active screening for these high-risk groups to effectively identify the source of colonization and infection, and take timely measures to control the source of infection. CR-GNB hospital infection prevention and control involves many departments. To ensure the successful implementation of preventive measures, a multi-departmental cooperation mechanism should be adopted, along with compliance monitoring of intervention measures, and regular analysis and feedback of monitoring outcomes. Given the variability in temporal scope, geographical distribution, hospital grade, age distribution, department distribution, and the different epidemiological characteristics of CR-GNB, continuous monitoring of local CR-GNB epidemiology is crucial to inform targeted prevention and control strategies.25
Rapid identification of people carrying or infected with CR-GNB and corresponding isolation are the main measures to prevent the spread of clonally transmitted strains. It is now understood that rational use of antimicrobial drugs to prevent the screening of drug-resistant strains under antimicrobial pressure is the primary prevention and control measure for drug-resistant plasmid-borne strains.27 Therefore, it is necessary to conduct further molecular epidemiological investigations of CR-GNB isolated in hospitals, clarify the causes of CR-GNB transmission in hospitals, and develop effective prevention and control measures to curb the nosocomial epidemic of CR-GNB.
Our study results showed that among the clinically isolated CR-GNB strains, the resistance rate to commonly used clinical antimicrobial drugs reached more than 50%, consistent with the research results of Ayobami.27 The resistance mechanism of CR-GNBs is complex and mainly involves the production of carbapenemases. CR-GNB in China exhibits a high resistance rate to most drugs, and the available drugs are extremely limited. Relevant treatment guidelines have been updated and published both domestic and abroad (IDSA, ESCMID and China) to provide new guidelines for the treatment of CR-GNB infections. In recent years, ceftazidime/avibactam, a new antimicrobial drug for CR-GNB, has been widely used; however, resistance to this agent is also emerging. Therefore, the characteristics of CR-GNB resistance can be clarified through further investigation of drug resistance genes.
In the present study, carbapenemases were found in 928 CRE strains, mainly class A serine proteases, accounting for 64.66%, followed by class B metalloenzymes (32.54%), and class D OXA-48. Our analysis of carbapenemase production revealed a significant prevalence of Ambler class A enzymes This distribution aligned with the results from studies in China and abroad.28–30 90% of the resistance phenotypes of CRE strains in China result from the acquisition of blaKPC-2 and blaNDM resistance genes.28 Genomic surveillance conducted by Professor Hu’s group has identified clonal dissemination as the predominant transmission mechanism of New Delhi metallo-β-lactamase-producing carbapenem-resistant Enterobacteriaceae (NDM-CRE) in pediatric healthcare institutions. Notably, the IncX3 plasmid harboring blaNDM demonstrates concerning zoonotic-anthroposophic prevalence, with genomic carriage rates reaching 57.7% in Escherichia coli (95% CI: 52.4–63.1%) and 91.3% in Klebsiella pneumoniae (95% CI: 87.6–94.8%) isolates across animal reservoirs and human clinical specimens.31 Therefore, elucidating CR-GNB resistance mechanisms necessitates systematic genomic interrogation of resistance determinants.
In addition, the elderly are gradually becoming carriers of multi-resistant bacteria, leading to their spread. The limited availability of effective drugs for treating these infections underscores the critical importance of drug accessibility in clinical practice. First of all, since drug-resistant bacteria are induced or screened out, clinicians should distinguish between colonizing bacteria and pathogenic bacteria when using antibiotics, advocate for cautious antibiotic use, and pay attention to the standardization of the use of antibiotics to minimize the risk of subsequent new infections in patients. In addition, improving patients’ immunity is very important, especially for CRAB and CRPA bacteria, which are “difficult to clear”. In addition to focusing on the use of antibiotics, clinicians should consider human factors more when treating infections, and the regulation of the host’s response represents a new direction in the post-antibiotic era.
