")
Back to Journals » Journal of Pain Research » Volume 18
Exploration of the Application Rules and Clinical Significance of Acupoints in Acupuncture Treatment of Migraine Based on Data Mining
Authors He Y , Wang X, Liu M, Li L, Han T, Wu Y, Li X
Received 1 April 2025
Accepted for publication 10 June 2025
Published 18 June 2025 Volume 2025:18 Pages 3049—3067
DOI https://doi.org/10.2147/JPR.S527987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yujun He,* Xiaoyi Wang,* Minhui Liu,* Lu Li, Tingfen Han, Yachao Wu, Xiaojun Li
Department of Traditional Chinese Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaojun Li, Department of Traditional Chinese Medicine, Taizhou Hospital of Zhejiang Province, 150 Ximen Street, Linhai City, Taizhou, Zhejiang, 317000, People’s Republic of China, Email [email protected]
Background: Abundant clinical investigations have attested to the efficacy of acupuncture in treating migraines. However, as each acupoint elicits distinct analgesic pathways and acupuncturists vary in their acupoint selection, there is currently an absence of evidence-based guidance for determining the optimal acupoint selection.
Objective: The aim of this study was to conduct an initial comprehensive data mining analysis to identify the most effective acupoints and their combinations for migraine treatment.
Methods: A comprehensive search was carried out in eight electronic bibliographic databases (PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure, Wanfang Database, Chinese Biomedical Literature Database, and Chongqing VIP Database) from their inception up to May 2025. Studies evaluating the effectiveness of acupuncture in treating migraines were selected. The literature was rigorously evaluated according to predefined inclusion and exclusion criteria, and relevant data were then extracted for analysis. Excel 2021 was used for descriptive statistical analysis. Association rule analysis was performed using SPSS Modeler 14.1. Exploratory factor analysis, cluster analysis, and decision tree analysis were conducted using SPSS Statistics 26.0.
Results: A total of 911 trials were identified, from which 1610 groups of effective prescriptions involving 181 acupoints were extracted. The most commonly used acupoints were Feng-chi (GB20), Tai-yang (EX-HN5), Shuai-gu (GB8), Bai-hui (GV20), and He-gu (LI4). The gallbladder meridian was the most frequently utilized meridian. Specific points, mainly crossing points, were predominantly used, with head and neck acupoints being the most common. The combination of “Feng-chi (GB20), Tai-yang (EX-HN5), and Shuai-gu (GB8)” was frequently used as the core acupoints group. Additionally, several acupoint combinations were obtained through exploratory factor analysis, cluster analysis, and decision tree analysis.
Conclusion: This research provides evidence-based support for the effectiveness of acupoint selection in migraine treatment and offers potential therapeutic recommendations, thereby facilitating collaborative decision-making between healthcare providers and patients.
Keywords: acupuncture, migraine, data mining, acupoint application rules
A Letter to the Editor has been published for this article.
Introduction
Migraine, encompassing migraine without aura, migraine with aura, and chronic migraine, is a globally prevalent neurological disorder.1,2 It is a disabling condition marked by recurrent episodes that exert a notable impact on an individual’s overall well-being.2 Migraine attacks typically manifest with symptoms like nausea, vomiting, and heightened sensitivity to light and sound. These symptoms severely disrupt an individual’s daily life, including personal, social, and work aspects, and ultimately affect their quality of life.3–5 In the general population, the prevalence of migraine is 12%, and females are three times more likely to experience it than males.6 Moreover, this condition is more common among individuals aged between 30 and 40.7 The American Migraine Prevalence and Prevention Study revealed that in the United States, the average annual direct cost per person for episodic migraines was $1757.8 Migraine significantly influences an individual’s well-being and quality of life, often leading to substantial impairment. Migraine episodes limit normal activities by up to 78% in those suffering from migraines.9 Due to its wide occurrence and significant health impact, migraine is an important condition worthy of research.1 Currently, the pharmacological preventive treatments for migraine involve beta blockers, calcium channel blockers, angiotensin - II receptor antagonists, anti - epileptic drugs, and antidepressants.10,11 However, the effectiveness of these therapies seems to be of moderate level, with response rates ranging approximately from 40% to 50%.12
Acupuncture has been extensively applied globally for treating headaches, especially migraines.13 Prior research indicates that acupuncture is an effective approach for treating and preventing migraines.14,15 Its mechanism of action might involve the suppression of meningeal vasodilation and inflammatory factors, along with the alleviation of neurogenic inflammation.14 Nevertheless, in numerous clinical studies, there has been a lack of uniformity in the selection of acupoints for migraine treatment. The choice of acupoints can vary according to the diverse perspectives and experiences of medical practitioners. The selection and combination of acupoints are regarded as the core elements of the acupuncture therapy system.16 In clinical practice, acupuncturists often combine multiple acupoints to optimize the interaction among them and enhance the effectiveness of acupuncture treatment. The increasing prevalence of effective acupuncture treatments for migraines mainly relies on the use of multi - acupoint prescriptions. The efficacy of these prescriptions is closely related to the compatibility of meridians and acupoints, resulting in a complex, conflicting, and ambiguous relationship. Thus, it is of great significance to utilize the existing data to explore the principles of acupoint selection and combination, aiming to improve the effectiveness of acupuncture treatment. Data mining technology allows for the identification and extraction of valuable information and knowledge from a vast amount of literature.17 The author and his research team have adopted this method to investigate the selection and combination of acupoints in acupuncture treatment for various pain - related conditions. These conditions include, but are not restricted to, carpal tunnel syndrome,18,19 piriformis syndrome,20,21 benign prostatic hyperplasia,22 neurogenic bladder,23 and metabolism - associated fatty liver disease.24 These studies have provided evidence that there is a distinct relationship between the acupoints of different meridians, and the success of acupuncture hinges on the appropriate selection and combination of these acupoints. Therefore, it is essential to ascertain the characteristics and principles governing the selection and combination of acupoints for migraine treatment, so as to offer guidance for future research and clinical practice. The objective of this study is to explore the correlation patterns of acupoints using data mining techniques and formulate a standardized treatment guideline for the application of acupoints in migraine treatment. Our research protocol has been published in the Journal of Pain Research.25
Methods and Analysis
Search Methods
An extensive search was conducted across both Chinese and English digital libraries, covering the period from their establishment up to May 2025. The databases searched included PubMed, Embase, Cochrane Library, Web of Science (WOS), China National Knowledge Infrastructure (CNKI), Wanfang Database, Chinese Biomedical Literature Database (CBM), and Chongqing VIP Database (VIP). The language scope was restricted to Chinese and English. The search terms used in this study were a combination of medical subject headings and free - text terms. As an illustration, Table 1 presents the search strategy for PubMed. This search approach was adjusted to meet the specific requirements and unique features of each database. Search strategies for other databases are shown in Supplemental Tables 1–7
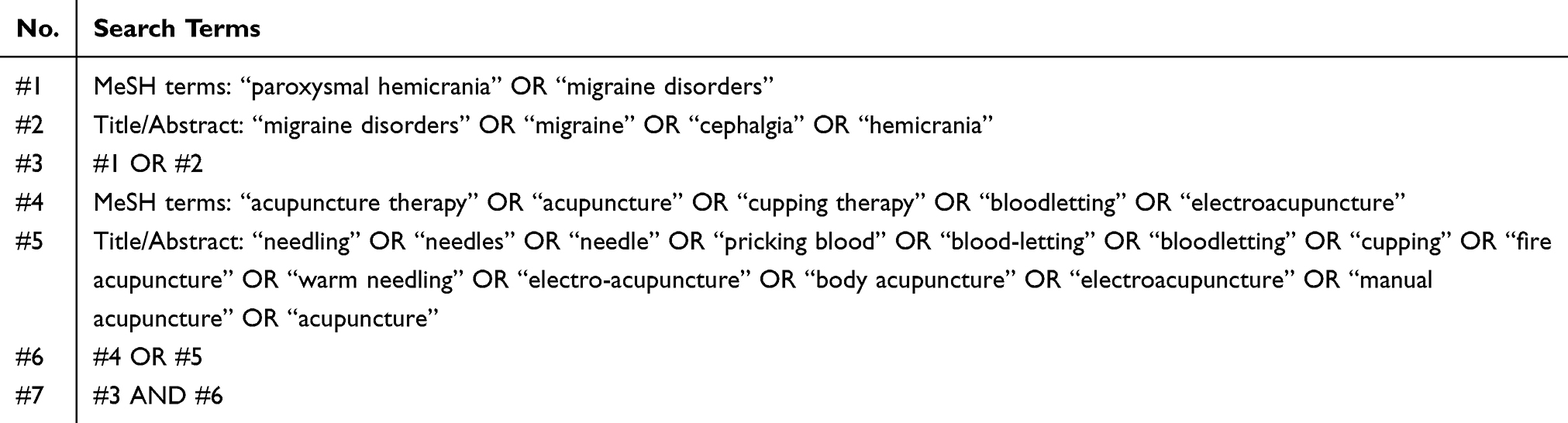 |
Table 1 Search Strategy for PubMed Database |
Review Process
Data Screening
The inclusion criteria were as follows: (1) Studies mainly focusing on acupuncture therapy as the main intervention, irrespective of whether randomised and/or controlled methods were utilized. (2) Each group or trial should involve at least ten patients. (3) Patients were diagnosed with migraine according to the diagnostic criteria established and applied in the clinical studies during that particular period. (4) Meridian points, extra points, or ashi points were used for needle insertion or moxibustion. This could be used alone or in combination with other therapies like acupuncture and/or moxibustion (for example, in combination with Chinese herbal medicine). (5) The analysis covered trials comparing different acupuncture methods for migraine treatment. (6) Only the most recent article by the same first author was included.
