")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Feasibility of Closed-Loop TCI Based on New EEG Baseline in the Presence of Low Dose of Esketamine: A Randomized Controlled Equivalence Trial
Authors Li X , Li S, Xu C, He H, Shao W, Zhan S, Xu B
Received 24 November 2024
Accepted for publication 4 April 2025
Published 25 April 2025 Volume 2025:19 Pages 3237—3252
DOI https://doi.org/10.2147/DDDT.S508264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Xiaoshan Li,1,2,* Shengchao Li,1,2,* Chanyan Xu,1 Huan He,1 Weidong Shao,1 Shuteng Zhan,1,2 Bo Xu1,2
1Department of Anesthesiology, General Hospital of Southern Theater Command of PLA, Guangzhou, Guangdong, People’s Republic of China; 2The First School of Clinical Medicine, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Xu, Department of Anesthesiology, General Hospital of Southern Theater command of PLA, 111 Liuhua Road, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Objective: This research aimed to quantify the impact of low dose of esketamine on BIS and validate the feasibility of closed-loop TCI system based on the new BIS baseline with low dose of esketamine.
Methods: This study consisted of two phases. The first phase was to quantify the impact of a low dose of esketamine (0.2mg kg− 1 bolus, 5μg kg− 1 min− 1 infusion for 30min) on BIS and establish a new BIS baseline for propofol-remifentanil general anesthesia. The second phase was used to validate the feasibility of closed-loop TCI system based on the new BIS baseline. One hundred and eleven patients were randomly and equally assigned to three groups (group A: adjusted group, group N: non-adjusted group and group C: control group). After administering a low dose of esketamine, group A adjusted drug dosage based on new BIS baseline, while group N based on the original BIS baseline of 50, group C adjusted drug doses based on the original baseline of 50 without esketamine. Main outcome was controller performance (% time within± 10units of the BIS setpoint). Secondary outcomes were drug consumption, occurrence of adverse events such as intraoperative awareness, treatment of hemodynamic changes and postoperative recovery quality.
Results: In the first phase, after administering a low dose of esketamine, the BIS increased from 49.9± 4.5 to 59.6± 6.0, p< 0.01. In the second phase, the controller performance in group A and N were within the range of high-performance systems, and both were equivalent with control group. Group A showed lower consumption of propofol compared to control group (5.58± 1.12 vs 6.69± 1.36 (mg·kg− 1·h− 1), p< 0.05). There was no difference in adverse events such as intraoperative awareness, recovery assessment and postoperative VAS, PONV and shivering, QoR-15 assessment after adjusting the BIS baseline.
Conclusion: It is feasible to operate the closed-loop TCI system based on the adjusted BIS baseline in the presence of low dose of esketamine.
Keywords: esketamine, new BIS baseline, EEG, closed-loop controlled system, depth of anesthesia
Introduction
Esketamine is the dextro-isomer of ketamine, which was approximately twice as affinized to NMDAR as ketamine and has faster metabolism, stronger potency, better sedation and analgesia effect and fewer side effects.1–3 As an adjuvant intravenous anesthetic drug, low dose of esketamine has been demonstrated to better maintain hemodynamic stability,4 offer analgesic effects5,6, reduce usage of opioids5 and promote postoperative recovery.7,8
Closed-loop target-controlled infusion (TCI) system can continuously adjust drug infusion rate or effect-site concentration in real-time based on patient’s physiological parameters and drug effects. Its purpose is to optimize drug delivery to meet the patient’s needs, improve safety and reduce the occurrence of underdosing or overdosing.9,10 The bispectral index (BIS), a derivation of the original electroencephalogram (EEG), is the only FDA-approved index for assessing depth of anesthesia11 by monitoring the functional state and changes in the prefrontal cortex. BIS is well correlated with anesthetics that mainly act via γ-aminobutyric acid receptors (GABARs), such as propofol, midazolam, and sevoflurane and has a dose-related effect with these drugs.12 With BIS-guided anesthesia, we can better adjust drug consumption, reduce the occurrence of neurological complications and facilitate early postoperative recovery.13,14 In recent years, a number of closed-loop control infusion systems of anaesthetics based on BIS are available and have been validated to be more superior than manual control.15
Theoretically, a combined use of low dose of esketamine can reduce other anesthetic drug consumption.16 However, due to the pharmacological property of esketamine to increase EEG index,17 esketamine application in closed-loop systems that rely solely on EEG as the feedback parameter has certain limitations. Napoleone et al have demonstrated that low dose of ketamine did not compromise the overall safety and stability of the closed-loop system but led to increased consumption of propofol and longer recovery time.18 Therefore, this study aimed to quantify the impact of low dose of esketamine (0.2mg·kg−1) on BIS (EEG) and validate the feasibility and safety of this new BIS (EEG) baseline in the application of closed-loop control TCI system. Through this research, not only can the advantages of esketamine be brought into play but also the dosage of general anesthetic drugs can be precisely controlled, thereby reducing complications.
Methods
Study Design and Ethical Approval
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of General Hospital of Southern Theater command of PLA (NZLLKZ) on 5th December 2024. Written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrollment at ClinicalTrial.gov (NCT06729892). Throughout this manuscript, CONSORT guidelines were adhered to (http://www.consort-statement.org/).
This study proceeded with two phases: In the first phase, we investigated and quantified the increase in BIS after the administration of low dose of esketamine (0.2mg·kg−1 bolus followed by a continuous 5 μg·kg−1·min−1 infusion) during propofol-remifentanil general anesthesia and established a new BIS baseline. Then, in the second phase, we validated the feasibility of the closed-loop TCI system based on the new BIS baseline by a randomized controlled equivalence trial.
Patient Population
We recruited adult patients (18–55 years of age), undergoing elective laparoscopic surgery at the Southern Theater General Hospital of PLA, Male or female, BMI 18–27kg/m2, with the American Society of Anesthesiologists (ASA) physical status I–II. All the patients were appropriate for propofol and remifentanil TCI. Any patients with the following criteria were excluded from the study: known or suspected neurological illnesses, strokes, tumors, degenerative neurological disorders, epileptic seizures, serious head injuries, cognitive disorders, post-traumatic stress disorder, mental illnesses, severe depression and psychosis; recent use of psychotropic drugs; history of drug abuse or drug addiction or during pregnancy; involvement in other clinical trials with other drugs or devices.
