")
Back to Journals » Journal of Pain Research » Volume 18
Explicit Motor Imaging Abilities Are Similar in Complex Regional Pain Syndrome, Chronic Limb Pain and Healthy Individuals: A Cross-Sectional Study
Authors Cohen-aknine G , Mottet D , Homs AF , Mura T , Jedryka F, Dupeyron AF
Received 7 October 2024
Accepted for publication 12 March 2025
Published 11 April 2025 Volume 2025:18 Pages 1949—1961
DOI https://doi.org/10.2147/JPR.S494546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Gabriel Cohen-aknine,1 Denis Mottet,2 Alexis F Homs,1 Thibault Mura,3 François Jedryka,4 Arnaud François Dupeyron1
1EuroMov Digital Health in Motion, Univ Montpellier, IMT Mines Ales, CHU Nimes, Nimes, France; 2EuroMov Digital Health in Motion, Univ Montpellier, IMT Mines Ales, Montpellier, France; 3Department of Biostatistics, Epidemiology, Public Health and Innovation in Methodology (BESPIM), CHU Nimes, Nimes, France; 4Department of Pain Management, CHU Nimes, Nimes, France
Correspondence: Gabriel Cohen-aknine, Centre Hospitalo-Universitaire de Nîmes, Place du Pr. Robert Debré, Nîmes Cedex 9, Nimes, 30029, France, Tel +334 66 68 34 59, Email [email protected]
Background: Complex regional pain syndrome (CRPS) is a chronic pain condition characterized by peripheral, central sensory and motor dysfunction. Implicit motor imagery is known to be impaired in CRPS patients, but evidence for explicit motor imagery is still lacking. Using a self-rated questionnaire, this study aims to compare explicit motor imagery abilities between individuals with CRPS, with chronic limb pain (CLP), and healthy controls, and to also examine differences between affected and unaffected limbs. We hypothesize that both CRPS and CLP patients will show a decrease in motor imagery abilities compared to healthy controls and in their affected limb compared to their own contralateral, unaffected side.
Patients and Methods: In this single-center observational study, 123 participants were recruited (CRPS = 40, chronic limb pain, CLP = 40, and healthy individuals = 43). Participants completed the Movement Imagery Questionnaire-Revised Second (MIQ-RS) once for each side of the body. The total MIQ-RS score, and the kinesthetic and visual subscores were compared between groups and between the affected and unaffected sides.
Results: A high degree of heterogeneity was observed in the explicit motor imagery scores and subscores, regardless of whether the participants were healthy or individuals with chronic pain. The MIQ-RS did not reveal any significant differences in explicit motor imagery abilities, neither between groups nor between the affected and unaffected side. Bayesian testing of the null hypothesis for kinesthetic motor imagery abilities indicated a sevenfold likelihood of no differences between groups and a more than a fivefold likelihood of no differences between sides.
Conclusion: Individuals with CRPS and chronic limb pain displayed preserved explicit motor imagery abilities, notably on the pain side. The preservation of these abilities supports the recommendation of mental imagery therapy to improve motor function and relieve pain in chronic pain patients.
Keywords: chronic pain, MIQ-RS, motor imagery questionnaire, imagery, psychotherapy, Bayes Theorem
Introduction
Complex regional pain syndrome (CRPS) is a rare, debilitating condition that primarily affects a single extremity and is characterized by pain that is disproportionate to the injury that originally provoked it.1,2 The International Association for the Study of Pain (IASP) classifies CRPS as chronic primary pain in the ICD-11 and suggests that it may also meet the criteria for nociplastic pain.3–5 The pathophysiology of CRPS involves complex interactions between immune-mediated inflammatory responses, vasomotor changes, genetic factors, psychological components and changes in the nervous system. These changes cause sensory, motor, autonomic and trophic dysfunctions1,6 such as allodynia or hyperalgesia, with 63% of patients experiencing a reduction in active movement.7 Sensory and motor dysfunction are associated with cortical changes, referred to as maladaptive plasticity.8–10
Engaging patients in active approaches improves motor recovery and promotes brain plasticity.11–13 This has motivated the use of motor imagery therapy, alone or in combination with other therapies, to activate motor neural networks, and reduce pain associated with physical movement.14 Motor imagery (MI) is a dynamic state in which individuals mentally simulate specific actions or gestures without actually performing the movement.15,16 Motor imagery training has shown promise in improving function and reducing pain by activating neural pathways similar to those used during actual movement execution.11,17,18 Although various theoretical models have proposed explanations for the motor imagery phenomenon, such as the motor simulation theory and the effect imagery model, there is no consensus on a definitive explanation of the observed effects.19,20
These therapies require patients to imagine their affected side in different modalities, and assessment methods are heterogeneous. Implicit motor imagery involves unconscious motor representations that are more related to prospective action and decision making in the spatial motor dimension. This type of motor imagery involves the accurate and timely identification of the laterality of a body part, often assessed in clinical settings by the Laterality Judgment Task. Explicit motor imagery, on the other hand, involves consciously imagining the movement of a body part from either a visual or kinesthetic perspective, often assessed in clinical settings by self-report questionnaires.21,22 In addition, previous studies have shown that explicit motor imagery may be more sensitive to the cognitive-evaluative and motivational-emotional dimensions of pain.23 Previous studies have shown that individuals with chronic musculoskeletal conditions, such as patients with chronic limb pain (CLP) or CRPS, have significant deficits in implicit MI compared to healthy controls and compared to their own contralateral, unaffected side, using the Laterality Judgment Task.24,25 Patients with both CRPS and CLP have demonstrated body perception disturbances, often referred to as the “neglect-like syndrome”.26–28 However, patients with CRPS appear to have greater severity than those with CLP.29 In addition, patients with CRPS differ from those with CLP in that CRPS patients have higher levels of central neuroinflammatory processes and clinical pain associated with allodynia and hyperalgesia.30 A previous study by La Touche et al31 showed that patients with another very common chronic primary pain condition, such as chronic low back pain (CLBP),32 had reduced performance on the explicit motor imagery dimension compared to asymptomatic controls.
Implicit and explicit motor imagery activate similar sensorimotor brain regions, as shown by spatial and time-frequency electroencephalography analyses.33 However, implicit motor imagery can be performed by inexperienced individuals,34 because it involves judging the laterality of the hand or foot, which involves a spatial dimension of the participant’s own body as a result of motor behaviors.35 Implicit and explicit motor imagery play an important role in the motor learning process. However, authors have suggested that explicit processes may involve higher cognitive demands related to the need to store information in working memory.36 Despite growing evidence of the impact of chronic pain on sensorimotor processes, explicit motor imagery abilities in people with CRPS are poorly understood.
