")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Evaluation of the Effect of a New Surgical Medical Drain Anti-Dislodgement Fixation Patch and Fixation Method in Postoperative Thyroid Care: A Randomized Trial
Authors Zhang C, Mi W, Zhu Y, Li Y , Cao Y, Li Z
Received 13 September 2024
Accepted for publication 5 December 2024
Published 9 December 2024 Volume 2024:20 Pages 837—847
DOI https://doi.org/10.2147/TCRM.S491307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Caizhen Zhang,1 Weiping Mi,1 Yajun Zhu,1 Yonghao Li,2 Yifan Cao,3 Zhensu Li1
1Department of Thyroid Surgery, The First Hospital of Shanxi Medical University, Taiyuan, 0370001, People’s Republic of China; 2Department of General Surgery, Department of Hepato-Bilio-Pancreatic Surgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China; 3The Fifth Clinical School of Shanxi Medical University, Taiyuan, 0370001, People’s Republic of China
Correspondence: Zhensu Li, The First Hospital of Shanxi Medical University, 85 Jiefang South Road, Yingze District, Taiyuan City, Shanxi Province, 030001, People’s Republic of China, Email [email protected]
Participants: This study enrolled 294 patients admitted to the Thyroid Surgery Department of the First Hospital of Shanxi Medical University between April and July 2024. Patients were randomly assigned to either the control group (145 patients) or the experimental group (149 patients).
Interventions: The control group received traditional adhesive tape fixation for drains, while the experimental group utilized a newly developed fixation patch combined with a unique “C” and “S” fixation method. Both groups employed vertical negative pressure drainage.
Specific Objectives or Hypotheses: The aim of this study was to assess the clinical effectiveness and patient satisfaction with a novel surgical drain fixation patch and method in the context of thyroid surgery. The hypothesis was that the novel fixation patch and method would reduce drain-related adverse events, improve patient comfort, and increase patient satisfaction.
Outcomes: The experimental group exhibited significantly lower rates of drain-related adverse events, including displacement, infection, and leakage, compared to the control group (3.40% vs 53.10%, P < 0.05). Additionally, patients in the experimental group reported lower neck/throat pain scores (mean score: 0.84 vs 1.40 in the control group, P < 0.05) and experienced no drain pulling pain (0% vs 1.16% in the control group, P < 0.05). Furthermore, the need for patch replacements was virtually eliminated in the experimental group (0% vs 70.86% in the control group, P < 0.05). Patient satisfaction with the fixation method was significantly higher in the experimental group (83.3% vs 46.9% in the control group, P < 0.05).
Randomization: Patients were randomly assigned to the control and experimental groups, ensuring the fairness and reliability of the study.
Trial Registration: The study was retrospectively registered with the China Clinical Trial Registry (ChiCTR2400087677) on August 1, 2024.
Keywords: anti-dislodgement fixation patch, cervical drains, thyroid surgery, nursing adverse events, patient’s satisfaction
Introduction
Thyroid cancer (TC) is the most common malignant tumor of the endocrine system. In recent years, the incidence of TC has been growing rapidly worldwide, and according to data from the National Tumors Registry, the incidence of thyroid cancer in women in urban areas of China ranks 4th among all malignant tumors in women.1,2 In the treatment of thyroid surgery, surgery is the primary treatment for patients with TC and nodular goiter, and the quality of postoperative care determines the quality of the patient’s postoperative recovery.3 After thyroid surgery, 1–3 10#(The outer diameter is 10mm) surgical drainage catheters are routinely placed in the surgical area for drainage. The placement of drainage tubes reduces the accumulation of blood and fluid in the surgical area, monitors the amount of bleeding and prevents tracheal compression, and facilitates the surgeon’s observation of wound drainage.4–6 However, due to the long and thin drainage tubes and the drainage site located in the neck, several adverse events frequently arise in postoperative nursing care. Poor fixation, folding, and even complete dislodgement of the drainage tubes are common issues. Additionally, patients often experience postoperative pulling pain as a result of the drainage tubes in clinical practice.7–9 It can be seen that the nursing care of patients with indwelling cervical drains after thyroid surgery is difficult, and strict attention should be paid to the application and improvement of drainage tube nursing care to reduce the incidence of adverse events related to patients’ cervical drains and to ensure effective negative pressure drainage. Conventional tape fixation of neck drains has the following problems: Adhesive tapes can suffer from several drawbacks when used for drain fixation. Prolonged adhesion time, combined with high ward temperatures and patient sweat, often leads to poor fixation, thereby increasing the incidence of drainage tube dislodgement. Furthermore, the adhesive on the tape necessitates special treatment for removal, which exacerbates the patient’s local discomfort. Additionally, the frequent need to change the tape due to these issues further augments the nursing workload. There is a great need to improve drain fixation method. In this study, we developed a new surgical medical drain anti-dislodgement fixation patch and method, building upon the traditional cervical drain fixation patch. To analyze the clinical significance of this new fixation patch in nursing, patients in the hospital were randomly divided into an experimental group and a control group.