Randomization and Blinding
Phase I: This phase was a self-controlled trial without randomization and blinding.
Phase II: This phase was a single center, randomized controlled trial with three parallel groups, blinded to both patients and assessors. Researcher A was responsible for patient enrollment and assignment to three groups: group A (adjusted group), group N (non-adjusted group) and group C (control group) based on a computer-generated random number table (stattrek.com/statistics/random-number-generator.aspx). The grouping information was securely sealed within an opaque envelope. Upon the patient’s arrival, the envelope was handed over to a skilled anesthesiologist who had extensive clinical experience and had received training in closed-loop TCI systems. It was important to note that this anesthesiologist was not directly involved in the data collection and analyze. To minimize information bias, researcher B, who was present but unaware of the patient’s BIS baseline and drug usage, conducted data collection of intraoperative vital signs and adverse events, drug consumption, recovery assessment during emergence period and postoperative follow-up. After collecting data from all the patients, EEG background data would be exported and handed over to a data analyst who was uninvolved in the study for analysis. Other data would be analyzed by researcher B. Unblinding occurred exclusively under predefined exigent circumstances (eg, severe allergic reactions, equipment malfunction, or intraoperative hemorrhage exceeding 20% blood volume), as determined by the attending anesthesiologist. Full group disclosure by Researcher A was deferred until database lock and completion of all statistical analyses.
Study Procedure
Phase I
Preparation and Induction of Anesthesia
All patients were fasted for 12h and no pre-medicine was given. On entry to the operating room, noninvasive blood pressure (NIBP), electrocardiography for heart rate (HR), and pulse oxygen saturation (SpO2) were applied to all patients (N15 Anesthesia Monitor, Mindray, China). BIS monitor (Vista v. 3.22, aspect Medical, covidien, Dublin, Ireland) was then connected to patient, ensuring that the electrode impedance remained below 5 kΩ. Depth of neuromuscular blocking monitor was also utilized (FI-00510, Finland). Throughout the entire anesthesia process, effect-concentration-based TCI models for propofol and remifentanil were selected. The Schnider model was used for propofol, and the Minto model was employed for remifentanil, with the infusion devices being the 8713030 Perfusor Space (Germany).
After loss of consciousness, 0.6 mg kg−1 rocuronium was injected intravenously. When BIS dropped to 60 and train-of-four (TOF) was 1–3, a laryngeal mask or tracheal tube was inserted for mechanical ventilation. The tidal volume was set at 8–12 mL kg−1 with a respiratory rate of 12 min−1, and an inspiratory to expiratory ratio of 1:2, aiming to maintain the end-tidal carbon dioxide partial pressure (PetCO2) within the range of 35–45 mmHg (1 mmHg = 0.133 kPa).
Anesthetic Maintenance and Intervention
Once the surgery began and depth of anesthesia was maintained steadily (BP and HR changes ≤20% and BIS maintained between 40–60) for 30 minutes, a low dose of esketamine (Lot No. H20193336, Jiangsu Hengrui Pharmaceutical Co., Ltd, Jiangsu, China) administered (0.2mg kg−1 administered intravenously over 30 seconds followed by a continuous infusion of 5 μg kg−1 for 30min).
After the esketamine administration, the BIS display interface was covered with an opaque curtain. During the following 30-minute period, the anesthesiologist empirically adjusted the dosages of propofol and remifentanil based on the patient’s clinical reactions. Other than regulating depth of anesthesia experimentally, required hemodynamic changes were treated in both phases. An injection of dopamine (1–2 mg) was administered when the blood pressure was less than 70% of the pre-induction value and nicardipine (titration of 1 mg in 10 minutes) followed when systolic BP exceeded 150mmhg; when HR was <45 bpm, atropine of 0.01mg/kg was administered and esmolol of 10mg when HR exceeded 140 bpm. To avoid EMG effect on EEG, continuous infusion of rocuronium (3–5 μg·kg−1·min−1) to maintain TOF between 1–319 and was halted 30 min before the anticipated end of the operation.
All interventions and adjustments were meticulously documented. After the completion of the trials for 24 cases, BIS data were extracted, and the changes in BIS after esketamine administration were analyzed and calculated for use in Phase II.
Phase II: Pre-anesthetic preparation and induction procedures were the same as in the first phase.
Anesthesia Maintenance and Intervention
After the initiation of mechanical ventilation and a 5-minute period of stable anesthesia depth and hemodynamics, esketamine administration commenced in Group A (the adjusted group) and Group N (the non-adjusted group). The regimen was a 0.2mg·kg⁻¹ bolus followed by an infusion of 5 μg·kg⁻¹·min⁻¹. Group C (the control group) received an equivalent volume of saline. Ten minutes after the start of esketamine infusion, in Group A, a closed-loop system based on an adjusted BIS baseline of 59.6 (derived from Phase I) was activated. In Group N and Group C, the closed-loop system was based on the original BIS baseline of 50.
All the three groups adjusted effect-site concentration of propofol and remifentanil every minute by the specific formular (details listed in the Supplementary Material and explanation).20 A standard personal computer was used as an interface to control communication with the BIS monitor and with both propofol and remifentanil infusion pumps via an RS232 serial port (Infusion Toolbox 95® version 4.11 software21,22). This interface enabled (1) providing a user interface to enter patient’s demographic data (sex, age, weight and height) and set modification of upper and lower limits of drug concentrations; (2) calculating effect-site concentrations of propofol and remifentanil using the pharmaco-kinetic populations; (3) displaying these calculated effect-site concentration estimates in real time; (4) controlling the propofol and remifentanil infusion pumps; and (5) recording BIS, and calculating effect-site concentrations. The controller has been described extensively in previous randomized controlled trials.20,23,24 The controller automatically adjusted the effect-site concentrations of propofol and remifentanil to maintain the BIS value as close as possible to 50 in Group N and Group C, and to the new BIS baseline of 59.6 in Group A. The target BIS range was 40 ~ 60 in Group N and Group C, and 50 ~ 70 in Group A. The target concentration ranges for propofol was 2.0–5.0 μg·mL⁻¹ and remifentanil was 3–7 ng·mL⁻¹.