The aim of this study is to compare explicit motor imagery abilities between CRPS patients, chronic limb pain (CLP) patients and healthy controls, and between the affected and unaffected limbs within these groups. Based on the observed impairments in implicit motor imagery in patients with chronic pain compared to healthy individuals, we hypothesize that CRPS and CLP patients will exhibit specific deficits in explicit motor imagery abilities. Furthermore, we hypothesize that both CRPS and CLP patients will show motor imagery impairments in their affected limb compared to their own contralateral, unaffected side.
Material and Methods
Design
This was a prospective, single-center, cross-sectional study conducted at the University Hospital of Nîmes (France). The study procedures complied with the ethical standards of the competent committee for human experimentation (local ethics committee 2020-A02281-38 designated “Comité de Protection des Personnes, Sud Méditérrannée IV” on 8/12/2020) and the Helsinki Declaration of 2013. The study protocol was registered on clinicaltrials.org on 11/01/2021 (NCT04703348). All individuals received an information letter and informed consent was obtained from all individuals. This paper has been pre-published on ResearchSquare as a preprint: https://www.medrxiv.org/content/10.1101/2023.04.02.23288051v4.
Participants and Setting
Individuals with CRPS were recruited at the Department of Pain Medicine (CHU Nîmes, France) between January 2021 and October 2022. Pain specialists recruited and classified patients based on the Budapest and eligibility criteria. Patients with CRPS were affected in either the upper or lower limb and on the dominant or non-dominant side. Healthy individuals were recruited through a poster campaign among hospital staff. Patients with chronic limb pain (CLP) were recruited and diagnosed at the Department of Physical Medicine and Rehabilitation by specialists in physical medicine and rehabilitation. They were included in the study if they had experienced limb pain for more than three months due to conditions such as musculoskeletal disorders, chronic post-traumatic pain, or post-operative pain, regardless of the underlying cause.
Inclusion criteria were: Age over 18 years, less than 150 minutes of moderate-to-vigorous physical activity per week, and education up to high school graduation or equivalent. The physical activity threshold was based on the World Health Organization 2020 guidelines.37 Individuals with higher levels of physical activity have been shown to have better motor imagery abilities,38 and to avoid potential bias, only participants classified as inactive were recruited. In addition, a previous study showed that explicit motor imagery scores were statistically lower in people with higher levels of education,39 hence our decision to include individuals with at least a high school diploma. Patients with CRPS had to meet the diagnostic criteria set out in the Budapest criteria.4,40 Both CRPS patients and those with chronic limb pain needed to have experienced pain for at least three months. In addition, individuals were excluded from the study if they met any of the following criteria CRPS secondary to stroke, stellate block performed within three weeks prior to the interview, presence of a central neurological disorder, diagnosis of chronic fibromyalgia or low back pain, pregnancy, postpartum or lactation, visual impairment that interfered with the use of the MIQ-RS questionnaire, history of limb amputation, previous experience with motor imagery practice, or recent psychiatric illness.
To characterize the population age, sex, body mass index (BMI), upper and lower dominant limb, education level, pain duration and physical activity level were recorded.
Protocol
After assessing the eligibility criteria and obtaining informed consent by the physician, individuals were asked to complete the Movement Imagery Questionnaire - Revised, Second Edition (MIQ-RS) during the consultation. Age, weight, height, pain duration and limb dominance (upper and lower) were self-reported. Patients were also asked to report their level of physical activity on a three-point scale (less than 1 hour, between 1 and 1.5 hours, and more than 1.5 hours of moderate to vigorous activity per week) and their level of education on a six-point scale (from high school to PhD and beyond).
Due to the Covid-19 pandemic, some individuals (60%) completed the questionnaire via videoconference with an investigator. The questionnaires were audio-recorded on REDCap© (online questionnaire).41 All participants completed a self-rated questionnaire twice, starting with the right side and then answering the left side, pausing if necessary. The session was administered in a single session, with no follow-up. The expected heterogeneity in dominance, laterality and upper or lower limb affected did not allow for randomization.
Outcome Measures
The Movement Imagery Questionnaire-Revised, Second Edition (MIQ-RS) was chosen for several reasons: its suitability for patients with motor limitations,42 its ability to measure lateralized imagery scores (comparing left and right sides), its validation in French,39 and its acceptable reliability and reproducibility.43 Furthermore, this questionnaire has been shown to correlate visual and kinesthetic scores with fMRI signals in stroke patients,44 although it has not yet been used in patients with CRPS.
The MIQ-RS is a validated self-rated questionnaire for the assessment of explicit motor imagery.42,43 It is a 14-item therapist-administered questionnaire in which patients first perform a movement, such as raising the knee, followed by visual and then kinesthetic motor imagery. Patients rate their abilities on a 7-point Likert scale, ranging from “very easy to see/feel” (1 point) to “very hard to see/feel” (7 points). The MIQ-RS offers two methods for scoring, as documented in the literature: the first method involves the calculation of a total score and two subscores for Kinesthetic Motor Imagery (KMI) and Visual Motor Imagery (VMI). The total possible score is 98, with each of the subscores (KMI and VMI) having a maximum of 49 points (Rimbert et al, 2019). Alternatively, the score can be derived by taking the mean of the responses for the total score and the two subscores on a 7-point Likert scale. There is no official cutoff point for assessing explicit motor imagery abilities. However, based on the systematic review by McInnes et al (2016), explicit motor imagery abilities were categorized into three levels: unable (scoring less than 48 out of 98), impaired (scoring between 49 and 73 out of 98), and normal (scoring more than 74 out of 98).
The primary outcome of the study was the characterization of motor imagery (MI) abilities for the three groups of participants. Secondary outcomes included differences in total and subscores of the MIQ-RS between the groups and differences in scores on the unaffected and affected sides within the CRPS and CLP groups.
No published results for this population were available for sample size calculation. Based on previous research using the MIQ-RS in patients with primary chronic pain conditions such as chronic low back pain, where La Touche et al31 found a minimum between-group effect size of 0.57 for the Visual Motor Imagery subscore. GPower 3.1.9.7 was used to calculate the required sample size.45 The use of a t-test analysis between independent groups was based on an alpha risk of 0.05 and a power of 0.2. The initial power calculation suggested 33 participants per group with a potential drop-out rate of 20%, which was adjusted to 40 participants per group, giving a total of 120 participants required for the study.
