")
Back to Journals » Journal of Pain Research » Volume 18
Exploring Perceived Barriers and Facilitators for Implementing Acute Pain Clinical Trials: A Mixed-Methods Analysis of Ketamine Infusions for Sickle Cell Pain
Authors Kenney MO , Limkakeng AT , Ochoa TN, Mathias, JG, Knisely MR, Keefe F
Received 4 December 2024
Accepted for publication 1 March 2025
Published 20 March 2025 Volume 2025:18 Pages 1465—1478
DOI https://doi.org/10.2147/JPR.S507983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Martha O Kenney,1 Alexander T Limkakeng,2 Timothy N Ochoa,3 Joacy G Mathias,4 Mitchell R Knisely,5 Francis Keefe6
1Division of Pediatric Anesthesiology, Department of Anesthesiology, Duke University School of Medicine, Durham, NC, USA; 2Department of Emergency Medicine, Duke University School of Medicine, Durham, NC, USA; 3Duke University School of Medicine, Durham, NC, USA; 4Division of Women’s and Population Health, Duke University School of Medicine, Durham, NC, USA; 5Duke University School of Nursing, Durham, NC, USA; 6Pain Prevention and Treatment Research Program, Department of Psychiatry and Behavioral Science, Duke University, Durham, NC, USA
Correspondence: Martha O Kenney, Division of Pediatric Anesthesiology, Department of Anesthesiology, Duke University Medical Center, Box 3094, Durham, NC, 27710, USA, Email [email protected]
Objective: Vaso-occlusive events (VOEs) are the primary cause of acute pain in individuals with sickle cell disease (SCD), where high-dose opioids are the current standard treatment. Ketamine, a non-opioid analgesic, holds potential for managing acute SCD due to its opioid-sparing properties. This study aimed to explore the barriers and facilitators to an inpatient clinical trial of ketamine infusion for treatment of acute SCD pain.
Methods: A mixed-methods design integrated quantitative survey data from 70 sickle cell and emergency medicine clinicians with qualitative insights from 10 patient focus group participants. Survey responses (n = 77 total, including seven registered nurses) were analyzed descriptively and via Fisher’s exact and Mann–Whitney U-tests, while focus groups were thematically coded using themes from the Consolidated Framework for Implementation Research.
Results: Clinicians showed varied comfort levels with ketamine, with significant differences between sickle cell and emergency medicine clinicians. Barriers to future trials included the lack of standardized protocols (50.6%) and providers’ attitudes regarding ketamine (32.5%). Patients cited trust in providers and potential health benefits as key facilitators but also expressed concerns about safety, confidentiality, and time commitment of trial participation.
Conclusion: Successful implementation of inpatient trials of pain interventions, such as ketamine infusions, requires a multidisciplinary approach, transparent communication about risks, strong clinical frameworks, and patient-centered trial designs. While study limitations, such as potential selection bias and low survey response rate, should be considered, these findings provide actionable insights to guide the design of future clinical trials and improve non-opioid pain management for SCD.
Keywords: sickle cell disease, acute pain, ketamine, clinical trial
Introduction
Sickle cell disease (SCD) is the most common inherited red blood cell disorder worldwide, affecting more than 7.7 million people.1 Severe, episodic acute pain from vaso-occlusive events (VOEs) is the hallmark of the disease. High dose opioids remain the standard treatment for acute SCD pain.2–4 However, inpatient management of pain remains ineffective and unsatisfactory for individuals living with SCD.5 The presence of chronic/persistent pain in 50–60% of adults living with SCD makes attaining effective pain management for acute SCD pain even more challenging.6,7 Chronic SCD pain is poorly understood and often challenging to distinguish from acute pain for both providers and patients. Consequently, it is often treated similarly to acute SCD pain, with high-dose opioids, which is not only ineffective but potentially harmful due to opioid induced hyperalgesia.8
Despite major gaps in pain management, most research and trials in SCD have focused on disease-modifying therapies for VOE prevention, with limited attention given to symptomatic pain management.9–14 There is an urgent need for effective non-opioid pain therapies in SCD. Recently, low-dose ketamine infusion has gained attention as a potential opioid-sparing adjunct for acute SCD pain,15 showing promise for reducing opioid-induced hyperalgesia and helping those with underlying chronic pain.16,17 However, ketamine use carries risks, including dizziness, nausea, hallucinations, dissociation and transient increase in blood pressure. Repeated ketamine administration in patients with frequent admissions may pose additional risks, including potential cognitive effects and tachyphylaxis, which should be considered when designing clinical trials and treatment protocols.16
Research on ketamine infusions for SCD pain remains limited, partly due to the complexity of conducting large, multicenter inpatient pain clinical trials in SCD.18,19 The IMPROVE study highlighted numerous challenges, such as recruitment issues, enrollment difficulties, and variability in SCD pain management, leading to early trial termination.18 Understanding the perspectives of key stakeholders, including individuals living with SCD and clinicians, is crucial for addressing these challenges. This study used clinician surveys and patient focus groups to explore perceptions regarding ketamine and barriers and facilitators to potential clinical trials for acute SCD pain, offering insights for future trial designs.
Methods
Study Design
The study used a mixed-method design, combining quantitative surveys administered to clinicians to assess their perspectives on ketamine infusion use in SCD, alongside focus groups conducted with adults living with SCD to explore their perspectives.
Ethics
This study protocol was reviewed by the Duke University Institutional Review Board (IRB) and determined to meet the criteria for exemption under Category 2 research, in accordance with United States federal regulations from the Office of Human Research Protections (OHRP). Category 2 research involves collecting data through surveys, interviews, or focus groups where participants remain anonymous, and the information gathered poses minimal risk if disclosed publicly. Based on these federal guidelines, the study was exempt from further IRB review. The IRB also approved a waiver of signed consent documentation for all components of the study, including both the surveys and focus groups. Verbal consent was obtained in lieu of written consent, consistent with the standards outlined in the National Institutes of Health (NIH) and Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule guidelines for exempt Category 2 research. As part of the verbal informed consent process, participants were informed that anonymized responses and direct quotes could be included in publications, and this was witnessed and documented by the study team. This approach is standard practice across institutions in the United States for studies involving surveys and focus groups and complies with HIPAA and the guidelines outlined in the Declaration of Helsinki.