Notably, if signs of inadequate analgesia such as tachycardia, hypertension, sweating, facial flushing, body movement, or if the BIS exceeded the target range occurred during the surgical procedure in any group, the attending anesthesiologist could override the system to maintain the BIS within the predefined range. Additionally, the trial could be terminated at the anesthesiologist’s discretion if necessary. During the anesthesia maintenance phase, the depth of muscle relaxation was continuously monitored to keep the TOF count between 1–3.
Esketamine infusion continued for 40 minutes in all three groups, and the closed-loop control based on different BIS baselines was maintained for 50 minutes. Hydromorphone 8 μg·kg−125 and ondansetron 8mg as analgesic and antiemetic drugs was given 20 to 30 minute before the anticipated end of surgery or after the end of closed-loop TCI control.
In each case, researcher B for data-collecting was presented to ensure compliance with the research protocol, record any adverse events and their management, as well as document the time and reasons for any open-loop adjustments of drug dosages.
Emergence Period and Post-Operative Follow-Up
At the end of the surgery, the drug infusion was tapered at the discretion of anesthesiologists. The endotracheal tube was removed from patients after their spontaneous respiration recovered and the TOF ratios ≥0.9. If necessary, muscle relaxant antagonist was administered. After endotracheal tube removal, patients were transferred to the Post-Anesthesia Care Unit (PACU) if they were able to provide oriented responses and have a muscle strength of level 4 or above. Adverse reactions such as pain,26 nausea and vomiting, and shivering27 were recorded upon admission to the PACU, as well as 30 minutes and 1 hour later. If the Visual Analogue Scale (VAS) score was >3, 0.1 μg·kg−1 of sufentanil was administered. On the 1st, 3rd, and 7th days after surgery, the Modified Brice questionnaire28 was used to assess the patient’s level of intraoperative awareness, and the Quality of Recovery (QoR - 1529) was evaluated.
Primary and Secondary Outcomes
Phase I: The main outcome was the changes in BIS value after the administration of esketamine.
Phase II: primary outcome: % of time within ± 10 units of the BIS setpoint during closed-loop control (performance metric). The time of closed-loop control for group A and group N was defined as starting 10 minutes after the addition of esketamine and lasting for 40min, ending until 10 minutes after the cessation of esketamine infusion. For group C, it was defined as starting when anesthesia depth stabilized 5 minutes after intubation, ending up with 50 min of closed-loop control.
Secondary outcomes: drug consumption, cases with treatment of hypotension or hypertension, treatment of tachycardia or bradycardia, open-loop drug adjustment, intraoperative somatic events. Postoperative recovery assessment included time to BIS >80, time to regain spontaneous breathing, time to answer questions and time to extubate. Additionally, VAS, extra analgesic drug application (0.1μg·kg−1 of sufentanil each time), cases with nausea and vomiting, shivering at administration, 30min and 1 hour at PACU and intraoperative awareness assessment, 15-item quality of recovery (QoR-15) on day 1st, 3rd and 7th after surgery were documented.
Statistical Methods
Sample Size
Phase II: The primary outcome of this phase was % time within ± 10 units of the BIS setpoint. Based on previous study, we assumed that this performance metric in control group was 85±10(%). A 20% change in this performance metric of the control group would be considered as a clinical meaningful difference.30 After adding esketamine, we assumed that these differences were equivalent by half;31 which is, ±10% of 85(%). When 95% CI for the differences between groups A and C, group N and C were entirely within the equivalence range, controller performance would be considered equivalent. Our analysis based on a “Two-Sample T-Tests for Equivalence Allowing Unequal Variance” determined that 72 participants would be required (24 patients each) to demonstrate equivalent controller performance, based on an equivalence range of ±8.5, an α of 0.05, and a power of 90%. We aimed to recruit 114 patients with a potential dropout rate of 35%.
The number of patients required in both phases was calculated using the PASS software (version 11.0.7; NCSS, LCC, Kaysville, UT).
Statistical Analysis
Continuous variables were tested for normal distribution using Kolmogorov–Smirnov. Normally distributed data were presented as mean ± SD, skewed data were presented as median (interquartile range, IQR) and categorical data were presented as number (%).
To assess between-group differences, normally distributed data (BIS, SEF, % time within ± 10 units of BIS setpoint, mean propofol dosage and mean remifentanil dosage) were compared using 2 independent t-test. Skewed data (Time to BIS>80(min), time to automatic breathing, time to answering question, time to extubate, VAS and extra sufentanil dosage, QoR-15) were compared using the Mann–Whitney test. Categorical data (treatment of hypertension or hypotension, treatment of tachycardia or bradycardia, treatment of manual drug and cases with PONV, shivering and intraoperative awareness) were analyzed using Fisher’s exact test. The criterion for determining the statistical significance of differences is a p value less than 0.05. Statistical analyses were performed using SPSS 24.0 (SPSS, Inc., Chicago, IL) and the GraphPad Prism software (version 10.00; GraphPad, San Diego, CA). Detailed information about each test was provided on the tables.
Results
In the first phase, 24 patients for selective laparoscopic surgery were included, with a male-to-female ratio of 13:11. The mean±SD age was 45 ± 12 years, and the mean±SD BMI was 23.9±2.7 kg· m−2. All the patients were ASA I–II. To evaluate the impact of esketamine on BIS, we compared BIS values at distinct time points (T0, T5, T10, T15, T20) with BIS(mean) prior to esketamine administration. Additionally, BIS values were compared at 5-minute intervals following esketamine injection. Notably, significant alterations in BIS were observed starting from T5, and BIS values remained stable from T10 to T30. Thus, we extracted and analyzed EEG recordings, without interference of other anesthetic drugs, state of inadequate depth of anesthesia such as hypertension and/or tachycardia, after the esketamine administration for 10 minutes. Compared to the previous 20min without esketamine, BIS increased from 49.9± 4.5 to 59.6 ± 6.0, mean difference ± SD: 9.6 ± 3.0, p<0.0001. (Figure 1, Table 1). There were no statistically significant differences in the Ce Propofol(ng/mL) and Ce Remifentanil(ug/mL) after esketamine administration, suggesting that esketamine was the only factor to affect BIS. Therefore, 59.6 (50+9.6) was set to be the new BIS baseline and 50–60 be BIS control range for closed-loop TCI control with low dose of esketamine in the second phase. After administering esketamine, 95% SEF increased from 12.15 ± 1.46 to 14.84 ± 1.43, p<0.0001 (Table 1).
