")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
Fecal Microbiota Transplantation in Children with Autism
Authors Li Y, Xiao P, Ding H, Wang H, Xu Q, Wang R, Zheng L, Song X, Wang Y , Zhang T
Received 30 August 2024
Accepted for publication 1 December 2024
Published 9 December 2024 Volume 2024:20 Pages 2391—2400
DOI https://doi.org/10.2147/NDT.S488001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Youran Li,1 Pei Xiao,1 Hongfang Ding,2 Hui Wang,2 Qiao Xu,1 Ruixue Wang,1 Lu Zheng,1 Xue Song,1 Yizhong Wang,1 Ting Zhang1,3
1Department of Gastroenterology, Hepatology and Nutrition, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Pediatrics, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China; 3Institute of Pediatric Infection, Immunity and Critical Care Medicine, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Correspondence: Ting Zhang; Yizhong Wang, Department of Gastroenterology, Hepatology and Nutrition, Shanghai Children’s Hospital, School of medicine, Shanghai Jiao Tong University, Shanghai, 200062, People’s Republic of China, Email [email protected]; [email protected]
Purpose: This research aimed to explore the clinical efficacy of fecal microbiota transplantation (FMT) in treating children with autism spectrum disorder (ASD).
Methods: In this single-arm prospective study, every participant received FMT therapy, followed by an 8-week follow-up. Children unable to swallow lyophilized capsules (Caps) received fecal solution through transendoscopic enteral tube (TET) or nasal jejunal tube (NJT) approaches. All participants underwent assessments of ASD core symptoms, gastrointestinal (GI) symptoms and sleep status initially, after treatment and during follow-up. The study outcomes included the changes in scores of the Autism Behavior Checklist (ABC), Childhood Autism Rating Scale (CARS), Social Responsiveness Scale (SRS), Gastrointestinal Symptoms Rating Scale (GSRS) and Sleep Disturbance Scale for Children (SDSC), as well as the adverse events (AEs).
Results: 98 participants were involved, consisting of 80 males and 18 females, with a median age of 7 years. 73 children received the FMT in the form of Caps, while 13 patients underwent the procedure through TET and 12 patients via NJT. Improvements were observed in all outcome measures for Caps and NJT groups at both the post-treatment and 8-week follow-up evaluations. Adjusted between-group analyses at post-treatment and follow-up showed that Caps and NJT group had greater reduction in ABC, CARS and SRS scores compared with TET group, while NJT group had greater reduction in SDSC scores compared with Caps and TET group. The incidence of AEs was 8.2% in the Caps group, 23.1% in the TET group, and 8.3% in the NJT group, with no serious AEs reported.
Conclusion: FMT treatment can improve the core symptoms, GI symptoms and sleep disturbances in children with ASD. The upper GI tract routes, including Caps and NJT, may be more effective and safe compared to the lower GI tract route of TET.
Keywords: Fecal microbiota transplantation, efficacy, autism spectrum disorder
Introduction
Autism spectrum disorder (ASD) is a condition related to neurodevelopment that impacts roughly 1% of children globally.1 The manifestations of ASD include challenges with social communication, repetitive actions, intensely focused interests, and it is typically diagnosed before the age of three.2 The challenges associated with ASD often continue into adulthood, resulting in difficulties with social integration, limited job opportunities, a higher prevalence of mental health problems, and low participation rates in the workforce among parents or caregivers.3 The burden of ASD worldwide is on the rise, posing a significant mental health challenge.4
Therapy of ASD aims to enhance an individual’s functioning and quality of life.5 There is strong evidence to support that using behavioral interventions in early childhood and throughout the lifespan can effectively enhance social communication interactions and reduce problem behaviors.6 Nonetheless, behavioral interventions typically take a long time, and some parents hold opposing views on the use of any punishment-based procedures.7 At present, there is no medication proven to be effective for the core symptoms of ASD.8 Medication interventions are used to alleviate concurrent behavioral and emotional regulation challenges in patients with ASD, such as aripiprazole and risperidone. However, these medications can cause side effects, with the most common being changes in appetite, weight, and sleep.9 Therefore, the current treatment of ASD requires further exploration of alternative or adjunct therapies.
