")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Exploring Gender Differences in the Relationship Between Thyroid Function and Aggressive and Impulsive Behaviors in Patients with Major Depressive Disorder
Authors Zhao S , Wang A, Han Y, Song C, Zhang H, He K, Chen J
Received 13 December 2024
Accepted for publication 5 March 2025
Published 14 March 2025 Volume 2025:21 Pages 563—574
DOI https://doi.org/10.2147/NDT.S510936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Taro Kishi
Shuai Zhao,1– 4 Anzhen Wang,1– 4 Yuqin Han,1– 4 ChenXia Song,1– 4 Hongqin Zhang,1– 4 Kongliang He,1– 4 Juan Chen1– 4
1Department of Psychiatry, the Affiliated Psychological Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Department of Psychiatry, Hefei Fourth People’s Hospital, Hefei, People’s Republic of China; 3Department of Psychiatry, Anhui Mental Health Center, Hefei, People’s Republic of China; 4Department of Psychiatry, Anhui Clinical Research Center for Mental Disorders, Hefei, People’s Republic of China
Correspondence: Kongliang He; Juan Chen, Email [email protected]; [email protected]
Purpose: Major depressive disorder (MDD) is a widespread mental health condition with significant global impact. Exploring the gender differences in the interplay between thyroid function, aggression, and impulsivity offers valuable insights into its multifactorial nature and management.
Patients and Methods: A cross-sectional study was conducted at Anhui Mental Health Center and included 113 MDD patients (56 males, 57 females) and 102 healthy controls (45 males and 57 females). Thyroid function was assessed through serum thyroid hormone levels, and impulsivity and aggression were measured using the Buss-Perry Aggression Questionnaire (BPAQ) and Barratt’s Impulsiveness Scale version 11 (BIS). Potential confounding factors such as age, education, and Hamilton Depression Rating Scale (HAMD) scores were adjusted for.
Results: Both male and female MDD patients showed significant changes in serum thyrotropin levels (F(1,213)=10.996, p=0.001), impulsivity (F(1,213)=151.521, p< 0.05), and aggression (F(1,213)=44.411, p< 0.05) compared to healthy controls. MANCOVA revealed significant differences in attentional impulsivity, motor impulsivity, physical aggression, anger, hostility, and self-directed aggression (all p< 0.05). Moreover, significant differences between genders were observed in these areas (all p< 0.05). In males, TSH levels were inversely related to several behavioral dimensions (all p< 0.05), while no such correlation was found in females.
Conclusion: This study highlights the role of thyroid function, especially TSH levels, in influencing impulsivity and aggression in male MDD patients, suggesting a gender-specific physiological-behavioral relationship. The findings contribute to the development of gender-specific treatment strategies. In the future, longitudinal studies with larger sample sizes should be conducted to explore molecular mechanisms for more personalized treatments.
Keywords: MDD, thyroid function, gender differences, aggressive and impulsive
Introduction
Major depressive disorder (MDD) is a primary contributor to global disability, impacting upwards of 300 million individuals.1 Amidst improvements in living standards, MDD has emerged as a substantial health concern due to its high incidence, recurrence, and disability rates, while imposing a considerable economic burden.2 However, the underlying pathophysiological mechanisms remain poorly understood. Management of the acute phase of MDD has improved over the past years, but its long-term treatment remains suboptimal, involving inadequate medication dosage and duration, recurrent and unwarranted modifications to drug therapy, and poor treatment adherence.3 Antidepressants utilized in clinical settings mainly function by targeting neurotransmitters such as monoamine, serotonin, and noradrenaline.4 This approach addresses certain biochemical aspects of MDD; however, numerous research studies have reported that MDD is a multifaceted disorder, involving disturbances in neuroendocrine systems and immune-inflammatory and metabolic abnormalities, suggesting the necessity for comprehensive treatment strategies.5
Numerous brain-centric mechanisms have been postulated for this multifaceted disease, emphasizing disruptions within the hypothalamus-pituitary-thyroid (HPT) axis, modifications in thyroid hormone (TH) synthesis and regulation, and subsequent implications on neuroplasticity and neural circuit functionality.6–8 HPT axis dysfunction influences both physiological and psychological aspects of health and behavior.9 Emotional and psychotic symptoms may be precipitated through possible disruptions in metabolic processes and intracellular signaling pathways, and personality traits like impulsivity and aggression are altered.10 Therefore, investigating the specific dynamics through which this dysfunction modulates such behaviors in the context of MDD holds significance.11,12 Research shows a complex link between MDD, aggression, and impulsivity.13 About one-third of MDD patients show signs of aggression, shifting the typical view of MDD away from only psychomotor inhibition to include visible behavioral changes like anger attacks.14,15 Nonetheless, aggression and impulsivity are not only symptoms but also affect the progression of the condition, requiring further study to understand how they influence each other.
The multifaceted nature of MDD invites consideration of various physiological mechanisms, particularly the potential influence of thyroid function abnormalities on behavior.16 Recent studies have found that thyroid dysfunction, particularly elevated thyroid peroxidase antibodies (TPOAb) and thyroglobulin antibodies (TGAb), is significantly associated with an increased risk of suicidal behavior in MDD patients.17,18 This suggests that impulsivity and aggression, potential traits of suicidal behavior, may be linked to thyroid abnormalities. An emerging hypothesis posits that thyroid dysfunction, notably in thyroid stimulating hormone (TSH) and thyroxine (T4) levels, may be intricately tied to escalated impulsivity and aggression observed in MDD.19,20 While neuroinflammation and oxidative stress have been traditionally implicated in MDD’s pathophysiology, the exploration of neuroendocrine dimensions.21 Specifically, the interplay between hormonal levels and behavioral manifestations introduces a novel frontier in comprehending and potentially targeting aggressive and impulsive behaviors in the context of depressive disorders.