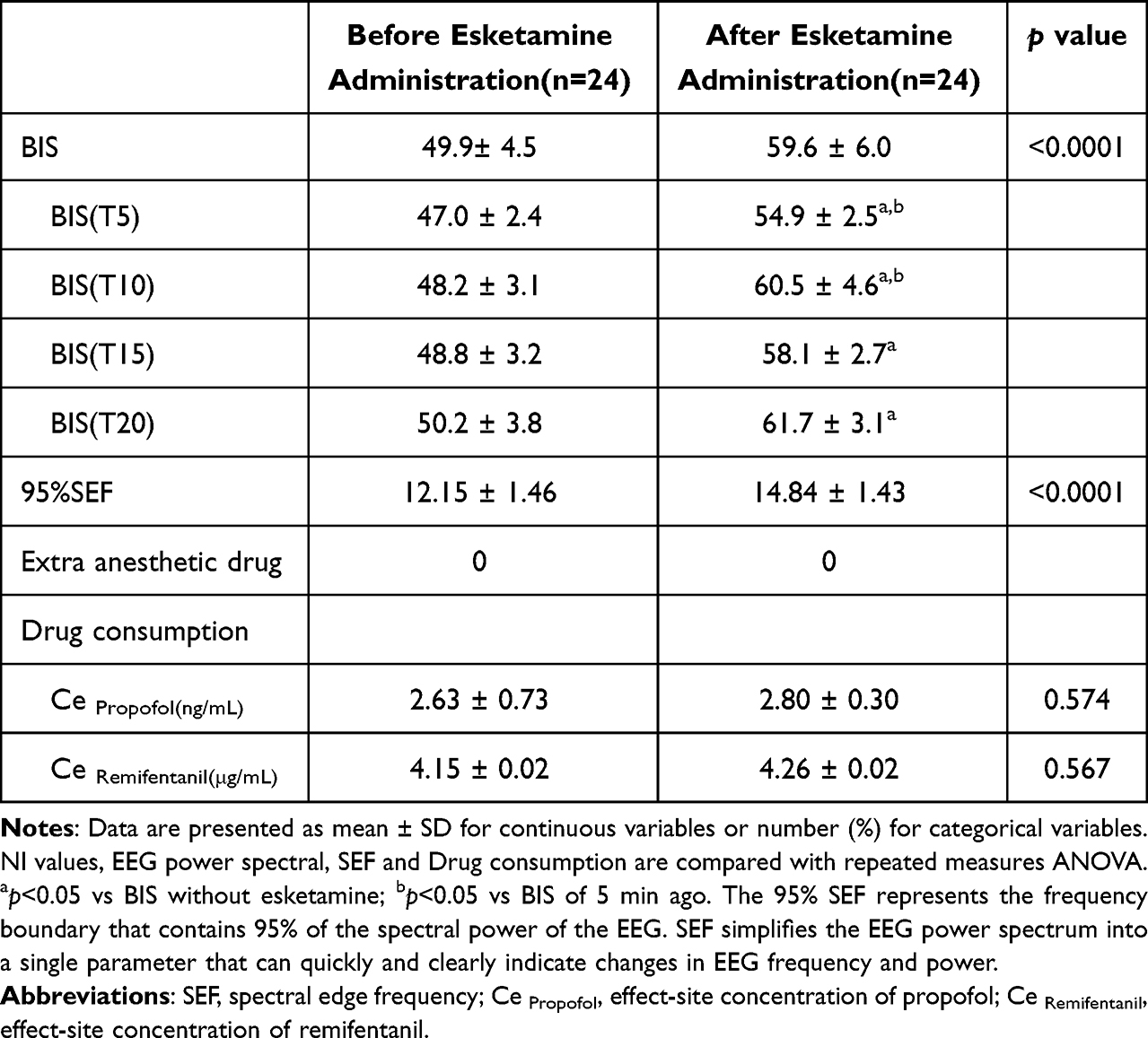 |
Table 1 EEG Data and Drug Consumption Before and After Administration of Esketamine in Phase I |
 |
Figure 1 Esketamine added after 30min of stable depth of anesthesia. After 10 min of administration of esketamine, BIS maintain stable; **Stable 20min maintenance of BIS after esketamine administration vs 20min of BIS before esketamine administration: p<0.01. |
In the second phase, a total of 140 patients were assessed for eligibility. Twenty-nine patients failed to be included for randomization. Consequently, 111 patients were included and randomly divided into three groups: group C (n = 37), group A(n = 37), and group N(n = 37) (Figure 2). Finally, a total of 78 patients (26 in group C, 27 in group A, and 25 in group N) were included in the final analysis. The general characteristics of the included subjects and basic surgery information were presented in Table 2.
 |
Table 2 General Characteristic of Patients and Basic Surgery Information in Phase II |
 |
Figure 2 CONSORT diagram in Phase II. CONSORT indicates CONsolidated Standards Of Reporting Trials. Abbreviations: Group C, Control group; Group A, BIS baseline adjusted group; Group N, BIS baseline non-adjusted group. |
EEG Data and Performance of Closed-Loop Controlled System Analysis in Phase II
After the administration of low-dose esketamine or saline and continuous infusion for a period, BIS in each group all fluctuated within ± 10 units of the BIS setpoint under closed-loop control (Figure 3, Table 3). Time ratio (%) of BIS within the target range (performance metric (%)) was 80.0 ± 7.7 (%) in the group A, 83.6 ± 10.0 (%) in the group N, and 84.8 ± 9.8 in group C (Table 3). Compare to group C, performance metric (%) of closed-loop control system in group A and group N were stable, and their 95% CI for the difference to group C were lied within the equivalence range: difference between group A and group C: (95% CI,-9.70 to 0.24),p=0.062; group N and group C: (95% CI,-6.80 to 4.50), p=0.692 (Table 3).
