")
Back to Journals » Vascular Health and Risk Management » Volume 21
Functional Compression of the Right Internal Carotid Artery by the Hyoid Bone in a Patient with Moyamoya Syndrome and Low Internal Carotid Artery Bifurcation: A Case Report
Authors Bicevska K, Skrastina S , Kupcs K, Raita A, Balodis A
Received 7 February 2025
Accepted for publication 2 May 2025
Published 16 May 2025 Volume 2025:21 Pages 383—389
DOI https://doi.org/10.2147/VHRM.S520022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Akash Batta
Klinta Bicevska,1,2 Sigita Skrastina,3 Karlis Kupcs,1,2 Anita Raita,4 Arturs Balodis1,2
1Institute of Diagnostic Radiology, Pauls Stradins Clinical University Hospital, Riga, Latvia; 2Department of Radiology, Riga Stradins University, Riga, Latvia; 3Riga Stradins University, Riga, Latvia; 4Clinic of Neurology, Pauls Stradins Clinical University Hospital, Riga, Latvia
Correspondence: Arturs Balodis, Pauls Stradins Clinical University Hospital, Pilsonu St. 13, Riga, LV-1002, Latvia, Email [email protected]
Background: Functional compression of the internal carotid artery by hyoid bone is a rare but potentially serious condition that can lead to vascular complications, particularly when coexisting with intracranial vascular abnormalities. This case report describes a 48-year-old woman with acute cerebral ischemia due to a combination of functional right internal carotid artery compression by the hyoid bone, low carotid bifurcation, and coexisting Moyamoya syndrome.
Case Report: In this article, we describe the clinical case of a 48-year-old woman who presented with sudden-onset weakness in her left arm. Imaging studies demonstrated acute ischemia in the territory supplied by the right middle cerebral artery. Further evaluation with computed tomography angiography revealed compression of the right internal carotid artery by the hyoid bone. However, additional imaging studies, including digital subtraction angiography and carotid Doppler ultrasound, did not reveal any signs of internal carotid artery stenosis. This suggested that the compression was functional, occurring only in specific positions of the head or arms. The patient was also newly diagnosed with Moyamoya syndrome, characterized by progressive stenosis of the intracranial vessels. Prompt recognition of these findings enabled timely management, including the initiation of antiplatelet therapy.
Conclusion: In cases of acute brain ischemia, it is crucial to consider both intracranial and extracranial vascular conditions. This case report underscores the significance of identifying anatomical variations in the relationship between the hyoid bone and the internal carotid artery, as it can lead to arterial compression and potentially trigger acute ischemic strokes, especially in combination with Moyamoya syndrome. Understanding these anatomical nuances is essential for early diagnosis and appropriate management.
Keywords: hyoid bone (D006928), carotid artery, internal (D002343), infarction, middle cerebral artery (D020244), moyamoya disease (D009072), cerebral angiography (D002533)
Background
The internal carotid artery (ICA) supplies blood to the front part of the brain and usually branches from the common carotid artery (CCA) near the C3–C4 vertebral level.1 The hyoid bone, located in the mid-neck, is a small, U-shaped structure suspended by muscles and ligaments.2,3 Although it typically is not involved in vascular issues, certain anatomical variations2 — such as a low carotid bifurcation, a medially positioned ICA,4,5 or an elongated hyoid bone — can bring the artery close enough to the bone to cause compression.6–9
This compression can be either mechanical (constant) or functional (dependent on head or neck position). While rare, it has been linked to arterial wall changes, plaque formation, and in some cases, stroke6–9 Depending on the severity, treatment options range from observation to hyoid bone resection or endarterectomy.6
To our knowledge, the combination of ICA compression by the hyoid bone and Moyamoya syndrome has not been reported before. Moyamoya is a condition involving progressive narrowing of intracranial arteries, often with the formation of collateral vessels. Even though these two findings may be unrelated, their coexistence in this case underlines the need to consider both intracranial and extracranial vascular factors, and shows the value of using multiple imaging methods, especially in complex or unusual stroke presentations. This report describes a case of a 48-year-old woman with the ICA compression by hyoid bone which, combined with Moyamoya syndrome, caused acute cerebral ischemia.
