")
Back to Journals » International Journal of Nanomedicine » Volume 20
Extracellular Vesicles in Acute Kidney Injury: Mechanisms, Biomarkers, and Therapeutic Potential
Authors Yan Q, Liu M, Mao J, Zhao Z, Wang B
Received 24 January 2025
Accepted for publication 10 May 2025
Published 17 May 2025 Volume 2025:20 Pages 6271—6288
DOI https://doi.org/10.2147/IJN.S519345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lijie Grace Zhang
Qianqian Yan,1 Mengyuan Liu,2 Jinyan Mao,2 Zihao Zhao,1,3 Bo Wang4
1Nephrology Research Center, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, People’s Republic of China; 2Department of Anesthesiology, Air Force Hospital of Western Theater Command, PLA, Chengdu, 610011, People’s Republic of China; 3Department of Radiology, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, People’s Republic of China; 4Department of Nephrology, Institute of Kidney Diseases, West China Hospital of Sichuan University, Chengdu, 610041, People’s Republic of China
Correspondence: Zihao Zhao, Email [email protected] Bo Wang, Email [email protected]
Abstract: Acute kidney injury (AKI) has a high morbidity and mortality rate but can only be treated with supportive therapy in most cases. The diagnosis of AKI is mainly based on serum creatinine level and urine volume, which cannot detect kidney injury sensitive and timely. Therefore, new diagnostic and therapeutic molecules of AKI are being actively explored. Extracellular vesicles (EVs), secreted by almost all cells, can originate from different parts of the kidney and mediate intercellular communication between various cell types of nephrons. At present, numerous successful EV-based biomarker discoveries and treatments for AKI have been made, such as the confirmed diagnostic role of urine-derived EVs in AKI and the established therapeutic role of mesenchymal stem cell-derived EVs in AKI have been confirmed; however, these related studies lack a full discussion. In this review, we summarize the latest progression in the profound understanding of the functional role of EVs in AKI caused by various etiologies in recent years and provide new insights into EVs as viable biomarkers and therapeutic molecules for AKI patients. Furthermore, the current challenges and prospects of this research area are briefly discussed, presenting a comprehensive overview of the growing foregrounds of EVs in AKI.
Keywords: extracellular vesicles, acute kidney injury, mesenchymal stem cells, therapeutic molecules, diagnostic biomarkers
Introduction
Acute kidney injury (AKI) is a renal injury syndrome characterized by a rapid decline in kidney function, mainly manifested as elevated serum creatinine and decreased urine volume, often caused by cell damage in the nephron.1,2 Due to population differences and inconsistencies in standardized AKI classification, estimates of AKI prevalence range from < 1% to 66%.3 Epidemiological data show that the incidence of AKI can reach more than 20% of the hospitalized population and exceed 50% in specific hospital units, resulting in approximately 1.7 million deaths worldwide.1,2 The Kidney Disease: Improving Global Outcomes (KDIGO) 2012 Clinical Practice Guideline for Acute Kidney Injury summarized the causes of AKI based on many observational studies, which include sepsis, circulatory shock, cardiac surgery, nephrotoxic drugs, radiocontrast agents, burns, trauma and so on.4 AKI pathogenesis remains elusive but centers on proximal tubular epithelial cell (PTEC) injury. While initial damage triggers transient regenerative mechanisms involving dedifferentiation and proliferation, persistent damage triggers pathological cascades culminating in tubular atrophy, inflammatory infiltration, fibrotic remodeling, and irreversible progression to CKD.5,6 Despite the more profound understanding of AKI’s diagnosis, pathogenesis, and treatment, the complexity and heterogeneity of its origin, pathophysiology, and clinical processes remain considerable barriers to overcoming the major global public health problem.7 The key pathophysiological processes of the progressive progression of AKI are caused by various causes, such as inflammation after renal tissue damage and renal fibrosis caused by abnormal damage repair.8,9
Extracellular vesicles (EVs), defined by the International Society for Extracellular Vesicles (ISEV) as lipid bilayer-enclosed particles released from cells, serve as carriers of bioactive molecules (eg, proteins and nucleic acids).10 Owing to their ubiquitous presence in biofluids and stable molecular composition, EVs exhibit remarkable potential as minimally invasive liquid biopsy tools for monitoring disease progression.11 Complex intracellular pathways are regulated by the intrinsic properties of EVs, which enhance their potential utility in the therapeutic control of diseases.12,13 An increasing number of studies have demonstrated that EVs have emerged as a prominent research field, serving as potential diagnostic biomarkers and therapeutic molecules for multiple system diseases, including AKI,14,15 Alzheimer’s disease,16 Parkinson’s disease,17 prostate cancer,18 diabetes,19 lung injury20 and so on. Meanwhile, EVs contain a variety of bioactive molecules, such as lipids, proteins, nucleic acids, and metabolites, which play a vital role in kidney disease by participating in inflammation and fibrosis processes.21 In addition, EVs can be regarded as paracrine factors that participate in cell-to-cell communication in AKI and induce epigenetic reprogramming of injured kidney cells. Various sources of EVs, including renal tubular epithelial cells (TECs), vascular endothelial cells, and mesenchymal stem cells (MSCs), have been shown to ameliorate the pathological status of AKI and delay its progression through a wide range of mechanisms.22–24 However, other studies have suggested that genetic material carried by EVs derived from TECs promotes the activation and proliferation of macrophages and fibroblasts, leading to kidney inflammation and fibrosis.1,2
Much progress has been made in diagnosing and treating AKI, but it remains a non-negligible issue in medical treatment. Therefore, searching for more sensitive biomarkers and effective treatments is still crucial in future research. In this review, we highlight the updated advancement of EVs in AKI, focusing on their role in the diagnosis and treatment of AKI and their future development prospects. Furthermore, we critically evaluate persistent methodological challenges in EV research, particularly regarding standardization of isolation protocols, and hope to propose solutions to these problems in the future.
Extracellular Vesicles
General Characteristics and Biogenesis of EVs
EVs, which widely exist in almost all body fluids, including urine, blood, saliva, and cerebrospinal fluid, are recognized as critical components in intercellular communication by transporting biomolecules from the parental cells to the recipient cells.25,26 The biomolecules can not only represent the characteristics of the parental cells but also effectively alter the biological response of the recipient cells.27 According to their size, biogenesis, and function, EVs can be classified into three main categories: exosomes (less than 150nm in diameter), microvesicles (150–1000nm in diameter), and apoptotic bodies (more than 1000nm in diameter).28,29 All three subtypes share comparable structural and compositional profiles, including surface molecule expression and cellular cargo mirroring their parental origins. Complete isolation remains technically challenging; however, exosomes demonstrate superior therapeutic efficacy, exhibiting enhanced anti-inflammatory properties compared to other subtypes.30,31 Of these, the most widely studied is exosomes, whose biogenesis consists of four steps: initiation, endocytosis, multivesicular bodies (MVBs) formation, and secretion of exosomes13 (Figure 1). First, plasma membrane (PM) invagination forms early endosomes (EE), which gradually develop into late endosomes (LE).32 LE transforms into intracellular MVBs with intraluminal vesicles (ILVs) by budding inward.33 Subsequently, ILVs of MVBs are expelled from the cell through fusion with the PM or exocytosis after phagocytosis of various biomolecules and finally form exosomes.13,32,33 The lipid bilayer membrane comprising EVs contains surface proteins, tetraspanins (CD9, CD81, and CD63), and receptors, which regulate EVs’ biological distribution and targeting ability and are used for their characterization34,35 (Figure 1).