Data Analysis
The softwares JASP © and R Studio © were used to perform the statistical analyses.
First, a frequentist statistical approach was used with significance set for a two-tailed α level of 0.05. As data were not distributed normally, we used non-parametric signed-rank tests and report median and interquartile range (IQR) with a 95% confidence interval. To assess the effect of group (CRPS vs CLP vs healthy) on motor imagery scores, we performed a Kruskal–Wallis test. To assess the effect of pain on motor imagery scores across limbs (unaffected vs affected), we performed a Wilcoxon signed-rank test. Finally, we assessed the dispersion of scores between groups using a coefficient of variation, calculated as the standard deviation divided by the mean, and reported it as the median and interquartile range (IQR).
In addition, a multivariable linear regression analysis was performed to assess the potential influence of confounding variables, including age, sex, upper limb and lower limb dominance, body mass index (BMI), physical activity level, education level, and pain duration, on the total, KMI, and VMI scores. Adjusted means were calculated from this model, and results are presented with their corresponding standard errors.
Secondly, we used a Null Hypothesis Bayesian Testing (NHBT) approach for the assessment of evidence of a lack of difference.46,47 Specifically, we calculated the Bayes factor (BF01), which quantifies the likelihood of the null hypothesis versus the alternative hypothesis (for example, BF01 = 7 indicates that, given the data, no difference is 7 times more likely than a difference). A Bayes factor between 5 and 10 indicates moderate evidence in favor of the null hypothesis.48 Levene’s method was used to measure the equality of variances between the groups and sides. This analysis was performed using JASP © software with a prior in favor of differences between groups according to our hypothesis.47
Results
We screened 129 participants for inclusion, and 123 were included after exclusion and age matching (40 participants in the CRPS and CLP group respectively and 43 participants in the healthy group). The main characteristics of the participants are described in Table 1 (further demographic details are provided in Supplementary Data S1, Table S1).
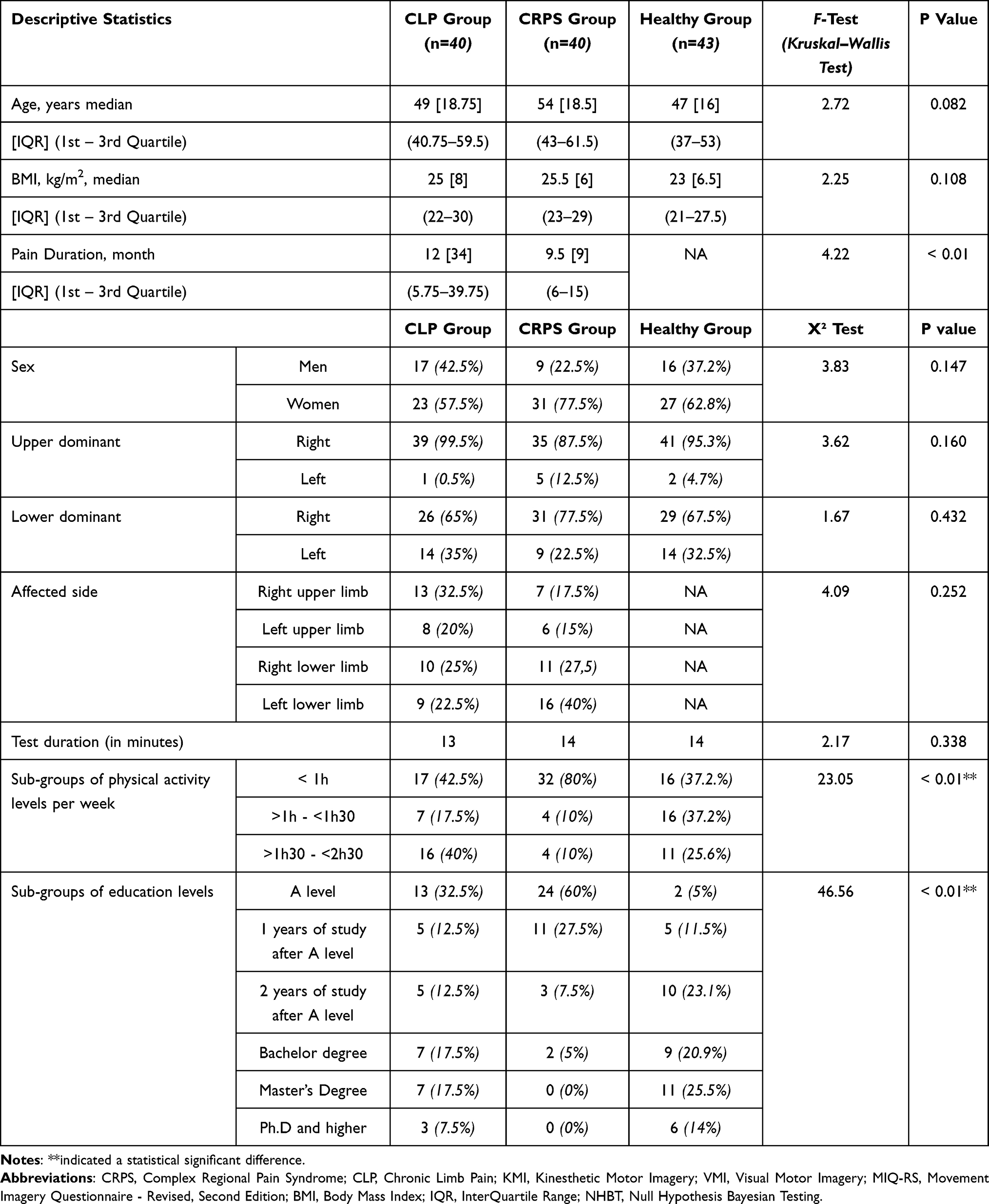 |
Table 1 Participant Demographic Characteristics. Data Are Presented as Medians for Continuous Variables and as Numbers and Percentages for Categorical Variables in Each Group |
Identification of Motor Imagery Abilities
The MIQ-RS total scores of the participants showed great heterogeneity, whether they were painful or healthy and regardless of the side of the limb (Figure 1).
 |
Figure 1 Violin plot of total MIQ-RS scores characterization among complex regional pain syndrome, chronic limb pain, and healthy groups. |
McInnes et al49 proposed three thresholds to account for three levels of motor imagery ability in participants with brain lesions. Our results showed a heterogeneous distribution of motor imagery abilities even within the “impaired” or “unable” thresholds, regardless of group (painful or healthy) or limb side (affected or contralateral unaffected). These results were not consistent with our hypothesis, which predicted a bimodal distribution with “unable” or “impaired” scores for the CRPS and CLP groups and a “normal” scores for the healthy group.