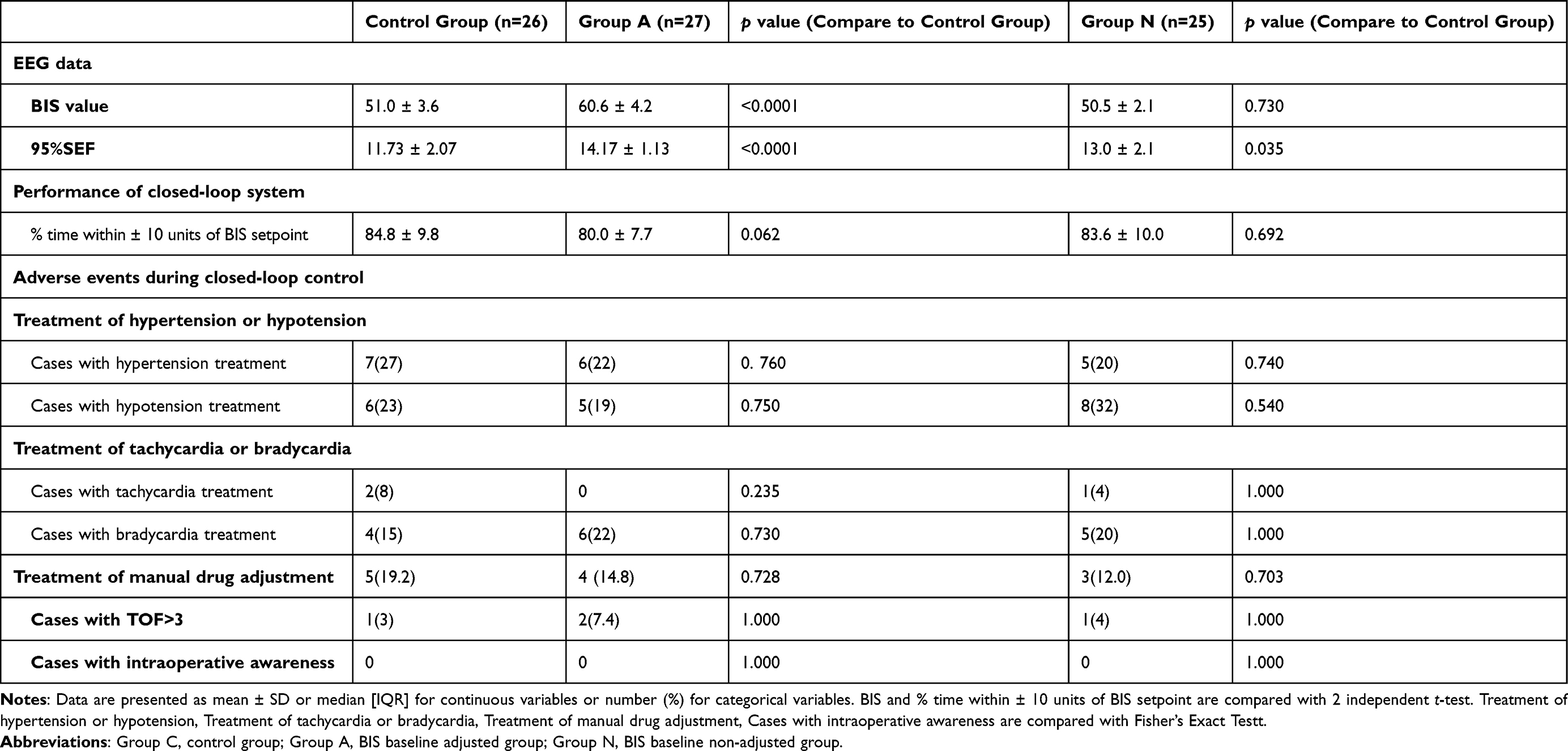 |
Table 3 EEG Data, Performance of Closed-Loop System, Adverse Events During Closed-Loop Control in Phase II |
 |
Figure 3 Duration of BIS recording analysis during closed-loop TCI in phase II. Abbreviations: Group C, control group; Group A, BIS baseline adjusted group; Group N, BIS baseline non-adjusted group. |
Drug Consumption in Each Group in Phase II
During the anesthesia maintenance under the closed-loop control, group A showed lower consumption of propofol compare to group C: 5.58 ± 1.12 vs 6.69 ± 1.36 (mg·kg−1·h−1), p=0.002 (Table 4, Figure 4). While compared to group C, group N(non-adjusted group) showed higher consumption of propofol: 8.16 ± 1.16 vs 6.69 ± 1.36 (mg·kg−1·h−1), p<0.001 (Table 4, Figure 4). Compared to group C, group N showed higher consumption of remifentanil: 0.15 ± 0.04 vs 0.12 ± 0.04 (μg·kg−1·h−1), p=0.025.(Table 4).
 |
Table 4 Drug Consumption During Closed-Loop Control in Phase II |
 |
Figure 4 Propofol consumption during closed-loop TCI in each group in phase II. Abbreviations: Group C, Control group; Group A, BIS baseline adjusted group; Group N, BIS baseline non-adjusted group. Note: Results are presented as box-plots.**p<0.01; ***p<0.001. |
Perioperative Adverse Events in Each Group in Phase II
Neither Group A nor Group N exhibited significant differences in the management of hypertension, hypotension, tachycardia, bradycardia, or in manual drug adjustments (Table 3). Additionally, in contrast to Group C, Group A had no occurrences of intraoperative awareness (Table 3).
However, in the assessment of postoperative consciousness recovery during the emergence period, which included parameters such as BIS > 80, the recovery of automatic breathing, the ability to answer questions, and extubation, Group N had significantly longer recovery times compared to Group C (Table 5). In contrast, no differences were observed between Group A and Group C (Table 5).
 |
Table 5 Comparison of Postoperative Recovery Assessment and Intraoperative Awareness in Phase II |
The postoperative follow-up outcomes at the PACU indicated that there were no statistically significant disparities between Group A and Group C in terms of the incidence of shivering, nausea and vomiting, Visual Analogue Scale (VAS) scores, additional analgesic drug dosages, and QoR-15 scores (Table 5).
There were no statistically significant differences in the TOF values at various time points during surgery in each group, as well as the loading dose of analgesic and antiemetic medication in three groups. Only 3 patients (1 in group A, 2 in group N) receive muscarinic antagonists during the emergence period. There was no patient-safety compromising harms or unintended adverse events in each group.
Discussion
The feasibility and safety of the closed-loop target-controlled infusion system in this study based on new BIS baseline was validated in the presence of low-dose esketamine. Although both adjusted and non-adjusted groups can maintain stable performance during closed-loop control after administering esketamine, it is noted that there was a reduction in propofol dosage under the new BIS baseline without increasing intraoperative awareness and other adverse events compared to control group.