Recent studies have suggested that the microbiota-gut-brain axis plays a crucial role in ASD and is being viewed as a potential target for therapeutic interventions.10 Research on the therapeutic effects of fecal microbiota transplantation (FMT) in individuals with ASD is limited, with insufficient evidence to demonstrate the effectiveness of FMT interventions and therapy options for children with ASD. Therefore, we analyzed clinical research data by applying a larger sample size and compared the differences in efficacy among various FMT treatment approaches on core symptoms (primary aim) as well as gastrointestinal (GI) symptoms and sleep disturbance (secondary aims) in ASD children. Exploratory objectives included analyzing the number of adverse events.
Methods
Study Design and Participants
Children with ASD who received treatment at the Gastroenterology, Hepatology, and Nutrition department of Shanghai Children’s Hospital from January 2022 to January 2024 were included if they met specific criteria: they needed to be under 18 years of age; they must fulfill the diagnostic requirements for ASD as outlined in the DSM-5 and other commonly used diagnostic tools; their legal guardian had to fully comprehend and sign the informed consent form, permitting the collection of clinical data by the researchers; and they should be capable of ongoing participation in the study and attending follow-up appointments. Patients were excluded from the study if they had any of the following: a confirmed diagnosis of Reye’s syndrome or other psychiatric disorders; a documented history of brain injury, cerebral palsy, encephalitis, or other organic brain conditions; use of probiotics, antibiotics, proton pump inhibitors, or any other medications that influence gut microbiota within the last three months; the presence of serious gastrointestinal diseases or organic intestinal issues, such as congenital megacolon, intestinal obstruction, or intussusception; or if they demonstrated poor adherence to study protocols.
Throughout the study, each child underwent FMT, followed by an observation phase lasting 8 weeks after the treatment concluded. All patients underwent assessments of core symptoms, GI symptoms, and sleep status at baseline (prior to FMT treatment), after treatment concluded and during the monitoring period. Any adverse events occurring after the initial transplantation were documented. The study was reviewed and approved by the Ethics Review Committee of Shanghai Children’s Hospital, School of medicine, Shanghai Jiao Tong University. The guardians of the participants provided written consent before the children were admitted to the study.
Recruitment and Screening of Donors
The study recruited three eligible donors after the screening process. The criteria for eligibility as stool donors included: being between the ages of 15 and 30; being generally healthy; having a body mass index (BMI) ranging from 18.5 to 23.9 kg/m²; and having consistent fecal excretions once or twice a day, particularly classified as type 4 on the Bristol stool scale. Exclusion criteria encompassed: a prior diagnosis of GI or chronic systemic diseases, cancer, or having undergone radiotherapy or chemotherapy; any ongoing medical conditions; use of antibiotics, probiotics, prebiotics, proton pump inhibitors, immunosuppressants, or blood products in the last 3 months; positive serum tests for hepatitis A, B, or C, HIV, syphilis, Epstein-Barr virus, or cytomegalovirus; positive stool tests for pathogens; and the presence of multidrug-resistant genes, such as extended-spectrum beta-lactamases and carbapenemases.11
Preparation of FMT Solution
Fresh stool samples from donors were obtained using a single-use container. The 100g of stool samples were diluted with 500mL of saline solution to achieve a homogeneous mixture. This process was completed within 6 hours using an automated microfiltration device (GenFMTer, Jiangsu Province, China). The fecal suspension was subsequently processed through the equipment according to the established schedule.12 After completing the microfiltration process, the suspension was transferred into 50 mL tubes and centrifuged at 1500g for 3 minutes. The resulting supernatant was discarded, and the sediment was reconstituted in normal saline to create the FMT solution. This fecal solution was then placed into a sterile bottle for administration to the patient within two hours, or it could be frozen at −80°C for further usage.
Preparation of Lyophilized FMT Capsules
The fecal solution was combined with lyophilized protective agent, and the mixture was then processed into a powder using a low-temperature freeze dryer. The final freeze-dried powder was placed into size 00 hypromellose capsules (Anhui Huangshan Capsule, Anhui Province, China) using a double-encapsulation process. The lyophilized capsules were stored at −80°C, and then kept at a temperature of −20°C for about two hours prior to being orally administered to the patient.