Methods
Patients
Based on the previous study and clinical practice, the experimental group and the control group were expected to have significant differences in the incidence of drainage-related adverse events. We calculated that a minimum of 294 patients (approximately 147 per group) would be needed to achieve the required power (80%) and confidence level (95%). To account for possible loss to follow-up and withdrawal, 294 patients were finally included. They all underwent surgical treatment in the thyroid surgery department of the First Hospital of Shanxi Medical University between April and July 2024. Participants were randomly assigned to either the control group (145 patients) or the experimental group (149 patients). Randomization was achieved with the use of a computer-generated random sequence that ensured balanced and unpredictable assignments. The inclusion criteria for the study were as follows: the surgeries had to be performed by the same team of physicians; postoperative neck drains were left in place for all patients; there was no cognitive impairment; and both patients and their family members volunteered to participate in the study. Exclusion Criteria are as follows: 1. The condition is critical; 2. Patients unable to co-operate with the questionnaire; 3. Incomplete patient information.
Novel Surgical Medical Drainage Tube Anti-Dislodgement Fixation Patch Structure and Fixation Method
The new surgical medical drainage tube anti-dislodgement fixation sticker is made of elastic cotton soft wide tape, which has good adhesion, elasticity, compliance, and can effectively fight against pulling, fixed firmly (Figure 1A and B); production method: After thyroid surgery, a uniform 10# surgical drainage catheter with a diameter of 3mm and an adhesive portion the width of an adult’s thumb (approx. 3cm) should be left in place, and the “elevated platform method” should be used to fix the catheter in conjunction with the catheter; therefore, the size of each new type of surgical medical drainage tube anti-dislodgement fixation patch is cut (length 6.6cm, width 3cm); cut the right angle of the ends of the adhesive patch into a curved shape to effectively reduce the occurrence of curled edges. At the same time, the outlet of the drainage tube should be fixed in a “C” shape with the adhesive tape fixation, which can effectively avoid the pulling pain and the risk of detachment during movement.
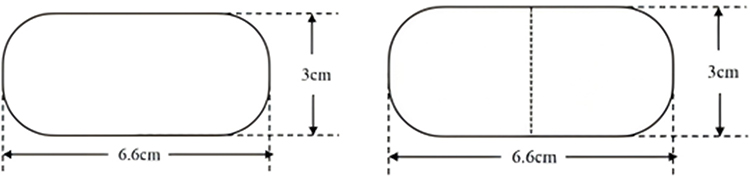 |
Figure 1 New Surgical Medical Drainage Tube Anti Dislodgement Fixation Patch (Left: the plan view; Right: the fixation method). |
Interventions
The Control Group
Patients to implement routine nursing methods, the patient returned to the ward after awakening from general anaesthesia, nursing staff will be neck drainage tube with double rows of tape fixed in the patient’s chest wall or shoulder and neck, the negative pressure suction ball comes with a plastic clip fixed in the hospital gown and organises the drainage bag (Figure 2A and B). Subsequently, pay close attention to the changes in the patient’s vital signs and the nature, colour and amount of fluid in the drainage tube, inform the patient and his family of the precautions to be taken to prevent the tube from prolapsing, and do a good job of teaching about the drainage tube. Because of the prolongation of the adhesive tape, the high temperature of the ward and some patients’ sweat wetting may cause poor fixation and adherence of dirt, the nursing staff of the night shift in the department routinely replaced the double rows of 3M adhesive tapes for each cervical drain and fixed them properly in the morning of the following day, which was included in the duties of the night shift nursing work. An improvement team was also set up to investigate the frequency of adverse events by developing a Checklist for the Occurrence of Adverse Events Related to Neck Drains in Patients. Patient’s cervical drain related adverse event checklist contents: date, bed number, name, days after surgery, type of related adverse event, and checker. The detailed flow chart of this study is detailed in Figure 3.
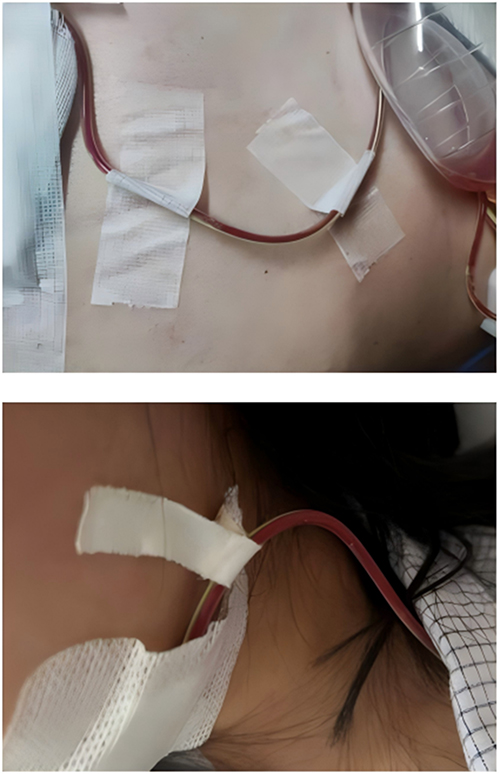 |
Figure 2 Traditional Surgical Medical Drainage Tube Anti-Dislodgement Fixation Patch (Top: non-woven adhesive patch; Bottom: cotton adhesive patch). |
 |
Figure 3 Flowchart of this study. |
The Experimental Group
The nursing staff of the whole department learnt the meaning of the use of the modified neck patch and the “C” type fixation method and then carried out a unified assessment, and only those who passed the assessment were allowed to participate in the nursing care of the patients in the research group in this study. Experimental group of patients with a single new type of surgical medical drainage tube anti-dislodgement fixation patch using the elevated platform method of adhesion, fixed with attention to the drainage tube outlet and adhesive stickers fixed at the “C” type, if secondary fixation is required, the adhesive tape is fixed to the patient’s shoulder, neck or chest wall in an “S” shape with the outlet of the drainage tube, and the plastic clip that comes with the negative pressure suction ball is fixed to the hospital gown, informing the patient of the importance of secondary fixation. Strengthen the relevant knowledge of the patient’s mission, strengthen the patient’s safety awareness of anti-dislodgement of drains, and enhance the patient’s medical compliance. Improvement team members completed a checklist for the occurrence of adverse events related to the patient’s cervical drain to the same standard as the control group and as required.