Presentation of the Case
A 48-year-old woman presented to the emergency department for sudden-onset weakness in her left arm that appeared the previous evening. A neurological examination showed deep paresis in the left palm and mild central facial paresis, along with the left upper arm and forearm. Her medical history was unremarkable, except for hypertension, which was well controlled with medication. Upon presentation, a non-contrast head computed tomography (CT) scan was performed, revealing acute ischemia in the right postcentral gyrus, without significant mass effect or hemorrhage.
Computed tomography angiography (CTA) demonstrated pronounced multisegmental stenoses of the intracranial vessels, ranging from 40% narrowing to complete occlusions, including complete occlusion of the right middle cerebral artery (MCA) and right posterior cerebral artery (PCA), with distinct collateral branches. The examination also revealed extracranial sub-occlusion of the right ICA, caused by calcification of the greater horn of the hyoid bone. The bifurcation of the right common carotid artery was located significantly lower than typical, approximately at the level of the C5–C6 vertebrae, while the left-side bifurcation was at the C3–C4 level. The right ICA was located medially, with the greater horn of the hyoid bone positioned between the ICA and the external carotid artery (ECA), compressing the ICA laterally against the transverse processes of the cervical spine (Figures 1 and 2).
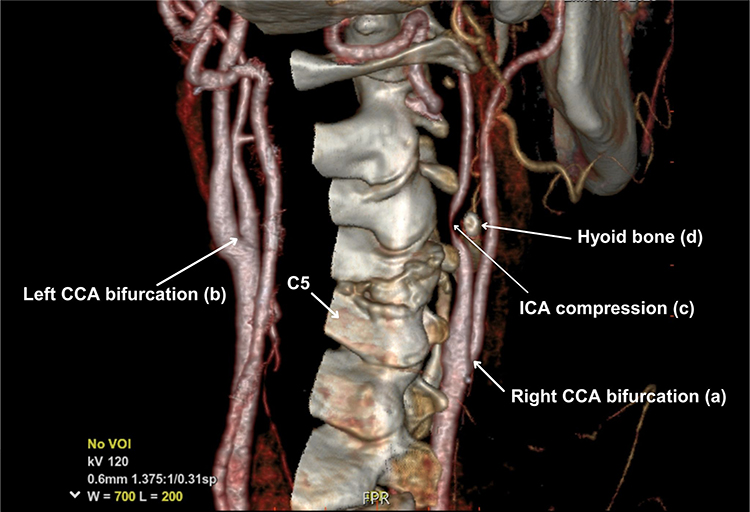 |
Figure 1 Three-dimensional reconstruction of CTA shows a low right CCA bifurcation approximately the level of the C5 – C6 vertebra (a), compared to the left side where it is at the level of C3–C4 (b). It also shows the extremely medial ICA position, with severe functional ICA compression (c) by hyoid bone (d) against the transverse vertebral processes. |
 |
Figure 2 (A) and (B): Axial (A) and multiplanar reconstruction image (B) from CTA shows extracranial ICA stenosis with the hyoid bone against the transverse vertebral processes (c). |
Cerebral angiography revealed that the diameter of the right internal carotid artery was smaller compared to the left side, and an abnormal vascular network at the base of the skull was observed, consistent with Moyamoya syndrome. Although the intracranial findings on digital subtraction angiography (DSA) closely matched those seen on CTA, the previously noted extracranial compression of the ICA by the hyoid bone was not visible (Figure 3). This discrepancy suggests functional compression, meaning that the narrowing of the artery is position-dependent and may not occur when the patient is imaged in a neutral supine position, as is typical during DSA.