FMT Procedure
According to our findings on FMT therapy for pediatric conditions, the dosage for each FMT course was determined by the weight of the donor stool sample and the body weight of the children with ASD. The ratio used was 1 gram of donor stool per 1 kilogram of the recipient’s body weight. Furthermore, by analyzing the changes observed in patients both prior to and following FMT procedure, we determined that the duration of the microbial colonization is approximately 4 weeks.13–15 Consequently, we opted to conduct three treatment courses to promote the establishment of the gut microbiota.
For the capsule group, the participants took a course of capsules before meals for 3 consecutive days. This course of capsules was repeated every 4 weeks, resulting in a total of 3 courses over a 12-week period. Meanwhile, patients who could not tolerate the capsule approach received fecal solution through the transendoscopic enteral tube or nasal jejunal tube. As the placement of the tube required general anesthesia and gastroenteroscopy, in order to reduce the risk and intolerance of multiple anesthesia procedures for the patients, the tube was left in place for 3 days. During this period, the patients received one course of fecal solution infusion over 5 minutes daily, resulting in a total of 3 courses over a 4-week period.
Evaluations and Data Collection
To assess symptoms associated with ASD, the following scales were employed: the Childhood Autism Rating Scale (CARS), the Autism Behavior Checklist (ABC) and the Social Responsiveness Scale (SRS). To assess the GI symptoms of each participant, parents were requested to fill out the Gastrointestinal Symptoms Rating Scale (GSRS), while the Sleep Disturbance Scale for Children (SDSC) was employed to evaluate sleep-related issues. The CARS, ABC, SRS, GSRS, and SDSC were administered to participants at three distinct time points: at baseline, after treatment, and at the conclusion of the follow-up period.
Statistical Analysis
Statistical analysis was conducted using descriptive methods and SPSS 29.0 software. Continuous variables were reported as medians along with interquartile ranges (IQR). Normality tests were carried out to determine the appropriate statistical tests to use. Additionally, the Kruskal–Wallis H-test was applied for comparing measurement data, while categorical data comparisons were performed using the chi-square test. A p-value of less than 0.05 was considered statistically significant.
Results
Patient Characteristics
98 participants were involved in the study, consisting of 18 females and 80 males. Among these children, 35 were diagnosed with severe autism, and 79 presented with comorbid GI symptoms including abdominal pain, reflux, indigestion, diarrhea and constipation. According to the acceptability of FMT, 73 patients (74.5%) received the FMT in the form of oral capsules, while 13 patients (13.3%) underwent the procedure through a transendoscopic enteral tube, and 12 patients (12.2%) received the transplant via a nasal jejunal tube (Table 1). The median age of the 73 children with ASD in the capsule group was 7 years, while the median ages were 4 years for the transendoscopic enteral tube group and 4.5 years for the nasal jejunal tube group, respectively. In addition, the condition of unbalanced diet behaviors, food allergies and fecal calprotectin levels were also assessed.