The median values of the MIQ-RS Total scores for the affected side and the unaffected side are shown in Supplementary Data S1 (Table S2).
Between-Individuals Coefficient of Variation
The coefficient of variation between individuals for the CRPS group is 24.53% for the affected side and 22.52% for the unaffected side. For the CLP group, the coefficient of variation is 18.13% for the affected side and 19.05% for the unaffected side. For the healthy group, the coefficient of variation is 15.84% for the right side and 17.85% for the left side. These results show a high dispersion of results, especially for the CRPS group, but with consistency between the affected and unaffected side for the pain groups.
Comparison of MI Abilities Between Groups
There were no statistical differences between the three groups for the MIQ-RS total mean score (H(2) = 1.795, p = 0.408, n² = −0.002) (Figure 2), the kinesthetic mean subscore (H(2) = 0.936, p = 0.626, n² = −0.009), or the visual mean subscore (H(2) = 4.175, p = 0.124, n² = 0.018) (Supplementary Data S1, Table S3).
 |
Figure 2 Violin plots of MIQ-RS mean scores between complex regional pain syndrome, chronic limb pain and healthy groups with Bayesian null hypothesis tests (BF01) between groups. |
Multivariable Analysis
There were no differences between the adjusted means of the groups for the total motor imagery scores (p = 0.135), the KMI subscore (p = 0.491) and the VMI subscore (p = 0.364).
Therefore, after accounting for confounding factors, there were no differences between the groups for the total motor imagery scores, the VMI, and KMI subscores.
Results are provided in the Supplementary Data S1 (Table S4).
Comparison of MI Abilities Between the Affected and Unaffected Sides
Complex Regional Pain Syndrome Group Analysis
There was no statistical difference between the affected side and the unaffected side for the MIQ-RS total mean score (W = 347.500, p = 0.826, r = 0.148), kinesthetic mean subscore (W = 377.000, p = 0.706, r = 0.086) and visual mean subscore (W = 272.500, p = 0.0881, r = 0.0187).The results are summarized in Supplementary Data S1 (Table S5).
Chronic Limb Pain Group Analysis
There was also no statistical difference between the affected side and the unaffected side for the MIQ-RS total mean score (W = 343.500, p = 0.910, r = 0.148), kinesthetic mean subscore (W = 372.500, p = 0.983, r = 0.334) and visual mean subscores (W = 317.500, p = 0.514, r = 0.006) in the CLP group (Supplementary Data S1, Table S5).
The complete inferential statistical analysis can be found in the Supplementary Data S1.
Bayesian Null Hypothesis Testing
Frequentist analysis showed no significant differences between the groups or between the affected and unaffected sides. In addition, Levene’s test indicated that the variances were homogeneous. Therefore, a Bayesian null hypothesis testing approach was used to draw conclusions about the null hypothesis and group similarities.46
Thus, we confirmed the absence of between-group differences in explicit motor imagery abilities with moderate evidence for the null hypothesis (BF01 > 5), specifically in Kinesthetic Motor Imagery (KMI) with a Bayesian factor of 7.28, as detailed in Supplementary Data S1 (Table S6). This indicates a 7-fold increase in the probability that there are no differences in Kinesthetic Motor Imagery abilities between the groups compared to the prior probability after observing the data.
We also confirmed the absence of differences in explicit motor imagery abilities between the affected and unaffected side in both the CRPS and CLP groups, with moderate evidence for the null hypothesis (BF01 > 5). Details are provided in Supplementary Data S1 (Table S7). This suggests a 5-fold increase in the probability that there are no differences in motor imagery abilities (both kinesthetic and visual) between the unaffected and affected sides in individuals with complex regional pain syndrome and chronic limb pain, compared to the prior probability after observing the data.
This suggests that chronic pain does not affect explicit motor imagery abilities as assessed by the MIQ-RS (Figure 2).
However, we could not confirm the similarity between groups for the total and visual subscores because the Bayes factor for the null hypothesis was less than 3, indicating that the evidence is not conclusive. This means that the data do not provide sufficient enough evidence to support or reject the null hypothesis for these subscores (Supplementary Data S1, Tables S6 and S7).
Discussion
In this study, we observed high inter-individual variability, with dispersion around the group medians ranging from 15% to 25% for total explicit motor imagery scores. There were no significant differences between groups or between the affected and unaffected sides. A secondary analysis showed similar explicit motor imagery abilities between groups and between the affected and unaffected sides. The significance of these findings will be discussed below.
First, our study revealed significant variability in explicit mental imagery abilities between participants, consistent with the broader spectrum of explicit imagery vividness identified in the literature, ranging from aphantasia to hyperphantasia, as reported by Zeman.50 The MIQ-RS was unable to discriminate between healthy and painful individuals, suggesting that it may not effectively capture explicit motor imagery at the group level. The observed heterogeneity between individuals in explicit motor imagery abilities does not reflect changes in these abilities over time, nor does it allow us to understand the dynamics, ie, whether individuals with chronic pain had the ability to engage in explicit mental imagery prior to the onset of chronic pain. Using a descriptive approach to our results, patients with CRPS appear to have higher variability than healthy controls, regardless of whether the affected or unaffected side is considered. This variability may be due to patient heterogeneity in clinical presentation and may be attributed to the potential subtypes of CRPS based on clinical presentation.51 However, no statistical comparisons of this variability were performed, so caution should be used in interpreting the results. In addition, the MIQ-RS is a self-report questionnaire in which healthy participants may give lower ratings for minor motor imagery difficulties because their self-assessments are based on a pain-free reference point. In contrast, patients with chronic pain may give higher ratings based on comparisons between their current and past motor imagery abilities, especially if their initial deficits have improved over time. If healthy participants tend to underestimate their abilities and patients tend to overestimate their abilities, these opposing biases could balance the results and possibly explain the lack of observed differences in questionnaire scores.