Assessment of Study Outcomes
The primary outcome of the study was the incidence of adverse events related to the neck drainage tube. Secondary outcomes may include patient satisfaction, pain scores, and time taken to change the adhesive decal of the neck drainage tube. The criteria for evaluating the relevant factors in this study were carried out as follows. ①Incidence of adverse events associated with neck drains: The number of cases of postoperative cervical drain-related adverse events (poor fixation, drain refolding, incomplete dislodgement, complete dislodgement, and local skin irritation) in both groups was regularly observed and recorded by the nurse in charge according to the level of patient care. ②Patient satisfaction with drain fixation: After the drain was fixed for 24h, a satisfaction questionnaire was distributed to the patients, and the satisfaction situation was classified into 4 grades: unsatisfied, generally satisfied, satisfied, and very satisfied. ③Comparison of pain scores produced by the two groups of patients. VAS pain scores produced by neck, throat, operative area, and drain pulling pain. It consists of pain scores, pain sites, nature of pain, assessment patterns, nursing measures, and signatures. A numerical pain scale was used to record pain scores at different sites, with 0 indicating no pain, 1 to 3 indicating mild pain, 4 to 6 indicating moderate pain, and 7 to 10 indicating severe pain.10,11 Pain scores generated by neck, throat, operative area, and drain pulling pain were recorded daily at 8:00 by the charge nurse until the patient was extubated. ④Comparison of the length of time it takes to change the adhesive patch on the neck drain in the two groups of patients. The length of time it took to routinely change the adhesive patch on each neck drain in the morning by the nursing staff on the night shift each day was recorded, ie from the start of the drain check to the end of the re-fixation. In this study, the same manufacturer’s electronic stopwatch was used to start timing from the time the nurse observed the drainage tube, and the timing ended when the replacement was completed and the drainage bulb was secured to the hospital gown with its own clip, which was defined as the time elapsed for 1 change of adhesive patches.
Statistical Analysis
All statistical analyses in this study were performed using SPSS (Version 25, IBM, USA). The continuous variables are expressed as mean ± standard deviation, categorical variables are reported as numbers and percentages, and the relevant clinical data of the control group and the experimental group were compared. Independent t-test and X2 test were used to compare the relevant variables and derive the differences between the two groups of patients in terms of relevant clinical data and postoperative outcome evaluation indexes. In this study, we utilized the Kolmogorov–Smirnov (K-S) test to assess and determine the normality of the distribution. When the p-value is less than or equal to 0.05, we consider there to be a statistically significant difference.
Results
Patient Baseline Characteristics
Tables 1 and 2 describe that there were 76 (19.3%) males and 218 (80.7%) females among all the patients; the mean age of the control group was 46.96 years (±13.517) and the mean age of the experimental group was 47.01 years (±12.554); 40 of all the patients suffered from hypertension and 10 from diabetes mellitus. There were 67 cases of nodular goitre in all patients, 57 cases of open surgery, 10 cases of endoscopic approach, 2 cases of 1 day of indwelling drain, 61 cases of 2 days of indwelling drain and 4 cases of 3 days of indwelling drain. There were 191 cases of thyroid cancer, of which 192 cases were operated by conventional open surgery, 19 cases by endoscopic approach, 154 cases with 2 days of indwelling drain and 37 cases with 3 indwelling drain; 36 cases of extended radical thyroidectomy, 3 cases with 2 days of indwelling drain after surgery, 17 cases with 3 days of indwelling drain after surgery, 13 cases with 4 days of indwelling drain; and 3 cases with 5 days of indwelling drain; the mean time of indwelling drain was 2.31 days (±0.629) in the control group and 2.32 days (±0.652) in the experimental group. There were 33 cases who indwell 2 drainage catheters after extended radical thyroid cancer surgery and 3 cases who indwell 3 drainage catheters after surgery; the mean time of indwelling drainage catheter was 1.16 days (±0.385) in the control group and 1.11 days (±0.359) in the experimental group.