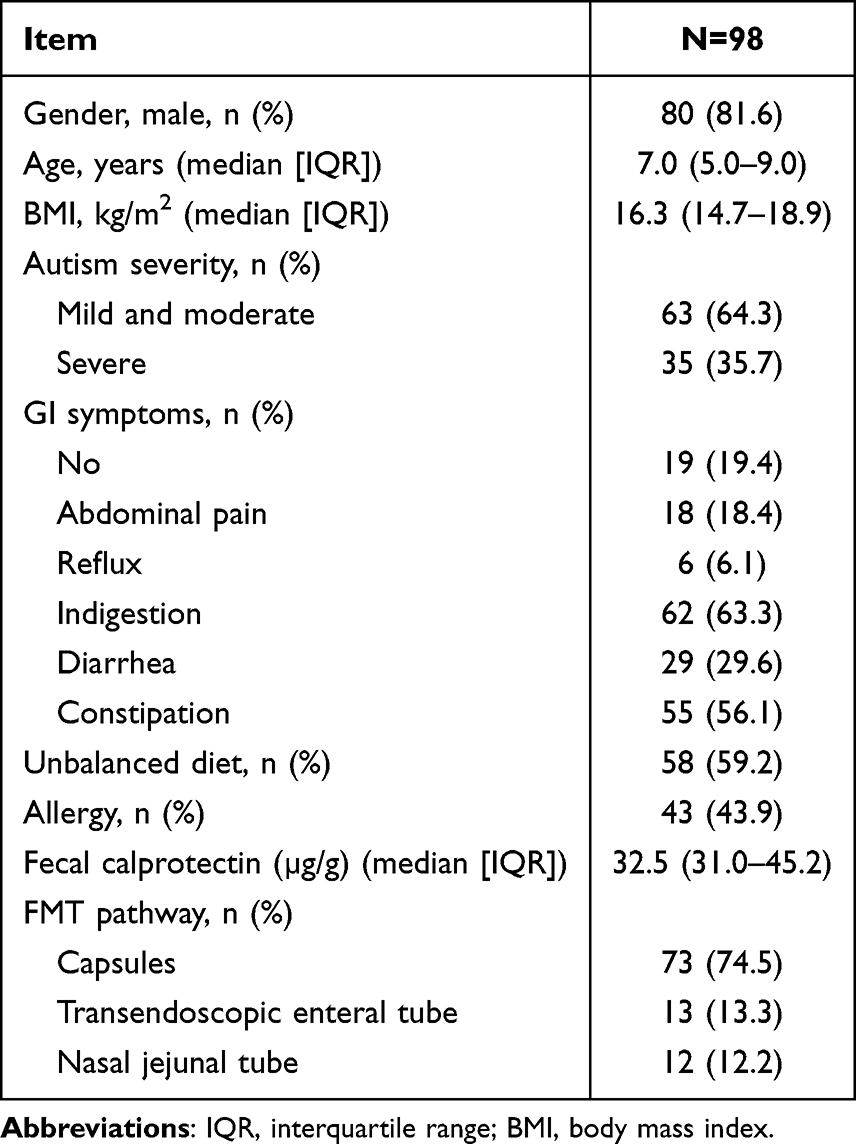 |
Table 1 Characteristics of Children with ASD |
Primary Outcome Measures
Improvements were observed in all primary outcome measures for capsule (Caps) and nasal jejunal tube (NJT) groups at both the post-treatment and 8-week follow-up evaluations (Figure 1). For the Caps group, the scores on the ABC, CARS, and SRS had the following changes: the median (IQR) decreased from 68.0 (57.5–90.5), 33.0 (31.0–39.5), and 161.0 (146.0–170.0) at baseline to 57.0 (46.0–76.0), 30.0 (27.0–36.0), and 149.0 (132.0–160.0) at follow-up, respectively (Table 2). Similarly, for the NJT group, the scores on the three scales had the following changes: the median (IQR) decreased from 76.0 (58.0–87.3), 34.0 (31.0–39.6), and 165.0 (158.5–175.3) at baseline to 56.0 (45.0–84.0), 30.0 (30.0–35.0), and 155.0 (138.0–169.0) at follow-up, respectively. For the transendoscopic enteral tube (TET) group, the scores on the ABC and CARS did not show a significant decline after the FMT treatment. By the follow-up period, the median (IQR) ABC score had decreased from 68.0 (61.0–77.5) at baseline to 65.0 (50.3–81.8). The median (IQR) SRS score had decreased from 162.0 (144.0–172.5) at baseline to 150.0 (140.0–169.0) after the FMT treatment, but then rebounded during the follow-up period. Adjusted between-group analyses at post-treatment and follow-up showed that Caps and NJT group had greater reduction in ABC, CARS and SRS scores compared with TET group.
 |
Table 2 Analyses of Primary Outcome Measures |
 |
Figure 1 The changes in ASD core symptoms after FMT. ASD core symptoms were assessed through ABC, CARS and SRS scales at three different time points: baseline, post-FMT and follow-up period. (A) Capsules group. (B) Transendoscopic enteral tube group. (C) Nasal jejunal tube group. The Wilcoxon test was used to determine the significance. ns, no significance, *P < 0.05, **P < 0.01, ****P < 0.0001. |
Secondary Outcome Measures
All treatment groups demonstrated some degree of improvement across all secondary outcome measures, both at the post-treatment evaluation as well as the 8-week follow-up assessment (Table 3). For the changes in GSRS scores across the three groups, the median (IQR) decreased from a baseline range of 20.0 (15.0–33.5) to 22.0 (18.0–32.5), down to 19.0 (15.0–22.0) to 19.5 (15.0–23.8) during the follow-up period. The Caps and NJT groups both showed decreases in their median (IQR) SDSC scores from baseline 45.0 (39.0–52.0) and 47.0 (32.0–57.8), to follow-up 40.0 (35.0–47.0) and 40.0 (32.0–51.3), respectively. Adjusted between-group analyses at post-treatment and follow-up showed that NJT group had greater reduction in SDSC scores compared with Caps and TET group.