The studies excluded according to the exclusion criteria were: (1) Reviews, protocols, animal experiments, case reports, systematic reviews, meta - analyses, and other non - clinical experimental articles. (2) Articles that had not been rigorously and comprehensively evaluated by subject - matter experts, such as theses, conference papers, and similar works. (3) Trials involving microacupuncture systems, ear needle, head needle, wrist and ankle needle, and other non - body needle techniques were excluded as they were not related to traditional acupoints. (4) Trials that only presented physiological or laboratory data were excluded. (5) In controlled trials, studies were excluded if acupuncture therapy, either as a sole treatment or in combination with other therapies, showed less beneficial effects for patients compared to the control group. (6) The acupoint prescription in the trial was considered invalid if it was either incomplete or non - existent.
Data Collection
Yujun He and Tingfen Han assessed all the titles and abstracts obtained from the literature search and excluded those that were evidently unrelated, like research centered on reviews, animal experiments, case reports, and related topics. All the remaining literature was collected and then underwent an additional round of scrutiny to eliminate any non - relevant publications. Subsequently, Yujun He, Minhui Liu, and Yachao Wu evaluated the eligibility of all the remaining publications in accordance with the pre - determined inclusion criteria. As noted by the third author, Xiaojun Li, discussions were employed to resolve any issues.
Establishing a Database and Processing Data Normalization
The literature retrieved from the search was imported into the document manager Endnote×9.2. Two researchers (Xiaoyi Wang and Lu Li) meticulously and objectively reviewed the literature, strictly following the predefined inclusion and exclusion criteria. Before further processing, Endnote was first used to eliminate duplicate entries, and then a manual check was carried out to remove any remaining duplicates by Xiaoyi Wang and Lu Li. Subsequently, the results were verified to ensure the accuracy of the included content.
The obtained data was loaded into Excel 2021 to create a database specifically for acupuncture treatments of migraines. An approach of combining primary and secondary acupoints to form acupoint prescriptions was adopted to generate effective prescriptions.26 Regarding the “Study of Meridians and Collaterals”27 and the latest national standards,28,29 we standardized the names of acupoints listed in the literature and established a unified naming rule for them. Additionally, we added more details regarding the relevant meridians, locations, and specific acupoint characteristics associated with each acupoint.
Data Management for Missing Data
To evaluate the data in accordance with the intention - to - treat principle, attempts were made to contact the original authors to obtain any crucial information that was lacking. In cases where comprehensive data was unavailable, only the currently accessible data was evaluated.
Data Analysis
Literature Quality Control
First, an initial assessment of all the written materials was conducted to verify the information. Subsequently, the data was processed following the established procedures, and the input personnel carried out a secondary assessment. The expert group provided evaluations on whether the doubtful contents should be incorporated. Finally, a comprehensive evaluation by expert staff was performed to ensure the reliability of the literature information.23,24
Descriptive Statistics
The acupoint prescriptions recorded in the literature were input into a table in Excel 2021. This table was used to generate a PivotTable, enabling descriptive statistical analysis of multiple aspects. These aspects encompassed the frequency of acupoint utilization, the meridians they pertained to, the locations of the points, and the specific acupoint characteristics of each acupoint.
High-Frequency Acupoints Analysis
According to Price’s law, high - frequency acupoints can be identified by the formula M=0.749(Pmax)1/2, where M represents the maximum frequency of the acupoint.30 In the event that the number of high - frequency acupoints determined by this method exceeds a threshold of 50 (n≥50), an alternative approach will be adopted. Calculate the average frequency of acupoints (X), where X is obtained by dividing the total frequency by the total number of acupoints. Acupoints with a frequency greater than or equal to X are categorised as high - frequency acupoints.31 A bar graph was utilised to display the top 10 most frequently used acupoints.
Association Rule Analysis
SPSS Modeler 14.1 software was employed to conduct an analysis of the association rules among high - frequency acupoints. The Apriori algorithm was utilized for this analysis. The support level represented the probability of both the antecedent and the consequent occurring, while the confidence level denoted the probability of the consequent appearing after the antecedent had already emerged. After carrying out multiple experiments, the optimal and minimum thresholds for support and confidence were established. The maximum value for the former (support) was set at 2. Subsequently, a detailed network graph was created to analyze the correlations among the acupoints.
Exploratory Factor Analysis
Exploratory factor analysis was carried out on the high - frequency acupoints using SPSS Statistics 26.0. Moreover, the prescription data were subjected to Kaiser - Meyer - Olkin (KMO) and Bartlett’s test of sphericity. Factor analysis was conducted when the KMO value was above 0.5 and the p - value (P) was less than 0.05. The main factor components were determined through maximum variance rotation. However, factor analysis was inappropriate when the KMO value was less than 0.5 or the P value was greater than 0.05.
Cluster Analysis
Cluster analysis was performed on the high - frequency acupoints using SPSS Statistics 26.0. The resulting cluster analysis dendrogram was utilised to explore the clustering relationships among the acupoints.
Decision Tree Analysis
Acupoints were analyzed using the CHAID algorithm in SPSS Statistics 26.0 software, with the application of a decision tree model. The objective was to identify the most efficient treatment strategy for migraine by minimizing the number of required acupoints. The CHAID growth method is suitable for binary variables. Specifically, the acupoint data types can be categorized as either “1” (indicating use) or “0” (indicating non - use).