Secondly, our Bayesian null hypothesis testing supports the conclusion of similar kinesthetic motor imagery abilities between groups, with a 7-fold probability in favour of no differences. However, we did not confirm these similarities for the total mean scores and the visual mean subscores. Visual and kinesthetic imagery have been shown to activate different sensorimotor brain areas.52 The kinesthetic subscore has been shown to activate more brain areas involved in motor imagery tasks and to correlate better with brain activity in fMRI studies compared to visual modalities.44,53 In healthy individuals, kinesthetic ability correlates with motor execution, whereas visual ability correlates with motor observation.54 Thus, KMI appears to activate sensorimotor brain areas that are closer to motor execution than VMI. In addition, our results contrast with our hypothesis of differences based on previous literature for implicit motor imagery. Implicit and explicit motor imagery tasks activate similar areas, particularly in the beta-band frequency of electroencephalography.33 However, implicit tasks are less spatially specific and more intense than explicit tasks, and some authors have suggested that the explicit modality may mobilize higher cognitive demands.23 Furthermore, individuals can perform implicit tasks (laterality judgment tasks) without using a motor imagery-based strategy.55 Chronic pain patients have been shown to have body perception disturbances, known as the “neglect-like syndrome”,29,56 which could interfere with implicit motor imagery tasks and may explain the differences observed between implicit and explicit MI abilities in our studies. Indeed, some authors suggest that implicit MI tasks could be used to assess body perception disturbance.26 Our findings suggesting preserved kinesthetic motor imagery abilities in patients with chronic limb pain are promising for rehabilitation, especially in individuals known to have high levels of fear of movement.57 However, attention should be paid to the amount of cognitive effort required during the kinesthetic motor imagery task.
Thirdly, our findings contrast with our initial hypothesis, which was based on a previous study reporting that patients with other primary chronic pain conditions, such as chronic low back pain, show impairments in explicit motor imagery abilities assessed with a similar questionnaire.31 In this study, patients showed prominent psychological factors, such as high levels of catastrophizing. However, psychosocial factors were not measured in our study. Personal factors related to psychological state and personality traits have been shown to influence mental training in athletes.58 Therefore, psychological factors may influence explicit motor imagery abilities, and our discrepancies may be explained by the presence of unmeasured psychological factors in our study.
Motor imagery tasks partially target some of the same brain networks as voluntary motor movements and motor imagery therapy has been shown to be effective in improving neural plasticity and motor behavior in both healthy and pathological individuals.14,15,18,59,60 The perceptual-cognitive model proposed by some authors suggests that motor imagery may be associated with a high level of motor planning, in that the selection of a motor plan activates a conscious experience of the sensory consequences of an action.19 Interestingly, participants with CRPS have shown no change in motor planning when engaged in object affordance tasks.61 However, further research is needed to better understand the relationship between motor imagery and motor planning.
Motor imagery is a key component of movement representation methods (MRMs), which include action observation, motor imagery and mirror therapy.23 These approaches have been shown to be effective in the management of chronic musculoskeletal pain, particularly in patients with complex regional pain syndrome (CRPS),62,63 and chronic pain conditions.59,62,64–66 Furthermore, a meta-analysis has shown that motor imagery, whether used as a stand-alone therapy or as an adjunct, significantly reduces pain and disability in CRPS patients in both the short and long term.18 This approach is particularly advantageous because motor imagery training can be self-administered, which promotes patient empowerment and is consistent with the self-management principles emphasized in chronic pain guidelines.12,67,68 Furthermore, motor imagery may be beneficial at all stages of chronic musculoskeletal conditions, as suggested by previous studies.69 However, engaging in explicit motor imagery tasks can induce pain and sudomotor symptoms in patients with CRPS suggesting the need for a graded approach to exposure even during motor imagery therapy sessions.70 Anecdotally, to our knowledge, no patient in our study reported pain during questionnaire administration. However, this may be due to the short duration of the assessment compared to the longer duration typically required for rehabilitation using motor imagery as a therapy.
Explicit imagery training is the second stage of Graded Motor Imagery (GMI) therapy, which consists of three phases: starting with implicit motor imagery tasks, progressing to explicit motor imagery tasks, and ending with mirror therapy. The sequence of these phases is thought to be important in determining the benefits of the therapy.14,71 Despite its effectiveness in some conditions, GMI shows inconsistent results, which may explained by the interindividual variability observed in our study and previously described by others.13,72 Individuals with lower explicit motor imagery abilities could exhibit hypoactivation, which could explain a form of motor disuse or dysfunction.73,74 Consequently, assessment of motor imagery vividness using more inclusive tools than the MIQ-RS could allow tailoring of rehabilitation programs to individual needs prior to mirror therapy. This personalized approach could effectively address the different subtypes of CRPS and improve recovery outcomes.51,75 Therefore, our results suggest that explicit motor imagery, in its kinesthetic modality, is preserved despite the condition of chronic limb pain and may be beneficial as a first-line therapy in rehabilitation.
Limitations include the non-random order of questionnaire completion and the aggregation of upper, lower and spinal motor imagery scores in the calculation of the MIQ-RS score, which may have masked specific limb scores. Furthermore, the lack of homogeneity of the subgroups in terms of physical activity level, education level, and pain duration may have biased our results, although all participants were inactive (physical activity less than 2.5 hours per week) and all pain groups were chronic (pain duration greater than three months). Education level appears to be a predictor of pain chronicity,76 and despite the lower education level in the pain groups, there were no differences in motor imagery abilities, which may mitigate the recruitment bias in our study. Our study did not assess pain intensity, which could have revealed potential sources of bias in different subtypes of chronic pain patients.51 Finally, previous studies in patients with CRPS have shown an association between pain duration and pain intensity, with pain duration having a significant effect on motor performance and resulting in a smaller brain somatosensory representation in the somatosensory cortex.77 In our study, the pain duration was less than 1 year, which may not reflect the general population of patients with chronic limb pain.
Future research should pursue a deeper understanding of the efficacy mechanisms underlying different motor imagery training tasks (explicit, implicit, external, internal) in patients with complex regional pain syndrome,78 using more objective measures such as brain imaging in longitudinal research designs. In addition, exploring patient categorization methods for personalized interventions, similar to those explored in chronic low back pain research,79 may help to identify individuals suitable for specific interventions.75
Conclusion
Individuals with CRPS and chronic limb pain showed high inter-individual variability in explicit motor imagery tasks, similar to that observed in healthy individuals, with preserved abilities between groups and sides. The integration of movement representation methods, particularly in the form of kinesthetic motor imagery, may be considered a viable first-line treatment given the relatively preserved abilities of patients with chronic limb pain.
Data Sharing Statement
The study data are available upon reasonable request to the corresponding author.