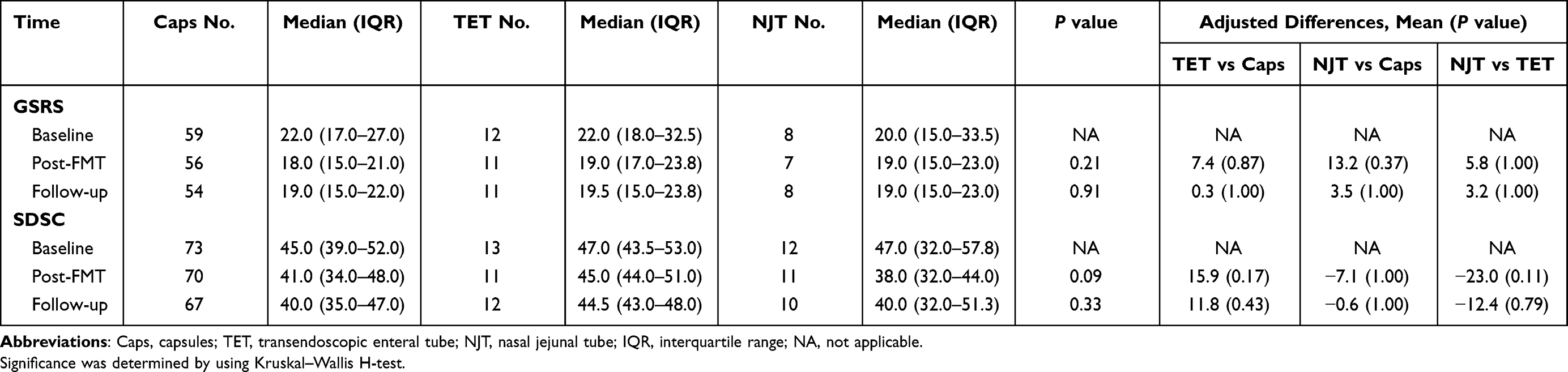 |
Table 3 Analyses of Secondary Outcome Measures |
Adverse Events of FMT
Adverse events (AEs) associated with FMT were categorized into short-term (within 48 hours post-FMT) and long-term (up to 3 months).16 Meanwhile, various AEs were monitored for the different FMT administration routes, including capsules, transendoscopic enteral tube and nasal jejunal tube (Table 4). All short-term AEs were mild, with patients becoming symptom-free within 48 hours, and during the follow-up period, a total of 10 (10.2%) minor AEs occurred that did not require any intervention or medication. The main AEs included 5 cases of vomiting, with 3 (4.1%) occurring in the Caps group, and the other 2 cases in the TET group (7.7%) and NJT group (8.3%), respectively. Additionally, there were 2 cases of abdominal pain, one each in the Caps group and the TET group. The Caps group also had 2 cases of nausea and fever, while the TET group had 1 case of headache. The treatment and follow-up period did not yield any reports of serious AEs.