Focus Groups
Sample and Recruitment
The study aimed to recruit 12–15 participants across two focus groups, with 4–6 participants each, a number considered sufficient for thematic saturation.20 Eligible participants were US-based adults with an SCD diagnosis, excluding non-English speakers. Recruitment ads were placed on social media platforms (Facebook and Reddit) for seven days in January 2023, yielding 95 responses. From these, 25 individuals were randomly selected for screening calls to confirm eligibility (ie sociodemographics and SCD diagnosis) and availability. Verbal consent was obtained during the calls. Twelve participants agreed to participate, with 10 attending the focus groups (5 per group).
Procedures
The focus group guide, which was based on the Consolidated Framework for Implementation Research (CFIR), targeted CFIR constructs most relevant to trial implementation (intervention characteristics, inner setting, and outer setting).21 The guide was reviewed by a consultant from the Qualitative Research Service Team at the North Carolina Translational and Clinical Sciences Institute (NC TraCS) and a patient advisor with lived experience of SCD. Questions covered participants’ experiences or knowledge about ketamine and presented a hypothetical clinical trial of ketamine infusion for treatment of acute SCD pain. Participants were provided background information about ketamine and then asked about factors influencing their likelihood of participating in such a trial.
The focus groups were conducted remotely using an institutional Zoom account in March 2023. Participants were asked to join from an isolated and quiet location. A patient advisor with lived experience with SCD was trained by a qualitative research consultant from NC TraCS to facilitate the focus groups. This training included participation in two mock focus groups: one with the lead investigator and members of the NC TraCS team, and a second with the research team. The sessions were recorded and securely stored. The lead investigator, MK, was present during both focus groups to provide support as needed, including providing a background on ketamine to ensure all participants had basic knowledge about ketamine prior to answering questions about clinical trial participation. Participants received compensation for their involvement, and each focus group session lasted approximately 90 minutes.
Analysis
Audio recordings were transcribed verbatim by an IRB approved vendor. Transcripts were verified by two members of the study team (TO and MK). Data were coded using a rapid coding process, with codes derived from selected CFIR themes. Initially, TO and MK independently applied codes using deductive approaches, later cross-referencing their work for thematic consistency and to explore interrelationships between codes. Coding was performed manually using Microsoft Excel. The coders held iterative discussions based on structured reconciliation framework, maintaining an audit trail to ensure transparency in decision-making. Consensus was reached through mutual agreement. After coding was completed, the final themes were reviewed by the lead investigator, MK, to ensure alignment with the study’s research objectives. Due to logistical constraints, member checking was not conducted. Peer debriefing and a consensus-based reconciliation framework, as detailed previously, were used to enhance reliability.
Survey
Sample and Recruitment
Clinicians specializing in SCD care were recruited via a purposive sampling approach. Survey invitations were sent through specialty-specific listservs. The SCD listserv included 130 clinicians, as previously published.22 Two academic emergency medicine listservs, covering around 100 members, were also used. Seventy-seven individuals, among whom 70 were clinicians (62 physicians and 8 advanced practice providers) and 7 were registered nurses, responded to the survey. Among the clinicians, 34 were from emergency medicine and 29 were SCD providers.
Procedures
The survey was developed using CFIR to guide question formulation and was reviewed for face validity by an external team, including an SCD researcher with qualitative expertise and two additional SCD clinicians/researchers. Participants received three Email invitations between June 19 and September 12, 2023. Built in REDCap, the survey questions assessed clinicians’ ketamine use experience, barriers to ketamine administration for acute SCD pain and timing considerations for ketamine initiation. Demographic data were also collected.
Analysis
Survey data were analyzed using R version 4.4.0. Data cleaning involved collapsing and identifying key respondent groups. Surveys were considered complete if respondents indicated their profession. Agree/disagree variables were coded as factor variables, and checklist questions (eg, barriers) were transformed into single variables for simplified analysis. Response options with no entries were recorded as 0 rather than being excluded. Missing responses to ketamine perception and barriers questions ranged 8–10% with no significant differences between emergency medicine and sickle cell clinicians. Descriptive statistics summarized survey questions, with categorical responses as frequencies and percentages, and continuous variables as mean (SD) or median [IQR]. Fisher’s exact tests were used for categorical data, and Mann–Whitney U-tests for non-parametric continuous data. No multiple comparison adjustments were made, except where Bonferroni correction was applied to checklist questions (eg, barriers). For example, with 17 possible barriers, an adjusted alpha threshold of 0.003 (0.05/17) was calculated to determine significance. Visualizations of survey responses were created using R packages, including ggplot2 and ggpubr.
Results
Focus Groups
The study included 10 African American adults with SCD, ages 19 to 32 years old, evenly split by gender. Two participants received care at comprehensive academic sickle cell center, while eight were seen in community-based hospitals. Three had received ketamine infusions for acute SCD pain in the past. Discussions were organized into three main areas: perceptions of ketamine, facilitators to trial participation, and barriers to trial participation, guided by CFIR constructs. Table 1 details the identified themes and subthemes.