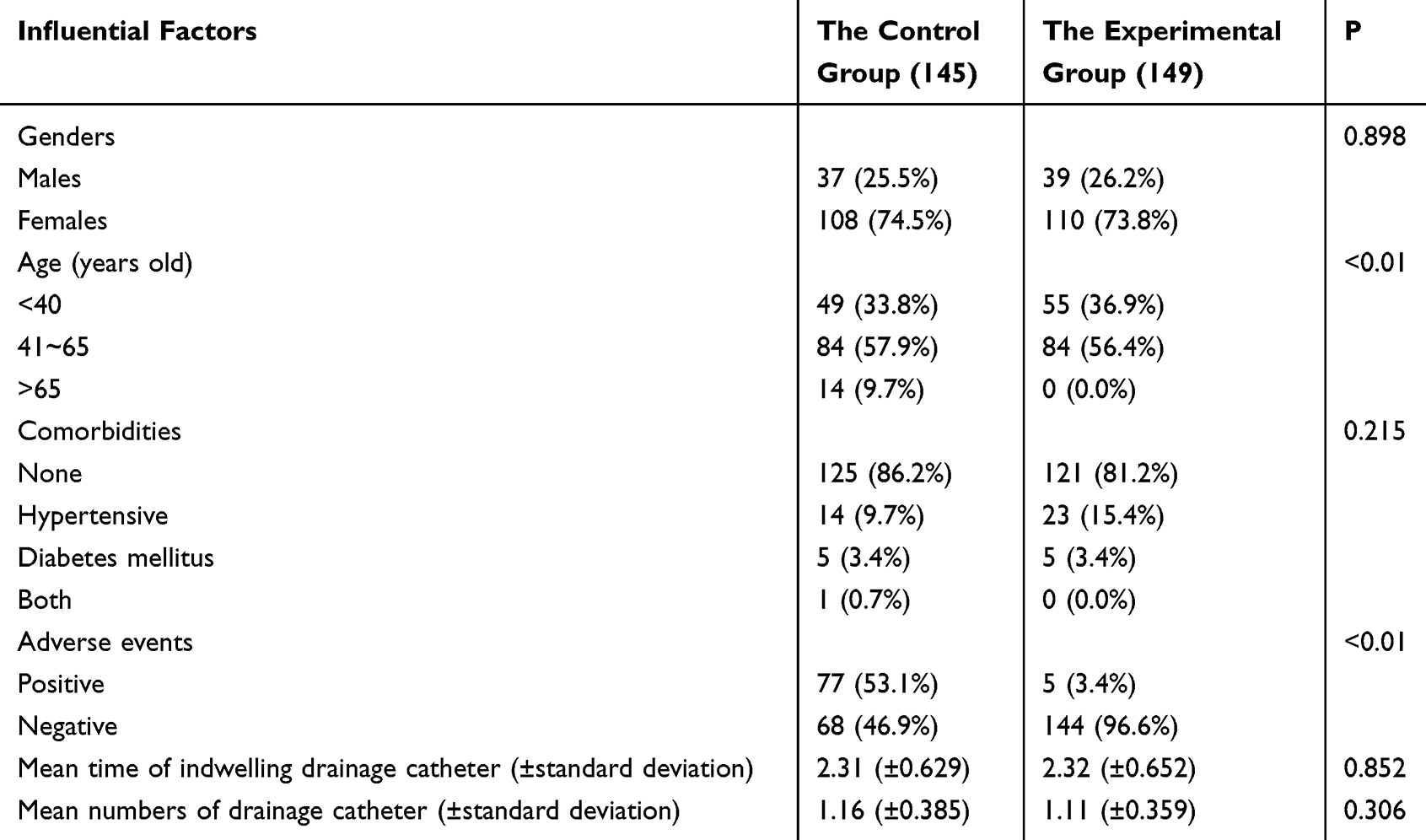 |
Table 1 Comparison of the General Data of the Two Groups of Patients Unit: Cases |
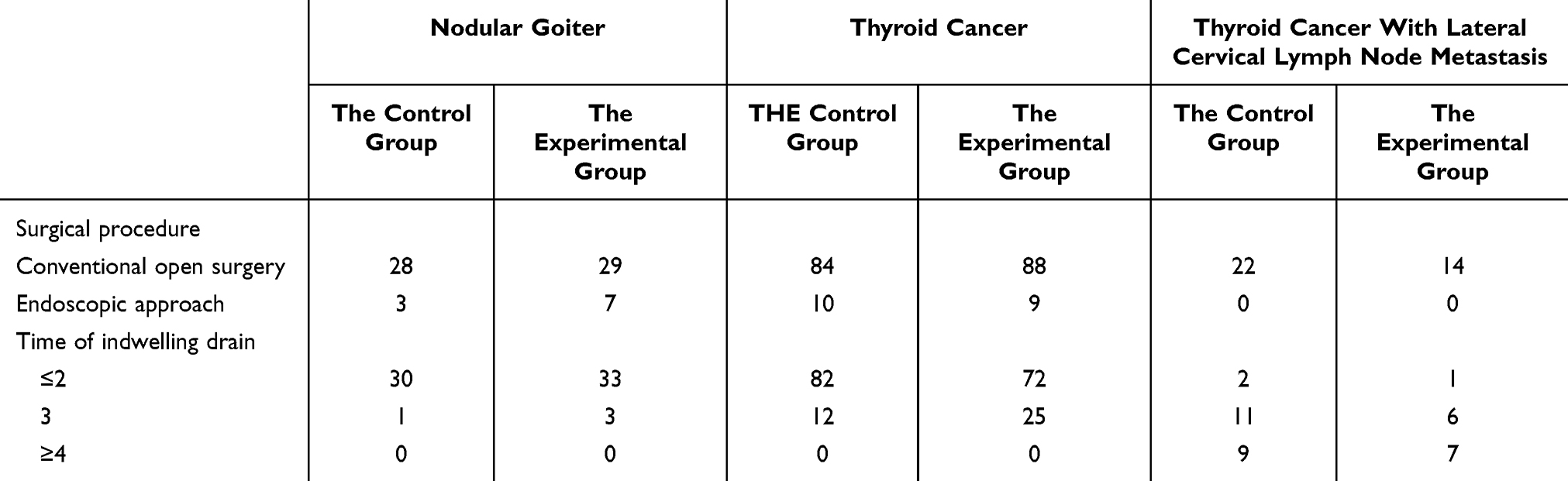 |
Table 2 Comparison of Time with Indwelling Drain Between the Two Groups |
Evaluation of Drainage Tube Adverse Events
As shown in Table 3, 71 cases (75.5%) in the control group were firmly fixed, 23 cases (24.5%) were not firmly fixed, 96 cases (90.0%) in the experiment group were firmly fixed, and 1 case (1.0%) was not firmly fixed. In the control group, there were 13 cases (13.8%) of drainage tube folding and 81 cases (86.2%) of non-folding, and in the experiment group, there were 1 case (1.0%) of drainage tube folding and 96 cases (99.0%) of non-folding. In the control group, there were 0 cases (0%) of complete decannulation without decannulation in 94 cases (100%), and in the experiment group, there were 0 cases (0%) of complete decannulation without decannulation in 97 cases (100%). The P values of the above neck drainage tube related adverse events were all <0.01. Similarly, in patients with nodular goiter and thyroid cancer with lateral cervical lymph node metastasis, there were still significant differences between the control group and the experiment group (P < 0.01).