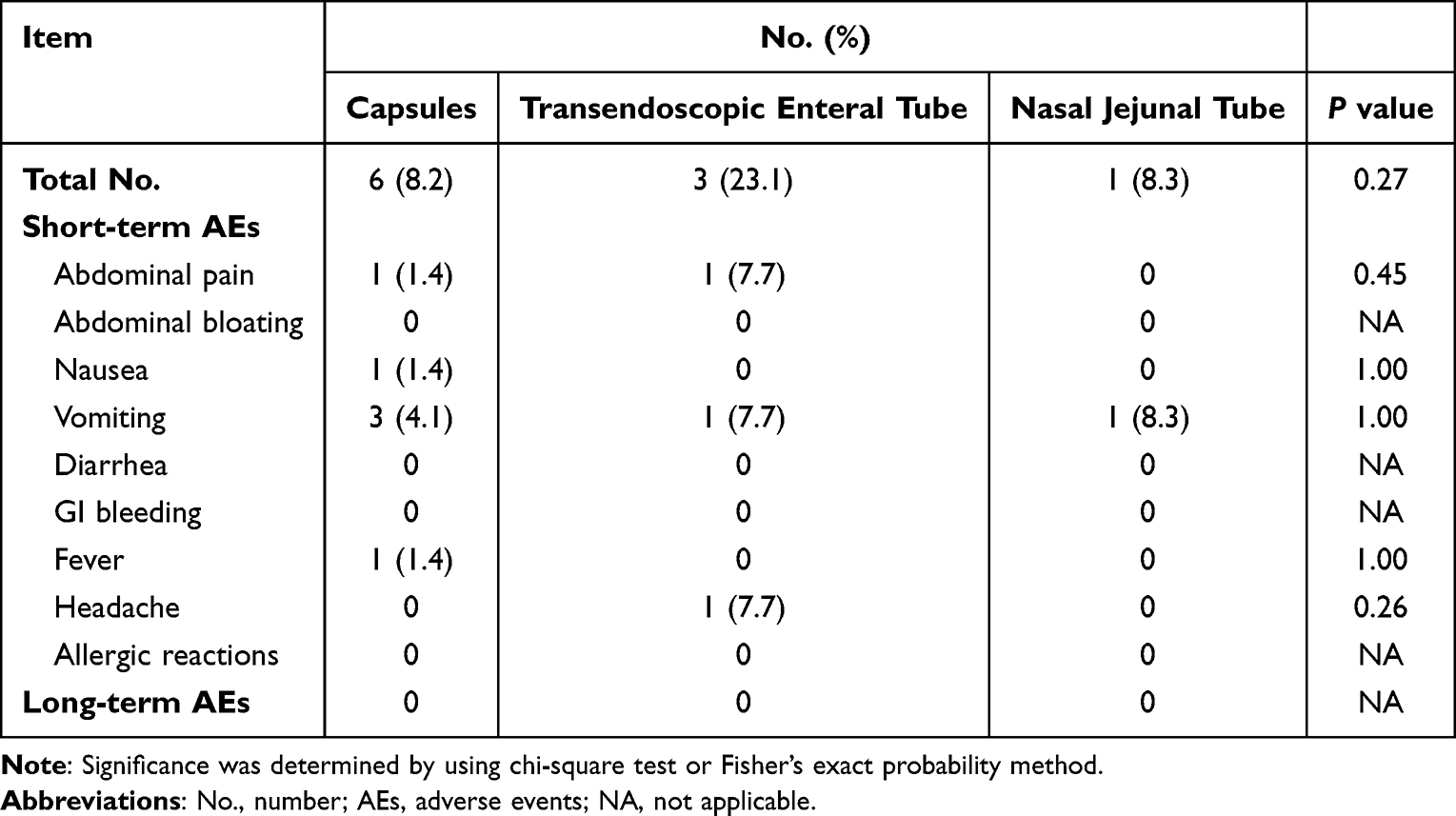 |
Table 4 Adverse Events of FMT |
Discussion
In this research, 98 children diagnosed with ASD were involved. Earlier studies indicated that FMT could alleviate core symptoms of ASD in small sample sizes and limited treatment methods,17–20 and the impact of different FMT administration routes on the efficacy has not been confirmed. This study followed up 98 ASD children to explore the therapeutic efficacy of different FMT administration routes on ASD. The study endpoints included the changes in ASD core symptoms (ABC, CARS and SRS scores), GI symptoms (GSRS scores), sleep disorders (SDSC scores), as well as the adverse events of FMT.