 |
Figure 1 Role of EVs in intra-nephron communication. The EVs secreted by the parental cells reach the kidneys, transporting the carried biomolecules to the recipient cells. In the left half of the image, the parent cell section shows the process of EV formation. In the middle of the picture, the EVs secreted by the parental cells can interact with all the cells of the kidney and the EVs they secrete, and together affect the progression of kidney disease. At the bottom of the middle section is a microscopic amplification of EVs. In the right part of the image, the receptor cell receives the biomolecules carried by the parental cell-derived EVs. Created in BioRender. Yan, Q. (2025) https://BioRender.com/l94g381. Abbreviations: ILVs, intraluminal vesicles; EE, early endosome; LE, late endosome; MVBs, multivesicular bodies. |
In addition to humoral-derived EVs that have been extensively studied, the underlying applications of mesenchymal stem cells-derived EVs (MSC-EVs) and engineered EVs in diseases have attracted tremendous attention because of their higher biocompatibility and lower toxicity recently36–38 (Figure 2). EVs secreted by certain types of cells have a therapeutic effect of their own since they carry various cargo molecules from parent cells such as MSC-EVs, while modified EVs are supposed to have an extra therapeutic function because they contain additional therapeutically efficient materials such as engineered EVs.39 A phospholipid bilayer structure modified with functional molecules allows the decoration of their initial framework by applying multiple approaches, including chemical procedures, direct parent cell membrane engineering, genetic engineering, and physical techniques.38 An enclosed parental matrix attracts interest in loading large amounts of siRNA, mRNA, or miRNA via lipofection, electroporation, calcium chloride treatment, or sonication.40 More and more proofs indicate that EVs as therapeutic approaches are ideal for personalized medicine because of their diversity and multifunctionality.41
 |
Figure 2 The extraction and characterization diagram of EVs. The three source EVs mentioned in the review must undergo a series of sequential processes to determine EVs, including the isolation and characterization of exosomes. Created in BioRender. Yan, Q. (2025) https://BioRender.com/g4unxkb. Abbreviations: dUC, differential ultracentrifugation; SEC, size exclusion chromatography; DG centrifugation, density gradient centrifugation; SEM, scanning electron microscopy; TEM, transmission electron microscopy; DLS, dynamic light scattering (DLS); NTA, nanoparticle tracking analysis; ELISA, enzyme-linked immunosorbent assay; WB, Western blot. |
Isolation and Identification of Extracellular Vesicles
Obtaining EVs from complex and varied components with a high yield and exosome-like characteristic is a challenge and critical point for further clinical applications, which is susceptible to isolation procedures.35 Unfortunately, there is no unified protocol or methodology for isolating and purifying EVs, as this step is determined by downstream analysis.35 Based on the diverse biological properties of EVs, such as shape, size, surface proteins, and density, numerous conventional approaches have been applied for isolating EVs, including precipitation, differential ultracentrifugation (dUC), density gradient centrifugation (DG centrifugation), immunoaffinity capture-based technology, size exclusion chromatography (SEC), ultrafiltration, and microfluidics-based technology42 (Figure 2). Although separation techniques are diverse and have advantages, each approach has limitations (Table 1). Ultracentrifugation is the gold standard and most commonly used method for separating electric vehicles, which can extract high-purity EVs but cannot further distinguish the diverse populations of EVs.15,43 SEC is reproducible, cost-efficient, and requires no particular laboratory equipment or user expertise, but it is time-consuming.42,44 In addition, precipitation can bring a high yield, but it also loses the specificity and purity of EVs to a large extent.45 On the contrary, immunoaffinity capture-based technology can ensure higher purity of EVs while reducing the yield.46 Optimizing purity may improve experimental specificity, and increasing EV yield is elementary to augment experimental sensitivity. Therefore, given the respective characteristics of the techniques, the researchers combined and optimized them to obtain high-purity and high-yield EVs.42 The complexity and diversity of EV isolation methods, inevitable non-EVs components, as well as the heterogeneity of EVs are enormous obstacles to identifying the isolated EVs.35,42,47 Traditionally, the identification of EVs involved three parts (Figure 2): characterizing cup-shaped morphology by scanning electron microscopy (SEM) and transmission electron microscopy (TEM), identifying size characterization using dynamic light scattering (DLS) and nanoparticle tracking analysis (NTA), and recognizing EVs proteins by enzyme-linked immunosorbent assay (Elisa) and Western blot (WB).42,47,48 The ISEV recommends using transmembrane or GPI-anchored proteins to identify EVs. The purity of EVs can be determined by exploring the existence or absence of non-EVs proteins.42,49
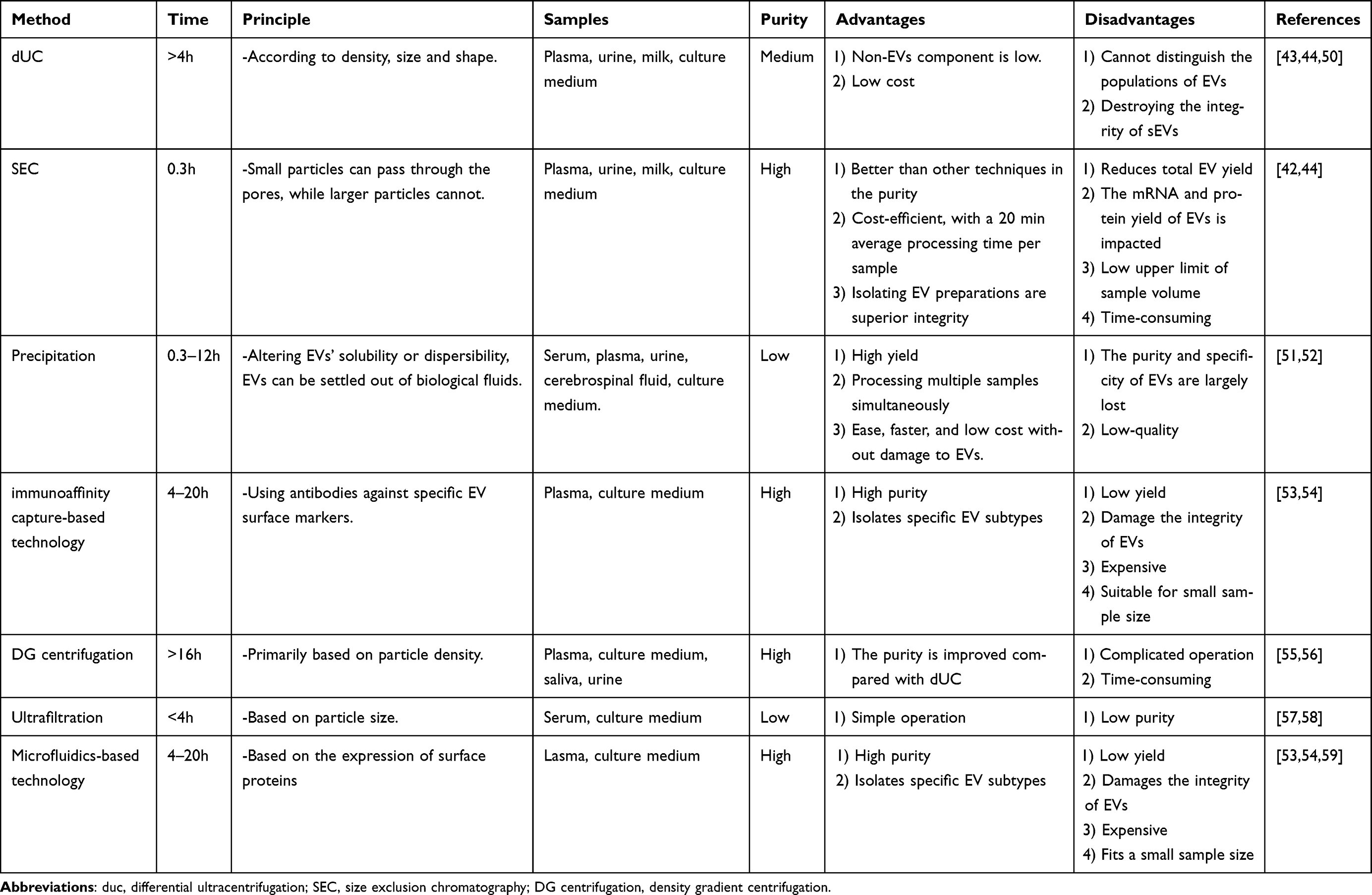 |
Table 1 Comparison of the EV Isolation Methods |
Role of EVs in Intra-Nephron Communication
EVs function in multiple biological processes and play a pathophysiological role in kidney diseases, including immune/inflammatory regulation, antibacterial effect, and kidney regeneration/repair.60 Cellular communication between numerous nephron cells can be mediated by EVs, which amplify kidney damage61 (Figure 1). When stimulated by harmful factors, EVs derived from glomerular endothelial cells transfer miRNA to podocytes to impair podocyte function, while podocyte-derived EVs lead to renal TECs injury.62,63 Under high glucose conditions, mesangial cell-derived EVs damaged podocytes, and the interaction of EVs secreted by the two types of cells affected glomerular function.64 In addition, EVs originating from upper segments of tubular cells deliver biomolecules to downstream cells and regulate their behavior, which are internalized by downstream cells.61,65 For example, renal proximal epithelial cells-derived EVs can go downstream through the urinary tract, arriving at distal tubules or collecting ducts.66 Gidea et al found that distal tubule and collecting duct immortalized cell lines can ingest CD63-EGFP or CD9-RFP labeled EVs from human renal proximal tubule cells.65 Furthermore, similar communication was found between renal tubule cells and interstitial cells. Proteinuria stimulates TECs to produce more EVs, in which loaded mRNA is transferred to macrophages and promotes their activation and migration, resulting in renal tubulointerstitial inflammation.64
Urinary extracellular vesicles (uEVs) mainly originate from urogenital tract cells, including glomerular, tubular, prostate cells, and bladder cells, and can mediate communication between glomerular and tubular cells and between different segments of renal tubules.61,67 Lv et al isolated EVs released by podocytes from urine, whose structure was positive for the markers of podocyte.68 Podocyte-derived EVs in urine may pass through the renal tubules to deliver the information to the TECs.69 uEVs are promising biomarkers for reflecting renal tissue injury and predicting renal function progression.