The clinical implications of our findings are profound, particularly in shaping treatment protocols and healthcare policies. This research emphasizes the importance of antibiotic stewardship programs, which can significantly influence treatment outcomes and reduce mortality rates associated with resistant infections. Furthermore, the identification of high-risk patient demographics, particularly among the elderly and those in intensive care units, suggests a need for targeted intervention strategies to prevent nosocomial infections. These findings not only inform clinical practice but also provide a basis for healthcare policies aimed at mitigating the impact of antibiotic resistance on patient care and hospital resources.29
Nevertheless, this study has several limitations that must be acknowledged. The retrospective design may introduce biases, particularly as data collection relied on electronic health records, potentially resulting in incomplete or inaccurate data. Besides, the relatively small sample size, despite being drawn from a large cohort of patients, might limit the generalizability of the findings. Future research should consider a more extensive multicenter approach to validate these results and further explore the genetic underpinnings of resistance mechanisms in CR-GNB. Enhanced data collection methodologies and more extended follow-up periods could also provide greater insights into the long-term outcomes and effectiveness of interventions implemented based on the findings of this study.30 In addition, the limitations of this study include a lack of experimental validation, which limits the ability to establish causal relationships between observed resistance patterns and clinical outcomes. While focusing on resistance monitoring and patient epidemiology, risk factor analysis of clinical outcomes was excluded due to prohibitive data collection demands. These factors underscore the need for further research employing larger, multicenter studies with robust methodological designs to comprehensively evaluate the complexities of CR-GNB infections and their resistance mechanisms.
Conclusion
This study underscores the pressing challenge posed by carbapenem-resistant Gram-negative bacteria in nosocomial infections, highlighting significant resistance patterns and their clinical ramifications. Our findings emphasize the necessity for ongoing surveillance and the development of effective treatment protocols tailored to the resistance profiles of these pathogens. By identifying high-risk populations and understanding the epidemiological trends, healthcare providers can enhance patient outcomes and optimize resource allocation, ultimately contributing to more effective management strategies against CR-GNB infections. Future research should focus on innovative therapeutic approaches and exploring novel antimicrobial agents to address this escalating public health concern.
Ethics Approval
This study has been approved by the ethics committee at Jiaxing’s First Hospital (Approval Number: 2024-LY-823). Prior to the commencement of the study, all participants were fully informed of the purpose, procedures, potential risks, and benefits of the study and signed an informed consent form. Participants had the right to withdraw from the study at any time without any adverse consequences. The research adhered fully to the principles outlined in the Declaration of Helsinki.
Acknowledgments
We are grateful to anonymous reviewers whose remarks and proposals contributed to the enhancement of this manuscript.
Funding
This study was funded by the Medical and Health Science and Technology of Zhejiang Province of China under Grant 2023KY330 and Clinical Laboratory Medical Diagnostics Fund of the First Hospital of Jiaxing of Zhejiang Province of China under Grant 2023-ZC-002.
Disclosure
The authors assert that the study was conducted without any business or financial affiliations that could be construed as a potential conflict of interests.