Research regarding the medicinal efficacy of FMT for individuals with ASD is still quite limited. In a prior open-label trial, 18 children with ASD who experienced moderate to severe GI issues underwent a two-week course of antibiotics and bowel preparation, followed by FMT. Participants were randomly assigned to receive FMT either rectally or orally, beginning with a higher initial dose, which was then maintained at a lower level for 8 weeks. They also took Prilosec during the treatment period. Follow-up evaluations conducted 8 weeks post-treatment revealed that 89% of the participants experienced improvements in GI symptoms as measured by GSRS scores, while CARS scores decreased by 24% throughout the treatment duration.17 Another study involved 40 children with ASD who exhibited GI symptoms, alongside 16 typically developing peers. The ASD participants underwent four weeks of FMT treatment, followed by an eight-week observation period. Among the ASD group, 27 received the FMT through oral freeze-dried capsules, while 13 were treated via colonoscopy. Prior to the FMT, all participants underwent bowel preparation. The findings indicated that both oral and colonoscopic methods effectively alleviated GI symptoms and improved core ASD symptoms, with no significant differences observed between the two administration methods.18 Additionally, another study showed that 49 ASD children who underwent at least two rounds of washed microbiota transplantation via the transendoscopic enteral tube method experienced effective improvement in their autism symptoms, sleep disturbances, stool consistency, and constipation.19,21 We have also conducted a pilot study on the usage of lyophilized capsules for the FMT therapy of 38 ASD children.20
Currently, FMT can be delivered through various administration routes, including oral fecal capsules, nasointestinal infusion, or endoscopic procedures.22 In this research, we compared three different routes for administering FMT on ASD: oral capsules, nasal jejunal tube and transendoscopic enteral tube. The findings indicated that the TET method appeared to offer the least benefits. The group using capsules had a notably higher number of participants compared to those in the TET and NJT groups. This disparity is likely due to the capsule method being more straightforward, convenient, and leading to better adherence from patients. However, there were no significant differences in the AEs reported among the three different administration methods.
The majority of adverse reactions to FMT treatment are GI symptoms, which typically resolve within 2–3 days.23 During the course of this study, a total of 10 (10.2%) AEs occurred, the most common being vomiting and abdominal pain. Compared to the capsule and NJT methods, the TET approach had the highest proportion of side effects. All adverse reactions were self-resolving, and no severe AEs observed during the monitoring period. In 2019, the FDA issued a warning about two donors who were inadequately screened, leading to serious infections after FMT, which unfortunately resulted in the death of one patient.24 However, our team has administered FMT for various pediatric conditions since 2013 without any incidents of serious adverse reactions.
The limitations of this study include its open-label design, the absence of a placebo group, and potential biases in recruitment, which should be taken into account when interpreting the findings. Due to medical ethics, we were unable to use a placebo group for the ASD children. The number of children receiving oral lyophilized powder capsule treatment was significantly higher than the other two administration routes, which may introduce potential bias in the data. Some patients who underwent TET had used polyethylene glycol bowel preparation prior to the treatment, which inevitably led to mild GI discomfort, but it was relieved within 24 hours.
Conclusion
This prospective single-arm study assessed the impact of FMT on treating ASD using a larger participant sample and compared the effectiveness of different FMT approaches. The findings indicated that FMT is both an effective and safe treatment option for children with ASD. Specifically, the upper gastrointestinal tract routes, including capsules and nasal jejunal tubes, may be more effective and safe compared to the lower gastrointestinal tract route of transendoscopic enteral tube.
Data Sharing Statement
The datasets produced or analyzed during the study can be requested from the corresponding author upon a reasonable inquiry.
Ethics Approval and Informed Consent
All procedures carried out in this research were compliant with the ethical standards approved by the Ethics Review Committee at the Shanghai Children’s Hospital, Shanghai Jiao Tong University (Approval number: 2021R117-F02). The FMT study has been registered with the Chinese Clinical Trial Registry (Registration Number: ChiCTR2200055943). Written informed consent was obtained from all guardians of the participants, in line with the principles outlined in the Helsinki Declaration.
Acknowledgments
The authors express their gratitude to all the children with ASD and their families for their collaboration during the data collection process.
Funding
This study was funded by the Medical innovation Research project of Shanghai Science and Technology Commission (Project No.: 22Y11903700).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: a systematic review update. Autism Res. 2022;15(5):778–790.
2. Lord C, Brugha TS, Charman T, et al. Autism spectrum disorder. Nat Rev Dis Primers. 2020;6(1):5.
3. Li Z, Yang L, Chen H, et al. Global, regional and national burden of autism spectrum disorder from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol Psychiatr Sci. 2022;31:e33.
4. Solmi M, Song M, DK Y, et al. Incidence, prevalence, and global burden of autism spectrum disorder from 1990 to 2019 across 204 countries. Mol Psychiatry 2022, 27(10):4172–4180.
5. Hirota T, King BH. Autism Spectrum Disorder: a Review. JAMA. 2023;329(2):157–168.
6. Lai MC, Anagnostou E, Wiznitzer M, Allison C, Baron-Cohen S. Evidence-based support for autistic people across the lifespan: maximising potential, minimising barriers, and optimising the person-environment fit. Lancet Neurol. 2020;19(5):434–451.