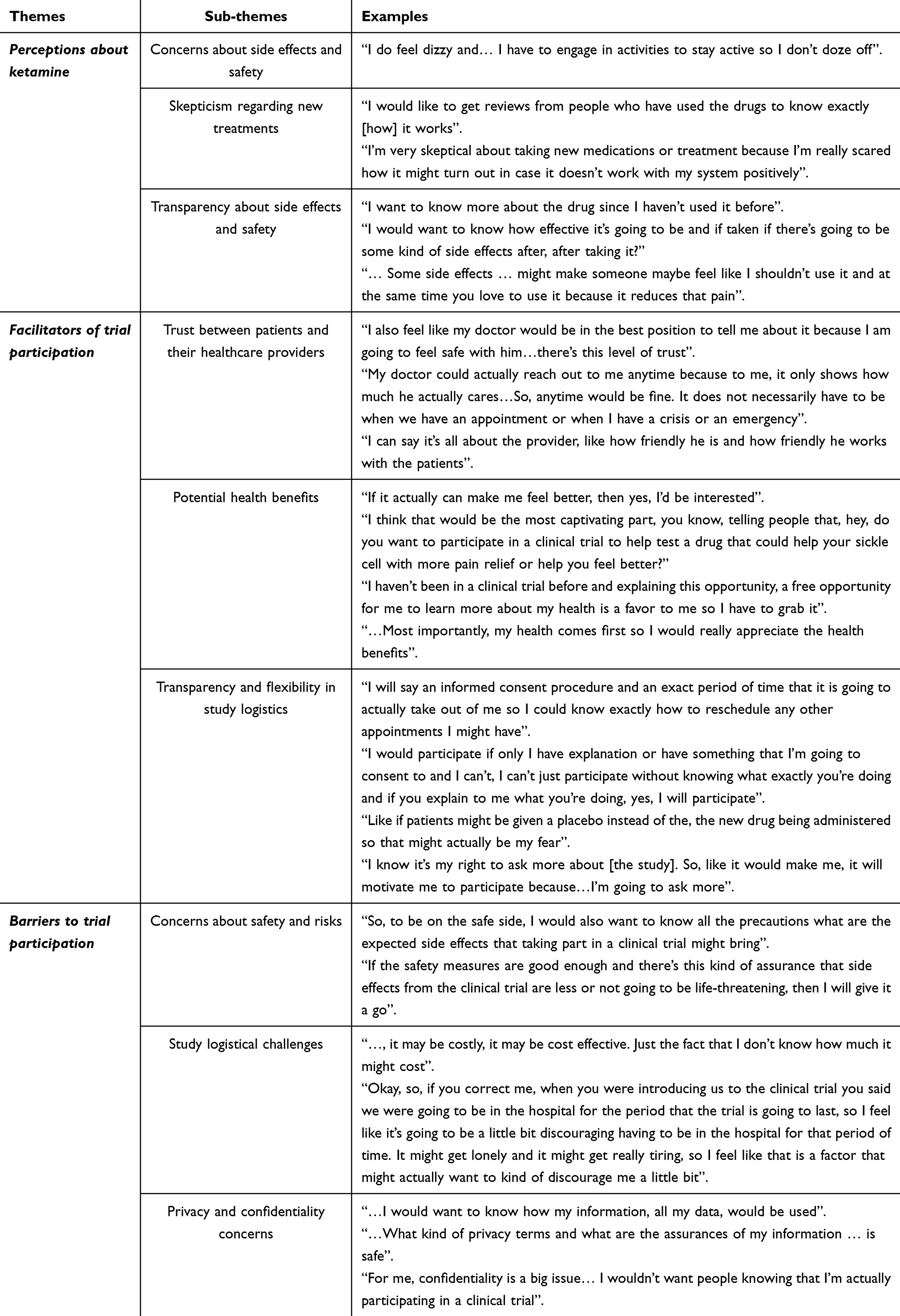 |
Table 1 Description of Emerging Themes from Focus Group Interviews |
Perceptions About the Intervention (Ketamine)
Participants expressed varied views on ketamine as a treatment for acute SCD pain. While some had prior experience with ketamine, most were unfamiliar and wanted more information. A recurring theme was concern about side effects and safety. The three participants with previous ketamine experience described significant side effects, with one sharing,
Sometimes you feel like you’re disconnected from the world and… you are having some dreams, like feelings out of your body experiences.
For participants without ketamine experience, skepticism regarding new treatments and a desire for transparency about side effects and safety emerged as recurrent subthemes. One participant expressed,
I’m very skeptical about taking new medications or treatment because I’m really scared how it might turn out in case it doesn’t work with my system positively.
Participants expressed a desire to understand the full range of side effects and their duration. One participant remarked,
I think I would love to know the various side effects and how long does it take for the side effects to manifest…
Facilitators to Trial Participation
Several factors were identified that could encourage trial participation among participants. Trust between patients and their healthcare providers emerged as a key facilitator. Participants consistently emphasized that they would be more likely to participate if their primary sickle cell provider recommended the trial. One participant shared,
I feel like my doctor would be in the best position to tell me about it because I am going to feel safe with him… there’s this level of trust.
Additionally, participants preferred to discuss trial participation when they were not experiencing a pain crisis. As one participant shared
I can say that I think it’s at that time that we have an appointment because you know, at that time I have already made my time available…
Participants were also motivated by potential health benefits. As one participant noted,
If it benefits me health wise, I would love to participate.
This prospect of learning more about their health and gaining access to potentially beneficial treatments was an important motivator.
Transparency and flexibility in study logistics were other important facilitators. Participants also emphasized the importance of flexible scheduling, with some suggesting that home-based participation could make trials more accessible.
Maybe a doctor could go to the residence of that person if they can’t make it to the hospital.
One participant suggested. Another added,
If they had transportation for people who couldn’t get to the study site, it would make it easier.
These statements were made despite the facilitator explaining that the trial would take place in the hospital, with potential outpatient follow-up. Participants also desired to know the details of the study procedures. One participant stated,
I can’t just participate without knowing what exactly you’re doing and if you explain to me what you’re doing, yes, I will participate.
Barriers to Trial Participation
Participants also highlighted several potential barriers that might prevent them from participating in this hypothetical inpatient clinical trial. Concerns about safety and risks were frequently mentioned. One participant stated
I would also want to know if there would be any risk. No matter how little they may be, I would like to be informed so I would know what I’m actually getting myself into.