Notably, the interaction between thyroid function and gender differences in MDD has received limited attention. Understanding how thyroid dysfunction manifests differently in men and women is essential, as thyroid issues are known to affect mood and behavior in gender-specific ways.22,23 The gap in the literature lies in the insufficient exploration of how thyroid function, particularly TSH and T4 levels, is associated with aggressive and impulsive behaviors in MDD, with gender differences remaining underexamined. This observational study aims to address this gap by examining how thyroid function relates to these behaviors in MDD patients, with a focus on gender differences.
Material and Methods
Participants
A total of 113 individuals (56 males, 57 females) diagnosed with MDD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and in good physical health were recruited between 2018 and 2021. The diagnostic evaluations were carried out by two experienced psychiatrists. Patients with a 17-item Hamilton Rating Scale for Depression (HAMD-17) score ≥18 were included in the study, indicating moderate to severe depressive symptoms. The exclusion criteria were: (1) Patients with other severe somatic or known thyroid diseases, including hyperthyroidism, hypothyroidism, and Hashimoto’s thyroiditis; (2) Those suffering from severe nervous system disorders; (3) alcohol or drug abuse or dependence; (4) pregnancy or breastfeeding. Additionally, subjects with abnormal thyroid function were excluded from participation.
Meanwhile, 102 (45 males, 57 females) healthy controls were recruited from local communities. The healthy controls were thoroughly evaluated by the research psychiatrist, excluding any lifetime psychiatric disorders. Unstructured psychiatric interviews were conducted with healthy controls to identify and eliminate Axis I disorders. Subjects with current mental health issues, psychiatric histories, and family psychiatric histories were excluded. A thorough medical history and physical examination were conducted to ensure that all subjects were in good physical health. Study participants with severe medical problems, histories of organic brain diseases, substance abuse, or dependence within six months before the study were also excluded.
The sample size was determined based on our previous study.24 This cross-sectional study was conducted at the Anhui Mental Health Center. The research protocol was approved by the Medical Ethics Review Committee of the Anhui Mental Health Center (83230230), and all the subjects provided signed informed consent. In addition, the study was conducted in accordance with the Declaration of Helsinki. This study aimed to examine the relationship between thyroid function, aggression, and impulsivity in MDD patients and explore potential gender differences.
Clinical Measures
Each subject filled out a detailed questionnaire, including information about their age, gender, education level, marital status, and medical and psychological conditions. Data on the onset of illness, duration of illness, and hospitalizations of patients were also obtained by consulting their medical records and by interview. The severity of depression was assessed using the HAMD-17. Two blinded psychiatrists used an appropriate scale to evaluate the participants’ psychopathology. Specially, an interobserver correlation coefficient exceeding 0.8 was obtained after repeated assessments of HAMD-17 total scores.
Serum THs Level Assessments
Peripheral blood samples were collected after subjects had undergone an overnight fast of 8 hours. The electrochemical luminescence method (Roche company Cobas E601 automatic immunoassay) was utilized to measure the TSH, free triiodothyronine (FT3), and free thyroxine (FT4) levels. The reference interval of TSH was 0.27–4.2 mIU/L. The reference interval of FT4 values was 12–22 pmol/L. The reference interval of FT3 values was 3.1–6.8 pmol/L.24,25
Assessment of Aggression and Impulsivity
Aggression and impulsivity were the co-primary outcome measures. The Chinese version of the Buss-Perry Aggression Questionnaire (BPAQ)26 and Barratt’s Impulsiveness Scale version 11 (BIS) were used to assess trait aggression and trait impulsivity. The BPAQ comprises 30 self-reported questionnaire items, measuring five domains of aggression: physical aggression (seven items), verbal aggression (five items), anger (six items), hostility (seven items), and self-aggression (five items). Each item is rated on a 5-point Likert scale ranging from 1 (“extremely uncharacteristic of m”) to 5 (“extremely characteristic of me”). The score for each sub-scale was calculated by summing the scores of the corresponding items, with higher scores indicating higher levels of aggression.
The Barratt Impulsiveness Scale-version 11 (BIS-11), a self-reported measure, was utilized to evaluate impulsive traits.27 This 30-item scale consists of three subscales: attentional impulsivity, motor impulsivity, and non-planning impulsivity. The scale assesses impulsivity, with higher scores indicating stronger impulsivity. Participants rate themselves on statements using a 4-point scale: rarely/never, occasionally, often or almost always. Both the BPAQ and BIS-11 have been applied in Chinese patient populations,28,29 demonstrating their validity and reliability in this context.
Statistical Analysis
The skewness-kurtosis test was used to assess the normality of data distribution before proceeding with further statistical analyses. Continuous variables conforming to a normal distribution were presented as the means ± SD, continuous variables not conforming to a normal distribution were presented as median (interquartile range), and categorical variables were displayed as percentages.
In the analysis comparing the BIS-11 and BPAQ assessments, age and education were included as covariates in the multivariate analyses of covariance (MANCOVA). The purpose was to examine significant gender differences across the dependent measures, including the total score and subscales of the BIS-11 and BPAQ. The independent predictors considered in the analysis included gender (male vs female), diagnosis (patients vs healthy controls), and the interaction between gender and diagnosis. Group comparisons between demographic characteristics and clinical variables among male and female patients were conducted by using two-sample t-tests for continuous variables and chi-square tests for categorical variables. Bonferroni correction was applied in the post hoc analyses to control for the increased risk of Type I errors due to multiple comparisons.
To determine the relationship between thyroid function (TSH, FT3, FT4) and total scores, as well as the subscales, of BIS-11 and BPAQ, separate multiple regression analyses using stepwise forward entry were conducted for males and females. These analyses were adjusted for age, education, and HAMD-17 total score. Two-tailed significance levels were set at 0.05. Statistical analysis was performed using SPSS 19.0.