References
1. Akram F, Imtiaz M, Haq IU. Emergent crisis of antibiotic resistance: a silent pandemic threat to 21st century. Microb Pathog. 2023;174:105923. PMID: 36526035. doi:10.1016/j.micpath.2022.105923
2. Hernando-Amado S, Laborda P, Martínez JL. Tackling antibiotic resistance by inducing transient and robust collateral sensitivity. Nat Commun. 2023;14(1):1723. PMID: 36997518; PMCID: PMC10063638. doi:10.1038/s41467-023-37357-4
3. Murray CJL, Ikuta KS, Sharara F; Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. PMID: 35065702; PMCID: PMC8841637. doi:10.1016/S0140-6736(21)02724-0
4. Castanheira M, Simner PJ, Bradford PA. Extended-spectrum β-lactamases: an update on their characteristics, epidemiology and detection. JAC Antimicrob Resist. 2021;3(3):dlab092. PMID: 34286272; PMCID: PMC8284625. doi:10.1093/jacamr/dlab092
5. Righi E, Mutters NT, Guirao X, et al. European society of clinical microbiology and infectious diseases/European committee on infection control clinical guidelines on pre-operative decolonization and targeted prophylaxis in patients colonized by multidrug-resistant Gram-positive bacteria before surgery. Clin Microbiol Infect. 2024;30(12):1537–1550. PMID: 39154859. doi:10.1016/j.cmi.2024.07.012
6. Hyun M, Lee JY, Kim HA, Ryu SY. Comparison of Escherichia coli and Klebsiella pneumoniae acute pyelonephritis in Korean patients. Infect Chemother. 2019;51(2):130–141. PMID: 31270992; PMCID: PMC6609746. doi:10.3947/ic.2019.51.2.130
7. Denis B, Lafaurie M, Donay JL, et al. Prevalence, risk factors, and impact on clinical outcome of extended-spectrum beta-lactamase-producing Escherichia coli bacteraemia: a five-year study. Int J Infect Dis. 2015;39:1–6. PMID: 26189774. doi:10.1016/j.ijid.2015.07.010
8. Yahav D, Giske CG, Grāmatniece A, Abodakpi H, Tam VH, Leibovici L. New β-Lactam-β-Lactamase Inhibitor Combinations. Clin Microbiol Rev. 2020;34(1):e00115–20. PMID: 33177185; PMCID: PMC7667665. doi:10.1128/CMR.00115-20
9. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
10. Sabour S, Harrington KRV, Martinson E, et al. Characterization of carbapenem-resistant enterobacterales and pseudomonas aeruginosa carrying multiple carbapenemase genes-antimicrobial resistance laboratory network, 2018-2022. J Clin Microbiol. 2024;62(12):e0122024. PMID: 39565121; PMCID: PMC11633150. doi:10.1128/jcm.01220-24
11. Lutgring JD. Carbapenem-resistant Enterobacteriaceae: an emerging bacterial threat. Semin Diagn Pathol. 2019;36(3):182–186. PMID: 31056277. doi:10.1053/j.semdp.2019.04.011
12. Weinstein MP, Lewis JS. The clinical and laboratory standards institute subcommittee on antimicrobial susceptibility testing: background, organization, functions, and processes. J Clin Microbiol. 2020;58(3):e01864–19. PMID: 31915289; PMCID: PMC7041576. doi:10.1128/JCM.01864-19
13. WHO Bacterial Priority Pathogens List Advisory Group; Sati H, Carrara E, Savoldi A, et al. The WHO bacterial priority pathogens list 2024: a prioritisation study to guide research, development, and public health strategies against antimicrobial resistance. Lancet Infect Dis. 2025;11:S1473–3099(25)00118–5. PMID: 40245910. doi:10.1016/S1473-3099(25)00118-5
14. Liu JY, Dickter JK. Nosocomial infections: a history of hospital-acquired infections. Gastrointest Endosc Clin N Am. 2020;30(4):637–652. PMID: 32891222. doi:10.1016/j.giec.2020.06.001
15. Halavaara M, Huotari K, Anttila VJ, Järvinen A. Healthcare-associated infective endocarditis: source of infection and burden of previous healthcare exposure. Antimicrob Steward Healthc Epidemiol. 2023;3(1):e152. PMID: 37771746; PMCID: PMC10523553. doi:10.1017/ash.2023.419
16. CTN 236 hPV in HIV Study Team; McClymont E, Lee M, Raboud J, et al. The efficacy of the quadrivalent human papillomavirus vaccine in girls and women living with human immunodeficiency virus. Clin Infect Dis. 2019;68(5):788–794. PMID: 29985988. doi:10.1093/cid/ciy575