Results
Eligible Studies
A total of 17074 relevant articles were found, including 3355 from CNKI, 3509 from VIP, 3035 from Wanfang, 2870 from CBM, 839 from PubMed, 2,038 from Embase, 26 from Cochrane Library, and 1402 from WOS. Out of these, 10550 duplicate studies were excluded. Subsequently, we assessed the titles and abstracts of the remaining 6524 papers in order to select 1770 that may potentially be considered as candidates. After thoroughly reviewing the complete texts, a total of 911 papers were selected for inclusion, whereas 859 publications were discarded (Figure 1) (The information of the included literatures can be found in the Supplementary Table 8).
 |
Figure 1 Flow diagram of the study selection process. |
Frequency of Acupoint Analysis
In total, 1610 prescriptions (Supplementary Table 9) were identified, which consisted of 181 acupoints, with an aggregate frequency of 10825. The five most frequently used acupoints were Feng - chi (GB20), Tai - yang (EX - HN5), Shuai - gu (GB8), Bai - hui (GV20), and He - gu (LI4) (Table 2 and Figure 2). Feng - chi (GB20) was the most commonly utilized acupoint, with 1171 occurrences, accounting for 10.82% of all acupoint usages. According to Price’s law, for high - frequency acupoints, M=0.749*(1171)1/2 ≈25.63, Thus, acupoints with a frequency of ≥ 26 could initially be considered as high - frequency acupoints. However, as per Table 1, 56 high - frequency acupoints were obtained in this manner, exceeding 50. Consequently, an alternative method was adopted to calculate high - frequency acupoints. X=10825/181 ≈59.81, Therefore, acupoints with a frequency of ≥ 60 were regarded as high - frequency acupoints. This included a total of 35 high - frequency acupoints ranging from GB20 to GV23.
 |
Table 2 Frequency of Acupoint Application for Migraine Treatment |
 |
Figure 2 High-frequency of acupoint application for migraine treatment. |
Frequency of Meridian Analysis
The investigation into meridian application provided significant insights into the distribution of selected acupoints. This encompassed the frequency and proportion of acupoints on each meridian, the number and proportion of used acupoints, as well as the frequency of each individual acupoint. The results demonstrated that the gallbladder meridian was the most frequently employed, with a total of 3405 instances (31.45%). The second most commonly used was the category of extra points or ashi points, with 1597 occurrences, representing 14.75% of the total. In contrast, the frequencies of other meridians were considerably lower. The gallbladder meridian had the largest number of acupoints, amounting to 32 (17.68%) (Table 3).
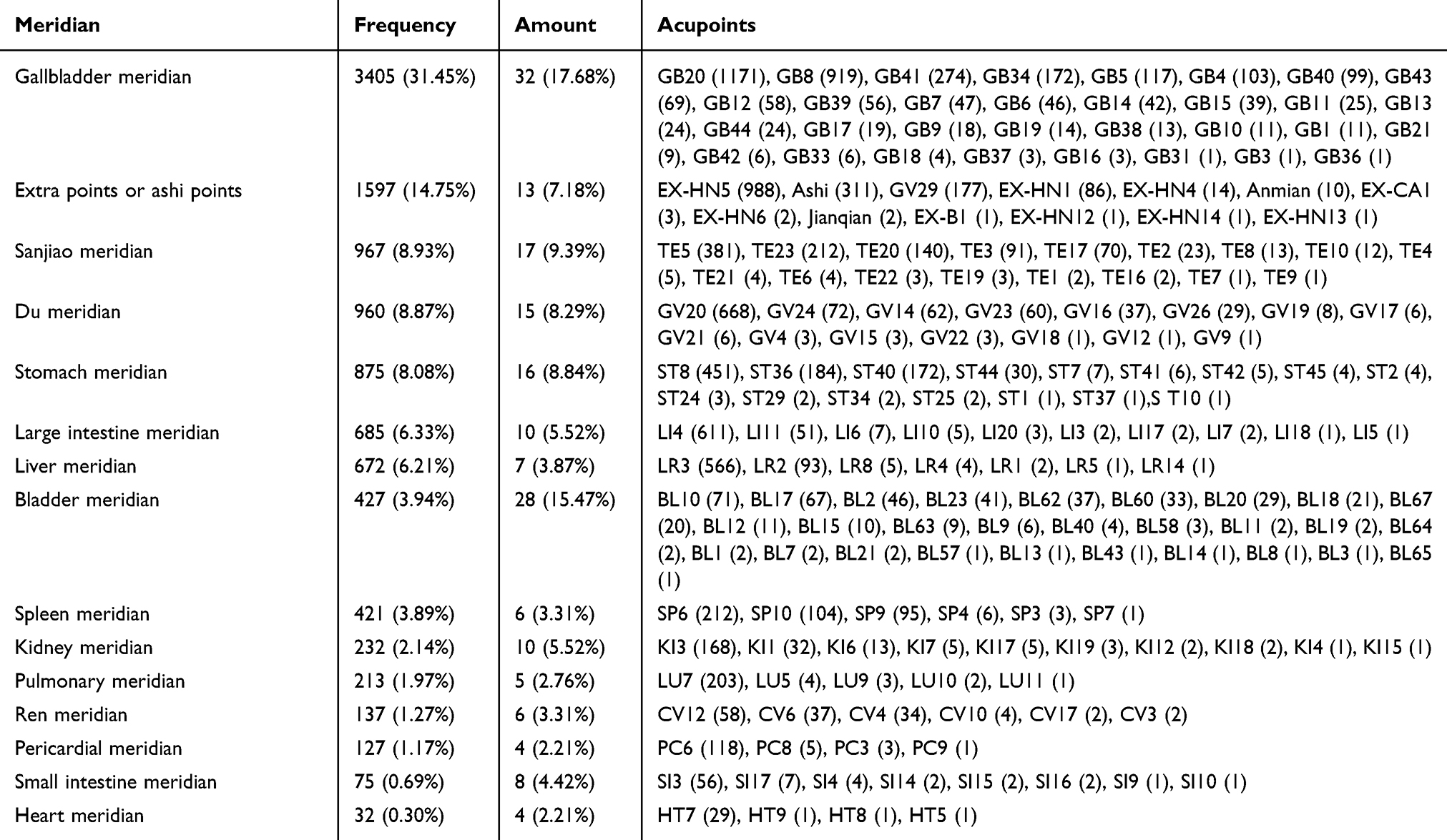 |
Table 3 Frequency of Meridian Application for Migraine Treatment |
Distribution of Acupoint Analysis
The analysis of acupoint distribution showed that acupoints in the head and neck area were used most frequently. There were a total of 6270 usages, which accounted for 57.92% of the overall count. These acupoints numbered 67, constituting 37.02% of the total. The frequencies and quantities of acupoints in other locations were relatively lower. The head and neck region had the highest number of acupoints, with 67 acupoints, which made up 17.68% of the total (Table 4).