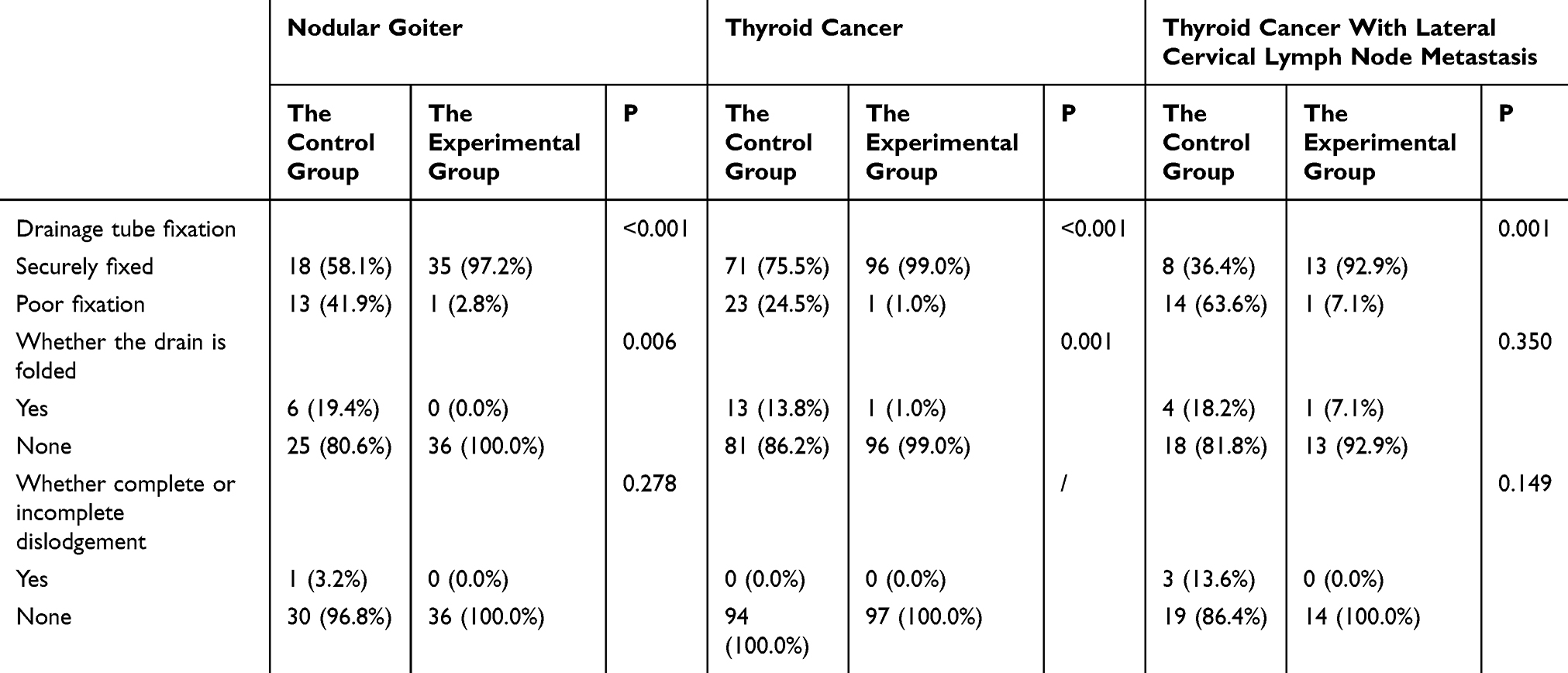 |
Table 3 Two Groups of Patients with Nodular Goiter, Thyroid Cancer, Thyroid Cancer with Lateral Cervical Lymph Node Metastasis |
Satisfaction Survey
As shown in Table 4, in the satisfaction survey of neck drainage tube, among 149 cases in the experiment group, 67 cases (45.0%) were very satisfied, 57 cases (38.3%) were satisfied, 23 cases (9.0%) were generally satisfied, and 0 cases (0%) were dissatisfied. The satisfaction rate of neck drainage tube fixation in the two groups (46.9% VS 83.3%) was significantly different (P < 0.01).
 |
Table 4 Comparison of Satisfaction with Drain Fixation in Two Groups of Patients Unit: Cases |
Time Evaluation of Changing the Glue of Neck Drainage Tube
As shown in Table 5, for 145 cases in the control group, the time for nurses to replace the patients’ neck drainage tube adhesive stickers was 70.86 (±55.136) seconds, and the experiment group did not need to replace the neck drainage tube adhesive stickers until discharge. The length of time for nursing staff to change the neck glue in the two groups was (70.86 ±55.136) VS 0, P < 0.01.