During general anesthesia, BIS is a sensitive and specific indicator of the depth of anesthesia under propofol-based general anesthesia.32 Due to the inhibition of the NMDA receptors in interneurons, ketamine leads to disinhibition of downstream excitatory neurons, resulting in dose-related increased cortical neuron activity.28 This excitatory effect is reflected in higher frontal cortical EEG frequency, such as the increase β-(15~25hz) and γ-range (25–40hz) oscillation.33,34 Hayashi et al found that ketamine had a dose-dependent shift in the peak frequency of the α-spindles when co-administered with propofol, which was also related to the increase higher-frequency oscillations.35
During propofol-remifentanil anesthesia, Van Heusden et al found that both doses of 0.5mg kg-1, 10 μg kg−1 · min−1 and 0.25mg· kg-1,5 μg kg−1 · min−1 of ketamine resulted in an increase in EEG index (median difference 95% CI: 10.2–19.2 and 4.7–20.4)32 by WAVcns monitor, which is consistent with the changes in BIS observed in our study. However, D. Faraoni et al found that low bolus infusion of ketamine 0.2 mg·kg−1 administered over a 5 min period did not increase the BIS value over the next 15 min.36 In a study compared the impact of bolus versus continuous infusion of intravenous ketamine on BIS under desflurane administration, Lucie Carrara37 found that a ketamine bolus (0.25mg·kg−1) significantly increased the BIS compared to ketamine infusion (0.25 mg·kg−1·h−1). A retrospective study showed that in the context of sevoflurane infusion, 20 mg of ketamine raised the BIS by 3.8, while 50 mg doses raising the BIS by about 10,38 which is consistent with Liyuan Ren,39 who found that there is a dose-dependent effect of esketamine on EEG. In conclusion, there were many factors associated with the effects of esketamine on EEG, which may be related to doses and regimens of drug administration and may be due to different anesthetic contexts. The main reason may be related to the blood concentration of esketamine and its impact on EEG activity. One other study40 conducted a pharmacokinetic simulation of plasma ketamine concentration found that either the slow administration of 0.2 mg∙kg−1 over 5 min or the rapid bolus administration of a dose of 0.5 or 0.4 mg∙kg−1 followed by 1 mg∙kg−1h−1, the peak plasma concentrations of ketamine were, respectively, 597, 2412 and 1900 ng∙mL−1 after these regimens. Compared to single injections, 0.4 mg∙kg−1 followed by a continuous infusion of 1 mg∙kg−1h−1 maintained a more stable plasma concentration below 1000ng∙m−12−1,40 which was probably account for stable effect of esketamine on EEG in our study. Napoleone and et al had confirmed that adding subanesthetic doses of ketamine (0.25 mg∙kg−1 bolus followed by a continuous 5 µg∙kg−1∙min−1 infusion) to a general anesthesia with propofol and remifentanil did not affect the stability of the closed-loop TCI system, but the doses of propofol had increased.18 Esketamine is the purified S-enantiomer of ketamine.16 Its effect on the EEG is assumed to be similar to that of ketamine. Based on these studies and our previous observation, we quantified the impact of low dose of esketamine on BIS (EEG) during a period of stable anesthesia maintenance and established a new BIS baseline, which was then validated to be feasible under closed-loop control.
In this study, the % time within ± 10 units of the BIS setpoint in the esketamine group and the control group were 80.3 ± 7.8 (%) and 84.6 ± 10.7 (%), respectively. This was within the range of target maintenance achieved by other high-performance closed-loop systems, which range from 75% ± 13% to 94% ± 12%.15 95% CI of the difference (performance metric) between these two groups was also lied within the equivalence range, which was defined to be ±10% of the control group (±8.5%). This indicates that the addition of a low dose of esketamine did not affect the use of the propofol-remifentanil closed-loop TCI system. With this system, drug administration with low dose of esketamine could be precisely titrated without human interference. Compared with the control group, there were no manifestations indicating insufficient depth of anesthesia, postoperative recovery of consciousness and short-term recovery quality.
Low dose of esketamine has addictive sedative and analgesic effects when combined with propofol and remifentanil without increasing unsatisfied psychotic-symptoms.2,6,16,40 Study has shown that 0.3 to 0.5 mg∙kg−1 of ketamine5 administration perioperatively can reduce acute pain, decrease occurrence of anxious41 and depression.8 As esketamine has a twice potent analgesic effect compared to ketamine,1 half dose of ketamine was considered to be properly for esketamine. Based on our previous observed, more than 0.2mg∙kg−1 of esketamine would greatly increase BIS up to 70 and more, which affects our judgment of anesthesia depth. Thus, a dose of 0.2mg∙kg−1 bolus and 5μg∙kg−1∙min−1 for continuous infusion to maintain a stable plasma concentration was appropriate. In this study, compared to group C, with the addition of esketamine and new BIS baseline in group A, anesthetic drug doses decreased slightly, while anesthesia maintained stable without adverse events occurring. The reduction of drug consumption may be caused by the increasing EEG baseline and the anesthetic effect of esketamine itself. Studies shown that the use of esketamine can reduce the incidence of postoperative nausea and vomiting6,shivering42 and pain score43 after surgery, which was unable to be shown in this experiment.
Limitations
The current EEG indexes for depth of anesthesia monitoring cannot well reflect the real depth of anesthesia after combining different anesthetic drugs. The design of this trial could only refine the additional drug dosage brought by the elevation of BIS by esketamine under the closed-loop system but was unable to quantify the real anesthetic effect of esketamine in the study. A new indicator of unconsciousness that is not disturbed by esketamine administration is required in the future. Second, due to the unstable EEG changes during induction of anesthesia, it was unable to quantify the effects of esketamine on the EEG and to well apply the control system for drug infusion during this phase. Therefore, instead of a bolus at induction followed by infusion recommended in other clinical guidelines,44 we could only add esketamine and started this closed-loop infusion system during the maintenance period of anesthesia. Thirdly, the plasma concentrations of esketamine were not monitored. Thus, it was impossible to analyze the association between changes in plasma concentration and BIS values. Finally, there was no stratified study based on different genders and ages. Further studies need to be investigated of EEG changes at different ages and by gender. Meanwhile, the study was not powered to evaluate differences in secondary outcomes, including adverse events such as postoperative nausea and vomiting and shivering.