Another participant raised questions about ketamine’s approval status:
For the ketamine clinical trial, I would like to know is ketamine already a drug that has been approved… or are people participating in the clinical trial the first ones to use the drug?
Study logistical challenges were another concern, particularly the time commitment and whether participation in a trial would extend their inpatient stay. One participant said,
It’s going to be a little bit discouraging having to be in the hospital for that period of time. It might get lonely and it might get really tiring.
Additionally, participants considered the length of the trial important when the possibility of outpatient longitudinal follow-up was introduced into the trial scenario. A shorter study appeared appealing, with one participant stating,
I really don’t want to participate in a study for close to two months. It might get tiring and draining at the end, so something like two weeks to a month would be great.
Privacy and confidentiality concerns were raised by several participants with them wanting assurance on data handling, as a participant noted,
I would want to know how my information, all my data, would be used… if they are going to go publicly, like as in publishing publicly, or if they are going to keep it [confidential].
Provider Survey
Among the 70 clinicians who completed the survey, 29 were sickle cell clinicians (13 adult hematologists, 13 pediatric hematologists, 2 internal medicine clinicians, and 1 APP), and 34 were emergency medicine physicians. Most (N = 57, 98.3%) practiced at academic hospitals, predominantly in urban settings (N = 41, 71.9%). Additional demographics and practice experience are outlined in Table 2.
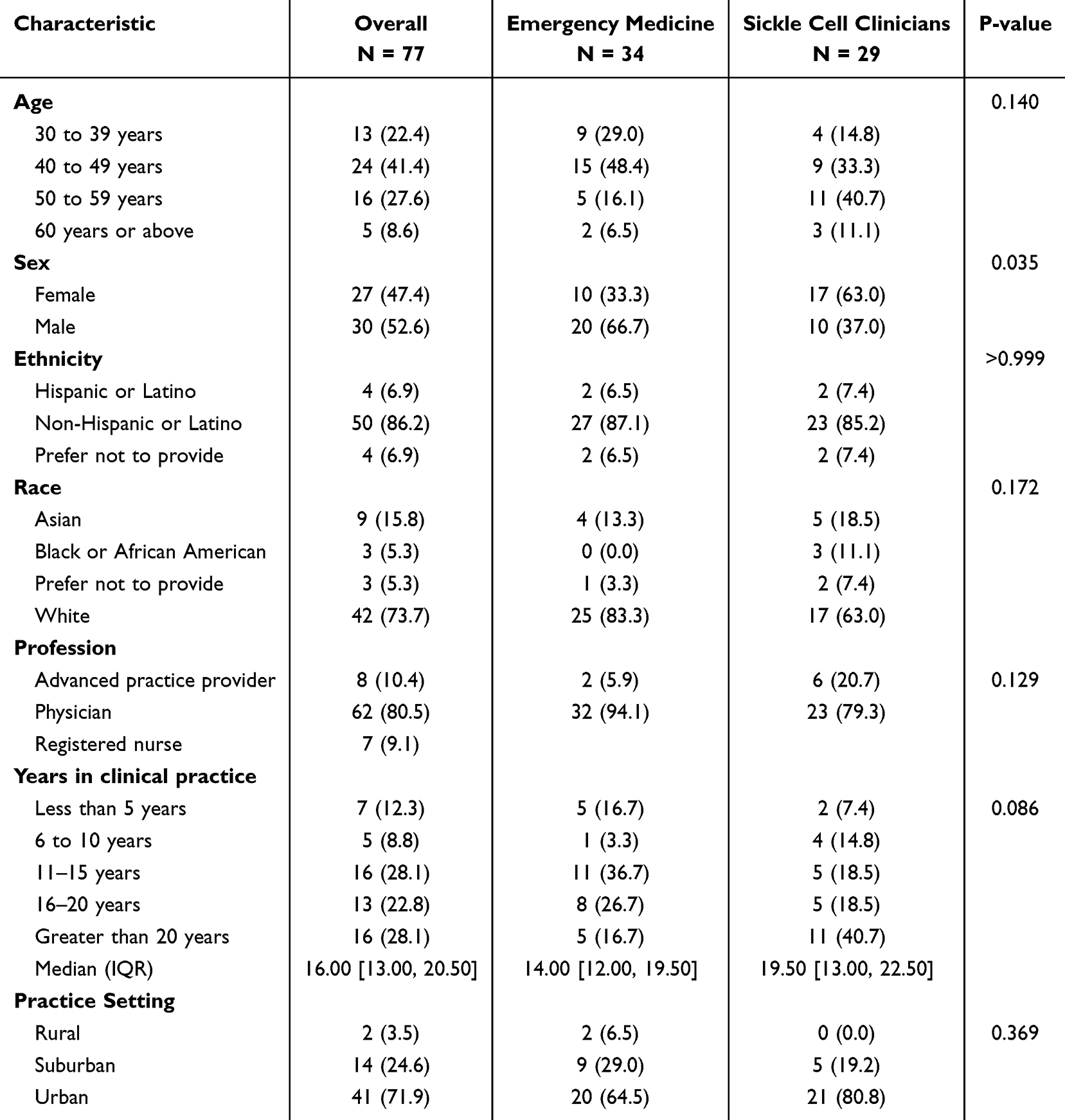 |
Table 2 Demographic and Practice Characteristics of Survey Respondents, (N, %) or Median (IQR) |
Perceptions/Comfort with Ketamine
Most clinicians were comfortable managing acute SCD pain (Table 3). However, SCD clinicians were more comfortable managing chronic SCD pain compared to emergency clinicians (p = 0.008), but less comfortable with ketamine infusions (p = 0.002). There were no significant differences in attitudes toward the use of ketamine for acute SCD pain management. Most agreed that ketamine is appropriate for acute SCD pain management (N = 15 [24.6%] strongly agreed; N = 34 [55.7%] agreed), but many were neutral or disagreed that it should be first line (N = 16 [25.8%] neutral; N = 28 [45.2%] disagree or strongly disagree). Many felt the quality of evidence for ketamine acute SCD pain was poor, with over 40% indicating a need for an RCT confirming efficacy before considering its use. Table 3 further details perceptions regarding ketamine.