EVs in AKI
EVs play a role in intercellular and interorgan crosstalk, potentially amplifying kidney damage and contributing to the progression of kidney disease61 (Figure 1). Based on EV-related studies, novel biomarkers and disease mechanisms have been identified in many kidney diseases, including AKI.70 In addition, EVs are used not only as information molecules to report disease characteristics and progression but also to deliver therapeutic molecules to specific target cells to improve the progression of AKI.71 We will focus on the role of EVs in the diagnosis, treatment, and mechanism of AKI caused by various etiologies (Table 2) (Figure 3).
 |
Table 2 Application of EVs in AKI |
 |
Figure 3 The mechanism of EVs in AKI. IRI-AKI: After using AIEgens to treat MSC-EVs, MSC-EVs-transferred miRNA-200a-p activated the Keap1-Nrf2 signaling pathway in TECs, thereby restoring renal function in IRI-AKI mice. S-AKI: FRC-EVs were modified with LTH-targeting peptides to navigate EVs to tubule cells, and CD5L in EVs was released into tubule cells to promote mitophagy, inhibit pyroptosis, and thus improve kidney injury. CDDP-AKI: The crosstalk between macrophages and TECs promotes disease progression in a CDDP-AKI mouse model, and autophagy-deficient macrophage (Atg7Δmye mice derived macrophage)-derived EVs damage the mitochondria of TECs in vitro, which possibly through the miR-195a-5p-SIRT3 axis. Created in BioRender. Yan, Q. (2025) https://BioRender.com/x59y496. Abbreviations: Atg7Δmye, macrophages -specific depletion of ATG7; Glycerol-induced AKI, uEVs promote kidney regeneration by transferring the renal protective factor Klotho to damaged kidney tissue. AIEgens, accumulation-induced emission luminous; TECs, tubular epithelial cells; FRC-EVs, Fibroblastic reticular cells-derived EVs. |
Ischemia/Reperfusion Injury-Related AKI
Ischemic/reperfusion injury (IRI), one of the primary causes of AKI, leads to significant morbidity and mortality.88 With a complex pathogenesis, IRI-related AKI (IRI-AKI) still has few effective interventions or management.72,89 MSC-EVs may hold great promise for treating IRI, not just IRI-AKI, and many animal model experiments have shown their therapeutic potential.72,90,91 Cao et al used a noninvasive technique, accumulation-induced emission luminous (AIEgens), to demonstrate that MSC-EVs-transferred miRNA-200a-p activated the Keap1-Nrf2 signaling pathway in TECs, thereby restoring renal function in IRI-AKI mice (Figure 3).72 MSCs derived from multiple tissues, including the placenta, adipose tissue, bone marrow, and the umbilical cord, have beneficial anti-inflammatory and antifibrotic effects, and the EVs released from them are regarded as valuable cell-free therapies for treating renal IRI.92,93 All four sources mentioned above of MSC-EVs have been studied in IRI, and the results show that they have a therapeutic effect on IRI by alleviating renal fibrosis, reducing inflammatory cell infiltration, restoring renal structure, inhibiting renal cell apoptosis, and promoting vascular regeneration.48,94 For example, the human Wharton’s jelly (hWJMSCs), a gel-like substance found in the umbilical cord, secreted EVs have renoprotective effects, such as improvement in renal function, cell proliferation, cell survival, and tissue fibrosis inhibition in renal IRI, a process that is induced by mitigating oxidative stress (OS).73,92 In addition to MSC-EVs, EVs from healthy renal tubular cells can protect renal function as well. Renal endothelial and tubular-derived EVs are essential in IRI recovering and healing.95 By intravenous administration of EVs derived from renal tubule cells, renal IRI was alleviated in rats, and the antioxidant capacity of the injured cells was enhanced.22
The development of IRI-AKI involves various mechanisms, including cell injury, cell dysfunction, and multiple cell death, among which tubular cell necrosis and apoptosis are considered to be the main causes of IRI-AKI in previous studies.89 EVs released from the apical and basolateral membranes of renal TECs can be isolated from plasma as a non-invasive biomarker monitoring AKI.96 Damage-associated molecular patterns may transmit to renal TECs via EVs, hindering renal tubule recovery.48 Moreover, once the immune response begins and IRI enters an initial inflammatory stage, renal tubular-derived EVs carrying biomolecules may activate and recruit innate immune cells, which promote the apoptosis of TECs and the damage of endothelial cells.48,97 Similarly, endothelial cells-derived EVs have pro-inflammatory functions, which can exacerbate vascular inflammation by attracting adaptive immune cells and inducing the production of autoantibodies.48,91–93,98 Biological factors delivered by endothelial progenitor cells (EPC-EVs) or MSC-EVs regulate inflammatory profiles and facilitate the repair of TECs and endothelial cells.97 Plasma, serum, and platelet-derived EVs have been extensively studied as biomarkers or therapeutics for myocardial IRI.99–101 Unfortunately, we did not find these sources of EVs in renal IRI research. Given the protective effect of these EVs on myocardial IRI, do they have a palliative effect on renal IRI to treat IRI-AKI? It is hoped that future studies will answer this question.
Sepsis-Associated AKI
Sepsis, one of the major causes of death after trauma, burns, and severe surgery, is closely related to ~50% of AKI patients.102 At present, researchers are still exploring the pathophysiological mechanism of sepsis-associated AKI (S-AKI), so organ support and etiological treatment, such as antibiotics and resuscitation, are the primary options for its treatment.102,103 Similar to IRI-AKI, MSC-EVs also have a therapeutic efficacy in S-AKI. The specific mechanisms involved in the treatment of AKI from different sources of MSC-EVs are diverse. For example, adipose tissue MSCs-derived EVs (AMSCs-EVs) activate the Sirt1, human umbilical cord MSCs-derived EVs (hucMSCs-EVs) attenuate NF-kB activity, and bone MSCs-derived EVs (BMSCs-EVs) block autophagy by the AMPK/mTOR pathway, the final result is the alleviation of S-AKI.104–106 Fibroblastic reticular cell-derived EVs (FRC-EVs), promising drug-delivery vehicles, can promote mitochondrial autophagy, restrict inflammasome activation, and accelerate the recovery of renal TECs to treat S-AKI.74 FRC-EVs were modified with LTH-targeting peptides to navigate EVs to tubule cells, and CD5L in EVs was released into tubule cells to promote mitophagy, inhibit pyroptosis, and thus improve kidney injury (Figure 3).74 Notably, approximately 70% of total plasma EVs in sepsis patients are derived from platelets, regarded as the major functional components of plasma EVs.75 However, these platelet-derived EVs promote inflammation, apoptosis, and OS, possibly exacerbating S-AKI by activating the ERK/Smad3/P53 pathway.75 S-AKI is also aggravated by macrophage-derived EVs, which have been shown to cause endothelial cell dysfunction and promote inflammation in vivo and in vitro.76
Serum creatinine and urine volume have limitations in the diagnosis of AKI.103,107 In particular, sepsis reduces muscle perfusion, slowing the increase of serum creatinine concentration and ultimately preventing early diagnosis.108 Although new biomarkers have been detected recently to diagnose S-AKI, they are low sensitivity.102,109 Consequently, there is an urgent need for non-invasive biomarkers with both sensitivity and specificity. uEVs, a non-invasive diagnostic modality, can reflect the molecular events of physiological and pathological changes in urinary diseases.110 So, uEVs activating transcriptional factor 3 (uATF3) may be an early indicator of S-AKI.111 Li et al used integrative multi-omics analysis to describe the molecular dynamics landscape of serum-derived EVs during sepsis for the first time, ultimately finding 354 differentially expressed proteins and 332 differentially expressed RNAs in serum EVs of sepsis patients.112 These differentially expressed molecules may provide valuable insights for diagnosing and treating S-AKI.
Drug-Induced AKI
Drug-induced kidney injury, a considerable pathogenic factor of AKI, has a clinical incidence of AKI as high as 60%.113 Drug-induced AKI is clinically manifested in various forms, the popular of which is tubular interstitial compartment injury.114 Among the drugs that can induce the AKI model, cisplatin and glycerol are commonly used.
Cisplatin-Induced AKI
Cisplatin (CDDP) is a chemotherapy drug widely used in the treatment of solid tumors, with the incidence of side effects of AKI achieving 30%.115,116 At present, the prevention of CDDP-induced AKI (CDDP-AKI) mainly includes diuretic hydration therapy and dose reduction or withdrawal of cisplatin.116,117 However, these measures cannot apply to patients with renal or cardiac dysfunction and hinder the treatment of tumors.116,117 Therefore, it is urgent to discover effective measures to prevent or treat CDDP-AKI. Kim et al found that a pan-peroxisome proliferator-activated receptor (PPAR) agonist can enhance the protective effect of induced mesenchymal stem cells derived EVs (iMSC-EVs) on kidney in CDDP-AKI mice.77 Beyond reagents, the researchers also explored physical methods such as pulsed focused ultrasound (pFUS) processing of tissue to increase the therapeutic effect of MSCs-EVs on CDDP-AKI.78 The possible reason is that pFUS enhances MSCs homing to save renal function safely and effectively.118 Ullah et al carried out a similar study. However, they denied the improved effect of pFUS on EVs homing to the kidney, suggesting that the better treatment outcome of this synergistic therapy was due to the up-regulation of the regenerative pathway (Sirt3, eNOS).78 Apoptosis and necrotic apoptosis of proximal TECs are deemed to be the principal pathologic forms of CDDP-AKI.115,119 The therapeutic effect of hucMSCs-EVs on CDDP-AKI has been extensively studied, which involves several mechanisms, including reducing serum inflammatory cytokines, inhibiting TECs’ mitochondrial apoptosis, and activating TECs’ autophagy.79 A recent study found that the crosstalk between macrophages and TECs promotes disease progression in the CDDP-AKI mouse model, and autophagy-deficient macrophage-derived EVs damage the mitochondria of TECs in vitro, which possibly through the miR-195a-5p-Sirt3 axis (Figure 3).80 EVs’ role in the CDDP-AKI progression mechanism has not been fully elucidated, and relevant studies are limited. We call for more research to understand the pathophysiological mechanisms of CDDP-AKI in more detail.