Results
Characteristics of Subjects
A total of 113 patients with MDD and 102 healthy controls (HCs) were recruited. The demographic data are shown in Table 1. No significant sex differences were observed between HCs and MDD patients in terms of age (F(1, 213) = 0.915, p = 0.340) and education (F(1, 213) = 0.198, p = 0.657).
 |
Table 1 Demographics, BIS, BPAQ Total Scores in MDD Patients and Healthy Controls Grouped by Sex |
Symptom Profiles in MDD Patients
No significant results were observed in terms of age (t = 0.817, p = 0.416), education (t = 1.199, p = 0.233), marriage (χ2 = 0.071, p = 0.790), recurrence (χ2 = 0.008, p = 0.928), age of onset (t = 0.087, p = 0.931), and HAMD-17 total scores (-t = 1.761, p = 0.080) (Table 2).
 |
Table 2 Sex Differences of Clinical Characteristics in Patients with MDD Mean ± SD |
Thyroid Function in MDD Patients and Healthy Controls
MANCOVA revealed significant differences in TSH levels between the patient group and the control group (F(1,213) = 10.996, p = 0.001, partial η² = 0.062). Moreover, sex effects in FT3 (F(1,213) = 23.866, p < 0.001, partial η² = 0.116) and TSH levels (F(1,213) = 8.019, p = 0.005, partial η² = 0.039).
Sex Differences in Aggression and Impulsivity in Different Groups
As shown in Table 1, MANCOVA indicated significant differences between patients and controls after adjusting for age and education. Specifically, significant group differences were observed in attentional impulsivity (F(1,213) = 8.705, p = 0.004, partial η² = 0.040), motor impulsivity (F(1, 213) = 36.999, p < 0.001, partial η² = 0.150), non-planning impulsivity (F(1, 213) = 5.627, p = 0.019, partial η² = 0.026), BIS-total scores (F(1, 213) = 41.899, p < 0.001, partial η² = 0.060), physical aggression (F(1, 213) = 10.458, p = 0.001, partial η² = 0.048), anger (F(1, 213) = 20.420, p < 0.001, partial η² = 0.089), hostility (F(1, 213) = 79.729, p < 0.001, partial η² = 0.276), self-directed aggression (F(1, 213) = 49.417, p < 0.001, partial η² = 0.191), and BPAQ total scores (F(1, 213) = 44.411, p < 0.001, partial η² = 0.175). In the gender subgroup analysis, significant differences in physical aggression (F(1, 213) = 20.547, p < 0.001, partial η² = 0.090), verbal aggression (F(1, 213) = 4.382, p = 0.038, partial η² = 0.21), hostility (F(1, 213) = 15.998, p < 0.001, partial η² = 0.090), self-directed aggression (F(1, 213) = 4.206, p = 0.042, partial η² = 0.020), and BPAQ total scores (F(1, 213) = 9.170, p = 0.003, partial η² = 0.042) were observed.
Correlations of Thyroid Function with Impulsivity and Aggression in Male and Female MDD Patients
Multiple linear regression analyses were conducted for male and female patients, with the impulsivity and aggression measures (total and subscale scores) as dependent variables. The serum levels of thyroid hormones were set as independent variables, while age, education duration, and HAMD scores were included as covariates.
In male patients, TSH levels were inversely associated with motor impulsivity (β = −0.359, t = −2.712, p = 0.009) (Table 3). Further multivariate regression analyses revealed a negative association between the TSH levels and hostility (β = −0.445, t = −3.513, p = 0.001), self-directed aggression (β = −0.349, t = −2.600, p = 0.012), and the BPAQ total scores (β = −0.394, t = −3.003, p = 0.004) (Table 4). In the female patients, no significant associations were found between thyroid function and the scores on the BIS-11 and BPAQ scores (all p >0.05).
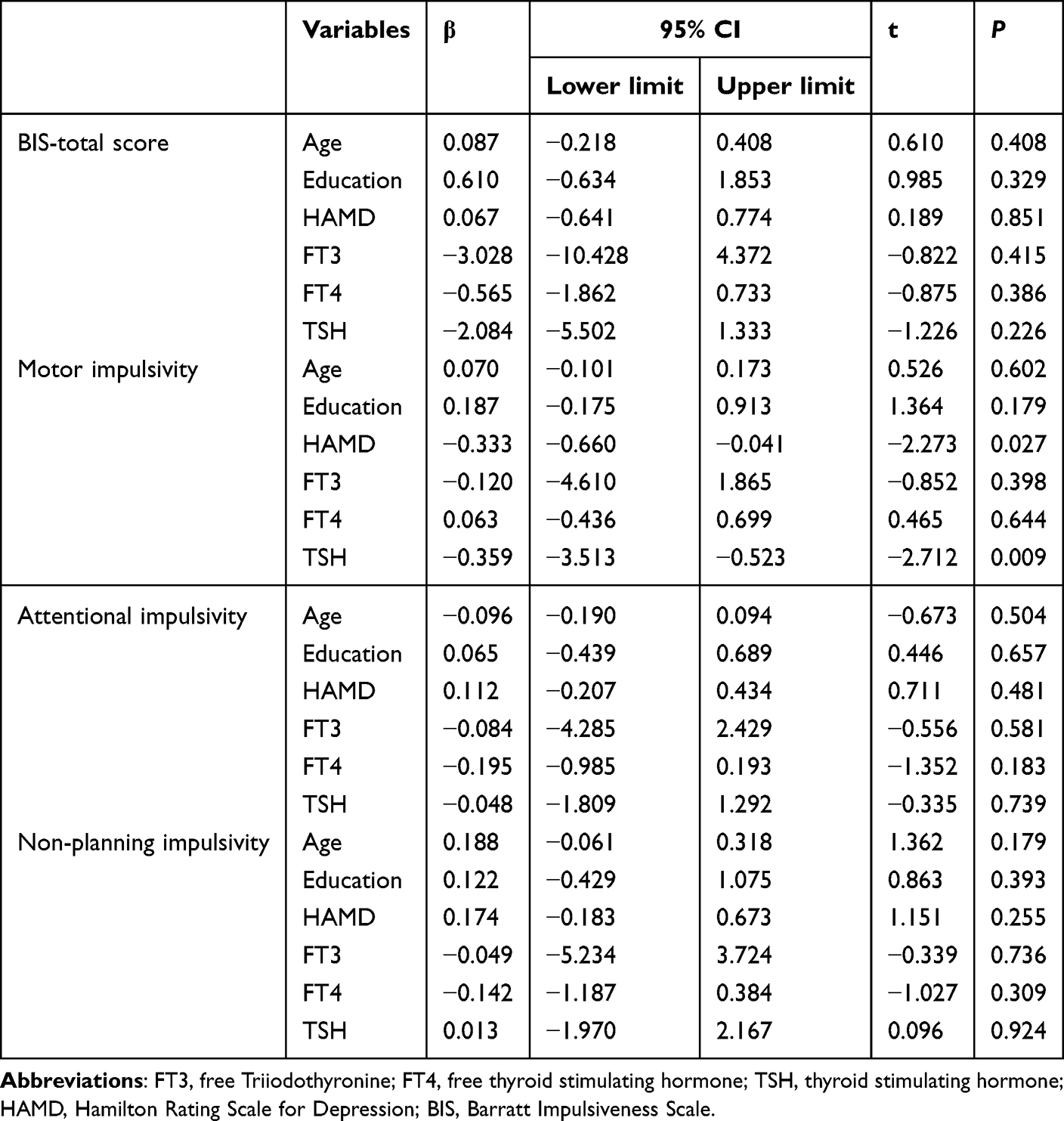 |
Table 3 Impact of Thyroid Function on Impulsivity in Male MDD Patients |
 |
Table 4 Impact of Thyroid Function on Aggression in Male MDD Patients |
Discussion
To the best of our knowledge, this study was the first to conduct a subgroup analysis based on gender to investigate the relationship between thyroid function and behavioral manifestations, such as aggression and impulsivity traits, in patients with MDD. The primary findings of this study include: (1) Significant differences in TSH levels between MDD patients and healthy controls were observed, with marked gender-related variations, particularly in FT3 and TSH levels. (2) Significant sex differences were identified in several domains of aggression and impulsivity were found between the male and female groups, as determined by the BIS-11 and BPAQ. (3) In male MDD patients, our multivariate regression analysis revealed that TSH levels could predict impulsivity and aggressive behaviors, underscoring a notable relationship between thyroid function and behavioral outcomes. This specific relationship was not discernible in female MDD patients. These findings suggest that assessing and managing thyroid function in a gender-specific manner could be crucial for addressing behavioral issues in MDD patients.