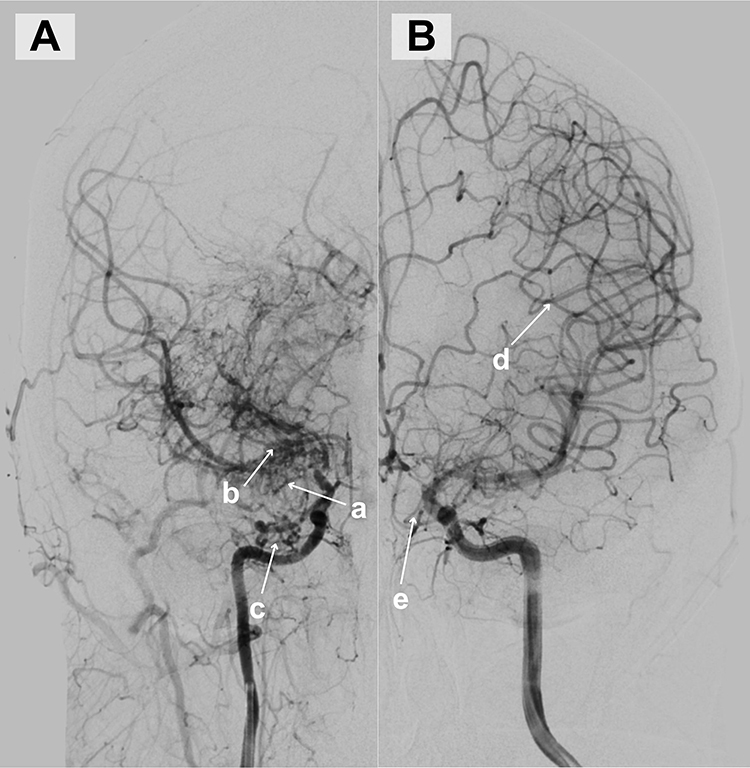 |
Figure 3 (A) DSA of the right side shows right MCA stenosis (a) with distinct collateral branches at the M1 segment (b) and a small abnormal intracranial collateral vessel network at the base of the skull indicating Moyamoya syndrome (c). (B) DSA on the left side shows good blood flow and collaterals (d), and Moyamoya vessels at the base of the skull (e). |
To further assess the right ICA, a Doppler ultrasound (US) examination of the carotid arteries was performed. It did not reveal significant stenosis or intraluminal thrombus, but showed subtle differences in flow velocities between the two sides.
As both DSA and Doppler US were conducted with the patient in relaxed, neutral positions and did not demonstrate stenosis—while CTA, likely performed in a slightly different neck or arm position, clearly showed right ICA narrowing—the diagnosis of functional ICA compression by the greater horn of the hyoid bone was established. Additionally, a low-lying bifurcation of the right CCA was noted, which may have contributed to the altered anatomical relationship and susceptibility to compression.
The patient received aspirin and was discharged with additional instructions to undergo physiotherapy aimed at improving motor skills in the right hand. Additionally, the patient was recommended to seek guidance from a neurologist regarding the future establishment of an extra-intracranial anastomosis.
In six months, the patient underwent a left-sided temporal craniotomy. An extra-intracranial anastomosis was performed between the left superficial temporal artery (frontal branch) and the left middle cerebral artery (M3/4 segment) to improve cerebral blood flow and mitigate future ischemic risks.
Discussion
The anatomical relationship between the ICA and the hyoid bone is subject to variability,10 often influenced by additional anatomical findings such as artery kinking, coiling or a low/high CCA bifurcation.4,5 Therefore, a comprehensive understanding of the variable anatomical relationships between the ICA and the hyoid bone, influenced by associated anatomical findings, is crucial for accurate diagnosis. Understanding these nuances in anatomy also underscores the importance of interdisciplinary collaboration between radiologists, neurologists, and vascular surgeons to optimize patient care pathways.
We present the first known case of an unusual combination involving a low right-sided CCA bifurcation, internal carotid artery (ICA) compression by the hyoid bone, and Moyamoya syndrome, diagnosed following an episode of ischemic stroke in a young patient. The presumed cause of the stroke lies in the interaction of these factors: vascular changes associated with Moyamoya syndrome and possible repeated mechanical irritation of the ICA wall by the hyoid bone. This may have contributed to the formation of an intimal thrombus, ultimately resulting in ischemia in the territory supplied by the anterior cerebral artery.
Our patient underwent multiple radiological examinations (CT, CTA, DSA, Doppler US carotid examination), but among these, only CTA clearly shows ICA stenosis. CTA also indicated that the CCA bifurcation on the right side was significantly lower localised (C5 - C6) compared to what is reported in the literature.1 Negative DSA and Doppler US carotid examination demonstrated that ICA stenosis occurs only in a certain position of the head.
In the literature there are variable variations on how the ICA, ECA and hyoid bone are positioned to each other, Manta et al retrospectively analysed 147 CT angiograms and classified bilateral variations of carotids–hyoid relationships in 12 possible types, where type when hyoid bone passes between ICA and ECA, as in our case, was present in only one patient of the entire group.10 Based on this study, we can conclude that such anatomical position of the ICA, ECA and hyoid bone is not entirely absent in the population, but to our knowledge, it has not yet been investigated how frequently this arrangement leads to functional stenosis or damage to the ICA and subsequent cerebrovascular events.