Glycerol-Induced AKI
Myolysis and hemolysis can occur after intramuscular injection of glycerol, which exposes the kidneys to a mass of myoglobin and hemoglobin, resulting in ischemic tubular injury.81,120 Fifteen years ago, a mouse model of glycerin-induced AKI was used to demonstrate that EVs derived from human BMSCs stimulated the proliferation of TECs and accelerated the recovery of AKI.81 This process may be related to paracrine factors facilitating the proliferation of surviving intrinsic epithelial cells.81 Five years later, Maria conducted a similar experiment, reaffirming stem cells’ therapeutic effect on glycerol-induced AKI and paracrine mechanisms (associated with the renal regenerative effect).120,121 Due to miRNA’s pro-regeneration ability on the kidney, electroporation transiently transfected the specific miRNA into MSCs to obtain engineered EVs, which not only retained their pro-regeneration effect but also prominently improved renal function and morphology in glycerol-induced AKI mice.122 In consideration of the ethical issues, invasive sample collection, and limited donors of MSCs therapy, Zhang et al made the first attempt and succeeded in isolating a type of adult stem cell with excellent proliferation potential and multidirectional differentiation ability from urine for the first time, called urine-derived stem cells (USCs).123 With Zhang’s help, Li et al demonstrated that injecting USCs intravenously into glycerin-induced AKI mice promotes TECs proliferation.124 Do uEVs have a therapeutic function on glycerin-induced AKI? Grange et al showed that uEVs promote kidney regeneration by transferring specific miRNA cargo to damaged kidney tissue and regulating the renal protective factor Klotho.82 The therapeutic effect of uEVs and MSCs-EVs on kidneys is similar, demonstrating their great potential in the future treatment of AKI.
Other drugs that can cause AKI contain antibiotics (gentamicin), contrast agents, and so on.114 Gentamicin, the most commonly used aminoglycoside drug, can cause kidney damage, which is mainly manifested as proximal tubular necrosis and glomerular hemodynamic changes.83 Studies have shown that BMSCs mediate the recovery of kidney function in gentamicin-induced AKI mice through RNA carried in EVs.83 Contrast-induced AKI is the third major cause of hospital-acquired AKI, whose exact pathogenesis remains unclear, and available treatments are minimal.125 Unfortunately, we did not find any studies of contrast-induced AKI and EVs. Given the therapeutic effect of EVs on other types of AKI and the limited treatment options for contrast-induced AKI, initiating relevant research in this area may bring significant benefits. It is worth noting that renal injury caused by intramuscular injection of glycerol belongs to the rhabdomyolysis-induced AKI model. Rhabdomyolysis can be caused by a variety of causes, including trauma, burns, high fever, strenuous exercise, and the previously mentioned drugs (glycerin), causing rhabdomyolysis and disintegration, with AKI occurring in approximately 40% of patients.126,127 Next, we will introduce the role of EVs in burn and trauma-induced AKI.
Burns/Trauma-Induced AKI
Patients with severe burns and tissue trauma are at risk for AKI due to hypotension, fluid loss, intensive immune-pathophysiological responses, and rhabdomyolysis.128–130 After severe injury, about a quarter of patients are forcefully affected by trauma to develop AKI, resulting in them being at high risk of adverse outcomes.131 In particular, up to 58% of people with severe burns experience AKI, which is strongly related to 90-day mortality.130,132 Despite the most conventional treatment for burn-related AKI is renal replacement therapy (RRT), MSCs therapy may be more appropriate for some specific burn patients due to its comprehensive therapeutic capabilities.132–134 However, with significant progress, the clinical use of MSCs still needs to be improved due to several obstacles, including thrombosis, low survival in vivo, and tumorigenesis.135,136 MSCs-EVs, a novel approach for treating kidney disease, can overcome the limitations of MSCs while reserving the therapeutic characteristics of MSCs and may have great potential for burns- or trauma-induced AKI treatment.77,135 Regrettably, research on the function of MSC-derived EVs in burns-induced AKI is limited. More research in this area could be done in the future to benefit patients.
Post-Transplant AKI
Kidney transplantation (KT), the preferred treatment for end-stage kidney disease (ESRD), is associated with renal ischemia and exposure to toxins, which can lead to AKI.137,138 Existing injury indicators such as creatinine, which has a long half-life and is widely distributed, make it impossible to measure kidney function and injury in real time accurately.137,139 So, the researchers recommended uEVs as new biomarkers of renal function after KT.140 The molecular components of uEVs can represent the pathophysiological state of the urinary system.84 For instance, neutrophil gelatinase-associated lipocalin (NGAL) carried in uEVs was a better candidate for monitoring renal dysfunction after KT than other components in urine.84 However, Peake et al suggested that the mRNA of kidney injury biomarkers in uEVs did not reflect or predict urinary biomarker levels after KT.137 In addition, hWJMSCs-EVs improve survival rate and renal function after KT by reducing renal cell apoptosis and inflammation and promoting proliferation.85 EVs have greatly interested researchers as a noninvasive way to diagnose or treat kidney diseases. If biomolecules in uEVs can predict or treat post-transplant AKI, KT’s success probability will significantly increase.
AKI Induced by Other Methods
Many other factors can cause AKI, such as cardiac surgery, unilateral ureteral obstruction (UUO), and scrub typhus-associated AKI. The research found that monitoring alters in EV levels in urine can forecast the onset of AKI in patients after cardiac surgery.86 BMSCs-EVs containing milk fat globule-epidermal growth factor-factor 8 (MFG-E8) improved kidney damage in UUO mice by inhibiting the RhoA/ROCK pathway.87 Not only is miRNA-21 in urine a biomarker of AKI, but Yun et al also demonstrated that the level of miRNA-21 in uEVs has diagnostic significance for AKI in patients with scrub typhus.84 The study of EVs and AKI caused by other factors needs to be more comprehensive. At the same time, studies on clarifying the relationship between EVs and AKI caused by these etiologies are insufficient, indicating a vast exploration space to fill the research gap in this area.
As a common refractory disease, the selection of multiple modeling methods for AKI should be based on the characteristics and objectives of the study, combining the advantages and feasibility of different models to make the research results credible. Coincidentally, most of the AKI studies involving EVs we collected focused on the role of MSCs-EVs. Moreover, most studies on MSCs-EVs focus on their therapeutic function in AKI. Due to the effects of reducing oxidative stress, anti-fibrosis, inducing renal tissue regeneration, and inhibiting renal cell apoptosis and inflammation, MSCs-EVs can be the next generation of cell-free therapies for AKI. Although MSCs-EVs are effective in treating AKI, these experimental conclusions are mainly derived from animal experiments, and the application of MSCs-EVs to humans is uncertain. It is worth noting that renal TECs injury is the central link causing AKI, but the number of studies of TECs-EVs in AKI has been unsatisfactory. Focusing on the potential role of TECs-EVs in the pathogenesis of AKI will greatly benefit the treatment of AKI. In addition, uEVs not only contain EVs secreted by all renal cells but also promote nephron cross-talk between the glomerular and renal tubular regions.141 Therefore, we have reason to believe that uEVs will have great value in the study of AKI in the future.
Challenges and Prospects of EVs in Clinical AKI Treatment
Although various experiments have shown the tremendous potential role of EVs in AKI, there are still many obstacles to their clinical application (Figure 4). First, the best way to deliver EVs into the body is still being determined. Most of the above animal experiments used intravenous (IV) injection to deliver EVs through the blood circulation to the kidney (Table 1). However, this method allows EVs to be retained by the upstream organ; thus, the uptake of EVs by the kidney is low.7 Intrarenal arterial (IA) injection can better increase the uptake of EVs to the kidney and transport therapeutic EVs directly to the injured kidney.142 In addition, IA injection can minimize systemic side effects and maximize the therapeutic efficacy, but it is an invasive procedure that may pose specific safety concerns.7,142 We only found one clinical trial in which MSCs-EVs were injected into the human internal renal artery. Although the results showed significant improvements in kidney function, more research is needed to demonstrate the safety of MSCs-EVs in clinical use.143 In the case of systemic repeated administration, it is necessary to be vigilant about the immunogenicity of EVs.7 In addition, the dose of EVs applied to the human body at each time, the best time to inject EVs, the clearance in the body, and whether it can be combined with other treatments are uncertain.7 Clinicians need to understand better the pharmacokinetics, pharmacodynamics, and biological distribution of every type of EV in the human body to determine the optimal dose and route of administration for each type of AKI.144 The source, extraction and pretreatment methods, culture and induction conditions of EVs all change their properties and functions, and may affect the therapeutic effect of AKI.145 Therefore, modifying EVs according to the different causes of AKI before the targeted treatment is wise.
 |
Figure 4 EVs from laboratory investigation to clinical application. The clinical application of EVs faces many challenges, but there have been studies on clinical patients. We believe that the clinical application of EVs in AKI can be realized in the near future. Created in BioRender. Yan, Q. (2025) https://BioRender.com/u72t307. |
There is no clinical precedent for using EVs to treat AKI, but the treatment of Alzheimer’s disease, sepsis, refractory macular holes, and coronavirus disease 2019 (COVID-19) has entered early clinical trials using EVs.145–147 Based on the examples presented above, circulating system and urine-derived EVs may serve as potential early biomarkers of AKI, while MSCs-EVs and engineered EVs have feasibility as therapeutic tools, especially engineered EVs can be used as the specific treatment. Additionally, the difficulties in isolation and purification of EVs need to be overcome before realizing the clinical application of EVs in treating AKI. A simple and safe method for EV extraction should be developed to achieve both high-yield and high-purity EVs to meet clinical needs.148 Finally, reliable criteria for evaluating the efficacy of EV therapies need to be established. Accurately evaluate the effect of EVs on AKI to determine the next course of treatment and avoid inconsistencies between preclinical studies and clinical applications. In any case, EVs hold promising prospects in the clinical application of AKI, whether as a treatment or a diagnostic method.