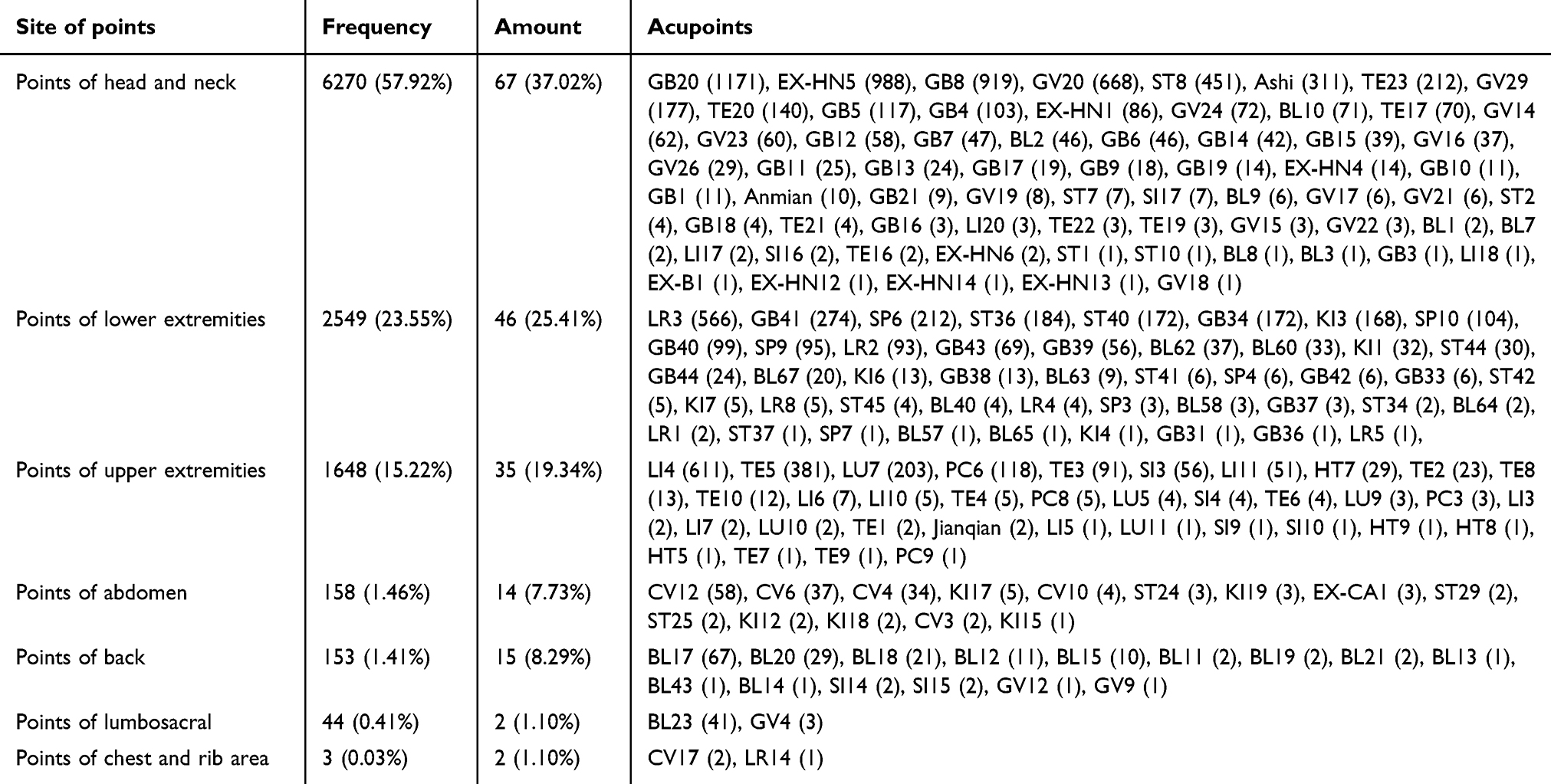 |
Table 4 Frequency of Site of Points Application for Migraine Treatment |
Frequency of Specific Acupoints Analysis
The exploration of specific acupoints clearly presented the frequency, quantity, and diversity of acupoints used in acupuncture prescriptions. Specifically, among the total 181 acupoints, 108 were explicitly recognised as specific acupoints. Some acupoints possessed multiple specific acupoint identities. The majority of the utilised specific acupoints were crossing points, with a frequency of 4185 occurrences (39.35%). Nevertheless, in terms of the number of acupoints, the five shu points had the largest count, amounting to 41 acupoints (31.30%) (Table 5).
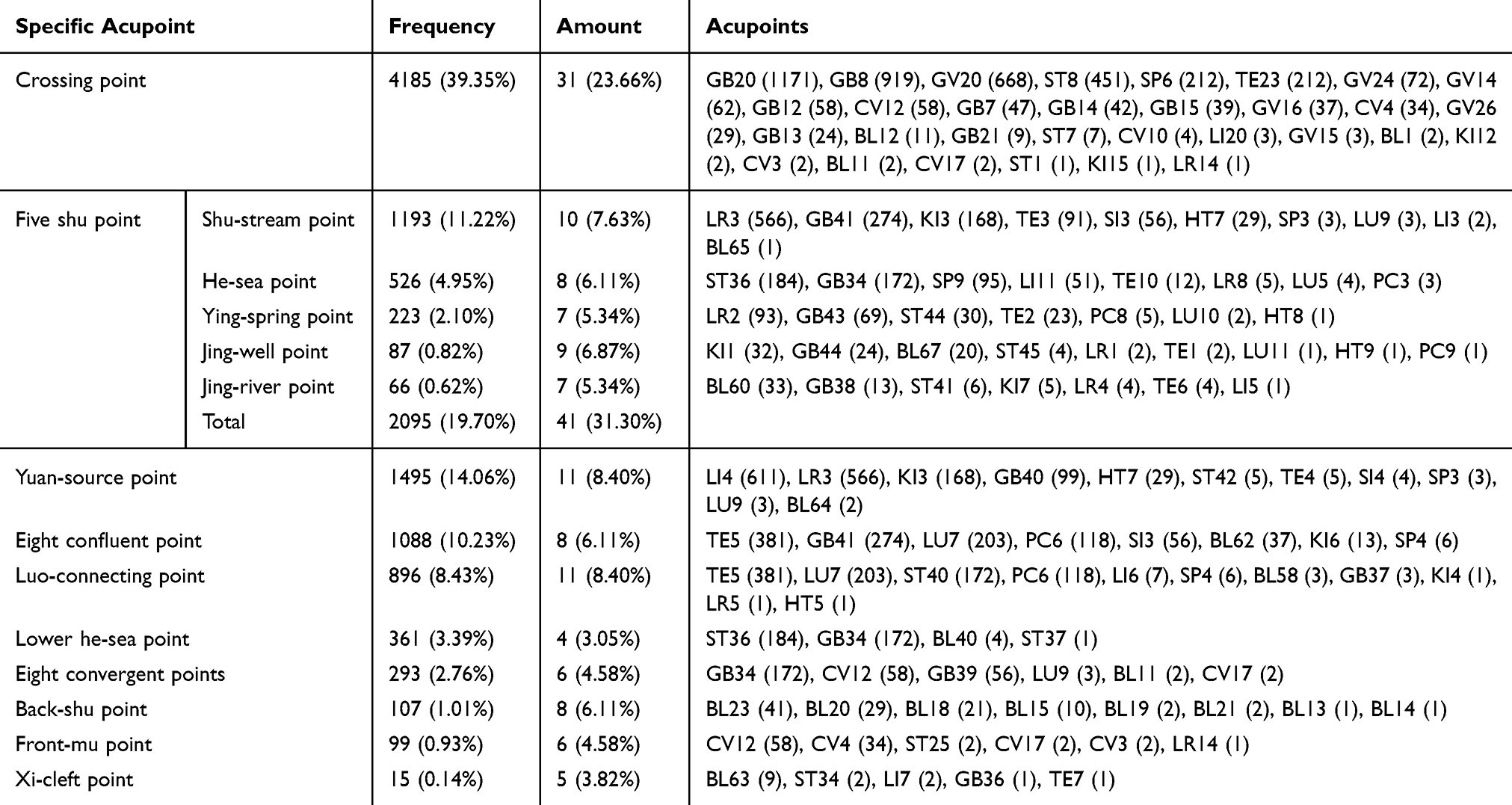 |
Table 5 Frequency of Specific Acupoints for Migraine Treatment |
Association Rule Analysis
The acupoints involved in the analysis were subjected to an association rule analysis using SPSS Modeler 14.1 software. After performing numerous experiments, it was determined that setting a minimum support threshold of 15% and a minimum confidence threshold of 80% yielded the best outcomes. According to the defined criteria, a comprehensive analysis was carried out on a total of 20 sets of acupoints that met the given conditions (Table 6). The acupoint combinations with the highest support were [Tai - yang (EX - HN5)] - [Feng - chi (GB20)], [Shuai - gu (GB8)] - [Feng - chi (GB20)], [Bai - hui (GV20)] - [Feng - chi (GB20)], [Shuai - gu GB8, Tai - yang EX - HN5] - [Feng - chi (GB20)], and [Tou - wei (ST8)] - [Tai - yang (EX - HN5)] (Table 6). Figure 3 illustrated a complex network structure, indicating that the core group was composed of “Feng - chi (GB20), Tai - yang (EX - HN5), and Shuai - gu (GB8)”.