Few cases are known that are similar to ours,6–9 for example, Liu et al also presented a case in which hyoid bone compression of ICA caused cerebral infarction,7 Martinelli et al reported a case in which the patient had a transient ischemic attack due to right atherosclerotic plaque stenosis of the ICA presumably due to chronic ICA compression with hyoid bone.6 In all these cases, ICA stenosis with hyoid bone is most often accompanied by some other anatomical change, for example, artery kinking, coiling,4,5 long hyoid bone greater horn or as in our case with a low bifurcation of ACC. Perlman et al documented a case with a comparable anatomical configuration to ours, featuring a high CCA bifurcation (in our case low bifurcation) and narrowing of the ICA lumen due to compression by the hyoid bone.9 Abdelaziz et al presented a case report detailing an anatomical anomaly where the ICA was found to be in a reversed orientation from its usual arrangement. This unusual positioning was combined with compression of the ICA by the hyoid bone.8
Beyond the hyoid bone, a spectrum of other neck space–occupying lesions can contribute to external compression at carotid arteries. It is important to systematically exclude alternative causes of mass effect in this anatomical region. Conditions such as schwannomas, carotid bulb tumors, thyroglossal duct cysts and lymphomas represent diverse entities capable of external compression upon the arteries.11,12 Recognition of these varied contributors to arterial compression underscores the necessity for assessment to ensure accurate diagnosis and effective therapeutic interventions.
Proving a direct causal relationship between an ischemic event and the compression of the ICA by the hyoid bone, particularly in cases of functional compression, poses a considerable challenge. Often other possible factors have caused it, like atherosclerosis, cardioembolic stroke or as in our case small vessel disease as Moyamoya syndrome.13 Unlike structural compression, which may be evident through all imaging studies, functional compression involves dynamic interactions that are not easily captured in static images.
Diagnostic tools and methodologies for detecting transient changes in blood flow or dynamic alterations caused by hyoid bone positioning remain limited. Carotid Doppler examination can be useful in such cases; however, due to the rarity of these cases in the literature, there are currently no well-established or standardized functional protocols for assessing positional ICA compression with Doppler imaging. This limitation may explain why no stenosis was observed on Doppler examination in this clinical case.6
The treatment of ICA compression by the hyoid bone remains individualized, given the limited number of reported cases and the lack of standardized surgical approaches. Similar cases described in the literature have primarily involved endarterectomy, particularly when compression by the hyoid bone is associated with atherosclerotic plaque formation, and resection of the affected segment of the greater horn of the hyoid bone to prevent recurrent vascular injury.7–9 Artery stenting is generally not recommended due to complex anatomical constraints and the technical challenges associated with stent placement in this specific context.6
This case report has several limitations. First, although computed tomography angiography (CTA) revealed compression of the ICA by the hyoid bone, we were unable to confirm its positional nature using dedicated dynamic imaging or real-time ultrasound maneuvers. Second, the absence of intraluminal thrombus or significant stenosis on Doppler ultrasound DSA limits our ability to establish a direct causal relationship between the anatomical variation and the ischemic event. Third, as this is a single case report, the findings may not be generalizable. Finally, long-term follow-up data were not available at the time of manuscript preparation, limiting conclusions regarding clinical outcomes and the prognostic significance of the observed anatomical variant.
Conclusion
This case highlights the value of multimodal imaging in the evaluation of acute cerebral ischemia. While the stroke was most likely caused by Moyamoya syndrome, the incidental finding of functional compression of the ICA by the hyoid bone, along with a low carotid bifurcation, represents a rare anatomical variant with potential clinical relevance. Although not the primary cause of ischemia, this type of position-dependent vascular compression can be missed on standard imaging. CTA was key in identifying the anomaly, while DSA and Doppler ultrasound, performed in neutral positions, did not show stenosis. Recognizing such variants is important for radiologists and clinicians, as it may influence diagnostic interpretation, patient monitoring, and long-term management.
Recommendations
- Clinical Practice: This case emphasizes the importance of considering extracranial anatomical variations, such as functional ICA compression by the hyoid bone, in the differential diagnosis of cerebrovascular events—particularly in patients without classic risk factors.
- Imaging Strategy: The findings highlight the value of multimodal and positional imaging, especially CTA, in detecting dynamic vascular compressions that may not be apparent on standard Doppler ultrasound or DSA.