Acknowledgments
We thank the following people for their support and help: Marine Ourmet, Brigitte Laffont for regulatory documents, Willy Fagart, Dr. Anaïs Pages, Julie Bourdier, Romain Dolin, Shuan Banh, Kevin Jezequel and Sarah Kabani for editing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Ferraro MC, O’Connell NE, Sommer C, et al. Complex regional pain syndrome: advances in epidemiology, pathophysiology, diagnosis, and treatment. Lancet Neurol. 2024;23(5):522–533. doi:10.1016/S1474-4422(24)00076-0
2. Goebel A, Barker C, Birklein F, et al. Standards for the diagnosis and management of complex regional pain syndrome: results of a European Pain Federation task force. Eur J Pain. 2019;23(4):641–651. doi:10.1002/ejp.1362
3. Goebel A, Birklein F, Brunner F, et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain. 2021;162(9):2346–2348. doi:10.1097/j.pain.0000000000002245
4. Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain. 2010;150(2):268–274. doi:10.1016/j.pain.2010.04.030
5. Schmidt H, Drusko A, Renz MP, et al. Application of the grading system for “nociplastic pain” in chronic primary and chronic secondary pain conditions: a field study. Pain. 2025;166(1):196–211. doi:10.1097/j.pain.0000000000003355
6. Birklein F, Ajit SK, Goebel A, Perez RSGM, Sommer C. Complex regional pain syndrome — phenotypic characteristics and potential biomarkers. Nat Rev Neurol. 2018;14(5):272–284. doi:10.1038/nrneurol.2018.20
7. Ott S, Maihöfner C. Signs and Symptoms in 1,043 Patients with Complex Regional Pain Syndrome. J Pain. 2018;19(6):599–611. doi:10.1016/j.jpain.2018.01.004
8. Ma T, Li ZY, Yu Y, et al. Gray Matter Abnormalities in Patients with Complex Regional Pain Syndrome: a Systematic Review and Meta-Analysis of Voxel-Based Morphometry Studies. Brain Sci. 2022;12(8):1115. doi:10.3390/brainsci12081115
9. Shokouhi M, Clarke C, Morley-Forster P, Moulin DE, Davis KD, St Lawrence K. Structural and Functional Brain Changes at Early and Late Stages of Complex Regional Pain Syndrome. J Pain. 2018;19(2):146–157. doi:10.1016/j.jpain.2017.09.007
10. Zangrandi A, Allen Demers F, Schneider C. Complex Regional Pain Syndrome. A Comprehensive Review on Neuroplastic Changes Supporting the Use of Non-invasive Neurostimulation in Clinical Settings. Front Pain Res. 2021;2:732343. doi:10.3389/fpain.2021.732343
11. Ferraro M, Cashin A, Wand B, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome- an overview of systematic reviews. Cochrane Database Syst Rev. 2023;6(6). doi:10.1002/14651858.CD009416.pub3
12. Harden RN, McCabe CS, Goebel A, et al. Complex Regional Pain Syndrome: practical Diagnostic and Treatment Guidelines. Pain Med. 2022;23(Suppl 1):S1–S53. doi:10.1093/pm/pnac046
13. Smart KM, Ferraro MC, Wand BM, O’Connell NE. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database Syst Rev. 2022. doi:10.1002/14651858.CD010853.pub3
14. Lotze M, Moseley GL. Clinical and Neurophysiological Effects of Progressive Movement Imagery Training for Pathological Pain. J Pain. 2022;23(9):1480–1491. doi:10.1016/j.jpain.2022.04.008
15. Decety J. Do imagined and executed actions share the same neural substrate? Cognit Brain Res. 1996;3(2):87–93. doi:10.1016/0926-6410(95)00033-X
16. Moran A, Guillot A, MacIntyre T, Collet C. Re-imagining motor imagery: building bridges between cognitive neuroscience and sport psychology. Br J Psychol. 2012;103(2):224–247. doi:10.1111/j.2044-8295.2011.02068.x
17. Hardwick RM, Caspers S, Eickhoff SB, Swinnen SP. Neural correlates of action: comparing meta-analyses of imagery, observation, and execution. Neurosci Biobehav Rev. 2018;94:31–44. doi:10.1016/j.neubiorev.2018.08.003
18. Ríos-León M, Cuñado-González Á, Domínguez-Fernández S, Martín-Casas P. Effectiveness of motor imagery in complex regional pain syndrome: a systematic review with meta-analysis. Pain Pract. 2024. doi:10.1111/papr.13348
19. Hurst AJ, Boe SG. Imagining the way forward: a review of contemporary motor imagery theory. Front Hum Neurosci. 2022;16. doi:10.3389/fnhum.2022.1033493.
20. Solomon JP, Hurst AJ, Lee J, Boe SG. Are observed effects of movement simulated during motor imagery performance? Behavioral Neuroscience. 2022;136(3):264–275. doi:10.1037/bne0000517
21. Chepurova A, Hramov A, Kurkin S. Motor Imagery: how to Assess, Improve Its Performance, and Apply It for Psychosis Diagnostics. Diagnostics. 2022;12(4):949. doi:10.3390/diagnostics12040949
22. Guillot A, Collet C. Contribution from neurophysiological and psychological methods to the study of motor imagery. Brain Res Brain Res Rev. 2005;50(2):387–397. doi:10.1016/j.brainresrev.2005.09.004
23. Cuenca-Martínez F, Suso-Martí L, León-Hernández JV, La Touche R. The Role of Movement Representation Techniques in the Motor Learning Process: a Neurophysiological Hypothesis and a Narrative Review. Brain Sci. 2020;10(1):27. doi:10.3390/brainsci10010027
24. Breckenridge JD, Ginn KA, Wallwork SB, McAuley JH. Do People With Chronic Musculoskeletal Pain Have Impaired Motor Imagery? A Meta-analytical Systematic Review of the Left/Right Judgment Task. J Pain. 2019;20(2):119–132. doi:10.1016/j.jpain.2018.07.004
25. Ravat S, Olivier B, Gillion N, Lewis F. Laterality judgment performance between people with chronic pain and pain-free individuals. A systematic review and meta-analysis. Physiother Theory Pract. 2020;36(12):1279–1299. doi:10.1080/09593985.2019.1570575
26. Acapo S, Osinski T, Rulleau T, Dupeyron A, Nizard J. Assessment of body perception disturbances in complex regional pain syndrome: a systematic review using the COSMIN guideline. Eur J Pain. 2022;26(10):2060–2073. doi:10.1002/ejp.2032
27. Lewis J. Body Perception Disturbance (BPD) in CRPS. Available from: https://www.practicalpainmanagement.com/pain/neuropathic/crps/body-perception-disturbance-bpd-crps.