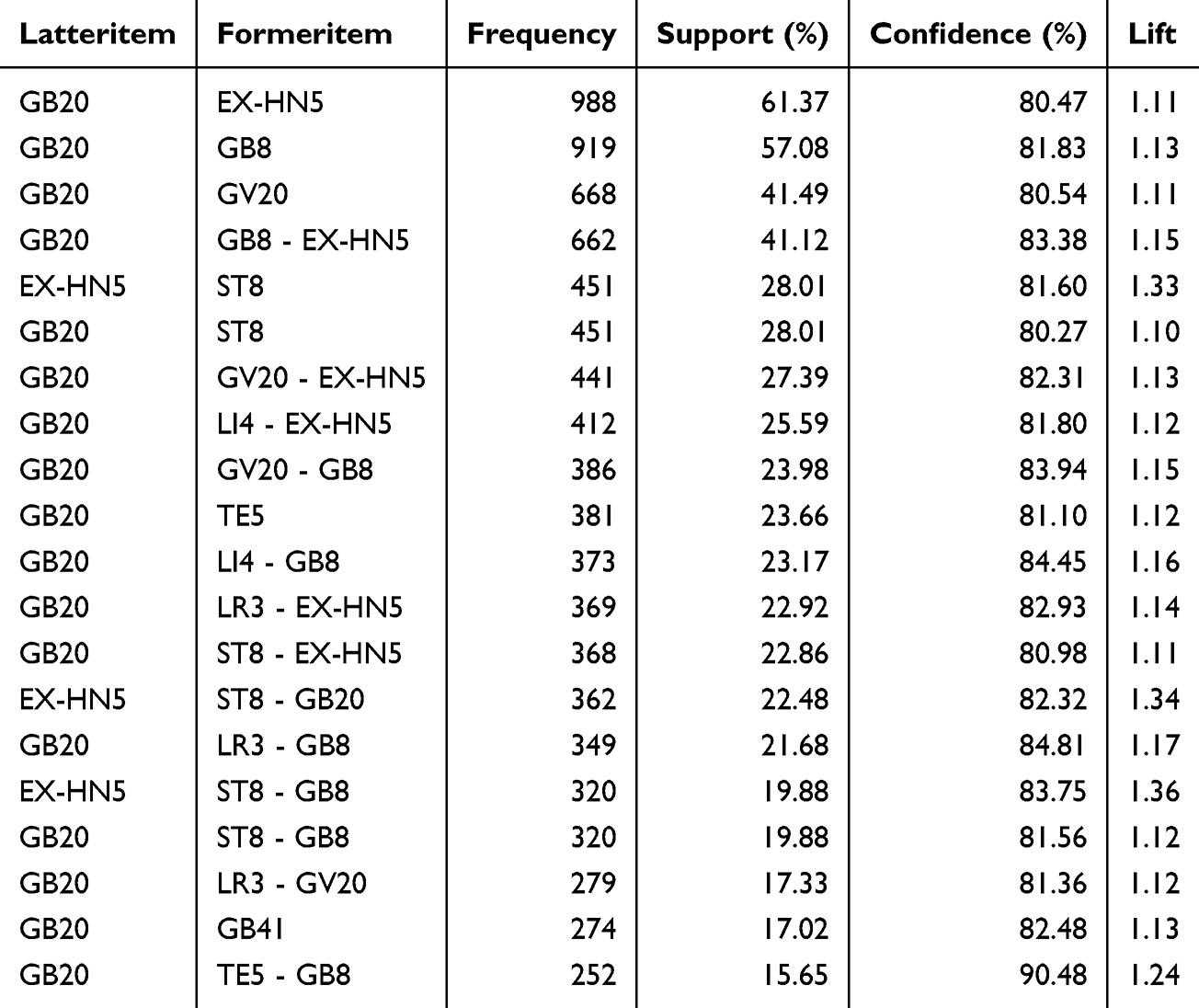 |
Table 6 Association Rules of Acupoints for Migraine Treatment |
 |
Figure 3 Core acupoint network of acupuncture treatment for migraine. |
Exploratory Factor Analysis
Exploratory factor analysis of high - frequency acupoints was carried out using the statistical software IBM SPSS Statistics 26.0. The results of the KMO and Bartlett’s test of sphericity demonstrated that exploratory factor analysis was suitable (KMO = 0.551, P < 0.001). A principal component analysis was performed, and 15 common factors with eigenvalues greater than 1 were extracted from the scree plot (Figure 4). The cumulative variance contribution rate of the extracted common components was 59.78%, indicating strong explanatory power and the capacity to represent a substantial part of the original information. After applying orthogonal rotation with Kaiser normalization, the factor loadings were calculated. Acupoints with an absolute value of the load coefficient greater than 0.5 were selected and included in the common factor extraction table (Table 7). Meanwhile, the rotated space - load diagram was obtained (Figure 5). The spatial position in the space - load diagram can be used as an indication of the correlation between acupoints.
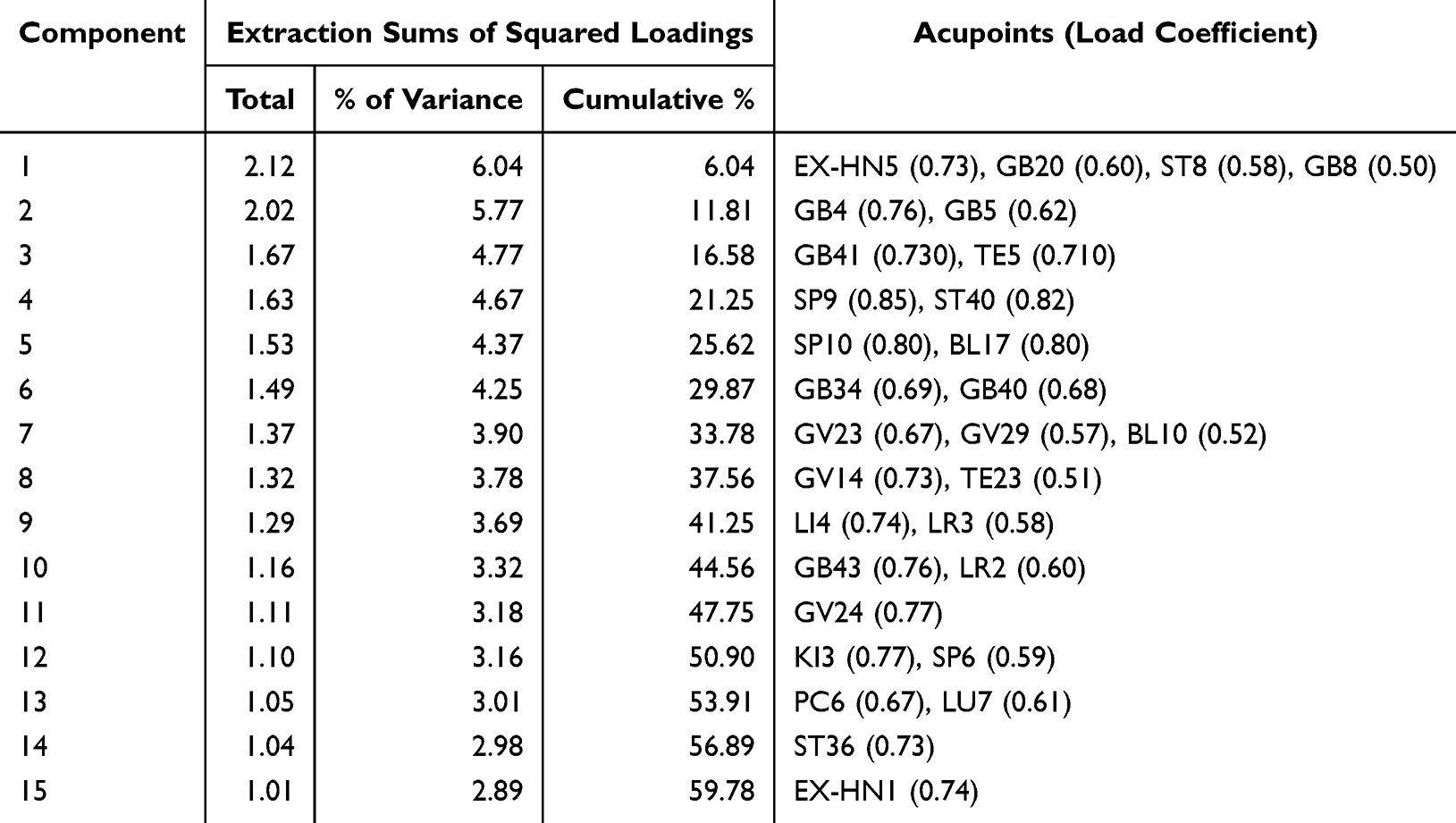 |
Table 7 Common Factor Extraction |
 |
Figure 4 Gravel map of common factor extraction of acupuncture treatment for migraine. |
 |
Figure 5 Space load diagram after rotation of acupuncture treatment for migraine. |
Cluster Analysis
The IBM SPSS Statistics 26.0 software was employed to perform cluster analysis, specifically concentrating on high - frequency acupoints. The results are presented in a dendrogram, which is a graphical representation utilised for clustering analysis. By means of a clustering method, the high - frequency acupoints were grouped into 9 main clusters according to the distance scale denoted by the red line in Figure 6. The resultant clusters are shown in Table 8.