Conclusion
EVs hold considerable promise as a diagnostic or treatment tool for AKI. However, many challenges still need to be overcome before clinical applications are realized, such as establishing standard EV separation and purification procedures, determining the optimal dose, treatment timing, and infusion mode of EVs for use in humans, and confirming reliable criteria for evaluating the efficacy of EVs treatment. Future research is required to conduct additional clinical trials after determining EVs’ safety and resolving other hindrances. This paper summarizes the potential application of EVs in various etiologies leading to AKI in recent years, emphasizing the excellent therapeutic value of MSCs-EVs. We are the first to summarize the application value of EVs in AKI caused by various etiologies, emphatically introducing IRI-AKI, S-AKI, and drug-induced AKI. Unfortunately, most studies focus on the therapeutic effect of MSCs-EVs on AKI, and few studies are exploring the functions of other sources of EVs in AKI.
In addition, the types of AKI we collected need to be more comprehensive. For some causes of AKI, such as contrast-induced AKI and burns/trauma-induced AKI, we do not find any studies related to EVs, although they are also common causes of AKI clinically. Overall, this paper emphasizes EVs’ promising therapeutic and diagnostic potential as a clinical tool for AKI and underscores the need for further research in this domain. The clinical application of EVs is hoped to be realized soon, and the research based on EVs can find better diagnostic markers and provide the perfect treatment for AKI.
Author Contributions
We declare that all authors made substantial contributions to the study. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the National Natural Science Foundation of China to Bo Wang (No. 82300840), a grant from the Natural Science Foundation of Sichuan Province to Bo Wang (No. 2024NSFSC1503). The figures were created with a free version of Biorender.com under agreement number TM289Q0T6R, DX289Q8HTY, FH289Q3KRK and UV289Q1850.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ronco C, Bellomo R, Kellum JA. Acute kidney injury. Lancet. 2019;394(10212):1949–1964. doi:10.1016/S0140-6736(19)32563-2
2. Mehta RL, Cerdá J, Burdmann EA, et al. International society of nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): a human rights case for nephrology. Lancet. 2015;385(9987):2616–2643. doi:10.1016/S0140-6736(15)60126-X
3. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625. doi:10.1038/s41581-018-0052-0
4. KDIGO Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(1):1. doi:10.1038/kisup.2012.1
5. Huang W, Wang BO, Hou YF, et al. JAML promotes acute kidney injury mainly through a macrophage-dependent mechanism. JCI Insight. 2022;7(14):e158571. doi:10.1172/jci.insight.158571
6. Guo C, Dong G, Liang X, Dong Z. Epigenetic regulation in AKI and kidney repair: mechanisms and therapeutic implications. Nat Rev Nephrol. 2019;15(4):220–239. doi:10.1038/s41581-018-0103-6
7. Lundy DJ, Szomolay B, Liao CT. Systems approaches to cell culture-derived extracellular vesicles for acute kidney injury therapy: prospects and challenges. Function. 2024;5(3):zqae012. doi:10.1093/function/zqae012
8. Wen Y, Yan HR, Wang B, Liu BC. Macrophage heterogeneity in kidney injury and fibrosis. Front Immunol. 2021;12:681748. doi:10.3389/fimmu.2021.681748
9. Liu BC, Tang TT, Lv LL, Lan HY. Renal tubule injury: a driving force toward chronic kidney disease. Kidney Int. 2018;93(3):568–579. doi:10.1016/j.kint.2017.09.033
10. Araldi E, Krämer-Albers EM, Hoen EN, et al. International society for extracellular vesicles: first annual meeting, April 17-21, 2012: ISEV-2012. J Extracell Vesicles. 2012;1:19995. doi:10.3402/jev.v1i0.19995
11. Colombo M, Raposo G, Théry C. Biogenesis, secretion, and intercellular interactions of exosomes and other extracellular vesicles. Annu Rev Cell Dev Biol. 2014;30:255–289. doi:10.1146/annurev-cellbio-101512-122326
12. Kurzhagen JT, Dellepiane S, Cantaluppi V, Rabb H. AKI: an increasingly recognized risk factor for CKD development and progression. J Nephrol. 2020;33(6):1171–1187. doi:10.1007/s40620-020-00793-2
13. Rajput A, Varshney A, Bajaj R, Pokharkar V. Exosomes as new generation vehicles for drug delivery: biomedical applications and future perspectives. Molecules. 2022;27(21):7289. doi:10.3390/molecules27217289
14. Ceccotti E, Saccu G, Herrera Sanchez MB, Bruno S. Naïve or engineered extracellular vesicles from different cell sources: therapeutic tools for kidney diseases. Pharmaceutics. 2023;15(6):1715. doi:10.3390/pharmaceutics15061715
15. Xiang H, Zhang C, Xiong J. Emerging role of extracellular vesicles in kidney diseases. Front Pharmacol. 2022;13:985030. doi:10.3389/fphar.2022.985030
16. Madhu LN, Kodali M, Upadhya R, et al. Extracellular vesicles from human-induced pluripotent stem cell-derived neural stem cells alleviate proinflammatory cascades within disease-associated microglia in Alzheimer’s disease. J Extracell Vesicles. 2024;13(11):e12519. doi:10.1002/jev2.12519
17. Zhang C, Shao W, Yuan H, et al. Engineered extracellular vesicle-based nanoformulations that coordinate neuroinflammation and immune homeostasis, enhancing Parkinson’s disease therapy. ACS Nano. 2024;18(34):23014–23031. doi:10.1021/acsnano.4c04674
18. Casanova-Salas I, Aguilar D, Cordoba-Terreros S, et al. Circulating tumor extracellular vesicles to monitor metastatic prostate cancer genomics and transcriptomic evolution. Cancer Cell. 2024;42(7):1301–1312.e7. doi:10.1016/j.ccell.2024.06.003
19. Lu W, Li X, Wang Z, et al. Mesenchymal stem cell-derived extracellular vesicles accelerate diabetic wound healing by inhibiting NET-induced ferroptosis of endothelial cells. Int J Biol Sci. 2024;20(9):3515–3529. doi:10.7150/ijbs.97150
20. Zi SF, Wu XJ, Tang Y, et al. Endothelial cell-derived extracellular vesicles promote aberrant neutrophil trafficking and subsequent remote lung injury. Adv Sci. 2024;11(38):e2400647. doi:10.1002/advs.202400647
21. miRNA signature of urine extracellular vesicles shows the involvement of inflammatory and apoptotic processes in diabetic chronic kidney disease - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/36859746/.
22. Dominguez JM, Dominguez JH, Xie D, Kelly KJ. Human extracellular microvesicles from renal tubules reverse kidney ischemia-reperfusion injury in rats. PLoS One. 2018;13(8):e0202550. doi:10.1371/journal.pone.0202550
23. MicroRNAs in extracellular vesicles protect kidney from ischemic injury: from endothelial to tubular epithelial - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/27884305/.
24. Microvesicles derived from mesenchymal stem cells enhance survival in a lethal model of acute kidney injury - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/22431999/.
25. Berumen Sánchez G, Bunn KE, Pua HH, Rafat M. Extracellular vesicles: mediators of intercellular communication in tissue injury and disease. Cell Commun Signal. 2021;19(1):104. doi:10.1186/s12964-021-00787-y
26. Zhu Z, Hu E, Shen H, Tan J, Zeng S. The functional and clinical roles of liquid biopsy in patient-derived models. J Hematol Oncol. 2023;16(1):36. doi:10.1186/s13045-023-01433-5
27. Wang C, Li Z, Liu Y, Yuan L. Exosomes in atherosclerosis: performers, bystanders, biomarkers, and therapeutic targets. Theranostics. 2021;11(8):3996–4010. doi:10.7150/thno.56035
28. Meng W, He C, Hao Y, Wang L, Li L, Zhu G. Prospects and challenges of extracellular vesicle-based drug delivery system: considering cell source. Drug Deliv. 2020;27(1):585–598. doi:10.1080/10717544.2020.1748758
29. Zhao J, Zhu W, Mao Y, et al. Unignored intracellular journey and biomedical applications of extracellular vesicles. Adv Drug Deliv Rev. 2024;212:115388. doi:10.1016/j.addr.2024.115388
30. Liu S, Wu X, Chandra S, et al. Extracellular vesicles: emerging tools as therapeutic agent carriers. Acta Pharm Sin B. 2022;12(10):3822–3842. doi:10.1016/j.apsb.2022.05.002
31. Wu T, Wang L, Gao C, et al. Treg-derived extracellular vesicles: roles in diseases and theranostics. Mol Pharm. 2024;21(6):2659–2672. doi:10.1021/acs.molpharmaceut.4c00233
32. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):eaau6977. doi:10.1126/science.aau6977
33. Sinha D, Roy S, Saha P, Chatterjee N, Bishayee A. Trends in research on exosomes in cancer progression and anticancer therapy. Cancers. 2021;13(2):326. doi:10.3390/cancers13020326
34. Ergunay T, Collino F, Bianchi G, Sedrakyan S, Perin L, Bussolati B. Extracellular vesicles in kidney development and pediatric kidney diseases. Pediatr Nephrol. 2024;39(7):1967–1975. doi:10.1007/s00467-023-06165-9
35. Exploring the role of urinary extracellular vesicles in kidney physiology, aging, and disease progression - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/37842748/.