In the present study, thyroid function, particularly regarding TSH and FT3 levels, emerged as a significant difference between MDD patients and healthy controls. Our findings indicate that MDD patients exhibited significantly lower serum TSH levels compared to HCs, which was consistent across both genders, reflecting the results of previous research findings.30 One potential explanation for the lower TSH levels observed in MDD patients, particularly in males, may involve a decreased sensitivity to TRH stimulation in the male demographic. This phenomenon has been observed in previous studies, suggesting a unique neuroendocrine profile in males with MDD.31 Furthermore, the interaction between thyroid hormones and serotonin is a critical area to explore. Both thyroid hormones and serotonin play essential roles in regulating mood and behavior, and disturbances in their interplay could exacerbate behavioral symptoms such as impulsivity and aggression.32,33 An extensive, community-based study reported similar findings, revealing lower serum TSH concentrations were lower in males compared to females MDD patients.34 This gender-based difference could also be associated with the divergent effects of thyroid hormones on the central nervous system, with estrogen in females possibly conferring protective effects on thyroid function, influencing the overall gender differences observed in MDD patients.35 Furthermore, our prior research indicated that female depressive inpatients exhibited double the rate of subclinical hypothyroidism compared to their male counterparts.22 This discrepancy might be linked to TRH hypersecretion, acting as a compensatory mechanism for serotonin and thyroid hormone regulation. These findings underscore the critical need for gender-specific considerations when assessing thyroid functions in MDD patients.
Multifactorial variance analysis highlighted markedly elevated scores on the BIS-11 scale for MDD patients across various subscales compared to their healthy counterparts. Consistent with prior research, our results emphasize the profound interplay between MDD and increased impulsivity, supporting the argument for impulsivity as a transdiagnostic factor prevalent in numerous psychiatric disorders.36–39 Moreover, the heightened impulsivity observed in MDD patients might indicate a trait-like endophenotype, reflecting the disorder’s more profound genetic or inherent attributes of the disorder.40 These findings imply that targeting impulsivity through behavioral interventions or medication could be effective in managing MDD. Additionally, understanding the genetic basis of impulsivity in MDD could promote the development of personalized treatment plans, potentially improving patient outcomes by addressing underlying genetic predispositions.
Notably, within these sub-scales, ‘motor impulsiveness’ exhibited a distinct gender disparity. This term refers to a behavioral trait characterized by acting on the spur of the moment, without forethought, often in a manner that is socially nonconforming or risky.41 Specifically, men, being generally more predisposed to impulsivity and aggressive behaviors than women, showcase a propensity to engage in unrestrained motor actions, potentially as a coping mechanism to stress and negative emotions.42,43 The male tendency towards higher motor impulsiveness could be attributed to both hormonal factors, particularly the influence of testosterone, and neurobiological differences. Testosterone has been shown to promote impulsive behavior,44 and male-specific differences in brain structure, particularly in regions like the ventrolateral prefrontal cortex (VLPFC),45,46 might further contribute to heightened motor impulsiveness in males with MDD. These findings highlight the need for further research to explore the neural mechanisms underlying motor impulsiveness in MDD, particularly in male patients. Understanding these mechanisms could inform the development of targeted interventions to reduce impulsive behaviors.