 |
Table 8 Cluster Extraction |
 |
Figure 6 Tree chart of the cluster analysis of acupuncture for migraine. |
Decision Tree Analysis
Decision tree analysis was carried out with Feng - chi (GB20), which had the highest frequency, serving as the root node. The values 1171 and 72.7% at the root node signify the utilization frequency of Feng - chi (GB20) and its proportion within the 1610 acupoint prescriptions, respectively. The most appropriate acupoint at a lower level corresponded to Shuai - gu (GB8). When the value of Shuai - gu (GB8) was 1, the decision path selected node 2. In this node, the frequency of Feng - chi (GB20) in the prescription containing Shuai - gu (GB8) was represented by the values 752 and 81.8% respectively. All the nodes beneath the acupoint Wai - guan (TE5) were terminal nodes, and further matching was carried out at a lower level to achieve optimal results. At this point, the course no longer corresponded, and the prescription was selected as “GB20 - GB8 - TE5”. When the value of Shuai - gu (GB8) was 0, the decision path chose node 1, and the most suitable acupoint at a lower level corresponded to Tai - yang (EX - HN5). The values 419 and 60.6% in node 1 denoted the frequency and percentage of Feng - chi (GB20) in prescriptions that did not contain Shuai - gu (GB8) but did contain Tai - yang (EX - HN5), respectively. When Tai - yang (EX - HN5) had a value of 1, it triggered the selection of node 4, which corresponded to the lower - level optimal acupoint Bai - hui (GV20). The values 243 and 74.5% in node 4 represented the frequency and percentage of Tai - yang (EX - HN5) in prescriptions that also included Bai - hui (GV20), respectively. Subsequently, there were no more acupoints that were more effective at a lower level. The acupoint - matching process ceased, resulting in the prescription “GB20 - EX - HN5 - GV20”. By following the same procedure, one could also obtain acupoint prescriptions such as “GB20 - GB8 - TE23” and “GB20 - GV20” (Figure 7).
 |
Figure 7 Decision tree analysis of acupuncture for migraine. |
Discussion
Migraine represents a common type of chronic pain that affects a billion people worldwide, causing impairment for hours or even days.32 In recent years, progress has been made in migraine treatments, including non - pharmacological methods. These therapies can be used alone, in combination with medications, or along with other non - pharmacologic treatments, providing more options for those who cannot tolerate or respond to medications, or prefer to avoid them.33 Despite the recent developments in calcitonin gene - related peptide - targeted therapies, many migraine sufferers still do not obtain satisfactory headache relief from the existing treatments. Thus, there is a need for effective and well - tolerated therapies specifically designed for migraines. It is crucial to explore medications that are not only more effective and safer but also have substantial data to support their capacity to regulate migraine pathways.34
Acupuncture has shown effectiveness in clinical trials for migraine treatment.35 It has been integrated into multiple guidelines for treating migraines.36,37 Since 2008, the domain of acupuncture for migraines has advanced.38 Research consistently indicates that acupuncture offers notable benefits for migraines. It can reduce the intensity, duration, and frequency of headaches, and also decrease the dependence on acute medications. Randomized controlled trials have provided data regarding both the immediate and long - term effects of acupuncture. In line with traditional Chinese medical theory, acupoints located near a particular area of concern are considered to relieve the associated discomfort. Scalp acupoints are frequently applied in clinical practice for treating migraines.39 These acupoints are thought to directly stimulate and modulate the corresponding areas of the brain’s cortex and their blood circulation.40 They might also influence the trigeminal nerve, which is associated with migraines.41 However, not just scalp acupoints can impact migraines; acupoints located elsewhere on the body can as well. These acupoints may affect migraines via different mechanisms.35 For instance, acupuncture near ST36 can raise the concentration of extracellular adenosine, a substance possessing neuroprotective, anti - inflammatory, and analgesic properties.42 Hence, different acupoints can relieve migraines through diverse pathways. It is essential to utilize scientific approaches to identify the most effective selection and combinations of acupoints.
This study employed data mining techniques to investigate the correlations among acupoints utilised in the treatment of migraine. The acupoints most frequently utilised for treating migraines, listed in descending order, are Feng-chi (GB20), Tai-yang (EX-HN5), Shuai-gu (GB8), Bai-hui (GV20), and He-gu (LI4). Studies have shown that the effects of these acupoints on migraine may be related to microglia-mediated neuroinflammation,43,44 microglial activation, microglia-neuron interaction,45 mitochondrial restoration,46 and so on.
The gallbladder meridian was the most commonly utilised meridian. The gallbladder meridian mostly runs along the lateral aspect of the cranium, coinciding with a frequently affected area in cases of migraine discomfort. For the site, acupoints in the head and neck area were most commonly used, which was related to the site of headache onset. Regarding specific acupoints, the utilisation frequency of crossing acupoints surpasses that of other types of specific acupoints. A crossing point is an acupoint where two or more meridians intersect. Hence, the crossing point has the ability to effectively address ailments resulting from damage in numerous meridians, including those impacted by migraines.
Through the examination of association rules, we have identified 20 sets of acupoint combinations that exhibit high levels of support and confidence. Simultaneously, we identified the core acupoint group “ Feng-chi (GB20), Tai-yang (EX-HN5) and Shuai-gu (GB8)” based on the complex network diagram. We utilised exploratory factor analysis and cluster analysis to derive 15 components and 9 cluster groups, respectively. When treating patients, these combinations of acupoints can be chosen based on the individual’s particular condition and symptoms. For instance, if the patient is experiencing migraine due to the presence of phlegm dampness, they can opt for the cluster 1 or factor 4 acupoint group that has the ability to dispel phlegm and dampness. Alternatively, if the migraine is caused by blood stasis, the patient can select either the factor 5 acupoint group or the clustered 3 acupoint group, both of which promote blood circulation and eliminate blood stasis. If the patient is experiencing migraines due to excessive activity of liver yang, they have the option to select either a factor 10 acupoint group or a cluster 7 acupoint group that possesses a soothing impact on the liver and latent yang.
Using decision tree analysis, we derived four different combinations of acupoint prescriptions. Prescription 1 “GB20 - GB8 - TE5” chooses certain acupuncture points along the Shaoyang meridian and combines both local and distal point selection to effectively regulate the functioning of the Shaoyang meridian. The second prescription is “GB20 - EX-HN5 - GV20”, which addresses both moderate pain in the upper part of the head and discomfort in the neck. Prescription 3 “GB8 - TE23” involves the simultaneous selection of local acupoints and the stimulation of the hand and foot Shaoyang meridians, with the aim of regulating both Shaoyang meridians. The prescription labelled “GB20 - GV20” is appropriate for individuals experiencing pain in the cranial region, as well as those with a deficiency in qi.
Data mining, a promising and practical approach, was employed to analyze the fundamental principles. It uses algorithms to find correlations between data points, measure item frequencies in the database, and identify links.47 The characteristics of each data mining method have been described in detail in our research protocol.25 By descriptive statistical analysis, we can find commonly used acupoints, meridians, locations, and specific acupoints for migraines. Association rule mining, a data mining technique, uses rule - based machine learning to find relationships in a dataset and create rules. The Apriori algorithm is one such algorithm for identifying frequent item sets in a database.48–51 Exploratory factor analysis reveals the underlying structure of variables and their correlations, aiming to find a scale’s potential structure and reduce item number by identifying redundant variables.52,53 Clustering analysis groups similar objects in data to understand data organization and simplify information.54,55 Decision tree analysis helps understand data structure and simplify complex information from large datasets. It makes decisions by iterative categorization of a hierarchical framework, using index factors to encode data and classify geographical characteristics. Each path from the main to end node represents a classification rule.56,57 Different data mining methods have their own pros and cons. We used the results of various data mining techniques to provide multiple references. This determined the optimal acupoint selection and combinations for migraines, offering evidence - based guidance for clinical practice.