36. Fang Z, Liu K. Plant-derived extracellular vesicles as oral drug delivery carriers. J Control Release. 2022;350:389–400. doi:10.1016/j.jconrel.2022.08.046
37. Birtwistle L, Chen XM, Pollock C. Mesenchymal stem cell-derived extracellular vesicles to the rescue of renal injury. Int J Mol Sci. 2021;22(12):6596. doi:10.3390/ijms22126596
38. Yao Y, Jiang Y, Song J, et al. Exosomes as potential functional nanomaterials for tissue engineering. Adv Healthc Mater. 2023;12(16):e2201989. doi:10.1002/adhm.202201989
39. Heo J, Kang H. Exosome-based treatment for atherosclerosis. Int J Mol Sci. 2022;23(2):1002. doi:10.3390/ijms23021002
40. Stranford DM, Simons LM, Berman KE, et al. Genetically encoding multiple functionalities into extracellular vesicles for the targeted delivery of biologics to T cells. Nat Biomed Eng. 2024;8(4):397–414. doi:10.1038/s41551-023-01142-x
41. Li SP, Lin ZX, Jiang XY, Yu XY. Exosomal cargo-loading and synthetic exosome-mimics as potential therapeutic tools. Acta Pharmacol Sin. 2018;39(4):542–551. doi:10.1038/aps.2017.178
42. Omrani M, Beyrampour-Basmenj H, Jahanban-Esfahlan R, et al. Global trend in exosome isolation and application: an update concept in management of diseases. Mol Cell Biochem. 2024;479(3):679–691. doi:10.1007/s11010-023-04756-6
43. Zou Z, Li H, Xu G, Hu Y, Zhang W, Tian K. Current knowledge and future perspectives of exosomes as nanocarriers in diagnosis and treatment of diseases. Int J Nanomedicine. 2023;18:4751–4778. doi:10.2147/IJN.S417422
44. Sidhom K, Obi PO, Saleem A. A review of exosomal isolation methods: is size exclusion chromatography the best option? Int J Mol Sci. 2020;21(18):6466. doi:10.3390/ijms21186466
45. Liangsupree T, Multia E, Riekkola ML. Modern isolation and separation techniques for extracellular vesicles. J Chromatogr A. 2021;1636:461773. doi:10.1016/j.chroma.2020.461773
46. Contreras-Naranjo JC, Wu HJ, Ugaz VM. Microfluidics for exosome isolation and analysis: enabling liquid biopsy for personalized medicine. Lab Chip. 2017;17(21):3558–3577. doi:10.1039/c7lc00592j
47. Théry C, Witwer KW, Aikawa E, et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the international society for extracellular vesicles and update of the MISEV2014 guidelines. J Extracell Vesicles. 2018;7(1):1535750. doi:10.1080/20013078.2018.1535750
48. Zhao X, Li Y, Wu S, et al. Role of extracellular vesicles in pathogenesis and therapy of renal ischemia-reperfusion injury. Biomed Pharmacother. 2023;165:115229. doi:10.1016/j.biopha.2023.115229
49. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13(2):e12404. doi:10.1002/jev2.12404
50. Jia Y, Yu L, Ma T, et al. Small extracellular vesicles isolation and separation: current techniques, pending questions and clinical applications. Theranostics. 2022;12(15):6548–6575. doi:10.7150/thno.74305
51. Li P, Kaslan M, Lee SH, Yao J, Gao Z. Progress in exosome isolation techniques. Theranostics. 2017;7(3):789–804. doi:10.7150/thno.18133
52. Weng Y, Sui Z, Shan Y, et al. Effective isolation of exosomes with polyethylene glycol from cell culture supernatant for in-depth proteome profiling. Analyst. 2016;141(15):4640–4646. doi:10.1039/c6an00892e
53. Koliha N, Wiencek Y, Heider U, et al. A novel multiplex bead-based platform highlights the diversity of extracellular vesicles. J Extracell Vesicles. 2016;5:29975. doi:10.3402/jev.v5.29975
54. Reiner AT, Witwer KW, van Balkom BWM, et al. Concise review: developing best-practice models for the therapeutic use of extracellular vesicles. Stem Cells Transl Med. 2017;6(8):1730–1739. doi:10.1002/sctm.17-0055
55. Gupta S, Rawat S, Arora V, et al. An improvised one-step sucrose cushion ultracentrifugation method for exosome isolation from culture supernatants of mesenchymal stem cells. Stem Cell Res Ther. 2018;9(1):180. doi:10.1186/s13287-018-0923-0
56. Zhu L, Sun HT, Wang S, et al. Isolation and characterization of exosomes for cancer research. J Hematol Oncol. 2020;13(1):152. doi:10.1186/s13045-020-00987-y
57. Xu X, Barreiro K, Musante L, et al. Management of Tamm-Horsfall protein for reliable urinary analytics. Proteomics Clin Appl. 2019;13(6):e1900018. doi:10.1002/prca.201900018
58. Shu SL, Yang Y, Allen CL, et al. Purity and yield of melanoma exosomes are dependent on isolation method. J Extracell Vesicles. 2020;9(1):1692401. doi:10.1080/20013078.2019.1692401
59. Dash M, Palaniyandi K, Ramalingam S, Sahabudeen S, Raja NS. Exosomes isolated from two different cell lines using three different isolation techniques show variation in physical and molecular characteristics. Biochim Biophys Acta Biomembr. 2021;1863(2):183490. doi:10.1016/j.bbamem.2020.183490
60. Lee SA, Choi C, Yoo TH. Extracellular vesicles in kidneys and their clinical potential in renal diseases. Kidney Res Clin Pract. 2021;40(2):194–207. doi:10.23876/j.krcp.20.209
61. Grange C, Bussolati B. Extracellular vesicles in kidney disease. Nat Rev Nephrol. 2022;18(8):499–513. doi:10.1038/s41581-022-00586-9
62. Jeon JS, Kim E, Bae YU, et al. microRNA in extracellular vesicles released by damaged podocytes promote apoptosis of renal tubular epithelial cells. Cells. 2020;9(6):1409. doi:10.3390/cells9061409
63. Hill N, Michell DL, Ramirez-Solano M, et al. Glomerular endothelial derived vesicles mediate podocyte dysfunction: a potential role for miRNA. PLoS One. 2020;15(3):e0224852. doi:10.1371/journal.pone.0224852
64. Lv LL, Feng Y, Wen Y, et al. Exosomal CCL2 from tubular epithelial cells is critical for albumin-induced tubulointerstitial inflammation. J Am Soc Nephrol. 2018;29(3):919–935. doi:10.1681/ASN.2017050523
65. Gildea JJ, Seaton JE, Victor KG, et al. Exosomal transfer from human renal proximal tubule cells to distal tubule and collecting duct cells. Clin Biochem. 2014;47(15):89–94. doi:10.1016/j.clinbiochem.2014.06.018
66. Lv LL, Feng Y, Tang TT, Liu BC. New insight into the role of extracellular vesicles in kidney disease. J Cell Mol Med. 2019;23(2):731–739. doi:10.1111/jcmm.14101
67. Erdbrügger U, Blijdorp CJ, Bijnsdorp IV, et al. Urinary extracellular vesicles: a position paper by the urine task force of the international society for extracellular vesicles. J Extracell Vesicles. 2021;10(7):e12093. doi:10.1002/jev2.12093
68. Lv LL, Cao YH, Pan MM, et al. CD2AP mRNA in urinary exosome as biomarker of kidney disease. Clin Chim Acta. 2014;428:26–31. doi:10.1016/j.cca.2013.10.003
69. Prunotto M, Farina A, Lane L, et al. Proteomic analysis of podocyte exosome-enriched fraction from normal human urine. J Proteomics. 2013;82:193–229. doi:10.1016/j.jprot.2013.01.012
70. Yavuz H, Weder MM, Erdbrügger U. Extracellular vesicles in acute kidney injury. Nephron. 2023;147(1):48–51. doi:10.1159/000526842
71. Oh S, Kwon SH. Extracellular vesicles in acute kidney injury and clinical applications. Int J Mol Sci. 2021;22(16):8913. doi:10.3390/ijms22168913
72. Cao H, Cheng Y, Gao H, et al. In vivo tracking of mesenchymal stem cell-derived extracellular vesicles improving mitochondrial function in renal ischemia-reperfusion injury. ACS Nano. 2020;14(4):4014–4026. doi:10.1021/acsnano.9b08207
73. Zhang G, Zou X, Miao S, et al. The anti-oxidative role of micro-vesicles derived from human Wharton-jelly mesenchymal stromal cells through NOX2/gp91(phox) suppression in alleviating renal ischemia-reperfusion injury in rats. PLoS One. 2014;9(3):e92129. doi:10.1371/journal.pone.0092129
74. Li Y, Hu C, Zhai P, et al. Fibroblastic reticular cell-derived exosomes are a promising therapeutic approach for septic acute kidney injury. Kidney Int. 2024;105(3):508–523. doi:10.1016/j.kint.2023.12.007
75. Lu X, Jiang G, Gao Y, et al. Platelet-derived extracellular vesicles aggravate septic acute kidney injury via delivering ARF6. Int J Biol Sci. 2023;19(16):5055–5073. doi:10.7150/ijbs.87165
76. Xiang H, Xu Z, Zhang C, Xiong J. Macrophage-derived exosomes mediate glomerular endothelial cell dysfunction in sepsis-associated acute kidney injury. Cell Biosci. 2023;13(1):46. doi:10.1186/s13578-023-00990-z