The Challenges and Future Directions of This Study are as Follows
1. Compatibility between the EEG characteristics of esketamine and the signal processing algorithm of close-loop TCI system: The EEG activity induced by esketamine is characterized by high-frequency γ-band (25–40 hz) bursts, which is significantly different from the δ/α wave pattern of propofol.45 It is necessary to develop targeted signal processing algorithms. Use wavelet transform or density spectral array (DSA) to distinguish the correlation between esketamine’s gamma bursts and the depth of anesthesia46 and avoid misjudgment of the BIS index. 2. Development of a TCI system for esketamine: Combined with the pharmacokinetics and pharmacodynamics (PK/PD) of esketamine, design an infusion algorithm to maintain the stability of the drug concentration. 3. Development of a multi-drug synergistic model: Ketamine is often used in combination with remifentanil or propofol to reduce side effects. It is necessary to construct a joint model based on the interaction between the NMDA receptor and the other two kinds of receptors to optimize the drug ratio. 4. Multi-modal signal fusion: Combine hemodynamic parameters (such as blood pressure, heart rate) with EEG characteristics to enhance the robustness of the assessment of the depth of anesthesia.
Conclusion
In our study, by appropriately adjusting the BIS feedback baseline, the additional propofol usage resulting from the increased EEG effect of esketamine has been optimized. This optimization avoids excessive drug consumption while not increasing the risk of intraoperative awareness and postoperative adverse events, which can further the application of closed-loop TCI system and offer some reference for the study of closed-loop system with more drugs and clinical conditions.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of General Hospital of Southern Theater command of PLA(NZLLKZ2023034) on 5 November 2024. The written informed consents were obtained from all patients before participation.
Acknowledgments
We thank our anesthesiology colleagues for their cooperation in facilitating this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by National Natural Science Foundation of China (NSFC) General Program[NO.82472110], Guangzhou Basic Research Program - Municipal-University-Enterprise Joint Funding Project [NO.SL2023A03J00955] and Guangdong Major Special Project for Science and Technology [NO.2021B0101410005].
Disclosure
The authors declare no competing interests.
References
1. Bonaventura J, Lam S, Carlton M, et al.. Pharmacological and behavioral divergence of ketamine enantiomers: implications for abuse liability. mol Psychiatry. 2021;26(11):6704–6722. doi:10.1038/s41380-021-01093-2
2. Wang J, Huang J, Yang S, et al.. Pharmacokinetics and safety of esketamine in Chinese patients undergoing painless gastroscopy in comparison with ketamine: a randomized, open-label clinical study. Drug Des Devel Ther. 2019;6(13):4135–4144. doi:10.2147/DDDT.S224553
3. Zanos P, Moaddel R, Morris PJ, et al.. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. 2018;70(3):621–660. doi:10.1124/pr.117.015198
4. Zhou N, Liang X, Gong J, et al.. S-ketamine used during anesthesia induction increases the perfusion index and mean arterial pressure after induction: a randomized, double-blind, placebo-controlled trial. Eur J Pharm Sci. 2022;1(179):106312. doi:10.1016/j.ejps.2022.106312
5. Schwenk ES, Viscusi ER, Buvanendran A, et al.. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456–466. doi:10.1097/AAP.0000000000000806
6. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
7. Zhu M, Xu S, Ju X, Wang S, Yu X. Effects of the different doses of esketamine on postoperative quality of recovery in patients undergoing modified radical mastectomy: a randomized, double-blind, controlled trial. Drug Des Devel Ther. 2022;16(16):4291–4299. doi:10.2147/DDDT.S392784
8. Voute M, Lambert C, Pereira B, Pickering G. Assessment of initial depressive state and pain relief with ketamine in patients with chronic refractory pain. JAMA Netw Open. 2023;6(5):e2314406. doi:10.1001/jamanetworkopen.2023.14406
9. Dumont GA, Ansermino JM. Closed-loop control of anesthesia: a primer for anesthesiologists. Anesth Analg. 2013;117(5):1130–1138. doi:10.1213/ANE.0b013e3182973687
10. Brogi E, Cyr S, Kazan R, Giunta F, Hemmerling TM. Clinical performance and safety of closed-loop systems: a systematic review and meta-analysis of randomized controlled trials. Anesth Analg. 2017;124(2):446–455. doi:10.1213/ANE.0000000000001372
11. Johansen JW, Sebel PS, Fisher D. Development and clinical application of electroencephalographic bispectrum monitoring. Anesthesiology. 2000;93(5):1336–1344. doi:10.1097/00000542-200011000-00029
12. Zorrilla-Vaca AA-O, Healy RJ, Wu CL, Grant MC. Relation between bispectral index measurements of anesthetic depth and postoperative mortality: a meta-analysis of observational studies. Can J Anaesth. 2017;64(6):597–607. doi:10.1007/s12630-017-0872-6
13. Radtke FM, Franck M, Fau - Lendner J, Lendner J, Fau - Krüger S. Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth. 2013(110):98–105. doi:10.1093/bja/aet055
14. Punjasawadwong Y, Phongchiewboon A, Fau - Bunchungmongkol N, Bunchungmongkol N. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev. 2014;2014(6):CD003843. doi:10.1002/14651858.CD003843.pub3
15. Pasin L, Nardelli P, Pintaudi M, et al.. Closed-loop delivery systems versus manually controlled administration of total IV Anesthesia: a meta-analysis of randomized clinical trials. Anesth Analg. 2017;124(2):456–464. doi:10.1213/ANE.0000000000001394
16. Zheng Y, Xu Y, Huang B, Mai Y, Zhang Y, Zhang Z. Effective dose of propofol combined with a low-dose esketamine for gastroscopy in elderly patients: a dose finding study using dixon’s up-and-down method. Front Pharmacol. 2022;20(13):956392. doi:10.3389/fphar.2022.956392
17. Maksimow A, Fau – Långsjö SM, Långsjö JW, et al.. Increase in high frequency EEG activity explains the poor performance of EEG spectral entropy monitor during S-ketamine anesthesia. Clin Neurophysiol. 2006;117(8):1660–1668. doi:10.1016/j.clinph.2006.05.011