Limitations
Our study had several limitations. Different data mining techniques have their own advantages and disadvantages, which led to differences in the results they generated. The optimal integration of these results, which needs to be verified by further clinical research, could potentially produce better outcomes. Additionally, the specific mechanisms by which acupoint combinations treat migraines remain unclear. Moreover, relying mainly on rating scales like the VAS score to evaluate the effectiveness of this condition may lead to biased results due to their subjective nature. Besides, literature in languages other than Chinese and English, as well as grey literature, were not included, which might introduce bias. Finally, the lack of consistency in research data prevented some studies from providing accurate acupuncture information regarding the specific duration, frequency, and intensity of stimulation.
Conclusion
Acupoints such as Feng - chi (GB20), Tai - yang (EX - HN5), Shuai - gu (GB8), Bai - hui (GV20), and He - gu (LI4) were frequently used in migraine treatment. The gallbladder meridian was the most often utilized meridian. Most of the specific acupoints used were crossing points, and head and neck acupoints were the most commonly applied. Feng - chi (GB20), Tai - yang (EX - HN5), and Shuai - gu (GB8) were among the key acupoints. Meanwhile, certain acupoint combinations were obtained through exploratory factor analysis, cluster analysis, and decision tree analysis. Clinically, acupuncturists can use the data from the selection of these basic acupoints to make decisions on whether to add or remove additional acupoints according to each patient’s individual situation. However, the results of this experiment were tentative and need to be validated by more studies.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and Supplementary Materials.
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by The third round of Taizhou Traditional Chinese Medicine (Integrated Traditional Chinese and Western Medicine) key (supported) disciplines (No: Tai Wei Fa [2020] 52).
Disclosure
Yujun He, and Xiaoyi Wang share first authorship. The authors have no conflicts of interest to declare for this work.
References
1. Cheng YC, Zeng BY, Hung CM, et al. Effectiveness and acceptability of noninvasive brain and nerve stimulation techniques for migraine prophylaxis: a network meta-analysis of randomized controlled trials. J Headache Pain. 2022;23(1):28. doi:10.1186/s10194-022-01401-3
2.. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
3. Takeshima T, Wan Q, Zhang Y, et al. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20(1):111. doi:10.1186/s10194-019-1062-4
4. Martelletti P, Schwedt TJ, Lanteri-Minet M, et al. My migraine voice survey: a global study of disease burden among individuals with migraine for whom preventive treatments have failed. J Headache Pain. 2018;19(1):115. doi:10.1186/s10194-018-0946-z
5. Ueda K, Ye W, Lombard L, et al. Real-world treatment patterns and patient-reported outcomes in episodic and chronic migraine in Japan: analysis of data from the Adelphi migraine disease specific programme. J Headache Pain. 2019;20(1):68. doi:10.1186/s10194-019-1012-1
6. Yeh WZ, Blizzard L, Taylor BV. What is the actual prevalence of migraine?. Brain Behav. 2018;8(e00950). doi:10.1002/brb3.950
7. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American migraine study II. Headache. 2001;41(7):646–657. doi:10.1046/j.1526-4610.2001.041007646.x
8. Munakata J, Hazard E, Serrano D, et al. Economic burden of transformed migraine: results from the American Migraine Prevalence and Prevention (AMPP) study. Headache. 2009;49(4):498–508. doi:10.1111/j.1526-4610.2009.01369.x
9. Edmeads J, Findlay H, Tugwell P, et al. Impact of migraine and tension-type headache on life-style, consulting behaviour, and medication use: a Canadian population survey. Can J Neurol Sci. 1993;20(2):131–137. doi:10.1017/s0317167100047697
10. Goadsby PJ, Sprenger T. Current practice and future directions in the prevention and acute management of migraine. Lancet Neurol. 2010;9(3):285–298. doi:10.1016/s1474-4422(10)70005-3
11. Evers S, Afra J, Frese A, et al. EFNS guideline on the drug treatment of migraine--revised report of an EFNS task force. Eur J Neurol. 2009;16(9):968–981. doi:10.1111/j.1468-1331.2009.02748.x
12. Puledda F, Goadsby PJ. An update on non-pharmacological neuromodulation for the acute and preventive treatment of migraine. Headache. 2017;57(4):685–691. doi:10.1111/head.13069
13. Du R, Wang Y, Liu X, et al. Acupuncture for acute migraine attacks in adults: a systematic review protocol. BMJ Open. 2015;5(e006968):e006968. doi:10.1136/bmjopen-2014-006968
14. Su P, Xie X, Xu Y, et al. Effectiveness of acupuncture in migraine rats: a systematic review. PLoS One. 2023;18(e0280556). doi:10.1371/journal.pone.0280556
15. Xu S, Yu L, Luo X, et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: multicentre, randomised clinical trial. BMJ. 2020;368(m697). doi:10.1136/bmj.m697
16. Tu M, Xiong S, Lv S, et al. Acupuncture for major depressive disorder: a data mining-based literature study. Neuropsychiatr Dis Treat. 2023;19:1069–1084. doi:10.2147/ndt.S405728
17. Yu S, Yang J, Yang M, et al. Application of acupoints and meridians for the treatment of primary dysmenorrhea: a data mining-based literature study. eCAM. 2015;2015:752194. doi:10.1155/2015/752194
18. He Y, Miao F, Fan Y, et al. Analysis of acupoint selection and combinations in acupuncture treatment of carpal tunnel syndrome: a protocol for data mining. J Pain Res. 2023;16:1941–1948. doi:10.2147/jpr.S411843
19. He Y, Miao F, He C, et al. A data mining study for analysis of acupoint selection and combinations in acupuncture treatment of carpal tunnel syndrome. J Pain Res. 2024;17:1153–1170. doi:10.2147/jpr.S452618
20. He Y, Miao F, Fan Y, et al. Analysis of acupoint selection and combinations in acupuncture treatment of piriformis syndrome: a protocol for data mining. J Pain Res. 2023;16:3265–3272. doi:10.2147/jpr.S422857
21. He Y, Y Fan, Miao F, et al. Acupoint selection law of acupuncture in treating piriformis syndrome based on data mining. Chin J Inf Traditional Chin Med. 2023;30:15–21. doi:10.19879/j.cnki.1005-5304.202210230
22. He Y, Miao F, Y Fan, et al. Analysis on acupoint selection law of acupuncture and moxibustion in treating benign prostatic hyperplasia based on data mining. Chin J Inf Traditional Chin Med. 2023;30:25–31. doi:10.19879/j.cnki.1005-5304.202303460
23. He YJ, Fan YS, Miao FR, et al. Acupoint selection rules of acupuncture and moxibustion in treating neurogenic bladder based on data mining. Zhen Ci Yan Jiu. 2024;49(2):198–207. doi:10.13702/j.1000-0607.20230018
24. He YJ, He JJ, Fan YS, et al. Analysis on acupoint selection rules in the treatment of metabolism-associated fatty liver disease based on data mining. Zhen Ci Yan Jiu. 2024;49(4):424–433. doi:10.13702/j.1000-0607.20221333
25. He Y, Wu Y, Li X. Analysis of acupoint selection and combinations in acupuncture treatment of migraine: a protocol for data mining. J Pain Res. 2024;17:4149–4157. doi:10.2147/jpr.S489296
26. Chen J, Xie Y, Lin Q, et al. Investigating acupoint selection and combinations of acupuncture for tic disorders: an association rule mining and network analysis study. Front Neurol. 2022;13:894951. doi:10.3389/fneur.2022.894951
27. Shen X. Meridian and Collaterals, Acupoints. Beijing: China Medical Science and Technology Press; 2020.
28. Regulation SAfM, China SAotPsRo. Nomenclature and Location of Meridian Points:gb/T 12346—2021(In Chinese). Beijing: Standards Press of China; 2021.