77. Kim H, Lee SK, Hong S, et al. Pan PPAR agonist stimulation of induced MSCs produces extracellular vesicles with enhanced renoprotective effect for acute kidney injury. Stem Cell Res Ther. 2024;15(1):9. doi:10.1186/s13287-023-03577-0
78. Ullah M, Liu DD, Rai S, Razavi M, Concepcion W, Thakor AS. Pulsed focused ultrasound enhances the therapeutic effect of mesenchymal stromal cell-derived extracellular vesicles in acute kidney injury. Stem Cell Res Ther. 2020;11(1):398. doi:10.1186/s13287-020-01922-1
79. Wang B, Jia H, Zhang B, et al. Pre-incubation with hucMSC-exosomes prevents cisplatin-induced nephrotoxicity by activating autophagy. Stem Cell Res Ther. 2017;8(1):75. doi:10.1186/s13287-016-0463-4
80. Yuan Y, Yuan L, Yang J, et al. Autophagy-deficient macrophages exacerbate cisplatin-induced mitochondrial dysfunction and kidney injury via miR-195a-5p-SIRT3 axis. Nat Commun. 2024;15(1):4383. doi:10.1038/s41467-024-47842-z
81. Bruno S, Grange C, Deregibus MC, et al. Mesenchymal stem cell-derived microvesicles protect against acute tubular injury. J Am Soc Nephrol. 2009;20(5):1053–1067. doi:10.1681/ASN.2008070798
82. Grange C, Papadimitriou E, Dimuccio V, et al. Urinary extracellular vesicles carrying klotho improve the recovery of renal function in an acute tubular injury model. Mol Ther. 2020;28(2):490–502. doi:10.1016/j.ymthe.2019.11.013
83. Reis LA, Borges FT, Simões MJ, Borges AA, Sinigaglia-Coimbra R, Schor N. Bone marrow-derived mesenchymal stem cells repaired but did not prevent gentamicin-induced acute kidney injury through paracrine effects in rats. PLoS One. 2012;7(9):e44092. doi:10.1371/journal.pone.0044092
84. Alvarez S, Suazo C, Boltansky A, et al. Urinary exosomes as a source of kidney dysfunction biomarker in renal transplantation. Transplant Proc. 2013;45(10):3719–3723. doi:10.1016/j.transproceed.2013.08.079
85. Wu X, Yan T, Wang Z, et al. Micro-vesicles derived from human Wharton’s jelly mesenchymal stromal cells mitigate renal ischemia-reperfusion injury in rats after cardiac death renal transplantation. J Cell Biochem. 2018;119(2):1879–1888. doi:10.1002/jcb.26348
86. Miller D, Eagle-Hemming B, Sheikh S, et al. Urinary extracellular vesicles and micro-RNA as markers of acute kidney injury after cardiac surgery. Sci Rep. 2022;12(1):10402. doi:10.1038/s41598-022-13849-z
87. Shi Z, Wang Q, Zhang Y, Jiang D. Extracellular vesicles produced by bone marrow mesenchymal stem cells attenuate renal fibrosis, in part by inhibiting the RhoA/ROCK pathway, in a UUO rat model. Stem Cell Res Ther. 2020;11(1):253. doi:10.1186/s13287-020-01767-8
88. Aghajani Nargesi A, Lerman LO, Eirin A. Mesenchymal stem cell-derived extracellular vesicles for kidney repair: current status and looming challenges. Stem Cell Res Ther. 2017;8(1):273. doi:10.1186/s13287-017-0727-7
89. Li C, Yu Y, Zhu S, et al. The emerging role of regulated cell death in ischemia and reperfusion-induced acute kidney injury: current evidence and future perspectives. Cell Death Discov. 2024;10(1):216. doi:10.1038/s41420-024-01979-4
90. Zou X, Gu D, Zhang G, et al. NK cell regulatory property is involved in the protective role of MSC-derived extracellular vesicles in renal ischemic reperfusion injury. Hum Gene Ther. 2016;27(11):926–935. doi:10.1089/hum.2016.057
91. Poh BM, Liew LC, Soh YNA, et al. MSC-derived small extracellular vesicles exert cardioprotective effect through reducing VLCFAs and apoptosis in human cardiac organoid IRI model. Stem Cells. 2024;42(5):416–429. doi:10.1093/stmcls/sxae015
92. Ali M, Pham A, Wang X, Wolfram J, Pham S. Extracellular vesicles for treatment of solid organ ischemia-reperfusion injury. Am J Transplant. 2020;20(12):3294–3307. doi:10.1111/ajt.16164
93. Rani S, Ryan AE, Griffin MD, Ritter T. Mesenchymal stem cell-derived extracellular vesicles: toward cell-free therapeutic applications. Mol Ther. 2015;23(5):812–823. doi:10.1038/mt.2015.44
94. Gao Z, Zhang C, Peng F, et al. Hypoxic mesenchymal stem cell-derived extracellular vesicles ameliorate renal fibrosis after ischemia-reperfusion injure by restoring CPT1A mediated fatty acid oxidation. Stem Cell Res Ther. 2022;13(1):191. doi:10.1186/s13287-022-02861-9
95. Quaglia M, Dellepiane S, Guglielmetti G, Merlotti G, Castellano G, Cantaluppi V. Extracellular vesicles as mediators of cellular crosstalk between immune system and kidney graft. Front Immunol. 2020;11:74. doi:10.3389/fimmu.2020.00074
96. Nørgård MØ, Svenningsen P. Acute kidney injury by ischemia/reperfusion and extracellular vesicles. Int J Mol Sci. 2023;24(20):15312. doi:10.3390/ijms242015312
97. Feigerlová E, Battaglia-Hsu SF, Hauet T, Guéant JL. Extracellular vesicles as immune mediators in response to kidney injury. Am J Physiol Renal Physiol. 2018;314(1):F9–F21. doi:10.1152/ajprenal.00336.2017
98. Dieudé M, West LJ, Muruve DA, et al. New answers to old conundrums: what antibodies, exosomes and inflammasomes bring to the conversation. Canadian national transplant research program international summit report. Transplantation. 2018;102(2):209–214. doi:10.1097/TP.0000000000001872
99. Vicencio JM, Yellon DM, Sivaraman V, et al. Plasma exosomes protect the myocardium from ischemia-reperfusion injury. J Am Coll Cardiol. 2015;65(15):1525–1536. doi:10.1016/j.jacc.2015.02.026
100. Paget D, Checa A, Zöhrer B, et al. Comparative and integrated analysis of plasma extracellular vesicle isolation methods in healthy volunteers and patients following myocardial infarction. J Extracell Biol. 2022;1(11):e66. doi:10.1002/jex2.66
101. Livkisa D, Chang TH, Burnouf T, et al. Extracellular vesicles purified from serum-converted human platelet lysates offer strong protection after cardiac ischaemia/reperfusion injury. Biomaterials. 2024;306:122502. doi:10.1016/j.biomaterials.2024.122502
102. Wang B, Xu J, Fu P, Ma L. MicroRNAs in septic acute kidney injury. Burns Trauma. 2023;11:tkad008. doi:10.1093/burnst/tkad008
103. Peerapornratana S, Manrique-Caballero CL, Gómez H, Kellum JA. Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019;96(5):1083–1099. doi:10.1016/j.kint.2019.05.026
104. Zhang R, Zhu Y, Li Y, et al. Human umbilical cord mesenchymal stem cell exosomes alleviate sepsis-associated acute kidney injury via regulating microRNA-146b expression. Biotechnol Lett. 2020;42(4):669–679. doi:10.1007/s10529-020-02831-2
105. Jin C, Cao Y, Li Y. Bone mesenchymal stem cells origin exosomes are effective against sepsis-induced acute kidney injury in rat model. Int J Nanomedicine. 2023;18:7745–7758. doi:10.2147/IJN.S417627
106. Xu L, Hu G, Xing P, Zhou M, Wang D. Corrigendum to ‘paclitaxel alleviates the sepsis-induced acute kidney injury via lnc-MALAT1/miR-370-3p/HMGB1 axis’ [life sci. 2020; 262:118505. doi:10.1016/j.lfs.2020.118505. Epub 2020 sep 28]. Life Sci. 2021;272:119159. doi:10.1016/j.lfs.2021.119159
107. Chawla LS, Davison DL, Brasha-Mitchell E, et al. Development and standardization of a furosemide stress test to predict the severity of acute kidney injury. Crit Care. 2013;17(5):R207. doi:10.1186/cc13015
108. Doi K, Yuen PST, Eisner C, et al. Reduced production of creatinine limits its use as marker of kidney injury in sepsis. J Am Soc Nephrol. 2009;20(6):1217–1221. doi:10.1681/ASN.2008060617
109. Petejova N, Martinek A, Zadrazil J, et al. Acute kidney injury in septic patients treated by selected nephrotoxic antibiotic agents-pathophysiology and biomarkers-a review. Int J Mol Sci. 2020;21(19):7115. doi:10.3390/ijms21197115
110. Zhu Q, Li H, Ao Z, et al. Lipidomic identification of urinary extracellular vesicles for non-alcoholic steatohepatitis diagnosis. J Nanobiotechnology. 2022;20(1):349. doi:10.1186/s12951-022-01540-4
111. Panich T, Chancharoenthana W, Somparn P, Issara-Amphorn J, Hirankarn N, Leelahavanichkul A. Urinary exosomal activating transcriptional factor 3 as the early diagnostic biomarker for sepsis-induced acute kidney injury. BMC Nephrol. 2017;18(1):10. doi:10.1186/s12882-016-0415-3
112. The multiomics landscape of serum exosomes during the development of sepsis - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/35777909/.