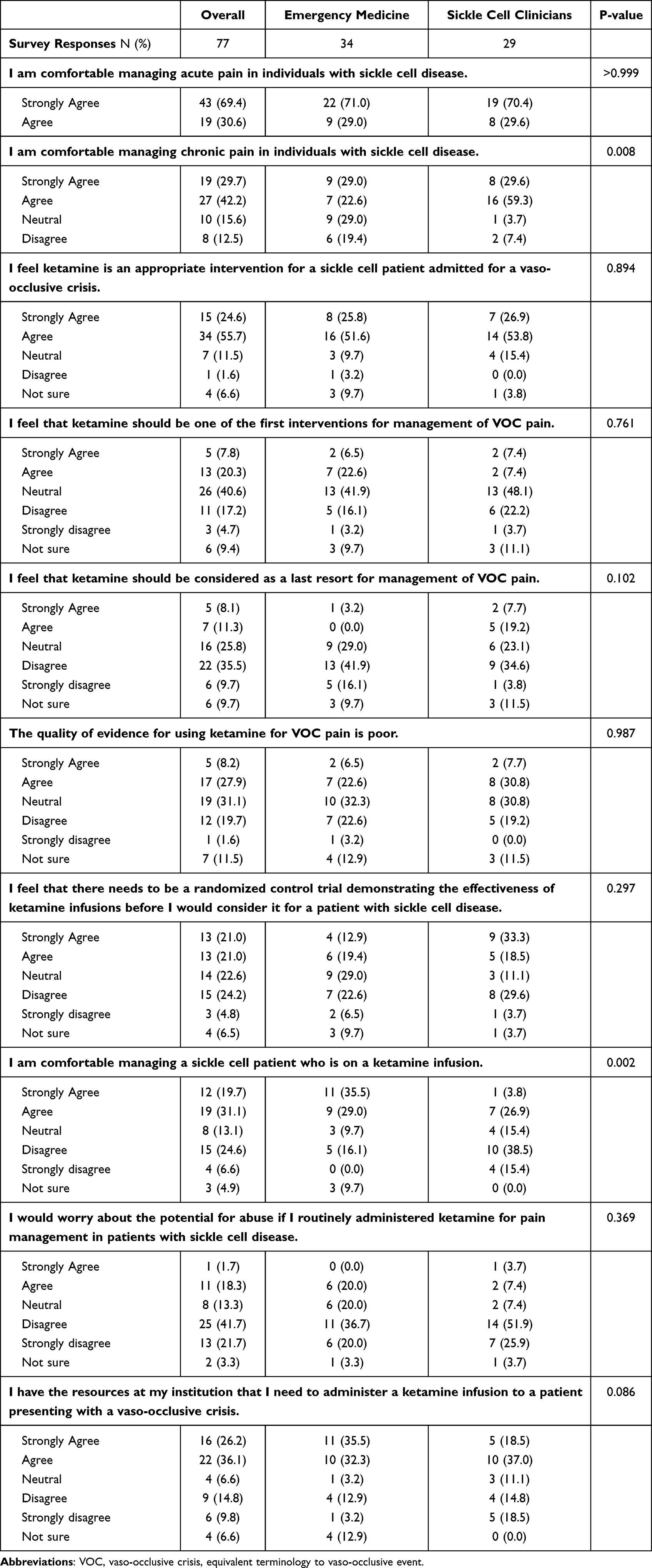 |
Table 3 Assessment of Clinician’s Comfort and Experience with Ketamine Infusions for Acute Sickle Cell Pain |
Barriers and Facilitators for Ketamine Use
Several barriers to ketamine infusion use for acute SCD pain secondary to a VOE were reported (Figure 1). The most common was the lack of standardized protocols (N = 39, 50.6%), followed by provider attitudes (N = 25, 32.5%). Forty-six percent of SCD clinicians stated that their institution lacked a standard protocol. Concerns about nursing staff shortage (N = 20, 26%) and nurse-to-patient ratios (N = 22, 28.6%) were also cited. SCD clinicians specifically noted pain medicine consultation as a barrier (N = 14, 48.3%, p < 0.001), and 37% disagreed that pain specialists are readily available for consultation on patients admitted with refractory acute SCD pain. Around 36% felt SCD patients were reluctant to use ketamine for their pain.
 |
Figure 1 Reported barriers to ketamine infusion use for management of acute pain secondary to vaso-occlusive episodes by clinician specialty. The figure shows the percentage of all respondents, emergency medicine, and hematology/internal medicine (ie, sickle cell) clinicians identifying key barriers to ketamine use. Significant differences between specialties are noted with an asterisk (*). |
In a hypothetical scenario where an RCT demonstrated ketamine infusions’ efficacy, differences emerged between specialties. Forty percent of SCD clinicians said they would be unable to start ketamine due to institutional policies, compared only 13% of emergency medicine clinicians (p = 0.0027). Regarding timing, 23% of SCD clinicians reported they would start ketamine in the ED, while 34.6% would start on admission day one. Most emergency clinicians would start ketamine in the ED immediately upon rooming, rather than waiting for admission.