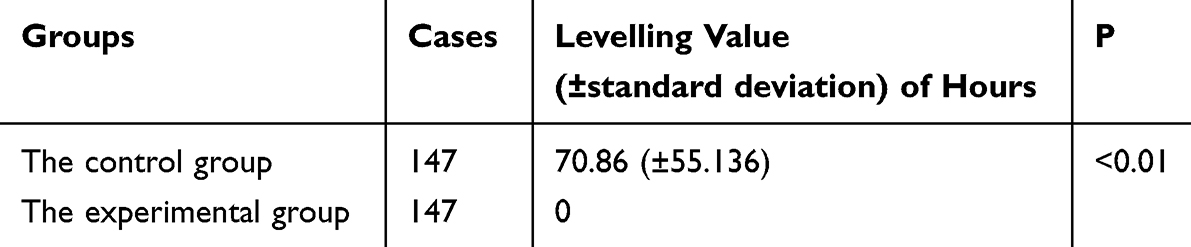 |
Table 5 Comparison of the Length of Time It Takes to Change the Adhesive Patch on the Neck Drain in Two Groups of Patients |
Postoperative Pain Score
As shown in Tables 6 and 7, in the control group, the average score of neck and throat pain was 1.40 (±1.324), the average traction pain of the drainage tube was 1.16 (±0.367); In the experiment group, the average score of neck and throat pain (± SD) of 149 patients was 0.84 (±0.570), and the average traction pain of drainage tube was 0.
 |
Table 6 Comparison of Neck and Throat Pain Scores Produced by the Two Groups of Patients |
 |
Table 7 Comparison of Drainage Tube Pulling Pain Scores Produced by the Two Groups of Patients |
Discussion
The primary objectives of this study were to investigate the effectiveness of a new type of surgical medical drain anti-dislodgement fixation patch and the “C” fixation method in reducing the incidence of drain-related adverse events in thyroid surgery patients and to assess patient satisfaction and comfort with this approach. In this study, we found that postoperative neck drain care is challenging due to factors such as insecure fixation, folding, or even dislodgement of the drainage tube, which can affect drainage effectiveness and patient recovery. In line with these objectives, the following discussion is divided into sections addressing the incidence of adverse events, patient satisfaction and comfort, as well as the implications for clinical practice.
To reduce the observation burden of medical staff and improve the efficiency of nursing work by using a new type of anti-detachment fixed patch for surgical drainage tube. An indwelling neck drain is a common treatment after thyroid surgery, which can further reduce the incidence of complications such as postoperative neck haematoma, fluid compression of the trachea and poor healing of incision infection, and ensure faster and better recovery of patients after thyroid surgery.12 However, after leaving a postoperative neck drain in place, ineffective drainage may occur due to the patient’s own factors, catheter factors, and caregiver factors, which is not conducive to the patient’s recovery.13,14 And due to the long and thin drainage tube, the postoperative nursing work often occurs insecure fixation, folding or even dislodgement and other adverse events, at the same time, due to the drainage tube caused by the patient’s postoperative pain in the clinic also occurs from time to time. It can be seen that it is difficult to care for patients with indwelling neck drains after thyroid surgery, and strict attention should be paid to the application and improvement of drainage tube care methods in order to reduce the incidence of adverse events related to patients’ neck drains and ensure effective negative pressure drainage.
In this study, 1–3 drains were routinely placed postoperatively in patients with nodular goiter, thyroid cancer, and thyroid cancer with lateral cervical lymph node metastases. Ensuring that negative pressure suction is effective15 is a priority in thyroid surgical care. The traditional non-woven adhesive tape has the characteristics of being light, thin and easy to tear, but it is easy to tear and leave residual glue in the process of fixation and replacement. In addition, the traditional cotton tape has the characteristics of poor viscosity and weak fixation. The new surgical drainage tube anti-stripping fixed patch is made of elastic cotton and soft material and is firmly fixed with the “C” type fixation method. There is no need to replace the adhesive patch during the first fixation to remove the neck drainage tube, which saves the operation time of nurses in each shift, improves work efficiency, and accelerates postoperative recovery. The results of this study showed that the average time of replacing the adhesive patch was 70.86 seconds for each patient with the traditional patch, while the new surgical drainage tube anti-detachment fixation patch did not need to be replaced.