113. Ghane Shahrbaf F, Assadi F. Drug-induced renal disorders. J Renal Inj Prev. 2015;4(3):57–60. doi:10.12861/jrip.2015.12
114. Perazella MA, Rosner MH. Drug-induced acute kidney injury. Clin J Am Soc Nephrol. 2022;17(8):1220–1233. doi:10.2215/CJN.11290821
115. Wu T, Ma W, Lu W, et al. Vaccarin alleviates cisplatin-induced acute kidney injury via decreasing NOX4-derived ROS. Heliyon. 2023;9(11):e21231. doi:10.1016/j.heliyon.2023.e21231
116. Zhu S, Huo L, Zeng J, et al. Differentiated management of ROS level in tumor and kidney to alleviate cis-platinum induced acute kidney injury with improved efficacy. J Nanobiotechnology. 2024;22(1):436. doi:10.1186/s12951-024-02710-2
117. Li S, He X, Ruan L, et al. Protective effect of mannitol on cisplatin-induced nephrotoxicity: a systematic review and meta-analysis. Front Oncol. 2021;11:804685. doi:10.3389/fonc.2021.804685
118. Burks SR, Nguyen BA, Tebebi PA, et al. Pulsed focused ultrasound pretreatment improves mesenchymal stromal cell efficacy in preventing and rescuing established acute kidney injury in mice. Stem Cells. 2015;33(4):1241–1253. doi:10.1002/stem.1965
119. Loren P, Saavedra N, Saavedra K, Zambrano T, Moriel P, Salazar LA. Epigenetic mechanisms involved in cisplatin-induced nephrotoxicity: an update. Pharmaceuticals. 2021;14(6):491. doi:10.3390/ph14060491
120. Herrera Sanchez MB, Bruno S, Grange C, et al. Human liver stem cells and derived extracellular vesicles improve recovery in a murine model of acute kidney injury. Stem Cell Res Ther. 2014;5(6):124. doi:10.1186/scrt514
121. Grange C, Iampietro C, Bussolati B. Stem cell extracellular vesicles and kidney injury. Stem Cell Investig. 2017;4:90. doi:10.21037/sci.2017.11.02
122. Tapparo M, Bruno S, Collino F, et al. Renal regenerative potential of extracellular vesicles derived from miRNA-engineered mesenchymal stromal cells. Int J Mol Sci. 2019;20(10):2381. doi:10.3390/ijms20102381
123. Zhang Y, McNeill E, Tian H, et al. Urine derived cells are a potential source for urological tissue reconstruction. J Urol. 2008;180(5):2226–2233. doi:10.1016/j.juro.2008.07.023
124. Li F, Zhao B, Zhang L, et al. Therapeutic potential of urine-derived stem cells in renal regeneration following acute kidney injury: a comparative analysis with mesenchymal stem cells. World J Stem Cells. 2024;16(5):525–537. doi:10.4252/wjsc.v16.i5.525
125. Li Y, Wang J. Contrast-induced acute kidney injury: a review of definition, pathogenesis, risk factors, prevention and treatment. BMC Nephrol. 2024;25(1):140. doi:10.1186/s12882-024-03570-6
126. Petejova N, Martinek A. Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care. 2014;18(3):224. doi:10.1186/cc13897
127. Ko A, Song J, Golovko G, et al. Higher risk of acute kidney injury and death with rhabdomyolysis in severely burned patients. Surgery. 2022;171(5):1412–1416. doi:10.1016/j.surg.2021.09.029
128. Schult L, Halbgebauer R, Karasu E, Huber-Lang M. Glomerular injury after trauma, burn, and sepsis. J Nephrol. 2023;36(9):2417–2429. doi:10.1007/s40620-023-01718-5
129. Rashidi HH, Makley A, Palmieri TL, et al. Enhancing military burn- and trauma-related acute kidney injury prediction through an automated machine learning platform and point-of-care testing. Arch Pathol Lab Med. 2021;145(3):320–326. doi:10.5858/arpa.2020-0110-OA
130. Rashidi HH, Sen S, Palmieri TL, Blackmon T, Wajda J, Tran NK. Early recognition of burn- and trauma-related acute kidney injury: a pilot comparison of machine learning techniques. Sci Rep. 2020;10(1):205. doi:10.1038/s41598-019-57083-6
131. Halbgebauer R, Karasu E, Braun CK, et al. Thirty-eight-negative kinase 1 is a mediator of acute kidney injury in experimental and clinical traumatic hemorrhagic shock. Front Immunol. 2020;11:2081. doi:10.3389/fimmu.2020.02081
132. Yang G, Tan L, Yao H, Xiong Z, Wu J, Huang X. Long-term effects of severe burns on the kidneys: research advances and potential therapeutic approaches. J Inflamm Res. 2023;16:1905–1921. doi:10.2147/JIR.S404983
133. Yun CW, Lee SH. Potential and therapeutic efficacy of cell-based therapy using mesenchymal stem cells for acute/chronic kidney disease. Int J Mol Sci. 2019;20(7):1619. doi:10.3390/ijms20071619
134. Tan BK, Liew ZH, Kaushik M, Cheah AKW, Tan HK. Early initiation of renal replacement therapy among burned patients with acute kidney injury. Ann Plast Surg. 2020;84(4):375–378. doi:10.1097/SAP.0000000000002197
135. Lu Y, Wang L, Zhang M, Chen Z. Mesenchymal stem cell-derived small extracellular vesicles: a novel approach for kidney disease treatment. Int J Nanomedicine. 2022;17:3603–3618. doi:10.2147/IJN.S372254
136. Zhang B, Tian X, Hao J, Xu G, Zhang W. Mesenchymal stem cell-derived extracellular vesicles in tissue regeneration. Cell Transplant. 2020;29:963689720908500. doi:10.1177/0963689720908500
137. Peake PW, Pianta TJ, Succar L, et al. A comparison of the ability of levels of urinary biomarker proteins and exosomal mRNA to predict outcomes after renal transplantation. PLoS One. 2014;9(2):e98644. doi:10.1371/journal.pone.0098644
138. Panah F, Ghorbanihaghjo A, Argani H, Asadi Zarmehri M, Nazari Soltan Ahmad S. Ischemic acute kidney injury and klotho in renal transplantation. Clin Biochem. 2018;55:3–8. doi:10.1016/j.clinbiochem.2018.03.022
139. Endre ZH, Pickering JW, Walker RJ. Clearance and beyond: the complementary roles of GFR measurement and injury biomarkers in acute kidney injury (AKI). Am J Physiol Renal Physiol. 2011;301(4):F697–707. doi:10.1152/ajprenal.00448.2010
140. Sedej I, Štalekar M, Tušek Žnidarič M, et al. Extracellular vesicle-bound DNA in urine is indicative of kidney allograft injury. J Extracell Vesicles. 2022;11(9):e12268. doi:10.1002/jev2.12268
141. Bernal C, How-Volkman C, Spencer M, El-Shamy A, Mohieldin AM. The role of extracellular vesicles in SARS-CoV-2-induced acute kidney injury: an overview. Life. 2024;14(2):163. doi:10.3390/life14020163
142. Ullah M, Liu DD, Rai S, et al. A novel approach to deliver therapeutic extracellular vesicles directly into the mouse kidney via its arterial blood supply. Cells. 2020;9(4):937. doi:10.3390/cells9040937
143. Nassar W, El-Ansary M, Sabry D, et al. Umbilical cord mesenchymal stem cells derived extracellular vesicles can safely ameliorate the progression of chronic kidney diseases. Biomater Res. 2016;20:21. doi:10.1186/s40824-016-0068-0
144. Roefs MT, Sluijter JPG, Vader P. Extracellular vesicle-associated proteins in tissue repair. Trends Cell Biol. 2020;30(12):990–1013. doi:10.1016/j.tcb.2020.09.009
145. Ding JY, Chen MJ, Wu LF, et al. Mesenchymal stem cell-derived extracellular vesicles in skin wound healing: roles, opportunities and challenges. Mil Med Res. 2023;10(1):36. doi:10.1186/s40779-023-00472-w
146. Zhang X, Liu J, Yu B, Ma F, Ren X, Li X. Effects of mesenchymal stem cells and their exosomes on the healing of large and refractory macular holes. Graefes Arch Clin Exp Ophthalmol. 2018;256(11):2041–2052. doi:10.1007/s00417-018-4097-3
147. O’Driscoll L. Extracellular vesicles from mesenchymal stem cells as a covid-19 treatment. Drug Discov Today. 2020;25(7):1124–1125. doi:10.1016/j.drudis.2020.04.022
148. Liu J, Sun X, Zhang FL, et al. Clinical potential of extracellular vesicles in type 2 diabetes. Front Endocrinol. 2020;11:596811. doi:10.3389/fendo.2020.596811
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Mesenchymal Stem Cell-Derived Small Extracellular Vesicles: A Novel Approach for Kidney Disease Treatment
Lu Y, Wang L, Zhang M, Chen Z
International Journal of Nanomedicine 2022, 17:3603-3618
Published Date: 13 August 2022
Emerging Role and Mechanism of Mesenchymal Stem Cells-Derived Extracellular Vesicles in Rheumatic Disease
Wang Z, Yang C, Yan S, Sun J, Zhang J, Qu Z, Sun W, Zang J, Xu D
Journal of Inflammation Research 2024, 17:6827-6846
Published Date: 30 September 2024
MSC-Derived Extracellular Vesicles: Roles and Molecular Mechanisms for Tissue Repair
Wu T, Liu Y, Wang S, Shi C
International Journal of Nanomedicine 2025, 20:7953-7974
Published Date: 21 June 2025