18. Napoleone G, van Heusden K, Cooke E, et al.. The effect of low-dose intraoperative ketamine on closed-loop-controlled general anesthesia: a randomized controlled equivalence trial. Anesth Analg. 2021;133(5):1215–1224. doi:10.1213/ANE.0000000000005372
19. Hallett M, DelRosso LM, Elble R, et al.. Evaluation of movement and brain activity. Clin Neurophysiol. 2021;132(10):2608–2638. doi:10.1016/j.clinph.2021.04.023
20. Liu N, Chazot T, Hamada S, et al.. Closed-loop coadministration of propofol and remifentanil guided by bispectral index: a randomized multicenter study. Anesth Analg. 2011;112(3):546–557. doi:10.1213/ANE.0b013e318205680b
21. Alexandre Joosten JR, Bardaji A, Bardaji A, et al.. Anesthetic management using multiple closed loop systems and delayed neurocognitive recovery. Anesthesiology. 2020;132(2):253–266. doi:10.1097/ALN.0000000000003014
22. Cantraine FRL, Coussaert EJA. F R Cantraine 1 EJC. The First Object Oriented Monitor For Intravenous Anesthesia. J Clin Monit Comput. 2000;16(1):3–10. doi:10.1023/a:1009904805940
23. Besch G, Liu N, Samain E, et al.. Occurrence of and risk factors for electroencephalogram burst suppression during propofol-remifentanil anaesthesia. Br J Anaesth. 2011;107(5):749–756. doi:10.1093/bja/aer235
24. Joosten A, Jame V, Alexander B, et al.. Feasibility of fully automated hypnosis, analgesia, and fluid management using 2 independent closed-loop systems during major vascular surgery: a pilot study. Anesth Analg. 2019;128(6):e88–e92. doi:10.1093/bja/aer235
25. Quigley C. Hydromorphone for acute and chronic pain. Cochrane Database Syst Rev. 2002;1:CD003447. doi:10.1002/14651858.CD003447
26. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
27. Apfel CC, Fau - Koivuranta LE, Koivuranta M, Greim C-A, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
28. John ER, Prichep LS. The anesthetic cascade: a theory of how anesthesia suppresses consciousness. Anesthesiology. 2005;102(2):447–471. doi:10.1097/00000542-200502000-00030
29. Stark PA, Myles Ps Fau - Burke JA, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
30. Puri GD, Mathew Pj Fau - Biswas I, Biswas I, et al. A multicenter evaluation of a closed-loop anesthesia delivery system: a randomized controlled trial. Anesth Analg. 2016;122(1):106–114. doi:10.1213/ANE.0000000000000769
31. Jones B, Jarvis P, Lewis JA, Ebbutt AF. Trials to assess equivalence: the importance of rigorous methods. BMJ. 1996;313(7048):36–39. doi:10.1136/bmj.313.7048.36
32. van Heusden K, Cooke E, Brodie S, et al.. Effect of ketamine on the NeuroSENSE WAV(CNS) during propofol anesthesia; a randomized feasibility trial. J Clin Monit Comput. 2021;35(3):557–567. doi:10.1007/s10877-020-00511-0
33. Akeju O, Song AH, Hamilos AE, et al.. Electroencephalogram signatures of ketamine anesthesia-induced unconsciousness. Clin Neurophysiol. 2016;127(6):2414–2422. doi:10.1016/j.clinph.2016.03.005
34. Chamadia S, Gitlin J, Mekonnen J, et al.. Ketamine induces EEG oscillations that may aid anesthetic state but not dissociation monitoring. Br J Anaesth. 2015;132(12):3010–3018. doi:10.1016/j.clinph.2021.08.021
35. Hayashi K, Tsuda N, Sawa T, Hagihira S. Ketamine increases the frequency of electroencephalographic bicoherence peak on the alpha spindle area induced with propofol. Br J Anaesth. 2007;99(3):389–395. doi:10.1093/bja/aem175
36. Faraoni D, Salengros JC, Engelman E, Ickx B, Barvais L. Ketamine has no effect on bispectral index during stable propofol-remifentanil anaesthesia. Br J Anaesth. 2009;102(3):336–339. doi:10.1093/bja/aen403
37. Carrara L, Nault M, Morisson L, et al.. The impact of bolus versus continuous infusion of intravenous ketamine on bispectral index variations and desflurane administration during major surgery. Eur J Anaesthesiol. 2021;38(11):1168–1179. doi:10.1097/EJA.0000000000001588
38. Schnetz MP, Reon BJ, Ibinson JW, et al.. Bispectral index changes following boluses of commonly used intravenous medications during volatile anesthesia identified from retrospective data. Anesthesia Analg. 2023;138(3):635–644. doi:10.1213/ANE.0000000000006633
39. Liyuan Ren JY, Yanshuang L, Wang Y. Effect of continuous infusion of different doses of esketamine on the bispectral index during sevoflurane anesthesia: a randomized controlled trial. Drug Des Devel Ther. 2024;2(18):1727–1741. doi:10.2147/DDDT.S457625
40. Okuyama K, Inomata S, Okubo N, Watanabe I. Pretreatment with small-dose ketamine reduces predicted effect-site concentration of propofol required for loss of consciousness and laryngeal mask airway insertion in women. J Clin Anesth. 2011;23(2):113–118. doi:10.1001/jamanetworkopen.2022.44514
41. Qiu D, Wang X-M, Yang -J-J, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy. JAMA Netw Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
42. Dal D, Kose A, Fau - Honca M, et al.. Efficacy of prophylactic ketamine in preventing postoperative shivering. Br J Anaesth. 2005;95(2):189–192. doi:10.1093/bja/aei148
43. Vincent Joly MD, Philippe Richebe MD, Bruno Guignard MD, et al. Remifentanil-induced postoperative hyperalgesia and its prevention with small-dose ketamine. Anesthesiology. 2005;103(1):147–155. doi:10.1097/00000542-200507000-00022
44. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American pain society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ committee on regional anesthesia, executive committee, and administrative council. J Pain. 2016;17(2):131–157. doi:10.1016/j.jpain.2015.12.008
45. Purdon PL, Sampson A, Pavone KJ, Brown EN. Clinical electroencephalography for anesthesiologists: part i: background and basic signatures. Anesthesiology. 2015;12(4):937–960. doi:10.1113/JP279705
46. Deane KA-O, Brunk MA-O, Curran AW, et al.. Ketamine anaesthesia induces gain enhancement via recurrent excitation in granular input layers of the auditory cortex. J Physiol. 2020;598(13):2741–2755. doi:10.1113/JP279705
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.