Discussion
Despite growing interest in ketamine as an adjunctive therapy for acute SCD pain, evidence remains limited regarding its efficacy and safety for managing acute pain during VOEs.15,16 The American Society of Hematology’s guidelines for acute and chronic SCD pain management recommend ketamine infusions as an option for pain refractory to opioids,15 but support primarily stems from case reports8,16,17 and two RCTs in emergency care settings, which tested single ketamine boluses against morphine.9,10 These studies provided limited insights into broader ketamine use for acute SCD pain. This study addresses a critical gap exploring barriers and facilitators to trial participation and ketamine implementation for acute SCD pain. Our findings emphasize the importance of a multidisciplinary approach, highlighting patient trust, transparent communication and institutional preparedness as key factors for implementing clinical trials in SCD pain management.18,23 This study is significant, as it highlights the complexities and coordination required for effective acute pain management in SCD – an ongoing challenge despite advancements in other therapeutic areas – while offering practical insights into how inpatient clinical trials can be better designed to engage both clinicians and patients.
Perceptions and Comfort with Ketamine
Clinicians and patients expressed varying levels of comfort with ketamine. A key finding was that sickle cell clinicians were less comfortable with ketamine infusions compared to emergency medicine clinicians, despite experiences managing SCD pain. This likely reflects differences in standard practices and familiarity with ketamine. Emergency medicine clinicians routinely use ketamine and are more comfortable with it for pain relief in SCD.24 In inpatient settings, pain medicine consultations are often required to initiate ketamine, so sickle cell providers are not directly administering or managing infusions.15 However, strong clinical frameworks and communication are essential for the success of inpatient trials,18,19 and sickle cell providers play a critical role in educating potential research participants to optimize recruitment efforts.25 Addressing this gap in knowledge among SCD providers is crucial for securing buy-in for large multicenter trials involving ketamine or other novel pain interventions in SCD. Focus group participants emphasized the need for transparency about ketamine’s side effects and safety. Those previously treated with ketamine described symptoms such as dizziness, disorientation, and hallucinations, which contributed to skepticism among participants unfamiliar with the drug.
These findings indicate a shared perception among both clinicians and patients regarding the need for a deeper understanding of ketamine’s complexity and associated risks. Administered intravenously, ketamine requires careful dosing and monitoring, making it more complex compared to standard oral medications.16 Insights from this study and others suggest that the CFIR domain of intervention characteristics –particularly its complexity– plays an important role in stakeholder buy-in for clinical trials. For example, a trial involving a single oral dose of gabapentin for pain during a VOE saw rapid initial enrollment due to its simple study design.19 This does not mean that complex interventions like ketamine are unfeasible, but they require a robust clinical framework to address the added complexity.18,26 To address patient concerns about risks and clinician apprehension regarding dosing, successful trial implementation requires clear communication between experts (eg, pain medicine specialists) and the primary clinical teams. This includes educating all stakeholders on the drug’s properties and monitoring requirements. For patients, educational initiatives should provide jargon-free explanation on intervention benefits and how risks are managed in the hospital setting.
Studies on research engagement among minoritized communities highlight transparency as crucial to building trust and increasing willingness for trial participation.26–28 This is especially true in SCD, where historical research misconduct and systemic and interpersonal racism contribute to distrust in healthcare and research.29 Transparency around interventions with limited data, such as ketamine for acute SCD pain, is critical for fostering trust and encouraging participation.
Facilitators to Trial Participation
In this study, trust between patients and their healthcare providers emerged as a major facilitator of trial participation. Focus group participants consistently stated that they would be more inclined to participate if their SCD provider recommended the trial. These findings align with prior research and suggest that trust between patients and providers plays a key role in both initial trial participation and sustained engagement.18,25,26,28 Trust, in this context, is multifaceted – participants valued both transparency about the trial’s details and the long-standing relationships they had with their SCD providers. Familiarity and history with their regular care teams strengthened participants’ comfort with trial participation.
Participants preferred discussing trials during non-crisis times, such as routine clinical visits, to avoid stress during pain crises. Research supports this, showing that the timing of trial presentations can impact participation.26,30 This aligns with the CFIR domain of “inner setting”, particularly the construct of “networks and communication”, where strong relationships and open dialogue between patients and providers foster research engagement. Inpatient trials face challenges due to time-sensitive enrollment and limited hospital stays. VOEs are episodic and unpredictable, so leveraging established relationships with regular providers can facilitate enrollment, even in inpatient settings. This approach mirrors other high-risk conditions, such as in seizure conditions, where elements of informed consent are often discussed prior to the acute event, streamlining enrollment during emergencies.31,32
Focus group participants were also motivated by the potential health benefits of ketamine, expressing interest in participating if the intervention could meaningfully improve their pain and quality of life. Clinicians in emergency medicine and SCD were willing to initiate ketamine infusions early during treatment for a VOE if presented with RCT evidence of its efficacy. Within the CFIR framework, the construct of “evidence strength and quality” –stakeholders’ perceptions of evidence supporting the intervention’s outcomes– could be a strong facilitator for trial implementation. Educating stakeholders about ketamine’s potential benefits in acute SCD pain management is crucial for trial participation.
Barriers to Trial Participation
Relatively few symptomatic pain intervention trials for acute SCD pain have been conducted. Most have been characterized by poor enrollment and retention and barriers like care coordination with emergency and inpatient teams and protocol standardization.13,18,19,28 In this study, key barriers included safety concerns, logistical challenges and time commitments, particularly if trials extended hospital stays. Isolation and fatigue during trials were frequent concerns among patients. To address this, trial designs should emphasize that (1) participation will not unnecessarily prolong the duration of hospital stay, (2) offer outpatient follow-up options, and (3) reduce isolation to improve engagement. If ketamine proves effective, it could potentially shorten the length of hospital stays by more rapidly controlling pain. Privacy and confidentiality concerns were also significant, with participants seeking reassurance that their personal data would remain confidential. Clear communication about data protection and confidentiality can help alleviate these concerns and foster trust. Among clinicians, logistical challenges in the inpatient setting, such as a lack of established protocols and variability in comfort with ketamine, were common barriers. For instance, 46% of sickle cell clinicians reported that their institution lacked standard guidelines for administering ketamine for acute SCD pain, suggesting a critical need for standardized protocols and education.