Furthermore, considering the critical role of the serotonin (5-HT) system in modulating impulsivity and aggression, particularly its pronounced involvement in male impulsivity as evidenced by Marazziti et al,47 adds an intriguing layer of complexity is added to our understanding of the neurobiological substrates underlying male-specific motor impulsiveness in MDD. This emphasizes the need to investigate the multifaceted interplay between serotonin, thyroid function, and behavioral tendencies. Intriguingly, the present research unveils a pivotal discovery, delineating a negative correlation between TSH levels and motor impulsiveness in male patients with MDD. A recent cross-sectional study echoes our findings, revealing a link between aberrant thyroid function and the risk of suicide attempts in males with MDD, thereby partially validating our innovative discovery.48 This confluence of findings provides a new perspective that enhances our understanding of the intricate relationships between thyroid function and behavioral tendencies in male MDD, underscoring the imperative of delving deeper into the neuroendocrine mechanisms involved.
Significantly, our findings align with existing research, highlighting an evident increase in aggressive behavior among individuals with MDD and thereby solidifying the well-established link between MDD and amplified aggression. Notably, the interplay between MDD and aggression is not merely symptomatic;49 aggression dysregulation is hypothesized to play a pivotal role in the disorder’s progression, potentially acting as a pacemaker through aggression dysregulation.15,50,51 Furthermore, our study unveils crucial gender differences, illustrating distinct aggression manifestations between males and females within the context of MDD. Research by Dumais et al52 showed that men tend to opt for violent suicide methods, which is linked to a history of impulsive-aggressive behaviors.53 This pattern, more common in males, could shed light on the higher aggression levels in our male MDD subjects. It suggests an intricate relationship between aggressive predilections and the comprehensive severity and expression of depressive disorders, particularly within the male population.54 Therefore, both the mechanistic and psychosocial factors propelling this gender-distinct divergence in aggression and suicidal behaviors within MDD should be meticulously explored, highlighting the need for gender-specific diagnostic tools and therapeutic strategies. Tailored interventions could potentially mitigate aggression and suicidal tendencies more effectively, thereby improving treatment outcomes and overall patient well-being.
Recent research has expanded our understanding of MDD and its association with aggressive behaviors, pointing to brain alterations influenced by disrupted myelination, oxidative stress, and neuroinflammation.55–59 Our study introduces a novel perspective by uncovering a potential connection between thyroid function and aggression in male MDD patients. Notably, a significant relationship was observed between TSH levels and distinct aggression sub-scales in this demographic, thereby highlighting an intriguing pathway that merits further investigation in the nexus between hormonal levels, MDD, and aggression. Previous research highlights a link between thyroid function, explicitly involving TSH and T4, and behavioral outcomes such as impulsivity and aggression, especially in various psychiatric disorders.21 Specifically, low TSH levels and sometimes high T4 have been associated with greater impulsivity, aggression, and even suicidal tendencies in different psychiatric conditions.19,60,61
Moreover, disrupted thyroid function has been correlated with increased severity in depressive disorders, possibly through mechanisms involving neurotransmitter changes in brain structure and function, direct impacts on emotion and behavior, and interplay with other endocrine systems.62,63 Thyroid hormones play a crucial role in the central nervous system, particularly in regulating neurotransmitters such as dopamine and serotonin. Disruption in thyroid function may imbalance these neurotransmitters, influencing impulsivity and aggression.64,65 Additionally, thyroid dysfunction can lead to alterations in specific brain regions, such as the prefrontal cortex, which play essential roles in impulse control and the regulation of aggressive behavior.66,67 This complex interplay between thyroid function and aggression in MDD indicates a need for future research to unravel the precise mechanisms involved, potentially opening avenues for hormone-targeted therapeutic strategies in managing aggressive behaviors in MDD.
Nevertheless, the limitations of the study should be acknowledged. Firstly, causal relationships between thyroid function, aggression, and MDD cannot be determined due to the cross-sectional study design. Secondly, the varied self-report and behavioral tools used to measure the multifaceted concept of impulsivity and aggression may introduce potential biases and affect the comparability of our findings. Thirdly, our focus on specific thyroid markers, TSH and T4, may overlook other biochemical or endocrine factors involved in the psychiatric and behavioral observations. Fourthly, the menstrual cycle phase during blood collection for female participants was not accounted for, which could influence thyroid hormone levels and affect the study results. Fifth, the participants were limited to a particular demographic and geographic location, so our findings cannot be extrapolated to other populations becomes restricted, thereby limiting our findings’ universality. Sixth, anxiety symptoms, which can influence aggression and impulsivity, were not assessed using a standardized tool like the Hamilton Anxiety Rating Scale (HAMA). Future studies should include such assessments to provide a more comprehensive understanding of these relationships. Seventh, our modest sample size limits the statistical strength and applicability of the findings, requiring validation from more extensive and diverse study populations. Finally, while the research introduces connections and proposes pathways between hormonal levels and behavioral outcomes, the mechanisms at the biological level remain speculative, warranting further investigation to unravel the exact biological underpinnings of these observations.
Conclusion
In summary, our study reveals notable links between thyroid function and behaviors, such as aggression and impulsivity, in MDD patients, with distinct variations between genders. A significant negative correlation was found between TSH levels and certain behavioral aspects, particularly in male patients. The observed sex differences in aggression and impulsivity domains highlight the necessity for gender-specific approaches in understanding and managing MDD. Future research should further explore the underlying mechanisms underlying these findings, analyzing the relationship between gender, thyroid function, and behavioral tendencies in MDD management and research.