7. Leaf JB, Cihon JH, Leaf R, et al. Concerns About ABA-Based Intervention: an Evaluation and Recommendations. J Autism Dev Disord. 2022;52(6):2838–2853.
8. Siafis S, Çıray O, Wu H, et al. Pharmacological and dietary-supplement treatments for autism spectrum disorder: a systematic review and network meta-analysis. Mol Autism. 2022;13(1):10.
9. Rodrigues R, Lai MC, Beswick A, et al. Practitioner Review: pharmacological treatment of attention-deficit/hyperactivity disorder symptoms in children and youth with autism spectrum disorder: a systematic review and meta-analysis. J Child Psychol Psychiatr. 2021;62(6):680–700.
10. Li Y, Wang Y, Zhang T. Fecal Microbiota Transplantation in Autism Spectrum Disorder. Neuropsychiatr Dis Treat. 2022;18:2905–2915.
11. Cammarota G, Ianiro G, Kelly CR, et al. International consensus conference on stool banking for faecal microbiota transplantation in clinical practice. Gut. 2019;68(12):2111–2121.
12. Zhang T, Lu G, Zhao Z, et al. Washed microbiota transplantation vs. manual fecal microbiota transplantation: clinical findings, animal studies and in vitro screening. Protein Cell. 2020;11(4):251–266.
13. Wang YZ, Xiao FF, Xiao YM, et al. Fecal microbiota transplantation relieves abdominal bloating in children with functional gastrointestinal disorders via modulating the gut microbiome and metabolome. J Dig Dis. 2022;23(8–9):482–492.
14. Li X, Gao X, Hu H, et al. Clinical Efficacy and Microbiome Changes Following Fecal Microbiota Transplantation in Children With Recurrent Clostridium Difficile Infection Front Microbiol 2018 Vol. 92622
15. [Chinese experts consensus on standardized methodology and clinical application of fecal microbiota transplantation]. Zhonghua Wei Chang Wai Ke Za Zhi. 2020;23(Z1):5–13. Hawaiian
16. Zhang XY, Wang YZ, Li XL, et al. Safety of fecal microbiota transplantation in Chinese children: a single-center retrospective study. World J Clin Cases. 2018;6(16):1121–1127.
17. Kang DW, Adams JB, Gregory AC, et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome. 2017;5(1):10.
18. Li N, Chen H, Cheng Y, et al. Fecal Microbiota Transplantation Relieves Gastrointestinal and Autism Symptoms by Improving the Gut Microbiota in an Open-Label Study. Front Cell Infect Microbiol. 2021;11:759435.
19. Pan ZY, Zhong HJ, Huang DN, Wu LH, He XX. Beneficial Effects of Repeated Washed Microbiota Transplantation in Children With Autism. Front Pediatr. 2022;10:928785.
20. Li Y, Xiao P, Cao R, et al. Effects and microbiota changes following oral lyophilized fecal microbiota transplantation in children with autism spectrum disorder. Front Pediatr. 2024;12:1369823.
21. Zhang Y, Zhang J, Pan Z, He X. Effects of Washed Fecal Bacteria Transplantation in Sleep Quality, Stool Features and Autism Symptomatology: a Chinese Preliminary Observational Study. Neuropsychiatr Dis Treat. 2022;18:1165–1173.
22. Gulati M, Singh SK, Corrie L, Kaur IP, Chandwani L. Delivery routes for faecal microbiota transplants: available, anticipated and aspired. Pharmacol Res. 2020;159:104954.
23. Dailey FE, Turse EP, Daglilar E, Tahan V. The dirty aspects of fecal microbiota transplantation: a review of its adverse effects and complications. Curr Opin Pharmacol. 2019;49:29–33.
24. DeFilipp Z, Bloom PP, Torres Soto M, et al. Drug-Resistant E. coli Bacteremia Transmitted by Fecal Microbiota Transplant. New Engl J Med. 2019;381(21):2043–2050.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fecal Microbiota Transplantation in Autism Spectrum Disorder
Li Y, Wang Y, Zhang T
Neuropsychiatric Disease and Treatment 2022, 18:2905-2915
Published Date: 15 December 2022