28. Halicka M, Vittersø AD, Proulx MJ, Bultitude JH. Neuropsychological Changes in Complex Regional Pain Syndrome (CRPS). Behav Neurol. 2020;2020:e4561831. doi:10.1155/2020/4561831
29. Frettlöh J, Hüppe M, Maier C. Severity and specificity of neglect-like symptoms in patients with complex regional pain syndrome (CRPS) compared to chronic limb pain of other origins. Pain. 2006;124(1–2):184–189. doi:10.1016/j.pain.2006.04.010
30. Karpin H, Vatine JJ, Bachar Kirshenboim Y, Markezana A, Weissman-Fogel I. Central Sensitization and Psychological State Distinguishing Complex Regional Pain Syndrome from Other Chronic Limb Pain Conditions: a Cluster Analysis Model. Biomedicines. 2022;11(1):89. doi:10.3390/biomedicines11010089
31. La Touche R, Grande-Alonso M, Cuenca-Martínez F, Gónzález-Ferrero L, Suso-Martí L, Paris-Alemany A. Diminished Kinesthetic and Visual Motor Imagery Ability in Adults With Chronic Low Back Pain. PM R. 2019;11(3):227–235. doi:10.1016/j.pmrj.2018.05.025
32. Leadley RM, Armstrong N, Lee YC, Allen A, Kleijnen J. Chronic Diseases in the European Union: the Prevalence and Health Cost Implications of Chronic Pain. J Pain Palliative Care Pharmacother. 2012;26(4):310–325. doi:10.3109/15360288.2012.736933
33. Osuagwu BA, Vuckovic A. Similarities between explicit and implicit motor imagery in mental rotation of hands: an EEG study. Neuropsychologia. 2014;65:197–210. doi:10.1016/j.neuropsychologia.2014.10.029
34. Ladda AM, Lebon F, Lotze M. Using motor imagery practice for improving motor performance – a review. Brain Cognition. 2021;150:105705. doi:10.1016/j.bandc.2021.105705
35. Wang S, Williams J, Wilmut K. Constraints on motor planning across the life span: physical, cognitive, and motor factors. Psychol Aging. 2020;35(3):421–433. doi:10.1037/pag0000408
36. Parsons LM. Integrating cognitive psychology, neurology and neuroimaging. Acta Psychologica. 2001;107(1):155–181. doi:10.1016/S0001-6918(01)00023-3
37. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
38. Debarnot U, Sperduti M, Di Rienzo F, Guillot A. Experts bodies, experts minds: how physical and mental training shape the brain. Front Human Neurosci. 2014;8. doi:10.3389/fnhum.2014.00280.
39. Loison B, Moussaddaq AS, Cormier J, et al. Translation and validation of the French Movement Imagery Questionnaire – revised Second version (MIQ-RS). Ann Phys Rehabil Med. 2013;56(3):157–173. doi:10.1016/j.rehab.2013.01.001
40. Mesaroli G, Hundert A, Birnie KA, Campbell F, Stinson J. Screening and diagnostic tools for complex regional pain syndrome: a systematic review. PAIN. 2021;162(5):1295–1304. doi:10.1097/j.pain.0000000000002146
41. Floridou GA, Peerdeman KJ, Schaefer RS. Individual differences in mental imagery in different modalities and levels of intentionality. Mem Cognit. 2022;50(1):29–44. doi:10.3758/s13421-021-01209-7
42. Gregg M, Hall C, Butler A. The MIQ-RS: a Suitable Option for Examining Movement Imagery Ability. Evid Based Complement Alternat Med. 2010;7(2):249–257. doi:10.1093/ecam/nem170
43. Butler AJ, Cazeaux J, Fidler A, et al. The Movement Imagery Questionnaire-Revised, Second Edition (MIQ-RS) Is a Reliable and Valid Tool for Evaluating Motor Imagery in Stroke Populations. Evid Based Complement Alternat Med. 2012;2012:1–11. doi:10.1155/2012/497289
44. Confalonieri L, Pagnoni G, Barsalou LW, Rajendra J, Eickhoff SB, Butler AJ. Brain Activation in Primary Motor and Somatosensory Cortices during Motor Imagery Correlates with Motor Imagery Ability in Stroke Patients. ISRN Neurol. 2012;2012:613595. doi:10.5402/2012/613595
45. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
46. Kruschke JK. Bayesian Analysis Reporting Guidelines. Nat Hum Behav. 2021;5(10):1282–1291. doi:10.1038/s41562-021-01177-7
47. van Doorn J, van den Bergh D, Böhm U, et al. The JASP guidelines for conducting and reporting a Bayesian analysis. Psychon Bull Rev. 2021;28(3):813–826. doi:10.3758/s13423-020-01798-5
48. Quintana DS, Williams DR. Bayesian alternatives for common null-hypothesis significance tests in psychiatry: a non-technical guide using JASP. BMC Psychiatry. 2018;18(1):178. doi:10.1186/s12888-018-1761-4
49. McInnes K, Friesen C, Boe S. Specific Brain Lesions Impair Explicit Motor Imagery Ability: a Systematic Review of the Evidence. Arch Phys Med Rehabil. 2016;97(3):478–489.e1. doi:10.1016/j.apmr.2015.07.012
50. Zeman A. Aphantasia and hyperphantasia: exploring imagery vividness extremes. Trends Cognitive Sci. 2024;28(5):467–480. doi:10.1016/j.tics.2024.02.007
51. Knudsen L, Santoro L, Bruehl S, Harden N, Brunner F. Subtypes of complex regional pain syndrome—a systematic review of the literature. Pain Rep. 2023;8(6):e1111. doi:10.1097/PR9.0000000000001111
52. Guillot A, Collet C, Nguyen VA, Malouin F, Richards C, Doyon J. Brain activity during visual versus kinesthetic imagery: an fMRI study. Hum Brain Mapp. 2009;30(7):2157–2172. doi:10.1002/hbm.20658
53. Lee WH, Kim E, Seo HG, et al. Target-oriented motor imagery for grasping action: different characteristics of brain activation between kinesthetic and visual imagery. Sci Rep. 2019;9(1):12770. doi:10.1038/s41598-019-49254-2
54. Yang YJ, Jeon EJ, Kim JS, Chung CK. Characterization of kinesthetic motor imagery compared with visual motor imageries. Sci Rep. 2021;11(1):3751. doi:10.1038/s41598-021-82241-0
55. Mibu A, Kan S, Nishigami T, Fujino Y, Shibata M. Performing the hand laterality judgement task does not necessarily require motor imagery. Sci Rep. 2020;10(1):5155. doi:10.1038/s41598-020-61937-9