Ethics Statement
The research protocol received approval from the Medical Ethics Review Committee of the Anhui Mental Health Center (83230230).
Acknowledgment
We would like to express our sincere gratitude to all the individuals who contributed to this research. Special thanks to the research participants for their valuable input. We also appreciate the support from the institutions and et.al who provided resources and guidance throughout the study. Our heartfelt thanks to Kongliang He and Juan Chen for their dedicated supervision and critical insights into the development of this work.
Funding
National Clinical Key Specialty Construction Project of China; Anhui Province University Research Project (2023AH050613); Anhui Province Clinical Medical Research Transformation Special Project (Grant Nos.202204295107020005, 202204295107020006).
Disclosure
The authors report no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors have also adhered to an excellent code of conduct and good ethical standards while conducting this study.
References
1. G.W.H.. Organization, Global Health Estimates 2018: Disease Burden by Cause, Sex, by Country and Region, 2000-2016. Geneva; 2018.
2. Arias-de la Torre J, Vilagut G, Ronaldson A. Prevalence and variability of current depressive disorder in 27 European countries: a population-based study. Lancet Public Health. 2021;6(10):e729–e738. doi:10.1016/S2468-2667(21)00047-5
3. Herrman H, Patel V, Kieling C, et al. Time for united action on depression: a lancet–world psychiatric association commission. Lancet. 2022;399:957–1022.
4. Berton O, Nestler EJ. New approaches to antidepressant drug discovery: beyond monoamines. Nat Rev Neurosci. 2006;7:137–151. doi:10.1038/nrn1846
5. Horowitz MA, Zunszain PA. Neuroimmune and neuroendocrine abnormalities in depression: two sides of the same coin. Ann N Y Acad Sci. 2015;1351:68–79. doi:10.1111/nyas.12781
6. Gold PW. Endocrine factors in key structural and intracellular changes in depression. Trends Endocrinol Metab. 2021;32:212–223. doi:10.1016/j.tem.2021.01.003
7. Soheili-Nezhad S, Sprooten E, Tendolkar I, Medici M. Exploring the genetic link between thyroid dysfunction and common psychiatric disorders: a specific hormonal, or a general autoimmune comorbidity. Thyroid. 2022.
8. Karakatsoulis GN, Tsapakis EM, Mitkani C, Fountoulakis KN. Subclinical thyroid dysfunction and major depressive disorder. Hormones. 2021;20:613–621. doi:10.1007/s42000-021-00312-3
9. Glombik K, Detka J, Bobula B, et al. Contribution of hypothyroidism to cognitive impairment and hippocampal synaptic plasticity regulation in an animal model of depression. Int J mol Sci. 2021;22:1599. doi:10.3390/ijms22041599
10. Sinai C, Hirvikoski T, Nordström AL. Thyroid hormones and adult interpersonal violence among women with borderline personality disorder. Psychiatry Res. 2015;227:253–257. doi:10.1016/j.psychres.2015.03.025
11. Li P, Ru X, Teng Y. Interaction between isolated maternal hypothyroxinemia and pregnancy-related anxiety on preschooler’s internalizing and externalizing problems: a birth cohort study. Psychoneuroendocrinology. 2023;152:106102. doi:10.1016/j.psyneuen.2023.106102
12. Wang S, Zhang J, Zhang S, Shi F, Feng D, Feng X. Exposure to melamine cyanuric acid in adolescent mice caused emotional disorder and behavioral disorder. Ecotoxicol Environ Saf. 2021;211:111938. doi:10.1016/j.ecoenv.2021.111938
13. Lunansky G, van Borkulo C, Borsboom D. Borsboom, personality, resilience, and psychopathology: a model for the interaction between slow and fast network processes in the context of mental health. Eur J Pers. 2020;34:969–987. doi:10.1002/per.2263
14. Fava M. Psychopharmacologic treatment of pathologic aggression. Psychiatr Clin North Am. 1997;20:427–451. doi:10.1016/S0193-953X(05)70321-X
15. Bak M, Weltens I, Bervoets C, et al. The pharmacological management of agitated and aggressive behaviour: a systematic review and meta-analysis. Eur Psychiatry. 2019;57:78–100. doi:10.1016/j.eurpsy.2019.01.014
16. Jermy BS, Glanville KP, Coleman JRI, Lewis CM, Vassos E. Exploring the genetic heterogeneity in major depression across diagnostic criteria. mol Psychiatry. 2021;26:7337–7345. doi:10.1038/s41380-021-01231-w
17. Feng XZ, Wang K, Li Z, et al. Association between thyroid autoimmunity and clinical characteristics in first-episode and drug-naive depressed patients with suicide attempts. Gen Hosp Psychiatry. 2023;83:156–163. doi:10.1016/j.genhosppsych.2023.05.008
18. Chen SW, Li X, Lang X, Li J, Zhang XY. Metabolic parameters and thyroid hormones in relation to suicide attempts in patients with first-episode and drug-naive major depressive disorder with comorbid glucose disturbances: a large cross-sectional study. Eur Arch Psychiatry Clin Neurosci. 2023;273:199–207. doi:10.1007/s00406-022-01490-w
19. Soderstrom H, Forsman A. Elevated triiodothyronine in psychopathy - possible physiological mechanisms. J Neural Transm. 2004;111:739–744. doi:10.1007/s00702-004-0137-8
20. Carver CS, Johnson SL, Joormann J. Serotonergic function, two-mode models of self-regulation, and vulnerability to depression: what depression has in common with impulsive aggression. Psychol Bull. 2008;134:912–943. doi:10.1037/a0013740
21. Hasan G, Balcioglu YH, Solmaz M. The role of impulsive and aggressive traits, albumin and thyroid functions in recent suicide attempters: an investigation with a transdiagnostic approach. Neurochem J. 2023;16:491–497. doi:10.1134/S1819712422040079