These findings once again underscore CFIR construct of “networks and communication”, emphasizing how effective clinician-patient communication is crucial for overcoming barriers in clinical trial implementation. Strong organizational communication networks also ensure that all stakeholders are informed and aligned, especially with complex interventions like ketamine infusions. Additionally, the “inner setting” CFIR construct highlights that organizational readiness –established protocols, adequate resources, and clear communication pathways across specialties– is essential for successful trial implementation in complex settings like inpatient SCD care.
Strengths and Limitations
This study has notable strengths, including its mixed-methods design and diverse stakeholder inclusion – healthcare professionals specializing in SCD and individuals living with SCD – which allowed for a detailed exploration of barriers, facilitators, and knowledge gaps in acute SCD pain trials. The use of CFIR provided a strong theoretical basis for data collection and analysis. However, limitations include the possibility of selection bias, as focus group participants were recruited via social media platforms, potentially affecting broader representativeness. Additionally, the clinician survey was limited to those responding via professional listservs and had a low response rate, which may also introduce selection bias. We were unable to perform subgroup analyses comparing pediatric and adult providers or differences between suburban and academic settings due to the survey sample size, though these perspectives would provide valuable insights into variations in pain management approaches. Additionally, while nurses are essential in executing inpatient pain protocols, our small sample of nurse respondents did not allow for a comprehensive assessment of their perspectives on ketamine use. Future studies should aim to capture these viewpoints to further refine strategies for trial design and implementation.
Member checking was not performed for the focus groups, which could limit the credibility of the qualitative findings, although peer debriefing and a reconciliation framework were used to enhance data reliability. Importantly, the study did not aim to gather SCD patients’ ketamine treatment experiences but rather explored reactions to ketamine as an analgesic and perspectives regarding participation in potential inpatient ketamine clinical trial. While ketamine use is increasing in SCD care, it remains relatively uncommon and is often reserved for refractory cases, particularly in non-academic hospital settings.16 Including participants from community settings, who are often underrepresented in SCD research, is a notable strength of the study. By identifying both barriers and facilitators, this study provides insights for designing future trials of non-opioid analgesics, such as ketamine infusions, for acute SCD pain management.
Conclusions
This study explored clinician and patient perspectives on barriers and facilitators to conducting an inpatient clinical trial of ketamine for acute SCD pain, addressing a critical gap in SCD pain management. Findings highlight the need for multidisciplinary collaboration, strong clinical frameworks, and transparent communication to improve trial feasibility and participation. Clinician concerns regarding ketamine use, particularly safety and dosing familiarity, underscore the importance of institutional preparedness, while patients emphasized trust in providers and logistical considerations as key factors in trial participation. Understanding these perspectives is essential for optimizing trial recruitment and implementation, especially for complex pain interventions. Future research should build on these findings to refine clinical trial designs that are both feasible and patient-centered.
Data Sharing Statement
The data and supporting materials are available from the corresponding author upon request.
Acknowledgments
The authors thank our patient advisor and North Carolina Translational and Clinical Sciences Institutes’ Qualitative Research Team for their assistance in conducting the focus groups in this study.
Funding
This work was supported by funding from the National Institute of Neurological Disorders and Stroke (3U24NS114416-01S2).
Disclosure
Dr Alexander Limkakeng reports grants from NIH, during the conduct of the study; grants from Roche, Inc., Abbott Laboratories, Siemens, Forest Devices, Inc., SENSE Neuro Diagnostics, and Ophirex, Inc., outside the submitted work. The authors have no other conflicts of interest in this work.
References
1. Thomson AM, McHugh TA, Oron AP, et al. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Haematol. 2023;10(8):e585–e599. doi:10.1016/S2352-3026(23)00118-7
2. Ballas SK, Gupta K, Adams-Graves P. Sickle cell pain: a critical reappraisal. Blood. 2012;120(18):3647–3656. doi:10.1182/blood-2012-04-383430
3. Fosdal MB, Wojner-Alexandrov AW. Events of hospitalization among children with sickle cell disease. J Pediatr Nurs. 2007;22(4):342–346. doi:10.1016/j.pedn.2006.09.001
4. Shah N, Bhor M, Xie L, Paulose J, Yuce H. Sickle cell disease complications: prevalence and resource utilization. PLoS One. 2019;14(7):e0214355. doi:10.1371/journal.pone.0214355
5. Maxwell K, Streetly A, Bevan D. Experiences of hospital care and treatment seeking for pain from sickle cell disease: qualitative study. BMJ. 1999;318(7198):1585–1590. doi:10.1136/bmj.318.7198.1585
6. Smith WR, Penberthy LT, Bovbjerg VE, et al. Daily assessment of pain in adults with sickle cell disease. Ann Intern Med. 2008;148(2):94–101. doi:10.7326/0003-4819-148-2-200801150-00004
7. Kenney MO, Wilson S, Shah N, et al. Biopsychosocial factors associated with pain and pain-related outcomes in adults and children with sickle cell disease: a multivariable analysis of the GRNDaD multicenter registry. J Pain. 2023;25(1):153–164. doi:10.1016/j.jpain.2023.07.029