The new type of surgical drainage tube anti-detachment fixation patch can reduce the incidence of adverse events of neck drainage tube. In the context of avoiding drain adverse events, Ruan et al have reduced the incidence of drain-related adverse events by making their own drain fixation devices, using flat bands as a carrier, knotting the bands and suspending them around the neck, and spring-loaded clasps to secure the drains. In order to facilitate the organisation of the drainage device, the negative pressure drainage ball and drainage bag were fixed on the patient’s gown, but with the prolongation of the banding time and the increase of drainage fluid, the width of the homemade flat bands itself was designed to be too narrow, and after a long period of time the flat bands rolled up the edge of the dimensions was too thin, and the pressure on the neck was increased, which increased the patient’s drawing pain and the risk of bleeding.16 Zhang et al have developed a strap-type neck drain fixation device that effectively prevents the incidence of drain adverse events and improves the efficiency of nursing care. However, the current thyroid surgery patients have a faster turnaround time in the hospital, short postoperative time with tubes and the vast majority of patients have only one drain placed in the neck, and the design of the strap-type neck drainage device is too cumbersome, and its cost-effectiveness and work efficiency are low.17 In this study, by using independent t-test and X2 test to compare the relevant variables, it is concluded that there is a significant difference between the experimental group and the control group in terms of postoperative effect evaluation indexes (P < 0.01), which indicates that the use of surgical medical drainage tube anti-dislodgement fixation stickers and fixation methods can reduce the incidence of drain-related adverse events, and the method of operation is convenient, easy to learn and easy to promote.
The new type of surgical drainage tube anti-detachment fixation plaster can avoid the pain of neck drainage tube and improve the comfort and satisfaction of patients. In this study, the results of applying surgical medical drain anti-dislodgement fixation patch are as follows:①The elastic soft cotton wide tape was cut to 6.6cm in length and 3cm in width, and the two ends were cut into a curved shape, which was shown to be a perfect fit for the 10# surgical drainage catheter used in this department, and effectively avoided the disadvantages of poor fixation of the tape. This new type of surgical medical drain anti-dislodgement fixation patch has good adhesion, elasticity and compliance, which can effectively counteract pulling and fix firmly, can effectively reduce the incidence of postoperative adverse events, and greatly reduces the possibility of allergy due to the patient’s local skin tearing, and improves the patient’s satisfaction. ②The new drainage tube with the use of “C” type fixation method improves the patients due to excessive pulling of the drainage tube caused by the pulling pain, and then promotes the patients to get out of bed early, effectively preventing the incidence of lower limb venous thrombosis, mobilising the patients’ postoperative rehabilitation and exercise enthusiasm.15 ③Although the traditional non-woven fixation patch has the characteristics of being light, thin and easy to tear, the fixation and replacement process is easy to tear and easy to leave the residual adhesive. In addition, the traditional cotton type adhesive tape there is poor adhesion and fixation of the characteristics of the weak, while the new surgical medical drainage tube anti-dislodgement fixation patch adopts elasticity of cotton and soft material of the abrasive gauze, with the “C” type fixation method, there is no need to change the neck patch frequently, which can greatly improve the comfort of the patients after the operation and the satisfaction of the patients during the hospitalisation period. ④As the surgical medical drain anti-dislodgement fixation patch is firmly fixed, there is no need to change the adhesive patch during the period from the first fixation to the removal of the cervical drain, which saves the operation time of nursing staff in all shifts, improves the work efficiency, and accelerates the postoperative recovery. In this study, the experimental group of patients implemented drain care, the new surgical medical drain anti-dislodgement fixation patch that effectively improves the safety of cervical drain fixation and the efficiency of nursing staff. In addition, in recent years, relevant studies have concluded that drainage tubes may not be used in the postoperative period after thyroidectomy,18 as they may reduce the pain, numbness and foreign body sensation in the neck of the patient’s incision. However, most studies have concluded that drainage after thyroid surgery is related to the extent of the surgical wound and the placement of drains is also related to operator experience and technique.19,20 The results of this study showed that the patients’ satisfaction with the nursing technical level, knowledge education ability and service attitude of the nurses in the study group were higher than those in the control group, and the differences were statistically significant (P < 0.001).
Although this study has confirmed the significant effect of the new surgical drainage tube anti-detachment fixation plaster in the postoperative care of thyroid surgery, there are still some limitations: First of all, this study was mainly conducted in the First Hospital of Shanxi Medical University. Although the sample size met the statistical requirements, there may be some regional and hospital specificity, which limits the wide applicability of the study results. Future studies can be considered to be conducted in multiple centers, different regions and hospitals to verify the general applicability of the fixator. Secondly, this study mainly focused on the short-term effect of drainage tube fixation after thyroid surgery, without in-depth discussion of the long-term effect. Although the short-term effect is remarkable, the safety and efficacy of long-term use still need to be further observed and studied. In the future, the study time can be extended to observe the performance of the new fixator over a longer period of time. Finally, this study was mainly based on clinical observation and statistical analysis, and no in-depth analysis was conducted on the specific material composition, air permeability and other physical and chemical properties of the new surgical drainage tube anti-detachment fixation patch. These physical and chemical properties may affect the skin comfort and allergic reactions of patients. Therefore, future research can further explore the material composition and physical and chemical properties of the fixator to optimize the product design and improve the comfort of patients.
Conclusions
The new surgical medical drainage tube anti-dislodgement fixed sticker operation is convenient, low cost and easy to promote, can be a good solution to the drainage tube fixed insecure pulling, extrusion, folding, twisting and lead to the problem of the pipeline is not smooth to avoid the occurrence of negative pressure failure and ineffective drainage. In this study, the use of the “C” method of drain fixation avoided pulling pain, thus improving the patient experience and satisfaction, and further promoting faster postoperative recovery. In addition, the opening above the negative pressure suction bulb of the cervical drain in the clinic is very prone to dislodgement leading to failure of the negative pressure, which can be improved in future studies.