56. Ten Brink AF, Bultitude JH. Predictors of Self-Reported Neglect-like Symptoms and Involuntary Movements in Complex Regional Pain Syndrome Compared to Other Chronic Limb Pain Conditions. Pain Med. 2021;22(10):2337–2349. doi:10.1093/pm/pnab226
57. Lundberg M, Archer KR. Fear of Movement: past, Present, and Future for Rehabilitation and Health. Phys Ther. 2022;102(2):pzac007. doi:10.1093/ptj/pzac007
58. Budnik-Przybylska D, Syty P, Kaźmierczak M, et al. Exploring the influence of personal factors on physiological responses to mental imagery in sport. Sci Rep. 2023;13(1):2628. doi:10.1038/s41598-023-29811-6
59. Bowering KJ, O’Connell NE, Tabor A, et al. The Effects of Graded Motor Imagery and Its Components on Chronic Pain: a Systematic Review and Meta-Analysis. J Pain. 2013;14(1):3–13. doi:10.1016/j.jpain.2012.09.007
60. Ruffino C, Papaxanthis C, Lebon F. Neural plasticity during motor learning with motor imagery practice: review and perspectives. Neuroscience. 2017;341:61–78. doi:10.1016/j.neuroscience.2016.11.023
61. Ten Brink AF, España MF, Navarro V, Dijkerman HC, Bultitude JH. Investigating Object Affordance in People with Complex Regional Pain Syndrome: no Alterations in the Automatic Activation of Motor Plans. J Pain. 2024;2024:S1526–5900(24)00353–5. doi:10.1016/j.jpain.2024.01.344
62. Cuenca-Martínez F, Reina-Varona Á, Castillo-García J, La Touche R, Angulo-Díaz-Parreño S, Suso-Martí L. Pain relief by movement representation strategies: an umbrella and mapping review with meta-meta-analysis of motor imagery, action observation and mirror therapy. Eur J Pain. 2022;26(2):284–309. doi:10.1002/ejp.1870
63. Thieme H, Morkisch N, Rietz C, Dohle C, Borgetto B. The Efficacy of Movement Representation Techniques for Treatment of Limb Pain—A Systematic Review and Meta-Analysis. J Pain. 2016;17(2):167–180. doi:10.1016/j.jpain.2015.10.015
64. Harris J, Hebert A. Utilization of motor imagery in upper limb rehabilitation: a systematic scoping review. Clin Rehabil. 2015;29(11):1092–1107. doi:10.1177/0269215514566248
65. Lee TH, Liu CH, Chen PC, Liou TH, Escorpizo R, Chen HC. Effectiveness of mental simulation practices after total knee arthroplasty in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2022;17(6):e0269296. doi:10.1371/journal.pone.0269296
66. Li R, Du J, Yang K, Wang X, Wang W. Effectiveness of motor imagery for improving functional performance after total knee arthroplasty: a systematic review with meta-analysis. J Orthopaedic Surg Res. 2022;17(1):65. doi:10.1186/s13018-022-02946-4
67. Kang Y, Trewern L, Jackman J. Chronic pain: supported self-management. BMJ. 2024;384:e072362. doi:10.1136/bmj-2022-072362
68. Nicholas MK, Blyth FM. Are Self-Management Strategies Effective in Chronic Pain Treatment? Pain Management. 2016;6(1):75–88. doi:10.2217/pmt.15.57
69. Lewis JS, Wallace CS, White P, et al. Early versus persistent Complex Regional Pain Syndrome: is there a difference in patient reported outcomes following rehabilitation? Eur J Pain. 2024;28(3):464–475. doi:10.1002/ejp.2196
70. Moseley GL, Zalucki N, Birklein F, Marinus J, van Hilten JJ, Luomajoki H. Thinking about movement hurts: the effect of motor imagery on pain and swelling in people with chronic arm pain. Arthritis Rheum. 2008;59(5):623–631. doi:10.1002/art.23580
71. Moseley GL. Is successful rehabilitation of complex regional pain syndrome due to sustained attention to the affected limb? A randomised clinical trial. Pain. 2005;114(1):54–61. doi:10.1016/j.pain.2004.11.024
72. Méndez-Rebolledo G, Gatica-Rojas V, Torres-Cueco R, Albornoz-Verdugo M, Guzmán-Muñoz E. Update on the effects of graded motor imagery and mirror therapy on complex regional pain syndrome type 1: a systematic review. J Back Musculoskelet Rehabil. 2017;30(3):441–449. doi:10.3233/BMR-150500
73. Kantak SS, Johnson T, Zarzycki R. Linking Pain and Motor Control: conceptualization of Movement Deficits in Patients With Painful Conditions. Phys Ther. 2022;102(4):pzab289. doi:10.1093/ptj/pzab289
74. Punt DT, Cooper L, Hey M, Johnson MI. Neglect-like symptoms in complex regional pain syndrome: learned nonuse by another name? PAIN. 2013;154(2):200. doi:10.1016/j.pain.2012.11.006
75. Mangnus TJP, Dirckx M, Huygen FJPM. Different Types of Pain in Complex Regional Pain Syndrome Require a Personalized Treatment Strategy. J Pain Res. 2023;16:4379–4391. doi:10.2147/JPR.S432209
76. Prego-Domínguez J, Khazaeipour Z, Mallah N, Takkouche B. Socioeconomic status and occurrence of chronic pain: a meta-analysis. Rheumatology. 2021;60(3):1091–1105. doi:10.1093/rheumatology/keaa758
77. Strauss S, Barby S, Härtner J, et al. Graded motor imagery modifies movement pain, cortical excitability and sensorimotor function in complex regional pain syndrome. Brain Commun. 2021;3(4):fcab216. doi:10.1093/braincomms/fcab216
78. Diers M. Neuroimaging the pain network - Implications for treatment. Best Pract Res Clin Rheumatol. 2019;33(3):101418. doi:10.1016/j.berh.2019.05.003
79. Simula AS, Malmivaara A, Booth N, Karppinen J. A classification-based approach to low back pain in primary care - protocol for a benchmarking controlled trial. BMC Fam Pract. 2020;21(1):61. doi:10.1186/s12875-020-01135-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Cognitive Behavioral Therapy Psychological Interventions May Not Make the Difference in Children and Adolescents With Chronic Pain
Perlman L, Malka N, Terry O, Nguyen A, Guimarães Ferreira Fonseca L, Ingelmo JI, Ingelmo P
Journal of Pain Research 2025, 18:1451-1464
Published Date: 20 March 2025