8. Kenney MO, Smith WR. Moving toward a multimodal analgesic regimen for acute sickle cell pain with non-opioid analgesic adjuncts: a narrative review. J Pain Res. 2022;15:879–894. doi:10.2147/JPR.S343069
9. Lubega FA, DeSilva MS, Munube D, et al. Low dose ketamine versus morphine for acute severe vaso occlusive pain in children: a randomized controlled trial. Scand J Pain. 2018;18(1):19–27. doi:10.1515/sjpain-2017-0140
10. Alshahrani MS, AlSulaibikh AH, ElTahan MR, et al. Ketamine administration for acute painful sickle cell crisis: a randomized controlled trial. Acad Emerg Med. 2022;29(2):150–158. doi:10.1111/acem.14382
11. Schlaeger JM, Molokie RE, Yao Y, et al. Management of Sickle Cell Pain Using Pregabalin: a Pilot Study. Pain Manag Nurs. 2017;18(6):391–400. doi:10.1016/j.pmn.2017.07.003
12. Bartolucci P, El Murr T, Roudot-Thoraval F, et al. A randomized, controlled clinical trial of ketoprofen for sickle-cell disease vaso-occlusive crises in adults. Blood. 2009;114(18):3742–3747. doi:10.1182/blood-2009-06-227330
13. Perlin E, Finke H, Castro O, et al. Enhancement of pain control with ketorolac tromethamine in patients with sickle cell vaso-occlusive crisis. Am J Hematol. 1994;46(1):43–47. doi:10.1002/ajh.2830460108
14. Rousseau V, Morelle M, Arriuberge C, et al. Efficacy and tolerance of lidocaine 5% patches in neuropathic pain and pain related to vaso‐occlusive sickle cell crises in children: a prospective multicenter clinical study. Pain Pract. 2018;18(6):788–797. doi:10.1111/papr.12674
15. Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain. Blood Adv. 2020;4(12):2656–2701. doi:10.1182/bloodadvances.2020001851
16. Alshahrani MS, Alghamdi MA. Ketamine for sickle cell vaso-occlusive crises: a systematic review. Saudi J Med Med Sci. 2021;9(1):3–9. doi:10.4103/sjmms.sjmms_218_20
17. Kenney MO, Becerra B, Mallikarjunan A, Shah N, Smith WR. Early initiation of sub-anesthetic ketamine infusion in adults with vaso-occlusive crises is associated with greater reduction in sickle cell pain intensity: a single center’s experience. Pain Med Malden Mass. 2022;23(12):2042–2049. doi:10.1093/pm/pnac094
18. Dampier CD, Smith WR, Wager CG, et al. IMPROVE trial: a randomized controlled trial of patient-controlled analgesia for sickle cell painful episodes: rationale, design challenges, initial experience, and recommendations for future studies. Clin Trials Lond Engl. 2013;10(2):319–331. doi:10.1177/1740774513475850
19. Nottage KA, Hankins JS, Faughnan LG, et al. Addressing challenges of clinical trials in acute pain: the pain management of vaso-occlusive crisis in children and young adults with sickle cell disease study. Clin Trials Lond Engl. 2016;13(4):409–416. doi:10.1177/1740774516636573
20. Hennink MM, Kaiser BN, Weber MB. What influences saturation? Estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
21. Damschroder LJ, Aron DC, Keither RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(50). doi:10.1186/1748-5908-4-50
22. Kenney MO, Becerra B, Beatty SA, Smith WR. Telehealth acceptability and opioid prescribing patterns of providers of painful chronic diseases during the COVID-19 pandemic: a survey of sickle cell providers. J Opioid Manag. 2021;17(6):489–497. doi:10.5055/jom.2021.0683
23. Darbari DS, Sheehan VA, Ballas SK. The vaso-occlusive pain crisis in sickle cell disease: definition, pathophysiology, and management. Eur J Haematol. 2020;105(3):237–246. doi:10.1111/ejh.13430
24. Corwell BN, Motov SM, Davis NL, Kim HK. Novel uses of ketamine in the emergency department. Expert Opin Drug Saf. 2022;21(8):1009–1025. doi:10.1080/14740338.2022.2100883
25. Badawy SM. Clinical trial considerations in sickle cell disease: patient-reported outcomes, data elements, and the stakeholder engagement framework. Hematol Am Soc Hematol Educ Program. 2021;2021(1):196–205. doi:10.1182/hematology.2021000252
26. Fogel DB. Factors associated with clinical trials that fail and opportunities for improving the likelihood of success: a review. Contemp Clin Trials Commun. 2018;11:156–164. doi:10.1016/j.conctc.2018.08.001
27. Ford JG, Howerton MW, Bolen S, et al. Knowledge and access to information on recruitment of underrepresented populations to cancer clinical trials. Evid Rep Technol Assess. 2005;122:1–11. doi:10.1037/e439572005-001
28. Lee LH, Whisenton LH, Benger J, Lanzkron S. A community-centered approach to sickle cell disease and clinical trial participation: an evaluation of perceptions, facilitators, and barriers. Blood Adv. 2021;5(23):5323–5331. doi:10.1182/bloodadvances.2020003434
29. Power-Hays A, McGann PT. When actions speak louder than words - racism and sickle cell disease. N Engl J Med. 2020;383(20):1902–1903. doi:10.1056/NEJMp2022125
30. Logan JK, Tang C, Liao Z, et al. Analysis of factors affecting successful clinical trial enrollment in the context of three prospective, randomized, controlled trials. Int J Radiat Oncol Biol Phys. 2017;97(4):770–777. doi:10.1016/j.ijrobp.2016.11.035
31. Niznick N, Lun R, Dewar B, Perry J, Dowlatshahi D, Shamy M. Advance consent for participation in randomised controlled trials for emergency conditions: a scoping review. BMJ Open. 2023;13(2):e066742. doi:10.1136/bmjopen-2022-066742
32. Navarro V, Dagron C, Demeret S, et al. A prehospital randomized trial in convulsive status epilepticus. Epilepsia. 2011;52(Suppl 8):48–49. doi:10.1111/j.1528-1167.2011.03236.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Ketamine versus Magnesium Sulphate as Adjuvants to Levobupivacaine in Ultrasound Bilevel Erector Spinae Block in Breast Cancer Surgery (a Double-Blinded Randomized Controlled Study)
El Sherif FA, Youssef HA, Fares KM, Mohamed SAB, Ali AR, Thabet AM
Local and Regional Anesthesia 2022, 15:87-96
Published Date: 23 September 2022