22. Zhao S, Chen Z, Wang X, Yao Z, Lu Q. Increased prevalence of subclinical hypothyroidism in female hospitalized patients with depression. Endocrine. 2021;72:479–485. doi:10.1007/s12020-020-02490-3
23. Huang X, Sun Y, Wu A, Zhang XY. Gender differences in the prevalence and clinical correlates of thyroid dysfunction in patients with first-episode and drug-naive major depressive disorder with comorbid suicide attempts: a large cross-sectional study. BMC Psychiatry. 2023;23:603. doi:10.1186/s12888-023-05089-w
24. Zhao S, Xia Y, Huang Y, et al. The correlation between thyroid function, frontal gray matter, and executive function in patients with major depressive disorder. Front Endocrinol. 2021;12:779693. doi:10.3389/fendo.2021.779693
25. Rogowicz-Frontczak A, Falkowski B, Grzelka-Wozniak A, Uruska A, Araszkiewicz A, Zozulinska-Ziolkiewicz D. Does autoimmune hypothyroidism increase the risk of neurovascular complications in type 1 diabetes? J Endocrinol Invest. 2020;43:833–839. doi:10.1007/s40618-019-01171-x
26. Maxwell JP. Development and preliminary validation of a Chinese version of the Buss-Perry Aggression Questionnaire in a population of Hong Kong Chinese. J Pers Assess. 2007;88:284–294. doi:10.1080/00223890701317004
27. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51:768–774. doi:10.1002/1097-4679(199511)51:6<768::AID-JCLP2270510607>3.0.CO;2-1
28. Gao L, Yang R, Fan HZ, et al. Correlation between aggressive behavior and impulsive and aggressive personality traits in stable patients with schizophrenia. Neuropsychiatr Dis Treat. 2023;19:801–809. doi:10.2147/NDT.S404176
29. Yang F, Tong J, Zhang SF, Zhang J, Zhong BL. Prevalence and correlates of suicide attempts in Chinese individuals with borderline personality disorder. Front Psychiatry. 2022;13:942782. doi:10.3389/fpsyt.2022.942782
30. Zhou Y, Ma Y, Wu Q, et al. Comparison of thyroid hormone levels between patients with major depressive disorder and healthy individuals in China. Front Psychiatry. 2021;12:750749. doi:10.3389/fpsyt.2021.750749
31. MacQueen GM, Joffe RT. A review of gender differences in studies of thyroid function and major depression. Psychiatr Ann. 2002;32:477–482. doi:10.3928/0048-5713-20020801-07
32. Duval F, Mokrani MC, Bailey P, et al. Thyroid axis activity and serotonin function in major depressive episode. Psychoneuroendocrinology. 1999;24:695–712. doi:10.1016/S0306-4530(99)00022-0
33. Trifu SC, Tudor A, Radulescu I. Aggressive behavior in psychiatric patients in relation to hormonal imbalance (Review). Exp Ther Med. 2020;20:3483–3487. doi:10.3892/etm.2020.8974
34. Hollowell JG, Staehling NW, Flanders WD, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): national health and nutrition examination survey (NHANES III). J Clin Endocrinol Metab. 2002;87:489–499. doi:10.1210/jcem.87.2.8182
35. Rajoria S, Suriano R, George AL, et al. Estrogen activity as a preventive and therapeutic target in thyroid cancer. Biomed Pharmacother. 2012;66:151–158. doi:10.1016/j.biopha.2011.11.010
36. Trofimova I, Sulis W. There is more to mental illness than negative affect: comprehensive temperament profiles in depression and generalized anxiety. BMC Psychiatry. 2018;18:125. doi:10.1186/s12888-018-1695-x
37. Fields SA, Schueler J, Arthur KM, Harris B. The role of impulsivity in major depression: a systematic review. Curr Behav Neurosci Rep. 2021;8:38–50. doi:10.1007/s40473-021-00231-y
38. Wang YY, Jiang NZ, Cheung EF, Sun HW, Chan RC. Role of depression severity and impulsivity in the relationship between hopelessness and suicidal ideation in patients with major depressive disorder. J Affect Disord. 2015;183:83–89. doi:10.1016/j.jad.2015.05.001
39. Moustafa AA, Tindle R, Frydecka D, Misiak B. Impulsivity and its relationship with anxiety, depression and stress. Compr Psychiatry. 2017;74:173–179. doi:10.1016/j.comppsych.2017.01.013
40. Fortgang RG, Hultman CM, van Erp TG, Cannon TD. Multidimensional assessment of impulsivity in schizophrenia, bipolar disorder, and major depressive disorder: testing for shared endophenotypes. Psychol Med. 2016;46:1497–1507. doi:10.1017/S0033291716000131
41. Chowdhury NS, Livesey EJ, Blaszczynski A, Harris JA. Pathological gambling and motor impulsivity: a systematic review with meta-analysis. J Gambl Stud. 2017;33:1213–1239. doi:10.1007/s10899-017-9683-5
42. Chapple CL, Johnson KA. Gender differences in impulsivity[J]. Youth Violence Juv Justice. 2007;5(3):221–234. doi:10.1177/1541204007301286
43. Chen P, Coccaro EF, Jacobson KC. Hostile attributional bias, negative emotional responding, and aggression in adults: moderating effects of gender and impulsivity. Aggressive Behavior. 2012;38:47–63. doi:10.1002/ab.21407
44. Aluja A, Garcia LF, Marti-Guiu M, et al. Interactions among impulsiveness, testosterone, sex hormone binding globulin and androgen receptor gene CAG repeat length. Physiol Behav. 2015;147:91–96. doi:10.1016/j.physbeh.2015.04.022
45. Goya-Maldonado R, Walther S, Simon J, Stippich C, Weisbrod M, Kaiser S. Motor impulsivity and the ventrolateral prefrontal cortex. Psychiatry Res. 2010;183:89–91. doi:10.1016/j.pscychresns.2010.04.006
46. Mou J, Zheng T, Long Z. Sex differences of brain cortical structure in major depressive disorder. Psychoradiology. 3;2023.