Data Sharing Statement
All data in this study can be obtained by contacting the corresponding author.
Ethical Approval and Consent to Participate
This study was approved by the Institutional Ethics Review Committee of the First Hospital of Shanxi Medical University (Number: NO.KYLL-2024-187), and all its procedures involving human participants were in accordance with the Declaration of Helsinki (revised 2013). Ethical approval adoption is March 2024. All participants signed the Knowledgeable Consent Form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Zhao X, Bie F, Luo C, et al. Distress, illness perception and coping style among thyroid cancer patients after thyroidectomy: a cross-sectional study [J]. Eur J Oncol Nurs. 2024;69:102517. doi:10.1016/j.ejon.2024.102517
2. Bytnar JA, Enewold L, Shriver CD, Zhu K. Incidence of papillary thyroid cancer: comparison of the military and the general population by race and tumor stage/size[J]. Cancer Epidemiol. 2024;89:4208.
3. Ying C, YiXuan L. Effect of high-quality nursing on alleviating depression and anxiety in patients with thyroid cancer during perioperative period: a protocol for systematic review. Medicine. 2020;99(45):e23018–e23018. doi:10.1097/MD.0000000000023018
4. Samraj K, Gurusamy KS. Wound drains following thyroid surgery. Cochrane Database Syst Rev. 2007;2007(4):1.
5. Zhaoyan P, Qian H, Liping J, et al. Application effects of targeted nursing model in patients undergoing thyroid surgery and its influence on patients’ negative emotions. Am J Transl Res. 2021;13(4):2822–2830.
6. Zaghal A, Tamim H, Habib S, et al. Drain or no drain following pancreaticoduodenectomy: the unsolved dilemma. Scand J Surg. 2020;109(3):228–237. doi:10.1177/1457496919840960
7. Yusuke M, Hiroyuki Y, Shinya S, et al. Usefulness of preoperative ice cream consumption and novel postoperative drainage management in patients undergoing left-sided neck dissection for thyroid cancer: a nonrandomized prospective study. Surg Today. 2023;54(6):642–50.
8. Gao-Xiang C, Cheng L, Zhang H. Drainage during endoscopic thyroidectomy. JSLS. 2019;23(1):e201800060–e201800060. doi:10.4293/JSLS.2018.00060
9. Wang Z, Qi P, Zhang L, et al. Is routine drainage necessary after thyroid surgery? A randomized controlled trial study Front Endocrinol. 2023;14. doi:10.3389/fendo.2023.1148832
10. Park J, Lee KD, Kim EJ, et al. Postoperative pain management using an intravenous combination of ibuprofen and Acetaminophen compared with acetaminophen alone after thyroidectomy: a prospective randomized controlled trial. Head Neck. 2024;46:2068–2075. doi:10.1002/hed.27701
11. He QQ, Ma HY, Zhu J, et al. Comparison of transoral vestibular robotic thyroidectomy with traditional low-collar incision thyroidectomy. J Rob Surg. 2024;18(1). doi:10.1007/s11701-024-01831-y
12. De Salvo L, Arezzo A, Razzetta F, Tassone U, Mattioli FP. Rapporto fra tipo di drenaggio e sepsi nella chirurgia tiroidea [Connection between the type of drainage and sepsis in thyroid surgery]. Ann Ital Chir. 1998;69(2):165–167.
13. Betancourt C, Sanabria A. Post-thyroidectomy pain relief is enhanced by wound infiltration. A systematic review of randomized controlled trials.[J]. Surgeon. 2024;22(3):e133–e140. doi:10.1016/j.surge.2024.02.002
14. Zhang ZQ, Zhang LX, Zhao HR, Liu MY. Application analysis of cognitive nursing in thyroid surgery patients.[J]. Eur Rev Med Pharmacol Sci. 2023;27:1. doi:10.26355/eurrev_202306_32743
15. Filetti S, Durante C, Hartl D, et al. Electronic address: [email protected]. thyroid cancer: ESMO clinical. practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(12):1856–1883. doi:10.1093/annonc/mdz400
16. Hongjuan R, Liping W, Wei, et al. Application of a novel cervical drainage tube fixation device in head and neck surgery. Evidence-Based Nurs. 2019;2019:958–960.
17. Han Z, Liu YAP, Heng Z, et al. Nursing research. 2022;36(1):1–7.
18. Kennedy SA, Irvine RA, Westerberg BD, Zhang H. Meta-analysis: prophylactic drainage and bleeding complications in thyroid surgery. J Otolaryngol Head Neck Surg. 2008;37(6):768–773. doi:10.2013/7070.2008.060088
19. Ziming W, Peng Q, Lixi Z, et al. Is routine drainage necessary after thyroid surgery? A randomized controlled trial study.[J]. Front Endocrinol. 2023;14:1148832
20. Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing. Curr Probl Surg. 2014;51(7):301–331. doi:10.1067/j.cpsurg.2014.04.001
21. Addasi N, Fingeret A, Goldner W. Hemithyroidectomy for thyroid cancer: a review. Medicina. 2020;56(11):586
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.