- Anatomical Awareness: Understanding the potential for position-dependent vascular anomalies—such as those involving a low carotid bifurcation or hyoid bone impingement—can help radiologists avoid misinterpretation of findings and identify rare but relevant contributors to cerebral ischemia.
- Interdisciplinary Collaboration: This case reinforces the importance of collaboration between radiologists, neurologists, and vascular surgeons in assessing complex stroke presentations and determining the significance of incidental anatomical findings.
Abbreviations
CCA, Common Carotid Artery; CT, Computed Tomography; CTA, Computed tomography angiography; DSA, Digital Subtraction Angiography; ECA, External Carotid Artery; ICA, Internal Carotid Artery; MCA, Middle Cerebral Artery; PCA, Posterior Cerebral Artery; US, Ultrasound.
Ethical Approval
The study was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Although institutional approval is not always required for retrospective single-patient case reports, this case was reviewed and approved by the Ethics Committee for Clinical Research at the Development Society of Pauls Stradins Clinical University Hospital (Approval number: 030225-7L), in line with internal policy and to ensure compliance with journal standards. Written informed consent for the publication of case details and accompanying images was obtained from the patient. Copies of the ethics approval and written consent form are available from the corresponding authors upon reasonable request.
Acknowledgments
We express our sincere gratitude to Riga Stradins University, particularly the Department of Radiology, for its academic support and contributions to this research.
We also extend our appreciation to Pauls Stradins Clinical University Hospital, including the Institute of Diagnostic Radiology and the Clinic of Neurology, for providing invaluable expertise, facilities, and clinical insights to our study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gulsen S, Caner H, Altinors N. An anatomical variant: low-lying bifurcation of the common carotid artery, and its surgical implications in anterior cervical discectomy. J Korean Neurosurg Soc. 2009;45(1):32–34. doi:10.3340/jkns.2009.45.1.32
2. AlJulaih GH, Menezes RG. Anatomy, Head and Neck: Hyoid Bone. Treasure Island (FL): StatPearls; 2023.
3. Gray H. Anatomy of the Human Body.
4. Sacco S, Totaro R, Baldassarre M, Carolei A. Morphological variations of the internal carotid artery: prevalence, characteristics and association with cerebrovascular disease. Int J Angiology. 2007;16(02):59. doi:10.1055/s-0031-1278249
5. Arumugam S, Subbiah NK. A Cadaveric Study on the Course of the Cervical Segment of the Internal Carotid Artery and Its Variations. Cureus. 2020. doi:10.7759/cureus.7663
6. Martinelli O, Fresilli M, Jabbour J, Di Girolamo A, Irace L. Internal Carotid Stenosis Associated with Compression by Hyoid Bone. Ann Vasc Surg. 2019;58:379.e1–379.e3. doi:10.1016/j.avsg.2018.09.043
7. Liu S, Nezami N, Dardik A, Nassiri N. Hyoid bone impingement contributing to symptomatic atherosclerosis of the carotid bifurcation. J Vasc Surg Cases Innov Tech. 2020;6(1):89–92. doi:10.1016/j.jvscit.2020.01.001
8. Abdelaziz OS, Ogilvy CS, Lev M. Is there a potential role for hyoid bone compression in pathogenesis of carotid artery stenosis? Surg Neurol. 1999;51(6):650–653. doi:10.1016/S0090-3019(99)00022-1
9. Pearlman RC, Naficy MA, Koby MB, Nyanzu M. Carotid Artery Compression by the Hyoid Bone. Vasc Endovascular Surg. 2012;46(8):686–687. doi:10.1177/1538574412460101
10. Manta MD, Rusu MC, Hostiuc S, Vrapciu AD, Manta BA, Jianu AM. The Carotid-Hyoid Topography Is Variable. Medicina. 2023;59(8):1494. doi:10.3390/medicina59081494
11. Kang J, Heo SH, Park YJ, Kim DI, Kim YW. Differential Diagnosis and Treatment Outcomes of Tumors at the Carotid Bifurcation. Vasc Specialist Int. 2020;36(3):128–135. doi:10.5758/vsi.200022
12. Corvino A, Pignata S, Campanino MR, et al. Thyroglossal duct cysts and site-specific differential diagnoses: imaging findings with emphasis on ultrasound assessment. J Ultrasound. 2020;23(2):139–149. doi:10.1007/s40477-020-00433-2
13. Nogles TE, Galuska MA. Middle Cerebral Artery Stroke. In: StatPearls - NCBI Bookshelf. 2023.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.