47. Weinstein A, Dannon P. Is impulsivity a male trait rather than female trait? exploring the sex difference in impulsivity. Curr Behav Neurosci Rep. 2015;2:9–14. doi:10.1007/s40473-015-0031-8
48. Ye G, Yuan Y, Li Z. Sex-differential association of suicide attempts with thyroid dysfunction in first-episode and drug-naive young major depressive disorder patients with comorbid anxiety. Sci Rep. 2023;13:13715. doi:10.1038/s41598-023-40948-2
49. Liu Q, Cole DA. Aggressive outbursts among adults with major depressive disorder: results from the collaborative psychiatric epidemiological surveys. J Psychiatr Res. 2021;135:325–331. doi:10.1016/j.jpsychires.2021.01.040
50. Swanson JW, Holzer CE 3rd, Ganju VK, Jono RT. Violence and psychiatric disorder in the community: evidence from the epidemiologic catchment area surveys. Hosp Community Psychiatry. 1990;41:761–770. doi:10.1176/ps.41.7.761
51. Knox M, King C, Hanna GL, Logan D, Ghaziuddin N. Aggressive behavior in clinically depressed adolescents. J Am Acad Child Adolesc Psychiatry. 2000;39:611–618. doi:10.1097/00004583-200005000-00015
52. Dumais A, Lesage AD, Lalovic A. Is violent method of suicide a behavioral marker of lifetime aggression? Am J Psychiatry. 2005;162:1375–1378. doi:10.1176/appi.ajp.162.7.1375
53. Oquendo MA, Bongiovi-Garcia ME, Galfalvy H, et al. Sex differences in clinical predictors of suicidal acts after major depression: a prospective study. Am J Psychiatry. 2007;164:134–141. doi:10.1176/ajp.2007.164.1.134
54. Brokke SS, Landro NI, Haaland VO. Impulsivity and aggression in suicide ideators and suicide attempters of high and low lethality. BMC Psychiatry. 2022;22:753. doi:10.1186/s12888-022-04398-w
55. Mosienko V, Bert B, Beis D, et al. Exaggerated aggression and decreased anxiety in mice deficient in brain serotonin. Transl Psychiatry. 2012;2:e122. doi:10.1038/tp.2012.44
56. Takahashi A, Flanigan ME, McEwen BS, Russo SJ. Aggression, social stress, and the immune system in humans and animal models. Front Behav Neurosci. 2018;12:56. doi:10.3389/fnbeh.2018.00056
57. D’Ambrosio F, Caggiano M, Schiavo L, et al. Chronic stress and depression in periodontitis and peri-implantitis: a narrative review on neurobiological, neurobehavioral and immune-microbiome interplays and clinical management implications. Dent J. 2022;10.
58. Coccaro EF, Lee R, Gozal D. Elevated plasma oxidative stress markers in individuals with intermittent explosive disorder and correlation with aggression in humans. Biol Psychiatry. 2016;79:127–135. doi:10.1016/j.biopsych.2014.01.014
59. Pomytkin I, Costa‐Nunes JP, Kasatkin V. Insulin receptor in the brain: mechanisms of activation and the role in the CNS pathology and treatment. CNS Neurosci Ther. 2018;24:763–774. doi:10.1111/cns.12866
60. Jose J, Nandeesha H, Kattimani S, Meiyappan K, Sarkar S, Sivasankar D. Association between prolactin and thyroid hormones with severity of psychopathology and suicide risk in drug free male schizophrenia. Clin Chim Acta. 2015;444:78–80. doi:10.1016/j.cca.2015.02.003
61. Peng R, Dai W, Li Y. Low serum free thyroxine level is correlated with lipid profile in depressive patients with suicide attempt. Psychiatry Res. 2018;266:111–115. doi:10.1016/j.psychres.2018.05.059
62. Duval F, Mokrani MC, Erb A, Gonzalez Opera F, Calleja C, Paris V. Relationship between chronobiological thyrotropin and prolactin responses to protirelin (TRH) and suicidal behavior in depressed patients. Psychoneuroendocrinology. 2017;85:100–109. doi:10.1016/j.psyneuen.2017.07.488
63. Hirtz R, Libuda L, Hinney A, et al. Lack of evidence for a relationship between the hypothalamus-pituitary-adrenal and the hypothalamus-pituitary-thyroid axis in adolescent depression. Front Endocrinol. 2021;12:662243. doi:10.3389/fendo.2021.662243
64. Bauer M, Whybrow PC. Thyroid hormone, neural tissue and mood modulation. World J Biol Psychiatry. 2001;2:59–69. doi:10.3109/15622970109027495
65. Sawicka-Gutaj N, Zawalna N, Gut P, Ruchala M. Relationship between thyroid hormones and central nervous system metabolism in physiological and pathological conditions. Pharmacol Rep. 2022;74:847–858. doi:10.1007/s43440-022-00377-w
66. Thompson CC. Thyroid hormone action in neural development. Cereb Cortex. 2000;10(10):939–945. doi:10.1093/cercor/10.10.939
67. Redman K, Ruffman T, Fitzgerald P, Skeaff S. Iodine deficiency and the brain: effects and mechanisms. Crit Rev Food Sci Nutr. 2016;56:2695–2713. doi:10.1080/10408398.2014.922042
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.