17. Craven DE, Steger KA, Hirschhorn LR. Nosocomial colonization and infection in persons infected with human immunodeficiency virus. Infect Control Hosp Epidemiol. 1996;17(5):304–318. PMID: 8727620. doi:10.1086/647300
18. Szabó S, Feier B, Capatina D, Tertis M, Cristea C, Popa A. An overview of healthcare associated infections and their detection methods caused by pathogen bacteria in Romania and Europe. J Clin Med. 2022;11(11):3204. PMID: 35683591; PMCID: PMC9181229. doi:10.3390/jcm11113204
19. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ; COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. PMID: 32497510; PMCID: PMC7263814. doi:10.1016/S0140-6736(20)31142-9
20. Zhang C, Wang M, Sun S, Yi M, Wang S. Impact of COVID-19 on the prevalence and drug resistance of bacteria isolated from bacterial meningitis cerebrospinal fluid in Shandong province: a multicenter retrospective study. J Med Virol. 2024;96(11):e70063. PMID: 39540426. doi:10.1002/jmv.70063
21. Bestetti RB, Furlan-Daniel R, Couto LB. Nonpharmaceutical public health interventions to curb the COVID-19 pandemic: a narrative review. J Infect Dev Ctries. 2022;16(4):583–591. PMID: 35544617. doi:10.3855/jidc.14580
22. Doi Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–S575. PMID: 31724043; PMCID: PMC6853760. doi:10.1093/cid/ciz830
23. Sweileh WM. Bibliometric analysis of peer-reviewed literature on antimicrobial stewardship from 1990 to 2019. Global Health. 2021;17(1):1. PMID: 33397377; PMCID: PMC7780390. doi:10.1186/s12992-020-00651-7
24. Chen D, Li H, Zhao Y, et al. Characterization of carbapenem-resistant Klebsiella pneumoniae in a tertiary hospital in Fuzhou, China. J Appl Microbiol. 2020;129(5):1220–1226. PMID: 32396222; PMCID: PMC7687251. doi:10.1111/jam.14700
25. Tacconelli E, Górska A, De Angelis G, et al. Estimating the association between antibiotic exposure and colonization with extended-spectrum β-lactamase-producing Gram-negative bacteria using machine learning methods: a multicentre, prospective cohort study. Clin Microbiol Infect. 2020;26(1):87–94. PMID: 31128285. doi:10.1016/j.cmi.2019.05.013
26. Margalit I, Kunwar D, Gadot C, et al. Clinical impact of active screening cultures for carbapenem-resistant Acinetobacter baumannii: a systematic review and meta-analysis. Am J Infect Control. 2024;52(12):1351–1358. PMID: 38936479. doi:10.1016/j.ajic.2024.06.017
27. Ayobami O, Brinkwirth S, Eckmanns T, Markwart R. Antibiotic resistance in hospital-acquired ESKAPE-E infections in low- and lower-middle-income countries: a systematic review and meta-analysis. Emerg Microbes Infect. 2022;11(1):443–451. PMID: 35034585; PMCID: PMC8820817. doi:10.1080/22221751.2022.2030196
28. Arman G, Zeyad M, Qindah B, et al. Frequency of microbial isolates and pattern of antimicrobial resistance in patients with hematological malignancies: a cross-sectional study from Palestine. BMC Infect Dis. 2022;22(1):146. PMID: 35144553; PMCID: PMC8832646. doi:10.1186/s12879-022-07114-x
29. Vrobel O, Tarkowski P. Can plant hormonomics be built on simple analysis? A review. Plant Methods. 2023;19(1):107. PMID: 37833752; PMCID: PMC10576392. doi:10.1186/s13007-023-01090-2
30. Liu C, Du P, Xiao N, Ji F, Russo TA, Guo J. Hypervirulent Klebsiella pneumoniae is emerging as an increasingly prevalent K. pneumoniae pathotype responsible for nosocomial and healthcare-associated infections in Beijing, China. Virulence. 2020;11(1):1215–1224. PMID: 32921250; PMCID: PMC7549996. doi:10.1080/21505594.2020.1809322
31. Fu B, Xu J, Yin D, et al. Transmission of blaNDM in Enterobacteriaceae among animals, food and human. Emerg Microbes Infect. 2024;13(1):2337678. PMID: 38629492; PMCID: PMC11034458. doi:10.1080/22221751.2024.2337678
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.