29. State Administration for Market Regulation SAotPsRoC. Nomenclature and Location of Extra Points in Common Use:gb/T 40997—2021(In Chinese). Beijing: Standards Press of China; 2021.
30. Zhang F, Fan Y, Miao F, et al. Analysis on acupoint selection rules of acupuncture in treating perimenopausal syndrome based on data mining. Chin J Inf Traditional Chin Med. 2019;14:1–8. doi:10.19879/j.cnki.1005-5304.202310228
31. Yujun HE, Jiujie HE, Yushan FAN, et al. Clinical application of Fengchi acupoint in ancient books based on data mining technology. Chin J Inf Traditional Chin Med. 2023;30:45–50. doi:10.19879/j.cnki.1005-5304.202303641
32. Biglione B, Gitin A, Gorelick PB, et al. Aspirin in the treatment and prevention of migraine headaches: possible additional clinical options for primary healthcare providers. Am J Med. 2020;133(4):412–416. doi:10.1016/j.amjmed.2019.10.023
33. Williams KA. Auricular therapy for migraine. Curr Pain Headache Rep. 2024;28(8):835–841. doi:10.1007/s11916-024-01261-3
34. Chiang CC, Porreca F, Robertson CE, et al. Potential treatment targets for migraine: emerging options and future prospects. Lancet Neurol. 2024;23(3):313–324. doi:10.1016/s1474-4422(24)00003-6
35. Chen Y, Liu Y, Song Y, et al. Therapeutic applications and potential mechanisms of acupuncture in migraine: a literature review and perspectives. Front Neurosci. 2022;16:1022455. doi:10.3389/fnins.2022.1022455
36. Nicholson RA, Buse DC, Andrasik F, et al. Nonpharmacologic treatments for migraine and tension-type headache: how to choose and when to use. Curr Treat Options Neurol. 2011;13(1):28–40. doi:10.1007/s11940-010-0102-9
37. Pryse-Phillips WE, Dodick DW, Edmeads JG, et al. Guidelines for the nonpharmacologic management of migraine in clinical practice. Canadian headache society. CMAJ. 1998;159(1):47–54.
38. Song X, Wang J, Bai L, et al. Bibliometric analysis of 100 most highly cited publications on acupuncture for migraine. J Pain Res. 2023;16:725–747. doi:10.2147/jpr.S396909
39. Wang D, Wen Y, Wen YY, et al. Status quo and thinking of acupoint optimization for preventive treatment of migraine. Zhongguo Zhen Jiu. 2019;39:896–900. doi:10.13703/j.0255-2930.2019.08.026
40. Wang J, Pei J, Cui X, et al. Individualized scalp acupuncture for motor dysfunction in stroke: a randomized controlled trial. Zhongguo Zhen Jiu. 2017;37:918–924. doi:10.13703/j.0255-2930.2017.09.002
41. Wang S, Wang J, Liu K, et al. Signaling interaction between facial and meningeal inputs of the trigeminal system mediates peripheral neurostimulation analgesia in a rat model of migraine. Neuroscience. 2020;433:184–199. doi:10.1016/j.neuroscience.2020.03.004
42. Goldman N, Chen M, Fujita T, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. 2010;13(7):883–888. doi:10.1038/nn.2562
43. Zhou M, Pang F, Liao D, et al. Electroacupuncture at Fengchi(GB20) and Yanglingquan(GB34) ameliorates Paralgesia through microglia-mediated neuroinflammation in a rat model of migraine. Brain Sci. 2023;13(4):541. doi:10.3390/brainsci13040541
44. Feng WX, Du XX, He JN, et al. Effects of moxibustion on serum levels of β-EP, SP and expression of IL-1β and COX-2 protein in brainstem in rats with migraine. Zhongguo Zhen Jiu. 2023;43:186–190. doi:10.13703/j.0255-2930.20220116-0001
45. Pei P, Cui S, Zhang S, et al. Effect of electroacupuncture at fengchi on facial allodynia, microglial activation, and microglia-neuron interaction in a rat model of migraine. Brain Sci. 2022;13(1):12. doi:10.3390/brainsci12081100
46. Luo J, Feng L, Wang L, et al. Restoring brain health: electroacupuncture at GB20 and LR3 for migraine mitigation through mitochondrial restoration. Brain Circ. 2024;10(2):154–161. doi:10.4103/bc.bc_95_23
47. Bayardo RJ, Agrawal R. Mining the most interesting rules.
48. Oyama T, Kitano K, Satou K, et al. Extraction of knowledge on protein-protein interaction by association rule discovery. Bioinformatics. 2002;18(5):705–714. doi:10.1093/bioinformatics/18.5.705
49. Reimer AP, Schiltz NK, Koroukian SM. High-risk diagnosis combinations in patients undergoing interhospital transfer: a retrospective observational study. BMC Emerg Med. 2022;22(1):187. doi:10.1186/s12873-022-00742-1
50. Paul S, Piontkivska H. Discovery of novel targets for multi-epitope vaccines: screening of HIV-1 genomes using association rule mining. Retrovirology. 2009;6(1):62. doi:10.1186/1742-4690-6-62
51. Zheng Y, Chen Y. The identification of Chinese herbal medicine combination association rule analysis based on an improved apriori algorithm in treating Patients with COVID-19 disease. J Healthc Eng. 2022;2022:6337082. doi:10.1155/2022/6337082
52. Oliveira MB, Ribeiro MP, Miguel SP, et al. In vivo high-content evaluation of three-dimensional scaffolds biocompatibility. Tissue Eng Part C Methods. 2014;20(11):851–864. doi:10.1089/ten.TEC.2013.0738
53. Wang K, Wang M, Gan C, et al. Residents’ diachronic perception of the impacts of ecological resettlement in a world heritage site. Int J Environ Res Public Health. 2019;16. doi:10.3390/ijerph16193556
54. Yang J, Teng Y, Song L, et al. Tracing sources and contamination assessments of heavy metals in road and foliar dusts in a typical mining city, China. PLoS One. 2016;11(12):e0168528. doi:10.1371/journal.pone.0168528
55. Ching-Yi C, Fun Y, editors. Particle swarm optimization algorithm and its application to clustering analysis.
56. Zhao Z, Chen M, Fan H, et al. Data analysis and knowledge mining of machine learning in soil corrosion factors of the pipeline safety. Comput Intell Neurosci. 2022;2022:9523878. doi:10.1155/2022/9523878
57. Pekel E. Estimation of soil moisture using decision tree regression. Theor Appl Climatol. 2020;139(3–4):1111–1119. doi:10.1007/s00704-019-03048-8
58. Olesen J. Headache classification committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bibliometric of Trends on Acupuncture Research About Migraine: Quantitative and Qualitative Analyses
He K, Zhan M, Li X, Wu L, Liang K, Ma R
Journal of Pain Research 2022, 15:1257-1269
Published Date: 28 April 2022
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, Zhang F, Yang P, Zhao X, Wang M, He C, He J
Journal of Pain Research 2023, 16:1941-1948
Published Date: 7 June 2023
Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Piriformis Syndrome: A Protocol for Data Mining
He Y, Miao F, Fan Y, He J, Zhang F, Wang Z, Wu Y, Zhao Y, Yang P
Journal of Pain Research 2023, 16:3265-3272
Published Date: 28 September 2023
Analysis of Traditional Chinese Medicine Symptoms in Children with Spastic Cerebral Palsy, a Protocol for Data Mining
Wang X, Pang F, Du XG
Journal of Multidisciplinary Healthcare 2023, 16:3143-3149
Published Date: 25 October 2023
A Data Mining Study for Analysis of Acupoint Selection and Combinations in Acupuncture Treatment of Carpal Tunnel Syndrome
He Y, Miao F, He C, Fan Y, Zhang F, Yang P, Wang M, He J
Journal of Pain Research 2024, 17:1153-1170
Published Date: 18 March 2024